final ihi expedition impacting hand hygiene at the front
TRANSCRIPT

8/14/2013
1
IHI ExpeditionImpacting Hand Hygiene at the
Front Line Session 2
Tuesday, August 13, 2013
These presenters have
nothing to disclose
Lisa Maragakis, MD, MPH
Tom Talbot, MD, MPH
Diane Jacobsen, MPH, CPHQ
Today’s Host2
Max Cryns, Project Assistant, Institute for Healthcare
Improvement (IHI), assists programming activities for
hospital settings including Expeditions (2-4 month web-
based educational programs), Passport memberships,
and mentor hospital relations. He also supports IHI’s
networking and knowledge efforts. Max is currently in
the Co-Operative Education Program at Northeastern
University in Boston, MA, where he majors in Business
Administration with concentrations in Entrepreneurship
and Marketing. He enjoys professional and collegiate
sports, playing basketball, music, the beach, and trivia.
8/14/2013
2
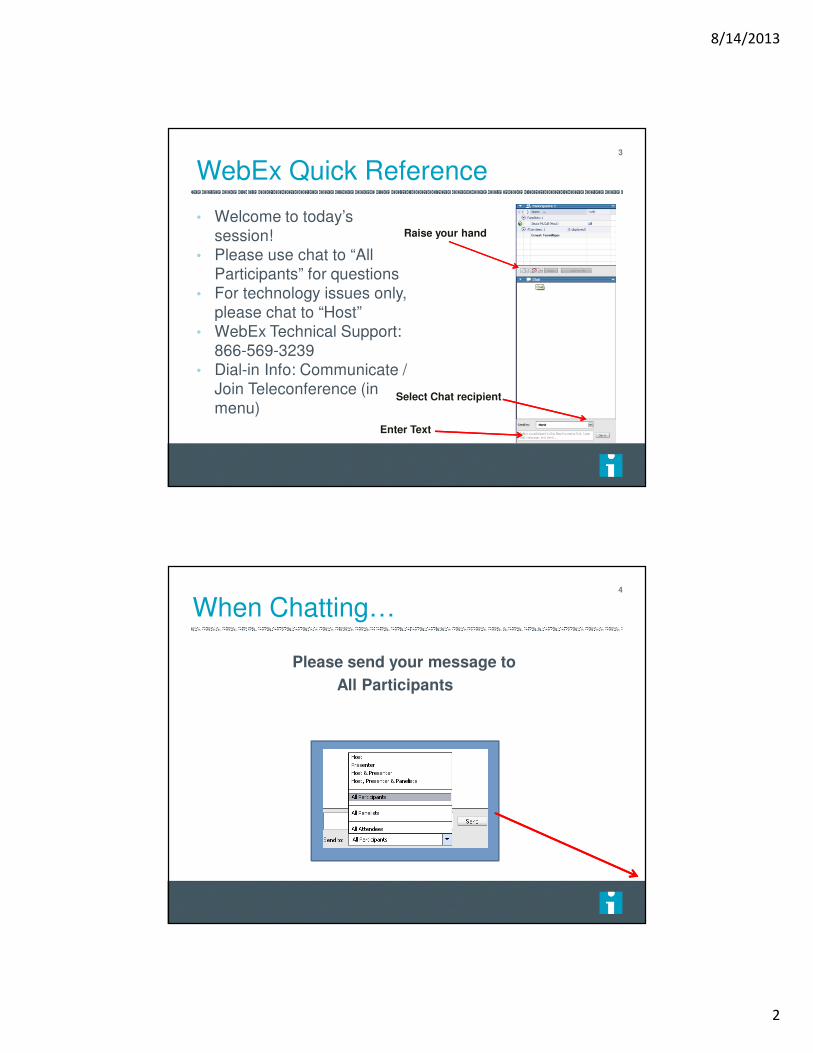
WebEx Quick Reference
• Welcome to today’s
session!
• Please use chat to “All
Participants” for questions
• For technology issues only,
please chat to “Host”
• WebEx Technical Support:
866-569-3239
• Dial-in Info: Communicate /
Join Teleconference (in
menu)
3
Raise your hand
Select Chat recipient
Enter Text
4
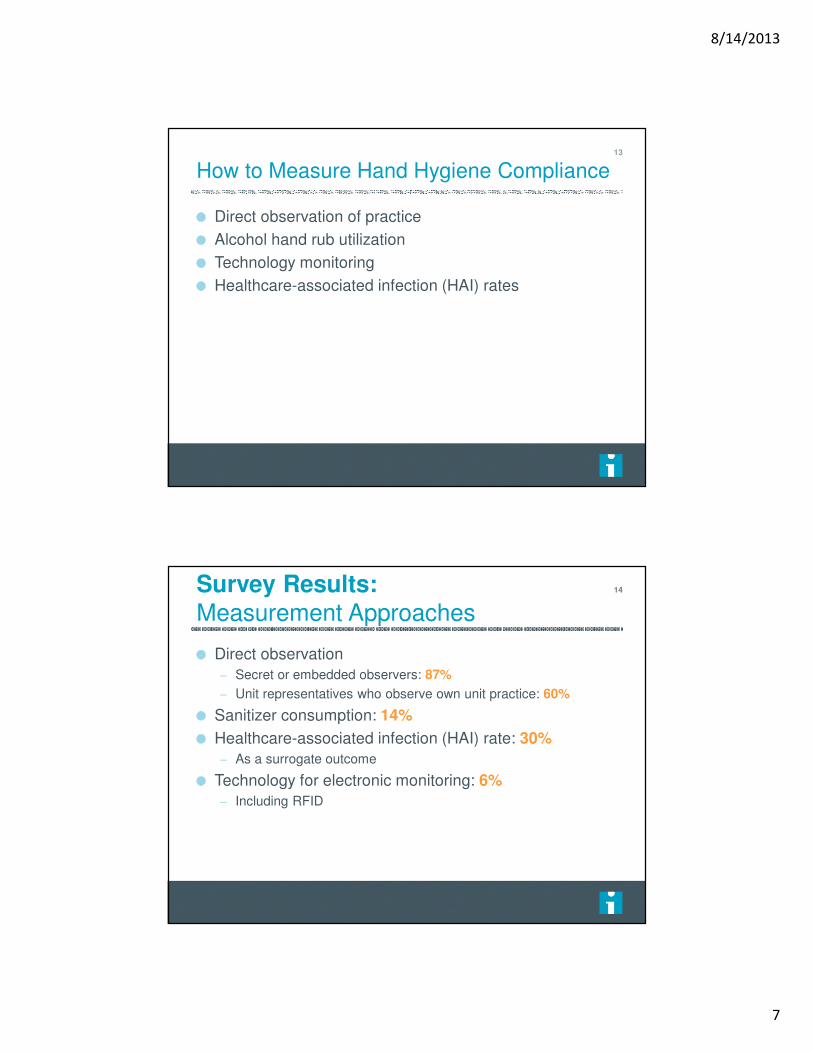
When Chatting…
Please send your message to
All Participants

8/14/2013
3
Expedition Director5
Diane Jacobsen, MPH, CPHQ, Director, Institute for Healthcare Improvement (IHI) is currently directing the CDC/IHI Antibiotic Stewardship Initiative, NSLIJ/IHI Reducing Sepsis Mortality Collaborative. Ms Jacobsen served as IHI content lead and improvement advisor for the California Healthcare-Associated Infection Prevention Initiative (CHAIPI) and directed Expeditions on Antibiotic Stewardship, Preventing CA-UTIs, Reducing C. difficileInfections, Sepsis, Stroke Care and Patient Flow. She served as faculty for IHI’s 100,000 Lives and 5 Million Lives Campaign and directed improvement collaboratives on Sepsis Mortality, Patient Flow, Surgical Complications, Reducing Hospital Mortality Rates (HSMR) and co-directed IHI's Spread Initiative She is an epidemiologist with experience in quality improvement, risk management, and infection control in specialty, academic, and community hospitals. A graduate of the University of Wisconsin, she earned her master's degree in Public Health-Epidemiology. from the University of Minnesota.
Today’s Agenda6
Introductions
Debrief Action Period Assignment
Measurement Approaches
Action Period Assignment

8/14/2013
4
Schedule of Calls
Session 1 – Call to Action for Hand HygieneDate: Tuesday, July 30, 2:30 PM – 4:00 PM ET
Session 2 – Measurement ApproachesDate: Tuesday, August 13, 2:30 PM – 3:30 PM ET
Session 3 – Supplies, Equipment, and the EnvironmentDate: Tuesday, August 27, 2:30 PM – 3:30 PM ET
Session 4 – Leadership and Culture for Hand HygieneDate: Tuesday, September 10, 2:30 PM – 3:30 PM ET
Session 5 – Frontline EngagementDate: Tuesday, September 24, 2:30 PM – 3:30 PM ET
Session 6 – Marketing and Communications Campaigns
Date: Tuesday, October 8, 2:30 PM – 3:30 PM ET
7
Faculty8
Tom Talbot, MD, MPH, FSHEA, FIDSA, Associate
Professor of Medicine and Preventive Medicine,
Vanderbilt University School of Medicine and Chief
Hospital Epidemiologist, Vanderbilt University Medical
Center, conducts research on healthcare epidemiology
and infection control and oversees healthcare-
associated infection prevention programs. Dr. Talbot
currently serves as a member of the Centers for
Disease Control and Prevention’s Healthcare Infection
Control Practices Advisory Committee (HICPAC).

8/14/2013
5
Faculty9
Lisa Maragakis, MD, MPH is an Assistant Professor of Medicine at The Johns Hopkins University, Department of Medicine, Division of Infectious Diseases and the Hospital Epidemiologist and Director of the Department of Hospital Epidemiology and Infection Control at The Johns Hopkins Hospital. She received her medical degree and post-doctoral Infectious Diseases training at The Johns Hopkins University School of Medicine and a master’s degree in public health from The Johns Hopkins University Bloomberg School of Public Health. She recently served as a Councilor on the Board of Directors of the Society for Healthcare Epidemiology of America (SHEA), as Vice-Chair of the SHEA Guidelines Committee and as the liaison representing SHEA to the Healthcare Infection Control Practices Advisory Committee at the Centers for Disease Control and Prevention. Her research interest is the epidemiology, prevention and control of healthcare-acquired infections caused by antimicrobial-resistant gram negative bacilli.
Debrief: Action Period Assignment
Complete 3 to 5 hand hygiene observations on one unit using the data collection tool provided by the Joint Commission (will be distributed on the listserv after the call) OR your organization’s current data collection tool– If using the Joint Commission tool, Watch “Improving Care
with Targeted Solutions Tool (TST)” video (6 minutes) http://www.centerfortransforminghealthcare.org/multimedia/improving-care-with-the-tst/
Based on what you observed, brainstorm ideas you could test to address current barriers to hand hygiene– Consider: visibility and availability of soap, visual reminders or
prompts, workflow obstacles related to availability and location of supplies, pace on the unit, etc.
10

8/14/2013
6
IHI Hand Hygiene Expedition
Measurement Approaches
Tom Talbot, MD, MPH
Why Measure Hand Hygiene Compliance?
To understand performance
To use data to change behaviors
To assess impact of interventions
12
8/14/2013
7
How to Measure Hand Hygiene Compliance
Direct observation of practice
Alcohol hand rub utilization
Technology monitoring
Healthcare-associated infection (HAI) rates
13
Survey Results:Measurement Approaches
Direct observation
– Secret or embedded observers: 87%
– Unit representatives who observe own unit practice: 60%
Sanitizer consumption: 14%
Healthcare-associated infection (HAI) rate: 30%
– As a surrogate outcome
Technology for electronic monitoring: 6%
– Including RFID
14
8/14/2013
8
Direct Observation
“Gold Standard”
Many different flavors:
– Audit own area vs. other
– Embedded vs. announced
– Different individuals: Employees (restricted work duty?),
students, visitors
Observe with correction or without?
How detailed?
– WHO 5 moments? Duration of wash? Amount of foam used?
15
Poll Question
For those that use direct observation, do you use secret
shoppers/embedded observers?
A. Yes
B. No
C. N/A – my organization does not use direct
observation
16

8/14/2013
9
Direct Observation
PROS:
Direct assessment of
practice
Can capture details of
behavior (empty foam
canisters, poor compliance
with glove use)
Raises awareness of
observer to poor
compliance
CONS:
Hawthorne effect
Observer bias (only see
compliance?)
Inter-rater reliability
Resource intensive
17
Changing the Observer Pool @ VUMC:
Shared Responsibility
Every inpatient and outpatient unit/clinic committed one
person as observer (often a manager)
Observers assigned to different area
Expected to perform 20 opportunities/month
Aims:
– Prioritize this program
– Shared responsibility
– Lessons learned from observing one
area are taken back to to
“home” unit
18

8/14/2013
10
Poll Question
For those that use direct observation, do you use
patients to collect data?
A. Yes
B. No
C. N/A – my organization does not use direct
observation
19
Patients as Observers?
What about engaging the
patient?
Concern about patient-
provider relationship
Grodon SC JAMA 2012;307:1591 + Longtin Y Arch Intern Med 2012
20

8/14/2013
11
Alcohol Hand Rub Consumption
• Using changes in utilization of alcohol hand
rub as marker for hand hygiene compliance
rates
Location Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
VUH
VUH Hand Hygeine
Campaign
SICU 48 64 45 48 17 47 25 35 29 33 44 10
Gyn Surg 0 0 0 0 14 0 0 0 1 3 6 0
11N
? Uses
foam
only
ED 18 42 60 18 18 24 48 37 45 52 56 6
GI Endo 0 0 0 0 0 0 0 0 0 0 24 0
21
Alcohol Hand Rub Consumption
PROS:
Cheap
Indicates usage
More
objective/standardized
Lacks selection bias
CONS:
How to account for bulk
purchasing
No assessment of timing
of hand hygiene
Cannot drill down to
specific group usage (e.g.
nursing vs. physicians)
Denominator?
Less tangible
22

8/14/2013
12
Technology Monitoring23
Technology Monitoring
RFID tied to dispenser
Alcohol sensors
Visual alerting (vibration)
24
8/14/2013
13
Technology Monitoring
PROS:
Large number of
observations
Reduces observer bias
Drill down to provider level
Not biased to specific
times/days
CONS:
Expensive
Clunky
May involve added
procedures to workflow or
equipment tracking
Sensor errors
Issues re: tracking
personal behaviors (Big
Brother)
25
HAI Rates
PROS:
Tangible, credible outcome
May help gain buy-in
CONS:
Impacted by other
practices
Not often available for all
practice settings (e.g.
clinics)
26

8/14/2013
14
Deciding on Measurement
Gain consensus
– Allow for input and trial
– Give people some “skin in the game”
Be pragmatic/practical
Consider excluding some areas/practices in order to
improve buy-in
– e.g. VUMC dermatology clinic/Mohs surgery
27
28

8/14/2013
15
29
Dealing with Challenges to the
Measurements
Your measurement could be imperfect or wrong
– Observer interpretation
– Failure to account for nuances in specific practice settings
E.g., trauma unit ICU door, room-to-room
30

8/14/2013
16
Dealing with Challenges to the
Measurements
Your measurement could be correct but poor
performance could be blamed on misperceptions about
the measurement
E.g., emergency department “status report”
31
Unintended Consequences of
Measurement
Observer fatigue/data entry
Provider behavior changes to
meet measurement
– Using foam outside room to count
for measurement AND using sink
inside room
32
8/14/2013
17
Poll Question
Do you collect names of those persons noted to be non-compliant with hand hygiene?
A. Yes
B. No
If you do not collect names, have you been asked to collect names of those persons noted to be non-compliant with hand hygiene?
A. Yes
B. No
C. N/A – my organization collect names
33
Taking Names
Addressing non-compliance by
identifying specific persons
Assumes issue is due to limited few
Within spirit of just culture?
– All persons equally under surveillance?
If responds unprofessionally to
reminder � different issue
34

8/14/2013
18
Now You’ve Measured. Now What?
Feedback the performance
Make it simple, clear, visual
Peer comparison good if done with right context/intent
Public display of data?
35
Split by PDF Splitter Hand Hygiene Compliance Report VUH Hand Hygiene FYTD Compliance by Unit
VUH Compliance Fiscal Year to Date Amber
Bar = Your Unit TVC HR/PACU Monday, January 31, 2011 www.mc.vanderbilt.edu/handhygiene Page 24 of 35

8/14/2013
19
Groups with Compliance Above Target (≥92%)
HAND HYGIENE COMPLIANCE FY13 to Date SUMMARY:
Type of Person Observed: INPATIENT
Groups with Compliance Between Threshold & Target (88-91%)
Groups with Compliance Below Threshold (<88%)
Group 1 PhysiciansCare Partners
EVSMedical Students
ED Nursing
NursingAnesthesiologists
Nurse PractitionersCRNA
Pt Care TechsSurgical Techs
* Must have at least 50 observations for current FY to be included
Nutrition SvcsPhys Therapy
SurgeonsTransport Svcs
Group 2 PhysiciansLPNs
Xray TechsAnesthesia TechNuc Med TechsRadiology Techs
Based on FY13 Compliance Data (July 2012 – January 2013)37
Other Concerns
Dealing with the Hawthorne Effect
Dealing with sample size (low N)
Dealing with “want to show patients that I washed my
hands” concern
Setting a goal
– Is 100% possible with your method or are you setting up for
failure?
38

8/14/2013
20
Questions?39
Raise your hand
Use the Chat
Insights from John’s Hopkins
At the beginning of our campaign, it was incredibly
important (& somewhat difficult) to get buy-in from key
stakeholders and frontline staff about our measurement
methodology & it took a fair amount of time (months to a
year)
Unit self-monitoring was a great way to get buy-in and
overcome objections about the measurement method
(I.e. Skeptical staff or leaders can see for themselves
that HH is not happening consistently and they become
advocates for HH improvement)
40

8/14/2013
21
Insights from John’s Hopkins
Needed to address a variety of special circumstances for
measurement clarity and consistency:
e.g. Transporters pushing patients across threshold; PT
assisting patients across threshold; nutrition or others
carrying things across threshold; open areas with curtain
dividers like the ED or PACU
Staff initially wanted to be able to enter the doorway to
speak to a patient without washing; we offered a "red
line" box as a "safe zone" just inside the door but
ultimately staff said that they did not want this for a
variety of reasons
41
Insights from John’s Hopkins
Use the "IN and OUT" methodology of measurement
Standardization of the measurement was very important
(training video for observers; standard data collection
forms; definitions; doubling checking observer data and
methods when outliers were found)
Good documentation, record keeping and open
communication was essential to build trust in the
measurement methodology
42

8/14/2013
22
Questions or Comments?43
Raise your hand
Use the Chat
Action Period Assignment
Test holding measurement rounds
– Identify a unit with low compliance or challenges getting buy-in with hand hygiene
– Schedule a time to round with key leader(s) on the unit (i.e., Nurse Manager, Medical director, Hospitalist)
– Spend ~15 min rounding on the unit
– Elicit feedback about barriers to measurement
– Identify the obstacles to hand hygiene and identify 1 PDSA cycle
Come prepared to share your insights and learning at
Session 3
44

8/14/2013
23
Expedition Communications
Listserv for session communications:
To add colleagues, email us at [email protected]
Pose questions, share resources, discuss barriers or
successes
45
Next Session
Tuesday, August 27, 2:30 PM – 3:30 PM ET
Session 3 –Supplies, Equipment & the Environment
46