final clinical req 4.19 - genesisnms red top g gray top sst lavender tube s blue top b u urine st...
TRANSCRIPT

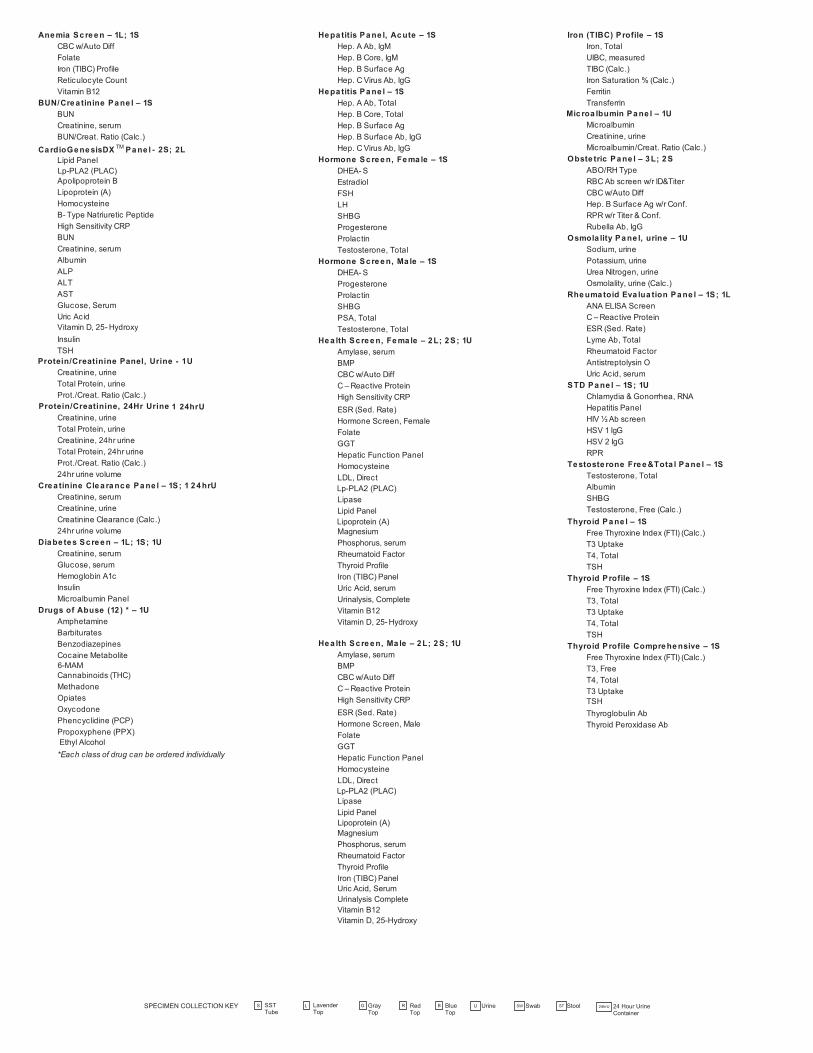
Cholesterol, Triglycerides, HDL, LDL, Cholesterol/HDL Ratio
Na, K, Cl, CO2, Ca, Creatinine, Glucose, BUN Na, K, CO2, Creatinine, Glucose, BUN, Alk. Phos., Albumin, Total Bilirubin, Total Protein, AST, ALT, Calcium
Albumin, Alk. Phos., ALT, AST, Total Bilirubin, Direct Bilirubin, Total Protein
Na, K, Cl, CO2 Na, K, Cl, CO2, Ca, Creatinine, Glucose, BUN, Albumin, Phosphorus
RENAL FUNCTION PANELELECTROLYTE PANELHEPATIC FUNCTION BASIC METABOLIC COMPREHENSIVE METABOLICLIPID PANEL
PATIENT INFORMATION
INSURANCE INFORMATION
TESTS AND PROFILES
ICD-10 DX CODES
CUSTOM PROFILES AND ADDITIONAL INSTRUCTIONS
ADDRESS
POLICY NUMBER
PATIENT RELATIONSHIP TO INSURED:
DATE OF BIRTH (MM/DD/YYYY)
FIRST NAME
CITY
SEX
MIDDLE INITIAL
STATE
SOCIAL SECURITY NUMBER
ZIP
PHONE (H)
SELF SPOUSE DEPENDANT
PATIENT SIGN HEREI hereby assign all rights and benefits under my health plan and all rights and obligations that I and my dependents have under my health plan to Genesis Diagnostics, its assigned affiliates and their authorized representatives for laboratory services furnished to meby Genesis Diagnostics. I irrevocably designate, authorize and appoint Genesis Diagnostics or its assigned affiliates and their authorized representatives as my true and lawful attorney-in-fact for the purpose of submitting my claims, obtain a copy of my health plandocument and SPD and pursuing any request, disclosure, appeal, litigation or other remedies in accordance with the benefits and rights under my health plan and in accordance with any federal or state laws. If my health plan fails to abide by my authorization andmakes payment directly to me, I agree to endorse the insurance check and forward it to Genesis Diagnostics immediately upon receipt. I hereby authorize Genesis Diagnostics, its assigned affiliates and authorized representatives to contact me or my health plan/administrator for billing or payment purposes by phone, text message, or email with the contact information that I have provided to Genesis Diagnostics, in compliance with federal and state laws. Genesis Diagnostics, its assigned affiliates and their authorizedrepresentatives may release to my health plan, their plan administrator, my employer and my authorized representative my personal health information for the purpose of procuring payment of my Genesis Diagnostic laboratory and toxicology claims. I understandacceptance of insurance does not relieve me from any responsibility concerning payment for laboratory services and that I am financially responsible for all charges whether or not they are covered by my insurance
STOP
ORDERING PHYSICIAN SIGN HERESTOP
Signature of Patient or Patient Representative / Relationship to Patient Date
Ordering Physician Signature Date
Creatinine, Urine
Physician must only order tests that are medically necessary for the diagnosis or treatment of a patient.
CLIA # 39D1099562 | 900 Town Center Dr, Ste H50, Langhorne, PA 19047TEL: (267) 212-2000 | FAX: (267) 212-2005 | www.genesisdx.com
Date Collected:_____________ Time Collected: _________________
LAST NAME
Commercial Medicare Medicaid Bill Patient Bill Client W/C (Date of injury):_____________
NAME OF INSURED (IF DIFFERENT FROM PATIENT)
PRIMARY INSURANCE NAME AND PLAN
EMPLOYER/GROUP NAME
(1SST) (1SST) (1SST) (1SST) (1SST) (1SST)
Please ensure Custom Panel has been established on new account form. Please refer to back of this form for a listing of tests in each panel. By ordering the custom profile on file, the ordering physician acknowledges, by signing below, laboratory tests being ordered are reasonable and necessary for the named patient. The ordering physician understands that they may change the custom profile on a case-by-case basis, by making their testing preferences clear in the space below.
ORDERING PHYSICIAN INFORMATION
123456__________
123456__________
123456__________
123456__________
123456__________
123456__________
DIAGNOSTIC PANEL*
Hep. B surface Ag w/Conf. S
HDL-Cholesterol S
HCG, Qual. S
Rheumatoid Factor S
Anemia Screen 1L; 1S Hep. B surface Ab, IgG S
Hemoglobin A1c L
Estradiol S
RPR S
CardioGenesisDXTM Panel 2S; 2L Hep. C Ab, IgG S
Homocysteine S
FSH S
Rubella Ab, IgG S
Protein/Creatinine Panel, Urine 1UCHEMISTRY
Iron, Total S
LH S
VZV Ab, IgG S
Diabetes Screen 1L; 1S; 1U Albumin S
LDL, direct S
Progesterone S
Thyroglobulin Ab S Alkaline Phos. S
Lipase
Lp-PLA2 (PLAC)
SS
Prolactin S
Thyroid Peroxidase Ab S Hormone Screen, Female 1S ALT S
Magnesium
S
PTH Intact S
MICROBIOLOGY Hormone Screen, Male 1S AST S
Potassium, serum
S
SHBG S
C&S, Urine U Health Screen, Female 2L; 2S; 1U
Amylase, serum S Ammonia L
Prealbumin
S
T3, Free S
Occult Blood, Stool ST Health Screen, Male 2L; 2S; 1U
Apolipoprotein A1 S
Protein, Total S
T3, Total S
URINE Hepatitis Panel 1S
Apolipoprotein B S
S
Sodium S
T3 UptakeT3, Reverse
S
Microalbumin U Hepatitis Panel, Acute 1S
Bilirubin, Direct S
Triglyceride S
T4, Free
SS
Creatinine, Urine U Microalbumin Panel 1U
Bilirubin, Total S
Transferrin S
Testosterone, Total S
Total Protein, Urine U Obstetric Panel 3L; 2S
BUN S
Uric Acid, serum S
TSH (Hypersensitive) S
Urinalysis, Complete U Rheumatoid Evaluation Panel 1S; 1L
B-Type Natriuretic Peptide L
Vitamin D 25 - Hydroxy S
TSH w/r T4, Free S
Urinalysis w/r Culture U STD Panel 1S; 1U
Calcium S
Vitamin B12 SIMMUNOLOGY
TOXICOLOGY Thyroid Panel 1S Carbon Dioxide (CO2) S
HEMATOLOGY
Antistreptolysin O S
Digoxin R 1S Chloride (Cl), serum S
CBC w/Auto Diff L
CRP (High Sensitivity) SC-Reactive Protein S
Lithium S 1S Cholesterol S
CBC wo/Auto Diff L
Phenytoin R 1S Creatine Kinase S
Hemoglobin & Hematocrit L
Valproic Acid R Testerone Free & Total Panel 1S Creatinine, serum S
Sedimentation Rate (ESR) L
Drugs of Abuse (12) UHIV SCREENING
HEPATITIS SCREENING
Cystatin C S
Reticulocyte Count L
TUMOR MARKERS HIV 1/2 Ab/Ag Combo Screen S Ferritin S
PT/INR B
HSV 1 IgG AFP SHEPATITIS SCREENING Folic Acid (Folate) S
APTT B
HSV 2 IgG
SCEA S
Hep. A
Ab, IgM S
Fasting Blood Sugar G
ENDOCRINOLOGY
Lyme
Ab,
Total
S
PSA, Total S Hep.
A
Abs,
Total S
GGT S
Cortisol, Total S
Measles
Ab, IgG
S
PSA, Free & Total S Hep. B Core, IgM S
Glucose, serum S
DHEA-S S
S
Hep. B Core, Total S
GlycoMark® S
βHCG, Quant. S
Mumps Ab, IgG S Other _________________
Other _________________
Lipoprotein (A)
FORMREQ
001-REV
04232019NMS
RedTop
G GrayTop
LavenderTop
SST Tube
S Blue Top
B U Urine StoolST 24hrU 24 Hour Urine Container
SwabSWRL
Protein/Creatinine, 24Hr Urine
Uric Acid, SerumUrinalysis CompleteVitamin B12Vitamin D, 25-Hydroxy
Ethyl Alcohol
Lp-PLA2 (PLAC)
Lp-PLA2 (PLAC)
6-MAM
Lp-PLA2 (PLAC)
Lipoprotein (A)
Lipoprotein (A)
Protein/Creatinine Panel, Urine - 1U
1 24hrU
- 2S; 2L
*Each class of drug can be ordered individually