fetal monitoring dr. anjoo agarwal professor dept of obs & gyn kgmu, lucknow
TRANSCRIPT

Fetal Monitoring
Dr. Anjoo AgarwalProfessorDept of Obs & gynKGMU, Lucknow
Objectives
• Understand aims of fetal monitoring• Understand methods of fetal monitoring• Understand limitations of fetal monitoring
Aims of Fetal Monitoring
• Prevention of fetal death• Avoidance of unnecessary interventions
ACOG, AAP 2012
• 23 yrs old woman G2P1+0 (1st FTND, A&H) presents at 38 wks pregnancy with C/o diminished fetal moments since 2 days.
Q. How significant do you think the problem is & what should be your next step?

Significance
• Diminished fetal activity, may be a harbinger of impending fetal death
Sadovsky, 1973

Low Risk vs High Risk
• Any pregnancy may become high risk any time• C/o diminished fetal activity important in all
cases
Role of Gestation ?
• Fetal activity starts at 7 wks• General body movements become organised
20-30 wks• Fetal movement maturation continues till 36
wks• Criteria for interpretation of tests varies with
gestation• Fetal viability an important consideration

Methods of Assessment
Antepartum :− DFMC− NST− CST− Biophysical Profile− Doppler VelocimetryIntrapartum:− External or Indirect− Internal or Direct− Fetal scalp blood sampling

DFMC
• Cardiff “Count to 10”• One hour after each meal

NST
• FHR Acceleration in response to fetal movements
• Test of fetal conditionNormal – reactiveAbnormal – non reactive

Reactive NST
• ≥ 32 weeks – 2 accelerations ≥ 15 bpm ≥ 15 sec during 20 min
• < 32 wks – 2 accelerations ≥ 10 bpm ≥ 10 sec during 20 min

Fetal Heart Rate Acceleration

Electronic Fetal MonitoringPattern Definition
Baseline • The mean FHR rounded to increments of 5 bpm during a 10 min segment, excluding−Periodic & episodic changes−Segment of baseline that differ by more than 25 bpm
• The baseline must be for a minimum 2 min in any 10 min segment or the baseline for that time period is indeterminate. In this case, one may refer to the prior 10 min window to determine of baseline• Normal FHR baseline: 110 – 160 bpm• Tachycardia: FHR baseline > 160 bpm• Bradycardia: FHR baseline < 110 bpm• Fluctuations in the baseline FHR that are irregular in amplitude & frequency
Baseline Variability
•Variability is visually quantified as the amplitude of peak-to-trough in bpm− Absent – amplitude range undetectable− Minimal – amplitude range detectable but ≤ 5 bpm or fewer− Moderate – amplitude range 6-25 bpm− Marked – amplitude range > 25 bpm
Acceleration • A visually apparent abrupt increase (onset to peak in < 30 sec) in the FHR• At 32 wks & beyond, an acceleration has a peak of 15 bpm or more have baseline, with a duration
or more but less than 2 min from onset to return• Before 32 wks, an acceleration has a peak of 10 bpm or more above baseline, with a duration of
≥ 10 sec < 2 min from onset to return• Prolonged acceleration lasts ≥ 2 min but < 10 min• If an acceleration last 10 min, it is a baseline change• Visually apparent usually symmetrical gradual decrease & return of the FHR associated with a
uterine contraction


No Variability

Minimal Variability

Moderate Variability
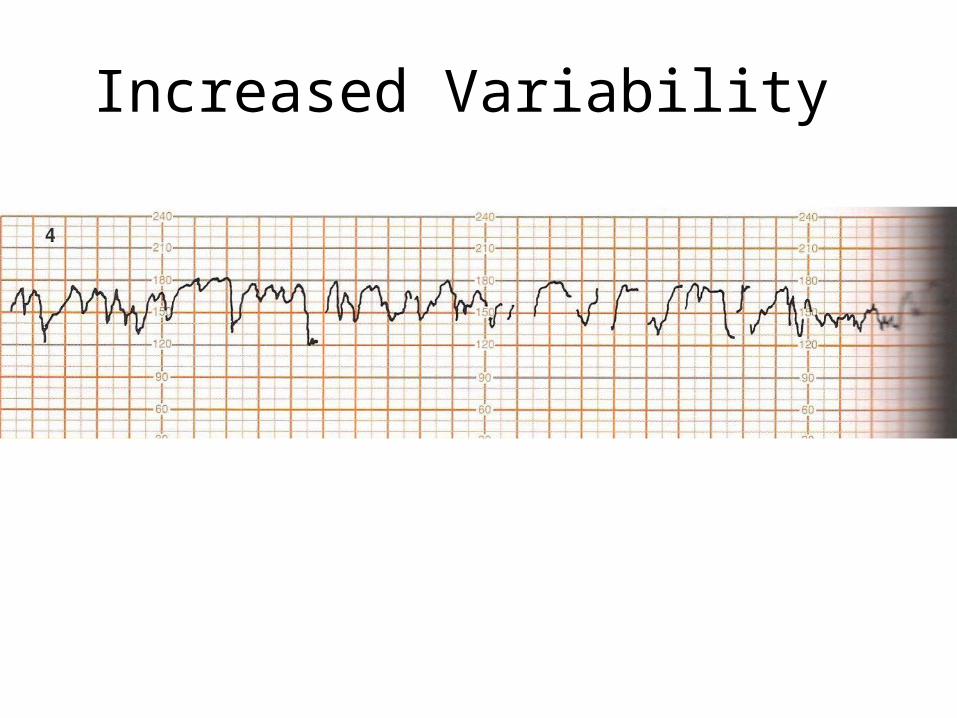
Increased Variability

Saltatory Pattern

CST/OCT
• Tests uteroplacental function contraction stimulated by oxytocin infusion
• Late decelerations indicate positive test

Biophysical Profile
• Nonstress test• Fetal breathing• Fetal movement• Fetal tone• Amniotic fluid volume

Modified Biophysical Profile
• NST + AFI (cut off 5 cm)

Doppler Velocimetry
• Umbilical artery• MCA• Ductus Venosus

Umbilical Artery Doppler
• Abnormal if – • S/D > 95% percentile for GA• Absent end diastolic flow – 10% PM• Reversed end diastolic flow – 33% PM• Utility only in FGR

MCA
• Fetal Hypoxia → brain sparing → ↑ Cerebro vascular resistance (RI)
• Also useful in fetal anaemia where ↑ PSV
Ductus Venosus
• Good correlation with perinatal outcome• But by the time affected it is too late• Still in experimental stage

Final Recommendations
• Start at 32-34 weeks in HR cases• Severe complications may require testing at
26-28 weeks• Repeat weekly/ every 7 days• Most commonly used – modified biophysical
profile
MCQ
NST is used to test1 uteroplacental bloodflow2 fetal condition3 response to uterine contractions4 fetal anaemia

MCQ
A 35 yr old G1 P0+0 presents at 34 wks with GDM. It is recommended that she be monitored by
1 weekly NST2 DFMC3 Daily doppler4 all of the above

MCQ
The acceleration of FHR in NST should be of1 at least 20 min duration 2 at least 20 sec duration3 at least 15 sec duration4 at least 15 min duration