femoral shaft-fractures
TRANSCRIPT

Case DiscussionBY EXT.JIRAWATH ASSAWADARACHAI
Patient profile
Chief Complaint
ขบัรถจกัรยานยนตช์นรถยนต ์1 ช ัว่โมงกอ่นมารพ.
Initial management
Primary survey
A : spontaneous speech,no cervical tenderness
B : clear both lung,CCT negative
C : BP 115/68 mmHg , P 94 /min,PCT negative
D : E4V5M6,pupil 3 mm RTLBE

Secondary survey
History
A : ไม่มปีระวตัแิพย้า แพอ้าหาร
M : ไม่มยีาประจ า
P : no underlying disease
L : ทานขา้วลา่สดุตอน 12.00 น.
E : 1 ช ัว่โมง กอ่นมารพ. ผูป่้วยขีร่ถจกัรยานยนตผ่์านสีแ่ยกไปชนกบั
รถยนต ์สลบ หลงัมสีตไิม่มคีลืน่ไส ้อาเจยีน ไม่ปวดศรีษะ ไม่ปวด
คอ ไม่เจ็บหนา้อก ไม่ปวดทอ้ง ไม่มเีลอืดไหลออกจากจมูก/ห ูมี
อาการเจ็บทีต่น้ขาขวา ลกุขึน้เดนิไม่ได ้ยงัสามารถขยบัขอ้เทา้ได ้
Physical examination
V/S : T 37 C,BP 115/68 mmHg,P 94/min,RR 20/min,BW 45
kg
GA : A Thai girl,good consciousness,look fatigue
HEENT : not pale conjunctiva,anicteric sclera
Chest : normal breath sound,no adventitious sound
Heart : normal s1,s2,no murmur
Abdomen : soft,not tender
Neuro : E4V5M6,pupil 3 mm RTLBE,motor power grade V
all extremities,sensory grossly intact
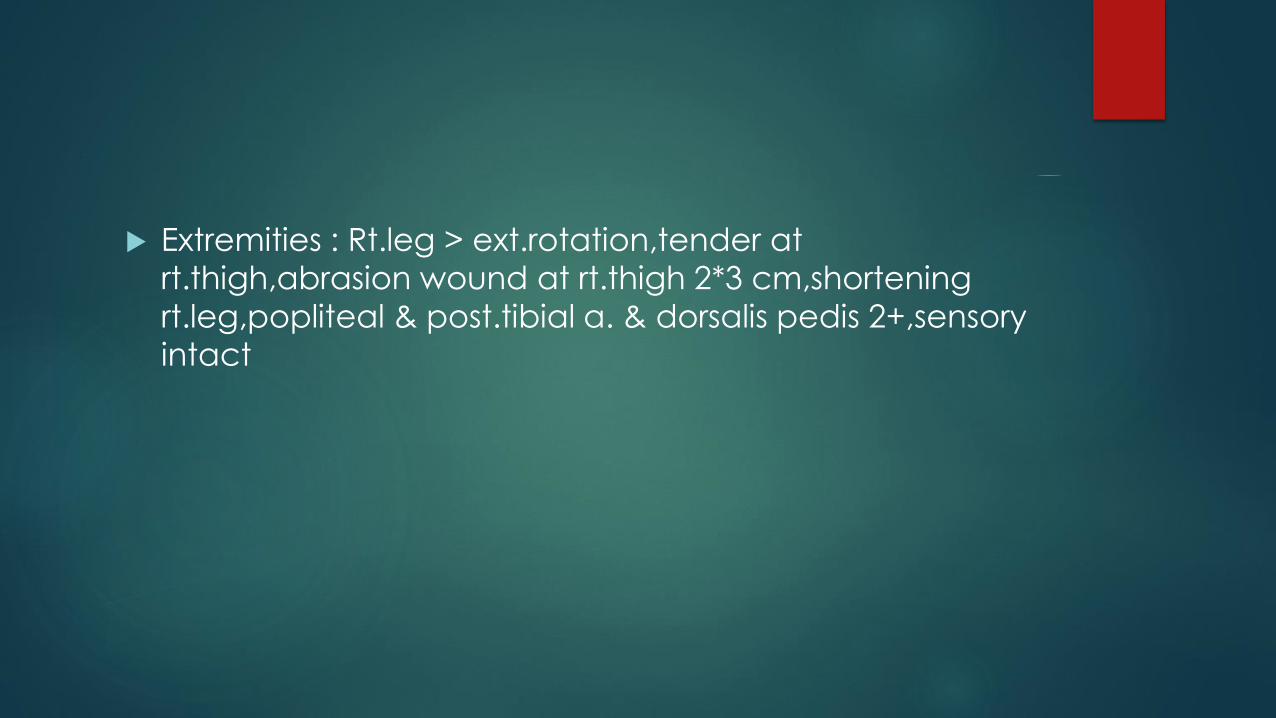
Extremities : Rt.leg > ext.rotation,tender at
rt.thigh,abrasion wound at rt.thigh 2*3 cm,shortening
rt.leg,popliteal & post.tibial a. & dorsalis pedis 2+,sensory intact

Investigation
Film Rt.femur AP/Lat
Film pelvis AP
Film Rt.knee AP/Lat
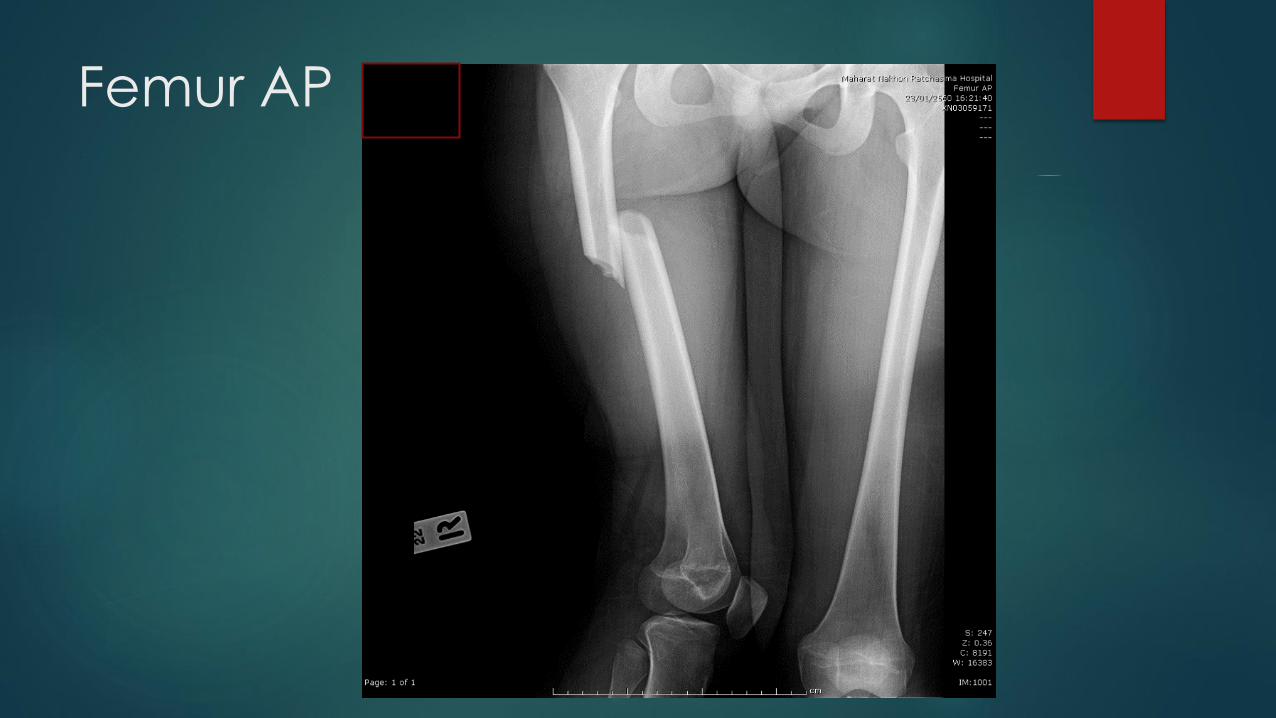
Femur AP
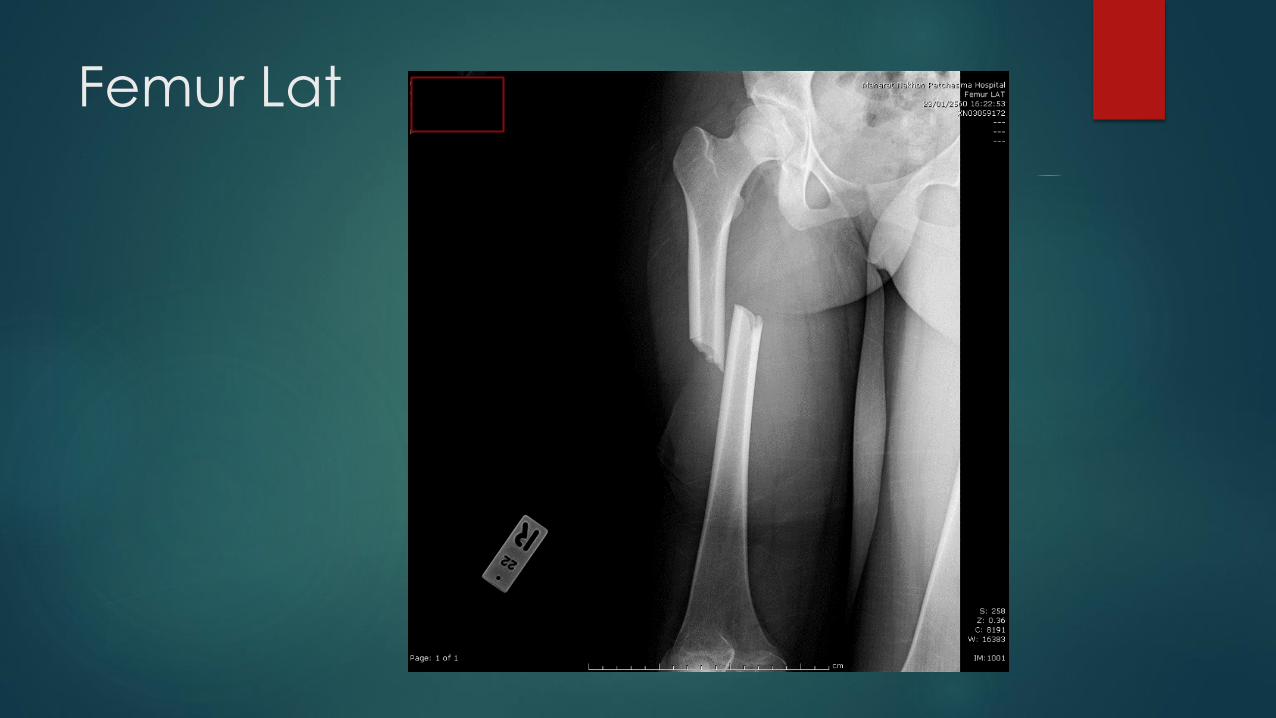
Femur Lat
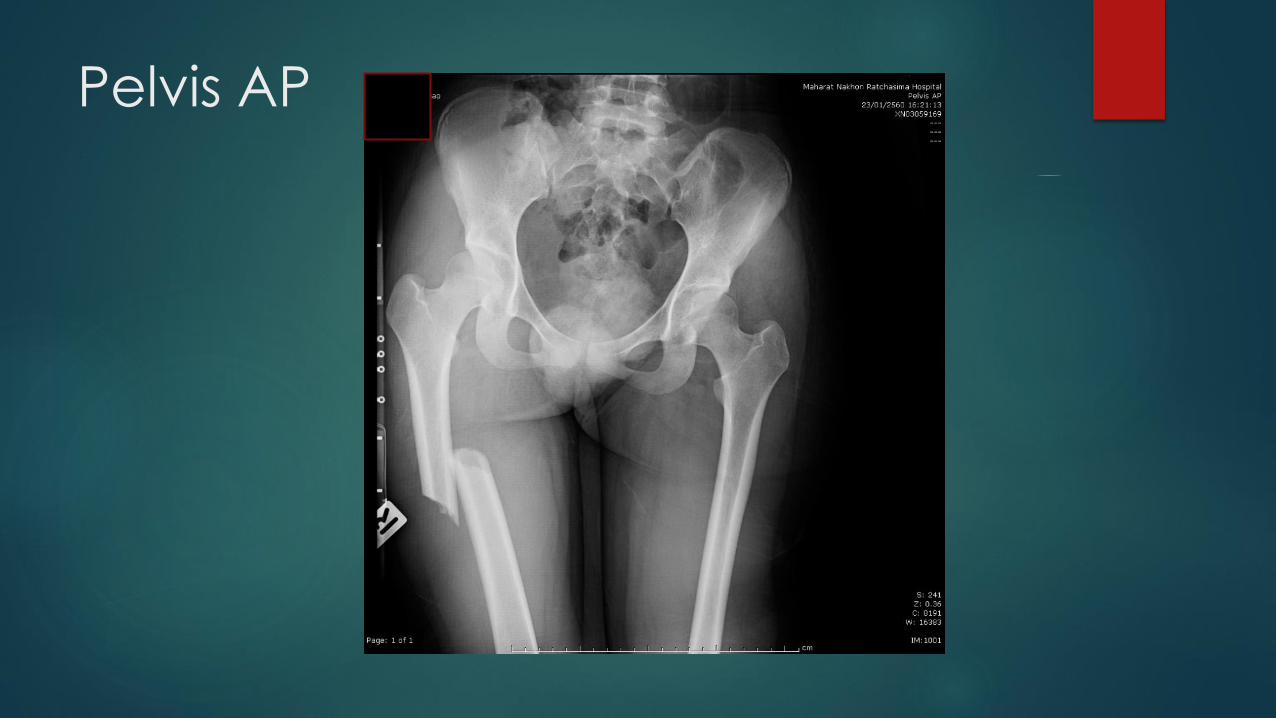
Pelvis AP

Knee AP

Knee Lat
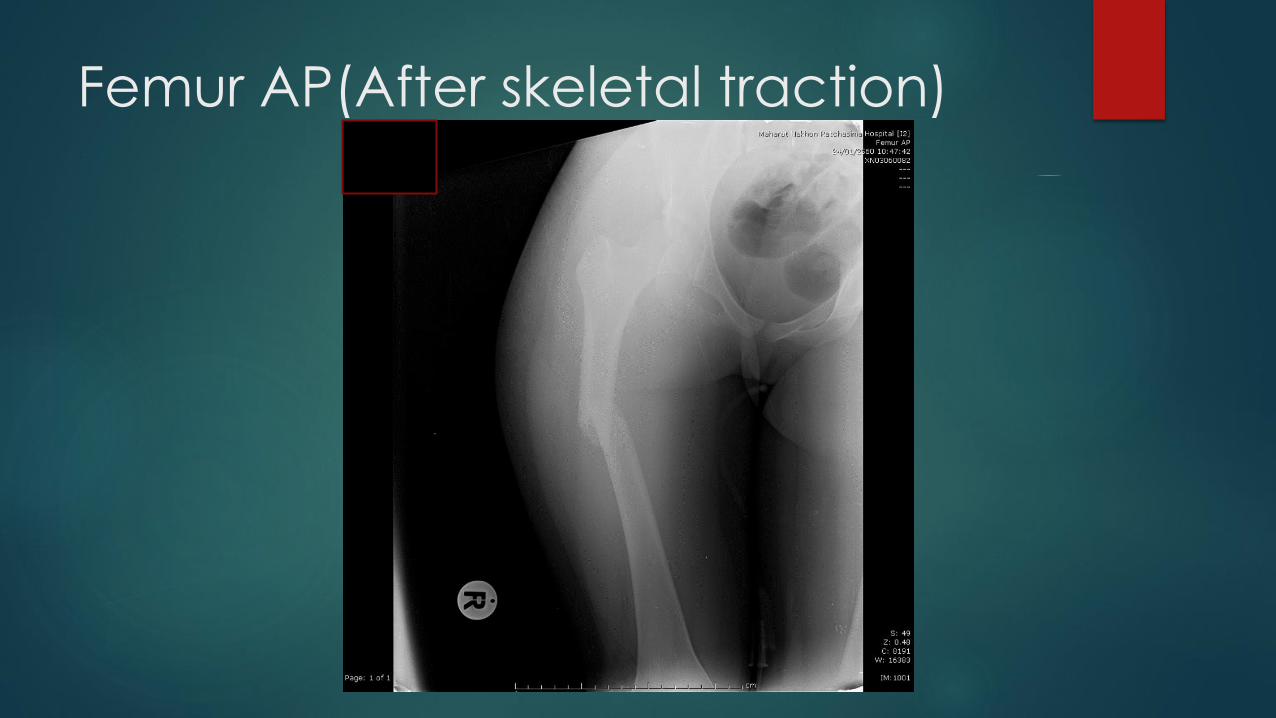
Femur AP(After skeletal traction)
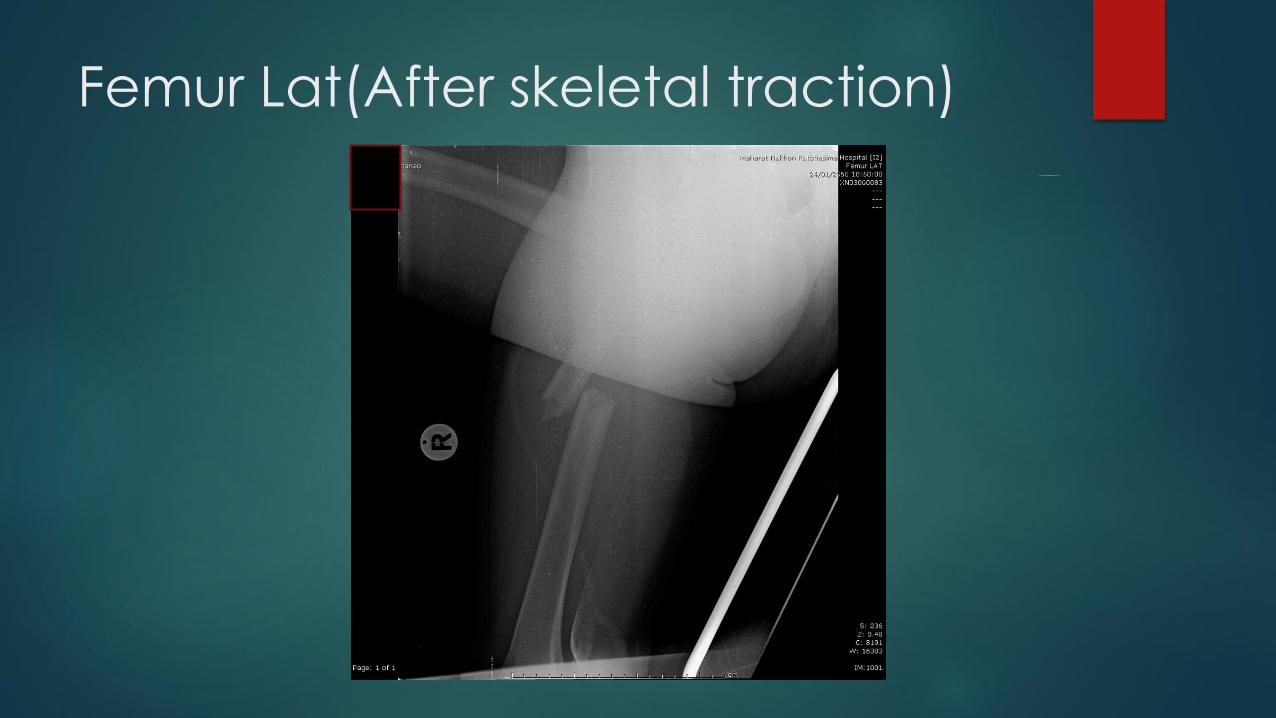
Femur Lat(After skeletal traction)
Management
Tramol 50 mg IV stat
On skeletal traction 5 kg at rt.leg
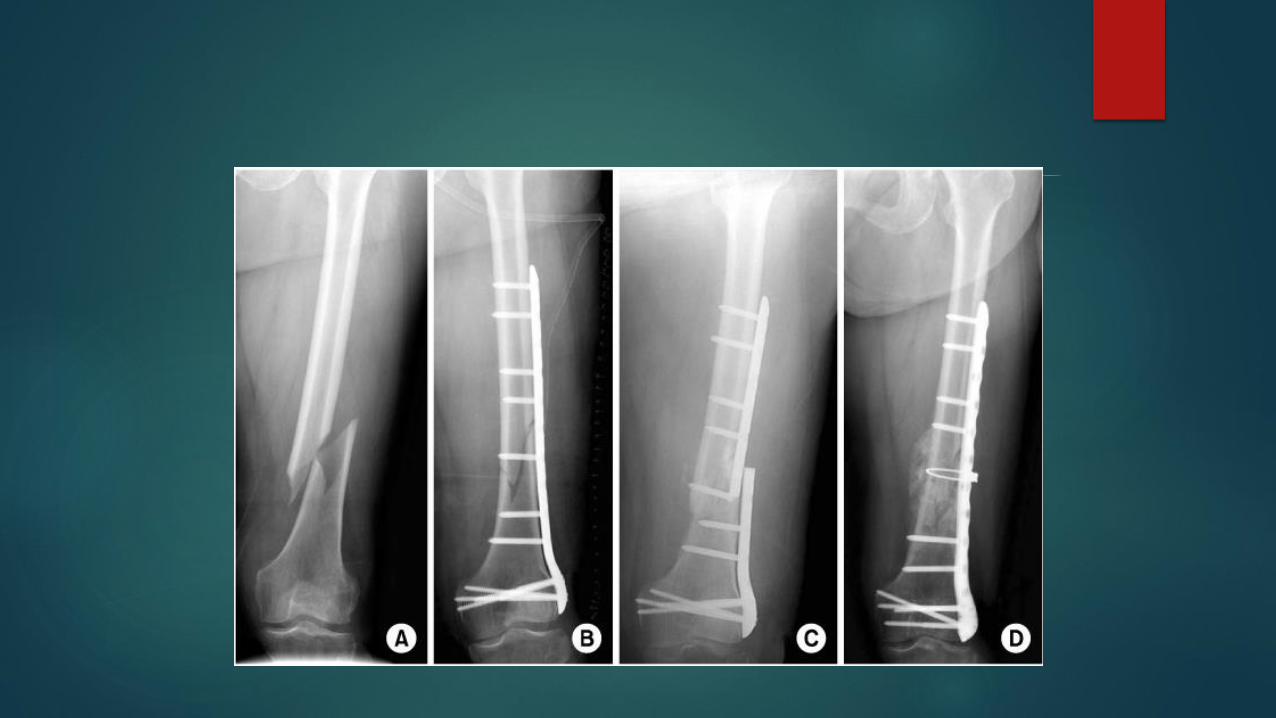
Wating for surgery > ORIF with plate & screw
Femoral Shaft Fractures
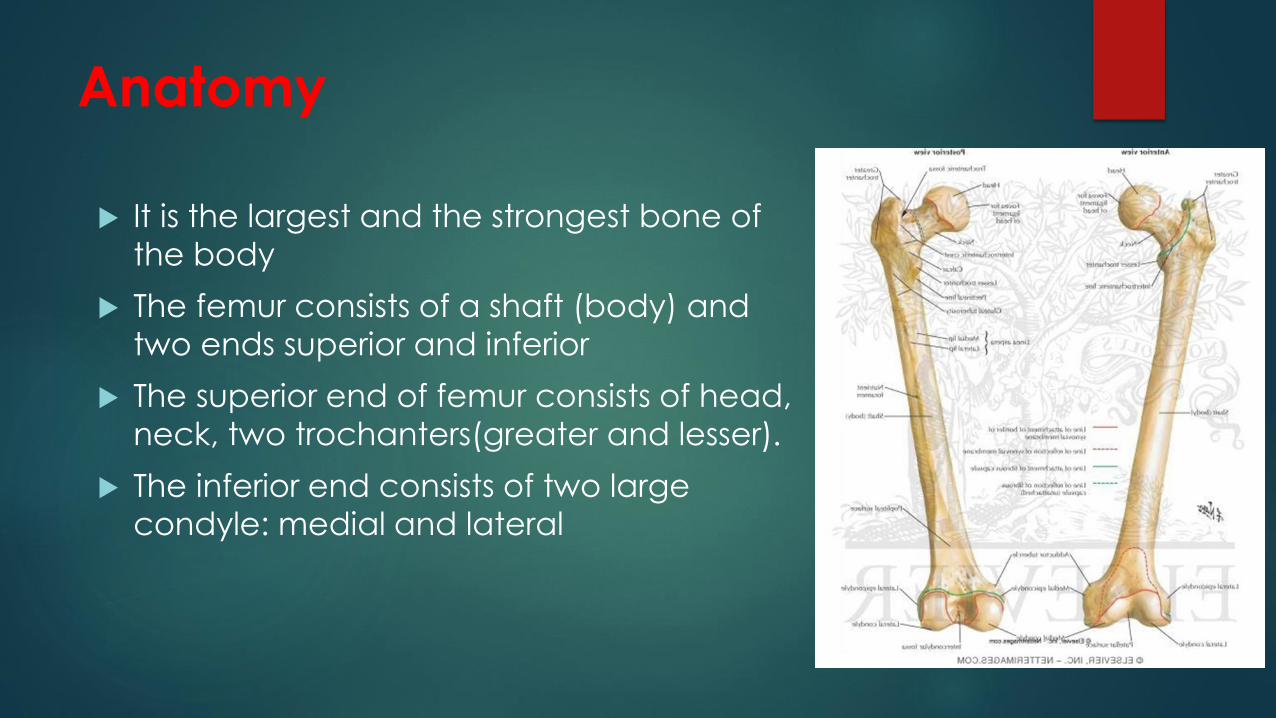
Anatomy
It is the largest and the strongest bone of
the body
The femur consists of a shaft (body) and
two ends superior and inferior
The superior end of femur consists of head,
neck, two trochanters(greater and lesser).
The inferior end consists of two large condyle: medial and lateral
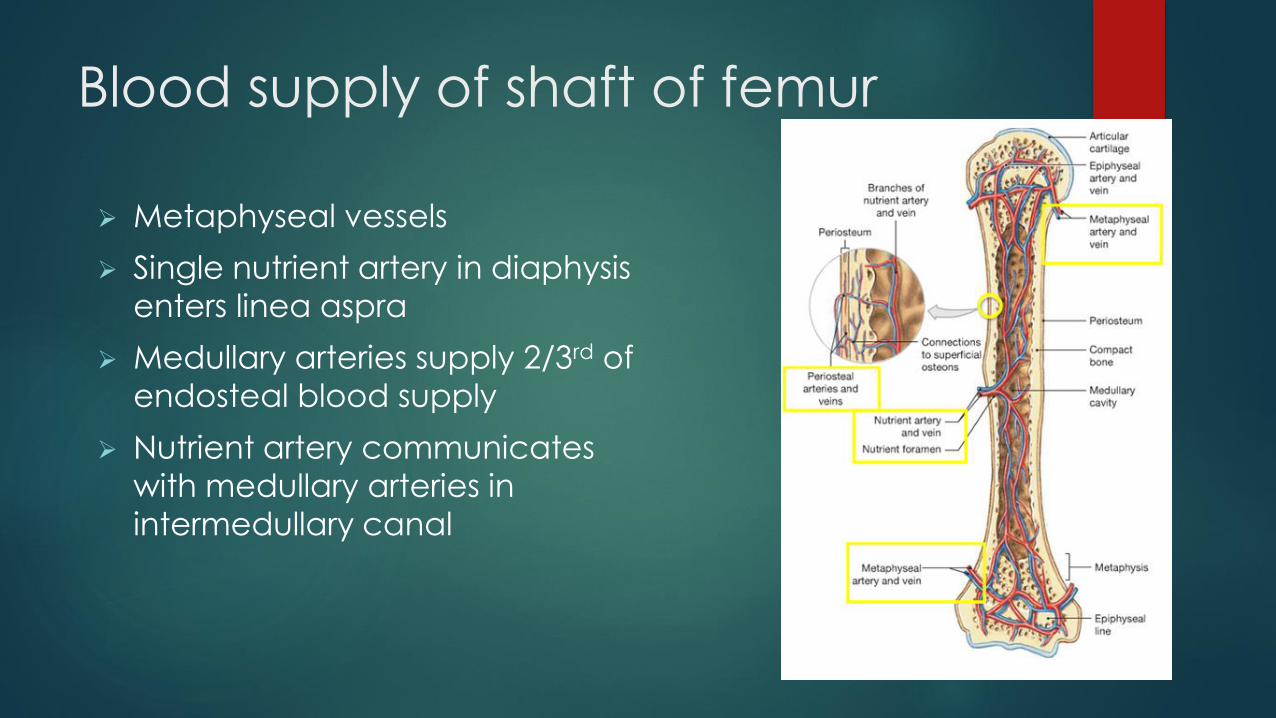
Blood supply of shaft of femur
Metaphyseal vessels
Single nutrient artery in diaphysis
enters linea aspra
Medullary arteries supply 2/3rd of
endosteal blood supply
Nutrient artery communicates
with medullary arteries in
intermedullary canal
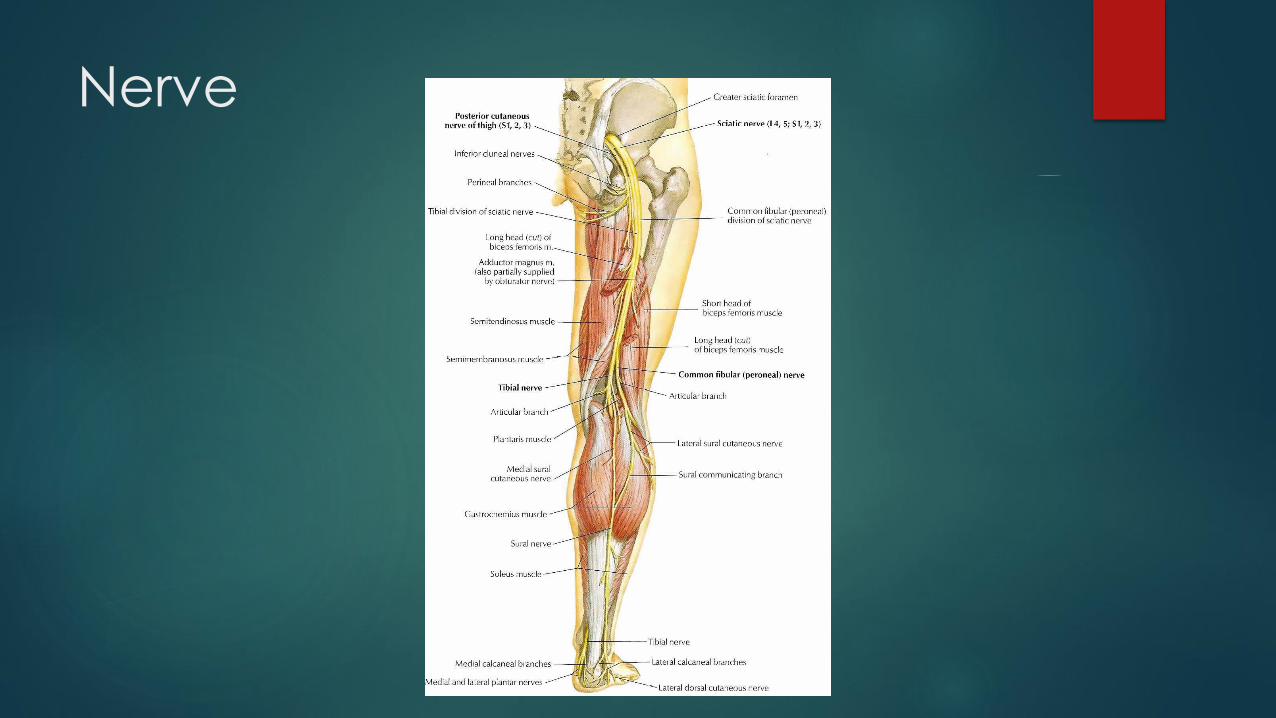
Nerve
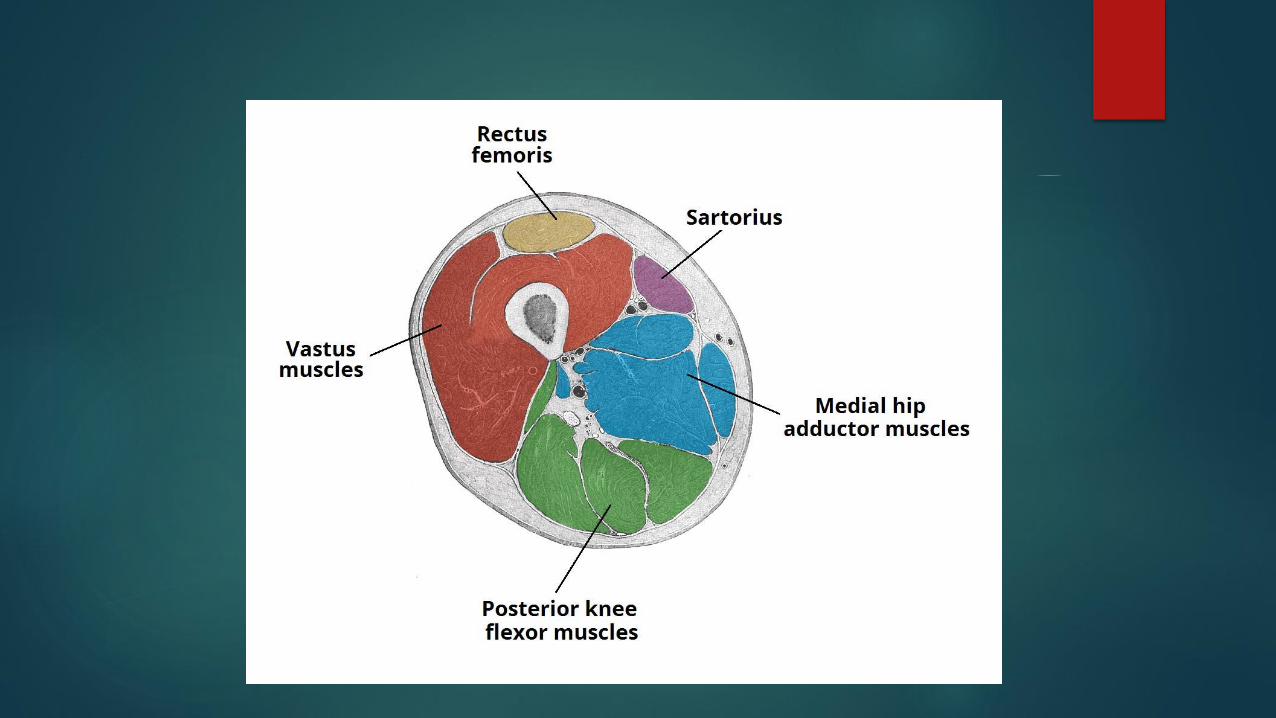
Muscle
Muscle of the thigh are arranged in three
Compartments
1-anterior compartment of thigh
-sartorius
-quadriceps(rectus femoris,vastusmedialis/lateralis/intermedius)
2-medial compartment of thigh
-gracilis
-adductor longus/brevis/magnus
3-posterior compartment of thigh
-hamstring(biceps femoris,semitendinosus,semimembranosus)
Femoral Shaft Fractures
Common injury due to major violent trauma
-1 femur fracture/ 10,000 people
-More common in people < 25 yo or >65 yo
-Motor vehicle, motorcycle and gunshot wound accidents
are most frequent causes
Mechanism of injury
High energy trauma
-Motor vehicle accident
-Gun shot injury
-Fall from height
Pathologic fractures
-especially in elderly ,commonly occur following a trivial fall
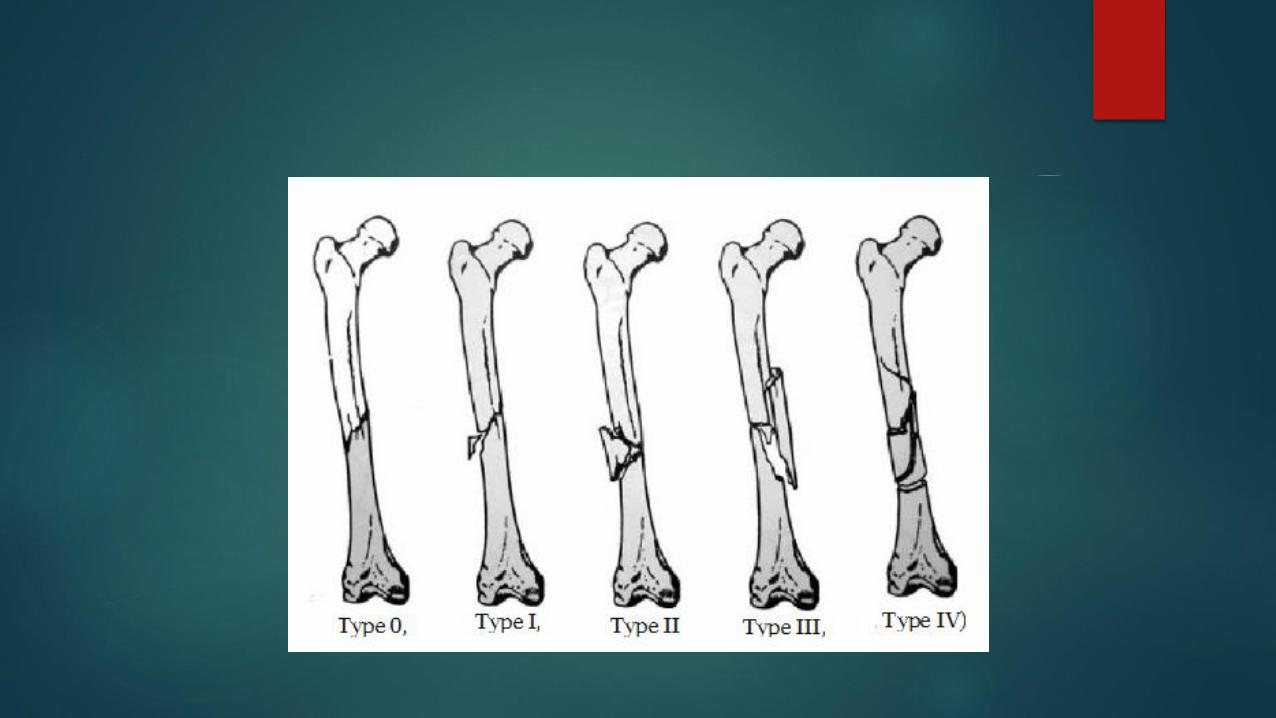
Classification of Femoral shaft
Fracture
Type 0 - No commination
* Type 1 - Insignificant butterfly fragment with transverse or short
oblique fracture
* Type 2 - Large butterfly of less than 50% of the bony width, > 50% of
cortex intact
* Type 3 - Larger butterfly leaving less than 50% of the cortex in
contact
* Type 4 - Segmental commination
Clinical
Non weight-bearing
Pain
Deformity
Leg position
-Ext.rotation,shortening

Associated injuries
Hemodynamic instability
Ipsilateral Fx neck of femur
Hip dislocation
Tibial shaft fx
Vascular injury
Nerve injury
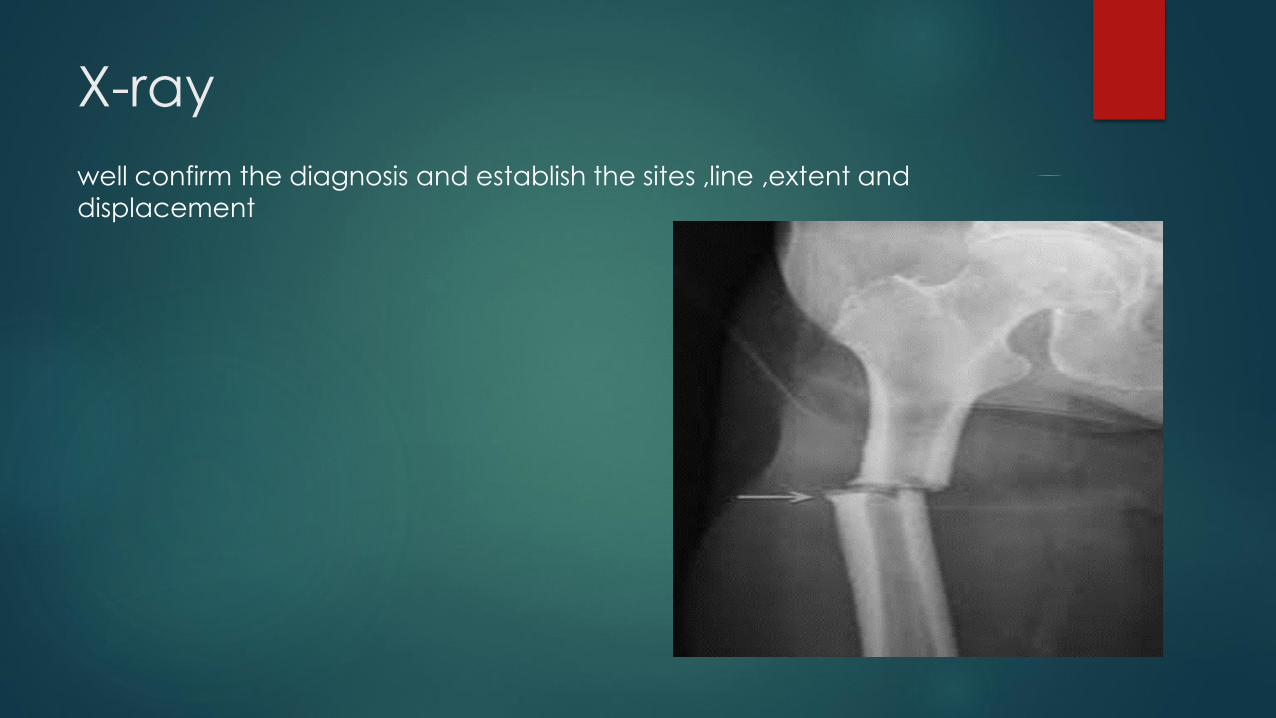
X-ray
well confirm the diagnosis and establish the sites ,line ,extent and displacement

Immediate management
ATLS resuscitation
Analgesia
X-ray
Skeletal traction
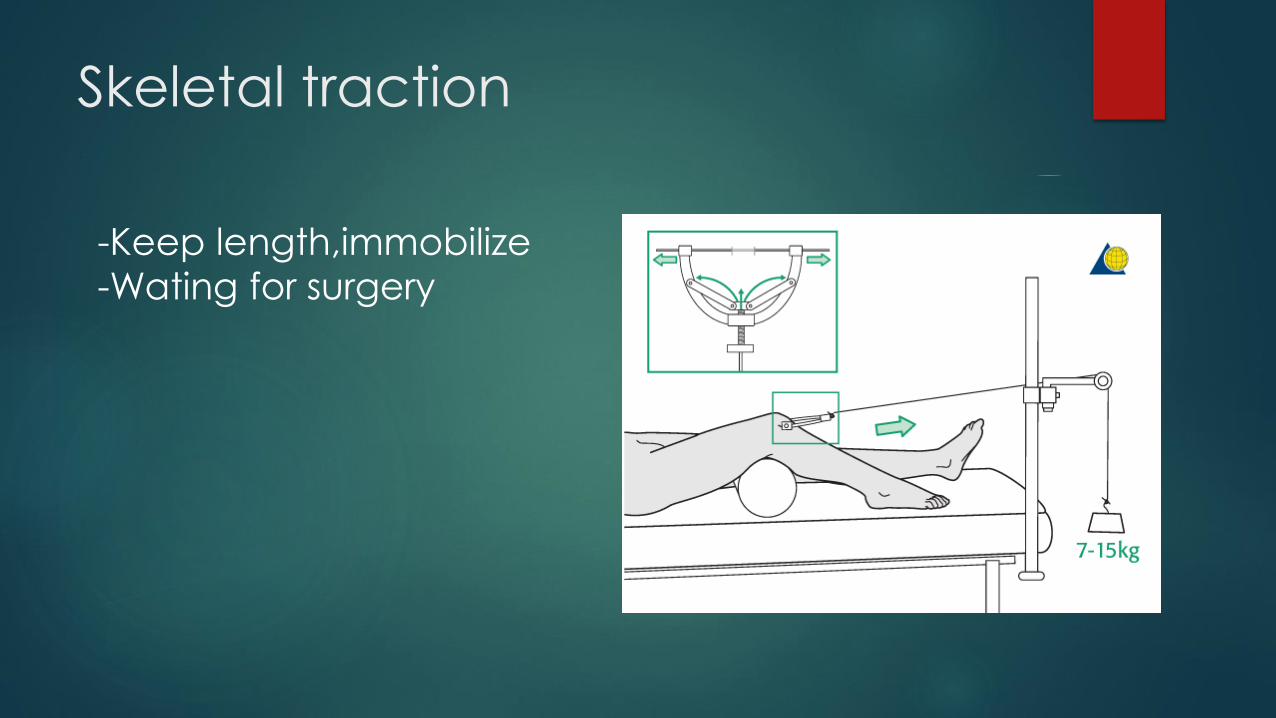
Skeletal traction
-Keep length,immobilize -Wating for surgery
Operative management
IM nail
Plate fixation
External fixation
IM nail
Advatage
-small wound
-less damage soft tissue
-rapid recovery
-decrease rate of infection
Weak point-Fx site not complete closed
IM nail is gold standard
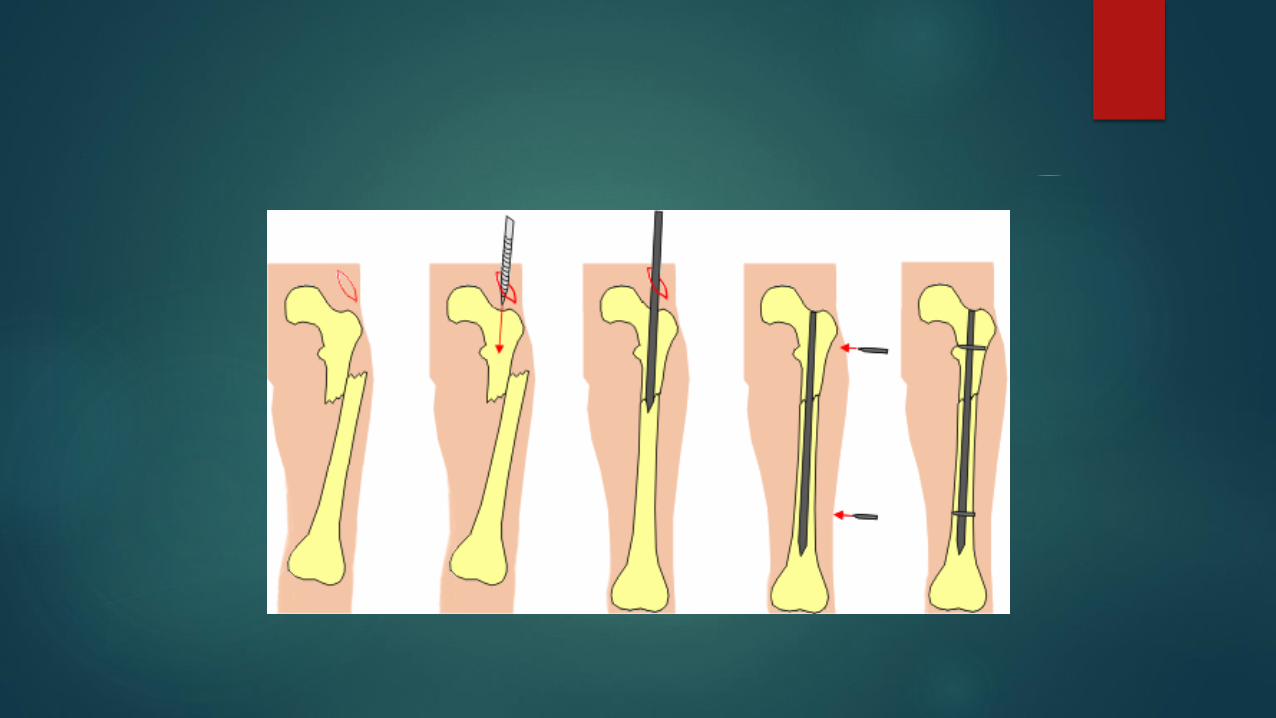

Plate fixation
Indication
-Ipsilateral fx neck of femur
Advantage-Rigid internal fixation
Weak point-Higher infection and implant failure rates
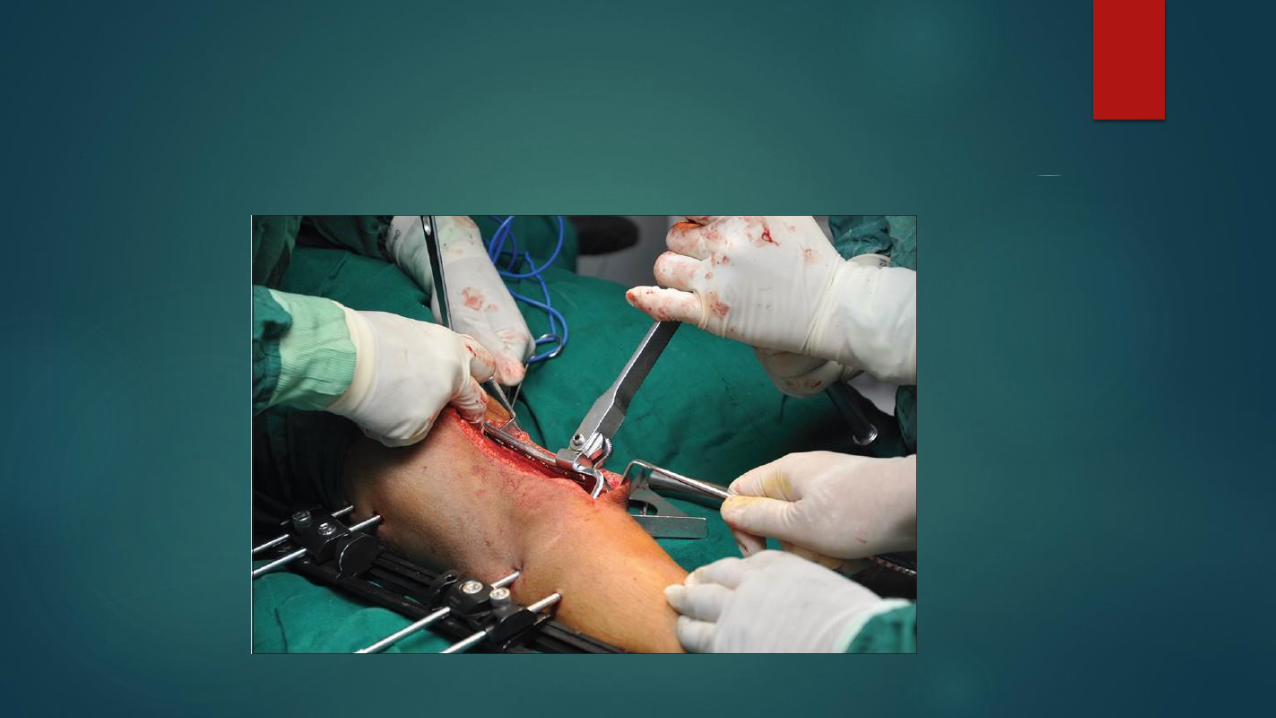
External fixation
Use temporarily before change to IM nail or
plate
Indication
-Dirty open fracture
-Vascular injury

COMPLICATION
Nerve injuries
Malunion
Nonunion
Heterotropic ossification
Vascular injuries

Thank you