female
DESCRIPTION
wanitaTRANSCRIPT

Female Female Hormone Hormone ReproductiReproductionon
Makassar, 24 April 2007
Battle of the sexes!!!
• Are males and females all that different?
• Well…..– Yes– And– No!

Anatomy
Male Female

Similarities
• 2 pouches– Testicles– Ovaries
• Start out inside body– Testicles “descend” before birth
• Fetus begins with “starter parts” that could develop into either gender.
Around 7th Week…
• Baby’s body is “told” by DNA to become either male or female.
• “Unused” parts disintegrate
• “Used” parts continue development
Male or Female???
• DNA determines baby’s gender
• XX = Female
• XY = Male
• Depends on which egg & sperm get together.
• Father determines baby’s gender.
Anatomy – similaritiesFunction – VERY different!
• Male– Uncomplicated– Produce sperm
• 2-4 MILLION every day
• Female– Very Complicated!– One egg– Once a month– Careful coordination of
hormones & body– Timing perfect!

1. Ovary – where eggs are stored and mature
2. when eggs are released by ovaries at ovulation, they are swept into the oviducts where fertilization occurs
3. Uterus – egg (or zygote, if its fertilized) arrives from the oviduct.
Here it either implants (if fertilized) in the endometrium,
or is released along with part of the uterine wall in menstruation,

• Oogenesis
– Most of the process occurs within the ovaries– Lifetime supply of primary oocytes is present at
birth– One primary oocyte matures each month to form
a secondary oocyte– If the secondary oocyte is fertilized, it completes
meiosis and becomes a haploid ovum

Figure 27.4B
Diploid cell In embryo
Differentiation andonset of MEIOSIS I
arrested in prophaseof MEIOSIS I
Present at birth
Completion of MEIOSIS Iand onset of MEIOSIS II
arrested at metaphaseof MEIOSIS II;
released from ovary
Firstpolar body
Entry of sperm triggerscompletion of MEIOSIS II
(haploid)
Secondpolar body
PRIMARY OOCYTE,
SECONDARY OOCYTE,
OVUM

• Development of an ovarian follicle
Figure 27.4C
Start: PRIMARY OOCYTE
within follicle
Growingfollicles
Mature follicle
Ovary
Ruptured follicleOVULATION
SECONDARYOOCYTE
CORPUS LUTEUM
Degeneratingcorpus luteum

Hormones synchronize cyclical changes in the ovary and uterus
Table 27.5
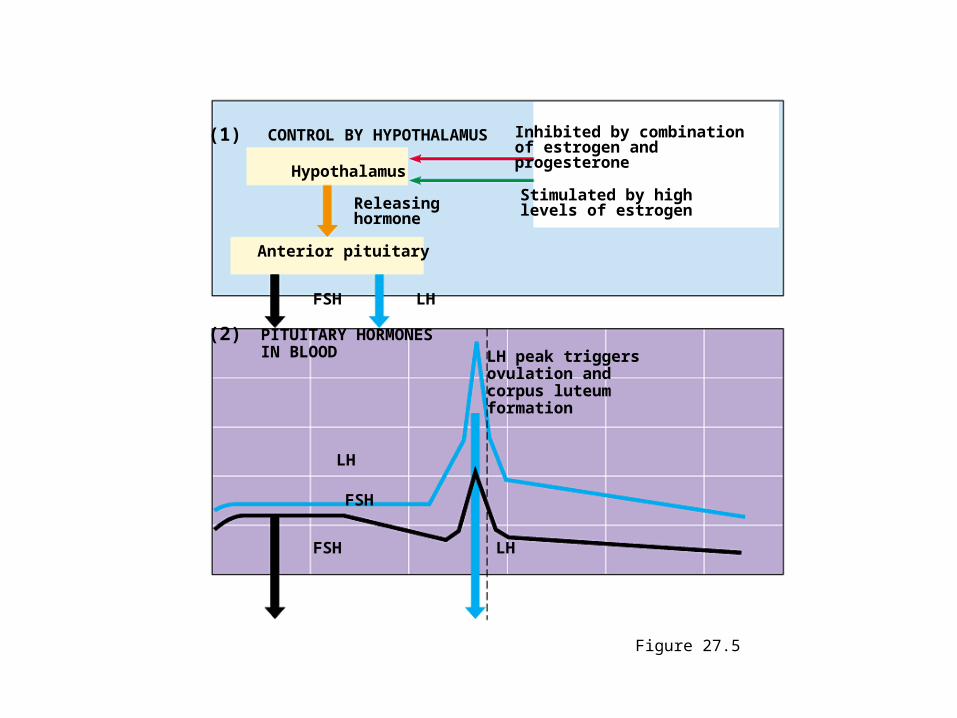
Figure 27.5
(1) CONTROL BY HYPOTHALAMUS Inhibited by combinationof estrogen and progesterone
Stimulated by highlevels of estrogen
Hypothalamus
Releasinghormone
Anterior pituitary
FSH LH
(2) PITUITARY HORMONESIN BLOOD LH peak triggers
ovulation andcorpus luteumformation
LH
FSH
FSH LH
What is the Menstrual Cycle?
• Controlled by hormones
• Lasts about one month
• the egg develops and is released from the ovary, and
• the uterus is prepared to receive the fertilized egg
• There are four stages to the menstrual cycle, the arrival of which are governed by the complex interactions of many hormones

What is the Menstrual Cycle?
Stage 1: Follicle Stage
• day 1 – 10
• Follicle Stimulating Hormone causes a follicle (an egg surrounded by a layer of “helper cells”) to mature
• Estrogen causes the lining of the uterus to thicken in preparation for receiving a fertilized (maybe) egg.

Stage 1: Follicle Stage
• Produksi estrogen oleh folikel meningkat
• Sekresi FSH menurun, tetapi sekresi LH terangsang dengan adanya produksi estrogen
• Pelepasan GnRH oleh Hipotalamus meningkat seiring sekresi estrogen
Stage 2: Ovulation
• day 11 – 14
• Luteinizing Hormone is released by the pituitary gland causing the follicle to rupture
• the egg is released into the fallopian tubes
Stage 3: Corpus Luteum Stage
• after the egg is released into the fallopian tubes and begins its journey to the uterus, the ruptured follicle changes into a mass of yellow cells – which is given the name “Corpus Luteum” (Latin for “yellow body”).
• The corpus luteum releases progesterone which causes the final development of the uterine tissue, preparing it to receive the fertilized (maybe) egg.

Stage 3: Corpus Luteum Stage
• Ditandai dengan meningkatnya produksi progesteron dan estrogen yang mengakibatkan turunnya kadar LH/FSH secara perlahan-lahan
• Meningkatnya hormon-hormon ini disebabkan oleh adanya corpus luteum yang terbentuk setelah folikel graaf melepaskan ovumnya
• Jika tidak dibuahi, maka corpus luteum mengalami penghancuran pada 4 hari sebelum menses berikutnya dan berubah menjadi corpus albicans

Stage 4: Menstruation
• day 21 – 28
• if fertilization does not occur, the egg will pass through the uterus, and the corpus luteum will begin to break down.
• Levels of estrogen and progesterone hormones decrease causing the lining of the uterus to break free from the uterine wall.
• This tissue, along with the egg and some blood leaves the body through the vagina

Figure 27.5 (continued)
(3) OVARIAN CYCLE
Growingfollicle
Maturefollicle
OvulationCorpusluteum
Degeneratingcorpusluteum
Pre-ovulatory phase Post-ovulatory phase
Estrogen Progesteroneand estrogen
(4) OVARIAN HORMONESIN BLOOD
Estrogen
Progesterone
Estrogen Progesteroneand estrogen
(5) MENSTRUAL CYCLE
Endometrium
Menstruation Days

If fertilized…
• Zygote begins to divide as it travels through oviduct
• Implants into lining of uterus
If not fertilized…
• Egg travels through oviduct to uterus
• Exits body with blood and tissues during menstruation

Conception/Fertilization

Conception/Fertilization
• Ejaculation– Release of 300-500 million sperm
• Egg needs to be in oviduct
• Sperm to egg, not an easy task– Go wrong direction : 2 paths – only 1 leads to
an egg– Get attacked by female’s white blood cells– Acidic environment

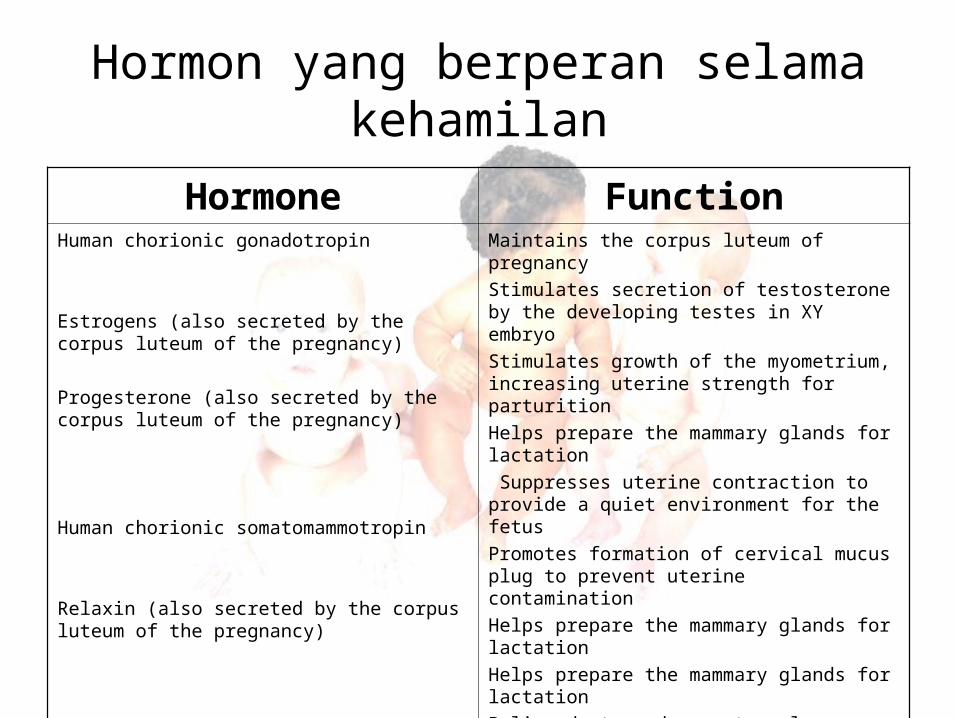
Hormon yang berperan selama kehamilan
Hormone FunctionHuman chorionic gonadotropin
Estrogens (also secreted by the corpus luteum of the pregnancy)
Progesterone (also secreted by the corpus luteum of the pregnancy)
Human chorionic somatomammotropin
Relaxin (also secreted by the corpus luteum of the pregnancy)
Maintains the corpus luteum of pregnancy
Stimulates secretion of testosterone by the developing testes in XY embryo
Stimulates growth of the myometrium, increasing uterine strength for parturition
Helps prepare the mammary glands for lactation
Suppresses uterine contraction to provide a quiet environment for the fetus
Promotes formation of cervical mucus plug to prevent uterine contamination
Helps prepare the mammary glands for lactation
Helps prepare the mammary glands for lactation
Believed to reduce maternal utilization of glucose so that greater amount of glucose might be shunted into the fetus
Soften the cervix in preparation for cervical dilation at parturition
Loosen the connective tissue between the pelvic bones in preparation for parturition
Prolactin
• Ditemukan pada wanita yang mengalami menstruasi, terbanyak pada urine wanita hamil, masa laktasi dan post menopause
• Kelebihan hormon ini menyebabkan gangguan pada ovulasi
• Sekresi prolactin pada wanita tidak menunjukkan perubahan siklus menstruasi (beda dengan gonadotropin)

Berdasarkan hasil penelitian
Sesaat sebelum ovulasi dan pada saat fase lutheal
Kadar prolactin sedikit meningkat, tapi tidak berarti
Penentuan hari pemeriksaan tidak menjadi masalah, namun sebaiknya:
• Dilakukan pada pagi hari• Puasa minimal 3 jam sebelumnya• Tidak dalam keadaan stress

Once egg is located…• Dissolve protective goo surrounding egg
• One gets through – enters egg
• Instant biochemical change in zygote– No more sperm allowed in

Zygote begins development
Time Lapse Development

Implants in uterine lining• Endometrium= outer lining of uterus
– Becomes placenta
• Uses mother’s nutrients
• Continues development

Fetal Development
• Anmion– Membrane surrounding baby– Contains amniotic fluid– Breaks just before birth = “water broke”
• Amniotic Fluid– The “water” – surrounding baby– Buoyant cradle for baby
• Protection• Free movement

Fetal Dev (cont’d)
• Umbilical Cord– Blood vessels from placenta to baby– Mom’s & baby’s blood do not circulate
together!• Can have 2 different blood types• Diffusion

Birth• Labor – muscles used to open cervix
• Baby flips upside down– Head first!– Feet first = Breech (bad)
• Cesarian Section (“C-section”) surgical removal of baby
• After baby is born mom delivers placenta (“afterbirth”) that detaches from uterus


The role and control of hormones involved in breast development
and lactationPregnancy
Prolactin and → Breast dev’tplacental lactogen →X Milk production
inhibition
Estrogen and progesteroneAfter birth
HypothalamusInhibition of hLH Pituitary→ OxytocinAnd hFSH Suckling
Prolactin→Milk production
Evaluasi infertilitas
Sejarah penderita: Kehidupan seksual
Keluarga
Fungsi reproduksi partner
Pemeriksaan fisik: Umum
Neurologik
Uji genital
Pemeriksaan laboratorium

Evaluasi infertilitas
ProgesteroneHigh (> 30nmol/l): patient ovulating; look for other causes of
infertility
Low
Prolactin High (>500miu/l): hyperprolactinemiaFSH High (>30iu/l): Primary ovarian failureLH High (>15 iu/l): Check if pregnant; LH but not
FSH high suggest PCOS
Low or normal
Estrogen status
AndrogensEstradiol17-hydroxyprogesterone
