fax: dermatology biologics phone: therapy prescription … · dermatology biologics therapy...
TRANSCRIPT

Please fill out page two...
Patient Information
Last Name
First Name
Home Address
Shipping Address (If different from above)
Home Address 2
Work Phone
Cell / Other Phone
Home Phone
Prescriber Information
Language Pref: English Spanish Other
Drug Allergies NKDA
DOB Last Four of SS# Gender: M F Physician’s Name
Office Contact Name
Today’s Date
Name of Practice / Hospital
Practice / Hospital Address
City State Zip
City State Zip Phone
DEA #
NPI #
Fax
Clinical Information (Section must be completed to process prescription)
Prior Treatment History
Abbvie Skilled Nurse Training:
In patient’s home or clinic In physician’s office
In patient’s home In physician’s office
Abbvie Skilled Nurse Training and Injection:
Nurse Training:
Does patient have Multiple Sclerosis or any demyelinating disease? Yes No
Does patient have CHF? Yes No
Height cm in kg lbsWeight
TB / PPD Test: Negative Positive
Years with DiseaseDate of Diagnosis
Medical Justification for Prescribing Biologic Therapy (or attach relevant history):
Contraindications (List)
Topicals (List) Duration
Duration PUVA Duration UVB
Side Effects, Lab Abnormalities, Toxicity Issues (List)
Other (List)Duration Sulfasalazine
Duration MethotrexateDuration Oral Retinoids (Soriatane, Accutane) Duration Cyclosporine
No Response to Previous Treatment (List)
Primary Diagnosis:
Body Surface Area Affected %
Date of Diagnosis
L40.59 Other psoriatic arthropathy
L40.1 Generalized pustular psoriasis
L40.2 Acrodermatitis continua
L40.3 Pustulosis palmaris et plantaris
L40.4 Guttate psoriasis
L40.8 Other psoriasis
L40.54 Psoriatic juvenile arthropathy
L40.0 Psoriasis vulgaris
L73.2 Hidradenitis suppurativa
Description
Other Diagnosis: ICD-10 Code
Non-Infectious Intermediate Uveitis
Posterior Uveitis
Panuveteitis
Insurance Information (Must fax a copy of patient’s insurance card including both sides)
Dermatology Biologics Therapy Prescription Form
Fax:
Phone:
Prior Authorization Reference number
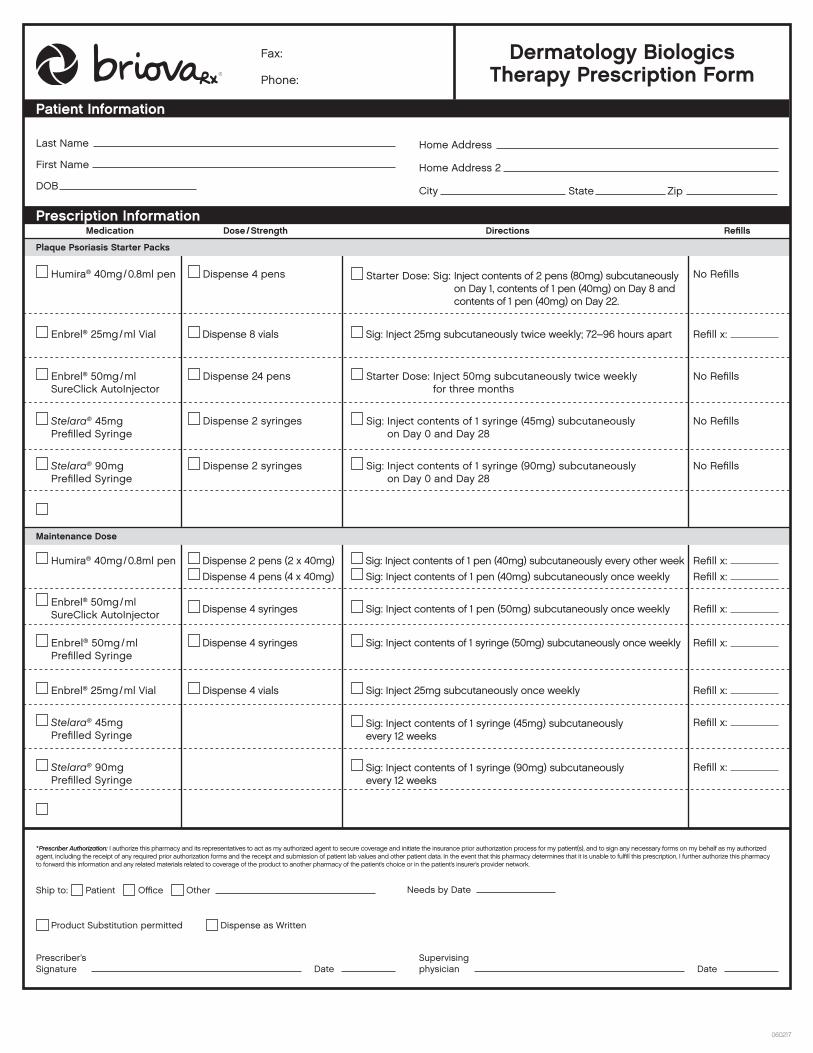
Plaque Psoriasis Starter Packs
Maintenance Dose
Medication Dose / Strength Directions RefillsPrescription Information
Ship to: Patient Office Other Needs by Date
Humira® 40mg / 0.8ml pen Starter Dose: Sig: Inject contents of 2 pens (80mg) subcutaneously on Day 1, contents of 1 pen (40mg) on Day 8 and contents of 1 pen (40mg) on Day 22.
Dispense 4 pens No Refills
* Prescriber Authorization: I authorize this pharmacy and its representatives to act as my authorized agent to secure coverage and initiate the insurance prior authorization process for my patient(s), and to sign any necessary forms on my behalf as my authorized agent, including the receipt of any required prior authorization forms and the receipt and submission of patient lab values and other patient data. In the event that this pharmacy determines that it is unable to fulfill this prescription, I further authorize this pharmacy to forward this information and any related materials related to coverage of the product to another pharmacy of the patient’s choice or in the patient’s insurer’s provider network.
No Refills Dispense 24 pens Starter Dose: Inject 50mg subcutaneously twice weekly for three months
Enbrel® 50mg / ml SureClick AutoInjector
No Refills Dispense 2 syringes Sig: Inject contents of 1 syringe (45mg) subcutaneously on Day 0 and Day 28
Stelara® 45mg Prefilled Syringe
No Refills Sig: Inject contents of 1 syringe (90mg) subcutaneously on Day 0 and Day 28
Dispense 2 syringes Stelara® 90mg Prefilled Syringe
Dispense 2 pens (2 x 40mg) Sig: Inject contents of 1 pen (40mg) subcutaneously every other week Humira® 40mg / 0.8ml pen Refill x:
Dispense 4 vials Sig: Inject 25mg subcutaneously once weekly Enbrel® 25mg / ml Vial Refill x:
Dispense 4 syringes Sig: Inject contents of 1 pen (50mg) subcutaneously once weekly Enbrel® 50mg / ml SureClick AutoInjector Refill x:
Dispense 4 syringes Sig: Inject contents of 1 syringe (50mg) subcutaneously once weekly Enbrel® 50mg / ml Prefilled Syringe
Refill x:
Sig: Inject contents of 1 syringe (45mg) subcutaneously every 12 weeks
Stelara® 45mg Prefilled Syringe
Refill x:
Sig: Inject contents of 1 syringe (90mg) subcutaneously every 12 weeks
Stelara® 90mg Prefilled Syringe
Refill x:
Dispense 8 vials Sig: Inject 25mg subcutaneously twice weekly; 72–96 hours apart Enbrel® 25mg / ml Vial Refill x:
Patient Information
Last Name
First Name
DOB City
Home Address
Home Address 2
State Zip
Dispense 4 pens (4 x 40mg) Sig: Inject contents of 1 pen (40mg) subcutaneously once weekly Refill x:
Dermatology Biologics Therapy Prescription Form
Fax:
Phone:
060217
Prescriber’s Signature
Supervising physicianDate Date
Product Substitution permitted Dispense as Written