family planning community medicine lecture
TRANSCRIPT
FAMILY PLANNINGFAMILY PLANNING
1] DEFINITION2] SCOPE3] HEALTH ASPECTS4] Methods







METHODS





DEFINITION• “A way of thinking and living that is
adopted voluntarily, upon the basis of knowledge, attitudes and responsible decisions by individuals and couples, in order to promote the health and welfare of the family group and thus contribute effectively to the social development of a country"
• A program to regulate no and spacing of children in a family through practice of contraception or other methods of birth control
• Programs or services designed to assist the family in controlling reproduction by either improving contraceptive use or by diminishing fertility there by limiting the no of child born
• A health service that helps couples decide when to have children n if so how many
FAMILY PLANNING aims at• Avoid unwanted births• Bring about wanted births• Regulate intervals between pregnancies• Control the time of birth in relation to ages of
parents• To determine the no of children in the family
CLASSIFICATION
METHODS
SPACING METODS
TERMINAL METHODS
MISCELLANEOUSMETHODS
SCOPE OF FAMILY PLANNING
• Proper spacing and limitation of births• Advice on sterility• Education for parenthood• Sex education• Screening for pathological conditions related to
the reproductive system (Ex. Cervical cancer)

Cont….d
• Genetic counseling• Premarital consultation and examination• Carrying out pregnancy tests• Marriage counseling• Preparation of couples for the arrival of their 1st
child
Cont ……..d
• Providing services for unmarried mothers
• Teaching home economics and nutrition
HEALTH ASPECTS OF FAMILY PLANNING
FETAL HEALTH
INFANTSAND
CHILDHEALTH
WOMENSHEALTH
WOMEN’S HEALTH• Pregnancy can mean
serious problems for women
• Health risk is 10-20 times greater in developing countries
• Risk Increases As: mother grows old
• With no of children

HEALTH IMPACT OF FAMILY PLANNING
METHOD
UNWANTEDPREGNANCY
NO OFBIRTHS
TIMING OF BIRTH
UNWANTED PREGNANCIES
CRIMINALABORTION
POTENTIALTHREAT TO
LIFE
UNWANTEDPREGNANCIES
UNSAFE ABORTION
LIMITING NO OF BIRTHS• Repeated pregnancies may cause mortality n
morbidity due to • Rupture of uterus• Toxemias of pregnancies• Placenta previa• Eclampsia • Severe anemia
TIMING OF BIRTHS
• Great risk of death is < 20 and >35 years of age
FETAL HEALTH
• A no of congenital anomalies are associated with advancing maternal age
• Quality of population can be improved by avoiding completely unwanted births, compulsory sterilization of all the adults who r suffering from certain diseases like leprosy and psychosis
CHILD HEALTH
BENEFITS
DECREASEDCHILD
MORTALITY
CHILD GROWTH
ANDDEVELOPMENT
INFECTIONSAND
INTELLIGENCE
WELFARE CONCEPTTABOOS
CULTURAL FACTORS
STERILISATION
MISCONCEPTIONS
SMALL FAMILY NORM
• Small diff. in family size will make big diff. in birth rate
• Symbolized by inverted red triangle• In 1970 slogan was “DO YAA TEEN BAS”
• In 1980 it was revised to 2 child norm

THE CURRENT EMPHASIS IS ON
1}SONS OR DAUGHTERS -2 WILL DO2}2nd child after 2-3yrs3}Universal immunization
ELIGIBLE COUPLES• Currently married couple
• Wife is in reproductive age group[15-45 ]
• Around 150-180 such couples per 1000 population
• Eligible couple register is a basic document for organizing F.P work
TARGET COUPLES• In order to pin point the couple who are the
priority groups within the broad definition of “eligible couples” the term target couple was coined
• Applies to couples who have had 2-3 living children and F.P was largely directed to such couples

COUPLE PROTECTION RATE• Its an indicator of prevalence of contraceptive
practice in the community
• It is defined as % of eligible couples effectively protected against child birth by one of the standard or approved methods of sterilization
• CPR is a dominant factor in reduction Net reproduction rate

BARRIER METHODS IN CONTRACEPTION

IDEAL CONTRACEPTIVE Safe Effective Acceptable Inexpensive Reversible Simple to administer Independent of coitus Long-lasting Little or no medical supervision.
CAFETERIA CHOICE :
THE PRESENT APPROACH IN FAMILY PLANNING PROGRAMMES
IS TO OFFER ALL METHODS FROM WHICH AN INDIVIDUAL CAN
CHOOSE ACCORDING TO HIS NEEDS AND WISHES AND TO PROMOTE
FAMILY PLANNING AS A WAY OF LIFE.

CONVENTIONAL CONTRACEPTIVES DENOTE METHODS USED THATREQUIRE ACTION AT THE TIME OF COITUS.E.g. : Condoms , spermicides , etc .
SUCCESS OF ANY CONTRACEPTIVEDEPENDS ON ITS EFFECTIVENESSAND RATE OF CONTINUATION .

CONTRACEPTIVE METHODS
SPACING METHODSSPACING METHODS TERMINAL METHODSTERMINAL METHODS
SPACING METHODSBARRIER METHODS
a) PHYSICAL METHODS b) CHEMICAL METHODS
c) COMBINED METHODSINTRA-UTERINE DEVICESHORMONAL METHODSPOST-CONCEPTIONAL METHODSMISCELLANEOUS

TERMINAL METHODS
MALE STERILISATION
FEMALE STERILISATION

BARRIER METHODSOCCLUSIVE METHODS:
THE AIM OF THESE METHODS IS TO PREVENT SPERM FROM MEETINGOVUM.ADVANTAGES : FREE FROM SIDE EFFECTS
ASSOCIATED WITH PILLS & IUD. PROTECTION FROM STD’S , PELVIC INFLAMMATORY DISEASES &
CANCER CERVIX.

DISADVANTAGES :
HIGH DEGREE OF MOTIVATION
LESS EFFECTIVE THAN PILL OR LOOP
THEY SHOULD BE USED CONSISTENTLY & CAREFULLY.

PHYSICAL METHODS CONDOMS :
MOST WIDELY USED METHOD BY MALES. NIRODH-TRADE NAME-MEANS PREVENTION. CONDOM IS FITTED OVER ERECT PENIS. AIR MUST BE EXPELLED FROM TEAT TO MAKE ROOM FOR EJACULATE. CONDOM PREVENTS DEPOSITION OF SEMEN IN VAGINA. IT SHOULD BE CAREFULLY WITHDRAWN TO AVOID SPILLAGE.
EFECTIVENESS CAN BE INCREASED BY APPLYING SPERMICIDAL JELLY .PREGNANCY RATE VARIES FROM 2-3PER1OOO OT >14 IN TYPICAL USERS.
ADVANTAGES : EASILY AVAILABLE SAFE & INEXPENSIVE EASY TO USE LIGHT,COMPACT & DISPOSABLE PROTECTS AGAINST PREGNANCY & STD’S.

DISADVANTAGES : INCORRECT USE. IT MAY SLIP OFF OR
TEAR DUE TO INTERFERES WITH SEX
SENSATION MANUFACTURED IN
INDIA AT HINDUSTAN LATEX IN
TRIVANDRUM & LONDON RUBBER
FACTORIES IN CHENNAI.

FEMALE CONDOM :POUCH MADE OF
POLYURETHRANE WHICH LINES VAGINA.INTERNAL RING COVERS
CERVIX ,EXTERNAL RING REMAINS
OUTSIDEVAGINA.PRELUBRICATED WITH SILICONHIGH COST & ACCEPTABILITY
AREMAJOR PROBLEMS .

DIAPHRAGMVAGINAL BARRIER , DUTCH CAPSYNTHETIC RUBBER ORPLASTIC MATERIAL.IT HAS A FLEXIBLE RIM OF IT IS
INSERTED BEFORE INTERCOURSE & KEPT
IN PLACE FOR UPTO 6hrs AFTER COITUS.
SPERMICIDAL JELLY SIDE EFFECTS ARE NILL.
FAILURE RATE IS 6 TO 12 PER 100 WOMEN
YEARS .
ADVANTAGES :NO SIDE EFFECTS .DISADVANTAGES :NEEDS DEMONSTRATIONAFTER DELIVERY , IT CAN BE USED ONLY AFTER COMPLETE INVOLUTIONTOXIC SHOCK SYNDROME NOT RECOMMENDED IN FAMILY WELFARE PROGRAMME .

VAGINAL SPONGESPONGE SOAKED IN VINEGAR OROLIVE OIL .TRADE NAME - TODAY.SMALL POLYURETHRANE SPONGESATURATED WITH SPERMICIDE ,NONOXYNOL-9.LESS EFFECTIVE , FAILURE RATE INPAROUS WOMEN IS 20 TO 40 FOR 100WOMEN YEARS. IN NULLIPAROUS WOMEN IT IS 9 TO 2PER100 WOMEN YEARS.

CHEMICAL METHODSSPERMICIDES - 4 CATEGORIES FOAMS : FOAM TABLETS & AEROSOLS CREAMS , JELLIES & PASTES SUPPOSITORIES–INSERTED MANUALLY SOLUBLE FILMS – C FILM
SPERMICIDES CONTAIN A BASE IN TOWHICH SPERMICIDE IS INCORPORATED .MODERN SPERMICIDES ARE SURFACE ACTIVE AGENTS . THEY ATTACH TOSPERMS AND INHIBIT OXYGEN UPTAKE.
DRAWBACKS OF SPERMICIDES
HIGH FAILURE RATE. MUST BE USED IMMEDIATELY BEFORE
COITUS & REPEATED EVERY TIME. MUST BE INTRODUCED INTO AREAS
WHERE SPERMS ARE DEPOSITED. MILD BURNING , IRRITATION BESIDES
MESSINESS.
NOT RECOMMENDED BY PROFESSIONALS.

INTRA UTERINE DEVICES
2 types of IUDs
Nonmedicated Medicated
Cu IUDs Hormone Releasing
• .

Non medicated/ Inert/ First generation IUDs : • These IUDs are available in different shapes and sizes
• Loops, spirals, coils, rings, bows etc.
LIPPES LOOP• Double ‘S’ shaped device
• It contains small amount of Baso4 • Loop has attached threads or tail • Tail made up of nylon • Importance of tail
easy to remove • Loop exists 4 sizes A,B,C & D
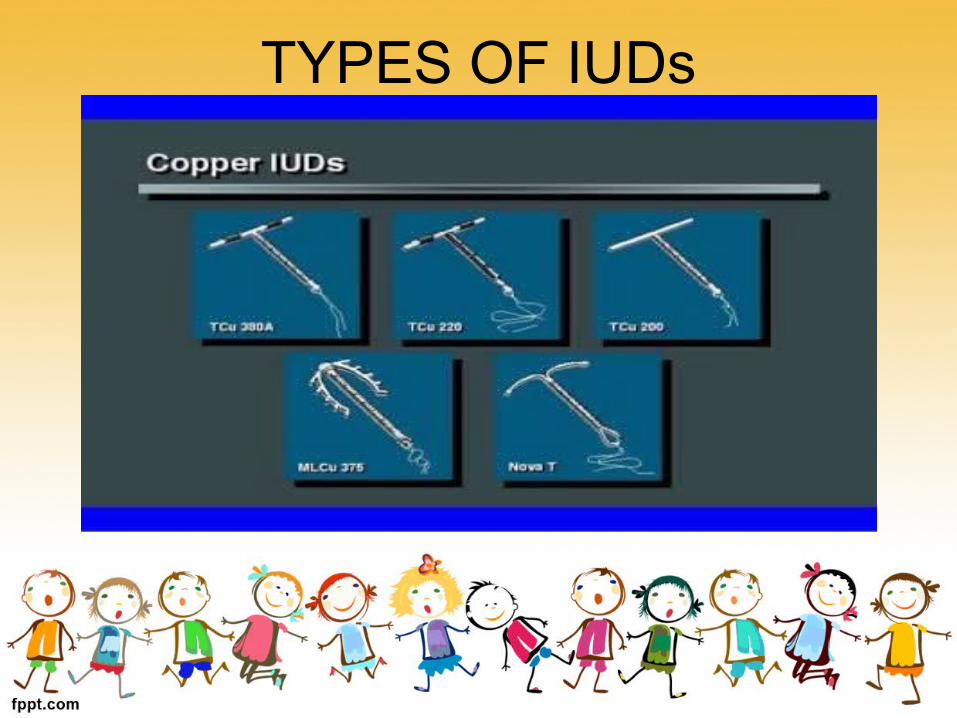
TYPES OF IUDs
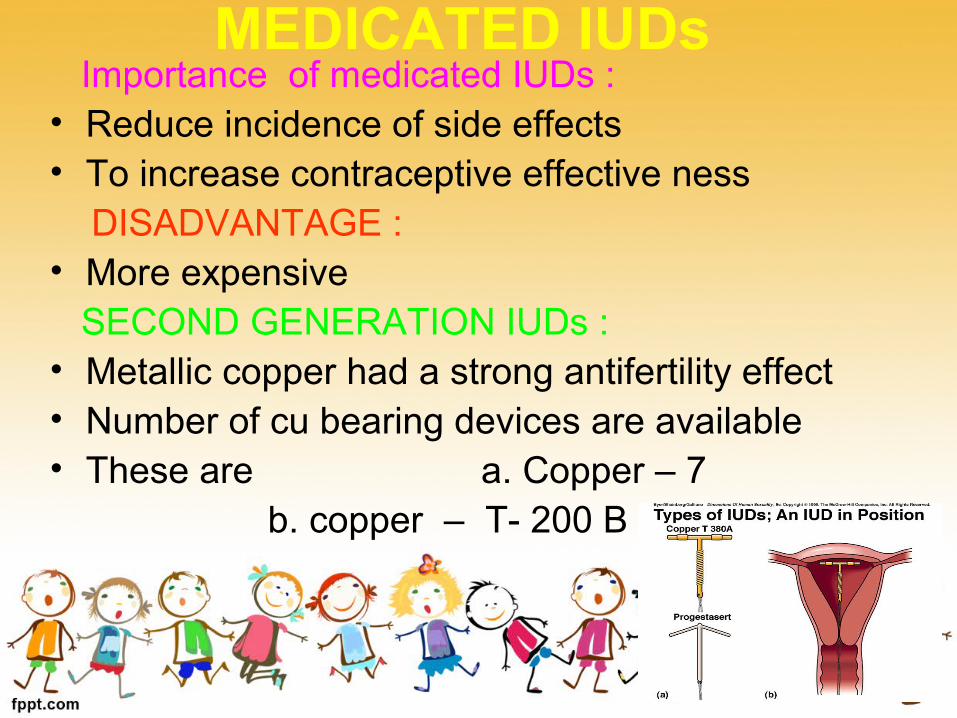
MEDICATED IUDs Importance of medicated IUDs : • Reduce incidence of side effects • To increase contraceptive effective ness DISADVANTAGE : • More expensive SECOND GENERATION IUDs : • Metallic copper had a strong antifertility effect• Number of cu bearing devices are available • These are a. Copper – 7 b. copper – T- 200 B
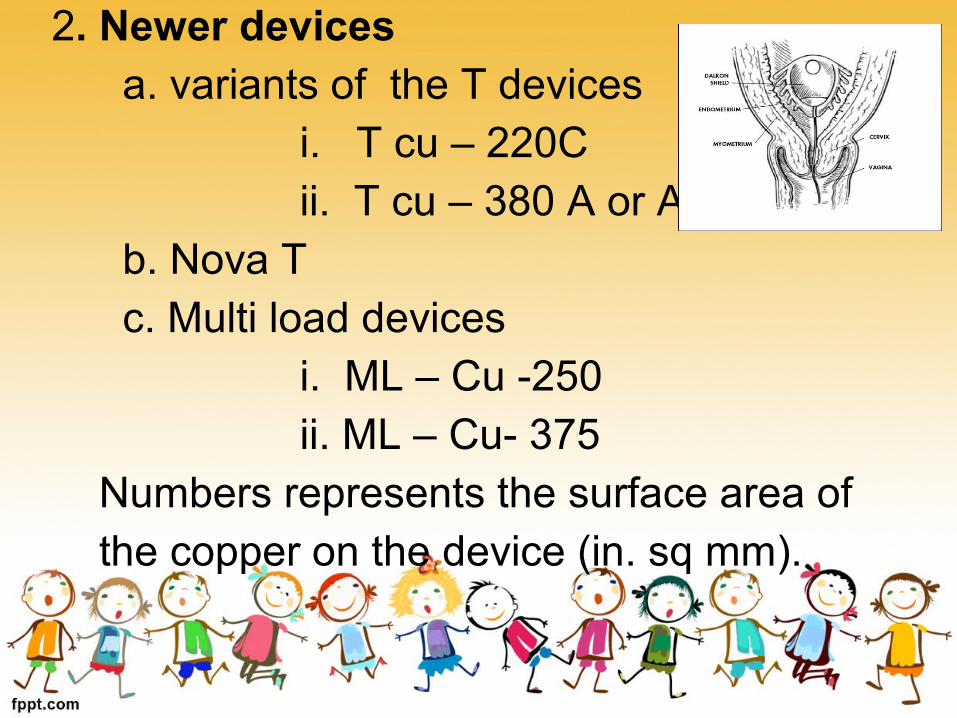
2. Newer devices a. variants of the T devices i. T cu – 220C ii. T cu – 380 A or Ag b. Nova T c. Multi load devices i. ML – Cu -250 ii. ML – Cu- 375 Numbers represents the surface area of the copper on the device (in. sq mm).

• ADVANTAGES OF COPPER DEVICES :
1. Low expulsion rate
2. Low incidents of side effects
3. High anti fertility effect
4. easier to fit even in nulliparous women
5. Post coital contraceptives
THIRD GENERATION IUD • Most widely used hormonal devices are 1.Progestasert • T shape device filled with 38 mg of
progesterone • It has direct effect on uterine lining, cervical
mucus and sperms • 2. Levonorgestrel (LNG – 20) • T shaped device • It has 1. low pregnancy rate 2. less number of ectopic pregnancies 3. Lower menstrual blood loss 4. Fewer days of bleeding
MECHANISM• Foreign body reaction. • Cellular and biochemical changes. • Impair the viability of the gamete. • Reduce the chances of fertilization rather than implantation. • Copper enhances the Cellular response in the endometrium. Affects the enzymes in the uterus. Alter biochemical composition of cervical mucus. • Hormonal devices increase viscosity of the cervical mucus.

TIMING OF INSERTION
• Loop can be inserted any time during a women's reproductive age group except during pregnancy
• Most propitus time for loop insertion During menstruation With in 10 days of begining of menstrual period After delivery • Immediate postpartum insertion (during 1st week) • Post puerperal insertion (after 6-8 weeks )
FOLLOW UP • Follow up is most important aspect of IUD insertion Objectives : 1.To provide motivational and emotional support for the women 2.To confirm the presence of the IUD 3.Diagnose and treat any side effects Time of Examination : 1.After her first menstrual period 2.After 3rd menstrual period 3.There after at 6 months or 1 year
EFFECTIVE NESS • Theoretical effective ness of IUD is Less than that of
oral and injectable hormonal contraceptives • Table shows

DEVICE PREGNANCY RATE(%)
EXPULSION RATE (%)
REMOVAL RATE(%)
Lippes loop 3 12-20 12-15
Cu-7 2-3 6 11
Tcu-200 3 8 11
Tcu-380A 0.5-0.8 5 14
Progesterone 1.3-1.6 2.7 9.3
Levonorgestrel 0.2 6 17
ADVANTAGES OF IUDs • 1. Simplicity • 2. Insertion takes few minutes • 3. Once inserted IUD stays in place as long as required • 4. Reversible • 5. In expensive • 6. High continuation rates • 7. Single act of motivation • 8. Free of systemic side effects
Absolute contra indications• i. Suspected pregnancy
• ii. Pelvic inflammatory disease
• iii. Vaginal bleeding
• iv. Cancer of cervix and uterus
• V. Previous H/o ectopic pregnancy

• i. Anaemia
• ii. Menorrhagia
• iii. History of pelvic inflammatory disease
• Iv. Purulent cervical discharge
RELATIVE CONTRA INDICATIONS

INTRA UTERINE COTRACEPTIVE DEVICE SIDE EFFECTS AND COMPLICATIONS
• IMMEDIATE• Difficulty in insertion.• Vasovagal shock.• Uterine cramps.• EARLY• Expulsion.• Perforation.• Spotting Menorrhagia.• Dysmenorrhoea.• Vaginal infection.• Actinomycosis.

• LATE• Pelvic inflammatory disease.• HIV/AIDS.• Ectopic pregnancy.• Perforation.• Memorrhagia.• Dysmenorrhoea.• OTHERS• FERTILITY.• LATE,TERATOGENELITY.• MORTALITY.

EXPULSION RATE TYPE OF IUCD GENERATION
12-20 % Lippes Loop Ist gen
6%8%5%
Cu 7Tcu-200Tcu-380
II gen
2.7%6%
Progesterone IUCDLevonorgestrel IUCD
III gen
EXPULSION • C/F:-• Complete • Partial.• Complete: As seen by person.• Partial:- Diagnosed by speculum examination.• FACTORS: skill. Timing of insertion: postpartum. Age: nulliparity, young women. Main Problem: pregnancy.

V) Perforation• Early and late complication.• Incidence: 1:150 – 1:9000.• FACTORS:-• Time of insertion: 48weeks – 60 weeks past partum.• Design of IUCD:• Skill:• Operators experience:• C/F:-• pain intestinal destruction.• Asymptomatic.• MISPLACED IUCD:-• Confirmed by pelvic X-ray• Treatment:-• Laparatomy & removal.
VI) Bleeding or Menorrhagia DYSMENNORHOEA:-
late or early. inert or medicated IUCD- commonest complaint• C/F:-• 1) greater volume.• 2) longer periods• 3) mid cycle bleed.• Complications:• Personal inconvenience.• Iron deficiency anemia.• Treatment:-• Generally settles within 1-2 months.• Ferrous sulphate 20mg tid.

• CAUSE OF REMOVAL.• RETURN OF NORMAL CYCLE• If not –full GYNAEC EXAM.• VAGINAL INFECTION/ACTINOMYCOSIS.
Non medicated Max
Copper T Less average
Hormonal Lower
• VII) PELVIC INFLAMATORY DISEASE(PID): • sub acute, chronic, conditions of ovaries, tubes, uterus,
connective tissue and pelvic peritoneum following infection.
• Incidence:- 2-8 times more than non IUCD users.• Risk:- polygamies, STD’s like HIV / AIDS, syphilis.• Etiology;_ Ascent OF INFECTION with the IUCD.• C/F:- • Vaginal discharge.• Pelvic pain.• Tenderness.• Abnormal bleeding.• Chills.• Fever.• In many cases• Asymptomatic.• Low grade.• Complications:- infertility.

• Treatment:-• Broad spectrum Antibiotics.• Prescribe the removal if not responding in 24-48
hrs• IIIV ) RISK REDUCTION:• 1)Washing hands & putting on gloves.• 2)Cleaning cervix & vagina water based iodophore
betadine or chlorhexidine.• 3)using “no touch instrument technique”• 4)Washing hands again and processing • instruments.• Processing for reuse:-• Decontamination:- 5% chlorine(10 min)• HIGH LEVEL DISINFECTON:-• Instruments & Gloves 30% in Activated• 2% glutaroldehyde• 8% formaldehyde• Washing thoroughly in boiled water or sterile water.
• LOW LEVEL DISINFECTANS:-• Zephiran(Benzalleonium
chloride)• Savlan(Cetrimole chlorhexioline)• Should never be used.• Costly Autoclave Sterilization not
required.• STORED DRY FOR WEEK IN
CONTAINER WITH A TIGHT FITTING LID.

IX) PREGNACY:
3% Lippes Loop
2-3% Copper T
3% Tcu-200
0.5 – 0.8% Tcu-380
1.3-1.6% Progesterone-IUCD
0.2% Levonorgestrel-IUCD

• 50% of pregnancies spontaneous Abortion• Early removal 30% resolution of
abortions.• Increase of “premature births” by
continuing pregnancy• Complications:-• Infection & spontaneous abortions• Prevention:-• legal induced abortion• Removal.

X) ECTOPIC PREGNANCY.• Ectopic pregnancy ratio/100 woman year 0.2
for levonorgestrel IUCD & Copper T 380 A• compared to 3-4.5 for non contraceptive.• Reason:- Mode of action for levonorgestrel differs from progesterone.

DANGER SIGNALS :-• lower abdominal pain.• Dark and scanty virginal bleeding and
amenorrhea.• Risk Persons:-• Previous pelvic inflammatory disease.• Other ectopic pregnancy.

XI):- Others Fertility after removal 70% conceive. No cancer or teratogenicity. Mortality Extremely rare. 1death /1,00,000 women years of
septic abortion as ectopic pregnancy.

HARMONAL CONTRACEPTIVES

HORMONAL CONTRACEPTIVES• Hormonal contraceptives when properly used
are the most effective methods of contraception• They provide the best means of ensuring
spacing between one childbirth and another
• GONADAL STEROIDES:
a. synthetic steroids: eg ethinyl oestradiol and mestranol.
b. synthetic progestogens: they are pregnanes , oestranes and gonanes.
CLASSIFICATION
a) ORAL PILLS1.Combined pills2.Progestogen only pill3.Post coital pill 4.Once a month pill 5.Male pill
b) DEPOT FORMULATIONS1. Injectables 2. Subcutaneous implants3. vaginal rings

ORAL PILLS1. Combined pill:
It is one of the major spacing methods of contraception.It contains 30-35 mcg of a synthetic oestrogen and 0.5 to 1 mcg of a progesterone.
The pill should be taken at a fixed time everyday.
Cont.,• The pill is given orally for 21 days starting
on the 5th day of menstrual cycle followed by a break of 7 days during which menstruation occurs.
• This is called withdrawal bleeding. • The department of family welfare , in the Ministry
of Health and Family Welfare Govt. of India has made available low dose of oral pills – MALA-N and MALA-D.

2. Progesterone only pill• It is called as minipill or micropill .it contains only
progesterone which is given in small doses through out the cycle.
• These pills have an increased pregnancy rate so not being used , but can be used for women with cardiovascular problem and for those with the risk factors for neoplasia.
3. Post coital contraception: It is used within 48 hrs of unprotected
intercourse.
Two methods are available.
a) IUD: e.g. copper device
b) Hormonal: combine oc pill is used. It contains double dose of the standard combined pill. 2 pills immediately followed by 2 pills 12 hours later.
For emergency contraception a women must take four instead of 2 in each dose.
4. Once a month long acting pill
• Quniestrol , a long acting estrogen is given in combination with a short acting progesterone.
• Disadvantage: high pregnancy rate and irregular bleeding.
5. Male pill: The approach is• a) preventing spermatogenesis.
b) interfering with sperm storage.
c) preventing sperm transport.
d) affecting the seminal fluid constitution.
• An ideal male contraceptive will decrease the sperm count while leaving testosterone at normal values.

Mode of action of oral pill:
• Combined only pill prevents the release of ova from the ovary by blocking the pituitary secretion of gonadotropin.
• Progesterone only pills render the cervical mucus thick and scanty and inhibit the sperm penetration.
Effectiveness :
• If taken according to the prescribed regimen oral contraceptives of the combined type are 100% effective.
• It is also influenced by drugs – rifampicin, phenobarbital, ampicillin.

BENEFICIAL EFFECTS Contraceptive benefits- prevention of unwanted
pregnancy (failure rate- 0.1per 100 women year).
Non contraceptive benefits- a. relief of: menorrhagia (50% ),
dysmenorrhoea (40% ), premenstrual tension syndrome, mittleschmerz syndrome. b. improvement of: iron def. anemia,hirsutism, acne, endometriosis, autoimmune disorders of thyroid, rheumatoid arthritis.

c. marked reduction in: pelvic inflammatory
disease, benign breast cancer, ectopic
pregnancy, fibroid uterus, functional
ovarian cysts, carcinoma of ovary (40% )
carcinoma of endometrium (50% ),
protection against osteoporosis.
b) DEPOT FORMULATIONS• Injectable contraceptives, sub dermal
implants and vaginal rings come in this category.
1. Injectable contraceptives: There are two types: PROGESTAGEN ONLY INJECTABLES:
• (a) DMPA: Depot medroxy - progesterone acetate.
• Dose is i.m injection of 150mg every 3months.
• Dose is i.m injection of 150mg every 3months.
• Action is by suppression of ovulation.
• It is safe effective and an acceptable contraceptive.
• Acceptable in the postpartum period as a means of spacing.
• Side effects: weight increase, irregular menstrual bleeding.
(b) NET-EN• Norethisterone enantate is given as i.m
injection dose of 200mg. every 60 days.
• Contraceptive action is by inhibiting ovulation and progesterogenic effects on cervical mucus.
ADMINISTRATION:• Both DMPA ,NET-EN should be given
during first five days of menstrual period.

• The injection site should never be massaged following injections.
SIDE-EFFECTS:• Unpredictable bleeding• AmenorrheaCONTRAINDICATIONS:• Breast cancers, all genital cancers.

B. COMBINED INJECTABLE :• They contain a progestogen and an oestrogen.• Given at monthly intervals.• Act by suppressing ovulation ,cervical mucus is
affected mainly by progestogen and inhibits sperm penetration.
• CONTRAINDICATIONS: confirmed or suspected pregnancy; past or present evidence of thromboembolic disorders; cerebrovascular or coronary artery disease; focal migraine; malignancy of breast and diabetes with vascular complications.
2. SUBDERMAL IMPLANTS:• Norplant : it consists of 6 silastic capsules
containing 35mg of levonorgesterel.
• The capsules are implanted beneath the skin of forearm or upper arm.
• Effective contraception is provided for 5
years.
• The contraceptive effect of Norplant is reversible on removal of capsules.
• DISADVANTAES: irregularities of menstrual bleeding and surgical procedures for inserting and removal of implants.
3. VAGINAL RINGS Vaginal rings containing levonorgesterel
are highly effective.
• The hormone is slowly absorbed through the vaginal mucosa , bypassing the digestive tract and liver and allowing a potentially lower dose.
• The ring is worn in the vagina for 3 weeks and removed for the 4th week.

POST CONCEPTIONAL PILL
Post Conceptional MethodsThese are the methods employed for the termination of the pregnancy.
It includesMenstrual regulation
Menstrual induction
Abortion
Menstrual regulation
• It consists of aspiration of uterine contents 6-14 days of a missed period but before most pregnancy tests can accurately determine whether or not a woman is pregnant.
• Complications : IMMEDIATE - Uterine perforation, Trauma LATE - Tendency to abortion, Infertility Menstrual disorders Increase in ectopic pregnancy Rh immunization
Menstrual regulation differs from abortion in the following respects :
• Lack of certainty if pregnancy is being
terminated.
• Lack of legal restrictions.
• Increased safety of early procedures.

Menstrual Induction
• Intrauterine application of 1-5 mg of PGF2
solution disturbs the normal progesterone prostaglandin balance.
• The uterus responds with a sustained contraction lasting about 7 minutes, followed by cyclic contractions continuing for 3-4 hours.
Abortion
• Definition : Termination of pregnancy before the foetus becomes viable (28wks).
• Types Spontaneous Induced• Spontaneous- Nature’s method of birth Control• Induced- Legal - MTP Illegal - Hazardous• In India, about 6 million abortions takes
place every year.

• Abortion Hazards :
Maternal morbidity and mortality• Complications :
Early Late
Hemorrhage Infertility
Shock Ectopic gestation
Sepsis Spontaneous abortion
Uterine perforation Reduced birth weight
Cervical injury
Thrombo embolism

Legislation of abortion
• MTP act was passed by Indian parliament in 1971. It came into force in April 1st 1972.
• It is a health care measure to reduce maternal morbidity and mortality resulting from illegal abortions.
Medical termination of Pregnancy Act• Conditions under which the pregnancy can be
terminated : Medical Eugenic Humanitarian Socio economic Failure of contraceptives•

Person who can perform abortion:
RMP having experience in OBG can perform abortion when the length of pregnancy does not exceed 12 weeks.
when the pregnancy is from 12-20 wks opinion of two RMP’s is necessary.
• Place where abortion can be done Govt. hospital or place approved for
purpose of this act.
MTP Rules 1975
• Initial rules and regulations are altered to eliminate time consuming procedure in MTP
• Approval by board: CMO of the district is empowered to certify a doctor to do abortion
• Qualification: If the doctor has assisted a RMP in performing 25 cases of MTP in a approved institution
• Place: Non Govt. institutions may also taken up abortions provided they obtain a license from CMO, District
• Illegal abortions are still rife although it is now more than 30 yrs MTP has been promulgated
“If abortion is considered as a disease, health education is the vaccine.”
Natural Methods of faMily PlaNNiNg

Miscellaneous Methods

Miscellaneous Methods• Abstinence
• Coitus interruptus
• Safe periods
• Natural family planning– basal body temperature– cervical mucus method– symptothermic method
• Breast feeding
• Birth control vaccine

Abstinence
• The only method of birth
control which is
completely effective is
complete
sexual abstinence
Coitus Interruptus
• This is the oldest method of voluntaryfertility controls.
• Widely practiced method.
• Preventing the deposition of the semen intothe vagina.
• Disadvantages– The pre-coital secretions of the male
may contain sperms.

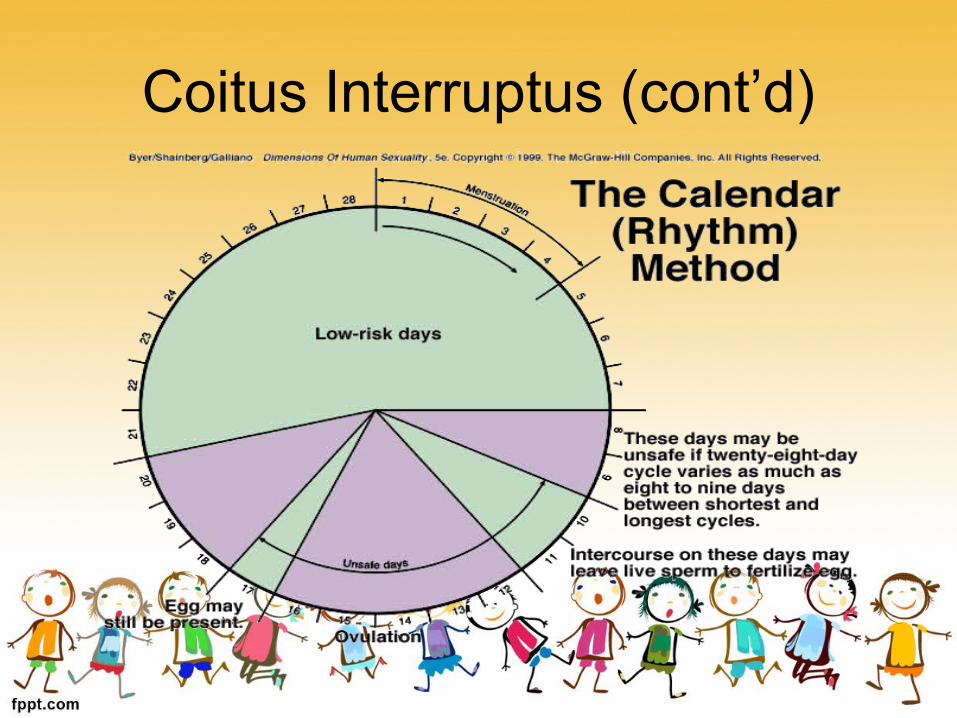
Safe Periods• It is also called
‘rhythm method’ or ‘calendar method’
• It is based on the fact that ovulation occurs from 12 to 16 days before the onset of menstruation.

Safe Periods (cont’d)
• The first day of the fertile phase is found by subtracting 18 days from the length of the shortest cycle.
• To find the last day of the fertile phase, subtract 11 days from the longest cycle.
• Sample– In this sample, the shortest menstrual cycle in
the past 6 months was 25 days. The longest menstrual cycle in the past 6 months was 35 days.

Coitus Interruptus (cont’d)• To calculate the fertile phase
– Subtract 18 from the shortest cycle (25 days) = 7
– Subtract 11 from the longest cycle(35 days) = 24
– This means the first day of the fertile phase is Day 7. The last day of the fertile phase is Day 24. If a couple is using this method to avoid intercourse during the fertile phase.
Coitus Interruptus (cont’d)

Coitus Interruptus (cont’d)• Disadvantages
– Women’s menstrual cycles are not always regular.
– It is only possible for this method to be used by educated and responsible couples with high degree of motivation and co operation.
– Compulsory abstinence of sexual intercourse for nearly one half of every month.
Coitus Interruptus (cont’d)
– This method is not applicable during the post-natal period.
– A high failure rate of 9 per 100 women years.
– Failures due to wrong calculations.
• Medical complications
– Ectopic pregnancy
– Embryonic abnormalities
Natural Family Planning Methods
• Variety of methods used to plan or prevent pregnancy, based on identifying the women’s fertile days.
• The term” natural family planning” is applied to three methods, they are …– basal body temperature method (BBT)– cervical mucus method– symtothermic method
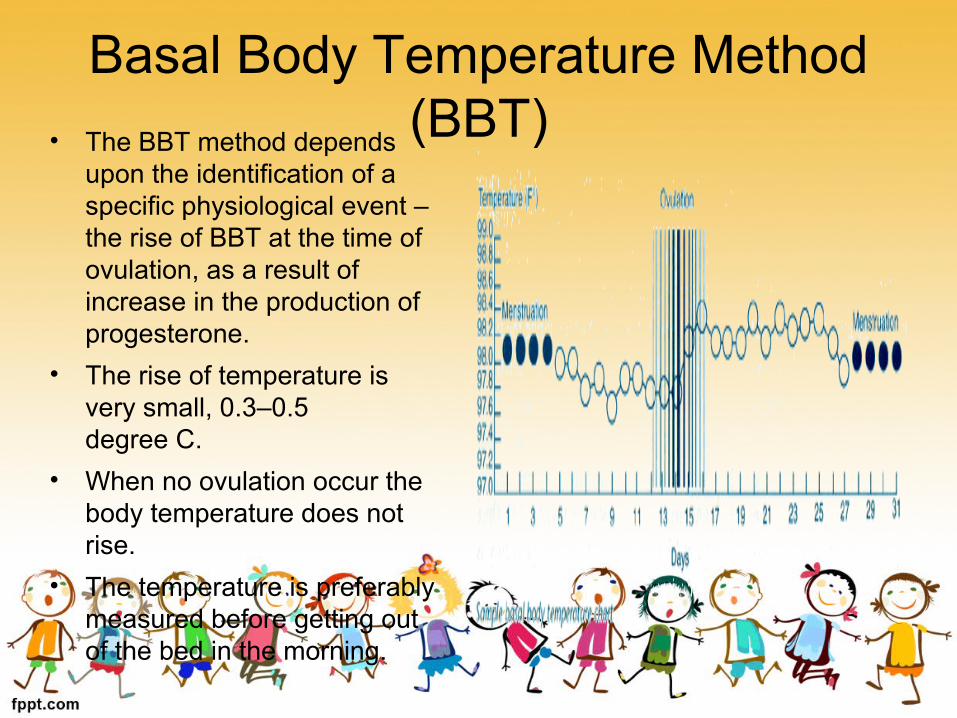
Basal Body Temperature Method (BBT)• The BBT method depends
upon the identification of a specific physiological event – the rise of BBT at the time of ovulation, as a result of increase in the production of progesterone.
• The rise of temperature is very small, 0.3–0.5degree C.
• When no ovulation occur the body temperature does not rise.
• The temperature is preferably measured before getting out of the bed in the morning.
Basal Body Temperature Method (BBT)
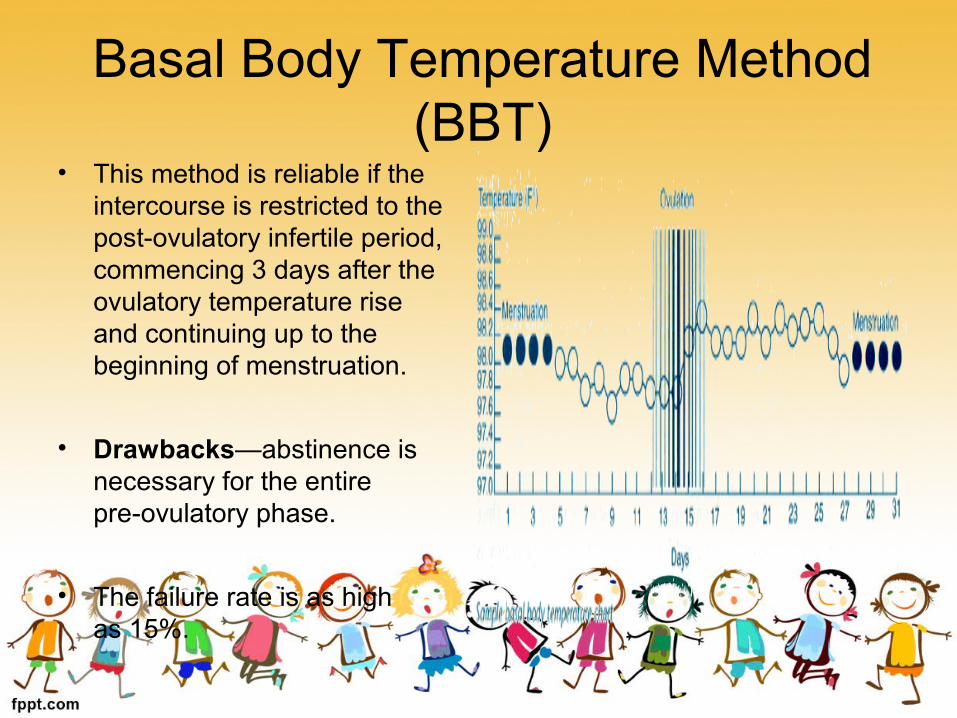
• This method is reliable if the intercourse is restricted to the post-ovulatory infertile period, commencing 3 days after the ovulatory temperature rise and continuing up to the beginning of menstruation.
• Drawbacks—abstinence is necessary for the entirepre-ovulatory phase.
• The failure rate is as highas 15%.
Cervical Mucus Method• This also known as “billings method” or “ovulation
method”.• This method is based on the observation of changes in
the characteristics of cervical mucus.• Cervical Mucus has regular, cyclic pattern changes. The
cycle starts with the beginning of period and ends at the beginning of the next period.
• At the time of ovulation, cervical mucus becomes watery clear resembling raw egg white, smooth, slippery and profuse.
• After ovulation ,under the influence of progesterone, the mucus thickens and lessens in quantity.
• From the beginning of the change in your mucus pattern until it disappears or changes (four days after the greatest volume) are the unsafe days.
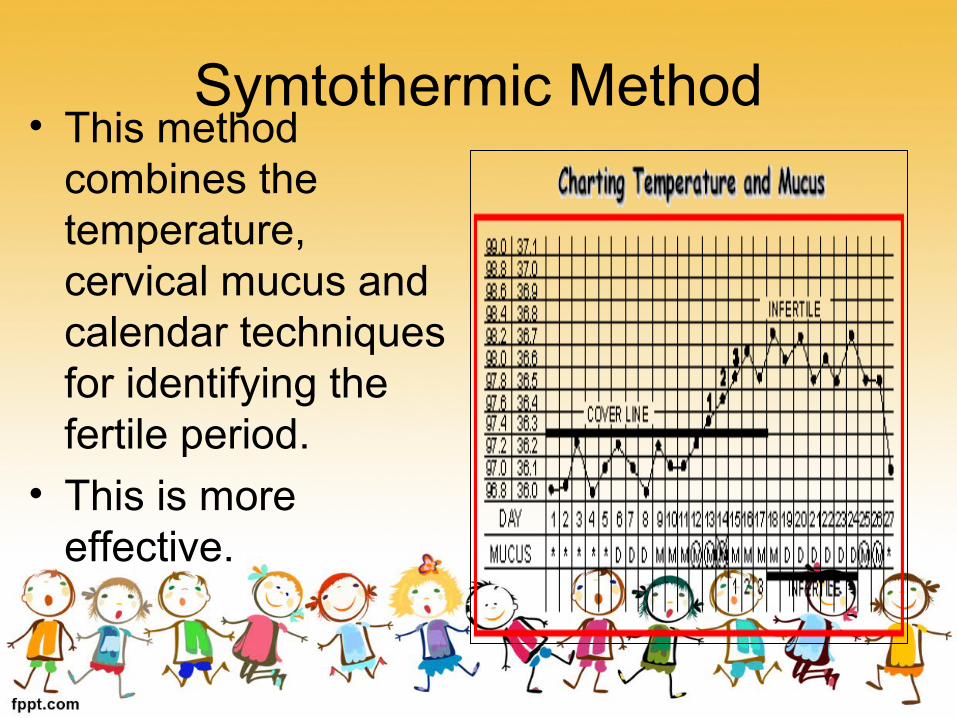
Symtothermic Method• This method
combines the temperature, cervical mucus and calendar techniques for identifying the fertile period.
• This is more effective.
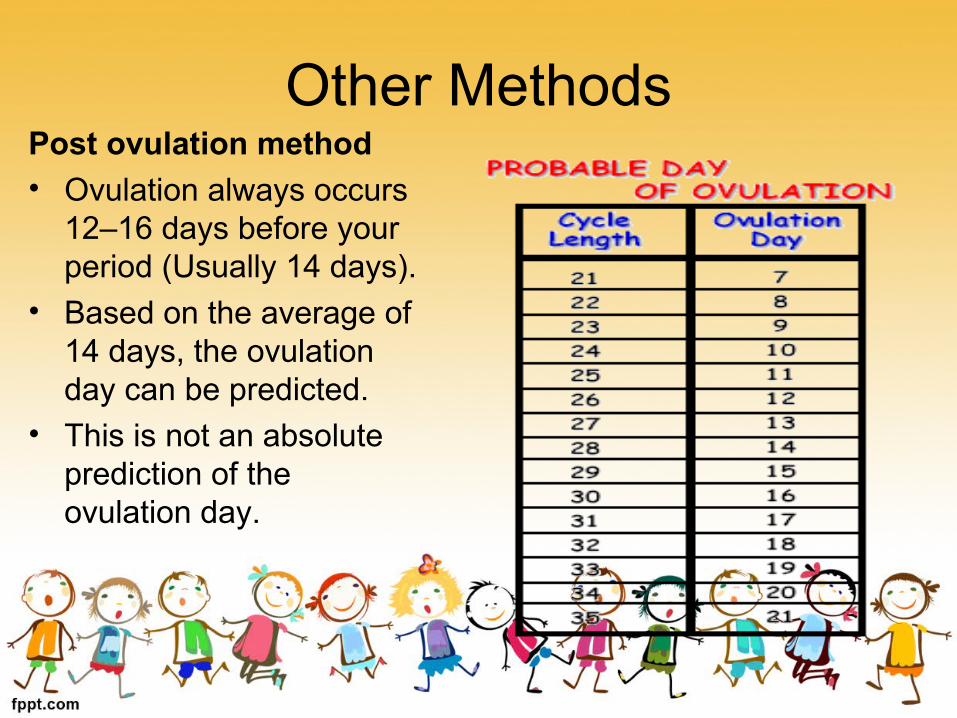
Other MethodsPost ovulation method• Ovulation always occurs
12–16 days before your period (Usually 14 days).
• Based on the average of 14 days, the ovulation day can be predicted.
• This is not an absolute prediction of the ovulation day.

The Two Day Method • The Two Day Method relies on a simple
algorithm, based upon the presence or absence of cervical secretions.
• If the woman notices any secretions on the current or previous day, then she is probably fertile today.
• If she notices no secretions today and yesterday (two days in a row without secretions), then she is not fertile today.
Breast-Feeding• Lactation prolongs postpartum amenorrhoea.• This is because levels of a certain hormone,
prolactin are increased.• However, once menstruation returns,
continued lactation no longer offers any protection against pregnancy.
• This method is most effective during the first 6 months of exclusive breastfeeding.
• Women using this method have a 2% chance of getting pregnant in the first 6 months.
Birth Control Vaccine• The most advanced research involves
immunization with a vaccine prepared from beta sub-unit of human chorionic gonadotropin (hCG).
• Immunization with hCG would block continuation of pregnancy.
• Antibodies appeared in about 4–6 weeks and reached maximum after about 5 months and slowly declined reaching zero levels after a period ranging from 6–11 months.
• The immunity can be boosted by a second dose.• But there are many uncertainties.

Terminal Methods of Sterilization
1. Male sterilization – Vasectomy (10-15%)2. Female sterilization – Tubectomy (85%)

Guidelines for family planning
Age of the husband should not be less than 25yrs or more than 50yrs
Age of the wife should not be less than 20yrs or more than 45 yrs
Couple must have 2 living children at the time of operation
If more than 3 children then the lower limit of age can be shortened
Informed consent required
Advantages of Terminal methods of Family Planning• Most effective method
• One time method
• Cost effective
• Does not require motivation

Male sterilization (VASECTOMY)
• First used in 1897 (experiments from 1785).
• Permanent sterilization in which the vasa deferentia of a man are cut and the cut ends are ligated.
• It is a minor surgical procedure.
• Can be performed by a trained MBBS doctor.
• NORMAL VASECTOMY- typically seals both ends of the vas deferens with stitches, heat, or both, after cutting.
• OPEN ENDED VASECTOMY- abdominal end of the resected vas in coagulated; testicular end is left open prevents congestive epididymitis.
• PER CUTANEOUS VAS-OCCLUSION (popular in China) - Polyurethane elastomere is injected into the vas which solidifies and forms a plug blocking sperm passage.
• NO SCALPEL VASECTOMY – commonly preferred technique at present.

Selection of candidates• Ideal-Sexually active and psychologically
adjusted husband having the desired number of children.
• Any misconception about the fear of castration, loss of hormones and impotency are to be removed by sympathetic conversation.
• Eczema & scabies on the scrotal area is a temporary contraindication.
• If hydrocele or hernia is present, it is corrected and then vasectomy is done.
Requirements
• Informed consent of the person is a must.
• The surgeon should be convinced about the family structure of the couple.
• Premedication not necessary.
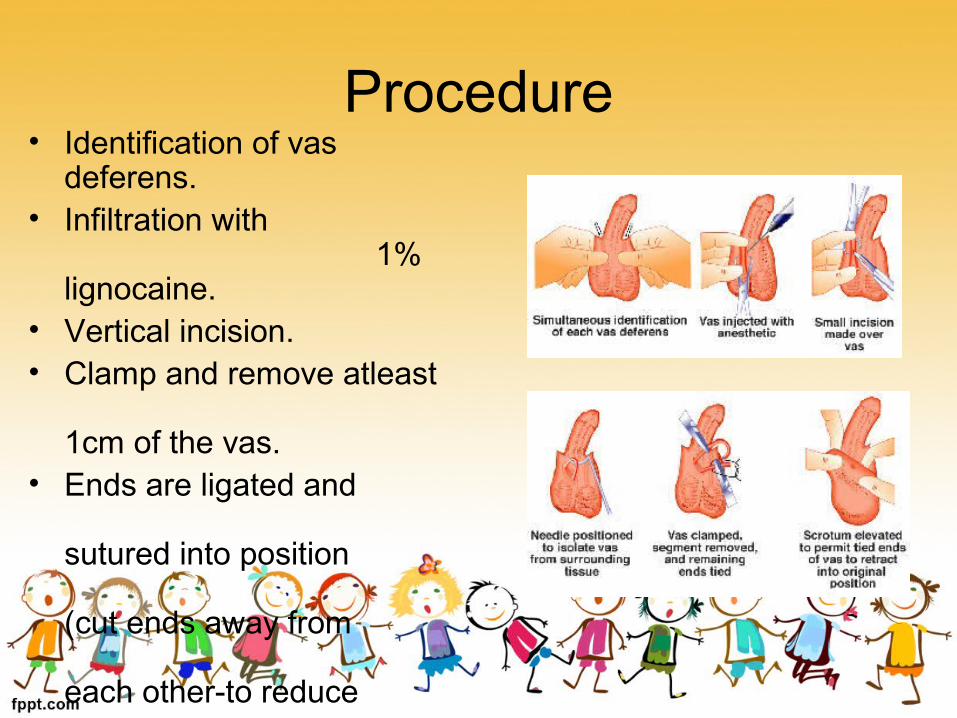
Procedure• Identification of vas
deferens.• Infiltration with
1% lignocaine.
• Vertical incision.• Clamp and remove atleast
1cm of the vas.
• Ends are ligated and sutured into position (cut ends away from each other-to reduce the risk of recanalisation)

Complications• Pain• Bruising and swelling (scrotal haematoma)• Infection (wound sepsiscellulitis &
abscess)• Sperm granuloma (5%)• Post-Vasectomy Pain Syndrome• Spontaneous Recanalization• Auto-immune response• Psychological

Post operative advice• At least 30 ejaculations may be
necessary for seminal examination to be negative (sterile)
• Usage of other methods of contraception until aspermia is established
• T-bandage or scrotal support to be worn for 15days
• Avoid cycling heavy work or lifting heavy weights
• Stitches removed on 5th day of operation

Advantages of Vasectomy• Simplicity of the surgical procedure• Lower cost • Effectiveness (early failure rates-below 1%, late failure
is very rare)• Done under local anaesthesia as opposed to general
anaesthesia usually needed for female sterilization.• Minimum training required• Can be done as an outdoor procedure or a mass
camp in remote villages• Complications – immediate or late are few

Causes of failure• Mistaken identifications of the vas
(histological examination is required).
• Spontaneous recanalisation.
• More than one vas on one side.
• Proper post-operative care not taken.

Social factors determining the acceptance of vasectomy
• Fear of impotency
• Lack of knowledge or awareness about vasectomy
• Apprehension regarding the surgery

REVERSAL

Reversal • By “Vasovasostomy”• First performed by Earl
Owen in 1971• Effective only in 50-70%
of the cases• Very costly procedure• Depends on the method
used and the time at which vasectomy was done (after 2 or more years occlusion of vas occurs)
• Sperm counts are not returned to normal

No scalpel Vasectomy (NSV)
• No-Scalpel Vasectomy is one of the most effective contraceptive methods available for males.
• First performed by a Chinese surgeon in 1974.
• It is an improvement on the conventional vasectomy with practically no side effects or complications.
• This new method is now being offered on a voluntary basis under the Family Welfare programme.
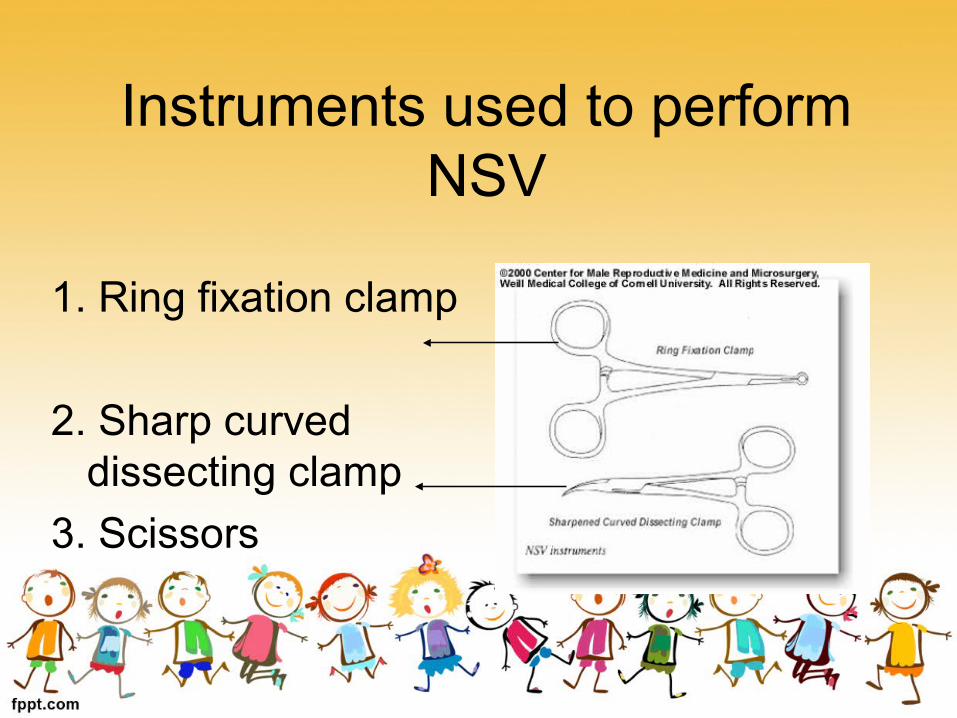
Instruments used to perform NSV
1. Ring fixation clamp
2. Sharp curved dissecting clamp
3. Scissors
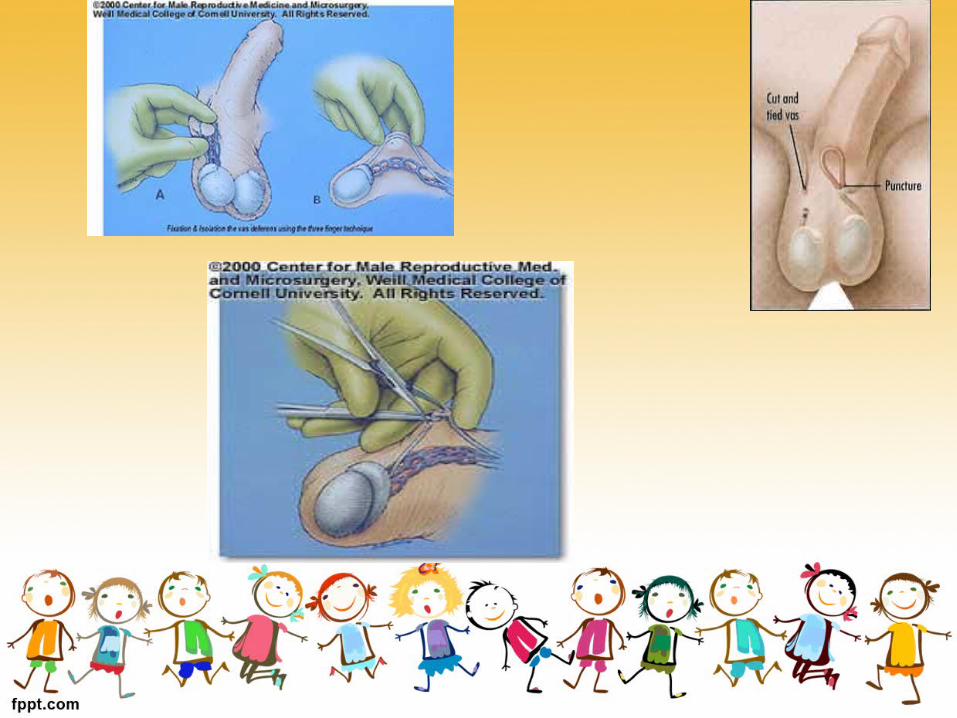
Procedure• Local anesthesia.• Vas deferens is fixed in the midline raphe of the
scrotum by a ring forceps.• A sharp curved dissections clamp is used to
puncture the skin, the puncture hole is enlarged to about twice the diameter of vas and the vas is delivered out.
• Part of the vas is dissected and ends ligated and then pushed back into the scrotum.
• Similar procedure done on the opposite side.• The puncture holes do not require any closure
(no suturing).

Advantages• Painless• Less invasive - no stitches or
sutures required• Less time-taking• Less discomfort• Economical• The person can leave the hospital
immediately after the procedure• Simpler than tubectomy (requires
hospitalization of the woman)• No side effects or complications• Quick recovery

Evaluation of Contraceptive methods &
Family planning

Evaluation of contraceptive methods
• Contraceptive methods are evaluated on the basis of Use – effectiveness.
• The two methods being used for measuring contraceptive efficacy are:-
1) Pearl index .
2) life – table analysis .
PEARL INDEX• It is defined as the number of “ failures per
100 women years of exposure (HWY) .”
• It is normally used for studying the effectiveness of a contraceptive.
Total accidental pregnancies
Failure rate per HWY= X 1200
Total months of exposure
• In the above formula, the numerator must include every known conception, whether this had terminated as live –births, still-births or abortions or had not yet terminated.
• The factor 1200 is the number of months in 100 years.
• The denominator is obtained by deducting from the period under review of 10 months for a full-term pregnancy,4 months for an abortion.
• A failure rate of 10 per HWY would mean that in the lifetime of the average woman about one-fourth or 2.5 accidental pregnancies would result , since the average fertile period of a woman is about 25 years .
• In designing and interpreting a use – effectiveness trial, a minimum of 600 months of exposure is usually considered necessary before any firm conclusion can be reached.
• The Pearl index is usually based on a specific exposure and, therefore , fails to accurately compare methods at various durations of exposure.
• This limitation is overcome by using the method of LIFE-TABLE ANALYSIS.

S.NO
Effectiveness in preventing pregnancy(pregnancies per 100users per year)
In Theory
In Practice
1 Vasactomy 0.15 0.2-0.5
2 Tubectomy 0.05 0.2-1
3 Implant 0.3 0.3
4 Injectable contraceptive 0.25 1
5 IUD 1-3 1-5
6 Oral contraceptive 0.5 1-8
7 Progestin – only pill 1 3-10
8 Condom 1-2 3-15
9 Diaphragm 2 4-25
10 Vaginal(chem.) contraceptives 3-5 10-25
11 Vaginal cont. sponge 11 15-30
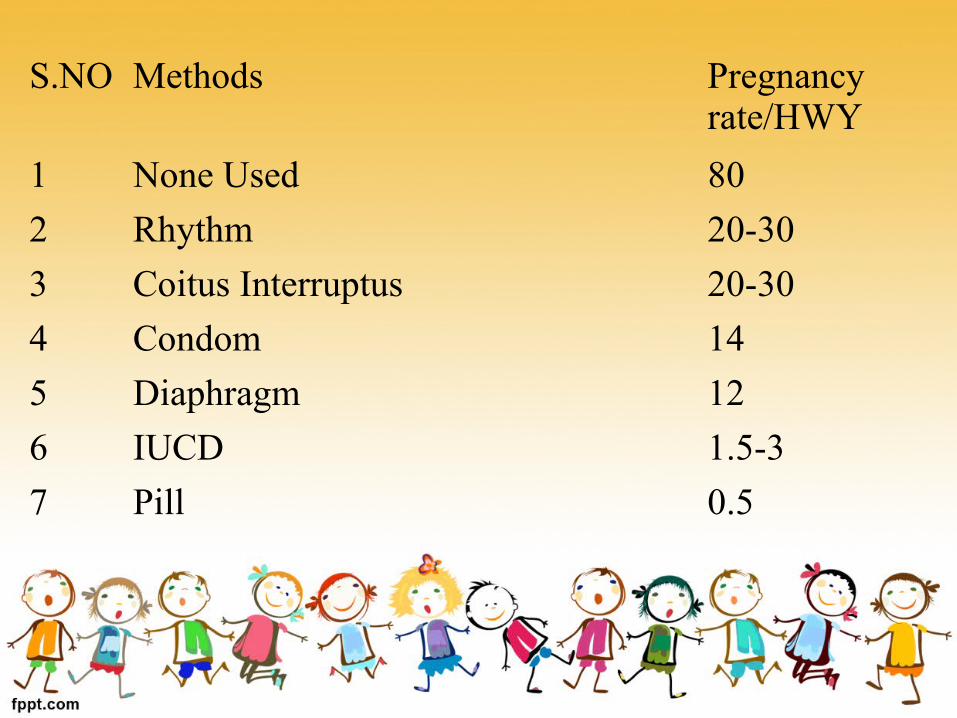
S.NO Methods Pregnancy rate/HWY
1 None Used 80
2 Rhythm 20-30
3 Coitus Interruptus 20-30
4 Condom 14
5 Diaphragm 12
6 IUCD 1.5-3
7 Pill 0.5
LIFE TABLE ANALYSIS• It caliculates a failure rate for each month of
use.
• A cumulative failure rate can then compare methods for any specific length of exposure.
• Women who leave a study for any reason other than unintended pregnancy are removed from the analysis, contributing their exposure until the time of the exit.
UNMET NEED FOR FAMILY PLANNING
• It was first explored in 1960s, when data from surveys of contraceptive knowledge attitude and practices (KAP) showed a gap between some women reproductive intention & their contraceptive behaviour.
• One of the first published use of the term “Unmet need” appeared in 1977.
• Many women who are sexually active would prefer to avoid becoming pregnant, but nevertheless are not using any method of contraception.
• These women are considered to have an “Unmet need” for family planning.

• The concept is usually applied to married women. however , it can applied to sexually active fecund women
and perhaps to men, but its measurement has been limited to married women only.
• It poses a challenge to family planning programme-to reach and serve millions of women whose reproductive attitude resembles those of contraceptive user.
• The most common reason for unmet need are-inconvenient or unsatisfactory services, lack of information, fears about contraceptive side effects and opposition from husband or relatives.
• According to the National Family Health Survey -2, about 16% of currently married women in India have an unmet need for family planning, the unmet need for spacing the births is the same as the unmet need for limiting the births.

• Unmet need for family planning is highest (27%) among women below age 20years and is almost entirely for spacing the births rather than for limiting the births.
• It is also relatively high for women in age group 20-24 years(24%) with about 75% of the need being for spacing the births.
• The unmet need for contraception among women aged 30 yrs and above are mostly limiting the births.
• Unmet need for family planning is higher in rural areas than urban areas.
• It is also varies by women education & religion.

• Mary is a 47 year old who has come in for a routine cervical smear. She asks when her Multiload IUD should be changed as it has been in for 6 years now. She is P2G3.
• Advise her it needs changing as soon as convenient • Discuss that it can remain until after menopause • Take out her IUD now and advise her she needs to use condoms until another can be inserted
Case 2
• Jotsna comes to talk to you about an IUD. She is a 20 year old P0G0 in a long term relationship. She likes the idea of having a contraceptive method that doesn’t contain hormones but her periods are already quite heavy and painful.
• that copper IUDs have no hormones but may worsen heavy, painful periods especially initially
• • Hormone releasing IUSs don’t usually cause hormonal side effects and will help her heavy, painful periods
• • • All of the above
Case 3
• Angha comes in to get emergency contraception. The condom broke last night. Her LMP started 12 days ago and she has a regular monthly cycle. She doesn’t take any medications. Her BMI is 32

• Give her I pill now but advise her she needs a postcoital IUD and arrange this for her

Case 4
• Preet wants to “go on the pill” and would like to try Mala D as her friend likes it. You check her personal and family history and her BP and BMI. All straightforward.

• You recommend she start with a second generation pill