family involvement in managing medications of older
TRANSCRIPT

RESEARCH ARTICLE Open Access
Family involvement in managingmedications of older patients acrosstransitions of care: a systematic reviewElizabeth Manias1* , Tracey Bucknall1,2 , Carmel Hughes3 , Christine Jorm4,5 and Robyn Woodward-Kron6
Abstract
Background: As older patients’ health care needs become more complex, they often experience challenges withmanaging medications across transitions of care. Families play a major role in older patients’ lives. To date, there hasbeen no review of the role of families in older people’s medication management at transitions of care. This systematicreview aimed to examine family involvement in managing older patients’ medications across transitions of care.
Methods: Five databases were searched for quantitative, qualitative and mixed methods empirical studies involvingfamilies of patients aged 65 years and older: Cumulative Index to Nursing and Allied Health Literature Complete, Medline,the Cochrane Central Register of Controlled Trials, PsycINFO, and EMBASE. All authors participated independently inconducting data selection, extraction and quality assessment using the Mixed Methods Appraisal Tool. A descriptivesynthesis and thematic analysis were undertaken of included papers.
Results: Twenty-three papers were included, comprising 17 qualitative studies, 5 quantitative studies and one mixedmethods study. Families participated in information giving and receiving, decision making, managing medicationcomplexity, and supportive interventions in regard to managing medications for older patients across transitions of care.However, health professionals tended not to acknowledge the medication activities performed by families. Whilefamilies actively engaged with older patients in strategies to ensure safe medication management, communicationabout medication plans of care across transitions tended to be haphazard and disorganised, and there was a lack ofshared decision making between families and health professionals. In managing medication complexity acrosstransitions of care, family members perceived a lack of tailoring of medication plans for patients’ needs, and believedthey had to display perseverance to have their views heard by health professionals.
Conclusions: Greater efforts are needed by health professionals in strengthening involvement of families in medicationmanagement at transitions of care, through designated family meetings, clinical bedside handovers, ward rounds, andadmission and discharge consultations. Future work is needed on evaluating targeted strategies relating to familymembers’ contribution to managing medications at transitions of care, with outcomes directed on family understandingof medication changes and their input in preventing and identifying medication-related problems.
Keywords: Transitions of care, Family, Medication management, Older patients, Family involvement, Hospitals, Home,Aged care facilities
© The Author(s). 2019 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, andreproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link tothe Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver(http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
* Correspondence: [email protected] for Quality and Patient Safety Research, School of Nursing andMidwifery, Deakin University, 221 Burwood Highway, Burwood, VIC 3125,AustraliaFull list of author information is available at the end of the article
Manias et al. BMC Geriatrics (2019) 19:95 https://doi.org/10.1186/s12877-019-1102-6

BackgroundAs older patients’ needs develop increased complexity,they are more likely to have changes in their health thatrequire treatment with medications. When older patientsbecome acutely ill, hospitalisation may be required,which necessitates medication management across tran-sitions of care. ‘Transitions of care’ refers to the timeswhen patients transfer between settings of care, such ashospitals, home, rehabilitation care and long-term care,between locations or within the same location, includingadmission and discharge [1]. Medication errors are likelyto occur at transitions of care because of the potentialfor communication breakdown during activities such asbedside handovers, ward rounds, and admission and dis-charge consultations between health professionals, olderpatients and families [2]. Previous research has shownthat medication error rates associated with transitionsbetween hospitals, residential aged care facilities andhome vary between 19 and 80% [3, 4].Many medication management activities are carried
out by families of older patients. These activities include:assisting with administering medications, recognisingtherapeutic benefits and adverse effects of medications,and clarifying information for patients [5, 6]. To date,there has been no review of the role of families in olderpeople’s medication management at transitions of care.Therefore, the aim of this systematic review was toexamine family involvement in managing older patients’medications across transitions of care. A specific mnemonicfor systematic reviews, PICo, was used to develop theresearch question. The components for the research ques-tion according to PICo are population (families),phenomenon of interest (managing older patients’ medica-tions) and context (transitions of care) [7]. The researchquestion that guided the systematic review is: how are fam-ilies involved in managing older patients’ medicationsacross transitions of care?
MethodsA systemic review was undertaken of research studiesusing a best practice guide for conducting systematicreviews [8].
Eligibility criteriaInclusion criteria comprised research of any design –qualitative, quantitative and mixed methods – involvingfamilies of older patients aged 65 years and older. Familieswere defined as formal relations of older patients or othersignificant individuals who played an important role in theolder people’s lives. Research had to involve older peoplemoving between different settings. Papers were still con-sidered if medication management was not the centralfocus of the study but was identified within the findings.Papers not published in English were excluded.
Information sourcesThe literature search was conducted in the followingelectronic bibliographic databases from inception to endDecember 2017: The Cumulative Index to Nursing andAllied Health Literature (CINAHL) Complete (Elton B.Stephens Co Host (Ebscohost)), Medical LiteratureAnalysis and Retrieval System Online (MEDLINE) (Ebs-cohost), the Cochrane Central Register of ControlledTrials (CENTRAL) (The Cochrane Library), Psycho-logical Information Database (PsycINFO) (Ebscohost),and Excerpta Medica Database (EMBASE) (refer toAdditional file 1 for Medline search) [9]. Hand searchingof reference lists was also conducted for relevant studies.Cochrane systematic reviews were searched to locaterelevant papers. However, reviews themselves were notincluded in the final dataset. The grey literature was alsosearched using Google Scholar to locate other original,peer-reviewed research.
Search and study selectionThe following key terms, and variations thereof, weresearched as four separate groups of terms: (1) family,carers, caregivers, and relatives; (2) older patients, olderpeople, and older adults, geriatric, seniors, elderly; (3)medication, medicines, medication management andmedicines management; and (4) admission, discharge,transfer, transition, transitions of care, and transitionpoints. These terms were subsequently combined. Oneauthor completed the search with assistance from theuniversity research librarian, and all authors independ-ently determined the eligibility of retrieved papers forinclusion at the abstract and full text levels. The authorscomprised individuals with different perspectives anddiscipline expertise. It was therefore perceived there wasvalue in each author independently checking the litera-ture to minimise selection bias, and to improve the rigorof the study selection process. There were a number ofstudies identified at the initial search that investigatedfamily involvement at transitions of care. At the full textlevel, unless there was some mention in the results offamilies’ contribution in older patients’ medications, aparticular study was excluded.
Data extraction and evaluationInformation was extracted from each paper on the typeof study conducted, and the settings in which each studywas undertaken. Information was also noted on the datacollection processes used, and the patients and familieswho participated. To prepare the data for synthesis,qualitative and quantitative data located within the re-sults section of papers were extracted and incorporatedinto a spreadsheet.Each paper was independently assessed by two
reviewers using the Mixed Methods Appraisal Tool
Manias et al. BMC Geriatrics (2019) 19:95 Page 2 of 21

(MMAT), which provided a quality score for qualitative,quantitative and mixed-method studies [10]. Any dis-crepancies were discussed until consensus was reached.No studies were excluded because of the quality score.
Data synthesisData synthesis of qualitative data was achieved using athematic approach. These data were read and re-read toincrease familiarity and understanding with the content.Line-by-line coding was undertaken using words andphrases within and across studies. Words and phraseswere grouped together, which were clustered into cat-egories. These categories were further examined foridentification of themes and subthemes [11].In synthesising quantitative results, it was not possible
to undertake meta-analysis due to the heterogeneity ofoutcomes and variability in operational definitions.Therefore, a descriptive synthesis was conducted of themajor findings. These quantitative studies were alsoexamined to determine how the results fitted into thethemes and subthemes generated from qualitative data.All quantitative data that were transferred to a spread-sheet were subsequently re-written and transformed intonarrative forms to describe and explain the results.These rewritten narrative forms were read several timesand examined to determine how they could be identifiedas categories. These categories were compared andcontrasted with other categories to determine how theycould be grouped into already developed themes andsubthemes, or whether they could be grouped into newthemes and subthemes. All authors scrutinised the con-tent and structure of themes and subthemes, and the waysin which studies of different research designs were repre-sented and mapped within these themes and subthemes.By means of an example, the quantitative results of the
Towle et al. paper [12] were integrated into themes in thefollowing way. The results were rewritten in a descriptiveway to explain the impact of an evidence-based qualityimprovement initiative to enhance patient and family pre-paredness in care transition. The following details weredocumented. After implementation of the quality improve-ment initiative, health professionals interacted with pa-tients and families in goal-directed ways to conveyinformation. Subsequently, family members’ understandinghad improved of the patients’ medical condition, medica-tions prescribed, treatment plan and follow up care. Theseresults mapped onto the theme: Giving information andreceiving feedback, and the subtheme: health professionalsinforming families. The results also mapped onto thetheme: Managing medication complexity across transitionsof care and the subtheme: supporting family participationin interventions. Mixed methods studies were handledaccording to the approaches described for both qualitativeand quantitative data. Only information from the results
section of included studies was used for synthesis and noinformation was used from the discussion section.
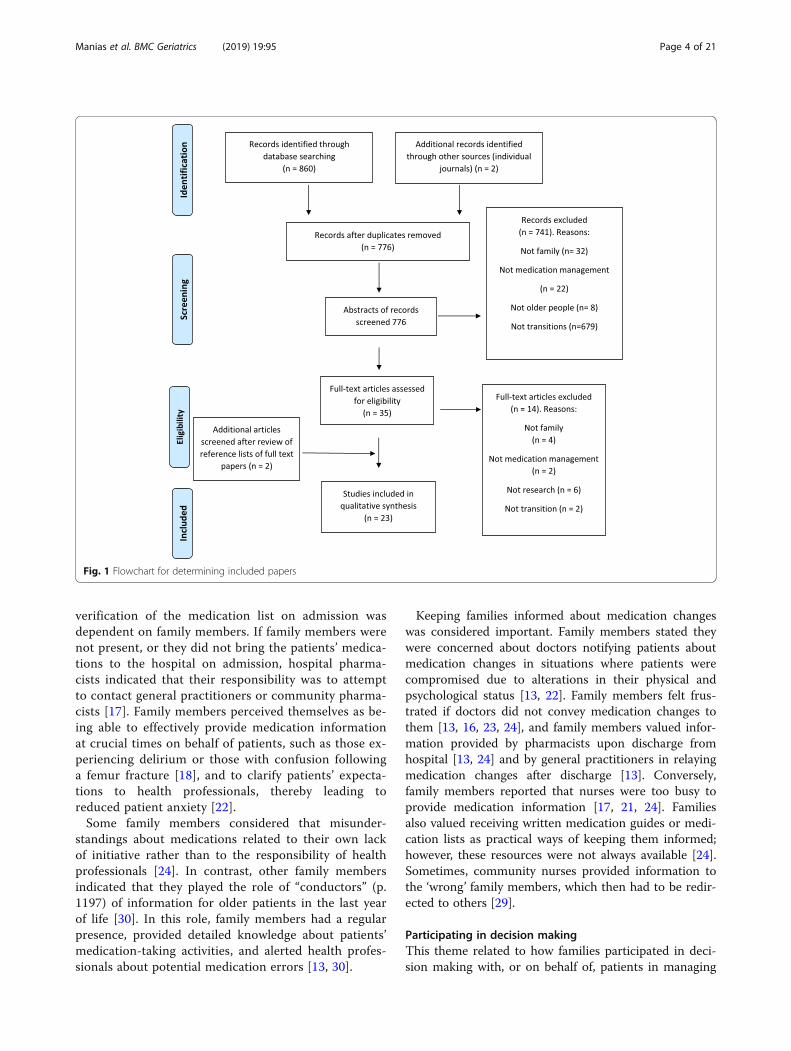
ResultsIn all, 860 papers were identified through databasesearching. An additional two papers were added follow-ing a manual screen of full text papers. A total of 23papers were eligible for inclusion (Fig. 1).Qualitative exploratory designs comprised data collection
methods involving semi-structured interviews (n = 11),observations (n = 2), diaries and interviews (n = 2), andfocus groups and interviews (n = 2). Quantitative designsincluded two randomised controlled trials, one quasi-ex-perimental study, two cross-sectional survey studies, andone mixed method study comprising interviews and anelectronic medical record review. MMAT findings showedthat 15 studies obtained a score of 75%, which meant thatthree-quarters of the criteria were met, and 6 had a score of50%, which meant that half of the criteria were met(Table 1).Four themes were identified: giving information and
receiving feedback, participating in decision making,managing medication complexity across transitions ofcare, and supporting family participation in interven-tions (Table 2).
Giving information and receiving feedbackEighteen studies addressed the theme of giving informa-tion and receiving feedback [12–29]. There were twosubthemes relating to this theme: families conveying infor-mation to health professionals about patients’ medication-taking behaviour and activities, and health professionalsinforming families about medication changes.Families played a crucial role in information giving
during patient admission to hospital, when patients withdementia moved to long term care [16], for patientsreceiving palliative care [28] or in their last year of life[30] and when patients moved from hospital to home[13, 18, 21, 24, 25, 29]. Family members perceived thattheir role was as ‘knowledge keepers’ about patients’medications, particularly those with chronic conditions[16, 18]. Whilst some family members indicated thatthey understood how to administer medications, theywere less clear about how these medications worked andtheir potential adverse effects, especially for patientswho had experienced a recent critical event, such as astroke [26, 29].In patients who lacked cognitive capacity such as
those with dementia, hospital doctors indicated that itwas difficult for them to obtain and verify a completeand accurate list of current medications, and to ad-dress the discrepancies between the medication listand medications actually consumed by patients [17]. Inthese situations, hospital pharmacists perceived that
Manias et al. BMC Geriatrics (2019) 19:95 Page 3 of 21
verification of the medication list on admission wasdependent on family members. If family members werenot present, or they did not bring the patients’ medica-tions to the hospital on admission, hospital pharma-cists indicated that their responsibility was to attemptto contact general practitioners or community pharma-cists [17]. Family members perceived themselves as be-ing able to effectively provide medication informationat crucial times on behalf of patients, such as those ex-periencing delirium or those with confusion followinga femur fracture [18], and to clarify patients’ expecta-tions to health professionals, thereby leading toreduced patient anxiety [22].Some family members considered that misunder-
standings about medications related to their own lackof initiative rather than to the responsibility of healthprofessionals [24]. In contrast, other family membersindicated that they played the role of “conductors” (p.1197) of information for older patients in the last yearof life [30]. In this role, family members had a regularpresence, provided detailed knowledge about patients’medication-taking activities, and alerted health profes-sionals about potential medication errors [13, 30].
Keeping families informed about medication changeswas considered important. Family members stated theywere concerned about doctors notifying patients aboutmedication changes in situations where patients werecompromised due to alterations in their physical andpsychological status [13, 22]. Family members felt frus-trated if doctors did not convey medication changes tothem [13, 16, 23, 24], and family members valued infor-mation provided by pharmacists upon discharge fromhospital [13, 24] and by general practitioners in relayingmedication changes after discharge [13]. Conversely,family members reported that nurses were too busy toprovide medication information [17, 21, 24]. Familiesalso valued receiving written medication guides or medi-cation lists as practical ways of keeping them informed;however, these resources were not always available [24].Sometimes, community nurses provided information tothe ‘wrong’ family members, which then had to be redir-ected to others [29].
Participating in decision makingThis theme related to how families participated in deci-sion making with, or on behalf of, patients in managing
Fig. 1 Flowchart for determining included papers
Manias et al. BMC Geriatrics (2019) 19:95 Page 4 of 21

Table
1Characteristicsof
includ
edpape
rsexam
iningfamily
involvem
entformanagingmed
ications
ofolde
rpatientsacross
transitio
nsof
care
(N=23)
Autho
r,year,cou
ntry,M
MAT
result
Designandsetting
Descriptio
nof
stud
yParticipants
KeyFind
ings
Allenet
al.2017[13]
Australia***
Design:Qualitative
exploratory.
Setting:
metropo
litan
public
health-carene
twork
Datacollection:interviews.
Transitio
npo
intsinvolved
:acute
wardsettingandrehabilitation
settingin
hospital,ho
me.
Med
icationmanagem
entprocess
involved
:adm
ission
instruction,
dischargeinstruction.
Patientsn=19.
78.9years(age
rang
e45–94
yearsforpatientsand
families).
Gen
der:no
tstated
.Family
n=7.
Gen
der:no
tstated
.
Caringrelatio
nships
with
health
profession
als:
-Nursesin
rehabilitationattend
edto
follow-up
phon
ecalls
tocheckon
dischargemanagem
ent.
-Lack
ofcontinuity
ofmed
icalpractitione
rsand
interactions
with
multip
lemed
icalpractitione
rs.
-Med
icalde
cision
makingabou
tdischarge
med
ications
with
outun
derstand
ingabou
tmed
ications
prescribed
byothe
rmed
ical
practitione
rs.
Seekinginform
ation:
-Ifpatientswas
tooun
welltoseek
inform
ation
durin
gtheiracuteillne
ss,fam
ilywantedto
have
med
icationinform
ationon
theirbe
half.
-Expe
ctationthat
doctorswou
ldsharemed
ication
inform
ationwith
them
durin
gtheho
spital
admission
.Thisdidno
talwaysoccur.
-Family
mem
berswerewellinformed
abou
tchange
sto
med
ications
inrehabilitationward
setting.
-Gen
eralpractitione
r(GP)
reliedon
accurate
and
timelydischargesummaryto
explainmed
ication
inform
ationto
family.
Colem
anet
al.2006[15]
UnitedStates**
Design:Rand
omised
controlledtrial.
Setting:
oneho
spital,eigh
tskilled
nursingfacilities,on
eho
mehe
alth
care
agen
cy.
Datacollection:ratesof
reho
spitalisationmeasuredat
30,90,
and180days.
Transitio
npo
intsinvolved
:commun
ity;skillednu
rsingfacility;
reho
spitalisation.
Med
icationmanagem
entprocesses
involved
:med
icationself-
managem
ent.
Interven
tion–four
pillars.
-Supp
ortpatientsandfamily
with
med
icationself-managem
ent,
med
icationreconciliation.
-Patient-cen
tred
record
toassist
with
site
transitio
ns.
-Timelyfollow-upwith
care.
-Supp
lypatientsandfamily
with
list
of“red
flags”forworsening
cond
ition
.
Patients:
n=379interven
tiongrou
p,n=371controlg
roup
.Age
forinterven
tiongrou
p:mean76.0years(SD7.1
years).
Age
forcontrolg
roup
:mean
76.4years(SD6.8years).
Gen
der:48%
femalefor
interven
tiongrou
p.52%
femaleforcontrol
grou
p.Med
icalcond
ition
:atleast1
of11
selected
acuteor
chroniccond
ition
s.Family
recruitedwith
patients:
n=no
tspecified
.Relatio
nshipwith
patient:not
specified
.
Outcomes:
Reho
spitalisationratesat
30days
–Interven
tiongrou
p=8.3%
Con
trol
grou
p=11.9%,p
=0.048.
Reho
spitalisationratesat
90days
–Interven
tiongrou
p=16.7%
Con
trol
grou
p=22.5%,p
=0.040.
Reho
spitalisationratesforthesamecond
ition
that
precipitatedtheinde
xho
spitalisationat
90days
–Interven
tiongrou
p=5.3%
Con
trol
grou
p=9.8%
,p=0.04.
Reho
spitalisationratesforthesamecond
ition
that
precipitatedtheinde
xho
spitalisationat
180days
-Interven
tionpatients:8.6%
Con
trol
patients:13.9%,p
=0.046.
Meanho
spitalcostsat
180days
-Interven
tionpatients:$2058
Con
trol
patients:$2546,log-transformed
p=0.049.
Colem
anet
al.2004[14]
UnitedStates***
Design:Quasiexpe
rimen
tal
stud
ywith
interven
tionand
controlg
roup
s.Setting:
onecommun
ity,
hospital.
Datacollection:ratesof
reho
spitalisationat
30,90and180
days;caretransitio
nmeasure
Transitio
npo
intsinvolved
:hospital,
commun
ityreside
ncefacility,ho
me.
Med
icationmanagem
entprocess
Patients:
n=158interven
tiongrou
p,n=1235
controlg
roup
from
administrativedata.
Age
forinterven
tiongrou
p:mean75.1years(SD6.4
Outcomes:
Reho
spitalisationat
30days
–Interven
tiongrou
pcomparedwith
controlg
roup
:0.52
(95%
confiden
ceinterval(CI)0.25,0.96)
Reho
spitalisationat
90days
–Interven
tiongrou
pcomparedwith
controlg
roup
:
Manias et al. BMC Geriatrics (2019) 19:95 Page 5 of 21

Table
1Characteristicsof
includ
edpape
rsexam
iningfamily
involvem
entformanagingmed
ications
ofolde
rpatientsacross
transitio
nsof
care
(N=23)(Con
tinued)
Autho
r,year,cou
ntry,M
MAT
result
Designandsetting
Descriptio
nof
stud
yParticipants
KeyFind
ings
involved
:med
icationself-
managem
ent.
Interven
tion–four
pillars.
-Supp
ortpatientsandfamily
with
med
icationself-managem
ent,
med
icationreconciliation.
-Patient-cen
tred
record
toassist
with
site
transitio
ns.
-Timelyfollow-upwith
care.
-Supp
lypatientsandfamily
with
list
of“red
flags”forworsening
cond
ition
.Interven
tioninvolved
:meetin
gswith
transitio
nscoach;commun
ication
tool
(personalised
med
icalrecord,
roleplays),follow
upph
onecalls.
years).
Age
forcontrolg
roup
:mean
78.5years(SD7.5years).
54%
femaleforinterven
tion
grou
p.55%
femaleforcontrol
grou
p.Med
icalcond
ition
:atleast
oneor
moreof
9med
ical
cond
ition
s.Family
recruitedwith
patients:
n=no
tspecified
.Relatio
nshipwith
patient:not
specified
.
0.57
(95%
CI0.25,0.72)
Reho
spitalisationat
180days
–Interven
tiongrou
pcomparedwith
controlg
roup
:0.57
(95%
CI0.36,0.92).
Interven
tiongrou
p-patientsrepo
rted
:highlevelo
fconfiden
cein
obtaininginform
ation,
commun
icatingwith
health
care
team
,and
unde
rstand
ingtheirmed
icationregimen
.Qualityof
care
transitio
nstaxono
my–
Interven
tiongrou
p:9.5%
ofpo
stho
spitaltransition
swerecomplicated
.Con
trol
grou
p:14.9%
oftransitio
ns,P
=0.35.
Crawford
etal.2015[16]
Australia***
Design:Qualitative,
exploratory.
Setting:
oneaged
rehabilitationandge
riatric
evaluatio
nandmanagem
ent
facility
Datacollection:
Semi-structuredinterviews.
Transitio
npo
intsinvolved
:acute
hospitalsettin
g,aged
rehabilitation
andge
riatricevaluatio
nand
managem
entfacility
Med
icationmanagem
entprocess
involved
:discharge
planning
.
Family
n=20.
Relatio
nshipwith
patient:
husbands,w
ives,d
augh
ters,
son,daug
hter-in
-law,close
frien
dsof
peop
lewith
demen
tia.
Them
es:
Adjustin
gto
new
rolefro
mcaregiverto
visitor–
-Difficulty
inrelinqu
ishing
role.
-Desire
tocontinue
tobe
involved
inde
cision
s.-Felton
goingrespon
sibilityto
commun
icate
med
icationne
eds.
-Beliefabou
tspecialised
know
ledg
eabou
trelative’s
care.
-Stayinginform
edhe
lped
caregiversto
cope
with
moveto
facility.
Deeks
etal.(2016)[17]
Australia**
Design:Qualitative,
exploratory.
Setting:
threeurbanprim
ary
andacutesites,on
erural
prim
aryandacutesite.
Datacollection:semi-structured
interviews.
Med
icationmanagem
entprocess
involved
:hospitaladm
ission
and
dischargeforpatientswith
demen
tia.
51participantscomprising
doctors,nu
rses,p
harm
acists,
occupatio
nalthe
rapists,
gene
ralp
ractition
ers,
Alzhe
imer’sAustraliastaff,
andfamily.
Family
n=no
tspecified
.Relatio
nshipwith
patient:not
specified
.
Them
es:
Med
icationreconciliation–
-Verifying
accurate
liston
admission
was
difficultif
family
mem
bersno
tpresen
tor
med
ications
not
brou
ghtto
hospital.
Lack
ofmod
ified
planning
forcare
transitio
ns–
-Lack
ofiden
tificationthat
patient
hadcogn
itive
prob
lemsas
they
moved
across
settings.
-Inadeq
uate
inform
ationabou
tmed
ication
change
sat
discharge.
-Carers’supp
ortforuseof
dose
administrationaids
bypatients,bu
tpo
tentialp
roblem
swith
errors.
Lack
ofassessmen
tof
patients’ability
touseaid.
-Desire
foron
ce-dailydo
sing
ifpaid
carerrequ
ired
tovisitat
homeafterdischarge.
Multip
leprescribers–
-Littleinform
ationshared
betw
eenprivateand
publicho
spitals.
-Treatm
entde
lays
betw
eenspecialistandge
neral
practitione
ras
commun
icationby
letter.
Reside
ntialage
dcare
facilities–
-Lack
ofaccurate
andcompleteinform
ationfro
m
Manias et al. BMC Geriatrics (2019) 19:95 Page 6 of 21

Table
1Characteristicsof
includ
edpape
rsexam
iningfamily
involvem
entformanagingmed
ications
ofolde
rpatientsacross
transitio
nsof
care
(N=23)(Con
tinued)
Autho
r,year,cou
ntry,M
MAT
result
Designandsetting
Descriptio
nof
stud
yParticipants
KeyFind
ings
hospital.
Med
icationreview
sby
pharmacists–
-Patientswith
demen
tiatrustedandbu
iltrapp
ort
with
commun
ityph
armacistsandge
neral
practitione
rs.Patientsno
treceptiveto
home
med
icinereview
s.
Dyrstad
etal.(2015)[18]
Norway**
Design:Qualitative,
exploratory.
Setting:
twoho
spitals
Datacollection:ob
servations,
conversatio
ns,o
bservatio
nalfield
notes.
Transitio
npo
intsinvolved
:tw
oem
erge
ncyde
partmen
ts(EDs),
sevenho
spitalw
ards;including
admission
sfro
mho
mebasedcare
ornu
rsingho
mes,and
discharge.
Med
icationmanagem
entprocess
involved
:adm
ission
instruction,
dischargeinstruction.
Patientsn=41.
Age
:mean86.0years,rang
e73–97years.
Gen
der:46%
female.
Med
icalcond
ition
:an
orthop
aedicdiagno
sisor
chroniccond
ition
,and
poly-
pharmacy(>
5med
ications
daily).
Family
n=28.
Relatio
nshipwith
patient:
son,daug
hter,w
ife.
Health
profession
alsn=no
tspecified
.Disciplines
involved
:paramed
ics,nu
rses,d
octors.
Them
es:
Inform
ationdissem
inationandde
cision
-making–
-Nosche
duleddischargeplanning
meetin
gswith
patient
andfamily.
-Nurse
phon
edfamily
toinform
them
ofdo
ctors’
decision
s.Nextof
kinim
portantadvocates–
-In
ED,p
rovide
dvaluableinform
ationabou
tmed
ications
takenbe
fore
admission
.-Family
administeredmed
ications
inED
durin
gbu
sytim
es.
-In
wards,noroutines
toinvite
family
toparticipate
ondo
ctor’sroun
ds.
-Inform
edon
dayof
dischargeabou
twardroun
dde
cision
s.-Somefamilies
hadto
seek
inform
ationabou
tmed
icationde
cision
sat
discharge.
Geo
rgiadis&Corrig
an2017
[19]
UnitedKing
dom***
Design:Ph
enom
enolog
ical.
Setting:
threeho
spitals.
Datacollection:Interview,aud
iodiary,writtendiary.
Transitio
npo
intsinvolved
:clinical
settings
(not
describ
ed),ho
me.
Med
icationmanagem
entprocess
involved
:med
icationcoun
selling
atdischarge.
18participants
Patientsn=12.
Age
:65.9years(SD17.2
years).
Gen
der:Mixed
,not
stated
.Med
icalcond
ition
:not
men
tione
d.Patientswith
non-med
icalcomplex
cond
i-tio
ns,w
hich
wereno
tde
fined
.Family
n=6.
Relatio
nshipwith
patient:not
specified
.
Them
es:
Limitedinvolvem
entin
discharge-care
prep
arations
– -Prem
aturedischarges
meant
lack
ofplanning
inmed
icationcoun
selling
.-Une
xpectedandde
layeddischarges
meant
that
family
unableto
bepresen
t.Weakserviceinterface
–-Expe
cted
organisatio
nof
appo
intm
entsfor
outpatient
clinicor
homevisitsdidno
thapp
en.
Relianceon
family
formed
icationadministration.
-Family
arrang
edprim
aryclinicto
assess
med
ications.
Haged
oorn
etal.2017[20]
TheNethe
rland
s***
Design:Qualitative
exploratory.
Setting:
Four
gene
ral
hospitals,
Datacollection:no
n-participantob
-servations,aud
io-recording
sof
planne
ddiscussion
sforadmission
anddischargediscussion
sandfamily
meetin
gs.
Transitio
npo
intsinvolved
:adm
ission
toward,
13clinicalwards
comprising
neurolog
y,pu
lmon
ary,internal
med
icine,cardiology,g
eriatrics.
Discharge
from
ward.
Med
icationmanagem
entprocess
involved
:adm
inistration,mon
itorin
g.
Patientsn=62.
Age
:76years(SD7.2years).
Gen
der:48%
female.
Med
icalcond
ition
:22
patients(36%
)had
3or
more
chronicdiseases.
Family
n=107at
planne
ddiscussion
s.Relatio
nshipwith
patient:
husband,
wife,son
,daugh
ter.
Them
es:
Socialne
tworksupp
ort–
-Supp
ortby
family
caregiversassistingwith
ormon
itorin
gmed
icationintake
atho
me.Not
addressedby
nurses
inho
spitalassessm
ent
sessions.
Coo
rdinationof
care
–-Duringdischargediscussion
snu
rses
review
edho
memed
icationlistwith
patientsandfamily.
-Family
askedspecificqu
estio
nsabou
tchange
sin
thepatients’ho
memed
ications.
Manias et al. BMC Geriatrics (2019) 19:95 Page 7 of 21

Table
1Characteristicsof
includ
edpape
rsexam
iningfamily
involvem
entformanagingmed
ications
ofolde
rpatientsacross
transitio
nsof
care
(N=23)(Con
tinued)
Autho
r,year,cou
ntry,M
MAT
result
Designandsetting
Descriptio
nof
stud
yParticipants
KeyFind
ings
Hvalvik&Reierson
,2015[21]
Norway***
Design:Ph
enom
enolog
ical
herm
eneutic
design
.Setting:
hospital.
Datacollection:in-dep
thinterviews.
Transitio
npo
intsinvolved
:hospital,
mun
icipalrehabilitation,short-term
care
facility,ho
me.
Med
icationmanagem
entprocess
involved
:discharge
planning
,self-
managem
entat
home.
Family
n=11.
Relatio
nshipwith
patient:
son,spou
se,d
augh
ter.
Them
es:
Balancingvulnerability
andstreng
th–
-Endu
ringem
otionalstresswith
discharge.
-Family
expe
cted
tobe
involved
indischarge,bu
twereno
tinclud
ed.
-Worry
abou
tbe
ingdischarged
tooearly
andlack
ofmed
icationinform
ation.
-Lack
ofcommun
icationabou
tmed
ications
durin
gstay.
-Senseof
respon
sibilityin
managingmed
ications.
-Lack
ofcommun
icationbe
tweenho
spitaland
commun
ityservices.Prescrip
tionof
med
ications
that
shou
ldhave
been
ceased
dueto
adverse
effectsor
allergies.
Cop
ingwith
analteredeveryday
life–
-Dealingwith
change
sto
family
routines.
-Anticipatingpo
ssibleprob
lemsifpatients
discharged
early.
-Com
preh
ensive
unde
rstand
ingabou
tolde
rpe
rson
’svulnerability,and
fragility.
Jeffs
etal.2017Canada***
Design:Qualitative
exploratory.
Setting:
orthop
edicinpatient
units
intw
oacutecare
hospitalsandon
eorthop
edic
unitat
acomplex
continuing
care
rehabilitationho
spital.
Datacollection:semi-structured
interviews.
Med
icationmanagem
entprocess
involved
:careinvolvingtransfer
from
anacutecare
hospitaltoa
rehabilitationho
spital.
Patientsn=13.
Age
:82.9years(rang
e:68–91
years).
Gen
der:69%
female.
Med
icalcond
ition
:non
-electivepatientswho
had
fallenor
sustaine
dafracture
thou
ghan
accide
nt.
Family
n=9.
Relatio
nshipwith
patient:
child,spo
use,partne
r,sibling.
Health
profession
alsn=50.
Them
es:
Watching–
-Alertto
med
icationadministrationandchange
sin
patients’status.
-Patients’lack
ofun
derstand
ingabou
tmed
ication
change
s.Beingan
activecare
provider
–-Respon
sibilityforprovidingcare
that
health
care
providerspe
rform
ed.
-Adm
inisterin
gmed
icationwas
easier
forfamily
todo
than
thenu
rses,asnu
rses
expe
rienced
challeng
eswith
thepatient
taking
med
ication.
-Lack
ofen
gage
men
tby
health
care
providers
abou
tinvolvingfamily.
Advocating–
-Beingsupp
ortiveof
patients’ne
edssuch
aschanging
med
icationtim
esto
suitpatients’
routines.
Navigatingthehe
alth
care
system
–-Askingqu
estio
nsandcoordinatin
gfollow-upcare.
-Arranging
appo
intm
entswith
vario
usmem
bersof
interdisciplinaryteam
.-Lack
ofavailabilityof
health
care
providersto
ask
questio
nsabou
ttransitio
nsplan.
King
etal.2013[23]
United
States***
Design:Qualitativestud
yusinggrou
nded
dimen
sion
alAnalysis.
Setting:
fiveno
n-profit
Datacollection:focusgrou
pand
individu
alinterviews
Transitio
npo
intsinvolved
:skilled
nursingfacilities,ho
spital.
Health
profession
alsn=27.
Disciplines
involved
:nurses.
Them
es:
Reconciling
hospitalinformation-
-Seekingmed
icationde
tails
from
families
was
prob
lematicas
sometim
esno
tadeq
uately
Manias et al. BMC Geriatrics (2019) 19:95 Page 8 of 21

Table
1Characteristicsof
includ
edpape
rsexam
iningfamily
involvem
entformanagingmed
ications
ofolde
rpatientsacross
transitio
nsof
care
(N=23)(Con
tinued)
Autho
r,year,cou
ntry,M
MAT
result
Designandsetting
Descriptio
nof
stud
yParticipants
KeyFind
ings
religious
andgo
vernmen
tskilled
nursingfacilities(SNF)
Med
icationmanagem
entprocess
involved
:hospitald
ischarge
.inform
edabou
tfamily
mem
berscontactde
tails.
-Askingfamilies
abou
tmed
icationde
tails
createda
poor
firstim
pression
ofSN
Fstaff.
Con
sequ
encesof
poor-qualitydischargecommun
i-catio
n–
-Carede
lays
andim
plem
entatio
nof
aninapprop
riate
med
icationplan.
-Inaccurate
hospitalinformationprod
uced
family
dissatisfaction.
-MadetheSN
Fappe
arun
organised.
Knight
etal.2013[24]
United
King
dom**
Design:Qualitative
exploratory.
Setting:
participants’hom
e
Datacollection:semi-structuredin-
terviews,med
icationdiary.
Transitio
npo
intsinvolved
:hospital,
home
Med
icationmanagem
entprocess
involved
:discharge
process.
Patientsn=7.
Age
:>75
years.
Gen
der:43%
female.
Med
icalcond
ition
:not
stated
.Family
n=12.
Relatio
nshipwith
patient:
wife,husband
.
Them
es:
Discharge
inge
neral–
-Long
delays
tilld
ischarge
orabrupt
notification
abou
tdischarge.
Obtaining
med
icationfordischarge-
-Waitin
gformed
ications
tobe
prep
ared
atho
spital
pharmacy.
Inform
ationregardingdischargemed
ication–
-Carer
beliefthat
itwas
theirrespon
sibilityto
check
unde
rstand
ingon
individu
almed
icines.
-Carer
satisfactionabou
tinform
ationprovided
but
notde
tailed.
-Med
icationchange
sin
hospitaln
otconveyed
tocarers.
-Inadeq
uate
explanations
ofne
wmed
icines
and
associated
risks
forthepatient.
Med
icationlists–
-Lack
ofwrittengu
ideavailableor
hadne
ver
received
alist.
Com
mun
icationabou
tmed
icationin
hospitaland
followingdischarge–
-Carersde
tected
med
icationom
ission
saftercareful
exam
ination.
-Neede
dto
feelbe
tter
prep
ared
with
med
ications
post-discharge
.
Lowsonet
al.2012United
King
dom***
Design:Qualitative
exploratory.
Setting:
participants’hom
e
Datacollection:semi-structured
interviews.
Transitio
npo
intsinvolved
:hospital,
home.
Med
icationmanagem
entprocess
involved
:med
icationinform
ationat
admission
.
Patientsn=27.
Age
:mean=79.0years(SD
4.25
years).
Gen
der:52%
female.
Med
icalcond
ition
:heart
failure
orcancer
inthelast
year
oflife.
Family
n=12.
Relatio
nshipwith
patient:
wife,husband
,daugh
ter,
sister,neigh
bour,friend
.
Them
es:
Con
ductors–
-Strong
contrib
utions
tomaintaining
good
care
throug
hout
illne
sstrajectory.
-Detailedknow
ledg
eabou
tmed
ications.
-Alerted
health
profession
alsabou
tpo
tential
med
icationerrors.
Second
fiddle–
-Followingho
spitaladm
ission
,abilityto
workwith
health
profession
alsto
influen
cede
cision
svastly
redu
ced.
-Carersinvested
effortin
maintaining
continuity
ofrelatio
nship.
Manias et al. BMC Geriatrics (2019) 19:95 Page 9 of 21

Table
1Characteristicsof
includ
edpape
rsexam
iningfamily
involvem
entformanagingmed
ications
ofolde
rpatientsacross
transitio
nsof
care
(N=23)(Con
tinued)
Autho
r,year,cou
ntry,M
MAT
result
Designandsetting
Descriptio
nof
stud
yParticipants
KeyFind
ings
-Advocated
onpatients’be
halfto
affect
bene
ficial
change
.
Nazarathet
al.2001United
King
dom***
Design:Rand
omised
controlledtrial.
Setting:
threege
neral
hospitals,one
long
-stay
hospital
Datacollection:
Transitio
npo
intsinvolved
:gen
eral
hospitalw
ards,hom
e.Med
icationmanagem
entprocess
involved
:discharge
inform
ation.
Interven
tion:(fo
rinterven
tion
stud
ies)Discharge
plansde
velope
dby
pharmacists,hom
evisitby
commun
ityph
armacist,coun
selling
patientsandfamily
onapprop
riate
dosesandpu
rpose.
Con
trol
grou
p:dischargeletter
toge
neralp
ractition
er.
Patients:
n=181interven
tiongrou
p,n=181controlg
roup
.Age
forinterven
tiongrou
p:mean84
years(SD5.2years).
Age
forcontrolg
roup
:mean
84years(SD5.4years).
Gen
der:
62%
femaleforinterven
tion
grou
p.66%
femaleforcontrol
grou
p.Med
icalcond
ition
:had
ameanof
threechronic
cond
ition
s.Family
(n=no
tspecified
)Includ
edin
interven
tionbu
tno
tstated
.
Outcomes:
Hospitalreadm
ission
at3mon
ths–
Interven
tiongrou
p:64
(39%
)Con
trol
grou
p:69
(39.2%
),p>0.05.
Hospitalreadm
ission
at6mon
ths–
Interven
tiongrou
p:38
(27.9%
)Con
trol
grou
p:43
(28.4%
),p>0.05
Nodifferences
betw
eengrou
ps:Patients’ge
neral
well-b
eing
,satisfactionwith
theserviceand
know
ledg
eof
andadhe
renceto
prescribed
med
ica-
tion(p>0.05).
Neiterm
anet
al.2015[25]
Canada**
Design:Qualitative
exploratory.
Setting:
participants’hom
e
Datacollection:interviews
Transitio
npo
intsinvolved
:hospital,
home
Med
icationmanagem
entprocess
involved
:med
icationmanagem
ent
atho
me
Patientsn=17.
Age
:70–89
years,mean=79
years.
Gen
der:41%
female.
Med
icalcond
ition
:diverse
chronicillne
sses.
Family
n=19.
Relatio
nshipwith
patient:
husband,
wife,m
othe
r,father,
daug
hter,son
,daugh
ter-in-
law,son
-in-law.
Them
es:
Dealingwith
med
icalconfusion–
-Po
st-discharge
med
icationmanagem
entwas
diffi-
cultbe
causeof
med
icationchange
s.Facilitatorsforrecovery:socialcapitaland
social
supp
ort-
-Family
mem
bersmadesure
that
med
ications
sche
duleswerefollowed
.-Family
was
overwhe
lmed
andexhausteddu
eto
constant
need
tocoordinate
care
anden
sure
patients’ne
edsmet.
Targeted
nursepractitione
rinitiative-
-Somecaregiversdidno
tfully
unde
rstand
the
nursepractitione
r(NP)
rolebu
treliedon
NPs
tooverseethemanagem
entof
med
ications.
Palagyietal.2016[26]
Australia***
Design:Qualitative
exploratory.
Setting:
threelong
-term
care
facilities
Datacollection:Focusgrou
psand
interviews
Transitio
npo
intsinvolved
:lon
g-term
care
facilities,ho
spital,commun
itycare.
Med
icationmanagem
entprocess
involved
:dep
rescrib
ingmed
ications.
Patientsn=25.
Age
:mean=87.6years,rang
e75–100.
Gen
der:77%
female.
Med
icalcond
ition
:not
stated
.Family
n=16.
Relatio
nshipwith
patient:not
men
tione
d.Health
profession
alsn=27.
Disciplines
involved
:gen
eral
practitione
rs,lon
g-term
care
facilitiesstaff.
Them
es:
Pitfallsof
coordinatedcare
--Lack
ofreview
ofacutemed
icationaftercond
ition
was
treated.
Neg
otiatin
gacomplex
system
--Family
concerne
dthat
compu
lsorytw
o-year
resi-
dentialm
edicationmanagem
entreview
sche
dule
was
toolong
.Manychange
soccurin
twoyears.
Med
icationknow
ledg
e-
-Family
wereun
familiar
with
specificmed
ication
indicatio
ns.-
Minim
alrecogn
ition
ofadversedrug
reactio
ns.
WhatevertheGPsays
goes
-
Manias et al. BMC Geriatrics (2019) 19:95 Page 10 of 21
Table
1Characteristicsof
includ
edpape
rsexam
iningfamily
involvem
entformanagingmed
ications
ofolde
rpatientsacross
transitio
nsof
care
(N=23)(Con
tinued)
Autho
r,year,cou
ntry,M
MAT
result
Designandsetting
Descriptio
nof
stud
yParticipants
KeyFind
ings
-Com
pletetrustin
thecare
andde
cision
sof
the
GP.
-Num
berof
specialistsinvolved
inreside
nts’care.
Needforrealistic
expe
ctations-
-Relatives
view
edlong
-term
care
facilitiesas
active
providersof
med
icalcare.G
Psregarded
itas
apal-
liativecare
environm
ent.
Ploe
get
al.2017[31]
Canada***
Design:Interpretive
descrip
tive.
Setting:
participants’hom
e
Datacollection:semi-structured
interviews.
Transitio
npo
intsinvolved
:hom
e,prim
arycare
settings,hospital.
Med
icationmanagem
entprocess
involved
:managingmed
ications
for
multip
lecomorbidities.
Patientsn=41.
Age
:17%
aged
85yearsand
over.
Gen
der:44%
female.
Med
icalcond
ition
:three
ormorechroniccond
ition
s.Family
n=47.
Relatio
nshipwith
patient:
wife,husband
,grand
father,
mothe
r-in-law,friend
s.Health
profession
alsn=42.
Disciplines
involved
:registered
nurse,registered
/licen
sedpracticalnu
rse,
person
alsupp
ortworker/
healthcare
aide
Them
es:
Expe
rienceof
managingmultip
lechronic
cond
ition
s-
-Em
otionally
draining
.Organisingpills
andappo
intm
ents-
-Managingchange
sto
med
ications
that
frequ
ently
occurred
afteran
acutecare
hospitalization.
-Abrup
tdischarge,with
outinpu
tfro
mcaregivers
abou
tpreferen
ces.
-Organisingappo
intm
entsto
discussbloo
dresults
andscansaffectingmed
ications.
Beingsplit
–-Receivingservices
from
multip
leproviderswho
focuson
asing
ledisease
-Lack
ofcommun
icationbe
tweenfamily
doctor
andspecialists.
Doing
whatthedo
ctor
says
--Family
believedde
cision
makingwas
physician-
directed
.Provide
rspe
rceivedtheirapproach
in-
volved
shared
decision
-making.
Pope
joy2011
[32]
United
States***
Design:Qualitative
exploratory.
Setting:
tertiary
care
hospital
Datacollection:semi-structured
interviews.
Transitio
npo
intsinvolved
:hospital,
home,reside
ntialage
dcare
facility.
Med
icationmanagem
entprocess
involved
:Discharge
planning
.
Patientsn=13.
Age
:mean=84
years,rang
e=72–89years.
Gen
der:62%
female.
Med
icalcond
ition
:no
cogn
itive
impairm
ent,at
least
pre-clinicallyfrail.
Family
n=12.
Relatio
nshipwith
patient:
spou
ses.
Health
profession
alsn=7.
Disciplines
involved
:registered
nurses,social
workers.
Them
es:
Chang
ingthedischargeplan
--Patientsandcaregiverswereadam
antabou
tgo
ingho
me(not
toreside
ntialcare).
-Health
profession
alswereworriedwhe
nfamily
hadtrou
bleun
derstand
ingabou
tmed
ications.
-Family
weresometim
esoldwith
health
prob
lems
them
selves,and
haddifficulties
coping
with
and
remem
berin
gto
offerpatients’med
ications
atho
me.
Tjiaet
al.2014[27]
United
States***
Design:qu
alitative
exploratory.
Setting:
Threeho
spice
agen
cies.
Datacollection:semi-structured
interviews
Transitio
npo
intsinvolved
:hospice,
outpatient
oncology,p
rimarycare
settings.
Med
icationmanagem
entprocess
involved
:med
icationprescribing
Patientsn=18.
Age
:mean=80
years(SD10
years).
Gen
der:42%
female.
Med
icalcond
ition
:advanced
cancer.
Family
n=8.
Them
es:
Med
icationcoordinatio
nandcommun
ication-
-Families
werekeen
tohave
compreh
ensive
med
icationreview
sup
ontransitio
nto
hospice
that
assessed
ongo
inguseof
long
standing
med
ications
forcomorbidillne
ss.
-Family
werereceptiveto
redu
cing
harm
fuland
Manias et al. BMC Geriatrics (2019) 19:95 Page 11 of 21

Table
1Characteristicsof
includ
edpape
rsexam
iningfamily
involvem
entformanagingmed
ications
ofolde
rpatientsacross
transitio
nsof
care
(N=23)(Con
tinued)
Autho
r,year,cou
ntry,M
MAT
result
Designandsetting
Descriptio
nof
stud
yParticipants
KeyFind
ings
across
transitio
ns.
Relatio
nshipwith
patient:not
stated
.Health
profession
alsn=17.
Disciplines
involved
:nurses,
physicians.
non-essentialm
edications.
Towleet
al.2012[12]
Sing
apore*
Design:Prospe
ctive
observational,cross-sectional.
Setting:
onetertiary
hospital
Datacollection:survey
questio
nnaire
Transitio
npo
intsinvolved
:hospital,
home.
Med
icationmanagem
entprocess
involved
:Discharge
process.
Interven
tion:(fo
rinterven
tion
stud
ies)BO
OST
(BetterOutcomefor
Older
adultsthroug
hSafe
Transitio
ns);an
eviden
ce-based
qual-
ityim
provem
entinitiativeto
en-
hancecare
transitio
nin
improving
patient/fam
ilyprep
ared
ness
for
discharge.
Patientsn=40.
Age
:not
stated
.Gen
der:no
tstated
.Med
icalcond
ition
:>1
chroniccond
ition
.Family
n=no
tstated
.Relatio
nshipwith
patient:not
stated
.
Outcomes:
Patient
andcaregiverun
derstand
ingof
med
ical
cond
ition
--Im
provem
entby
70%.
Patient
andcaregiverun
derstand
ingof
med
ications-
-Im
provem
entby
67%.
Patient
andcaregiverun
derstand
ingof
treatm
ent
plan
--Im
provem
entby
81%.Patient
andcaregiver
unde
rstand
ingof
follow-up-
-Im
provem
entby
41%.
Trollor1997
[28]
Australia****
Design:Cross-sectio
nal.
Setting:
Com
mun
itypalliative
care
service.
Datacollection:qu
estio
nnaire.
Transitio
npo
intsinvolved
:palliative
care
services,hom
e,prim
arycare
services.
Med
icationmanagem
entprocess
involved
:sym
ptom
managem
ent.
Patientsn=26.
Age
:not
stated
.Gen
der:31%
female.
Med
icalcond
ition
:patients
with
palliativecare
need
s.Family
n=26.
Relatio
nshipwith
patient:
wives,d
augh
ters,husband
s.
Them
es:
-13
outof
26family
mem
berswerein
charge
ofpatients’med
ication.
-Ro
lein
dealingwith
gene
ralp
ractition
ersand
palliativecare
specialists,toadministermed
ication
forpain,sleep
ingdifficulty
andloss
ofappe
tite
weremostchalleng
ing.
White
etal.2015[29]
United
States***
Design:Qualitative
exploratory.
Setting:
Twoho
spitals.
Datacollection:semi-structured
interviews.
Transitio
npo
intsinvolved
:hospital,
home.
Med
icationmanagem
entprocess
involved
:Discharge
planning
.
Patientsn=20.
Age
:mean=77
years(SD8.8
years).
Gen
der:47%
female.
Med
icalcond
ition
:stroke
survivors.
Family
n=9.
Relatio
nshipwith
patient:
husband,
wife,son
,daugh
ter.
Them
es:
Prep
aringto
goho
meafterthestroke
--Im
portance
ofhe
alth
profession
alsun
derstand
ing
family’sne
edsfollowingdischargeso
that
specific
situationcouldbe
addressed.
-Wrong
family
mem
bertargeted
forproviding
inform
ation.
Com
plexity
ofmed
icationmanagem
ent-
-somefamily
wereconfiden
tabou
ttheir
know
ledg
e.-Somefamily
lacked
unde
rstand
ingabou
tthe
purposeof
med
ication.
-Usuallyfamily
mem
berwho
managed
med
ications.
-Difficultiesin
managingmed
ications
forpatients
with
swallowingprob
lems.Rand
omde
cision
sabou
twhich
med
ications
shou
ldbe
crushe
d.
Manias et al. BMC Geriatrics (2019) 19:95 Page 12 of 21

Table
1Characteristicsof
includ
edpape
rsexam
iningfamily
involvem
entformanagingmed
ications
ofolde
rpatientsacross
transitio
nsof
care
(N=23)(Con
tinued)
Autho
r,year,cou
ntry,M
MAT
result
Designandsetting
Descriptio
nof
stud
yParticipants
KeyFind
ings
White
etal.2014[33]
United
States**
Design:Mixed
metho
ds.
Setting:
Twoho
spitals.
Datacollection:semi-structuredin-
terviews,electron
icmed
icalrecord
review
.Transitio
npo
intsinvolved
:hospital,
home.
Med
icationmanagem
entprocess
involved
:Discharge
planning
.
Patientsn=310.
Age
:mean=76
years(SD9.8
years).
Gen
der:Not
stated
.Med
icalcond
ition
:stroke
survivors.
Family
n=20
combine
dwith
patients.
Relatio
nshipwith
patient:not
stated
.
Them
es:
With
inon
emon
thof
discharge,10%
were
readmitted
and25%
with
in6mon
ths.
Reason
sforreadmission
wererecurren
tstroke/
transien
tischaemicattack
(19%
),pn
eumon
iaand
urinarytractinfection(19%
),sw
allowingprob
lems
andde
hydration(9%),andcardiaccauses
(7%).
-Needforgu
idance
onwhatto
expe
ctat
home.
-Needfollow-upin
commun
ityabou
tearly
iden
tifi-
catio
nof
prob
lems.
-Com
plexity
ofmed
icationmanagem
ent
sometim
esledto
lack
ofun
derstand
ing.
Note:
Thesymbo
ls*,**,***
and****
referto
scores
of25
,50,
75an
d10
0%respectiv
elyob
tained
ontheMixed
Metho
dsApp
raisal
Tool
(MMAT)
Manias et al. BMC Geriatrics (2019) 19:95 Page 13 of 21

Table
2Synthe
sisedthem
esfro
minclud
edstud
ies
Them
esandsubthe
mes
Stud
ieswith
thefirstnamed
author
andyear
Allen
2017
Colem
an.
2006
Colem
an2004
Crawford
2015
Deeks.
2016
Dyrstad
2015
Geo
rgiadis
2017
Haged
oorn
2017
Hvalvik
2015
Jeffs
2017
King
2013
Knight
2013
Givinginform
ationandreceivingfeed
back
Families
conveyinginform
ationto
health
profession
als
XX
XX
XX
X
Health
profession
alsinform
ingfamilies
XX
XX
XX
XX
XX
X
Participatingin
decision
making
Med
icationde
cision
soccurringon
admission
X
Med
icationde
cision
soccurringtransfersanddischarge
XX
XX
XX
XX
Med
icationde
cision
soccurringafterdischarge
XX
X
Characteristicsof
health
profession
alsandfamilies
XX
Managingmed
icationcomplexity
across
transitio
nsof
care
Challeng
esin
managingmed
icationcomplexity
from
hospitaladm
ission
todischarge
X
Difficultiesaffectingmed
icationcomplexity
inthe
commun
ityandaged
care
facilities
XX
XX
X
Possibilitiesforindividu
alised
tailoredcare
XX
Supp
ortin
gfamily
participationin
interven
tions
XX
Manias et al. BMC Geriatrics (2019) 19:95 Page 14 of 21

Them
esandsubthe
mes
Stud
ieswith
thefirstnamed
author
andyear
Lowson
2012
Nazarath
2001
Neiterm
an2015
Palagyi
2016
Ploe
g2017
Pope
joy
2011
Tjia
2014
Towle
2012
Trollor
1997
White
2015
White
2014
Givinginform
ationandreceivingfeed
back
Families
conveyinginform
ationto
health
profession
als
XX
XX
X
Health
profession
alsinform
ingfamilies
XX
XX
Participatingin
decision
making
Med
icationde
cision
soccurringon
admission
Med
icationde
cision
soccurringtransfersanddischarge
XX
Med
icationde
cision
soccurringafterdischarge
XX
X
Characteristicsof
health
profession
alsandfamilies
XX
X
Managingmed
icationcomplexity
across
transitio
nsof
care
Challeng
esin
managingmed
icationcomplexity
from
hospital
admission
todischarge
XX
Difficultiesaffectingmed
icationcomplexity
inthecommun
ityand
aged
care
facilities
XX
XX
XX
X
Possibilitiesforindividu
alised
tailoredcare
XX
Supp
ortin
gfamily
participationin
interven
tions
XX
Manias et al. BMC Geriatrics (2019) 19:95 Page 15 of 21

medications across transitions of care. Fourteen studiesexamined this theme [13, 16–21, 23–26, 30–32]. Foursubthemes underpinned this theme: medication decisionsoccurring on admission to hospital, those occurringduring transfers and at discharge, those that happenedafter discharge home and to aged care facilities, and char-acteristics of health professionals and family members infostering participation in decision making.In one participant observation study in emergency
departments, family members made decisions aboutadministering medications [18]. They determined thespecific times to give medications to patients. This oc-curred at busy times while patients waited to be trans-ferred to other settings. An example included a daughterproviding anti-epileptic medications to her motherbecause of understaffing and heavy nursing workloads inthe emergency department [18].Many challenges impeded family participation in deci-
sion making during transfers and at discharge. Unex-pected or delayed transfers and discharges due to staffconstraints of doctors, nurses and pharmacists resulting ininsufficient time and planning, led to limited opportunitiesfor families to participate in medication decisions [19, 20,24, 25, 31]. Family members believed that some healthprofessionals, such as community nurses or specialists fo-cused on treating a single condition, that health profes-sionals did not listen to them, and that healthprofessionals organised discharge medications without un-derstanding about patients’ concerns and the home situ-ation that could impact on their treatment regimen [13,16, 31]. There was lack of family participation in medica-tion decisions in diverse communication encounters, in-cluding informal bedside conversations, ward rounds, anddischarge consultations [17–19]. The absence of struc-tured routines for family communication meant that fam-ily members were not present at times when goals of carewere discussed [18]. For example, family members com-plained about nurses contacting them by phone to informthem about medication decisions on the day of discharge,with these decisions having been made much earlier dur-ing the patients’ hospital stay. Family members preferredthat doctors and nurses had a routine of contacting themabout participating on the doctors’ rounds relating toplanning for discharge. [18].Planning activities for patient transfer or discharge
often lacked an individualised approach, as shown by theabsence of dedicated sessions to discuss goals of treat-ment [17, 19]. Some assertive family members ques-tioned nurses about how patients would use medicationsto deal with worsening symptoms, such as difficulties inbreathing or increasing confusion [20], and the effects ofchanged medications at the time of discharge [17].Nevertheless, opportunities for their involvement tendedto be more apparent if nurses organised specific family
meetings where family members could ask questions[20]. In patients with dementia who had changingdemands for managing behavioural and psychologicalsymptoms, transitioning between various environmentswas common [16]. Their families believed that theyplayed a vital role in making decisions at home; however,their roles blurred and shifted between being an activecaregiver and a passive bystander as patients transferredfrom home, to acute care, rehabilitation and geriatricevaluation and management units, and back to home[16]. Family member sought to be called by healthprofessionals to enable pre-planning to organise a timeto discuss about medications.Lack of involvement during transitions contributed to
safety concerns about medications [19, 20, 24, 25, 31]. Fam-ilies were given little time to plan for assisting with medica-tion administration at home [20] and they were confusedabout the changes made, which meant they did not knowwhat to do when patients went home [24, 25, 31]. Familymembers commented that they did not feel involved indecisions because they received inadequate explanations formedication changes [24, 31]. Family members’ lack of par-ticipation sometimes led to increased risk, such asprescribing medications for patients where allergies existedand were not clarified [31].Following discharge, family members participated in
decisions by assisting with, and monitoring medication in-take for, patients at home. In examining patients’ medica-tion regimens, community nurses rarely discussed thepatients’ home situation [20]. At home, family membersperceived themselves as advocating for patients’ needs, bychanging medication times to suit patients’ individualisedroutines [22], and by reminding health professionals aboutthe medication schedules followed at home [25]. Forpatients discharged home after receiving palliative careservices, 13 out of 26 family members indicated that theytook charge of patients’ medications at home, to managesymptoms such as pain, sleeping difficulty and loss of ap-petite [28]. Conversely, for residents situated in long-termcare facilities, care workers tended to exclude familymembers from decision making. In these environments,some family members experienced difficulties in relin-quishing their carer role and wanted to retain their role indecisions [16]. Family members of patients discharged toaged care facilities were frustrated about their lack of in-clusion in decisions made at the acute care hospitals fromwhere the patients were transferred. They observed agedcare nurses making multiple requests to the acute carehospitals, seeking clarification of unclear discharge ordersfor patients discharged to aged care services [23]. Further-more, family members felt uncomfortable in questioninggeneral practitioners about the medication plans theyprepared for individuals situated in residential aged carefacilities [26].
Manias et al. BMC Geriatrics (2019) 19:95 Page 16 of 21

Interpersonal characteristics of health professionalsand family members affected how and whether deci-sion making took place. Family members commentedthat if nurses and doctors exuded a positive attitudeand explained their role, this approach facilitated fam-ily participation [13]. Some health professionals wereperceived to lack empathy, with an inability to ac-tively listen to family concerns about medications.Pharmacists and doctors believed it was their role toconsider the complexities of managing older patients’multiple medications. However, these health profes-sionals felt challenged in addressing the risk-benefitconcerns in following individual guidelines and tryingto tailor medication regimens for older patients withseveral health conditions [31]. Family members oftenfelt a sense of responsibility for managing patients’medications [21]. Patients delegated this responsibilityto family members because they did not want to beperceived as bothersome and complaining to clinicalstaff [30]. Health professionals sometimes changedtheir belief that family members would be able tocope with managing patients’ medications when theysought information from family members [32].
Managing medication complexity across transitions ofcareThere were 14 studies that focused on managing medi-cation complexity across transitions of care [13, 17, 19,21–26, 29–33]. Medication complexity referred to rap-idly changing dose and frequency orders, medicationsprescribed to treat several co-existing conditions, andcomplicated administration and storage requirements.Three subthemes related to this theme: challenges inmanaging medication complexity from hospital admis-sion to discharge, difficulties affecting medication com-plexity in the community and aged care facilities, andpossibilities for individualised tailored care for managingmedications.In managing medication complexity from hospital ad-
mission to discharge, families experienced difficulties inunderstanding how the health system operated in hospi-tals [21], while at the same time, they felt responsible forsupporting patients’ complex needs. Families describedplaying a “second fiddle” role (p. 1197) during hospital ad-mission of patients living with heart failure or lung cancerin their final year of life, where families felt subordinate todoctors and the hospital system [30]. Families consideredthat health professionals perceived them as outsiders, andthey had to be assertive to have their views heard [22].Hospital discharge meetings were organised in an
attempt to help patients and families to understand pa-tients’ complex treatment regimens [13, 19, 22]. However,families perceived that discharge activities were not tai-lored to patients’ complex needs. Quick discharge
processes were organised for patients with multiplechronic conditions [31] and planning was not modified totake account of patients with cognitive problems [17].Family members also had a poor first impression of
skilled nursing facilities (a form of aged care facility inthe United States), when health providers asked themabout medications prescribed after patients’ transferfrom hospital to these facilities. Instead, family mem-bers believed that health professionals in hospitalsshould provide clarification about these prescriptions atthe point of transfer [23]. In this particular circum-stance, family members felt it was wrong that they wereexpected to provide this clarification.Several studies reported difficulties in administering
complex medication regimens in the community andaged care facilities [17, 21, 25, 32]. For pharmacists offer-ing dose administration aids to patients at discharge,there was often insufficient screening to determine theappropriateness of using these aids at home. Olderpatients needed to have a reasonable degree of cognitionin order to work out the timing of doses, and to pushout medications from the aids [17]. Interviews withnurses working in a skilled nursing facility identifiedpoor communication and inappropriate medicationplans as patients moved from the hospital to the facility.Nurses believed that health professionals in hospitals didnot utilise families effectively to obtain informationduring transfers. Complicated medication changes at dis-charge created disruptions to daily routines at home forpatients and families [25] and since families were unableto understand the rationale for some changes, they didnot remember to remind patients about when to con-sume these medications [32]. Families preferred patientsto have once-daily doses of medications, especially forthose patients with multiple medications as paid carersoften only visited patients once a day. However, thispreference was not usually considered by prescribers[17]. Families also found themselves frequently remind-ing home nurses about medication orders that thesenurses should have stopped due to a patient’s history ofallergies or adverse events because of medications lead-ing to vomiting and confusion [21].For patients needing home palliative care services,
families were challenged in dealing with unresolvedsymptoms of pain, sleeplessness and loss of appetite,along with the diagnosis of cancer. As these patients’symptoms worsened, constant changes had to be madeto medication orders, thereby adding difficulties forfamilies [28]. Similarly, families wanted patients to havea compulsory medication review by hospice nurses inhospice environments to assess ongoing need for medi-cations used for long-standing conditions. However,hospice nurses perceived doctors were reluctant to dis-continue medications in these patients, and that these
Manias et al. BMC Geriatrics (2019) 19:95 Page 17 of 21

doctors lacked confidence in making medication assess-ments [27]. Furthermore, for older people moving intoAustralian residential aged care facilities, familiesbelieved that 2 years was too long to wait for a plannedformal medication review [26]. There was also concernabout acute conditions being treated for months afterconditions had subsided, including antihistamines andantibiotics [26]. At the same time, families were uncer-tain about what medications that doctors should pre-scribe following a patient’s stroke compared to whatthey prescribed prior to a stroke, and when patients hadmultiple comorbidities, such as hypertension andParkinson’s disease [29, 33]. Families also had to contendwith multiple prescribers who managed patients’ condi-tions [17, 31]. Prescribers often focused on single diseasestates and therefore did not always consider the effectsof their prescriptions on other chronic conditions ormedications being taken [21].Medication changes created the challenge of new
side-effects requiring additional monitoring, which weresometimes not adequately conveyed to family members[31]. For example, in the study by White et al. [29]involving patients following a stroke with impaired swal-lowing, families did not receive clear information fromdoctors about which medications could be crushed.Several studies considered possibilities for individua-
lised tailored care, which was more likely when healthprofessionals delayed patient discharge to provide moretime for coordinating medication regimens [19, 21, 30,31]. Proactive approaches used between family members,such as maintaining regular contact with each other,enabled continuity of care for patients with heart failureor cancer in the last year of life [30]. Such approachesenabled greater family understanding of how medicationchanges occurred as patients’ condition altered [21, 31].However, there was little focus of how patients’ demo-graphic characteristics such as those from disadvantagedor vulnerable backgrounds could affect tailored care formanaging medication regimens.
Supporting family participation in interventionsFour studies focused on supporting family participation,together with that of patients, in interventions aimed atimproving patients’ experiences at transitions of care[12, 14, 15, 34]. In two papers by Coleman and col-leagues [14, 15], an intervention was delivered by anadvanced practice nurse to patients and families thatincluded medication self-management, a patient-centredrecord, primary care and specialist follow-up, and know-ledge of warning signs or symptoms that indicated aworsening condition. This intervention was designed toenhance patient and family self-management skillsacross transitions of care. To provide support with medi-cation self-management, the advanced practice nurse
reviewed each medication with the patient, as well as thefamily member if available, to ensure that the patientunderstood its purpose, instructions, and potential ad-verse effects. Aside from identifying that family memberswere involved as recipients of the intervention, nodetails were provided of how they perceived these inter-ventions, how they were specifically involved as a separ-ate or collaborative entity to patients, and how theirinvolvement influenced outcomes. In both studies, therewere significant reductions in rehospitalisation rates andcosts after discharge from the initial hospitalisation (p <0.05). No outcomes relating to medication errors werereported.In the intervention study by Nazarath et al. [34], dis-
charge plans were developed by hospital pharmacists,home visits occurred with community pharmacists, andcounselling took place with patients and family onappropriate doses and purpose of medications. No differ-ences were found between control and interventiongroups in terms of readmission at 3 months and 6months, or in patients’ well-being, satisfaction with theservice, and knowledge of and adherence to prescribedmedications (p > 0.05). There was no specific investiga-tion of how family involvement may have influenced theclinical outcomes.In Towle et al.’s [12] prospective observational study,
the focus was on evaluating the effectiveness of BOOST(Better Outcome for Older adults through Safe Transi-tions) in improving transition from hospital to home.After delivery of the intervention, comprising a bundleof evidence-based tools on discharge processes, the au-thors reported patients’ and families’ improved under-standings of medications by 67%, of the treatment planby 81%, and follow-up by 41%. No details were providedof the families’ specific contributions in achieving theseoutcomes.
DiscussionFour major themes were identified in this systematicreview: information giving and receiving, participation indecision making, managing medication complexity, andfamily participation in supportive interventions. In thestudies identified, families’ involvement in medicationmanagement tended to be subsumed in various aspectsof patients’ care. It was therefore sometimes difficult toidentify discrete details about the family perspective onmedication management.Information giving was a key area of family involve-
ment, which tended to occur in restricted ways. Healthprofessionals acknowledged family members as keysources of information about the medications that olderpeople were prescribed. However, the process of elicitinginformation from family members largely focused on pa-tient admission to hospital [18, 20]. There was also some
Manias et al. BMC Geriatrics (2019) 19:95 Page 18 of 21

indication of information seeking from family membersfor older patients with dementia who moved from acutecare settings to long term care [16] and of older patientsat their last year of life from hospital to home [30]. Noevidence was found with regard to information seekingfrom family members as older patients moved betweenvarious settings within hospitals. As health professionalsmainly sought information from families on patient ad-mission, this creates the possibility of medication dis-crepancies at future transitions of care. Informationgiving needs to occur in diverse environments, includingwhen older patients move to home or to residential agedcare facilities.Receiving information by family members from health
professionals was a relatively disorganised and haphaz-ard process [17–19]. There was little evidence of familiesreceiving information from health professionals if olderpatients moved between different acute care settingswithin hospitals, or when movements occurred fromacute care to subacute care or long-term care settings.Information receipt that focused on the time of dis-charge from hospital to home, sometimes created amanagement burden as health professionals attemptedto provide medication counselling and education at asingle time point. Medication errors were therefore apossibility following discharge. Rather than focusing in-formation receiving at discharge, it may be more effect-ive if this activity occurs throughout the patients’hospital stay. Similarly, efforts in information giving andreceiving could be reorganised such that different ap-proaches are available to deal with differing levels of pa-tient and family understanding.Participation in decision making demonstrated that
families communicated with patients about strategies touse when taking medications as they moved from oneenvironment to another. In some environments wherehealth professionals were affected by time constraints,understaffing, and heavy workloads, there was some-times little opportunity for health professionals to attendto older patients’ medication needs [18]. In these situa-tions, families were recipients rather than active partici-pants of decisions [35]. Greater attention should beplaced on enabling shared decision making duringplanned communication encounters including familymeetings, bedside handovers, ward rounds, and admis-sion and discharge consultations.In managing medication complexity across transitions
of care, family members perceived a lack of tailoring ofmedication plans for patients’ needs, and believed theyhad to display perseverance to have their views heard. Instudies that dealt with medication complexity, there wasinsufficient demographic information to indicate whetherfamilies had disadvantaged or vulnerable circumstances,such as being of non-English speaking backgrounds, low
socioeconomic groups, or low health literacy. Improvingunderstanding about medication complexity at transitionsof care requires fundamental changes in the way thathealth professionals and families interact with each other.Some past work has focused on the use of patientteach-back to address misinterpretations about the medi-cation regimen [36, 37]. As an extension of that process,family teach-back could be an effective means of identify-ing key information whereby family members use theirown words to explain to health professionals what theyknow about patients’ medications. Individuals can thencollectively verify understandings, address misconceptionsand improve family and health professional comprehen-sion [38].Four interventions were identified as being directed to
patients and families; however, the specific contributionof families was not clearly distinguished [12, 14, 15, 34].Improvements in family understanding about medica-tions were identified in one intervention study [12] whilein another, no improvements were found in medicationknowledge or understanding [34]. The remaining twostudies had no information about medication manage-ment outcomes [14, 15]. While families were named asrecipients of interventions, there was insufficient clarityabout the extent of their involvement, and of how theirinvolvement affected outcomes achieved. No detailswere provided about compliance with interventions, ordifficulties encountered with family involvement. To ad-dress gaps in past work, targeted strategies need to focusmore specifically on family members’ active contributionto managing medications at transitions of care, with out-comes directed on family understanding of medicationchanges and their input in preventing and identifyingmedication-related problems.There are limitations associated with the systematic
review. Since the review only included papers publishedin English, it is possible that those published in otherlanguages may have provided further insights on thetopic. As most papers did not specifically focus on theobjective of this systematic review, it was sometimes dif-ficult to extract the required information. There was alsono attempt to exclude papers on the basis of quality.There were a number of methodological issues relating
to the included studies. In terms of strengths, of thestudies included in the review, 65% had obtained aMMAT score of 75%, thereby indicating the majority ofthe studies were relatively well-conducted. Interviewstudies showed that the data were rich, comprehensive,and revealed clear insights into the contextual challengesaffecting older patients across transitions of care. In rela-tion to methodological limitations, transitions of caretended to be examined at only particular time points,namely, movements of patients during admission to ordischarge from hospital. Given that the focus of the work
Manias et al. BMC Geriatrics (2019) 19:95 Page 19 of 21

involves family involvement, it is interesting that only twostudies comprised qualitative observational designs.The systematic review indicates the need for further re-
search. Future studies should focus on examining families’contribution and involvement in managing older patients’medications across transitions of care. Most past workgenerally only addressed family involvement in general as-pects of patient movement across transitions of care.Greater consideration needs to be given to family involve-ment in the continuum of patient journey at differentcontexts of care, from admission to hospital, through totransfers across wards and across hospitals, and dischargehome or to residential aged care facilities.
ConclusionsFamilies play an important role in supporting older pa-tients in managing their medications as these patientsmove across different settings. Nevertheless, there is lackof acknowledgement from health professionals of the activ-ities performed by families before, during and followingthese movements. While families actively engage witholder patients in strategies to ensure medication safety, fur-ther work is needed on measuring the effectiveness onthese strategies on medication outcomes, facilitatingshared decision making between families and healthprofessionals, and clarifying medication plans of careacross transitions.
Additional file
Additional file 1: Search History/Alerts Medline (Ebscohost) [9]. Searchhistory for Medline. (DOCX 54 kb)
AbbreviationsBOOST: Better Outcome for Older adults through Safe Transitions;CENTRAL: Cochrane Central Register of Controlled Trials; CINAHL: CumulativeIndex to Nursing and Allied Health Literature; Ebscohost: Elton B. StephensCo Host; EMBASE: Excerpta Medica Database; MEDLINE: Medical LiteratureAnalysis and Retrieval System Online; MMAT: Mixed Methods Appraisal Tool;PICo: population, phenomenon of interest and context;PsycINFO: Psychological Information Database
AcknowledgementsNot applicable.
FundingAustralian Research Council, Discovery Grant Scheme, DP170100308. The fundingbody had no role the design of the systematic review and collection of papers,analysis and interpretation of papers, and in writing the manuscript.
Availability of data and materialsDatabase search strategies available as a supplementary file.
Authors’ contributionsAll authors: conception and design; EM, TB: provision of study materials; EM, TB:collection and assembly of data; All authors: data analysis and interpretation; Allauthors: manuscript writing and editing; All authors: final approval ofmanuscript.
Ethics approval and consent to participateNot applicable.
Consent for publicationNot applicable.
Competing interestsThe authors declare that they have no competing interests.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims in publishedmaps and institutional affiliations.
Author details1Centre for Quality and Patient Safety Research, School of Nursing andMidwifery, Deakin University, 221 Burwood Highway, Burwood, VIC 3125,Australia. 2Alfred Health, Commercial Road, Prahran, VIC 3181, Australia.3School of Pharmacy, Queen’s University Belfast, University Road, Belfast,Northern Ireland BT7 1NN, UK. 4Sydney Medical School, The University ofSydney, Edward Ford Building A27, Fisher Road, Camperdown, NSW 2050,Australia. 5NSW Regional Health Partners, 72 Watt St, Newcastle, NSW 2300,Australia. 6School of Medicine, The University of Melbourne, Grattan Street,Parkville, VIC 3052, Australia.
Received: 1 November 2018 Accepted: 8 March 2019
References1. Coleman EA. Falling through the cracks: challenges and opportunities for
improving transitional care for persons with continuous complex careneeds. J Am Geriatr Soc. 2003;51(4):549–55.
2. World Health Organization. Transitions of care: technical series on saferprimary care. Geneva: World Health Organization; 2016.
3. Callen J, Alderton M, McIntosh J. Evaluation of electronic dischargesummaries: a comparison of documentation in electronic and handwrittendischarge summaries. Int J Med Inform. 2008;77(9):613–20.
4. Elliott RA, Tran T, Taylor SE, Harvey PA, Belfrage MK, Jennings RJ, Marriott JL.Gaps in continuity of medication management during the transition fromhospital to residential care: an observational study (MedGap study).Australas J Ageing. 2012;31(4):247–54.
5. Manias E. Communication relating to family members’ involvement andunderstandings about patients’ medication management in hospital. HealthExpect. 2015;18(5):850–66.
6. Disdier Moulder MP, Larock JM, Garofoli A, Foley DA. Family help withmedication management: a predictive marker for early readmission. MayoClin Proc. 2017;1(3):211–8.
7. The Joanna Briggs Institute. Joanna Briggs institute reviewers’ manual: 2014edition. Adelaide: The Joanna Briggs Institute; 2014.
8. Siddaway AP, Wood AM, Hedges LV. How to do a systematic review: a bestpractice guide for conducting and reporting narrative reviews, meta-analyses, and meta-syntheses. Ann Rev Psychol. 2019;70:747–70.
9. Gallagher PE, Allen TY, Wyer PC. How to find evidence when you need it,part 2: a clinician's guide to MEDLINE: the basics. Annals Emerg Med. 2002;39(4):436–40.
10. Pace R, Pluye P, Bartlett G, Macaulay AC, Salsberg J, Jagosh J, Seller R.Testing the reliability and efficiency of the pilot mixed methodsappraisal tool (MMAT) for systematic mixed studies review. Int J NursStud. 2012;49(1):47–53.
11. Cochrane consumers and communication review group: data synthesis andanalysis [cccrg.cochrane.org/sites/cccrg.cochrane.org].
12. Towle RM, Kheng JH, Lee KH, Low LL, Tan SY. Evaluation of theeffectiveness of boost-a programme to improve the transition process fromhospital to home. Proc Singapore Healthcare. 2012;21:S359.
13. Allen J, Hutchinson AM, Brown R, Livingston PM. User experience and carefor older people transitioning from hospital to home: patients’ and carers’perspectives. Health Expect. 2017. https://doi.org/10.1111/hex.12646.
14. Coleman EA, Smith JD, Frank JC, Min SJ, Parry C, Kramer AM. Preparingpatients and caregivers to participate in care delivered across settings: thecare transitions intervention. J Am Geriatr Soc. 2004;52(11):1817–25.
15. Coleman EA, Parry C, Chalmers S, Min SJ. The care transitionsintervention: results of a randomized controlled trial. Arch Intern Med.2006;166(17):1822–8.
Manias et al. BMC Geriatrics (2019) 19:95 Page 20 of 21

16. Crawford K, Digby R, Bloomer M, Tan H, Williams A. Transitioning fromcaregiver to visitor in a long-term care facility: the experience of caregiversof people with dementia. Aging Ment Health. 2015;19(8):739–46.
17. Deeks LS, Cooper GM, Draper B, Kurrle S, Gibson DM. Dementia, medicationand transitions of care. Res Soc Admin Pharm. 2016;12(3):450–60.
18. Dyrstad DN, Laugaland KA, Storm M. An observational study of olderpatients’ participation in hospital admission and discharge – exploringpatient and next of kin perspectives. J Clin Nurs. 2015;24(11–12):1693–706.
19. Georgiadis A, Corrigan O. The experience of transitional care for non-medically complex older adults and their family caregivers. Global QualNurs Res. 2017;4:1–9.
20. Hagedoorn EI, Paans W, Jaarsma T, Keers JC, van der Schans C, Luttik ML.Aspects of family caregiving as addressed in planned discussions betweennurses, patients with chronic diseases and family caregivers: a qualitativecontent analysis. BMC Nurs. 2017;16:37.
21. Hvalvik S, Reierson IÅ. Striving to maintain a dignified life for the patient intransition: next of kin’s experiences during the transition process of an olderperson in transition from hospital to home. Int J Qual Stud Health Well-being. 2015;10. https://doi.org/10.3402/qhw.v10.26554.
22. Jeffs L, Kitto S, Merkley J, Lyons RF, Bell CM. Safety threats and opportunitiesto improve interfacility care transitions: insights from patients and familymembers. Patient Pref Adher. 2012;6:711–8.
23. King BJ, Gilmore-Bykovskyi AL, Roiland RA, Polnaszek BE, Bowers BJ, Kind AJH. Theconsequences of poor communication during transitions from hospital to skillednursing facility: a qualitative study. J Am Geriatr Soc. 2013;61(7):1095–102.
24. Knight DA, Thompson D, Mathie E, Dickinson A. ‘Seamless care? Just a listwould have helped!’ older people and their carer's experiences of supportwith medication on discharge home from hospital. Health Expect. 2013;16(3):277–91.
25. Neiterman E, Wodchis WP, Bourgeault IL. Experiences of older adults intransition from hospital to community. Can J Aging. 2015;34(1):90–9.
26. Palagyi A, Keay L, Harper J, Potter J, Lindley RI. Barricades and brickwalls – aqualitative study exploring perceptions of medication use anddeprescribing in long-term care. BMC Geriatr. 2016;16:15.
27. Tjia J, Gallagher J, Han P, Cutrona SL, Mazor K. Patient-centered prescribingof medications for comorbid illness in older adults with advanced cancer: aqualitative study. J Clin Oncol. 2014;32(31):122.
28. Trollor J. A survey of carers in the North West Health District of New SouthWales. Aust Social Work. 1997;50(1):51–5.
29. White CL, Brady TL, Saucedo LL, Motz D, Sharp J, Birnbaum LA. Towards abetter understanding of readmissions after stroke: partnering with strokesurvivors and caregivers. J Clin Nurs. 2015;24(7–8):1091–100.
30. Lowson E, Hanratty B, Holmes L, Addington-Hall J, Grande G, Payne S,Seymour J. From 'conductor' to ‘second fiddle’: older adult care recipients’perspectives on transitions in family caring at hospital admission. Int J NursStud. 2013;50(9):1197–205.
31. Ploeg J, Matthew-Maich N, Fraser K, Dufour S, McAiney C, Kaasalainen S,Markle-Reid M, Upshur R, Cleghorn L, Emili A. Managing multiple chronicconditions in the community: a Canadian qualitative study of theexperiences of older adults, family caregivers and healthcare providers. BMCGeriatr. 2017;17:40.
32. Popejoy LL. Complexity of family caregiving and discharge planning. J FamNurs. 2011;17(1):61–81.
33. White CL, Brady TL, Saucedo LL, Motz D, Sharp JA, Birnbaum LA. A betterunderstanding of readmission after stroke by including stroke survivor andcaregiver perspectives. Stroke. 2014;45(Issue Supplement 1):NS15.
34. Nazareth I, Burton A, Shulman S, Smith P, Haines A, Timberal H. A pharmacydischarge plan for hospitalized elderly patients--a randomized controlledtrial. Age Ageing. 2001;30(1):33–40.
35. Hoffmann T, Légaré F, Simmons M, McNamara K, McCaffery K, Trevena L,Hudson B, Glasziou P, Del Mar C. Shared decision making: what do cliniciansneed to know and why should they bother? MJA. 2014;201(1):35–9.
36. Negarandeh R, Mahmoodi H, Noktehdan H, Heshmat R, Shakibazadeh E.Teach back and pictorial image educational strategies on knowledge aboutdiabetes and medication/dietary adherence among low health literatepatients with type 2 diabetes. Prim Care Diabetes. 2013;7(2):111–8.
37. Dennis Emralino D. A critical review of the effectiveness of ‘teach-back’technique in teaching COPD patients self-management using respiratoryinhalers. Health Educ J. 2013;73(1):41–50.
38. Tamura-Lis W. Teach-Back for quality education and patient safety. UrolNurs. 2013;33(6):267–71 98.
Manias et al. BMC Geriatrics (2019) 19:95 Page 21 of 21