factors influencing blood pressure and heart rate...
TRANSCRIPT

Factors Influencing Blood Pressure and HeartRate Variability in Hypertensive Humans
JOHN S. FLORAS, M. OSMAN HASSAN, JOHN VANN JONES, BARBARA A. OSIKOWSKA,
PETER S. SEVER, AND PETER SLEIGHT
SUMMARY We examined the influence of baroreceptor reflex sensitivity (the increase in pulseinterval in response to a phenylephrine-induced increase in blood pressure), age, blood pressure, and/3-adrenergic receptor blockade on the variability of blood pressure and heart rate in essentialhypertension. Fifty-six subjects were studied before treatment; intra-arterial blood pressure wasrecorded outside the hospital for 24 hours. Variability was defined (from all beats occurring whilesubjects were awake) as the standard deviation about the average waking value for mean arterialpressure (MAP) or pulse interval. The correlation (r) between baroreceptor reflex sensitivity andblood pressure variability was -0.47 (p<0.0002). Baroreceptor reflex sensitivity was the onlyindependent determinant of blood pressure variability on multiple regression analysis. Thirty subjectswere restudied after 5 months of /3-adrenergic receptor blockade. Ambulatory blood pressure waslower during treatment, whereas pulse interval, its variability, and baroreceptor reflex sensitivitywere higher. Blood pressure variability was unchanged. The variability of MAP was inversely corre-lated with baroreceptor reflex sensitivity before (r = -0.42, p<0.02) and during ( r= -0 .45 ,p < 0.02) treatment, but it was unrelated to the average ambulatory MAP or to the variability of pulseinterval either before or during /3-blockade. Sixteen subjects whose average waking ambulatory bloodpressure was 140/90 mm Hg or less were not treated. This group of borderline hypertensive subjectshad less variable MAP than did the remaining 40 subjects (12.4 ± 2.3 [SD] vs 14.5 ± 2.5 mm Hg;p<0.01). We conclude that 1) the decline in baroreceptor reflex sensitivity is the principal determi-nant of increased blood pressure variability in hypertension, 2) MAP and its variability are regulatedindependently, 3) heart rate variability is not influenced by baroreceptor reflex sensitivity and isunrelated to blood pressure variability, and 4) the blood pressure of subjects with borderline hyper-tension is not excessively labile. (Hypertension 11: 273-281, 1988)
KEY WORDS • ambulatory blood pressure • baroreceptor reflex sensitivity • /3-adrenergicreceptor blockade • borderline hypertension • labile hypertension • age
INTRA-ARTERIAL ambulatory blood pressurerecordings demonstrate graphically the greatbeat-to-beat variability of blood pressure present
From the Department of Cardiovascular Medicine, University ofOxford, John Radclifife Hospital, Headington, Oxford, and the De-partment of Clinical Pharmacology, St. Mary's Hospital, NorfolkPlace, London, United Kingdom.
Supported in part by a grant from the British Heart Foundation.Dr. Floras was supported by a Rhodes Scholarship and currentlyholds a Career Scientist Award from the Ministry of Health of theProvince of Ontario. Dr. Hassan was in receipt of a ResearchFellowship from the Medical Research Council (UK).
Dr. Hassan's present address: Department of Medicine, KingAbdul Aziz University Hospital, Jeddah, Kingdom of Saudi Ara-bia. Dr. Jones's present address: Department of Cardiology, BristolRoyal Infirmary, Bristol, Avon, United Kingdom.
Part of this work was presented at the Second Gent Workshop onBlood Pressure Variability, Gent, Belgium, 1981.
Address for reprints: Dr. John S. Floras, Division of Cardiology,Toronto General Hospital, 12 EN-234,200 Elizabeth Street, Toron-to, Canada M5G 2C4.
Received June 25, 1987; accepted October 26, 1987.
in normal and hypertensive humans,1 but factors thatmight influence and regulate this variability remainimperfectly understood. Considerable experimentalevidence supports the concept that the arterial barore-ceptor reflex is intimately involved in the short-termregulation of arterial blood pressure. Denervation ofthe sinoaortic baroreceptors in rats and dogs consis-tently increases the beat-to-beat variation of bloodpressure but has less dramatic and disputed effects onits level.2"5 Central interruption of the baroreceptorreflex by lesioning nucleus tractus solitarii produceshypertension, tachycardia, and increased blood pres-sure variability in awake animals.6 Selective removalof the noradrenergic innervation of this nucleus doesnot induce hypertension, but it does cause an increasein blood pressure variability that is inversely related toa decrease in the baroreceptor reflex control of heartrate.7
In hypertension, the threshold for baroreceptor fir-ing is reset8 and the receptors themselves are less sensi-
273
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from
274 HYPERTENSION VOL 11, No 3, MARCH 1988
tive to further increases in arterial pressure.9 One mightpredict, as a consequence, that the reflex parasympa-thetic and sympathetic responses to a similar pressorstimulus would be attenuated. Indeed, the ability of thearterial baroreceptor reflex to inhibit efferent sympa-thetic activity is impaired in several experimental mod-els of hypertension,10"13 and the lability of blood pres-sure is increased in rabbits whose baroreceptor afferentdischarge is reduced, whether due to renal hyperten-sion, experimental atherosclerosis, or medial sclero-
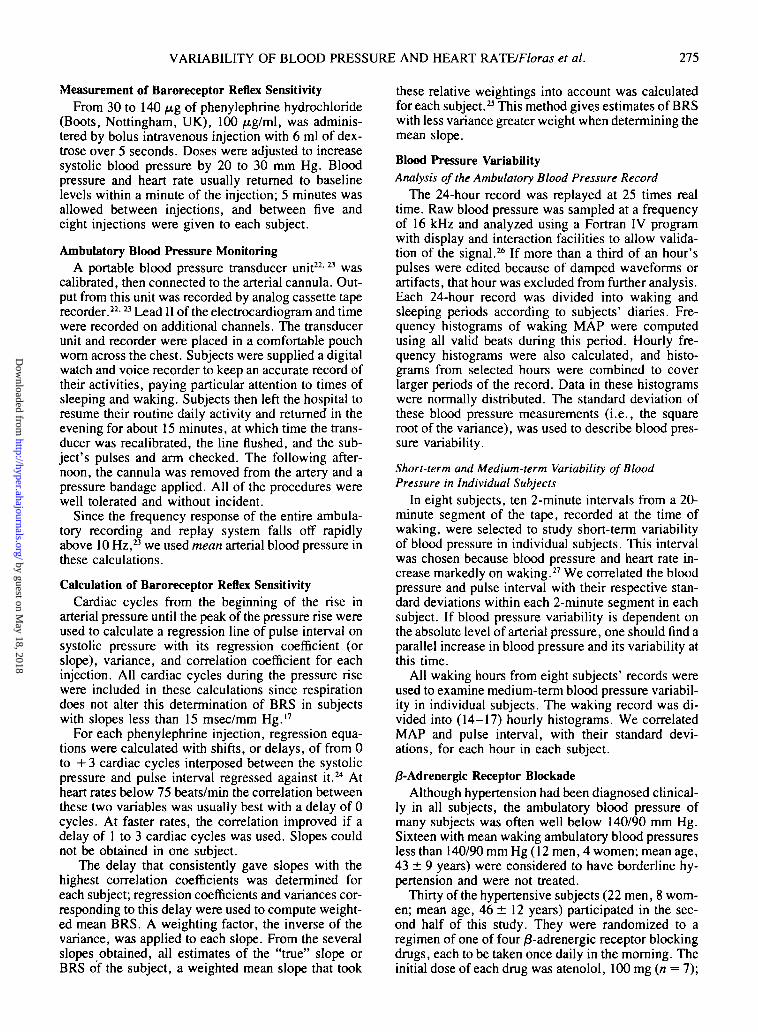
TABLE 1. Subject Characteristics
SIS. 14-16
In humans, the arterial baroreceptor reflex control ofcardiac cycle length has been well studied using tech-niques that quantify the reflex changes in heart rate inresponse to stimuli that alter blood pressure. If phen-ylephrine is administered, a linear relationship be-tween the systolic blood pressure of each beat and thesubsequent pulse interval can be established over thecourse of the pressure rise. The slope of this line hasbeen used as an index of baroreceptor reflex sensitivity(BRS). This technique examines primarily the para-sympathetic efferent limb of this reflex.17 Persons withmore sensitive baroreceptor reflexes exhibit a greaterreflex bradycardia for a similar absolute increase inblood pressure. Increasing age and mean arterial pres-sure (MAP) act independently to lower the slope of thisresponse.18
The aim of the present investigations was to deter-mine the influence of factors such as age, blood pres-sure, heart rate variability, and /3-adrenergic receptorblockade on intra-arterial blood pressure variability inawake, ambulatory subjects. Our hypotheses were that1) the reduction in BRS in hypertension would beassociated with increased variability of ambulatoryblood pressure, 2) the variability of blood pressurewould be inversely related to the variability of heartrate, 3) subjects with greater plasma norepinephrineconcentrations would also display increased bloodpressure variability, and 4) /3-adrenergic receptorblocking drugs would increase BRS and reduce thelability of blood pressure.
Subjects and MethodsFifty-six subjects (41 men, 15 women) were re-
ferred for assessment of newly diagnosed, untreatedhypertension. They ranged in age from 16 to 69 years(mean age, 46 ± 11 [SD] years; Table 1).
Hypertension was diagnosed if supine cuff pres-sures, obtained on three or more separate occasionsover 1 week apart were 140/90 mm Hg (Phase V dia-stolic) or greater in subjects under 40 years of age and160/95 mm Hg or greater in subjects over 40 years ofage. Readings below these values were recorded atother times in some subjects. Their average clinic pres-sure ranged from 137 to 216 mm Hg systolic (mean,172 ± 19 [SD] mm Hg) and from 80 to 137 mm Hgdiastolic (mean, 107 ± 10 mm Hg).
No subject had fundal changes greater than Grade2.19 In 18, the chest radiograph or electrocardiogramshowed changes of left ventricular enlargement. Nonewere in heart failure. Secondary hypertension was ex-
Variable
Age (yr)
MAP (mm Hg)
VMAP (mm Hg)
PI (msec)
VPI (msec)
LBRS
PNE
At rest (pg/ml)
Exercise (biking; pg/ml)
% Change
All subjects(n = 56)
46±11
118.3±17.9
13.8±2.4
678 ±87
132±34
0.78 ±0.30*
—
—
—
. Subjects in whomPNE was measured
(n = 44)
45±11
119.0±18.5
13.5 + 2.3
691 ±82
13O±3O
0.80±0.30
651+228
1112±448
81+81
Values are means ± SD. PNE = plasma norepinephrine;V = variability; PI = pulse interval; LBRS = log baroreceptor re-flex sensitivity.
*n = 55.
eluded by routine investigations in all patients but one,who had renal artery stenosis. Two were taking medi-cations concurrently: One was taking digoxin, 0.125mg/day, for control of atrial fibrillation, and another,sulfasalazine, 2 g/day, for Crohn's disease.
The purpose and nature of the protocol were ex-plained during recruitment and again on the morning ofthe first study, when informed written consent wasobtained. Consent was also obtained before the secondstudy day, when the protocol was repeated duringlong-term /3-adrenergic receptor blockade. Permissionfor these investigations was granted by the hospitalethics committee.
ProtocolSubjects arrived at 0930 after a light breakfast at
home, avoiding tea, coffee, or cigarettes. There wereno other dietary restrictions.
Arterial pressure was recorded from a left brachialcatheter connected to a strain gauge transducer cali-brated at all times at midchest level.20 An adjacentantecubital vein was cannulated for blood sampling orphenylephrine injection. The electrocardiogram (LeadII) and blood pressure were displayed on an oscillo-scope and recorded continuously onto ultraviolet light-sensitive paper, magnetic tape, and minicomputerdisk.
Plasma NorepinephrineVenous blood was withdrawn from the antecubital
catheter in 44 of these subjects as they sat quietly for 15minutes on a bicycle ergometer and again in the 10thminute of upright bicycle exercise (5 minutes at 50 W,then 5 minutes at 75 W). A 10-ml sample was obtainedand immediately centrifuged for 10 minutes at roomtemperature (1000 g) and frozen and stored at - 40 ° C.Norepinephrine concentration was measured by ra-dioenzymatic assay.21 Interassay and infra-assay coef-ficients of variation were 9.6% and 8.7%, respec-tively.
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from
VARIABILITY OF BLOOD PRESSURE AND HEART RATE/Floras et al. 275
Measurement of Baroreceptor Reflex SensitivityFrom 30 to 140 fig of phenylephrine hydrochloride
(Boots, Nottingham, UK), 100 ptg/ml, was adminis-tered by bolus intravenous injection with 6 ml of dex-trose over 5 seconds. Doses were adjusted to increasesystolic blood pressure by 20 to 30 mm Hg. Bloodpressure and heart rate usually returned to baselinelevels within a minute of the injection; 5 minutes wasallowed between injections, and between five andeight injections were given to each subject.
Ambulatory Blood Pressure MonitoringA portable blood pressure transducer unit22'a was
calibrated, then connected to the arterial cannula. Out-put from this unit was recorded by analog cassette taperecorder.22'H Lead II of the electrocardiogram and timewere recorded on additional channels. The transducerunit and recorder were placed in a comfortable pouchworn across the chest. Subjects were supplied a digitalwatch and voice recorder to keep an accurate record oftheir activities, paying particular attention to times ofsleeping and waking. Subjects then left the hospital toresume their routine daily activity and returned in theevening for about 15 minutes, at which time the trans-ducer was recalibrated, the line flushed, and the sub-ject's pulses and arm checked. The following after-noon, the cannula was removed from the artery and apressure bandage applied. All of the procedures werewell tolerated and without incident.
Since the frequency response of the entire ambula-tory recording and replay system falls off rapidlyabove 10 Hz,23 we used mean arterial blood pressure inthese calculations.
Calculation of Baroreceptor Reflex SensitivityCardiac cycles from the beginning of the rise in
arterial pressure until the peak of the pressure rise wereused to calculate a regression line of pulse interval onsystolic pressure with its regression coefficient (orslope), variance, and correlation coefficient for eachinjection. All cardiac cycles during the pressure risewere included in these calculations since respirationdoes not alter this determination of BRS in subjectswith slopes less than 15 msec/mm Hg.17
For each phenylephrine injection, regression equa-tions were calculated with shifts, or delays, of from 0to + 3 cardiac cycles interposed between the systolicpressure and pulse interval regressed against it.24 Atheart rates below 75 beats/min the correlation betweenthese two variables was usually best with a delay of 0cycles. At faster rates, the correlation improved if adelay of 1 to 3 cardiac cycles was used. Slopes couldnot be obtained in one subject.
The delay that consistently gave slopes with thehighest correlation coefficients was determined foreach subject; regression coefficients and variances cor-responding to this delay were used to compute weight-ed mean BRS. A weighting factor, the inverse of thevariance, was applied to each slope. From the severalslopes obtained, all estimates of the "true" slope orBRS of the subject, a weighted mean slope that took
these relative weightings into account was calculatedfor each subject.23 This method gives estimates of BRSwith less variance greater weight when determining themean slope.
Blood Pressure VariabilityAnalysis of the Ambulatory Blood Pressure Record
The 24-hour record was replayed at 25 times realtime. Raw blood pressure was sampled at a frequencyof 16 kHz and analyzed using a Fortran IV programwith display and interaction facilities to allow valida-tion of the signal.26 If more than a third of an hour'spulses were edited because of damped waveforms orartifacts, that hour was excluded from further analysis.Each 24-hour record was divided into waking andsleeping periods according to subjects' diaries. Fre-quency histograms of waking MAP were computedusing all valid beats during this period. Hourly fre-quency histograms were also calculated, and histo-grams from selected hours were combined to coverlarger periods of the record. Data in these histogramswere normally distributed. The standard deviation ofthese blood pressure measurements (i.e., the squareroot of the variance), was used to describe blood pres-sure variability.
Short-term and Medium-term Variability of BloodPressure in Individual Subjects
In eight subjects, ten 2-minute intervals from a 20-minute segment of the tape, recorded at the time ofwaking, were selected to study short-term variabilityof blood pressure in individual subjects. This intervalwas chosen because blood pressure and heart rate in-crease markedly on waking.27 We correlated the bloodpressure and pulse interval with their respective stan-dard deviations within each 2-minute segment in eachsubject. If blood pressure variability is dependent onthe absolute level of arterial pressure, one should find aparallel increase in blood pressure and its variability atthis time.
All waking hours from eight subjects' records wereused to examine medium-term blood pressure variabil-ity in individual subjects. The waking record was di-vided into (14-17) hourly histograms. We correlatedMAP and pulse interval, with their standard devi-ations, for each hour in each subject.
/3-Adrenergic Receptor BlockadeAlthough hypertension had been diagnosed clinical-
ly in all subjects, the ambulatory blood pressure ofmany subjects was often well below 140/90 mm Hg.Sixteen with mean waking ambulatory blood pressuresless than 140/90 mm Hg (12 men, 4 women; mean age,43 ± 9 years) were considered to have borderline hy-pertension and were not treated.
Thirty of the hypertensive subjects (22 men, 8 wom-en; mean age, 46 ± 12 years) participated in the sec-ond half of this study. They were randomized to aregimen of one of four /3-adrenergic receptor blockingdrugs, each to be taken once daily in the morning. Theinitial dose of each drug was atenolol, 100 mg (n = 7);
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from
276 HYPERTENSION VOL 11, No 3, MARCH 1988
metoprolol, 200 mg (n = 9); pindolol, 15 mg (n = 8);propranolol, 160 mg (n = 1); and slow-release pro-pranolol, 160 mg (n = 6). The manufacturers providedwhite, unmarked formulations. The randomizationschedule was held in the hospital pharmacy until afterthe second study.
Subjects were evaluated subsequently at monthlyintervals at the same time of day, and doses weretitrated as required.20 After 3 to 8 months (mean time, 5months), the protocol was repeated at the same time ofday as in the first (control) study with the assigned drugtaken as usual at 0800. Average doses were atenolol,121 ±57 mg (mean±SD); metoprolol, 300 ± 107mg; pindolol, 32 ± 10 mg; and propranolol, 457 ± 194mg. The average clinic blood pressure of these subjectswas 175 ± 25/107 ± 11 mm Hg before the first (con-trol) study and 146 ± 24/93 ± 15 mm Hg at the lastclinic visit before the second (treatment) study.
Rest and exercise samples of venous blood for plas-ma norepinephrine concentrations were obtained onboth study days in 21 of these subjects.
StatisticsThe Statistical Package for the Social Sciences Pro-
gram (SPSS) was used for paired comparisons (Stu-dent's / test), stepwise multiple regression analysis,and calculation of partial correlation coefficients.28
The Bonferroni method29 was used to calculate a modi-fied t statistic when multiple comparisons were per-formed. Partial correlation coefficients were also cal-culated to determine the relationship between twovariables while excluding the confounding effect ofother variables. Results are reported as means ± SDthroughout.
ResultsAH SubjectsBaroreceptor Reflex Sensitivity
Mean weighted baroreceptor reflex slopes (ex-pressed as BRS) ranged from 1.6 to 38.1 msec/mm Hg(mean, 8.0 ± 7.8 msec/mm Hg; n = 55), and as de-scribed by Gribbin et al. ,18 they were inversely relatedto age and MAP and displayed a skewed distribution.A normal distribution and linear relationships betweenBRS, age ( r= -0.62,p<0.0001), and systolic bloodpressure (r = - 0 . 6 1 , p< 0.0001), but not heart rate,were established when these slopes were transformedlogarithmically (log]0 BRS; LBRS). Therefore, LBRSwas used to represent BRS in subsequent calculations.
Correlation Between Short-term and Medium-termVariability of Blood Pressure and Level of PressureWithin Subjects
In no subject was the short-term variability of bloodpressure (2-minute intervals about the time of waking)related to the absolute level of arterial pressure (Table2). In three of the eight subjects studied, pulse intervaland its variability were positively correlated.
Over the medium term (1-hour segments), variabil-
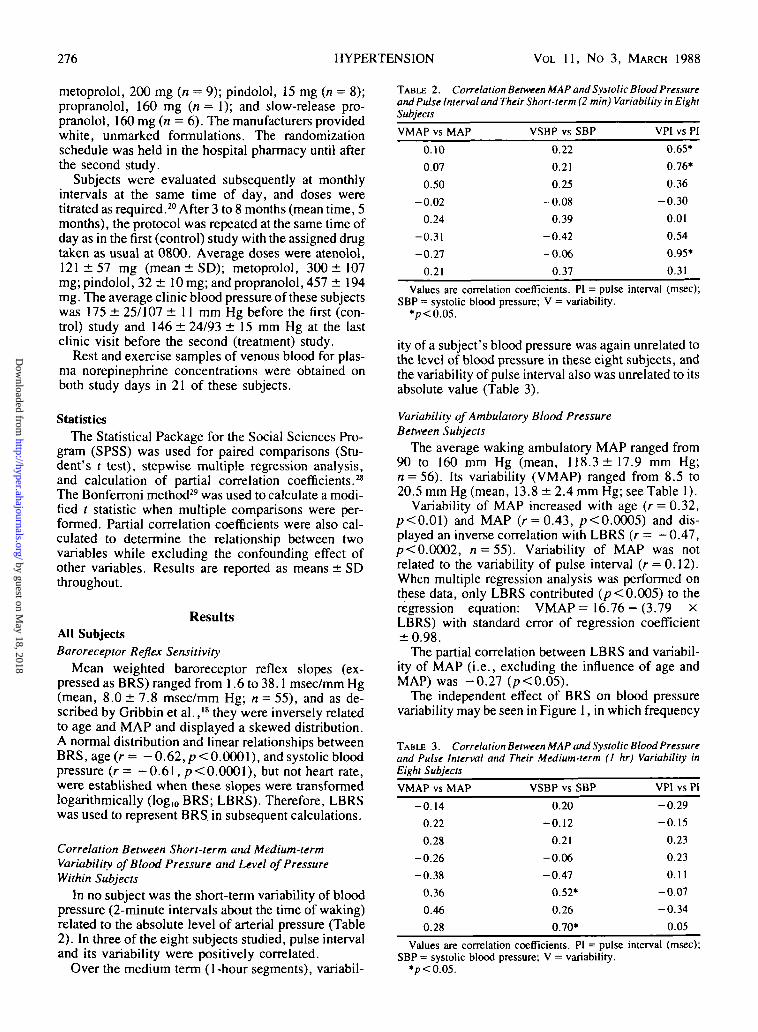
TABLE 2. Correlation Between MAP and Systolic Blood Pressureand Pulse Interval and Their Short-term (2 min) Variability in EightSubjects
VMAP vs MAP
0.10
0.07
0.50
-0.02
0.24
-0.31
-0.27
0.21
VSBP vs SBP
0.22
0.21
0.25
-0.08
0.39
-0.42
-0.06
0.37
VPI vs PI
0.65*
0.76*
0.36
-0.30
0.01
0.54
0.95*
0.31
Values are correlation coefficients. PI = pulse interval (msec);SBP = systolic blood pressure; V = variability.
*p<0.05.
ity of a subject's blood pressure was again unrelated tothe level of blood pressure in these eight subjects, andthe variability of pulse interval also was unrelated to itsabsolute value (Table 3).
Variability of Ambulatory Blood PressureBetween Subjects
The average waking ambulatory MAP ranged from90 to 160 mm Hg (mean, 118.3 ± 17.9 mm Hg;n = 56). Its variability (VMAP) ranged from 8.5 to20.5 mm Hg (mean, 13.8 ± 2.4 mm Hg; see Table 1).
Variability of MAP increased with age (r = 0.32,p<0.01) and MAP (r = 0.43, p<0.0005) and dis-played an inverse correlation with LBRS (r = —0.47,p<0.0002, n = 55). Variability of MAP was notrelated to the variability of pulse interval (r = 0.12).When multiple regression analysis was performed onthese data, only LBRS contributed (p<0.005) to theregression equation: VMAP = 16.76 - (3.79 XLBRS) with standard error of regression coefficient±0.98.
The partial correlation between LBRS and variabil-ity of MAP (i.e., excluding the influence of age andMAP) was -0.27 (p<0.05).
The independent effect of BRS on blood pressurevariability may be seen in Figure 1, in which frequency
TABLE 3. Correlation Between MAP and Systolic Blood Pressureand Pulse Interval and Their Medium-term (1 hr) Variability inEight Subjects
VMAP vs MAP
-0.14
0.22
0.28
-0.26
-0.38
0.36
0.46
0.28
VSBP vs SBP
0.20
-0.12
0.21
-0.06
-0.47
0.52*
0.26
0.70*
VPI vs PI
-0.29
-0.15
0.23
0.23
0.11
-0.07
-0.34
0.05
Values are correlation coefficients. PI = pulse interval (msec);SBP = systolic blood pressure; V = variability.
*p<0.05.
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from
VARIABILITY OF BLOOD PRESSURE AND HEART RATE/Floras et al. 277
3DCD
g. mo
i 10M
50 100 150 200
Man Arterial Prtssurt DUD Hg
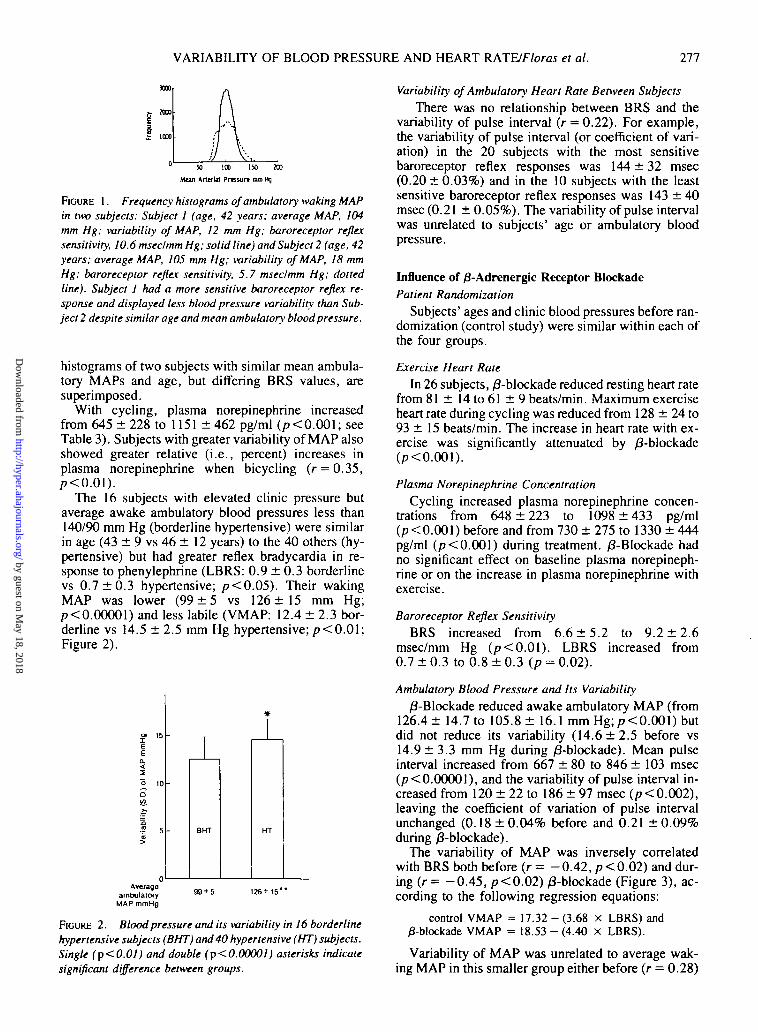
FIGURE 1. Frequency histograms of ambulatory waking MAPin two subjects: Subject 1 (age, 42 years; average MAP, 104mm Hg; variability of MAP, 12 mm Hg; baroreceptor reflexsensitivity, 10.6 msec/mm Hg; solid line) and Subject 2 (age, 42years; average MAP, 105 mm Hg; variability of MAP, 18 mmHg; baroreceptor reflex sensitivity, 5.7 msec/mm Hg; dottedline). Subject 1 had a more sensitive baroreceptor reflex re-sponse and displayed less blood pressure variability than Sub-ject 2 despite similar age and mean ambulatory blood pressure.
histograms of two subjects with similar mean ambula-tory MAPs and age, but differing BRS values, aresuperimposed.
With cycling, plasma norepinephrine increasedfrom 645 ± 228 to 1151 ± 462 pg/ml (p<0.001; seeTable 3). Subjects with greater variability of MAP alsoshowed greater relative (i.e., percent) increases inplasma norepinephrine when bicycling (r = 0.35,p<0.0l).
The 16 subjects with elevated clinic pressure butaverage awake ambulatory blood pressures less than140/90 mm Hg (borderline hypertensive) were similarin age (43 ± 9 vs 46 ± 12 years) to the 40 others (hy-pertensive) but had greater reflex bradycardia in re-sponse to phenylephrine (LBRS: 0.9 ± 0.3 borderlinevs 0.7 ± 0 . 3 hypertensive; p<0 .05) . Their wakingMAP was lower (99 ± 5 vs 126 ± 1 5 mm Hg;p<0.00001) and less labile (VMAP: 12.4 ± 2.3 bor-derline vs 14.5 ± 2.5 mm Hg hypertensive; p< 0.01;Figure 2).
BHT
Averageambulatory
MAP mmHg3 + 5 126+ IS
FIGURE 2. Blood pressure and its variability in 16 borderlinehypertensive subjects (BHT) and 40 hypertensive (HT) subjects.Single (p<0.01) and double (p<0.00001) asterisks indicatesignificant difference between groups.
Variability of Ambulatory Heart Rate Between Subjects
There was no relationship between BRS and thevariability of pulse interval (r = 0.22). For example,the variability of pulse interval (or coefficient of vari-ation) in the 20 subjects with the most sensitivebaroreceptor reflex responses was 144 ± 32 msec(0.20 ±0.03%) and in the 10 subjects with the leastsensitive baroreceptor reflex responses was 143 ± 40msec (0.21 ± 0.05%). The variability of pulse intervalwas unrelated to subjects' age or ambulatory bloodpressure.
Influence of /9-Adrenergic Receptor BlockadePatient Randomization
Subjects' ages and clinic blood pressures before ran-domization (control study) were similar within each ofthe four groups.
Exercise Heart Rate
In 26 subjects, /3-blockade reduced resting heart ratefrom 81 ± 14 to 61 ± 9 beats/min. Maximum exerciseheart rate during cycling was reduced from 128 ± 24 to93 ± 15 beats/min. The increase in heart rate with ex-ercise was significantly attenuated by )3-blockade0><0.001).
Plasma Norepinephrine Concentration
Cycling increased plasma norepinephrine concen-trations from 648 ± 2 2 3 to 1098 ±433 pg/ml(p<0.001) before and from 730 ± 275 to 1330 ± 444pg/ml (p< 0.001) during treatment. /3-Blockade hadno significant effect on baseline plasma norepineph-rine or on the increase in plasma norepinephrine withexercise.
Baroreceptor Reflex SensitivityBRS increased from 6.6 ± 5 . 2 to 9.2 ± 2 . 6
msec/mm Hg (p<0.01) . LBRS increased from0.7 ± 0 . 3 to 0.8 ± 0 . 3 (p = 0.02).
Ambulatory Blood Pressure and Its Variability
/3-Blockade reduced awake ambulatory MAP (from126.4± 14.7 to 105.8 ± 16.1 mm Hg;/7<0.001) butdid not reduce its variability (14.6 ± 2 . 5 before vs14.9 ± 3.3 mm Hg during /3-blockade). Mean pulseinterval increased from 667 ± 80 to 846 ± 103 msec(p<0.00001), and the variability of pulse interval in-creased from 120 ± 22 to 186 ± 97 msec (p< 0.002),leaving the coefficient of variation of pulse intervalunchanged (0.18 ± 0.04% before and 0.21 ± 0.09%during /3-blockade).
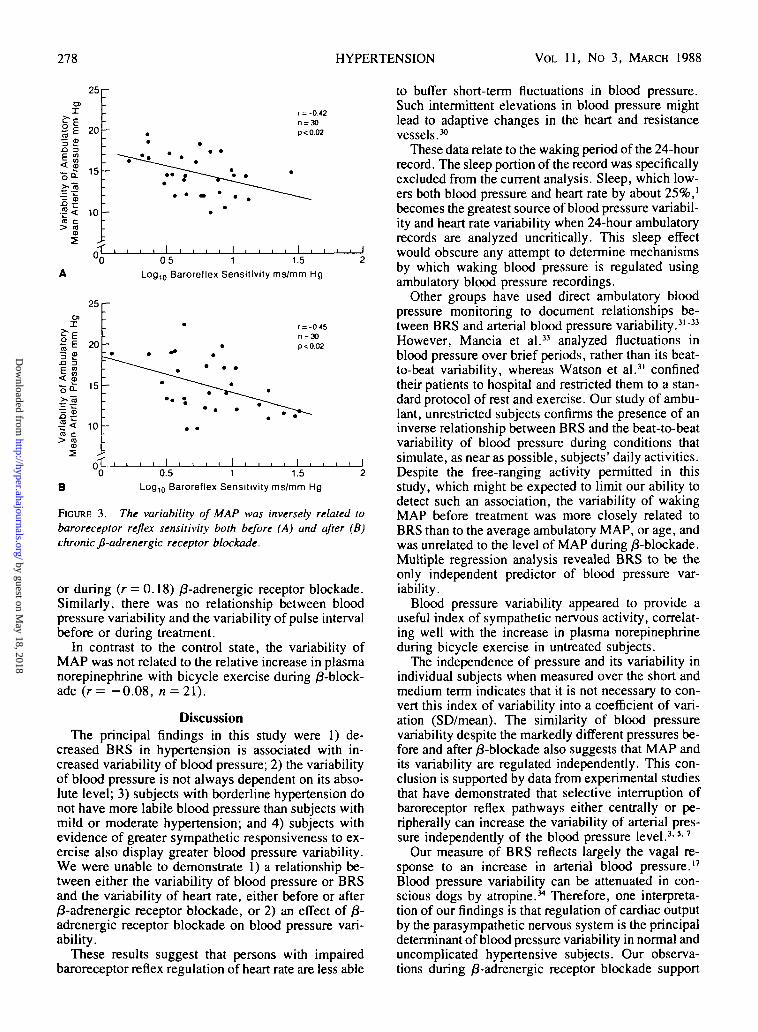
The variability of MAP was inversely correlatedwith BRS both before (r = - 0 . 4 2 , p<0.02) and dur-ing (r = - 0 . 4 5 , p<0.02) /3-blockade (Figure 3), ac-cording to the following regression equations:
control VMAP = 17.32-(3.68 x LBRS) and0-blockade VMAP = 18.53 - (4.40 x LBRS).
Variability of MAP was unrelated to average wak-ing MAP in this smaller group either before (r = 0.28)
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from
278 HYPERTENSION VOL 11, No 3, MARCH 1988
25OP
fi3 £
20
- n £ 15
.5 <CO c> co
CD
10
r = -0.42n = 30p<0.02
I I I05 1 1.5
Log,0 Baroreflex Sensitivity ms/mm Hg
25C3J
fi3 £3
5 •>< CD
>.&
20
15
°< 10
B
I I I0.5 1 1.5
Log,0 Baroreflex Sensitivity ms/mm Hg
FIGURE 3. The variability of MAP was inversely related tobaroreceptor reflex sensitivity both before (A) and after (B)chronic fi-adrenergic receptor blockade.
or during (r = 0.18) /3-adrenergic receptor blockade.Similarly, there was no relationship between bloodpressure variability and the variability of pulse intervalbefore or during treatment.
In contrast to the control state, the variability ofMAP was not related to the relative increase in plasmanorepinephrine with bicycle exercise during ^-block-ade ( r = - 0 . 0 8 , n = 2l).
DiscussionThe principal findings in this study were 1) de-
creased BRS in hypertension is associated with in-creased variability of blood pressure; 2) the variabilityof blood pressure is not always dependent on its abso-lute level; 3) subjects with borderline hypertension donot have more labile blood pressure than subjects withmild or moderate hypertension; and 4) subjects withevidence of greater sympathetic responsiveness to ex-ercise also display greater blood pressure variability.We were unable to demonstrate 1) a relationship be-tween either the variability of blood pressure or BRSand the variability of heart rate, either before or after/3-adrenergic receptor blockade, or 2) an effect of £-adrenergic receptor blockade on blood pressure vari-ability.
These results suggest that persons with impairedbaroreceptor reflex regulation of heart rate are less able
to buffer short-term fluctuations in blood pressure.Such intermittent elevations in blood pressure mightlead to adaptive changes in the heart and resistancevessels.30
These data relate to the waking period of the 24-hourrecord. The sleep portion of the record was specificallyexcluded from the current analysis. Sleep, which low-ers both blood pressure and heart rate by about 25%,'becomes the greatest source of blood pressure variabil-ity and heart rate variability when 24-hour ambulatoryrecords are analyzed uncritically. This sleep effectwould obscure any attempt to determine mechanismsby which waking blood pressure is regulated usingambulatory blood pressure recordings.
Other groups have used direct ambulatory bloodpressure monitoring to document relationships be-tween BRS and arterial blood pressure variability.31"33
However, Mancia et al.33 analyzed fluctuations inblood pressure over brief periods, rather than its beat-to-beat variability, whereas Watson et al.3' confinedtheir patients to hospital and restricted them to a stan-dard protocol of rest and exercise. Our study of ambu-lant, unrestricted subjects confirms the presence of aninverse relationship between BRS and the beat-to-beatvariability of blood pressure during conditions thatsimulate, as near as possible, subjects' daily activities.Despite the free-ranging activity permitted in thisstudy, which might be expected to limit our ability todetect such an association, the variability of wakingMAP before treatment was more closely related toBRS than to the average ambulatory MAP, or age, andwas unrelated to the level of MAP during /3-blockade.Multiple regression analysis revealed BRS to be theonly independent predictor of blood pressure var-iability.
Blood pressure variability appeared to provide auseful index of sympathetic nervous activity, correlat-ing well with the increase in plasma norepinephrineduring bicycle exercise in untreated subjects.
The independence of pressure and its variability inindividual subjects when measured over the short andmedium term indicates that it is not necessary to con-vert this index of variability into a coefficient of vari-ation (SD/mean). The similarity of blood pressurevariability despite the markedly different pressures be-fore and after /3-blockade also suggests that MAP andits variability are regulated independently. This con-clusion is supported by data from experimental studiesthat have demonstrated that selective interruption ofbaroreceptor reflex pathways either centrally or pe-ripherally can increase the variability of arterial pres-sure independently of the blood pressure level.33 '7
Our measure of BRS reflects largely the vagal re-sponse to an increase in arterial blood pressure.17
Blood pressure variability can be attenuated in con-scious dogs by atropine.34 Therefore, one interpreta-tion of our findings is that regulation of cardiac outputby the parasympathetic nervous system is the principaldeterminant of blood pressure variability in normal anduncomplicated hypertensive subjects. Our observa-tions during /3-adrenergic receptor blockade support
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from

VARIABILITY OF BLOOD PRESSURE AND HEART RATEJFloras et al. 279
such an interpretation: The significant inverse correla-tion between BRS and blood pressure variability waspreserved. Indeed, although ^-blockade may reduceblood pressure variability during selected periods ofactivity,35 neither a-adrenergic nor /J-adrenergic re-ceptor blockade appears to alter ambulatory bloodpressure variability overall.36
Although arterial compliance is a major determinantof BRS, the baroreceptor reflex can be altered indepen-dently of changes in arterial compliance at the level ofthe central nervous system, autonomic ganglia, or theneuroeffector junction. Angiotensin, for example, de-creases BRS in humans37 through a central mechanism,likely at the level of the area postrema, and facilitatesnoradrenergic transmission through a prejunctional ac-tion. In addition, there is considerable evidence thatmodulation of these reflexes by ionic mechanisms,endogenous peptides, and drugs can occur at the levelof sensory afferents; these changes can occur indepen-dently of alterations in arterial compliance.38 Our datapermit us to conclude that the baroreceptor reflex con-trol of pulse interval, as assessed by the phenylephrinetechnique, bears an inverse correlation with bloodpressure variability. Without an accurate measure ofarterial compliance, we are not able to determinewhether this is the major determinant of blood pressurevariability in hypertensive subjects or whether the ef-fect of arterial compliance on the BRS of each of thesesubjects may have been modulated by one or more ofthese mechanisms.
We did not observe a significant relationship be-tween blood pressure variability and heart rate vari-ability, in contrast to others, or between blood pressureand heart rate variability either before or after ^-block-ade.32' 33 Differing patient populations or methods maybe responsible. We included all cardiac cycles in ouranalysis of these data, whereas Mancia et al.33 pro-cessed their records to provide mean values for each 3-second interval. The latter approach may have contrib-uted to their finding by eliminating extremes of bloodpressure and heart rate (regression to the mean). Fur-ther, we assessed the variability of pulse interval, rath-er than heart rate itself. The use of pulse interval hasseveral advantages: The unit interval of time is used inthe calculation of BRS; the use of pulse interval per-mits analysis of beat-to-beat variability of the cardiaccycle length; and frequency histograms of pulse inter-val over the waking period are normally distributed,whereas those of heart rate, its. inverse, are skewed.39
Nonetheless, the standard deviation may be too crudean expression of heart rate or blood pressure variabil-ity. More sophisticated techniques, such as spectralanalysis,4041 may provide additional insight into therelationship between these two variables.
Recent studies have suggested an important contri-bution of heart rate to the buffering of acute changes inblood pressure in humans, such that subjects with moresensitive baroreceptor reflexes buffer these changes(and hence reduce arterial pressure variability) bygreater variations in pulse interval.42 However, ourresults did not permit us to conclude that the variability
of cardiac cycle length is influenced by either BRS orblood pressure variability. The variability of heart ratemay reflect emotional and physical factors that cannotbe controlled in studies of unrestricted subjects. Thispossibility may explain our inability to identify a rela-tionship between BRS and cardiac cycle variability.The effect of such factors on the baroreceptor reflexcontrol of heart rate is well documented. Mental arith-metic,43 handgrip,44'43 and dynamic exercise46 attenu-ate (probably centrally) the baroreceptor reflex regula-tion of heart rate. The extent of this attenuation cannotbe predicted from heart rate responses to pressor dosesof phenylephrine given when subjects are restingquietly.
In contrast to the regulation of heart rate, the carotidarterial baroreceptor reflex regulation of blood pres-sure, as tested by the neck collar technique, is notsuppressed by mental stress47 or isometric exercise.48 Itmay be attenuated during supine (not upright) bicycleexercise in humans.49 This latter point remains contro-versial; arterial baroreceptor reflexes of consciousdogs appear to continue to operate effectively duringtreadmill exercise.50"52 The strong association we ob-served between BRS and blood pressure variabilitycould be explained if the reflex regulation of bloodpressure was preserved during physical activity butwas less potent in hypertensive than in normal sub-jects.
Intermittent, noninvasive ambulatory monitoring53
and clinic blood pressure measurements54 have beenused to investigate the variability of blood pressure inborderline hypertension. Although such techniquescannot evaluate beat-to-beat blood pressure variabil-ity, our observations support the overall conclusion ofthese studies, namely, that blood pressure is not exces-sively labile in borderline hypertension. Blood pres-sure variability in untreated subjects was directly relat-ed to the level of arterial pressure and age; youngborderline hypertensive subjects had less variableblood pressure than older, more hypertensive subjectsdid, even though the latter may have been less active.
We conclude that 1) of the factors studied, the de-cline in BRS that occurs in both borderline and estab-lished hypertension diminishes the ability to bufferchanges in arterial pressure and becomes the principaldeterminant of increased blood pressure variability inessential hypertension; 2) MAP and its variability areregulated independently; 3) blood pressure variabilityis not affected by /3-adrenergic receptor blockade; 4)heart rate variability is not influenced by BRS and isunrelated to blood pressure variability; and 5) patientswith borderline hypertension do not have more labilepressure than those with established hypertension. It isnot known how variability over the 24-hour periodrelates to blood pressure variability in the same subjectover weeks, months, or years. Nor is it clear whetheran increase in variability of blood pressure leads, withtime, to more cardiovascular complications,30" orwhether the impairment of BRS may itself contributeto the development and maintenance of essentialhypertension.
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from
280 HYPERTENSION VOL 11, No 3, MARCH 1988
AcknowledgmentThe cost of plasma norepinephrine determinations was borne by
Astra Pharmaceuticals (UK) and the Wellcome and Rhodes Trusts.
References1. Floras JS, Sleight P. Ambulatory monitoring of blood pres-
sure. In: Sleight P, Jones JV, eds. Scientific foundations ofcardiology. London: Heineman, 1983:155-164
2. Cowley AW, Liard JF, Guyton AC. Role of the baroreceptorreflex in daily control of arterial blood pressure and othervariables in dogs. Circ Res 1973;32:564-576
3. Jones JV, Hallback M. Cardiovascular reactivity and design inrats with experimental "neurogenic hypertension." Acta Phys-iol Scand 1978;102:41-49
4. Ito CS, Scher AM. Hypertension following denervation ofaortic baroreceptors in unanaesthetized dogs. Circ Res1979;42:230-236
5. Alper RH, Jacob HJ, Brody MI. Central and peripheral mecha-nisms of arterial pressure lability following baroreceptor dener-vation. Can J Physiol Pharmacol 1987;65:1615-1618
6. Nathan MA, Reis DJ. Chronic labile hypertension produced bylesions of the nucleus tractus solitarii in the cat. Circ Res1977;40:72-81
7. Snyder DW, Nathan MA, Reis DJ. Chronic lability of arterialpressure produced by selective destruction of the catechola-mine innervation of the nucleus tractus solitarii in the rat. CircRes 1978;43:662-671
8. McCubbin JW, Green JH, Page IH. Baroreceptor function inchronic renal hypertension. Circ Res 1956;4:205-210
9. Sleight P, Robinson JL, Brooks DE, Rees PM. Characteristicsof single carotid sinus baroreceptor fibres and whole nerveactivity in the normotensive and the renal hypertensive dog.Circ Res 1977;41:75O-758
10. Coote JH, Sato Y. Reflex regulation of sympathetic nerveactivity in the spontaneously hypertensive rat. Circ Res1977;40:571-577
11. Judy WV, Farrell SK. Arterial baroreceptor reflex control ofsympathetic nerve activity in the spontaneously hypertensiverat. Hypertension 1979;l:605-614
12. Guo GB, Thames MD, Abboud FM. Arterial baroreflexes inrenal hypertensive rabbits: selectivity and redundancy of baro-receptor influence on heart rate, vascular resistance, and lum-bar sympathetic activity. Circ Res 1983;53:223-234
13. Guo GB, Abboud FM. Impaired central mediation of the arteri-al baroreflex in chronic renal hypertension. Am J Physiol1984;246:H720-H727
14. Angell-James JE. Arterial baroreceptor activity in rabbits withexperimental atherosclerosis. Circ Res 1974;34:27-39
15. Angell-James JE. Pathophysiology of aortic baroreceptors inrabbits with vitamin D sclerosis and hypertension. Circ Res1974;34:327-338
16. Angell-James JE, George MJ. Time-course of the reduction ofbaroreceptor sensitivity in experimental hypertensive rabbits.Clin Sci Mol Med 1976;51:369-372
17. Pickering TG, Gribbin B, Strange Petersen E, CunninghamDJC, Sleight P. Effects of autonomic blockade on the barore-flex in man at rest and during exercise. Circ Res 1972;30:177—185
18. Gribbin B, Pickering TG, Sleight P, Peto R. The effect of ageand high blood pressure on baroreflex sensitivity in man. CircRes 1971;29:424-431
19. Keith NW, Wagner HP, Barker NW. Some different types ofessential hypertension: their course and prognosis. Am J MedSci 1939;197:332-343
20. Floras JS, Hassan MO, Jones JV, Sleight P. Cardioselectiveand nonselective beta-adrenoceptor blocking drugs in hyper-tension: a comparison of their effect on blood pressure duringmental and physical activity. J Am Coll Cardiol 1985;6:186-195
21. Henry DP, Starman BJ, Johnson DG, Williams RH. A sensi-tive radioenzymatic assay for norepinephrine in tissues andplasma. Life Sci 1974; 16:375-384
22. Millar-Craig MW, Hawes D, Whittington J. New system for
recording ambulatory blood pressure in man. Med Biol Eng1978,16:727-731
23. Stott FD. The Oxford portable blood pressure transducer. In:Clement DL, ed. Blood pressure variability. Lancaster, UK:MTP Press 1979:55-60
24. Pickering TG, Davies J. Examination of the conduction timeof the baroreceptor cardiac reflex in man. Cardiovasc Res1973;7:213-219
25. FlorasJS, Hassan MO, Jones JV.etal. Baroreceptor control ofblood pressure and plasma noradrenaline. In: Sleight P, ed.Arterial baroreceptors and hypertension. Oxford, U.K.: Ox-ford University Press, 1980:470-475
26. Sleight P, Floras J, Jones JV. Automatic analysis of continuousintra-arterial blood pressure recordings. In: Clement DL, ed.Blood pressure variability. Lancaster, U.K.: MTP Press,1979:61-66
27. Floras JS, Jones JV, Johnson JA, Brooks DE, Hassan MO,Sleight P. Arousal and the circadian rhythm of blood pressure.Clin Sci Mol Med 1978;55:395s-397s '
28. Nie NH, Hull CH, Jenkins JG, Steinbrenner K, Bent D. SPSS,statistical package for the social sciences. New York:McGraw-Hill, 1975. 661 p
29. Wallenstein S, ZuckerCL, Fleiss JL. Some statistical methodsuseful in circulation research. Circ Res 1980;47:I-9
30. Parati G, Pomidossi G, Albini F, Malaspina D, Mancia G.Relationship of 24-hour blood pressure mean and variability toseverity of target-organ damage in hypertension. J Hypertens1987;5:93-98 ,
31. Watson RDS, Stallard TJ, Flinn RM, Littler WA. Factorsdetermining direct arterial pressure and its variability in hyper-tensive man. Hypertension 1980;2:333-341
32. Ogawa J, Arai S, Takata S, et al. Daily profile of baroreflexsensitivity and the variability of blood pressure in essentialhypertensive patients. Clin Sci I981;61:157s—159s
33. Mancia G, Parati G, Pomidossi G, Casadei R, Di Rienzo M,Zanchetti A. Arterial baroreflexes and blood pressure and heartrate variabilities in humans. Hypertension 1986;8:147-153
34. Clement DL, Jordaens LJ, Heyndrickx GR. Influence of vagalnervous activity on blood pressure variability. J Hyperten1984;2:391-393
35. Watson RDS, Stallard TJ, Littler WA. Influence of once-dailyadministration of /3-adrenoreceptor antagonists on arterialpressure and its variability. Lancet 1979; 1:1210—1213
36. Clement DL, Cardon E, Castro M, De Pue N, Packet L, VanMaele GO. Effect of metoprolol and guanfacine on ambulatoryblood pressure and its variations. Br J Clin Pharmacol1983;15:471s-478s
37. Mace PJE, Watson RDS, Skan W, Littler WA. Inhibition ofthe baroreceptor heart rate reflex by angiotensin II in normalman. Cardiovasc Res 1985;19:525-527
38. Mark AL. Sensitization of cardiac vagal afferent reflexes at thesensory receptor level: an overview. Fed Proc 1987;46:36—40
39. Floras JS. Neural regulation of blood pressure in hypertension[Dissertation]. Oxford, U.K.: University of Oxford, 1981.199 p
40. deBoer RW, Karemaker JM, Stackee J. Relations betweenshort term variability in resting subjects: I. A spectral analysisapproach. Med Biol Eng Comput 1985;23:352-358
41. Pagani M, Lombardi F, Guzzetti S, et al. Power spectral analy-sis of heart rate and arterial pressure variabilities as a marker ofsympathovagal interaction in man and conscious dog. Circ Res1986^9:178-193
42. Conway J. Blood pressure and heart rale variability. J Hyper-tens 1986;3:261-266
43. Sleight P, Fox P, Lopez R, Brooks D. The effect of mentalarithmetic on blood pressure variability and baroreflex sensi-tivity in man. Clin Sci Mol Med 1978;55:381s-382s
44. Cunningham DJC, Strange Petersen E, Peto R, Pickering TG,Sleight P. Comparison of the effect of different types of exer-cise on the baroreflex regulation of heart rate. Acta PhysiolScand 1972;86:444-455
45. Mancia G, Iannos J, Jamieson GG, Lawrence RH, SharmanPR, Ludbrook J. Effect of isometric hand-grip exercise on the
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from
VARIABILITY OF BLOOD PRESSURE AND HEART RATE/F/ora5 et al. 281
carotid sinus baroreceptor reflex in man. Clin Sci Mol Med1978;54:33-37
46. Bristow JD, Brown EB, Cunningham DJC, et al. Effect ofbicycling on the baroreflex regulation of pulse interval. CircRes 1971;28:582-592
47. Foreman L, Lindblad LE. Effect of mental stress on barorecep-tor-mediated changes in blood pressure and heart rate and onplasma catecholamines and subjective responses in healthymen and women. Psychosom Med 1983;45:435-445
48. Ludbrook J, Faris IB, Iannos J, Jamieson GG, Russell WJ.Lack of effect of isometric handgrip exercise on the responsesof the carotid sinus baroreceptor reflex in man. Clin Sci MolMed 1978;55:189-194
49. Fiocchi R. Carotid baroreceptor control of heart rate and bloodpressure at rest and exercise in man [Dissertation]. Leuven,Belgium: Catholic University of Leuven, 1986: appendix 1.37 p
50. Vatner SF, Franklin D, Van Citters RL, Braunwald E. Effects
of carotid sinus nerve stimulation on blood-flow distribution inconscious dogs at rest and during exercise. Circ Res1970;27:495-503
51. Melcher A, Donald DE. Maintained ability of carotid barore-flex to regulate arterial pressure during exercise. Am J Physiol1981;241:H838-H849
52. Walgenbach SC, Donald DE. Inhibition by carotid baroreflexof exercise-induced increases in arterial pressure. Circ Res1983;52:253-262
53. Horan MJ, Kennedy ML, Padgett NE. Do borderline hyperten-sive patients have labile blood pressure? Ann Intern Med1981;94(part l):466-468
54. Kannel WB, Sorlie P, Gordon T. Labile hypertension: a faultyconcept? The Framingham Study. Circulation 1980;61:l 183—1187
55. Floras JS, Jones JV, Hassan MO, Osikowska B, Sever PS,Sleight P. Cuff and ambulatory blood pressure in subjects withessential hypertension. Lancet 1981;2:107-109
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from

J S Floras, M O Hassan, J V Jones, B A Osikowska, P S Sever and P SleightFactors influencing blood pressure and heart rate variability in hypertensive humans.
Print ISSN: 0194-911X. Online ISSN: 1524-4563 Copyright © 1988 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Hypertension doi: 10.1161/01.HYP.11.3.273
1988;11:273-281Hypertension.
http://hyper.ahajournals.org/content/11/3/273the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://hyper.ahajournals.org//subscriptions/
is online at: Hypertension Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document.
Permissions and Rights Question and Answer Further information about this process is available in therequested is located, click Request Permissions in the middle column of the Web page under Services.not the Editorial Office. Once the online version of the published article for which permission is being
can be obtained via RightsLink, a service of the Copyright Clearance Center,Hypertensionpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on May 18, 2018
http://hyper.ahajournals.org/D
ownloaded from