face to face and oasis - home | homecare …...supposed to be seen by her doctor after her soc but...
TRANSCRIPT
OASISCNAVIGATING YOURWAY TONAVIGATINGYOURWAYTO
SUCCESSSUCCESSAPRIL 2013
1Presented by Selman-Holman & Associates, LLCTeresa Northcutt BSN, RN, COS-C, HCS-D
Selman‐Holman&Associates,LLC2
Teresa Northcutt BSN, RN, COS-C, HCS-D Home Health Insight—Consulting, Education and
ProductsCoDR—Coding Done RightCoDR Coding Done Right
606 N. Bell Ave.Denton, Texas 76209
214.550.1477972.692.5908
teresa@selmanholman [email protected]
www.selmanholman.com
AccreditationStatement3
Selman-Holman & Associates, LLC is an approved ppprovider of continuing nursing education by the Texas Nurses Association, an accredited approver by the American Nurses Credentialing Center’s y gCommission on Accreditation.
To receive contact hours for this continuing education activity the participant must:education activity, the participant must: Sign in at the admission table at the beginning of each
dayA d h f ll l h d Attend the full class each day
Fill out and turn in a course evaluation form Once successful completion has been verified a Once successful completion has been verified, a
“Certificate of Successful Completion” will be awarded for 11.5 contact hours.
Terminology
CMS—Center for Medicare/Medicaid Services (also known as
4
Medicare and used to be known as HCFA) CASPER—Certification and Survey Provider Enhancement Reports CoPs—Conditions of Participation found at 42 CFR 484 CoPs Conditions of Participation found at 42 CFR 484 CWF—Common Working File (Medicare data system with records of
beneficiaries and the providers that have treated the beneficiary)E i d E i d b ith t i d (60 d ) Episode—Episodes can be either payment episodes (60 days) or quality episodes (SOC/ROC to Transfer/DC)
PEP—Partial Episode Payment (episode payment is pro-rated from f )first billable visit to last billable visit)
RAP—Request for Anticipated Payment (not considered a claim per se but either 60% of the payment or 50% of the payment is available at beginning of episode)
Terminology
MAC—Medicare Administrative Contractor used to be k R i l H H l h I di
5
known as Regional Home Health Intermediary ROC—Resumption of Care (assessment timepoint, as
well as the first visit after the patient has been pdischarged from a facility during an episode)
SCIC—Significant Change in Condition (actually an obsolete billing term but has become the slang term g gfor the Other Follow-Up assessment that is required when the patient has a major improvement or decline in condition)
SOC—Start of Care (the first billable visit in the first episode of care)
Transfer—also known as TIF (transfer to inpatient Transfer also known as TIF (transfer to inpatient facility) or TRN and TRF and TRS
MDataItems
The following OASIS information is from Ch. 3 of 6
gOASIS Guidance Manual and other CMS sources.Ch t 3 li t th OASIS it d fi iti ti Chapter 3 lists the OASIS item, a definition, time points for collection, response-specific instructions, and assessment strategies.instructions, and assessment strategies.
Besides Chapter 3 there are many questions with answers from CMS that will be referenced.
Sometimes agency policy or state law will conflict with these federal regulations. In that case, the agency and clinicians should comply with theagency and clinicians should comply with the strictest of the requirements.
Accurate & consistent answersto ALL OASIS questions
will yield
Optimal reimbursement and Optimal reimbursement and Optimal reimbursement and Optimal reimbursement and Better risk adjustment and outcomes Better risk adjustment and outcomes
7
F F d OASISFacetoFaceandOASIS8

FaceToFaceEncounterJanuary2012
Mrs. Cline was admitted to ABC Home Health on 9
January 1, 2012. She had not seen her physician since August, 2011.
Upon admission the RN explained the F2FUpon admission the RN explained the F2F regulation and was assured by the patient and her family that a visit would be scheduled prior to the 30 day point of January 31stto the 30 day point of January 31st .
Mrs. Cline’s appointment was scheduled forMrs. Cline s appointment was scheduled for February 4th , 35 days after the SOC OASIS assessment………
In this scenario, the date when all Medicare eligibility was met would be 30 days prior to theeligibility was met would be 30 days prior to the F2F encounter (with the F2F encounter date counted as day 1). y )
The (M0090) Date Assessment Completed should be reported as the actual date the new OASIS assessment is being generated, even if no visit is provided on that date.
Timing warnings from the OASIS state system may be generated based on the difference between the start of care date and the date thebetween the start of care date and the date the assessment was completed (> 5 days), but these warnings may be unavoidable in thesethese warnings may be unavoidable in these situations and can be disregarded.
10
Someparticularstobeawareof:
M0110 may need to be changed to reflect the correct i d i i
11
episode timing M2200 may need to be changed to exclude therapy visits
provided before the date of eligibility. p g y Medicare will not pay for services provided before the date on
which all Medicare HH eligibility have been met, which in the scenario described would refer to any services provided in the first five days of carefirst five days of care.
If the original OASIS assessment had already been submitted to the State, it should be deleted, and the newly generated SOC OASIS assessment (with modifiedgenerated SOC OASIS assessment (with modified M0030/M0090 dates, M0110, M2200, etc.) submitted.
All assessments should be maintained in the agency clinical record with documentation explaining theclinical record, with documentation explaining the situation.
The‘WrapUp’forMrs.Cline…..
Agency provides first skilled visit January 1st
12
Agency provides first skilled visit January 1st Face-to-Face encounter occurs February 4th (Day 35) Date when all Medicare eligibility was established
J 6th (30 d i t th F2F t ithJanuary 6th (30 days prior to the F2F encounter, with F2F encounter date counted as "day 1")
Non-covered visit period (January 1st-5th) (M0030) SOC Date on generated OASIS (The date of
the first visit on or after January 6th) (M0090) Date Assessment Completed on generated (M0090) Date Assessment Completed on generated
OASIS (The actual date new assessment is generated –on or after the February 4th F2F encounter.)

Whatdoes‘generate’mean?g
“Generate" means that the OASIS can be copied from the previous one in its entirety except for updating specific questions mentioned (like M0030 M0090 M0110mentioned, (like M0030, M0090, M0110, and M2200) with indifference to the actual condition of the patient at (or close to) the
f SOCtime of the new SOC date. 1st quarter 2012
Generated means no one is actually doing an assessment so it does not have to beassessment so it does not have to be generated by the same qualified clinician who did the most recent OASIS. 1st quarter 2012q
SOCDate/NewPOC/
SOC date is date patient became eligible for care (30 days prior to p g ( y pF2F encounter) OR the first billable visit after the date of eligibility.
First billable visit means any discipline making a billable visit (first covered visit).A new Plan of Care (POC) must be developed based on the new A new Plan of Care (POC) must be developed based on the new SOC date with specific orders for services.
Begin date/SOC date that equals the date of the first billable service provided on or after the patient became eligible for the Medicare p p ghome health benefit (30 days prior to the F2F encounter). This POC should match the SOC date on the newly generated SOC OASIS.
The new Plan of Care must include all existing orders beginning with the new SOC date as well as any additional orders obtained to coverthe new SOC date as well as any additional orders obtained to cover the 9-week cert period. The orders may have changed over time, and the new POC should reflect all orders relevant to the certification period of the new Medicare-covered episode. Th i i l POC h ld b k t i th li i l d f f The original POC should be kept in the clinical record for reference and documentation should be in the record explaining the late face-to-face and related actions.
Anotherexample:p
Mrs. Dee’s SOC was January 1. She was 15
ysupposed to be seen by her doctor after her SOC but then the doctor went skiing
d th i it did ’t h N ’and the visit didn’t happen. Now, you’ve just done your end of episode audit and figured out that there is no F2Ffigured out that there is no F2F documentation on the chart. You call the physician’s office and you are politely told th t th i it h d t b h d l d dthat the visit had to be rescheduled and Mrs. Dee will be seeing the doctor next week That is day 70!!week. That is day 70!!
WhatiftheF2Fdoesnotoccuruntilthenext recert period?nextrecert period?
Medicare will not pay for services provided before the d hi h ll M di HH li ibili h b
16
date on which all Medicare HH eligibility have been met, which in the scenario described would refer to any services provided in the first 40 days of care. (F2F day –30 days)30 days)
Any original OASIS assessments which may already have been submitted to the State, (likely SOC and RecertA t i thi i ) h ld b d l t d d thAssessments in this scenario) should be deleted, and the newly generated SOC OASIS assessment (with modified M0030/M0090 dates, M0110, M2200, etc.) submitted. All t h ld b i t i d i th All assessments should be maintained in the agency clinical record, with documentation explaining the situation.
Example:
Agency provides first skilled visit January 1st
17
Agency provides first skilled visit January 1st Face-to-Face encounter occurs March 11th (Day 70) Date when all Medicare eligibility was established
F b 10th (30 d i t th F2F t ithFebruary 10th (30 days prior to the F2F encounter, with F2F encounter date counted as "day 1")
Non-covered visit period (January 1st – February 9th) (M0030) SOC Date on generated OASIS (The date of the
first visit on or after February 10th) (M0090) Date Assessment Completed on generated (M0090) Date Assessment Completed on generated
OASIS (The actual date new assessment is generated –on or after the March 11th F2F encounter.)
ClosestOASISAssessment
Closest assessment is the Recertification The Recertification OASIS only includes payment items. An incomplete OASIS cannot be submitted to the state
system and you may not "create" answers. y y y You will generate your new SOC OASIS based on the
existing data from the assessment conducted closest to the date of eligibility.
If the closest assessment is a Follow-Up Assessment (i.e., a Recert or Other Follow-up), generate the new SOC using all the available Recert items first, then finish generating the assessment by using items from the SOC or ROC that wasassessment by using items from the SOC or ROC that was conducted closest to the date of eligibility.
Remember to update specific items, (like M0030, M0090, M0110 M2200 etc )M0110, M2200, etc.)
ClosestOASISAssessment
Closest assessment is a Discharge g Generate the new SOC using all available
Discharge items first, continue with ti th t b ddigenerating the new assessment by adding
additional items available from the Follow-up assessment (if any) that was conducted up assess e ( a y) a as co duc edclosest to the date of eligibility, and then finish generating the assessment by using items from the SOC or ROC that wasitems from the SOC or ROC that was conducted closest to the date of eligibility.
Remember to update specific items, (like Remember to update specific items, (like M0030, M0090, M0110, M2200, etc.)
M0110,M0102/M0104, /
M0110 Since the non-covered visits did not constitute a
Medicare PPS episode, that episode would not be considered for M0110.
M0102/M0104 A late F2F is treated as a payer change. In the
specific situation where a new SOC comprehensivespecific situation where a new SOC comprehensive assessment is generated for the sole purpose of changing the payer to Medicare, M0102 – Date of Physician-ordered SOC would be “NA”. For M0104 –yDate of Referral, enter the day prior to the new Start of Care date.
1st quarter 2012

TherapyCountspy
Because the therapy visits provided before the 21
py pnew start of care date (post-face-to-face completion) are not covered by Medicare, those visits do not count towards the Medicare-covered visit count for assessment timing. As was discussed in the CY 2012 final rule, only Medicare-covered visits are to be consideredMedicare covered visits are to be considered and counted. HHAs should track both Medicare-covered and non-covered therapy visits to keep count of the appropriate number of Medicare-count of the appropriate number of Medicare-covered therapy visits in these situations.
DeletingPreviousAssessments Original SOC assessment must be deleted
before the newly "generated" SOC assessment is t itt d t th t ttransmitted to the state.
All of the linked assessments must also be deleted All new assessments that occurred afterdeleted. All new assessments that occurred after the new SOC date will need to be generated and transmitted The new info (TRS/ROC etc) will betransmitted. The new info (TRS/ROC,etc) will be linked to the new SOC assessmentWhen generating new assessments copy the g g py
OASIS data from the original assessments except for updating, when appropriate, OASIS items like M0030, M0090, M0110, M2200, etc,.
OASIS C iOASISCorrections23
OASISDataTransmissionvsBillingBilling
OASIS data is required to be transmitted (exported)
24
OASIS data is required to be transmitted (exported) via the state to CMS for data quality purposes. Within 30 days of M0090 (prior to submitting final bill)
F t l d i t d b dit i th t Fatal errors and warnings created by edits in the system For example: Cannot mark a Stage II pressure ulcer as
partial/early granulation. OASIS data is used to determine outcomes and OASIS data is used to determine outcomes and
provided back to the agency in reports, both on CASPER and on Home Health CompareOASIS data (certain items) are used in the grouper to OASIS data (certain items) are used in the grouper to determine an HHRG. The HHRG will determine payment for that episode. RAPs and final claims are sent to Medicare intermediariessent to Medicare intermediaries.
Scenario
Question: Our clinician reported an ostomyQuestion: Our clinician reported an ostomyas a surgical wound in the OASIS M1340 Surgical Wound item TheM1340, Surgical Wound item. The clinician no longer works for the agency, so we cannot contact her about the errorso we cannot contact her about the error.
Can this OASIS change be made by the DON ith t ki t th li i i ?DON without speaking to the clinician?
2-Q37.4
Other correction policy info at 2-Q37.3p y
True OASIS scoring error was discovered during the audit process The assessment was completethe audit process. The assessment was complete.
The patient had an ostomy, a clear, non-disputable fact based on the entire clinical record.disputable fact based on the entire clinical record. The assessing clinician responsible for completing the assessment misunderstood, wasn't aware, or made an error based on the OASIS scoring guidance, which states all ostomies are excluded
i l d i M1340as surgical wounds in M1340. When the original documenter is not available, the
clinical supervisor or quality staff may make theclinical supervisor or quality staff may make the correction to the documentation following the correction policycorrection policy.
The supervisor must document why the original assessing clinician is not available to make theassessing clinician is not available to make the correction and how the error was identified and validated as a true error. Wh ti d t t When corrections are made to assessments submitted to state, you must determine the impact of the correction on the POC, HHRG, RAP and make corrections to those documents and billing, as applicable.
Keep the original and the new assessment Keep the original and the new assessment. Follow guidance found in CMS Survey & Cert Letter
01-12 New Outcome and Assessment Information Set (OASIS) Correction Policy for Home Health Agencies (HHAs)—ACTION and INFORMATION at www.cms.hhs.gov/SurveyCertificationGenInfo/downlowww.cms.hhs.gov/SurveyCertificationGenInfo/downloads/scletter01-12.pdf
FeaturedOASISApplications
OBQI
pp28
OBQIOBQM / Potentially Avoidable Events Best Practices/Process MeasuresCase Mix ProfileCase Mix ProfileRisk Adjustment
Home Health CompareHome Health CompareEnhanced SurveyPPS/HHRG

OutcomeBasedQualityImprovement,OutcomeBasedQualityMonitoring/Management
andProcessMeasures29
Risk-Adjusted End Result Outcome MeasuresImprovement in Stabilization
Grooming Mgmt of Oral Meds Upper Body GroomingGroomingDyspneaBathing
Bed
Mgmt of Oral MedsUrinary
IncontinenceConfusion
Upper Body Dressing
Lower Body Dressing
GroomingBathing
Bed TransferringLight MealBed
TransferringToilet
Transferring
Confusion Frequency
Urinary Tract Infections
DressingLight Meal
PreparationPhone Use
Light Meal PreparationPhone Use
Mgmt. of Oral MedsEating
Speech andLanguage
Bowel IncontinenceAmbulation/Locomo
tionS f S i l
Anxiety LevelCognitive
Functioning
Speech and LanguageCognitive
F i iStatus of Surgical Wounds
Behavior Problem Freq
FunctioningAnxiety Level
Toilet TransferringToileting HygieneFreq.
Pain Interfering w/Activity
Toileting Hygiene
Risk-Adjusted Utilization Outcome MeasuresDischarged to Community
Acute Care Hospitalization
Emergency Dept Use w/ HospitalizationEmergency Dept Use w/o Hospitalization
30
OASISTimepoints
SOC -------------- DC31
SOC DCSOC -------------- TransferROC DCROC -------------- DCROC -------------- TransferTh D fi iti f E i d C BThe Definition of an Episode Can Be
D I f ff r e tD I f ff e r e n t
Quality vs payment episode, and ‘short y p y pterm’ vs ‘long term’ episode
Outcomes
OASIS data items are arranged from32
OASIS data items are arranged from least impaired or independent, to most impaired or dependentimpaired or dependent.
The answer at SOC/ROC is compared to th t T f /DC t d t ithe answer at Transfer/DC to determine if there has been improvement, decline
t bili ti th t ti lor stabilization on that particular outcome.

Example—AtSOC,Mr.Brownwasmarked as a 3markedasa3.
33
X
AtDC,Mr.Brownwasmarkedasa2ashehadbeentrainedbytherapytousea2handeddevice,buthe
ill d d i l istillneededoccasionalassistance.34
X
EpisodesExcludedfromOutcomeEpisodesEpisodes
35
Those episodes that score a zeroFor example patient is scored a zero on
transferring transferring will not betransferring—transferring will not be evaluated on that particular patient for the rest of his stayy
Those episodes that don’t change either up or down (unless there is a p (stabilization outcome for that particular item)
Episodes longer than one year
PotentiallyAvoidableEventsEmergent Care for Injury Caused by Fall
Discharged to community needing wound care or medication
Substantial Decline in 3 or more Activities of Daily
Development of Urinary Tract Infection
medication assistance Living
Emergent Care for Discharged to Substantial Decline Increase in Wound Infections, Deteriorating Wound Status
community with behavioral problems
in Mngt of Oral Medications
Number of Pressure Ulcers
Emergent Care for Improper Medication Administration, Medication Side
Discharged to the community needing toileting assistance
Medication Side EffectsEmergent Care for Hypo/Hyperglycemia
Discharged to the community with a yp yp g y yunhealed Stage II pressure ulcer
36

ExampleM2310 Reason for Emergent CareM2310ReasonforEmergentCare
37
X
X
X
X
OutcomevsProcessMeasure
Outcome Measures determine the impact of our /i i
38
process/interventions How many patients were acutely hospitalized? Utilization outcome
Outcome measures are specific, measureable indicators of the successes of our interventions-the quality of care provided
P M d t i if t i Process Measures determine if certain processes are in place that promote good outcomes-best practices
H ti t i i d? How many patients were immunized? How many diabetics received foot exam and teaching?
Process Measures suggest that good patient outcomes are being pursued and may eventually be obtainedare being pursued and may eventually be obtained
ProcessMeasures
Future Value-Based Purchasing39
Future Value-Based PurchasingLink home health payment to:1. Improvements in patient outcomes
and/or2. Adoption of evidence-based care
processes
StandardizedTools A standardized tool is one that
1) has been scientifically tested on a population with characteristics similar to that of the patient (community dwelling elders) being assessed and shown to be effective in identifying ((theshown to be effective in identifying ((the problem)); and
2) includes a standard response scale (e g a2) includes a standard response scale (e.g., a scale where patients rate pain from 0-10).
The standardized tool must be appropriately The standardized tool must be appropriately administered as indicated in the instructions and must be relevant for the patient's ability to respond. p y p
CMS does not endorse a specific tool.

Q&A#1April2013Q p
There is no Medicare requirement that 41
qstandardized assessment tools be embedded in agency’s comprehensive
t ( t PHQ 2 i M1730) Itassessment (except PHQ-2 in M1730). It is acceptable for clinician to supplement agency’s comprehensive assessment withagency s comprehensive assessment with additional standardized assessment forms to meet the criteria for the OASIS best
ti it I l d f i di lpractice items. Include form in medical record with comprehensive assessment.
What is Risk Adjustment?WhatisRiskAdjustment?42
ImpactofRiskAdjustment
Y d it ti t t h All
43
You admit a patient to home care. All outcomes that you did not answer ‘0’ on will be included in the outcome measures.
Other answers on the OASIS will be used to risk adjust the expectedused to risk adjust the expected outcomes for that patient.
ImpactofRiskAdjustmentTh f i k dj t t i t t ti ti ll The purpose of risk adjustment is to statistically compensate (or adjust) for risk factor differences in the two samples so that the outcome rates can be
d l iti t l d it th diff i i kcompared legitimately despite the differences in risk factors.
May affect positively or negatively May affect positively or negativelyEach outcome measure used in producing risk-
adjusted outcome reports for OBQI tends to haveli it d b f i k f t (f 20 t b ta limited number of risk factors (from 20 to about
50)
44

Home Health CompareHomeHealthCompare
Home Health Quality Initiative45
Home Health Quality Initiative
Empowers consumers• www.medicare.gov/HHcompareEmpowers consumersStimulates providers
Compares your agency againstCompares your agency against other agencies across the nation (with names)( )
Risk adjusted outcomesNQF endorsed process measuresNQF endorsed process measures
EnhancedSurveyProcessy
Outcomes selected from the OBQM46
Outcomes selected from the OBQMOutcomes from OBQI included in
protocolAcute conditions and diagnosescute co d t o s a d d ag osesSubmission statistics
EError summary
HomeHealthResourceGroup
OASIS is the basis for payment47
p y HHRG produced through grouper softwareDetermined by 25 OASIS itemsyThree domainsClinical SeverityyFunctional StatusService utilization
45 HHRGs; 153 case mix weightsC1F1S1 to C3F3S5 for four different
equations (five different groupings)(five different C1F1S1s) 48

M0110EpisodeTiming0 0 p sode g49
M0110Guidance
A “sequence of adjacent Medicare home health payment episodes” is a continuous series of Medicare payment
50
episodes is a continuous series of Medicare payment episodes, regardless of whether the same home health agency provided care for the entire series. Number of days from the last day of one episode until the first
day of the next episodeday of the next episode.
“Adjacent” means that there was no gap between Medicare-covered episodes of more than 60 days.
Periods of time when the patient is "outside" a Medicare payment episode but on service with a different payer -such as HMO, Medicaid, or private pay - are counted as
d h ti th f M digap days when counting the sequence of Medicare payment episodes.
M0110Guidance “Early” means the only episode OR the first or
second episode in a sequence of adjacent episodes.episodes.
“Later” means the third or later episode in a sequence of adjacent episodessequence of adjacent episodes.
Use the “UK - Unknown” response if the placement of this payment episode in the sequence ofof this payment episode in the sequence of adjacent episodes is unknown. For the purposes of assigning a case mix code to the episode, this will have the same effect as selecting the “Early”have the same effect as selecting the Early response.
E t “NA” if M di i i t b51
Enter “NA” if no Medicare case mix group is to be defined for this episode.
EpisodeTiming Medicare will automatically adjust episodes early-
>late or late->early (up or down)
Low utilization payment adjustment (LUPA ) episodes (less than 5 total visits) are counted.
E i d dj t if th t d b Episodes are adjacent if they were separated by no more than a 60-day period between claims.Medicare Advantage plans don’t count whenMedicare Advantage plans don t count when
considering episode timingWill count from day 60 without regard to anWill count from day 60 without regard to an
early DC in the previous episode, except in the case of a PEP.
52 In PEP cases, Medicare will count from the last
billable visit
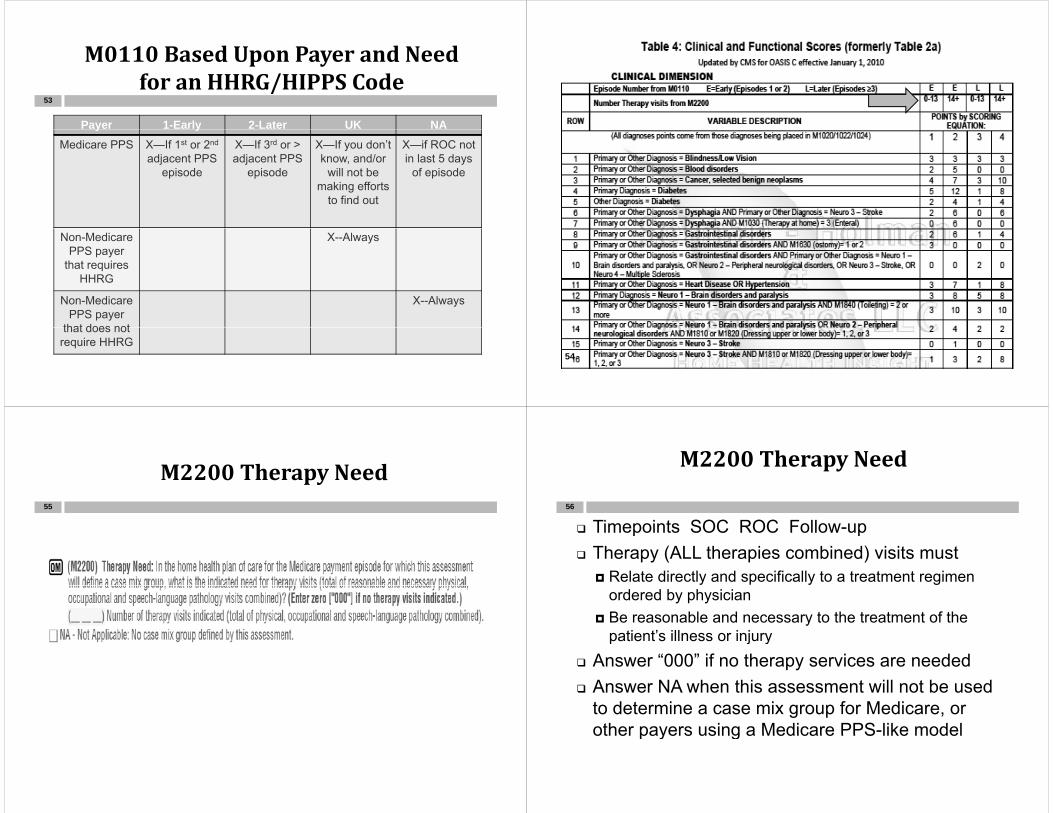
M0110BasedUponPayerandNeedfor an HHRG/HIPPS CodeforanHHRG/HIPPSCode
Payer 1-Early 2-Later UK NA
53
y yMedicare PPS X—If 1st or 2nd
adjacent PPS episode
X—If 3rd or > adjacent PPS
episode
X—If you don’t know, and/or
will not be
X—if ROC not in last 5 days
of episodemaking efforts
to find out
Non-Medicare PPS payer
that requires HHRG
X--Always
HHRG
Non-Medicare PPS payer
that does not
X--Always
that does not require HHRG
54
M2200TherapyNeed55
M2200TherapyNeed
Timepoints SOC ROC Follow-up56
p p Therapy (ALL therapies combined) visits must
Relate directly and specifically to a treatment regimen ordered by physician
Be reasonable and necessary to the treatment of the patient’s illness or injurypatient s illness or injury
Answer “000” if no therapy services are neededAnswer NA when this assessment will not be used Answer NA when this assessment will not be used to determine a case mix group for Medicare, or other payers using a Medicare PPS-like modelother payers using a Medicare PPS like model

M2200TherapyNeed
How many combined therapy visits?
57
How many combined therapy visits? Social work does not count as a therapy
If therapy services are ordered how many total If therapy services are ordered, how many total visits are indicated over the 60-day payment episode?episode?
If number is uncertain, provide best estimate.
M2200
In responding to M2200 Therapy Need In responding to M2200, Therapy Need, if a physician provides a specific order for therapy services and the therapist py pwho performs the evaluation does not feel the patient will require that number of visits, should the response for M2200 be the physician-ordered number of i it th th i t’ l ti f thvisits or the therapist’s evaluation of the
patient’s therapy needs?4b Q171 11 4b-Q171.11
M2200
M2200 should reflect the total number of M2200 should reflect the total number of reasonable and necessary therapy visits (e.g. therapy visits that meet the Medicare home health coverage criteria) that the agency plans to provide during the payment episode even if that number is less thanepisode, even if that number is less than the physician's orders. It would be important for the therapist to includeimportant for the therapist to include documentation of the number of covered therapy visits in the clinical documentation.py
M2200TherapyNeed
Medicare will adjust both up and60
Medicare will adjust both up and down based on the actual number of visits provided.visits provided.
ExampleYou believe patient needs 6 therapyYou believe patient needs 6 therapy
visits at the beginning of episode. You are paid RAP based on 6 therapy visits.are paid RAP based on 6 therapy visits. Patient falls in episode and ends up with 16 visits. You will be paid final claim pbased on 16 visits.

HowtoAnswerROC
ROC in the last 5 days of the episode61
y pAnswer based on estimated need for
therapy in the next episode. ROC any other time in the episode
Answer any way you’d like (doesn’t impact payment)payment).Number of therapy visits in episodeNumber of therapy visits left to do pyNA—No HHRG is needed (dependent on
software)000000
4b-Q171.10
WhatifM0110andM2200arewrong?wrong?
No action required62
No action required. Claims will automatically be adjusted so
CMS expects no extraordinary efforts toCMS expects no extraordinary efforts to be taken after SOC, ROC or Follow up to ensure M0110 or M2200 is correctensure M0110 or M2200 is correct.
Follow-up assessment is only required if your policy requires (Is it a major declineyour policy requires (Is it a major decline or improvement in the patient’s condition?)condition?)
4b-Q23.18
ExampleExamplePatient in early episode with 12 therapy
63
y p pyvisits with CHF, diabetes (takes insulin), blindness and is recovering from gall bladder s rger (no f ll epitheliali ationbladder surgery (no full epithelializationyet)has the following scores on OASIS data itemsdata items
M1200 = 2 M1810/1820 = 1M1242 = 2 M1830 = 2M1242 2 M1830 2M1342 = 3 M1840 = 2M1400 = 2 M1850 = 2M1400 2 M1850 2M2030 = 1 M1860 = 2
Non‐routine supplies (NRS)Non routinesupplies(NRS)
Gets its own points system based on64
Gets its own points system based on certain OASIS questions and diagnosesdiagnoses
6 non-routine supply levelsS-X supplies providedS X supplies provided1-6 supplies not provided
Are required to bill suppliesq ppRevenue code 0270 or 0623Charges, not cost

Assessment Data CollectionCollection
65
TheHow,Who,What&WhenofOASIS‐C:OASIS C:
thePatients,h h dtheCoPs,theTimepointsand
theConventions
OASIS TimepointsOASISTimepoints
All OASIS comprehensive assessments 67
prequire an actual visit to the patient’s home and may not rely on a telephone interview with the patient caregiver or other healthwith the patient, caregiver or other health care providers.
The only exceptions to the requirement for being “in the physical presence of the
ti t” th OASIS d t id d fpatient” are the OASIS data provided for TRN and Death at home (RFA 6, 7 and 8).
OASISisrequiredif:
OASIS is required if 68
qMedicare and/or Medicaid is payerYes, required on Medicaid skilled patients!
Any patient answered as 1-4 on M0150Any patient answered as 1-4 on M0150OASIS is not required if: Private pay or insurance (any other payer Private pay or insurance (any other payer
besides Medicare and Medicaid) Maternity (unless Medicare is payor)
P di t i ( l M di i ) Pediatric (unless Medicare is payor) Personal care Housekeeping and chore services Housekeeping and chore services Single visit quality episodes 1-Q1
If OASIS is not required:IfOASISisnotrequired:HHAs must provide each patient, regardless of payment
69
source, with a patient-specific comprehensive assessment that accurately reflects the patient’s current health status. The comprehensive assessment
t l id tif th ti t’ ti i d fmust also identify the patient’s continuing need for home care, medical, nursing, rehab, social and discharge planning needs.Only exception is housekeeping and chore services
Comprehensive assessment includes drug regimen review.review.
HHAs may continue to collect OASIS data on non-Medicare/non-Medicaid patients for agency use, BUT do not transmit the infodo not transmit the info.
Who can collect OASIS data?WhocancollectOASISdata?
Qualified clinicians70
Qualified clinicians RN PT ST OT (but not on SOC)
Who CANNOT collect OASIS? SW
LVN/LPN LVN/LPN PTA OTA OTA And of course, HHAs
The Conditions of ParticipationTheConditionsofParticipation42CFR484.55
71
TheCoPs—ComprehensiveAssessmentp
Initial assessment visit72
Initial assessment visitCompletion of the comprehensive
assessmentDrug regimen reviewug eg e e eUpdate of the comprehensive
assessmentassessment Incorporation of the OASIS data set42 CFR 484.55 CoPs OASIS

OASISdataitemsarenotmeanttobeacomprehensive assessmentcomprehensiveassessment
Not meant to be a complete assessment73
Not meant to be a complete assessment by themselves
Integrate the OASIS data items into your own comprehensive assessment and throw the redundancy out
+ + =OASIS Data Items
Agency Core Items
Discipline Specific
Items
Comprehensive Assessment
Items Items Items
IncorporationofOASISDataItems74
EXACTLY AS WRITTENL d i i t i dLanguage and groupings maintained
Clinically meaningful arrangementy g gSkip patterns must be right (and they
change sometimes depending on thechange sometimes depending on the time point)
DrugRegimenReview
Required at every comprehensive assessment75
M2000 Drug Regimen Review SOC/ROC M2002 Medication Follow-up TRN/DC M2010 Medication Intervention SOC/ROC M2010 Medication Intervention SOC/ROC M2015 Patient Caregiver Drug Education Intervention
TRN/DCA i f ALL di ti th t i tl i i A review of ALL medications the pt is currently using in order to identify any potential adverse effects and drug reactions, including ineffective drug therapy, significant side effects significant drug interactions duplicate drugside effects, significant drug interactions, duplicate drug therapy, and noncompliance with drug therapy.
This requirement applies to all pts being serviced by the HHA regardless of whether the specific requirements ofHHA, regardless of whether the specific requirements of OASIS apply.
InitialAssessment
Determines immediate care needs76
Determines immediate care needs and homebound status
Must be conducted eitherWithin 48 hours of referralWithin 48 hours of return homePhysician-ordered SOC datePhysician ordered SOC date
InitialAssessment
Must be conducted by RN unless77
Must be conducted by RN, unless therapy only case
If therapy only If therapy only Appropriate therapist may perform
initial assessmentinitial assessment OT may only complete assessment if
need for OT establishes programneed for OT establishes program eligibility (cannot perform a SOC on a Medicare patient)Medicare patient)
ComprehensiveAssessment
Completed in timely manner78
Completed in timely mannerConsistent with patient’s immediate needsNo later than 5 days after SOC (SOC dateNo later than 5 days after SOC (SOC date
is day 0) RN only unless therapy only case RN only unless therapy only case May perform initial assessment and comprehensive
assessment on same visit or on different visits If no skilled service is delivered, the visit is not the
SOC or reimbursable ( will not be accepted by HAVEN as SOC)
SOCDeterminationformulti‐disciplinary casesdisciplinarycases
In multidiscipline cases regulatory requirements
79
In multidiscipline cases, regulatory requirements (such as the CoPs) and agency policy will establish which discipline’s visit is considered the SOC. A reimbursable service must be delivered to bereimbursable service must be delivered to be considered the start of care for Medicare patients.
For Medicare reimbursement (42CFR409.46), a ( )physician must specifically order that a particular skilled service be furnished during the evaluation in which the agency accepts the beneficiary for g y p ytreatment and all other coverage criteria must be met for this visit to be billable as a skilled nursing visit.visit.
Q My agency has a nurse conduct a comprehensiveQ. My agency has a nurse conduct a comprehensive assessment before the therapist begins a therapy-only case. Thus, the nurse’s assessment is done before the start of careassessment is done before the start of care date. Can we continue this practice?
A. The “from” date on the initial certification is the first billable visit (which is the therapist’s visit). The comprehensive assessment performed prior to the therapist’s visit is non-compliant. Theto the therapist s visit is non compliant. The agency sending a clinician to the client’s home to provide a non-billable service does not establish the SOCestablish the SOC.
There is a solution…………………………2-Q12-12.1
80

If the agency chooses to have an RN conduct the If the agency chooses to have an RN conduct the comprehensive assessment, the RN should perform an assessment on or after the therapist’sperform an assessment on or after the therapist s SOC date (within 5 days to be compliant with the regulation.
2-Q12-12.1
Any comprehensive assessment info collected prior to the SOC date may not contribute to theprior to the SOC date may not contribute to the SOC comprehensive assessment.
2-Q36.1
81
Whatmakesavisitskilledorbillable?billable?
Therapy—the evaluation itself is billable82
Therapy—the evaluation itself is billable Nursing—the assessment is not billable What makes nursing skilled? What makes nursing skilled?
Intermittent—medically recurring need What’s the fix?
Th d h i i i l iTherapy does the initial assessment prior to, or on the same day as, the nurse completes OASIS.p
If therapy does initial assessment, must get consent signed
Nursing established the start of care with aNursing established the start of care with a truly billable visit.
Whocanconducttheassessment?83
If the RN’s entry in the case is known at SOC (i.e. the nursing is scheduled even if only for one visit)if only for one visit) then the case is NOT therapy-only, and the
RN should conduct the SOC assessment. If th d f th RN i t k t If the order for the RN is not known at SOC and originates from a verbal order after SOC, a te SOC, then the case is therapy only at SOC, and the
therapist can perform the SOC comprehensive assessment.comprehensive assessment.
2-Q10
TherapyOnly???
For skilled PT or SLP to perform the start of84
For skilled PT or SLP to perform the start of care visit for a Medicare patient: the HHA is expected to have orders from the
patient’s physician indicating the need for physical therapy or SLP prior to the initial assessment visit;assessment visit;
no orders are present for nursing at the start of care;
a reimbursable service must be provided; and the need for this service establishes program
eligibilit for the Medicare home health benefiteligibility for the Medicare home health benefit (42 CFR 484.55(a)(2).

Whocanconducttheassessment?
If therapy and aides are ordered:85
If therapy and aides are ordered:Because this is considered a therapy-
l (i th i th l kill donly case (i.e. therapy is the only skilled service), the PT or ST could perform the comprehensi e assessment and allcomprehensive assessment and all subsequent assessmentsRN i i i bill blRN supervisory visits are not billable visits
2-Q11
Who Can Start First?WhoCanStartFirst?
If PT and HHA are ordered—who can start86
If PT and HHA are ordered who can start first?
The aide’s visit is a reimbursable visitThe aide s visit is a reimbursable visit.Registered nurse does a non-billable initial
assessment visit to establish needs andassessment visit to establish needs and eligibility for a therapy only patient and sets up the aide care plan.sets up the aide care plan.
The aide visits the same day as the RN.Do we now have a SOC date?Do we now have a SOC date?2-Q48
Comprehensiveassessmentmustbe updated and revisedbeupdatedandrevised
Not less frequently than the last 5 days87
Not less frequently than the last 5 days of every 60 day episode beginning with the SOC date (days 56-60) (Follow-Up)( y ) ( p)
Major decline or improvement in condition (Other Follow-Up)
Within 48 hours of patient’s return home from an inpatient facility admission of 24 hours or more for reasons other thanhours or more for reasons other than diagnostic tests (ROC)
At discharge (DC) At discharge (DC)
UpdateoftheComprehensiveAssessmentAssessment
88
Any “qualified skilled” discipline may perform the updates, e.g. the nurse does
t h t f th t d thnot have to perform the recert and the discharge just because the RN had to do the admissionthe admission.
RN, PT and OT are ordered at SOC PT and OT are continuing into the next PT and OT are continuing into the next
episode OT continuing into the next episode OT continuing into the next episode What about SLP? 2-Q12.2
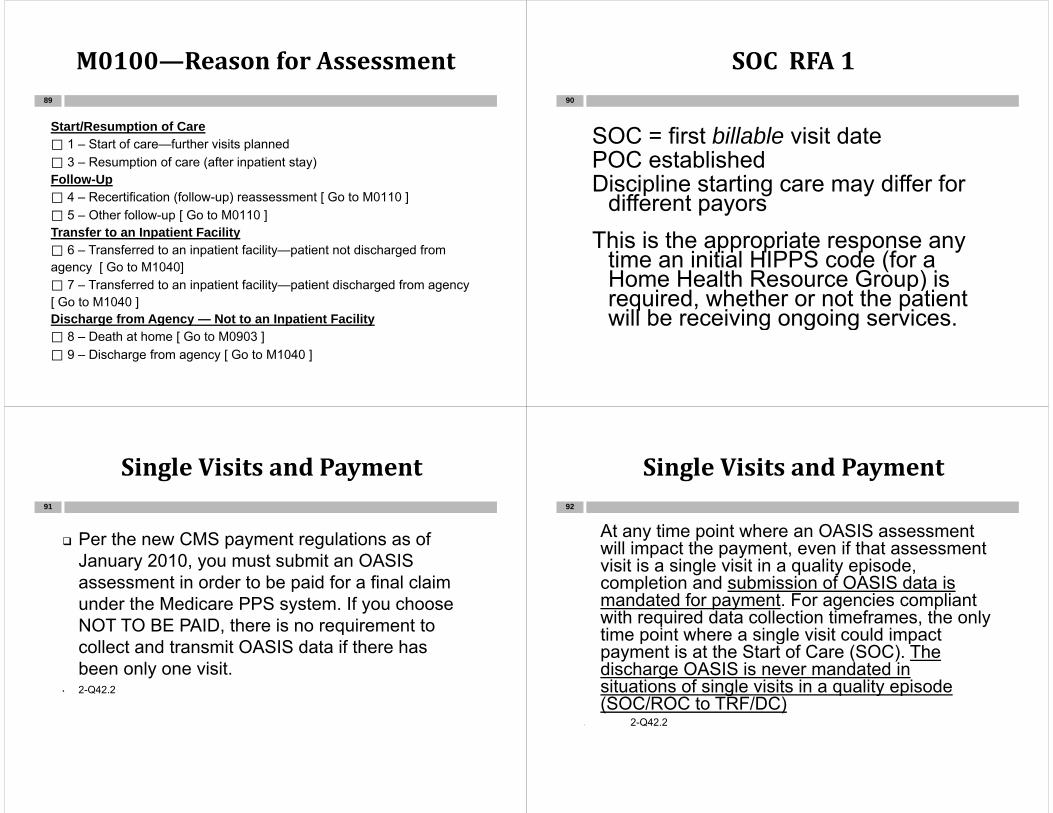
M0100—ReasonforAssessment
Start/Resumption of Care
89
Start/Resumption of Care ⃞ 1 – Start of care—further visits planned ⃞ 3 – Resumption of care (after inpatient stay) Follow UpFollow-Up ⃞ 4 – Recertification (follow-up) reassessment [ Go to M0110 ] ⃞ 5 – Other follow-up [ Go to M0110 ] T f t I ti t F ilitTransfer to an Inpatient Facility ⃞ 6 – Transferred to an inpatient facility—patient not discharged from agency [ Go to M1040] ⃞ 7 – Transferred to an inpatient facility—patient discharged from agency [ Go to M1040 ] Discharge from Agency — Not to an Inpatient Facility ⃞ 8 – Death at home [ Go to M0903 ] ⃞ 9 – Discharge from agency [ Go to M1040 ]
SOCRFA1
SOC fi t bill bl i it d t
90
SOC = first billable visit datePOC establishedDi i li t ti diff fDiscipline starting care may differ for
different payorsThis is the appropriate response any
time an initial HIPPS code (for a Home Health Resource Group) isHome Health Resource Group) is required, whether or not the patient will be receiving ongoing services.g g g
SingleVisitsandPayment
Per the ne CMS pa ment reg lations as of
91
Per the new CMS payment regulations as of January 2010, you must submit an OASIS assessment in order to be paid for a final claimassessment in order to be paid for a final claim under the Medicare PPS system. If you choose NOT TO BE PAID, there is no requirement to qcollect and transmit OASIS data if there has been only one visit.
• 2-Q42.2
SingleVisitsandPayment
At any time point where an OASIS assessment92
At any time point where an OASIS assessment will impact the payment, even if that assessment visit is a single visit in a quality episode, completion and submission of OASIS data iscompletion and submission of OASIS data is mandated for payment. For agencies compliant with required data collection timeframes, the only time point where a single visit could impacttime point where a single visit could impact payment is at the Start of Care (SOC). The discharge OASIS is never mandated in situations of single visits in a quality episodesituations of single visits in a quality episode (SOC/ROC to TRF/DC)
• 2-Q42.2

Whatifjustonevisit?
The patient is admitted to home care (single visit 93
p ( gis made) and then the patient refuses any further visits, is an OASIS required?
The agency is not required to assess the OASISThe agency is not required to assess the OASIS items, nor encode and submit their assessment (as of 12/2003). The comprehensive assessment would be placed in the medicalassessment would be placed in the medical record.
HOWEVER, you cannot bill without an HHRG.If you want to be paid for that single visit, you
must collect, encode and submit the assessmentassessment.
What if just one visit?Whatifjustonevisit?
What if you’ve already completed OASIS94
What if you ve already completed OASIS (SOC or ROC), encoded and/or transmitted, and then no further visits are made?
Conduct no further assessments.D t th t f th i it d Document that no further visits occurred.
Patient’s name will appear on data system for 6 monthsfor 6 months
If patient is readmitted, there will be a warning that OASIS is out of sequence but g qwill not prevent OASIS from being transmitted
Whathappensif…..pp
During the SOC assessment the patient has dyspnea
95
During the SOC assessment the patient has dyspneaand has to be transferred to the hospital before the entire admission process is completed? If skilled care was provided and eligibility was If skilled care was provided and eligibility was
established and the patient is not admitted to the facility, then the clinician still has five days after the SOC to complete the assessment. Has to be the same clinician.
Answers can be changed after the patientAnswers can be changed after the patient returns from the facility to reflect new condition
2-Q17.1
Whathappensif…
The patient is admitted to the facility?96
The patient is admitted to the facility?You must start over when the patient
is discharged with a new SOC assessment.

ExampleandRamifications
SOC completed and then patient97
SOC completed and then patient transferred into hospital—instruction is to readmit. If a TRN was done instead, then you are stuck
with an acute hospitalization when you didn’t have a chance to even try to prevent thehave a chance to even try to prevent the hospitalization.
If a TRN was done instead, you are stuck with , ythe original HHRG after the hospitalization (no opportunity for billing a SCIC)
This is only true if ONE visit is made!This is only true if ONE visit is made!
EvenNon‐BillableVisitCounts
If nursing performs a non-billable admit for a PT 98
g ponly case, the PT goes the same day completing an evaluation only, and there is no further need for therapy, are we required to py, qcomplete the RFA 9 OASIS Discharge?
For skilled Medicare and skilled Medicaid patients OASIS data collection is required ifpatients, OASIS data collection is required if more than one visit was made in a quality episode. In your scenario, the nurse made one visit and the PT made one visit Therefore bothvisit and the PT made one visit. Therefore both the SOC (RFA 1) and DC (RFA 9) comprehensive assessments are required. This i t if f th i it bill blis true even if one of the visits was non-billable.
2-Q42.1-42.1.1
M0100 RFA 3 ROCM0100RFA3ROC99
Following an inpatient stay of 24 hours or llonger
For reasons other than diagnostic testsN d t d t th P ti t T ki Sh t fNeed to update the Patient Tracking Sheet for the most recent ROC date
ROC date not necessarily the dateROC date not necessarily the date assessment is done
ROCClarification—NoOrdertoReturn to Home is RequiredReturntoHomeisRequired
CMS advised that when the patient 100
preturns home:
Home health services are resumed; The patient is reassessed; The orders for services are reviewed and
reestablished from that point forward; and A b l d d ti th d f A verbal order updating the orders for services and frequency of services must be obtained NAHC Report Nov 12 2009be obtained. NAHC Report Nov 12, 2009
2-Q18

RFA3ResumptionofCare
If the patient returns home from an101
If the patient returns home from an inpatient stay during the last 5 days
f th i dof the episodeComplete ROC, not Follow-UpWill determine the case mix for the
subsequent episode so answer M2200 and M0110 accordingly
Returns home on day 54…what now?y3-Q5
ResumptionofCare
Can the RN do the ROC on a therapy102
Can the RN do the ROC on a therapy only case before the therapist visits?The ROC assessment must beThe ROC assessment must be
performed within 48 hours of the patient’s return home after an inpatient p pfacility stay.Before or after the therapist visit.pROC date (M0032) is the first visit,
regardless who makes it, or whether or g ,not it is billable. 2-Q51.2
M0100RFA4Recertification&RFA 5 Other Follow UpRFA5OtherFollow‐Up
103
Days 56-60 (Follow Up aka Recertification)Recertification)
Due to a major decline or improvement i ti t diti (Oth F llin patient condition (Other Follow-Up) Updates the patient’s plan of care Your policy dictates when you have to
do another assessment
M0100 RFA 4 RecertificationM0100RFA4Recertification
If Days 56-60 are missed do not DC and104
If Days 56 60 are missed, do not DC and readmit. M0090 is the date assessment is doneM0090 is the date assessment is done Include in clinical documentation reason late
Will t iWill get a warning messageLegal considerations!!Example: Start of episode is October 15 Recert shouldExample: Start of episode is October 15. Recert should
have been done Oct 10-14, but due to error was not performed until October 18. M0090 is 10-18, but SOE p ,is still October 15.
3-Q11
Situation
The patient is admitted to the hospital105
The patient is admitted to the hospital before or during the recert window, in an inpatient bed more than 24 hoursan inpatient bed more than 24 hours but only for diagnostic purposes, then comes home on day 61comes home on day 61…
Treat this situation as a missed recertification and complete therecertification, and complete the Recert asap. Oct 2012
MissedtheRecertand Decided to DCandDecidedtoDC
If there was a need for continuing services into the ifi i i d b h li i i i dnext certification period, but the clinician missed
completing the recertification assessment between day 56-60 and on the first visit in the new episode it was determined the patient had reached goals andwas determined the patient had reached goals and needed to be discharged, do I have to complete both the Recert and the Discharge OASIS?Y Wh R tifi ti t i i d it Yes. When a Recertification assessment is missed it should be completed as soon as possible.
If the clinician determined the patient was ready for di h th fi t i it i th i d thdischarge on the first visit in the new episode, the Discharge comprehensive assessment is also required. The discharge is the endpoint of the quality episode which is not captured with a recertificationepisode, which is not captured with a recertification assessment. 3Q11.1
M0100 RFA 4 RecertificationM0100RFA4Recertification
Wh if d l ?
107
What if done too early?Do it over within the right timepoints.
E if i t th t i d hEven if into the next episode when you figure it out. 3-Q11.2
A clinician may start the comprehensive A clinician may start the comprehensive assessment on day 56 and complete it on any day on or before day 60. Only one clinician may complete though, so if Nurse A begins, then Nurse A must complete 3 Q5 1complete. 3-Q5.1
RFA6TransfertoInpatientFacility Not DischargedFacility–NotDischarged
Admission of 24 hours or longer
108
Admission of 24 hours or longer
Reasons other than diagnostic tests Reasons other than diagnostic tests
Patient expected to resume carep
Does not require a home visit
If patient does not return, a DC visit/OASIS is not required (a DC summary is required)not required (a DC summary is required)

RFA7TransfertoInpatientFacility DischargedFacility–Discharged
109
Admission of 24 hours or longer
Reasons other than diagnostic tests
Is not expected to return to home care or does not return by the end of the episodedoes not return by the end of the episode
D t i h i it Does not require a home visit
RFA6vs.RFA7
If the HHA plans on the patient returning after
110
If the HHA plans on the patient returning after their inpatient stay, the RFA6 should be completed.
There will be times when the RFA7 is necessary to use, but only when the HHA does NOT anticipate the patient will be returning to care 2 Q3anticipate the patient will be returning to care. 2-Q3
Providers should not discharge (use RFA 7) when goals have not been met at transfer. 2-Q3g Q
What if we complete a 6 and the patient does not return? No need to cancel—will be on data
fsystem for 6 months.
Do we have to complete an OASIS D/C on a ptDo we have to complete an OASIS D/C on a pt who has been hospitalized over a specific time period?
The agency will choose one of two responses to OASIS item M0100 when a pt is transferred to anOASIS item M0100 when a pt is transferred to an inpatient facility for a 24-hr (or longer) stay for any reason other than for diagnostic testing:
M0100 6 T f t I ti t F ilitM0100=6 - Transfer to an Inpatient Facility--patient not discharged from agency; or
M0100=7 - Transfer to an Inpatient Facility—M0100 7 Transfer to an Inpatient Facilitypatient discharged from agency.
111
Whatisconsideredadiagnostic test?diagnostictest?
112
Tests, scans and procedures utilized to yield a diagnosisto yield a diagnosisX-rays, UGI, CT scansCardiac catheterization?Cardiac catheterization?
Requires that each case be considered individuallyy

Whatisanadmission?
In order to qualify for the Transfer to Inpatient113
In order to qualify for the Transfer to Inpatient Facility OASIS assessment timepoint, the patient must meet 3 criteria:p , p1) Be admitted to the inpatient facility (not the ER,
not an observation bed in the ER)2) Reside as an inpatient for 24 hours or longer
(does not include time spent in the ER)3) Be admitted for reasons other than diagnostic3) Be admitted for reasons other than diagnostic
testing onlyAn admission to an inpatient facility for observation p y
is not an admission for diagnostic testing only. This is considered a hospitalization. 4-Q23.7
Quiz
Patient is transported to hospital and114
Patient is transported to hospital and is placed on observation on June 26. O J 28 h i d i dOn June 28, he is admitted as an inpatient. What is the transfer date? What is M0090 date on the transfer?June 28 is transfer dateJune 28 is transfer dateM0090 date is June 29 or within 48
hours of transferhours of transfer
Quiz
You make a routine visit and discover the115
You make a routine visit and discover the patient was in the hospital for two days earlier in the week. You find that it was a qualifying stay in an inpatient facility.
Within 2 calendar days of knowledge of y gtransferComplete the RFA 6 (TRN) and the RFA 3 p ( )
(ROC) True or False?
M0100RFA8Deathathome
Complete Death at home while still under116
Complete Death at home while still under the care of the agencyAt homeWhile in route to or before treatment in an ERBefore inpatient admission (pronounced DOA)
Exception--Complete transfer assessment INSTEAD, if
f f ( )Death while under care of facility (in ER)Regardless of length of time in the facility2-Q222 Q22

M0100 RFA 9 DischargeM0100RFA9Discharge
Not due to an inpatient facility admission117
Not due to an inpatient facility admission Not due to death at home
Vi i i i d l h Visit is required to complete the assessment Except in cases of unexpected discharge
Unplanned or unexpected dischargesp p gAssessment must report patient status at an
actual visitLast visit conducted by a qualified clinician
UnplannedorUnexpectedDischarges
Who can complete the DC OASIS?118
Who can complete the DC OASIS? Last qualified clinician that visited the
patient should complete the DCpatient should complete the DC comprehensive assessmentHow do you show that you completed the
OASIS without a visit? (“based on visit of /dd/ ”)mm/dd/yyyy”)
Complete the OASIS based on information il bl t th l t lifi d li i i ’ i itavailable at the last qualified clinician’s visit
UnplannedorUnexpectedDischarges
Wh t if th l t lifi d li i i i
119
What if the last qualified clinician is no longer available?DC matches the SOC ORDo not complete the DC OASIS (CoP
problem)A supervisor in the office cannot p
create an assessment as if it were fact without seeing the patient.g p2-Q37
UnplannedorUnexpectedDischargesDischarges
D t i l d t th t
120
Do not include any events that occurred after the last qualified clinician’s visit.Include the ER visit that occurred after c ude t e s t t at occu ed a te
the last qualified clinician’s visit??Consider that all the teaching aboutConsider that all the teaching about
heart failure symptoms occurred since the last qualified clinician’s visit??the last qualified clinician s visit??
Quiz:Whichsequencesofassessments are correct?assessmentsarecorrect?
121
1. SOC, with only one visit performed2. SOC, FU, Transfer, Discharge3 SOC FU FU FU DC3. SOC, FU, FU, FU, DC4. SOC, FU, Transfer5. SOC, ROC, FU, DC
General OASIS ItemGeneralOASISItemConventions
122
GeneralOASISItemConventions123
Understand the time period under consideration for each item.
Report what is true on the day of assessmentNote: Specific item guidance--a differentNote: Specific item guidance a different
time period may be indicated Day of assessment is defined as the 24 hours Day of assessment is defined as the 24 hours
immediately preceding the home visit and the time spent by the clinician in the home p y
GeneralOASISItemConventions
If the patient’s ability or status varies on the day of th t t th ti t’ ‘ l t t ’
124
the assessment report the patient’s ‘usual status’ or what is true greater than 50% of the assessment time frametime frame
Unless the item specifies differently such as: M2020 Management of Oral Meds M2030 Management of Injectable Meds M2100e Management of Equipment
Instead of ‘usual status’ or greater than 50%Instead of usual status or greater than 50% of the time,’ consider the medication or equipment for which the most q passistance is needed.

GeneralOASISItemConventions
Minimize the use of NA and Unknown responses
125
Minimize the use of NA and Unknown responses Documentation of a patient’s current status should
be based on independent observation Of the patient’s condition and ability at the time of
the assessment Without referring back to prior assessments Without referring back to prior assessments
(unless collection of the item includes review of the care episode, e.g. process items).
C bi b ti i t i d th l t Combine observation, interview, and other relevant strategies to complete OASIS data items as needed
When assessing physiologic or functional health When assessing physiologic or functional health status, direct observation is the preferred strategy.
GeneralOASISItemConventions
Data collection for items that state ‘since
126
Data collection for items that state since the previous OASIS assessment’ will Require review of the episodeRequire review of the episodeThe ‘review period’ begins from the time of
the last OASIS assessmentthe last OASIS assessment These instructions are included in item
guidance for the relevant OASIS questions.guidance for the relevant OASIS questions. “since the previous OASIS assessment"
should be interpreted to mean "at or sinceshould be interpreted to mean at or since the time of the last OASIS assessment."
GeneralOASISItemConventions127
When an OASIS item refers to assistance, this means assistance from another person (or more than one person) unless otherwise specified within the itemAssistance is not limited to physical contact
and includes both verbal cues and supervisionsupervision
Complete OASIS items accurately and comprehensively and adhere to skipcomprehensively, and adhere to skip patterns
GeneralOASISItemConventions
Understand what tasks are included and excluded128
Understand what tasks are included and excludedScore item based only on what is included
Consider medical restrictions when determining gability and selecting responseActivity restrictions should be considered e.g.,
functional items related to ambulation, transferring, etc.
Understand the definitions of words as used in the Understand the definitions of words as used in the OASIS
Follow rules included in the Item Specific Follow rules included in the Item Specific Guidance

GeneralOASISItemConventions129
Stay current with evolving CMS OASIS guidance updates
One clinician takes responsibility for accurately completing a comprehensive y gassessmentSelected items allow for collaboration e.g.,
Medication items M2000-M2004These exceptions are noted in the Item
S ifi G idSpecific Guidance.
Definitions to NoteDefinitionstoNote
One calendar day = Until the end of the next130
One calendar day Until the end of the next calendar day (e.g., M2002 Medications Follow-Up)
Same day = same daySa e day sa e day i.e., = ‘only in these circumstances’ or ‘that is’
Scoring of the item should be limited to theScoring of the item should be limited to the examples listed
e.g., = ‘for example’ e g , o e a p eThe clinician may consider other relevant
examples when scoring this item p g
Patient Tracking Sheet M0010‐M0150;PatientTrackingSheetM0010 M0150;ClinicalRecordItemsM0080 M0110M0080‐M0110
PatientTrackingSheet
This is information that doesn’tThis is information that doesn t usually change from one episode to
hanother.Paperwork Reduction—Medicare p
requires that we complete this at SOC and then review for neededSOC and then review for needed changes at other timepoints.

PatientTrackingSheet
M0010-M0030—Agency Information and g ythe agency assigned Patient ID
M0030—Start of Care M0032—Resumption of Care M0040-M0060—Patient Information M0063-M0140—Demographics M0150-Current Payment Sourcesy Some of this info can be completed by
clerical as long as assessing clinician ifiverifies. 4b-Q3
M0150CurrentPaymentSourcesFor Home CareForHomeCare
M0150CurrentPaymentSources
Just consider any services on theJust consider any services on the POC that will be billed by your home
i i thcare agency in answering the question.
Do not consider any equipmentDo not consider any equipment, medications, or supplies being paid for by the patient in part or in fullfor by the patient, in part or in full.
M0150CurrentPaymentSources
A Medicare patient is referred for home health but it is determined that h i t h b d Th ti the is not homebound. The patient agrees to pay privately. Should M0150 be answered ‘1’ and ‘10’?M0150 be answered 1 and 10 ? 4b-Q27
No. Medicare is not a payor. If at a future date his condition changes andfuture date his condition changes and he becomes homebound a new SOC is requiredis required.

MEDICAREasPayor
If the payor is Medicare as primary or p y p ysecondary payor then Medicare must be checked
Do you want to check Medicare anytime Medicare MAY pay for the services? 4b-Q29.5
If th h t M di th If the payor changes to Medicare, there must be a new SOC date.
If the payor changes from Medicare to If the payor changes from Medicare, to another payor, just change M0150 on the next OASIS timepoint, unless the payorp , p yhas other requirements. 4b-Q28
Clinical Record ItemsClinicalRecordItemsM0080‐M0110
M0080DisciplineofPersonCompleting AssessmentCompletingAssessment
Referred to as Qualified Clinicians
M0080DisciplineofPersonCompleting AssessmentCompletingAssessment
Discipline completing the Discipline completing the comprehensive assessment at an actual home visit ORactual home visit OR
The clinician reporting the transfer t th i ti t f ilit d th tto the inpatient facility or death at home.
Only one individual completes the assessment, even when collaboration and coordination is needed.

M0090DateAssessmentCompleted
Does not have to coincide with a visitDoes not have to coincide with a visitWill not coincide with a visit at
transfertransferWill probably not coincide with a visit
ith D th t Hwith Death at HomeMay not coincide with a visit
considering the best practices in OASIS C.
M0090 info at 4bQ14-19.5
M0090DateAssessmentCompletedCompleted
The patient is admitted with a billable visit on The patient is admitted with a billable visit on Oct 15. The surgical wound has a dressing that is not to be removed until the physician’s appt on Oct 18. The RN returns on Oct 19, assesses the wound and is able to answer M1342, Status
f S i l W d Wh t i th M0090 d t ?of Surgical Wound. What is the M0090 date? The patient was transported to the hospital on
1/25 and was placed on observation She was1/25 and was placed on observation. She was admitted as an inpatient on 1/26. What is the date of transfer (M0903) What is your M0090date of transfer (M0903) What is your M0090 date on the transfer? 4b-Q191.1
M0102DateofPhysician‐orderedSOC/ROC; M0104 Date of ReferralSOC/ROC;M0104DateofReferral
M0102DateofPhysician‐orderedSOC/ROCSOC/ROC
Timepoints—SOC/ROC If the original order for SOC (ROC) is delayed due to the
patient’s condition or physician request then the date specified on the updated/revised order to start home p pcare services would be considered the date of physician-ordered SOC (ROC).
FL23—Verbal SOC and Nurse’s Signature and Date--gThe RN or qualified therapist would indicate the date the verbal order was received and/or the date the plan of care was reviewed and signed by the RN. Note: This fi ld b d th b l d t ith b ifield may be used as the verbal order to either begin services or to recertify services and will cover the services being rendered until the physician signs and dates the POC prior to billing the final claim to thedates the POC prior to billing the final claim to the intermediary.
No ranges

M0104DateofReferral
Most recent date that verbal, written, or , ,electronic authorization to begin home care was received.
If dates are revised, enter the most recent date.D t i l d d t ti d Does not include documentation and calls from others such as ALF staff or family Referral defined at 2-Q50family Referral defined at 2-Q50
Not the date authorization was received from the patient's payerp p y
Date received, not date processed. 10.2011
M0102/M0104
You discover that a patient’s insuranceYou discover that a patient s insurance changed months ago and the new payer requires a new SOC withpayer requires a new SOC with OASIS data. You will be performing OASIS data collection on JanuaryOASIS data collection on January 10th. You have orders for the care but not for a specific date and ofbut not for a specific date and, of course, you do not have a paper referral for that new episodereferral for that new episode.
4b-Q23.11.2
• What will you enter for the M0102 date?• N/A-No specific ordered SOC date
• Do you need to obtain a physician’s ordered SOC date or a referral date? • No, because you are not initiating care, just
changing payer source.• How will M0104 (Date of Referral) be answered ?
• Enter the day prior to the new SOC date—if you know the date the insurance is ychanging then actual dates can be used. 4b-Q23.11.2
I understand that the initial assessment visit (orI understand that the initial assessment visit (or Resumption of Care assessment) is to be done within 48 hours of the referral (or hospital ( pdischarge). What do we do if the patient puts us off longer than that? For example, the patient says, "I have an appointment today (Friday); please come Monday.“
C diti f P ti i ti i th t th ROCConditions of Participation require that the ROC assessment be performed within 48 hours of return home (no flexibility)return home (no flexibility).
2-Q18

ROCandM0102
There is no regulatory allowance for a physician-d d R i f C d d b d 2
149
ordered Resumption of Care date to extend beyond 2 calendar days of the facility discharge. If the physician orders the agency to resume care on a specific date that falls within 2 calendar days of the inpatient facilitythat falls within 2 calendar days of the inpatient facility discharge, the specific ROC date ordered by the physician should be reported in M0102 Date of Physician-ordered SOC/ROC If the physician ordersPhysician-ordered SOC/ROC. If the physician orders the agency to resume care on a specific date that extends beyond 2 calendar days of the inpatient facility discharge, "NA" would be selected for M0102,facility discharge, NA would be selected for M0102, Date of Physician-ordered SOC/ROC, and the date of the referral for resumption of home care services would be entered into M0104, Date of Referral. ,Clinical documentation would explain the timing of the patient's ROC visit. Oct 2012
Patient History and DiagnosesPatientHistoryandDiagnosesM1000‐M1055
M1000InpatientFacilities M1000InpatientFacilities
Timepoints SOC/ROCp Count 14 days back from the SOC or ROC date
(date of assessment is day zero) Exception for ROC in last 5 days of episode count Exception for ROC in last 5 days of episode—count
14 days back from first day of new episode 4b-Q32.1
DC that occurs on the day of assessment tcounts
If in Medicare certified SNF, but not paid by Part A, check Response 1A, check Response 1
SNF—Medicare certified, skilled care under Part A, during the past 14 days (also includes transitional care unit)transitional care unit)

M1000InpatientFacilities
Long term care hospital—average LOS Long term care hospital average LOS of greater than 25 days
ICF/MR is included in ‘other’ ICF/MR is included in otherALF is not a facility!
Swing bed—hospital SNF or nursing Swing bed—hospital, SNF or nursing home??
Access the CWF in determining the type Access the CWF in determining the type of inpatient services received and the date of inpatient facility dischargedate of inpatient facility discharge.
M1000InpatientFacilities
Our client was admitted to the hospitalOur client was admitted to the hospital for less than 24 hours and returned home. Two days later the patient was y pdischarged from the agency and a DC OASIS was done. Approximately 1 week later, the patient was readmitted to home care. On the new SOC assessment, how d k M1000? “3” h t t tdo we mark M1000? “3” short term acute hospital or “NA” Patient was not discharged from an inpatient facilitydischarged from an inpatient facility.
M1000InpatientFacilities
In the scenario the patient was In the scenario the patient was admitted and discharged from an i ti t f ilit ithi 14 d f thinpatient facility within 14 days of the SOC.
M1000 does not ask you to only report inpatient facility stays thatreport inpatient facility stays that meet the criteria for transfer.
4b-Q32.2
M1000InpatientFacilities
We keep getting patients who have been p g g pon observation in the hospital.
If the patient was admitted and put on observation, it is considered a hospital discharge.If th ti t l d d If the patient was placed under observation utilizing one of the two G-codes for hospital outpatient deptcodes for hospital outpatient dept observation, then it would not be considered a discharge. 4b-Q32.3

RegardingallCodingDataItems
The assessing clinician determines the primary g p yand secondary diagnoses and records the symptom control ratings. The clinician should write in the diagnoses and a coding specialist g g pmay enter the actual ICD-9 codes once the assessment is completed.
P and P should allow for correction or clarification P and P should allow for correction or clarification of records to meet professional standards. It is prudent to allow for a p and p that includes correction or completion of a clinical record in thecorrection or completion of a clinical record in the absence of the original clinician due to vacation, sick time or termination.
This applies to M1010, M1016 and M1020/1022/1024.
M1010InpatientDiagnosisActively Tx in Hospital!!!ActivelyTx inHospital!!!
M1010InpatientDiagnosis
Timepoints—SOC/ROC Timepoints SOC/ROC May or may not correspond with the hospital
admitting diagnosis.“A ti l t t d" h ld b d fi d i i “Actively treated" should be defined as receiving something more than the regularly scheduled medications and treatments necessary to ymaintain or treat an existing condition.
SOC is counted as day zero.No surgical V or E codes List the underlying No surgical, V or E codes. List the underlying diagnosis.
Not necessary to fill in every line if the patient y y phad fewer than six inpatient diagnoses.
M1012InpatientProcedure

M1012InpatientProcedures
CMS has determined that the data fromCMS has determined that the data from M1012 is not currently used for payment quality measure developmentpayment, quality measure development, or risk adjustment. Therefore, effective immediately any response reported forimmediately, any response reported for M1012 ("UK", "NA", or the reporting of procedures and codes) is acceptable toprocedures and codes) is acceptable to report, and the impact of the response is insignificant Note that at this time theinsignificant. Note that at this time, the item cannot be left blank. 4b-Q39.3
M1016DiagnosesRequiringMedicalorTreatmentRegimenChangeg g
M1016DiagnosesRequiringMedicalor Treatment Regimen ChangeorTreatmentRegimenChange
Timepoints SOC/ROC Changes that have occurred to the treatment regimen,
health care services or medications during the past 14health care services, or medications during the past 14 days. SOC/ROC is day zero.
No surgical, V or E codes—list underlying diagnosis.A h i i t f l t h b it lf i t A physician appt or referral to home care by itself is not a change in treatment regimen. 4b-Q40
Change occurring on day zero does count. Improvement doesn’t count. All treatments/disciplines ordered at SOC do not count
but any change to those treatments/disciplines duringbut any change to those treatments/disciplines during the episode do count as a change. 4b-Q42.2
N d M1020/1022/1024 HERE Need M1020/1022/1024 HERE

M1020/1022Diagnoses,SymptomControl,andPayment DiagnosesPaymentDiagnoses
Timepoints SOC/ROC/Follow-up Timepoints SOC/ROC/Follow up Medicare’s rules for coverage and payment Each patient’s overall medical condition and Each patient s overall medical condition and
care needs must be comprehensively assessed BEFORE the HHA identifies and assigns each gdiagnosis for which patient is receiving care.
No resolved conditions Skilled services are used in judging relevancy of
a diagnosis to the POC and to the OASIS
M1020/1022Diagnoses,SymptomControl,andPayment DiagnosesPaymentDiagnoses
M1020 Primary diagnosisM1020 Primary diagnosisDiagnosis most related to the POCMost acute diagnosisChief reason for providing home care
M1020/1022Diagnoses,SymptomControl,andPayment DiagnosesPaymentDiagnoses
M1022b-f Other diagnosesgEach diagnosis should be supported by
medical record documentation (POC)Not only conditions actively addressed but
also any co-morbidity affecting the patient’s responsiveness to treatment and rehabresponsiveness to treatment and rehab prognosis, even if the condition is not the focus of any home health treatment itself.A id li ti di th t fAvoid listing diagnoses that are of mere historical interest and without impact on patient progress or outcome.p p g
M1020/1022/1024Diagnoses,SymptomControl and Payment DiagnosesControl,andPaymentDiagnoses
Case mix diagnosis—diagnosis that gives a patient i f PPS i ipoints for PPS case-mix group assignment.
Avoid assigning excessive V codes to the OASIS. V codes are less specific to the clinical condition of V codes are less specific to the clinical condition of
the patient than are numeric diagnoses. V codes are appropriately assigned when a patient with a resolving disease or injury requires specific aftercare of that j y q pdisease or injury (i.e., surgical aftercare or aftercare for rehab).
Acute fracture codes are only to be used for the initial, y ,acute episode of care, which is why the acute fracture code is no longer appropriate once the patient has been discharged from the hospital to home health. Fracture code is placed in M1024.

M1020/1022Diagnoses,SymptomControl,andPayment DiagnosesPaymentDiagnoses
Rate the degree of symptom control for the condition listed in Column 1 using the following scale:using the following scale:
0 - Asymptomatic, no treatment needed at this time 1 - Symptoms well controlled with current therapy 2 S t t ll d ith diffi lt ff ti d il f ti i ti t2 - Symptoms controlled with difficulty, affecting daily functioning; patient
needs ongoing monitoring 3 - Symptoms poorly controlled; patient needs frequent adjustment in
treatment and dose monitoring g4 - Symptoms poorly controlled; history of re-hospitalizations Note that in Column 2 the rating for symptom control of each
diagnosis should not be used to determine the sequencing of th di li t d i C l 1 Th t it dthe diagnoses listed in Column 1. These are separate items and sequencing may not coincide. Sequencing of diagnoses should reflect the seriousness of each condition and support the disciplines and services provided.
M1020/1022Diagnoses,SymptomControl,andPayment DiagnosesPaymentDiagnoses
Assessing degree of symptom control g g y pincludes review of presenting signs and symptoms, type and number of medications frequency of treatmentmedications, frequency of treatment readjustments, and frequency of contact with health care provider.
Inquire about the degree to which each condition limits daily activities. Assess the patient to determine if symptoms arepatient to determine if symptoms are controlled by current treatments. Clarify which diagnoses/symptoms have been g y ppoorly controlled in the recent past.
M1024Diagnoses,SymptomControl,andPayment DiagnosesPaymentDiagnoses
Column 3: (OPTIONAL) If a V-code from category V54.1x ( ) g yor V54.2x is assigned to any row in Column 2, in place of a traumatic or pathological fracture code, place the fracture code in M1024 Column 3fracture code in M1024 Column 3
Column 4: No longer used since ONLY fracture codes are now placed in M1024 pNo resolved conditions in M1024No DM, Skin 1 or Neuro 1 conditions in M1024
For DM, Skin 1 or Neuro 1 diagnoses that would earn more case-mix points when primary, if a V-code replaces them in M1020 place the DM Skin 1 or Neuro 1 code inthem in M1020, place the DM, Skin 1 or Neuro 1 code in M1022b immediately under the V-code in M1020a.
M1020/1022Diagnoses,SymptomControl, and Payment DiagnosesControl,andPaymentDiagnoses
A t St t i Assessment Strategies Interview patient/caregiver to obtain past
health histor additional information mahealth history; additional information may be obtained from the physician.
Review current medications and otherReview current medications and other treatment approaches. Determine if add’ldiagnoses are suggested by current g gg ytreatment regimen, and verify this info with the patient/caregiver and physician.
Use the current ICD-9-CM guidelines.

M1024—Use1/1/13
1 Use M1024 when the V code1. Use M1024 when the V code replaces a fracture
2. Use M1022b when the V code as primary in M1020 replaces a Neuroy1, Skin 1 or diabetes case mix diagnosisdiagnosis
3. No longer place resolved conditions in M1024conditions in M1024
M1030Therapiesthepatientreceivesathomehome
M1030Therapiesthepatientreceivesat home:athome:
Timepoints SOC/ROC/Follow-upp p Is the patient receiving the therapy at home?
(whether or not the HHA is administering the therapy)therapy)
If the patient will be receiving the therapy as a result of this assessment, then mark the
li bl thapplicable therapy. Response 1 includes heparin and saline flushes,
hemodialysis or peritoneal dialysis at home,hemodialysis or peritoneal dialysis at home, intrathecal, epidural, subcutaneous (must be infusion, not injection), insulin pumps, pain pumps eclipse bulbspumps, eclipse bulbs
Irrigations/infusions of the bladder do NOT count.
M1030Therapiesthepatientreceivesat home:athome:
Do not select Response 1 if there are orders for infusion if parameters are met, but those are not met on the day ofbut those are not met on the day of assessment.Example—prn ordersp p
TPN and flush other lumens—mark all that applyR 3 t iti th h f di t b Response 3—nutrition through feeding tube (no flushes, not just medications, not Pedialyte)Pedialyte)
M1030 guidance at 4b-Q47-53.9

M1032RiskforHospitalization M1032RiskforHospitalization
Timepoints SOC/ROCp Response 3=witnessed and reported
(unwitnessed) falls Response 4=includes OTC meds Recent decline refers to significant changes
i th t th t i t thoccurring over the past year that may impact the patient’s ability to remain safely at home and increase likelihood of hospitalizationincrease likelihood of hospitalization
Fraility includes wt loss in past year, self-reported exhaustion, and slower movements
M1034OverallStatus M1034OverallStatus
Timepoints SOC/ROC Timepoints SOC/ROC Info from other providers and clinical
judgmentjudgment Current health status, medical
diagnoses and info from physician anddiagnoses, and info from physician and patient/family on expectations of recovery or life expectancyrecovery or life expectancy
A DNR order does not need to be in place for Responses 2 or 3.place for Responses 2 or 3.
M1036RiskFactors M1036RiskFactors
Timepoints SOC/ROCp If response 5 is marked, no other response is
marked.CMS does not provide specific definitions CMS does not provide specific definitions.
Amount and length of exposure should be considered.
Should evaluate risks to current health conditions from behaviors that were stopped in the pastthe past.
For determination of obesity, consider using BMI.
M1040InfluenzaVaccine
Info on flu vaccines at 4b-Q62.1-62.5
M1040InfluenzaVaccine
Timepoints TRN/DCp Process Outcome--Responses to M1040 and M1045 are
combined to report the percentage of eligible patients h i d i fl i i ti f th t flwho received influenza immunization for the current flu
season. Episode is defined as SOC to DC or SOC to TRN or ROC Episode is defined as SOC to DC or SOC to TRN or ROC
to DC or ROC to TRN Check the CDC for timeframes for administration for each
flu season Check ‘yes’ only if your agency provided the vaccine in
an outcome episode that includes ANY dates betweenan outcome episode that includes ANY dates between Oct 1-March 31.
Check NA if entire episode is outside the flu season.
Example
Patient admitted to hh on Sept 13• Patient admitted to hh on Sept 13 and given the vaccine on September 17 Y di h i17. You are now discharging on December 10. Do you mark ‘Yes’ ‘No’ or ‘NA’?
Admit Sept 13
VaccineDC—Dec 10
October 1
M1040QuestionQ
Can I answer M1040, Influenza Vaccine, “1-Yes” if we C 0 0, ,gave the patient the influenza vaccine during this episode of care for the current flu season even if no day in the quality episode fell between 10/1 and 3/31?day in the quality episode fell between 10/1 and 3/31? I understand it won't be included in the process measure computation, but it would be easier for my p ystaff if they could just answer yes or no, without needing to worry about determining if the episode is within the measure calculation time frame Forwithin the measure calculation time frame. For example, my patient was administered the flu vaccine in September, but was discharged on September 30.
4b-Q62.2.1
Andtheansweris…
No “NA” is the appropriate response for No. NA is the appropriate response for M1040, Influenza Vaccine, when no day in the quality episode fell between October 1 and March 31 This means at the Transferand March 31. This means at the Transfer or Discharge, you are only considering the time period from the SOC or ROC, p ,whichever is most recent, to the Transfer or Discharge date. If no day in this period of time fell between October 1 and March 31time fell between October 1 and March 31, NA is the appropriate M1040 response, even if the influenza vaccine was given for the current flu season.
M1045ReasonInfluenzaVaccinenotreceivedreceived
If the other responses do not apply, then If the other responses do not apply, then Response 7 should be chosen.
Not required that your agency offered the q y g yvaccine, just that the patient was offered the vaccine and they refused
Contraindications are listed in Chapter 3. What if the agency is not allowed to
transport the vaccine, but the family obtains and the HHA is asked to administer?
Response 2 if you gave the patient a flu shot at a previous flu clinic

M1045
The physician doesn’t want the patient to have The physician doesn t want the patient to have the flu vaccine for at least 6 weeks after his joint replacement surgery. Joint replacement surgery is not one of the reasons listed at the CDCis not one of the reasons listed at the CDC website as a medical contraindication. What is the appropriate M1045, Reason Influenza Vaccine not received?Vaccine not received?
If the assessing clinician confirmed the fact that the physician medically restricted the patient f i i th fl i f thfrom receiving the flu vaccine for any reason, the appropriate response for M1045 would be “4-Assessed and determined to have medical contraindications”. 4b-Q62.3
M1050PneumococcalVaccine
M1055PneumococcalVaccine
Responses to M1050 and M1055 areResponses to M1050 and M1055 are combined to report the percentage of eligible patients who ever receivedeligible patients who ever received PPV.
If the response to M1050 is ‘No’ and If the response to M1050 is No and none of the responses apply in M1055, then Response 5 should beM1055, then Response 5 should be chosen.
Contraindications are listed inContraindications are listed in Chapter 3, but have been updated.
PPVContraindications
September 2010— September 2010 The important changes are that persons ages 18-64 with
asthma or those who smoke are included in the groups for whom routine administration of PPV is recommended.
Those removed from routine PPV administration include American Indians and Alaska Natives age < 65 unlessAmerican Indians and Alaska Natives age < 65 unless they have a condition that qualifies them for PPV.
The recommendations regarding those age 65 and older g g gand re-vaccination were not changed.
4b-Q62.6

M1055Q&AApril2013Q p
Q2: What if the physician ordered us not to193
Q2: What if the physician ordered us not to administer it for reasons not included in the CDC list of medical contraindications?the CDC list of medical contraindications?A2: If the assessing clinician confirmed the
h i i di ll t i t d th ti tphysician medically restricted the patient from receiving the vaccine for any reason,
i t i “3”appropriate response is “3”
Living Arrangements M1100LivingArrangementsM1100SensoryStatusM1200‐M1242
M1100 Patient Living SituationM1100PatientLivingSituation M1100PatientLivingSituationg
Timepoints SOC ROCTimepoints SOC ROC
Using the care provider’s professional judgment decide a) whether thejudgment, decide a) whether the patient is living alone or with other(s) and b) the availability of caregiver(s)and b) the availability of caregiver(s) (other than home health agency staff) t id i i tto provide in-person assistance.

M1100 Patient Living SituationM1100PatientLivingSituation
Physical assistance includes assistance Physical assistance includes assistance with ADLs and IADLsmeal preparationmeal preparationmedication managementDoes not include assistance by phone emergencyDoes not include assistance by phone, emergency
assistance that can be accessed by Lifeline or 911 In M1100, “availability of assistance” refers In M1100, availability of assistance refers
to in-person assistance provided in the home of the patient (adult day care not p ( yincluded) Jan 2013
M1100PatientLivingSituation
If the patient’s living situation varies caregiver temporarily staying with the g p y y g
patient family member living with the patient whofamily member living with the patient who
occasionally travels out of townthen select the response that bestthen select the response that best reflects the usual living arrangements.
M1100PatientLivingSituation
Usual status—the living arrangementUsual status the living arrangement prior to illness, injury, or exacerbation of condition for which the patient isof condition for which the patient is receiving care in this episode, unless there exists a new living arrangementthere exists a new living arrangement which is expected to be permanent.
Expected availability and willingnessExpected availability and willingness of caregivers for the upcoming outcome episode of careoutcome episode of care.
M1100PatientLivingSituation
Around the clock—someone available in the home to id i h i 24 h d ( i hprovide assistance to the patient 24 hours a day (with
infrequent exceptions) Regular daytime—someone is in the home and g y
available to provide assistance during daytime hours every day with infrequent exceptions (no spec hrs)
Regular nighttime—someone is in the home and g gavailable to provide assistance during nighttime hours every night with infrequent exceptions (no spec hrs)
Occasional/short-term assistance—someone is available to provide in-person assistance only for a few hours a day or on an irregular basis, or may be only able to help occasionally
No assistance available—no one available to provide any in-person assistance.

S S M1200SensoryStatusM1200s
M1200Vision(withcorrectivelensesifthepatientusuallywearsthem):p y )
M1200Vision
Timepoints SOC ROC Follow-up Identifies patient’s functional visionpability to see and visually manage safely
within his/her environment, wearing , gcorrective lenses if these are usually worn
Includes neck injury and orbital swelling 4b-j y gQ64.1
“Nonresponsive” means that the patient i t bl t dis not able to respond
M1200Vision
A magnifying glass (as might be used to g y g g ( gread newsprint) is not an example of corrective lensescorrective lenses.
Reading glasses (including "grocery t " di l ) id dstore" reading glasses) are considered
to be corrective lenses

M1200 VisionM1200Vision
Assessment strategies Assessment strategiesAsk the patient about vision problemsCataractsWhether or not the patient uses glassesObserve ability to locate signature line on consent
formformCount fingers at arm’s lengthAbility to differentiate between medications
i ll if di ti lf d i i t despecially if medications are self administered. Be sensitive to requests to read, as patient
may not be able to read though vision ismay not be able to read though vision is adequate.
M1210Abilitytohear
M1210 Ability to hearM1210Abilitytohear Timepoints SOC ROC Identifies the patient’s ability to hear spoken language
and other sounds (e.g., alarms). Evaluate with hearing aids or devices if patient usually Evaluate with hearing aids or devices if patient usually
uses them Assure devices are in place, turned on and workingResponse“UK” Response“UK”Patient not able to respond Impossible to assess hearing Impossible to assess hearingsevere dementiaSchizophrenia
U iUnconscious
M1220 Understanding Verbal ContentM1220UnderstandingVerbalContent

M1220UnderstandingVerbalContent
Ti i SOC ROC Timepoints SOC ROC Identifies the patient’s
F ti l bilit t h d kFunctional ability to comprehend spoken words
Ability to follow instructions in theAbility to follow instructions in the patient’s primary language (must be fluent).
Hearing and cognitive abilities may impact a patient's ability to understand verbal contentverbal content.
M1220UnderstandingVerbalContentContent
If patient can comprehend lip reading If patient can comprehend lip reading, they have the ability to understand verbal content even if they are deafcontent, even if they are deaf.
Response ‘UK’Selected if the patient is not able to respond Or otherwise impossible to assess
understanding of spoken words and instructions.
Interpreter may be necessary
M1230SpeechandOral(Verbal)Expressionof Language (in patient's own language):ofLanguage(inpatient sownlanguage):
No Dynavox 4b-Q66.2
M1240PainAssessment
C t I t it f P iCaptures Intensity of PainPresence of pain at the time of the formal
assessment not the ‘day of assessment ’ 4b Q70 3assessment, not the day of assessment. 4b-Q70.3

M1240PainAssessment
Identifies if a standardized pain assessment was pconducted to determine a clinically significant level of pain.P h ’ f Process measures to capture the agency’s use of best practices (Reported on OBQI and Home Health Compare)Compare)
Response 0--Standardized tool was not used to assess pain
Response 1 or 2--Pain assessment must be conducted by assessing clinician during the time frame specified by CMS for completion of theframe specified by CMS for completion of the assessment
M1240 Pain AssessmentM1240PainAssessment
Severe pain is defined according to theSevere pain is defined according to the scoring system for the standardized
l b i dtool being used. If the standardized tool does not define
levels of "severe" pain, then the agency or care provider should use the level(s)or care provider should use the level(s) of pain identified in the standardized tool that best reflect the concept oftool that best reflect the concept of "severe." (e.g. FACES scale)
How Does M1240 Relate to OtherHowDoesM1240RelatetoOtherProcessMeasuresre:Pain?
M2250PlanofCareSynopsisy p216
NO: POC contains orders for only one of the interventions (e.g., pain meds but no monitoring)
YES: POC contains interventions to monitor AND mitigate pain. Interventions may include medication, massage, p y , g ,visualization, biofeedback and other intervention approaches
NA: Comprehensive assessment indicates NO pain

Example A patient is documented to have chronic arthritic joint pain
that interferes with activity at least daily and is taking a pain medication daily as previously ordered. If thepain medication daily as previously ordered. If the clinician only has orders to assess the effectiveness of the current pain medication treatment, is this order only an order to MONITOR pain (M2250e “no”) or would thisan order to MONITOR pain (M2250e no ), or would this be enough to answer “yes”, that we have an order to both monitor and mitigate pain?
An ordered pain medication is considered an intervention to mitigate pain. Assessing for the effectiveness of the pain medication is considered an intervention to monitorpain medication is considered an intervention to monitor pain. If both the pain medication and an order related to pain assessment are included in the physician-ordered plan of care, M2250e would be “Yes”. 4b-Q172.8.2
217
NO: POC contains interventions (meds and/or another approach e.g. massage, meditation), but no monitoring or no pp g g , ), gsupportive documentation is in the clinical record or POC does not include interventions.
YES: POC contains interventions to monitor AND mitigate pain and the clinical record contains documentation that these i i f d h i f h i OASISinterventions were performed at the time of the previous OASIS assessment or since that time
218NA: Formal assessment did not indicate pain (must have done a formal assessment of pain to mark NA)
M2400andPain
At the time of a visit, the patient reports mild pain and the b th t th ti t' f ti i i t li it dnurse observes that the patient's functioning is not limited
by the mild pain. The POC includes prn analgesic for pain management, which is offered, however the patient feels the pain is tolerable and elects no intervention at this timethe pain is tolerable and elects no intervention at this time. Can I select “Yes” for M2400d, Pain Interventions, because the intervention was ordered, offered to patient, but not felt by the patient to be needed?
If there were orders to assess pain and relieve pain (prnanalgesic), and record review revealed that since the previous OASIS assessment, the clinician assessed pain, and offered the analgesic but it was never taken becauseand offered the analgesic, but it was never taken because of documented lack of need, as evidenced by patient's subjective comments that the pain did not warrant the medication, then M2400d may be answered "Yes". The ed cat o , t e 00d ay be a s e ed es eintervention was implemented when the attempt to provide it was made, and the lack of need identified. 4b-Q182.6
M1242FrequencyofPainInterferingwithpatient's activity or movement:patient sactivityormovement:
M1242FrequencyofPainInterferingwithpatient's activity or movement:patient sactivityormovement:
Timepoints SOC/ROC/FU/Dischargep g Identifies how often pain interferes with
activities and/or treatments if prescribedactivities and/or treatments if prescribed
All ti iti t j t ADL l i All activities, not just ADLs, e.g. sleeping, recreational activities, watching television.
M1242FrequencyofPainInterferingwithpatient's activity or movement:patient sactivityormovement:
Pain interferes with activity when the pain Pain interferes with activity when the pain results In activity being performed less often than In activity being performed less often than
otherwise desired 4b-Q72
Requires patient to have additionalRequires patient to have additional assistance in performing the activity
Causes the activity to take longer toCauses the activity to take longer to complete
Medication reviewPain medication
ClarificationofTimePeriod
If a patient reports they have no pain currently because they have modified their activity level several weeks or months ago to exclude anmodified their activity level several weeks or months ago to exclude an activity they know will cause pain, do we answer M1242 based on the fact that they have modified their activity level (e.g., aren’t even attempting to perform that activity due to the possibility of the pain returning) or do we not even consider that activity when answering thereturning), or do we not even consider that activity when answering the question because the patient has excluded it from their activities a “long” time ago. And if that is true, what would be the time frame for a “long” time ago?
Timeframe under consideration is the day of assessment and recent pertinent past.
If the patient has stopped performing an activity in order to be free of pain the patient HAS pain that is interfering with activity If a patient atpain, the patient HAS pain that is interfering with activity. If a patient at some point stopped performing activity because of pain and there is no reasonable expectation that they could or would ever perform the activity again, an assessing clinician’s judgment may determine that the activity is not considered to be in the pertinent past Examples: stoppedactivity is not considered to be in the pertinent past. Examples: stopped skiing after a knee injury 20 years ago. 4b-Q73.1
M1242Q&AApril2013Q p
Q3: How does a physician order to 224
p yimmobilize a surgical extremity impact scoring of M1242?A3 If ti t h t d f i ti itA3: If patient has stopped performing activity due to a medical restriction, not due to pain, the pain is not considered to be interfering e pa s o co s de ed o be e e gwith activity. However, if the patient is experiencing other pain that does interfere with activity or movement or restricting otherwith activity or movement or restricting other activity due to pain, it would be reported in M1242.

Integumentary StatusIntegumentary StatusM1300‐M1350
225
The OASIS manual and the opinions of the Wound Ostomy and Continence Nurses (WOCN) and the National Pressure Ulcer Advisory Panel y(NPUAP) are to be used as our officialguidance when documentingguidance when documenting information about pressure ulcers and venous stasis ulcersvenous stasis ulcers.
•http://www.wocn.org/pdfs/GuidanceOASIS-C.pdfg p p
WOCNandNPUAPDocuments
Definitions of Healing StatusDefinitions of Healing StatusDefinitions of Other Terms related to
WoundsDefinition of a Pressure Ulcere t o o a essu e U ceDescriptions of Pressure Ulcer
StagesStagesDefinition of a Stasis Ulcer
PressureUlcerDefined
• A localized injury to the skin and/or underlying tissue usually over a bony
i lt fprominence, as a result of pressure, or pressure in combination with shear and/or friction A number ofand/or friction. NPUAP A number of contributing or confounding factors are also associated with pressure ulcers;also associated with pressure ulcers; the significance of these factors is yet to be elucidated Added by WOCN 2009to be elucidated. Added by WOCN 2009
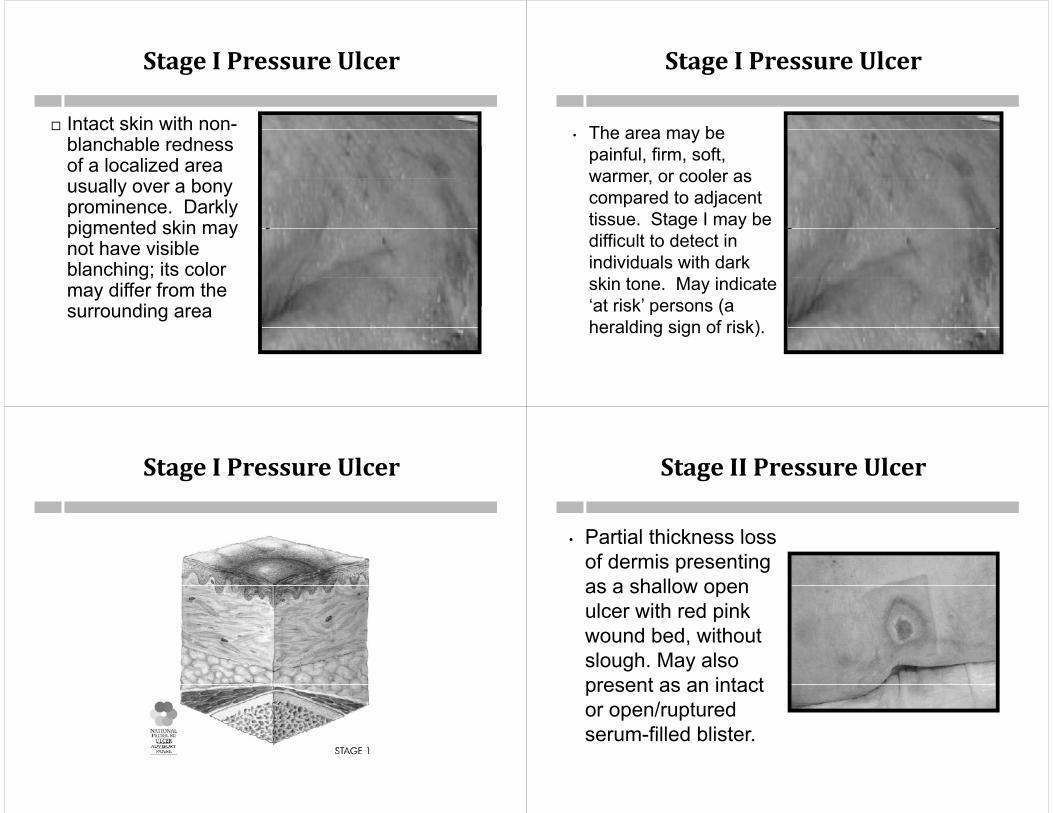
StageIPressureUlcer
Intact skin with non- Intact skin with nonblanchable redness of a localized area
ll busually over a bony prominence. Darkly pigmented skin maypigmented skin may not have visible blanching; its color g;may differ from the surrounding area
StageIPressureUlcer
The area ma be• The area may be painful, firm, soft, warmer or cooler aswarmer, or cooler as compared to adjacent tissue. Stage I may be g ydifficult to detect in individuals with dark ki t M i di tskin tone. May indicate
‘at risk’ persons (a heralding sign of risk)heralding sign of risk).
StageIPressureUlcer StageIIPressureUlcer
Partial thickness loss• Partial thickness loss of dermis presenting as a shallow openas a shallow open ulcer with red pink wound bed withoutwound bed, without slough. May also present as an intactpresent as an intact or open/ruptured serum filled blisterserum-filled blister.
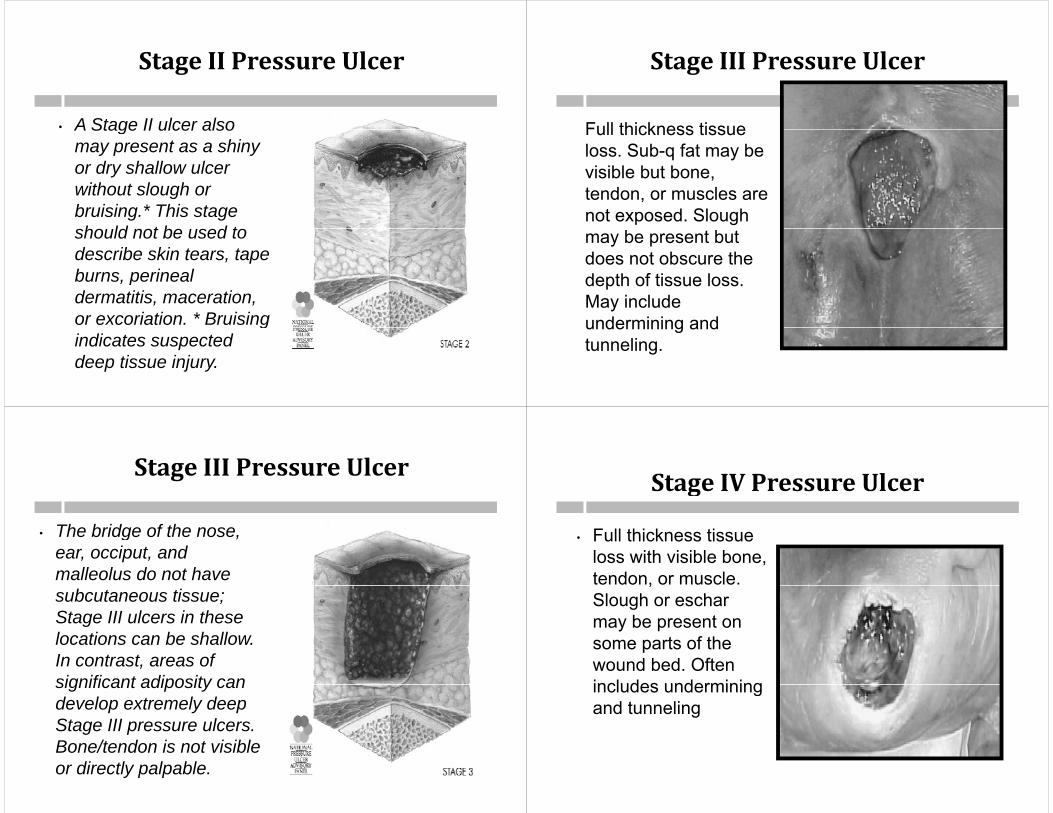
StageIIPressureUlcer
• A Stage II ulcer alsoA Stage II ulcer also may present as a shiny or dry shallow ulcer without slough or bruising.* This stage h ld t b d tshould not be used to
describe skin tears, tape burns perinealburns, perineal dermatitis, maceration, or excoriation. * Bruising gindicates suspected deep tissue injury.
StageIIIPressureUlcer
Full thickness tissueFull thickness tissue loss. Sub-q fat may be visible but bone, ,tendon, or muscles are not exposed. Slough may be present but does not obscure the depth of tissue lossdepth of tissue loss. May include undermining andundermining and tunneling.
StageIIIPressureUlcer
• The bridge of the nose,The bridge of the nose, ear, occiput, and malleolus do not have subcutaneous tissue; Stage III ulcers in these l ti b h lllocations can be shallow. In contrast, areas of significant adiposity cansignificant adiposity can develop extremely deep Stage III pressure ulcers. g pBone/tendon is not visible or directly palpable.
Stage IV Pressure UlcerStageIVPressureUlcer
Full thickness tissue• Full thickness tissue loss with visible bone, tendon, or muscle. ,Slough or eschar may be present on some parts of the wound bed. Often includes underminingincludes undermining and tunneling
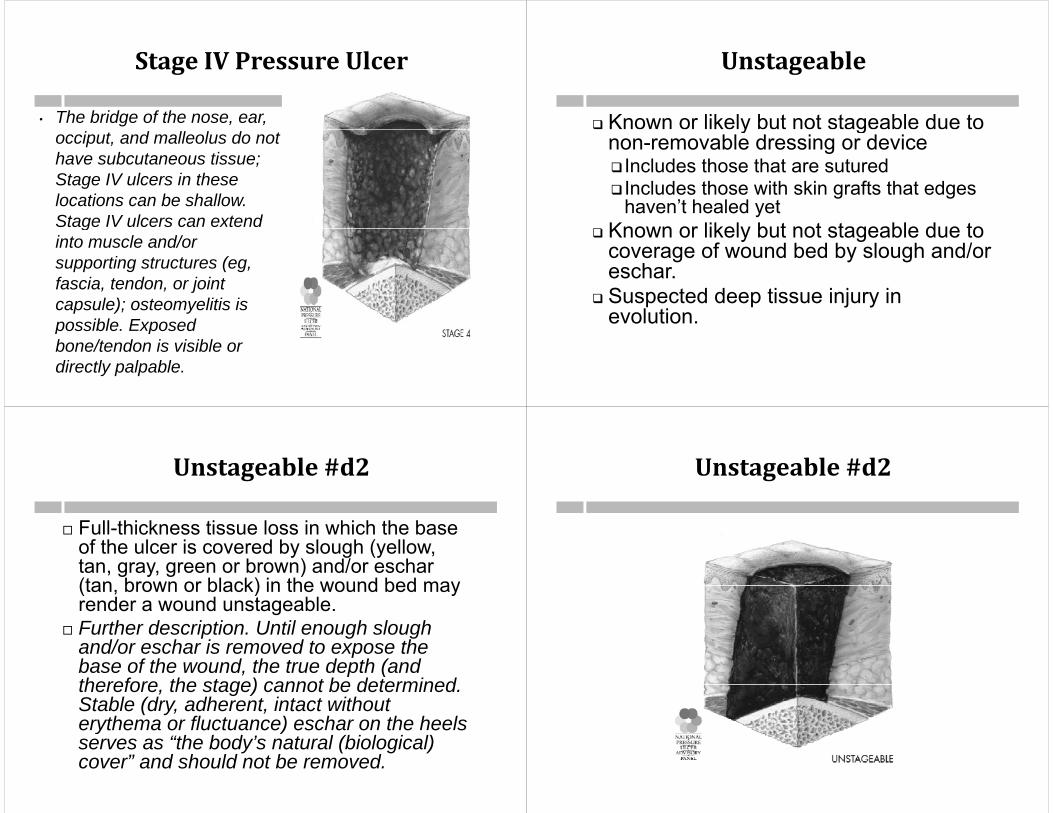
StageIVPressureUlcer
• The bridge of the nose, ear, occiput, and malleolus do not have subcutaneous tissue; Stage IV ulcers in theseStage IV ulcers in these locations can be shallow. Stage IV ulcers can extend ginto muscle and/or supporting structures (eg, f i t d j i tfascia, tendon, or joint capsule); osteomyelitis is possible Exposedpossible. Exposed bone/tendon is visible or directly palpable.
Unstageable
Known or likely but not stageable due to y gnon-removable dressing or device Includes those that are sutured Includes those with skin grafts that edges
haven’t healed yet Known or likely but not stageable due to Known or likely but not stageable due to
coverage of wound bed by slough and/or eschar.eschar.
Suspected deep tissue injury in evolution.
Unstageable#d2
Full-thickness tissue loss in which the base of the ulcer is covered by slough (yellow, tan, gray, green or brown) and/or eschar(tan brown or black) in the wound bed may(tan, brown or black) in the wound bed may render a wound unstageable.
Further description. Until enough slough u e desc p o U e oug s ougand/or eschar is removed to expose the base of the wound, the true depth (and therefore the stage) cannot be determinedtherefore, the stage) cannot be determined. Stable (dry, adherent, intact without erythema or fluctuance) eschar on the heels y )serves as “the body’s natural (biological) cover” and should not be removed.
Unstageable#d2
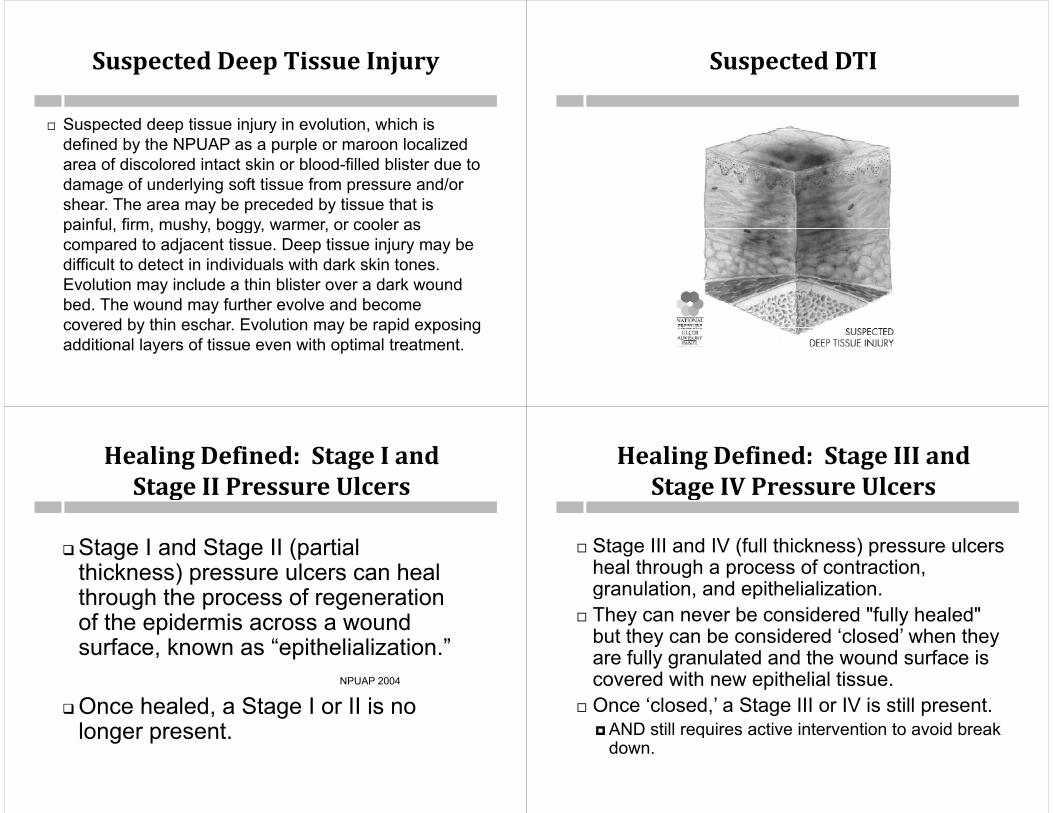
SuspectedDeepTissueInjury
Suspected deep tissue injury in evolution, which is Suspected deep tissue injury in evolution, which is defined by the NPUAP as a purple or maroon localized area of discolored intact skin or blood-filled blister due to d f d l i ft ti f d/damage of underlying soft tissue from pressure and/or shear. The area may be preceded by tissue that is painful, firm, mushy, boggy, warmer, or cooler aspainful, firm, mushy, boggy, warmer, or cooler as compared to adjacent tissue. Deep tissue injury may be difficult to detect in individuals with dark skin tones. Evolution may include a thin blister over a dark wound bed. The wound may further evolve and become covered by thin eschar Evolution may be rapid exposingcovered by thin eschar. Evolution may be rapid exposing additional layers of tissue even with optimal treatment.
SuspectedDTI
HealingDefined:StageIandStage II Pressure UlcersStageIIPressureUlcers
Stage I and Stage II (partial thickness) pressure ulcers can heal through the process of regeneration of the epidermis across a wound surface, known as “epithelialization.”
NPUAP 2004NPUAP 2004
Once healed, a Stage I or II is no longer presentlonger present.
HealingDefined:StageIIIandStage IV Pressure UlcersStageIVPressureUlcers
Stage III and IV (full thickness) pressure ulcers heal through a process of contraction, granulation and epithelializationgranulation, and epithelialization.
They can never be considered "fully healed" but they can be considered ‘closed’ when theybut they can be considered closed when they are fully granulated and the wound surface is covered with new epithelial tissue.covered with new epithelial tissue.
Once ‘closed,’ a Stage III or IV is still present.AND still requires active intervention to avoid breakAND still requires active intervention to avoid break
down.

PressureUlcerGeneral GuidanceGeneralGuidance
Do not reverse stage Do not reverse stage A muscle flap, *skin advancement flap, or
rotational flap performed to surgicallyrotational flap performed to surgically replace a pressure ulcer is a surgical wound and is no longer a pressure ulcerwound and is no longer a pressure ulcer.
A pressure ulcer that has been surgically debrided remains a pressure ulcer It doesdebrided remains a pressure ulcer. It does not become a surgical wound.
A pressure ulcer with a skin graft is still a A pressure ulcer with a skin graft is still a pressure ulcer.
PressureUlcers(2nd q2012)( q )
Stage II pressure ulcer at SOC that isStage II pressure ulcer at SOC that is now closed and only red
No reverse staging! Not a Stage 1No reverse staging!—Not a Stage 1 If reepithelialized and healed—then
t t dnot reported. If a new non-blanching erythema at
the site where the Stage 2 healed, this is a new Stage 1.
IssueonPressureUlcerswithSkin GraftsSkinGrafts
Pressure ulcer with a skin graft is a pressure Pressure ulcer with a skin graft is a pressure ulcer.
Also cannot visualize the wound bed to be able to so ca o sua e e ou d bed o be ab e ostage.
So what to do with a pressure ulcer covered with pa skin graft??Unepithelialized edges = unstageable by
presence of device or graftEdges epithelialized = closed ulcer at original
stage
PressureUlcerGeneral GuidanceGeneralGuidance
Unhealed: The absence of the skin’s original integrity (includes closedoriginal integrity. (includes closed Stage III and Stage IV)
Non-epithelialized: The absence of regenerated epidermis across aregenerated epidermis across a wound surface.

M1300PressureUlcerAssessmentM1302RiskofDevelopingPressureUlcersp g
Process MeasureProcess Measure
M1300PressureUlcerAssessmentAssessment
Timepoints SOC ROCp Identifies patient’s risk of developing pressure
ulcersulcers CMS does not require the use of standardized
tools, nor does it endorse one particular tool.tools, nor does it endorse one particular tool. This item is used to calculate process
measures to capture the agency’s use of bestmeasures to capture the agency s use of best practices
The best practices stated in the item are not The best practices stated in the item are not necessarily required in the CoPs
M1300PressureUlcerAssessmentAssessment
If Response to M1300 was “0” (No pressure If Response to M1300 was 0 (No pressure ulcer risk assessment) note skip pattern
Use of validated standardized screening tool Use of validated standardized screening toolUse the scoring parameters to identify if a
patient is at risk for developing pressure ulcersp p g p If tool does not define levels of risk or if eval
was based on clinical factors (w/o a (validated standardized screening tool), then the care provider may define what p yconstitutes risk
M1300PressureUlcerAssessmentAssessment
Response 1--Patient's risk for pressureResponse 1 Patient s risk for pressure ulcer development was clinically assessed but no formal pressure ulcerassessed, but no formal pressure ulcer screening tool was used.
Response 2--Formal standardized tool was used.

M1300
If a patient scores no risk on the Braden Scale but the RNBraden Scale but the RN performs an evaluation of clinical factors and determines thefactors and determines the patient is at risk for pressure ulcers how do we answerulcers, how do we answer M1300?
4b-Q87.3
NewAnswerJan.2013Q&AJ Q
The response to M1300 should be “2-Yes,254
The response to M1300 should be 2 Yes, using a standardized tool, e.g., Braden, Norton, other” if a standardized, validated tool assessment tool, e.g., Braden, Norton, was utilized, regardless of whether another non standardized tool or clinical evaluationnon-standardized tool or clinical evaluation was also conducted. If both a standardized pressure ulcer assessment AND anpressure ulcer assessment AND an evaluation of clinical factors were conducted, the response to M1302 should pbe “1-Yes” if either the clinical evaluation or the standardized tool is positive for risk.
M1306UnhealedPressureUlcerat Stage II or HigheratStageIIorHigher
M1306UnhealedPressureUlceratStage II or HigherStageIIorHigher
Timepoints SOC/ROC/FU/DC Timepoints SOC/ROC/FU/DC Select Response 1 – Yes, if the patient has an unhealed Stage II ORunhealed Stage II, OR a Stage III, or Stage IV pressure ulcer at any
healing status level ORhealing status level OR if the patient has an unstageable ulcer(s)R 0 ‘N ’ if• Response 0 ‘No’ ifThe only pressure ulcer(s) is Stage 1 OR if a former Stage 2 pressure ulcer has healed
AND the patient has no other pressure ulcers
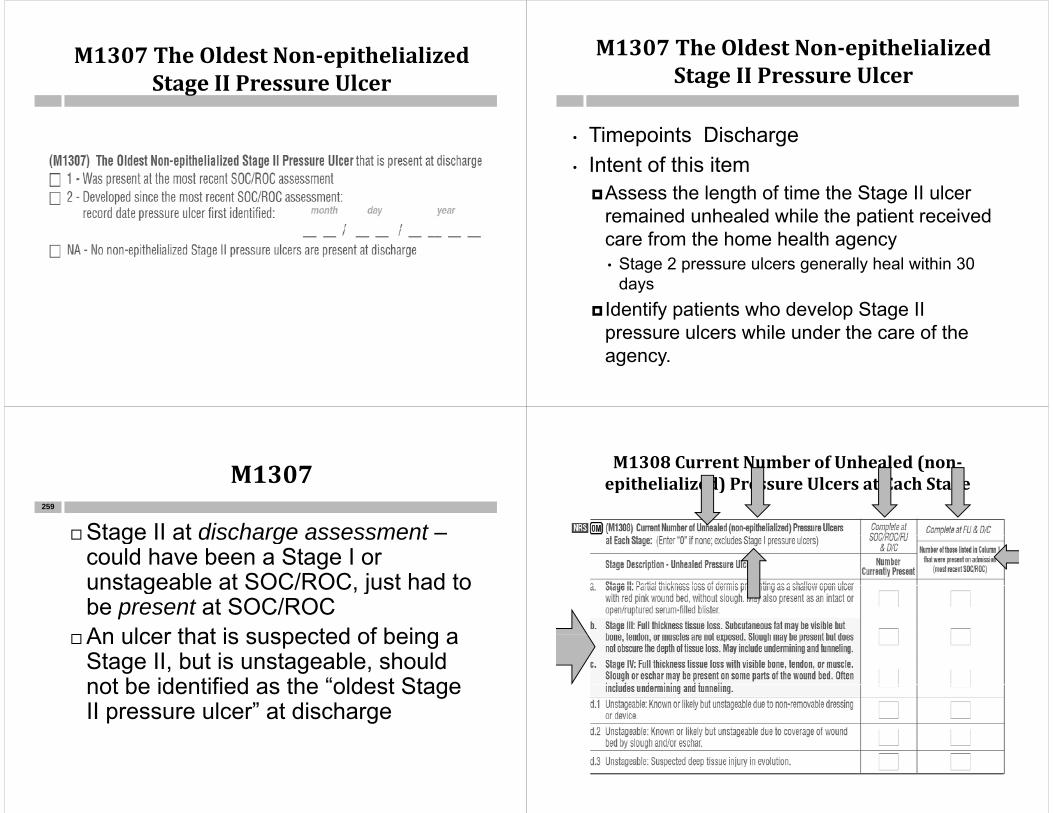
M1307TheOldestNon‐epithelializedStage II Pressure UlcerStageIIPressureUlcer
M1307TheOldestNon‐epithelializedStage II Pressure UlcerStageIIPressureUlcer
Ti i t Di h• Timepoints Discharge• Intent of this item
Assess the length of time the Stage II ulcer remained unhealed while the patient received care from the home health agency• Stage 2 pressure ulcers generally heal within 30
ddays Identify patients who develop Stage II
l hil d th f thpressure ulcers while under the care of the agency.
M1307
Stage II at discharge assessment –259
Stage II at discharge assessmentcould have been a Stage I or unstageable at SOC/ROC just had tounstageable at SOC/ROC, just had to be present at SOC/ROC
An ulcer that is suspected of being aAn ulcer that is suspected of being a Stage II, but is unstageable, should not be identified as the “oldest Stagenot be identified as the oldest Stage II pressure ulcer” at discharge
M1308CurrentNumberofUnhealed(non‐epithelialized) Pressure Ulcers at Each Stageepithelialized)PressureUlcersatEachStage

M1308CurrentNumberofUnhealed(non‐epithelialized)PressureUlcersatEachStagep ) g
Cli i i h ld k ff t t Clinician should make every effort to determine the wound’s most severe stage Contact previous providersContact physicianThere are exceptions if unstageable now
An ulcer's stage can worsen and this item An ulcer s stage can worsen, and this item should be answered appropriately if this occursoccurs.
M1308CurrentNumberofUnhealed(non‐epithelialized)PressureUlcersatEachStagep ) g
Although the wording in M1308 includes the term ‘non epithelialized ’ for this itemthe term non epithelialized, for this item, a closed Stage III or Stage IV pressure ulcer should be reported as a pressure p pulcer at its worst stage, even if it has re-epithelialized.
An epithelialized stage II is not reported. Why? y
Exercise:PatienthasnoStageIIonadmission but has a Stage II at FU.admissionbuthasaStageIIatFU.
AALL
ZEROOES
Exercise:PatienthasnoStageIIonadmission but has a Stage II at FU.admissionbuthasaStageIIatFU.
1 01 0
ZZERO
ERO O
ES
OES SS

M1308CurrentNumberofUnhealed(non‐epithelialized)PressureUlcersatEachStagep ) g
Patient has no Stage II pressure ulcers on admission, g p ,but develops one during the first episode that is present at the time of follow-up.
In this case, row a, column 1 would be “0” at SOC.At follow-up, row a, column 1 would be “1” and row a
column 2 would be “0,” indicating the pressure ulcer was not present on admission.
Exercise:PatienthasaStageIIIonadmission that is a Stage IV at FUadmissionthatisaStageIVatFU
1
0
1
0
0
0
0
Exercise:PatienthasaStageIIIonadmission that is a Stage IV at FUadmissionthatisaStageIVatFU
00
0 0
00
1 1
00 0
0
0
0
00
M1308CurrentNumberofUnhealed(non‐epithelialized) Pressure Ulcers at Each Stageepithelialized)PressureUlcersatEachStage
Example 2: Patient has a Stage III pressure ulcerExample 2: Patient has a Stage III pressure ulcer on admission that is assessed to be a Stage IV at follow-up. In this case, row b, column 1 would be “1” at SOC. At follow-up, row b, columns 1 and 2 would both be “0,” as the patient no longer has a Stage III ulcer. Row c, column 1 would be “1” and column 2 would be “1” indicating the ulcer was present onbe 1 indicating the ulcer was present on admission, even though it was at a different stage.stage.

Exercise:StageIIonadmissionthathealswithinthefirst2weeks,butthendevelopsanotherstageIIprior
toDCatweek4.
1
ALL
ZZEROES
Exercise:StageIIonadmissionthathealswithinthefirst2weeks,butthendevelopsanotherstage
IIpriortoDCatweek4.
1 0
ZER
0
0
ZER R
OES
0
0
ROES S0S
M1308CurrentNumberofUnhealed(non‐epithelialized) Pressure Ulcers at Each Stageepithelialized)PressureUlcersatEachStage
Example 3: Patient has a Stage II pressure ulcer on Example 3: Patient has a Stage II pressure ulcer on admission that heals within the first 2 weeks, but then develops another Stage II pressure ulcer prior to discharge at week 4discharge at week 4.
In this case, row a, column 1 would be “1” at SOC. At Follow-up, row a, column 1 would be “1” and row a, p, , ,column 2 would be “0”, indicating the pressure ulcer that is present at follow up or discharge was not present on admissionon admission.
For both Columns 1 and 2: Mark a response for each row of this item: a, b, c, d1, d2, and
d3. If there are NO ulcers at a given stage, enter “0” for that stage.
M1308ROC&Recert
Mrs. I. M. Onabiggawound was released from ggthe hospital on day 57 of the episode. You will be completing the ROC assessment and you know that it will also serve as theand you know that it will also serve as the Recertification assessment.
She has a stage III pressure ulcer. S e as a s age p essu e u ceWill you complete column 2 (Current
Number of Unhealed Pressure Ulcers at E h St ) M1308 ill lEach Stage) on M1308 or will you leave column 2 blank?

HowtoCompleteM1308ontheROC/Recert
1
0LEAV1
ZE
VE
BEROE
LANKS K
M1308Q&AApril2013Q p
Q4: Patient had a closed Stage IV274
Q4: Patient had a closed Stage IV pressure ulcer at SOC. Two weeks l t it d t b h lllater, it appeared to be a shallow open ulcer. Can I report it as a Stage II or is it a non-observable Stage IV because I can’t visualize bone, muscle or ,tendon?
M1308Q&AApril2013Q p
A4: A previously closed Stage III or Stage 275
p y g gIV pressure ulcer that opens again should be reported as its worst stage. As long as th d b d i f f l h dthe wound bed is free of slough and eschar, it may be reported as a Stage IV. If slough or eschar is present obscuringIf slough or eschar is present, obscuring the wound bed, it may not be staged and is reported in M1308 as d.2: known or lik l b t t bl d t flikely but unstageable due to coverage of wound bed by slough and/or eschar.
M1310,M1312,M1314LargestSurface DimensionSurfaceDimension
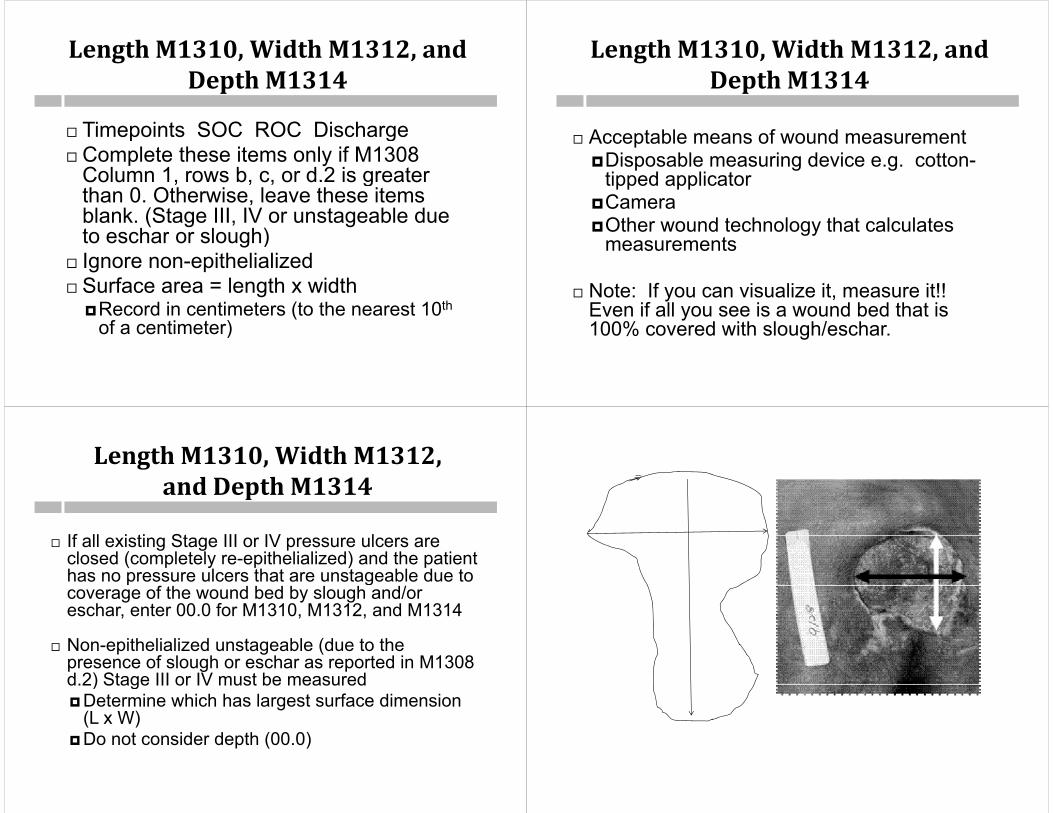
LengthM1310,WidthM1312,andDepth M1314DepthM1314
Timepoints SOC ROC Discharge Timepoints SOC ROC Discharge Complete these items only if M1308
Column 1 rows b c or d 2 is greaterColumn 1, rows b, c, or d.2 is greater than 0. Otherwise, leave these items blank. (Stage III, IV or unstageable due t h l h)to eschar or slough)
Ignore non-epithelializedS f l th idth Surface area = length x width Record in centimeters (to the nearest 10th
of a centimeter)of a centimeter)
LengthM1310,WidthM1312,andDepth M1314DepthM1314
A bl f d Acceptable means of wound measurementDisposable measuring device e.g. cotton-
tipped applicatortipped applicator Camera Other wound technology that calculatesOther wound technology that calculates
measurements
Note: If you can visualize it, measure it!! Even if all you see is a wound bed that is 100% covered with slough/eschar100% covered with slough/eschar.
LengthM1310,WidthM1312,and Depth M1314andDepthM1314
If ll i ti St III IV l If all existing Stage III or IV pressure ulcers are closed (completely re-epithelialized) and the patient has no pressure ulcers that are unstageable due to gcoverage of the wound bed by slough and/or eschar, enter 00.0 for M1310, M1312, and M1314
Non-epithelialized unstageable (due to the presence of slough or eschar as reported in M1308 d.2) Stage III or IV must be measuredd.2) Stage III or IV must be measuredDetermine which has largest surface dimension
(L x W)D t id d th (00 0)Do not consider depth (00.0)
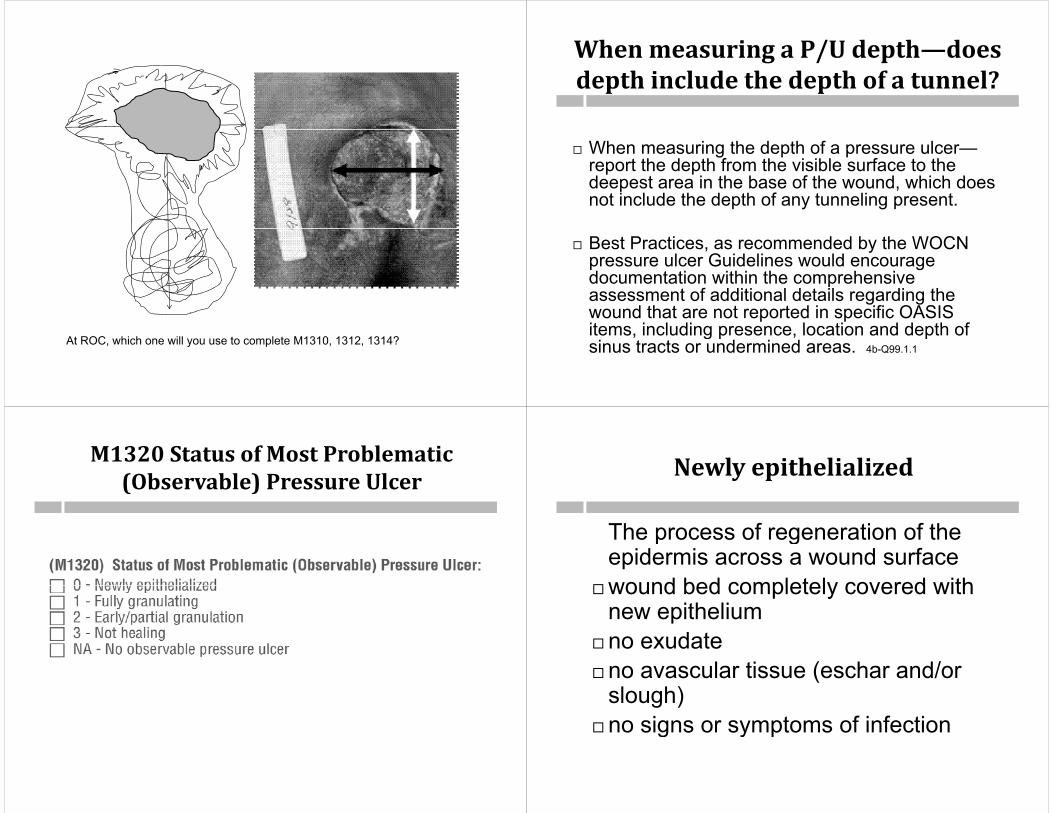
At ROC, which one will you use to complete M1310, 1312, 1314?
WhenmeasuringaP/Udepth—doesdepth include the depth of a tunnel?depthincludethedepthofatunnel?
When measuring the depth of a pressure ulcer—report the depth from the visible surface to the deepest area in the base of the o nd hich doesdeepest area in the base of the wound, which does not include the depth of any tunneling present.
Best Practices, as recommended by the WOCN pressure ulcer Guidelines would encourage documentation within the comprehensivedocumentation within the comprehensive assessment of additional details regarding the wound that are not reported in specific OASIS items including presence location and depth ofitems, including presence, location and depth of sinus tracts or undermined areas. 4b-Q99.1.1
M1320StatusofMostProblematic(Observable) Pressure Ulcer(Observable)PressureUlcer Newlyepithelialized
The process of regeneration of theThe process of regeneration of the epidermis across a wound surface
wound bed completely covered withwound bed completely covered with new epithelium
d tno exudateno avascular tissue (eschar and/or
slough)no signs or symptoms of infectiong y p

FullyGranulating
wound bed filled with granulation tissue to the level of the surrounding skinto the level of the surrounding skin
no dead spaceno avascular tissue (eschar and/or
slough)g )no signs or symptoms of infection
d dwound edges are open
Early/PartialGranulation
≥ 25% of the wound bed is covered≥ 25% of the wound bed is covered with granulation tissue
< 25% of the wound bed is covered with avascular tissue (eschar(and/or slough)
no signs or symptoms of infectionno signs or symptoms of infectionwound edges open
NotHealing
≥ 25% avascular tissue ORS/S of infection ORClean but non granulating wound bed
ORClosed/hyperkeratotic wound edges
ORPersistent failure to improve despite
appropriate comprehensive wound pp p pmanagement
M1320StatusofMostProblematic(Observable) Pressure Ulcer:(Observable)PressureUlcer:
Timepoints SOC/ROC/DCTimepoints SOC/ROC/DC Identifies the degree of healing visible
i th t bl ti b blin the most problematic observable pressure ulcer, stage II or higher. (St I t id d )(Stage Is are not considered.)
Visualization of the wound is necessary to identify the degree of healing evident in the ulcer identified in M1320.

M1320StatusofMostProblematic(Observable) Pressure Ulcer:(Observable)PressureUlcer:
Most problematicMay be the largesty gThe most advanced stageThe most difficult to access for treatmentThe most difficult to access for treatmentThe most difficult to relieve pressure, etc., If th ti t h l b bl If the patient has only one observable pressure ulcer, then that ulcer is the most problematic.
M1320StatusofMostProblematic(Observable) Pressure Ulcer:(Observable)PressureUlcer:
Response 0 ‘Newly epithelialized’Response 0 Newly epithelializedTissue has completely covered the wound
surface of the pressure ulcersurface of the pressure ulcer• Regardless of how long the pressure
ulcer has been re-epithelializedulcer has been re-epithelialized.This is an appropriate response for
Stage III and IV pressure ulcers butStage III and IV pressure ulcers, but not for Stage II ulcers as fully epithelialized Stage II ulcers should notepithelialized Stage II ulcers should not be reported.
M1320StatusofMostProblematic(Observable) Pressure Ulcer:(Observable)PressureUlcer:
• Response 1 – Fully Granulating Stage III or IV that epithelial tissue has notStage III or IV that epithelial tissue has not
completely covered the wound surfaceResponse 3 Not healing• Response 3 - Not healing Stage II
D t l t th f t b• Do not granulate, therefore, must be reported as Response ‘3’ not healing
S spected deep tiss e inj r that has not Suspected deep tissue injury that has not evolved is considered not healing.
M1320StatusofMostProblematic(Observable) Pressure Ulcer:(Observable)PressureUlcer:
NA No observable pressure ulcerNA- No observable pressure ulcerIncludes only those that cannot be
b d d t th fobserved due to the presence of a dressing or device that cannot be removed (including casts)(including casts).
When determining the healing status of a pressure ulcer for answering M1320a pressure ulcer for answering M1320, the presence of necrotic tissue does NOT make the pressure ulcer NA – No pobservable pressure ulcer.

M1320StatusofMostProblematic(Observable) Pressure Ulcer:(Observable)PressureUlcer:
A pressure ulcer with necrotic tissue (eschar/slough) obscuring the wound ( g ) gbase cannot be staged, but its healing status is either Response 2 – Early/partial granulation if necrotic or avascular tissue covers <25% of the wound bed, or R 3 N t h li if th dResponse 3 - Not healing, if the wound has ≥25% necrotic or avascular tissue.
JustAlmostClosedJ
My patient has a Stage III pressure ulcer that is closing. H d I t th t d t t h th i hHow do I report the stage and status when the opening has shrunk to a pinpoint size and does not present a viewable base due to the small opening?If you have a Stage III that is in the process of closing it If you have a Stage III that is in the process of closing, it remains an observable Stage III unless the wound bed was covered with a dressing that could not be removed or the wound bed was obscured with avascular tissue. If the wound margins are open and have now closed to the point where the opening is a pinpoint, the pressure ulcer would remain a Stage III. The status could be either Early/partial granulation or Fully granulating based on the descriptors ingranulation or Fully granulating, based on the descriptors in the WOCN Guidance on OASIS-C Integumentary Items, until the wound margins closed, at which time it would be considered a newly epithelialized Stage III pressure ulcer. co s de ed a e y ep t e a ed Stage p essu e u ce4b-Q99.3
M1322CurrentNumberofStageIPressure UlcersPressureUlcers
TimepointsSOC/ROC/FU/DischargeSOC/ROC/FU/Discharge
NRS
M1324StageoftheMostProblematicUnhealed (observable) Pressure UlcerUnhealed(observable)PressureUlcer

M1324StageofMostProblematicUnhealed(Observable) Pressure Ulcer(Observable)PressureUlcer
Timepoints SOC/ROC/FU/Discharge Must be able to visualize ulcer Determine the most problematic pressure
ulcer Identify the degree of damage evident in the
ulcer. If the patient has only one observable
pressure ulcer, then that ulcer is the most p ,problematic.
M1324StageofMostProblematicUnhealed(Ob bl ) P Ul(Observable)PressureUlcer
Follow NPUAP to make determination No reverse Follow NPUAP to make determination--No reverse staging!!
“NA” NO pressure ulcers Pressure ulcers cannot be observed due to necrotic
tissue (including eschar or slough) that obscurestissue (including eschar or slough) that obscures visualization of the wound base A pressure ulcer that is covered with slough or eschar cannot be
staged until the wound bed is visible (even if previously staged) g ( p y g )4b-Q98-98.1
Non-removable dsg or cast Until the SDTI evolves and opens, the Stage will be p g
considered NA, as the wound bed cannot be visualized
NA—M1320v.M1324
M1324 St
299
Only those covered Non-removable
M1320 Healing Status M1324 Stage
with non-removable dressing or device
dressing or device Eschar and/or slough SDTI not evolved
TheSpecificsonSuturedPressureUlcersp
How do I categorize a pressure ulcer that has beenHow do I categorize a pressure ulcer that has been sutured closed?Since it is relatively uncommon to encounter direct
t l f l it i i t t tsuture closure of a pressure ulcer, it is important to make sure that the pressure ulcer was not closed by a surgical procedure (such as a skin advancement flap rotation flap or muscle flap) Aadvancement flap, rotation flap, or muscle flap). A pressure ulcer that is sutured closed (without a flap procedure) would still be reported as a pressure ulcer While this approach (direct suture closure)ulcer. While this approach (direct suture closure) may rarely be attempted due to a low success rate, home care providers are reporting occurrence.
4b-Q89.2

SuturedPressureUlcer
Since the pressure ulcer is sutured
X
Since the pressure ulcer is sutured closed, the pressure ulcer is
id d t blXconsidered unstageable.Treated as unstageable due to non-g
removable dressing or device. 4b-Q89.2
M1308-d1M1308 d1M1310-M1314-Leave blankM1320-NAM1320 NAM1324-NA
TheSpecificsonPressureUlcersWithSkin GraftsSkinGrafts
Mrs Rose was admitted for aftercare post skinMrs. Rose was admitted for aftercare post skin graft of a Stage III pressure ulcer of the hip with orders for the pressure dressing to remain in place until the patient’s first office visitplace until the patient s first office visit.
What will you report at the SOC assessment for M1308, M1320, and M1324?
M1308 d1M1320 NAM1320 NAM1324 NA
4b-Q98.5
PressureUlcers/SkinGrafts/HealedCMSQ&A July2010Q&AJuly2010
At Discharge, Mrs. Rose’s graft site has healed with some contracture and discoloration of the grafted site, and full epithelialization what is the appropriate
f M1308 M1320 dresponse for M1308, M1320, and M1324?
4b Q98 54b-Q98.5
PressureUlcers/SkinGrafts/Healed
1
0 0
11
0
1
ZE
0
0
ROES0
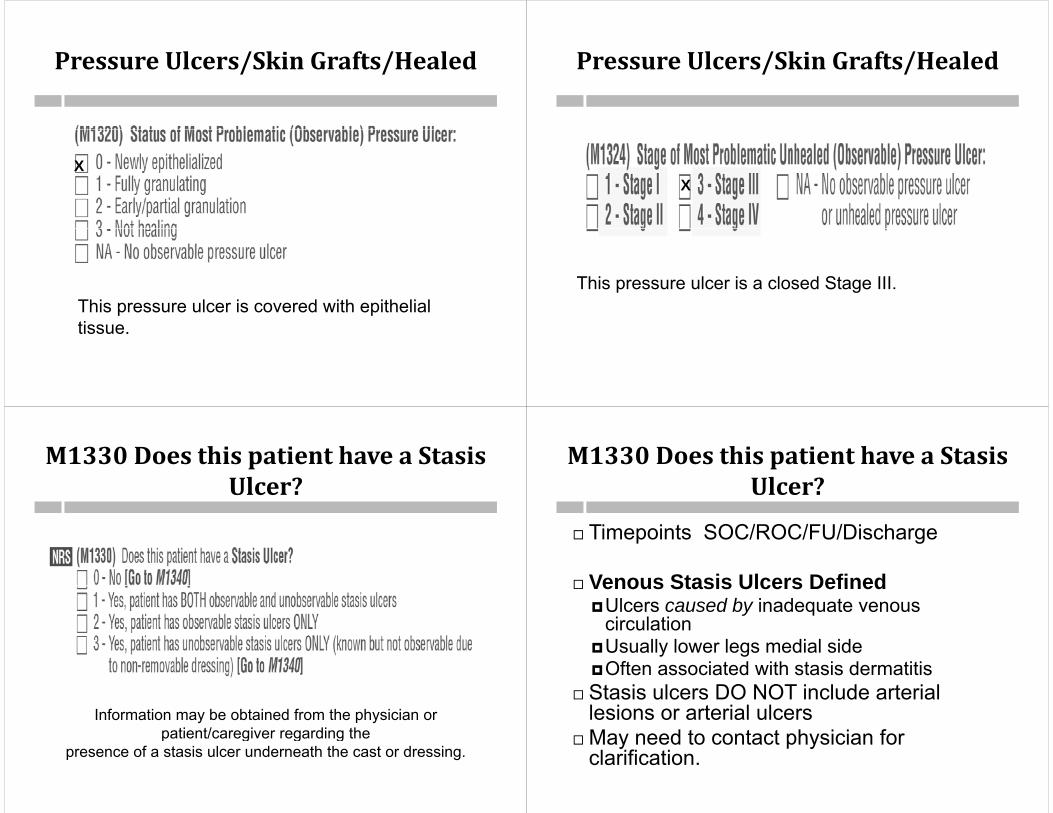
PressureUlcers/SkinGrafts/Healed
X
This pressure ulcer is covered with epithelial tissuetissue.
PressureUlcers/SkinGrafts/Healed
X
Thi l i l d St IIIThis pressure ulcer is a closed Stage III.
M1330DoesthispatienthaveaStasisUlcer?Ulcer?
Information may be obtained from the physician or patient/caregiver regarding thepatient/caregiver regarding the
presence of a stasis ulcer underneath the cast or dressing.
M1330DoesthispatienthaveaStasisUlcer?Ulcer?
Timepoints SOC/ROC/FU/Discharge Timepoints SOC/ROC/FU/Discharge
Venous Stasis Ulcers Defined Venous Stasis Ulcers DefinedUlcers caused by inadequate venous
circulationUsually lower legs medial sideOften associated with stasis dermatitisS i l DO NOT i l d i l Stasis ulcers DO NOT include arterial lesions or arterial ulcersMay need to contact physician for May need to contact physician for clarification.

M1330Q&AJan2013Q J
Our patient’s lower extremity wound originated as a d d f ll Th i l h
309
trauma wound due to a fall. The patient also has diagnoses of venous insufficiency and stasis dermatitis. The physician stated the wound is not healing due to the venous insufficiency Is there ahealing due to the venous insufficiency. Is there a point in time when the wound is no longer classified as a traumatic wound and considered a stasis ulcer for M1330?for M1330?
M1330, “Does this patient have a Stasis Ulcer?” identifies patients with ulcers caused by inadequate circulation in the area affected The healing process ofcirculation in the area affected. The healing process of other types of wounds, e.g. traumatic wounds, surgical wounds, burns, etc., may be impacted by the venous insufficiency but it would not change thevenous insufficiency, but it would not change the traumatic or surgical wound into a venous stasis ulcer.
M1332CurrentNumberof(Observable)Stasis UlcerStasisUlcer
M1332CurrentNumberof(Observable) Stasis Ulcer(s)(Observable)StasisUlcer(s)
Timepoints SOC/ROC/FU/DischargeTimepoints SOC/ROC/FU/Discharge
All stasis ulcers except those that are covered by a nonremovable dressing or y gcast are considered observable.
M1334StatusofMostProblematic(Observable) Stasis Ulcer(Observable)StasisUlcer

M1334StatusofMostProblematic(Observable) Stasis Ulcer(Observable)StasisUlcer
Ti i t SOC/ROC/FU/Di hTimepoints SOC/ROC/FU/Discharge Identifies the degree of healing present g g p
in the most problematic, observable stasis ulcer.
If the patient has only one stasis ulcer, that ulcer is the most problematic.that ulcer is the most problematic.
Do not use Newly epithelialized!Stasis ulcers once epithelialized are noStasis ulcers, once epithelialized, are no
longer stasis ulcers.
M1340DoesthispatienthaveaSurgical Wound?SurgicalWound?
• Timepoints SOC/ROC/FU/Discharge• Old surgical wounds that have resulted in
k l id f ti t id dscar or keloid formation are not considered current surgical wounds and should not be included in this itemincluded in this item.
M1340DoesthispatienthaveaSurgical Wound?SurgicalWound?
For the purpose of this OASIS item, a surgical site closed primarily (witha surgical site closed primarily (with sutures, staples or a chemical bonding agent) is generally described inagent) is generally described in documentation as a surgical wound until re epithelialization has beenuntil re-epithelialization has been present for approximately 30 days, unless it dehisces or presents signs ofunless it dehisces or presents signs of infection.
M1340DoesthispatienthaveaSurgical Wound?SurgicalWound?
After 30 days, it is generally described as a scar and should not be included in this item. If the home health clinician conducting the assessment is not sure the wound fits the definition of a surgical incision, the clinician should contact the physician for clarification.
How many days since surgery?y y g y
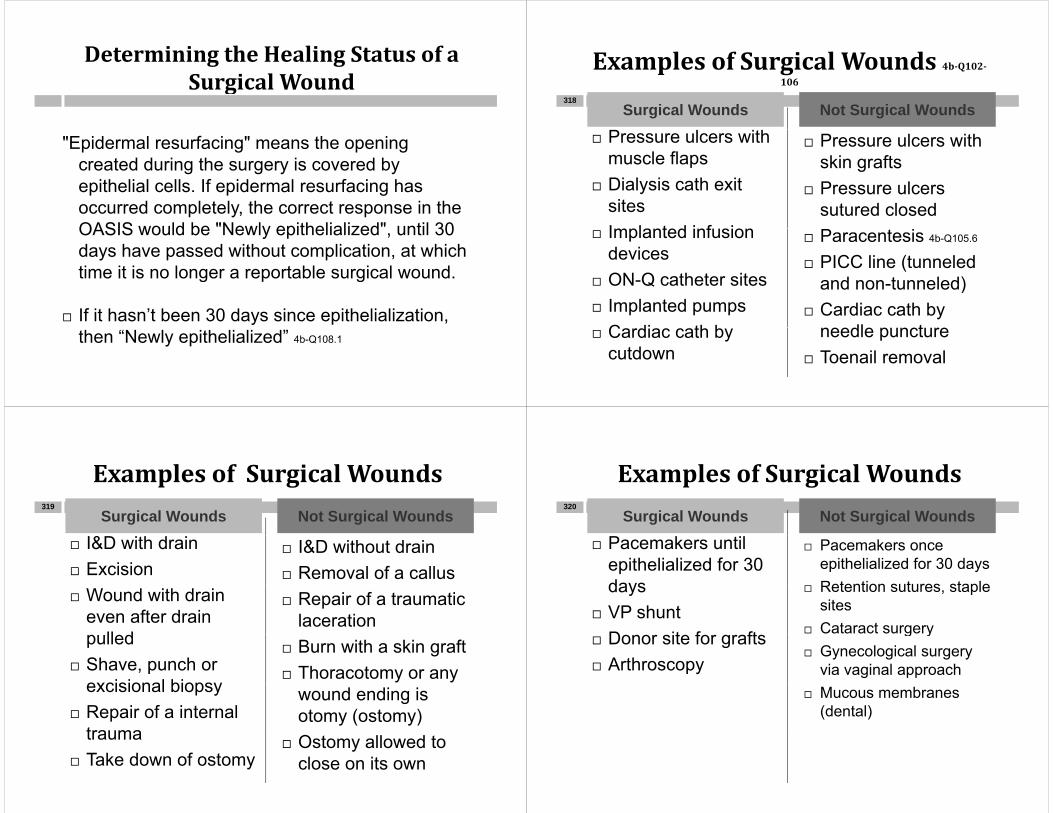
DeterminingtheHealingStatusofaSurgical WoundSurgicalWound
"Epidermal resurfacing" means the opening created during the surgery is covered by
f fepithelial cells. If epidermal resurfacing has occurred completely, the correct response in the OASIS would be "Newly epithelialized" until 30OASIS would be Newly epithelialized , until 30 days have passed without complication, at which time it is no longer a reportable surgical wound.time it is no longer a reportable surgical wound.
If it hasn’t been 30 days since epithelialization, then “Newly epithelialized” 4b-Q108.1
ExamplesofSurgicalWounds4b‐Q102‐106106
Surgical Wounds Not Surgical Wounds318
Pressure ulcers with muscle flapsDi l i th it
Pressure ulcers with skin grafts
Dialysis cath exit sitesImplanted inf sion
Pressure ulcers sutured closed
Implanted infusion devices
ON Q catheter sites
Paracentesis 4b-Q105.6
PICC line (tunneled d t l d) ON-Q catheter sites
Implanted pumpsC di th b
and non-tunneled) Cardiac cath by
dl t Cardiac cath by cutdown
needle puncture Toenail removal
ExamplesofSurgicalWoundsp gSurgical Wounds Not Surgical Wounds
319
I&D with drain Excision
I&D without drain Removal of a callus
Wound with drain even after drain p lled
Repair of a traumatic laceration
pulled Shave, punch or
excisional biopsy
Burn with a skin graft Thoracotomy or any
excisional biopsy Repair of a internal
trauma
wound ending is otomy (ostomy)
trauma Take down of ostomy
Ostomy allowed to close on its own
ExamplesofSurgicalWoundsp gSurgical Wounds Not Surgical Wounds
320
Pacemakers until epithelialized for 30 days
Pacemakers once epithelialized for 30 days
Retention sutures stapledays VP shunt
Donor site for grafts
Retention sutures, staple sites
Cataract surgery Donor site for grafts Arthroscopy
g y Gynecological surgery
via vaginal approach Mucous membranes
(dental)

SurgicalWoundorThoracotomy?
A surgical incision was created to perform A surgical incision was created to perform exploratory surgery. When closing the wound, the surgeon inserted a chest tube utilizing the opening created for the surgery. Can this closed incision with a chest tube be counted as a
i l d h l ti M1340?surgical wound when completing M1340? The wound described should be considered a
thoracostomy and is not considered a surgicalthoracostomy and is not considered a surgical wound when completing the OASIS data set item M1340item M1340.
• 4b-Q105.16.1
Mammosite DeviceinaLumpectomy SiteLumpectomySite
Receives radiation bead insertion through this catheter Receives radiation bead insertion through this catheter
X
X
Kyphoplastyyp p y
If the kyphoplasty procedure was If the kyphoplasty procedure was performed percutaneously and resulted in a pinpoint needle puncture site wherein a pinpoint needle puncture site where the bone cement was injected, it would not be considered a surgical woundnot be considered a surgical wound.
If the kyphoplasty procedure involved an h i i i lopen approach, requiring a surgical
incision, the resulting wound would be id d i l d f M1340considered a surgical wound for M1340.
M1342StatusofMostProblematic(Observable) Surgical Wound(Observable)SurgicalWound
Status of healing definitions apply to surgical wounds h li b i i t ti d t th h li bhealing by primary intention and to those healing by secondary intention.

M1342StatusofMostProblematic(Observable)SurgicalWound( ) g
• Timepoints SOC/ROC/FU/Discharge• Timepoints SOC/ROC/FU/Discharge • Patient has only one observable
surgical wound that wound is the mostsurgical wound, that wound is the most problematicM t bl ti b• Most problematic may be LargestMost resistantInfected surgical wound, etc., depending on
the specific situation.
Newlyepithelialized
wound bed completely wound bed completely covered with new epithelium
no exudate no avascular tissue
(eschar and/or slough) no signs or symptoms of
infection (Newly epithelialized for
30 days when closed by primary intention)
FullyGranulating
wound bed filled with wound bed filled with granulation tissue to the level of the surrounding skin
no dead space no avascular tissue
(eschar and/or slough) no signs or symptoms
of infection wound edges are
open
Early/PartialGranulation
≥ 25% of the wound bed is covered≥ 25% of the wound bed is covered with granulation tissue
< 25% of the wound bed is covered with avascular tissue (eschar(and/or slough)
no signs or symptoms of infectionno signs or symptoms of infectionwound edges open

NotHealing
≥ 25% avascular tissue OR
S/S of infection ORClean but non Clean but non granulating wound bed OR
Closed/hyperkeratoticwound edges OR
Persistent failure to Persistent failure to improve despite appropriate comprehensive woundcomprehensive wound management
GuidanceonSurgicalWoundsHealingbyPrimary IntentionPrimaryIntention
Surgical incisions healing by primary g g y p yintention do not granulate. Because of this the only response that could be appropriate for a surgical wound healing by primaryfor a surgical wound healing by primary intention would be: 0-Newly epithelialized or y p 3-Not healing. 4b-Q112.5.2
“Newly epithelialized” should be chosen if the s rgical incision has epidermalthe surgical incision has epidermal resurfacing across the entire wound surface, and no signs/symptoms of , g y pinfection exist.
ImplantedVenousAccessDevicesDevices
Response 0 pFor implanted venous access devices and
infusion devices when the insertion site is healed.When first implanted the incision is the When first implanted, the incision is the surgical wound. The assessing clinician will follow the 12/09 WOCN guidance to gdetermine the healing status of the incision. Once it is fully epithelialized, the site due to the implanted device will remain a currentthe implanted device will remain a current surgical wound with a status of “Newly epithelialized" for as long as it is present in the patient's body, unless it later develops complications. 4b-Q105.3
GuidanceonVascularAccessDevices
If an extremely large bore needle or traumatic y gentry or removal occurs there may be a resulting wound that heals by secondary intention. A scab may mean that full epithelialization has not y poccurred, therefore look to WOCN guidance to determine healing status. 4b-Q112.6
Some sites, because they are being held open by a drain, line or needle, cannot fully granulate and may remain "non-healing" while the drain, line or needle is in place. 4b-Q112.6.1

DeterminingtheHealingStatusofaSurgical WoundSurgicalWound
1st Determine if the surgical incision is healing by: P i I i Ed ll i d Primary Intention: Edges well approximated
OR Secondary intention: Due to dehiscence or interruption Secondary intention: Due to dehiscence or interruption
of the incision. If the wound is healing solely by primary intention, the
assessing clinician will observe if the incision line has re-gepithelialized. (If there is no interruption in the healing process, this generally takes from a matter of hours to three days.)
If there is not full epithelial resurfacing, such as in the case of a scab adhering to underlying tissue, then the correct g y g ,response would be "not healing" for the wound healing by primary intention.
DeterminingtheHealingStatusofaSurgical WoundSurgicalWound
The presence of a scab does not automaticallyThe presence of a scab does not automatically equate to a "not healing" response. The clinician must first assess if the wound is healing entirely by primary intention (complete closure with noby primary intention (complete closure with no openings), or if there is a portion healing by secondary intention.
If it is determined that there is incisionalseparation, healing will be by secondary intention, and the clinician will then have to ,determine the status of healing, which may be "Not healing” "Early/partial granulation” "Fully granulating" and eventually "Newlygranulating and eventually Newly epithelialized".
WoundHealingbySecondaryIntentionIntention
M1350DoesthispatienthaveaSkinLesion or OpenWound, other than…LesionorOpenWound,otherthan…

M1350DoesthispatienthaveaSkinLesion or OpenWoundLesionorOpenWound
Timepoints SOC/ROC/FU/Dischargep g Identifies the presence or absence of a skin lesion
or open wound NOT ALREADY ADDRESSED IN PREVIOUS ITEMS h i i i li i lPREVIOUS ITEMS that is receiving clinical assessment or intervention from the home health agency.health agency. Does not include: bowel ostomies, pressure
ulcers, stasis ulcers and surgical woundsDoes include: peripheral IVs, all other ostomies,
all other skin lesions and open wounds B t l l th ki l iBut only as long as those skin lesions or open wounds require assessment or intervention
M1350DoesthispatienthaveaSkinLesion or OpenWoundLesionorOpenWound
A lesion is a broad term used to describe an area of pathologically altered tissuepathologically altered tissue Sores Skin tears Burns Ulcers (except pressure and stasis) Rashes Diabetic ulcers Cellulitis Abscesses Wounds caused by trauma of various kinds, etc.
Primary lesions, secondary lesions, changes in shape (edema), texture, color, breaks in skin and vascular(edema), texture, color, breaks in skin and vascular lesions
4b-Q112.7
M1350DoesthispatienthaveaSkinLesion or OpenWoundLesionorOpenWound
Skin lesions or open wounds that are not receiving clinical intervention from the homereceiving clinical intervention from the home health agency should not be considered when responding to this questionwhen responding to this question.
Any skin condition that is being clinically assessed on an ongoing basis as indicatedassessed on an ongoing basis as indicated on the POC (e.g., wound measurements), h ld b d “Y ”should be answered “Yes.”
M1350DoesthispatienthaveaSkinLesion or OpenWoundLesionorOpenWound
PICC line and peripheral IV sites are PICC line and peripheral IV sites are considered skin lesions / open wounds. Ostomies other than bowel ostomies (e g Ostomies, other than bowel ostomies, (e.g., tracheostomy, thoracostomy, urostomy) ARE considered to be skin lesions or openARE considered to be skin lesions or open wounds if clinical interventions (e.g., cleansing dressing changes) are beingcleansing, dressing changes) are being provided by the home health agency during the home health care episode. p

M1350ExcludesBowelOstomies
“E l d b l t i ” “Excludes bowel ostomies” means those ostomies that are used for b l li i tibowel elimination.
Gastrostomies and jejunostomies are j jnot considered bowel ostomies. (G tubes and J tubes are reported in pM1350)
• 4b-Q112.10.1
M1350DoesthispatienthaveaSkinLesion or OpenWoundLesionorOpenWound
This item does not address/include This item does not address/includecataract surgery surgery to mucosal membranessurgery to mucosal membranesgynecological surgical procedures by a vaginal
approachapproach. This item does not address/include
tattoos tattoosPiercingsOr other skin alterations unless ongoingOr other skin alterations unless ongoing
assessment and/or clinical intervention is ordered on the POC
QuizQ
Our patient had a burn with orders for the nurse to d h h d i i kl Th
343
assess and change the dressing twice weekly. The patient is leaving the geographical area. The PT is making the last visit and completing the Discharge comprehensive assessment She will not be changingcomprehensive assessment. She will not be changing the burn dressing on the discharge visit. How do we answer M1350? Is M1350 asking whether or not the agency provided intervention to the wound on the dayagency provided intervention to the wound on the day of discharge or is it asking whether or not the patient had a wound on the day of assessment that required intervention from the agency, even though they didn'tintervention from the agency, even though they didn t receive a specific intervention on the day of the discharge? 4b-Q112.13
Intervention does not have to be performed on THAT day.
R i S M1400RespiratoryStatusM1400s
RESPIRATORY STATUS
344
RESPIRATORY STATUS

M1400Whenisthepatientdyspneicornoticeably Short of Breath?noticeablyShortofBreath?
M1400Whenisthepatientdyspneicornoticeably Short of Breath?noticeablyShortofBreath?
Timepoints SOC/ROC/FU/DischargeTimepoints SOC/ROC/FU/DischargeHow to assess?If patient uses oxygen continuouslyAssess with oxygen in use
If the patient uses oxygen intermittentlyAssess without the use of oxygenyg
What if ordered continuously but only used intermittently?used intermittently?
Sleep apnea ≠ dyspnea
M1400WhenisthepatientdyspneicornoticeablyShort of Breath?ShortofBreath?
Chairfast or bedbound patient:Chairfast or bedbound patient:Evaluate the level of exertion required to
produce shortness of breathproduce shortness of breathThe chairfast patient can be assessed for
le el of d spnea hile performing ADLs orlevel of dyspnea while performing ADLs or at rest
R 0• Response 0 Patient has not been short of breath
during the day of assessment
M1400Whenisthepatientdyspneicornoticeably Short of Breath?noticeablyShortofBreath?
Chairfast or bedbound patient:• Response 1 (When walking more than 20 p ( g
feet…)• Appropriate if demanding bed-mobility activities
d d i th b db d ti t (produce dyspnea in the bedbound patient (or physically demanding transfer activities produce dyspnea in the chairfast patient).dyspnea in the chairfast patient).
Responses 2, 3, and 4 for assessment examples for these patients as well as p pambulatory patients.

M1410RespiratoryTreatments M1410RespiratoryTreatments
Timepoints SOC/ROC/DischargeExcludes any respiratory treatmentsExcludes any respiratory treatments
that are not listed in the itemDoes not include nebulizers inhalersDoes not include nebulizers, inhalers
Option 3 reflects both CPAP and BiPAP.
M1410—RespiratoryTreatments
You are completing a D/C OASIS on Mr. Martinez. The 485 i l d PRN d f i / Y485 includes a PRN order for oxygen via n/c. You have reviewed the chart and noticed there was no mention of oxygen use on any skilled notes. You interview the patient and the caregiver and they state oxygen has not been used since Mr. Martinez’s admission to home health. 4b-Q114.2
How will you answer M1410- Respiratory Treatments ( til t CPAP BiPAP) tili d t(oxygen, ventilator, CPAP, BiPAP) utilized at home?
X
C di S M1500CardiacStatusM1500s352

M1500SymptomsinHeartFailurePatientsPatients
M1500SymptomsinHeartFailurePatientsPatients
Identifies if patient has experienced signs/ Identifies if patient has experienced signs/ symptoms of heart failure at time of most recent OASIS assessment or since that time
Used to calculate process measures to pcapture the agency’s use of best practices
The best practices/assessments stated in The best practices/assessments stated in the item are not necessarily required in the Conditions of Participation.p
M1500SymptomsinHeartFailurePatientsPatients
Timepoints Transfer Discharge Timepoints Transfer Discharge If patient has a diagnosis of heart failure in
M1010 Inpatient DiagnosisM1010 Inpatient DiagnosisM1016 Diagnoses Causing Chg in TreatmentM1020/1022/1024 Primary/Secondary dx OR anyM1020/1022/1024 Primary/Secondary dx OR any
other place on the comprehensive assessment ( regardless of whether the diagnosis is documented elsewhere in the OASIS assessment)elsewhere in the OASIS assessment).
Clinician will select Response options 0, 1, or 2 Select “NA” if the patient does not have a Select NA if the patient does not have a
diagnosis of heart failure AT ALL.
M1500SymptomsinHeartFailurePatientsPatients
ConsiderNew or ongoing heart failure symptoms since
previous OASIS Review clinical record
physical assessment datai ht t d weight trends
clinical notes D i t f h t f il d hil itDyspnea is a symptom of heart failure and while it may
also be a symptom of another co-existing disease process, such as pneumonia, it would still be reported p p pin M1500 and M1510, Heart Failure Follow-up, if the patient has a diagnosis of heart failure.
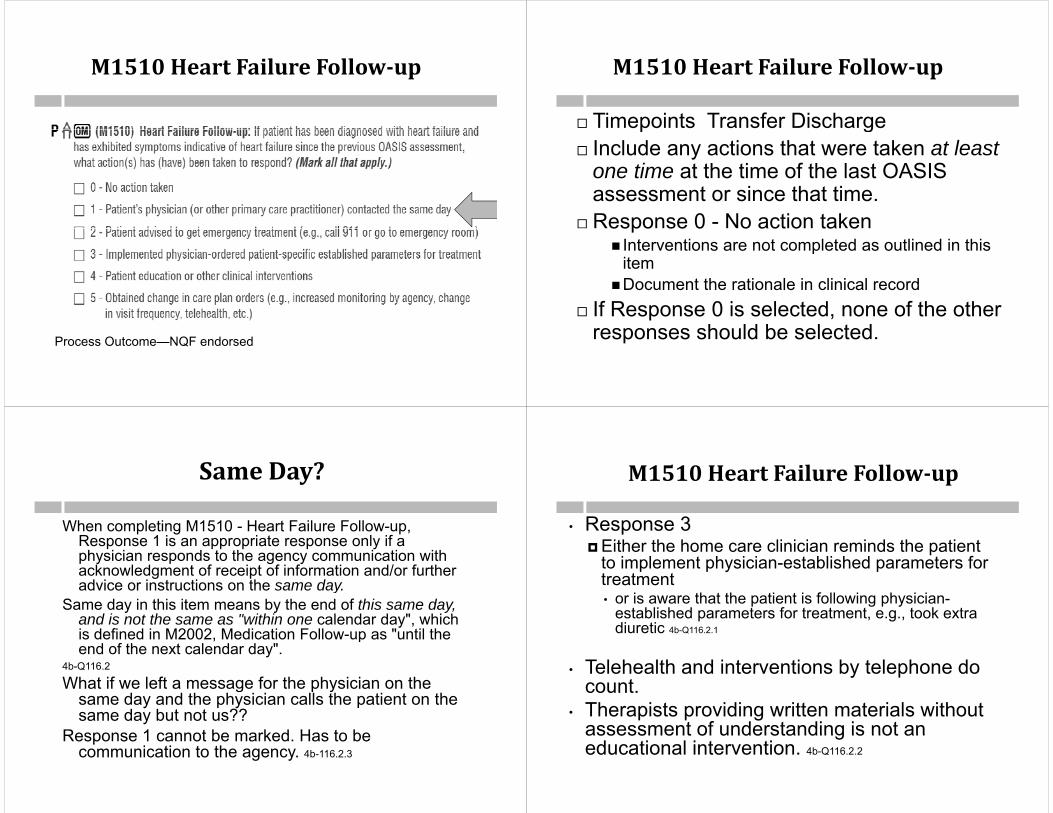
M1510HeartFailureFollow‐up
Process Outcome—NQF endorsed
M1510HeartFailureFollow‐up
Timepoints Transfer Dischargep g Include any actions that were taken at least
one time at the time of the last OASIS assessment or since that time.
Response 0 - No action takenespo se 0 o act o ta e Interventions are not completed as outlined in this
item Document the rationale in clinical record
If Response 0 is selected, none of the other h ld b l t dresponses should be selected.
SameDay?
When completing M1510 - Heart Failure Follow-up, R 1 i i t l ifResponse 1 is an appropriate response only if a physician responds to the agency communication with acknowledgment of receipt of information and/or further advice or instructions on the same dayadvice or instructions on the same day.
Same day in this item means by the end of this same day, and is not the same as "within one calendar day", which is defined in M2002 Medication Follow-up as "until theis defined in M2002, Medication Follow-up as until the end of the next calendar day".
4b-Q116.2
What if we left a message for the physician on theWhat if we left a message for the physician on the same day and the physician calls the patient on the same day but not us??
Response 1 cannot be marked Has to beResponse 1 cannot be marked. Has to be communication to the agency. 4b-116.2.3
M1510HeartFailureFollow‐up
• Response 3 Either the home care clinician reminds the patient
to implement physician-established parameters for treatmentea e• or is aware that the patient is following physician-
established parameters for treatment, e.g., took extra diuretic 4b-Q116.2.1
• Telehealth and interventions by telephone do countcount.
• Therapists providing written materials without assessment of understanding is not anassessment of understanding is not an educational intervention. 4b-Q116.2.2
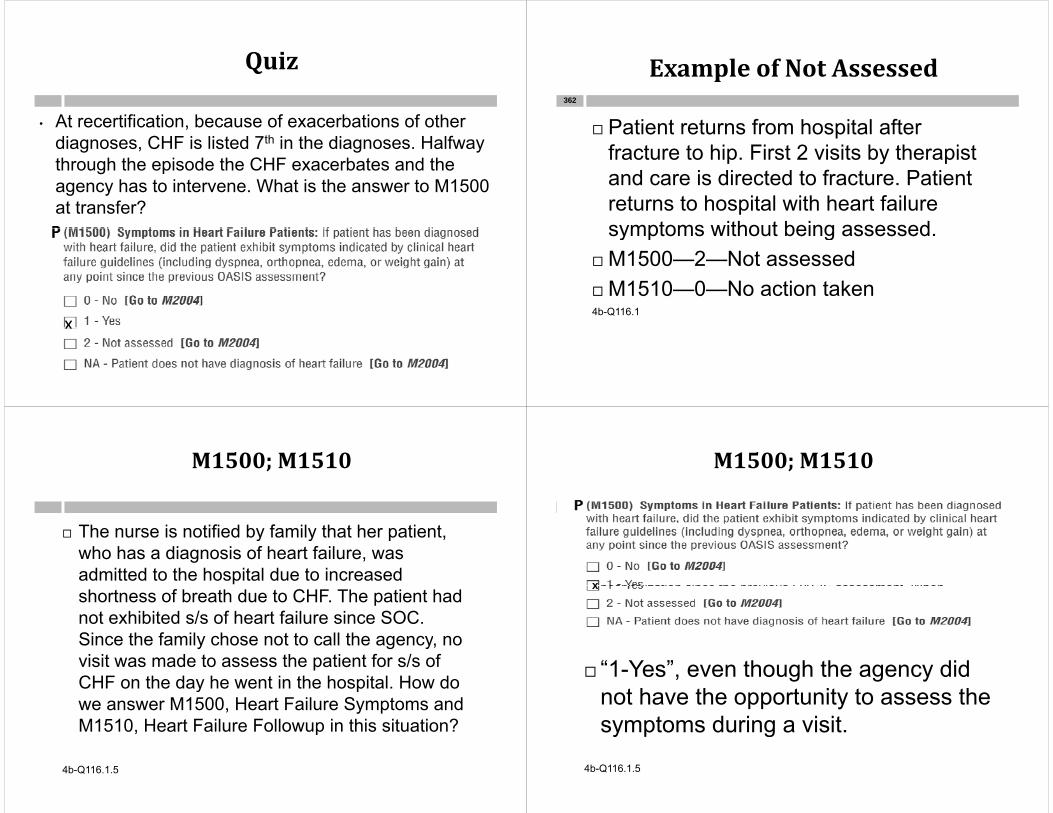
Quiz
• At recertification, because of exacerbations of other ,diagnoses, CHF is listed 7th in the diagnoses. Halfway through the episode the CHF exacerbates and the agency has to intervene. What is the answer to M1500 at transfer?
XX
ExampleofNotAssessedp
Patient returns from hospital after362
Patient returns from hospital after fracture to hip. First 2 visits by therapist and care is directed to fracture Patientand care is directed to fracture. Patient returns to hospital with heart failure symptoms without being assessedsymptoms without being assessed.
M1500—2—Not assessed M1510—0—No action taken4b-Q116.1
M1500;M1510
The nurse is notified by family that her patient, The nurse is notified by family that her patient, who has a diagnosis of heart failure, was admitted to the hospital due to increased shortness of breath due to CHF. The patient had not exhibited s/s of heart failure since SOC. Si th f il h t t ll thSince the family chose not to call the agency, no visit was made to assess the patient for s/s of CHF on the day he went in the hospital How doCHF on the day he went in the hospital. How do we answer M1500, Heart Failure Symptoms and M1510, Heart Failure Followup in this situation?, p
4b-Q116.1.5
M1500;M1510
“1-Yes” is the appropriate response if the patient had a diagnosis of heart failure and exhibited symptoms of heart failure at or since the previous OASIS assessment. In your scenario, the patient had a diagnosis of heart failure and the record review revealed that the patient experienced SOB which resulted in a qualifying hospitalization since the previous OASIS assessment Whenx hospitalization since the previous OASIS assessment. When completing the Transfer OASIS, the clinician would answer M1500
x
“1-Yes”, even though the agency did not have the opportunity to assess the symptoms during a visit.y p g
4b-Q116.1.5

x
When answering M1510, Heart Failure Follow-up, you report the actions your agency took inyou report the actions your agency took in response to the heart failure symptoms and if none were taken, Response “0-No action taken” would be appropriate. Include an explanation of the "No" in the clinical record. 4b-Q116.1.5
Eli i i S M1600EliminationStatusM1600s366
M1600 UTI in the past 14 days?M1600UTIinthepast14days?M1600HasthispatientbeentreatedforaUrinary
Tract Infection in the past 14 days?TractInfectioninthepast14days?
Timepoints SOC ROC DischargeTimepoints SOC ROC DischargeResponse 0-No Patient has not been treated for a UTI
within the past two weekspPatient may have had symptoms of a
UTI or a positive culture for which theUTI or a positive culture for which the physician did not prescribe treatment
Or treatment ended more than 14 daysOr treatment ended more than 14 days ago

M1600HasthispatientbeentreatedforaUrinaryTractInfectioninthepast14days?p y
Response 1-YespPatient has been prescribed an antibiotic
within the past 14 days specifically for a confirmed or suspected UTI.
Patient is on prophylactic treatment and develops a UTI.
Response NApPatient is on prophylactic treatment to
prevent UTIs.UK not an option at discharge
M1600
My patient has an order for Sulfa BID x5 days, during h fi fi d f h U SOCthe first five days of every month. Upon my SOC
assessment on 11/1, the patient complained of s/s of UTI. The physician was notified, but no order was obtained for a urinalysis since the patient was justobtained for a urinalysis since the patient was just beginning her prophylactic treatment that day. How should I answer M1600?If th ti t tibi ti d d l d UTI If the patient was on antibiotics and developed a UTI, the answer would be ‘Yes”.
The physician must diagnose a UTI to answer ‘yes’ so th i NAthe answer is NA.
4b-Q116.6
M1610UrinaryIncontinenceorUrinary Catheter PresenceUrinaryCatheterPresence
M1610UrinaryIncontinenceorUrinaryCatheter PresenceCatheterPresence
Ti i t SOC/ROC/DC• Timepoints SOC/ROC/DC • Response 0-No incontinence or anuriapPatient has anuria or an ostomy for
urinary drainage (e.g., an ileal conduit)urinary drainage (e.g., an ileal conduit)Patient has a urinary diversion that is
pouched (ileal conduit urostomypouched (ileal conduit, urostomy, ureterostomy, nephrostomy), with or without a stomawithout a stoma

M1610UrinaryIncontinenceorUrinaryCatheter PresenceCatheterPresence
Response 1-Patient is incontinentResponse 1 Patient is incontinentIf patient is incontinent AT ALL (i.e.,
“occasionally ” “only when I sneeze ”occasionally, only when I sneeze, “sometimes I leak a little bit,” etc.)
Patient is incontinent or is dependent onPatient is incontinent or is dependent on a timed-voiding programTimed voiding is defined as scheduled g
toileting assistance or prompted voiding to manage incontinence based on identified patterns Time voiding is a compensatorypatterns. Time voiding is a compensatory strategy; it does not cure incontinence.
M1610UrinaryIncontinenceorUrinaryCatheter PresenceCatheterPresence
R 2 Pt i i th t Response 2 Pt requires urinary catheterCatheter or tube is utilized for drainage
(even if catheterizations are intermittent).Patient requires the use of a urinary q y
catheter for any reason (e.g., retention, postsurgery, incontinence). g y )
Select Response 2 and follow the skip pattern if the patient is both incontinent p pand requires a urinary catheter.
M1610UrinaryIncontinenceorUrinaryCatheterPresence
Does the patient admit having difficulty Does the patient admit having difficulty controlling the urine?
Do you have orders to change a catheter? Do you have orders to change a catheter? Is your stroke patient using an external
catheter? Any odors? Consider
Physiologic reasonsCognitive impairmentsMobility problems
M1615WhendoesUrinaryIncontinenceOccur?Occur?
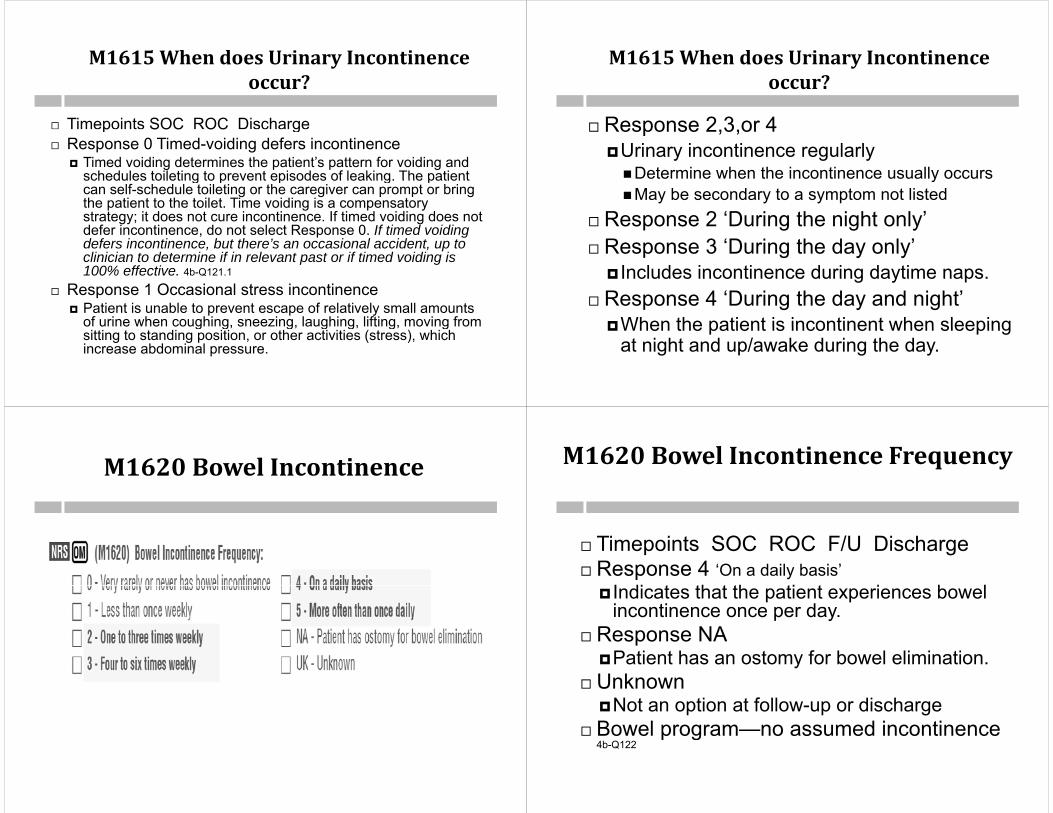
M1615WhendoesUrinaryIncontinenceoccur?occur?
Timepoints SOC ROC Dischargep SOC OC g Response 0 Timed-voiding defers incontinence
Timed voiding determines the patient’s pattern for voiding and schedules toileting to prevent episodes of leaking The patientschedules toileting to prevent episodes of leaking. The patient can self-schedule toileting or the caregiver can prompt or bring the patient to the toilet. Time voiding is a compensatory strategy; it does not cure incontinence. If timed voiding does not defer incontinence do not select Response 0 If timed voidingdefer incontinence, do not select Response 0. If timed voiding defers incontinence, but there’s an occasional accident, up to clinician to determine if in relevant past or if timed voiding is 100% effective. 4b-Q121.1
Response 1 Occasional stress incontinence Patient is unable to prevent escape of relatively small amounts
of urine when coughing, sneezing, laughing, lifting, moving from g g, g, g g, g, gsitting to standing position, or other activities (stress), which increase abdominal pressure.
M1615WhendoesUrinaryIncontinenceoccur?occur?
Response 2 3 or 4 Response 2,3,or 4Urinary incontinence regularly Determine when the incontinence usually occurs yMay be secondary to a symptom not listed
Response 2 ‘During the night only’p g g y Response 3 ‘During the day only’
Includes incontinence during daytime naps. Includes incontinence during daytime naps. Response 4 ‘During the day and night’
When the patient is incontinent when sleepingWhen the patient is incontinent when sleeping at night and up/awake during the day.
M1620BowelIncontinence M1620BowelIncontinenceFrequency
Ti i SOC ROC F/U Di h Timepoints SOC ROC F/U Discharge Response 4 ‘On a daily basis’
I di t th t th ti t i b l Indicates that the patient experiences bowel incontinence once per day.
Response NA Response NAPatient has an ostomy for bowel elimination.
Unknown UnknownNot an option at follow-up or discharge
Bowel program—no assumed incontinence Bowel program no assumed incontinence 4b-Q122

M1620BowelIncontinenceFrequency
Review the bowel elimination patternDifficulty controlling stoolsDiarrhea
Note cleanlinessAround the toilet ClothingClothingAt F/U may ask the aide
Consider ConsiderPhysiologic reasonsCognitive impairmentsMobility problems
M1630—Ostomy for Bowel EliminationM1630 OstomyforBowelElimination
M1630Ostomy forBowelElimination
Timepoints SOC ROC FUTimepoints SOC ROC FU
Add b l t i ONLYAddresses bowel ostomies ONLYApplies to any type of ostomy for bowel
li i ti ( l t il t )elimination (e.g., colostomy, ileostomy)
If an ostomy has been reversed, then the patient does not have an ostomy at the time of assessment
N /E i l/B h i l
M1700
Neuro/Emotional/Behavioral384
M1700s
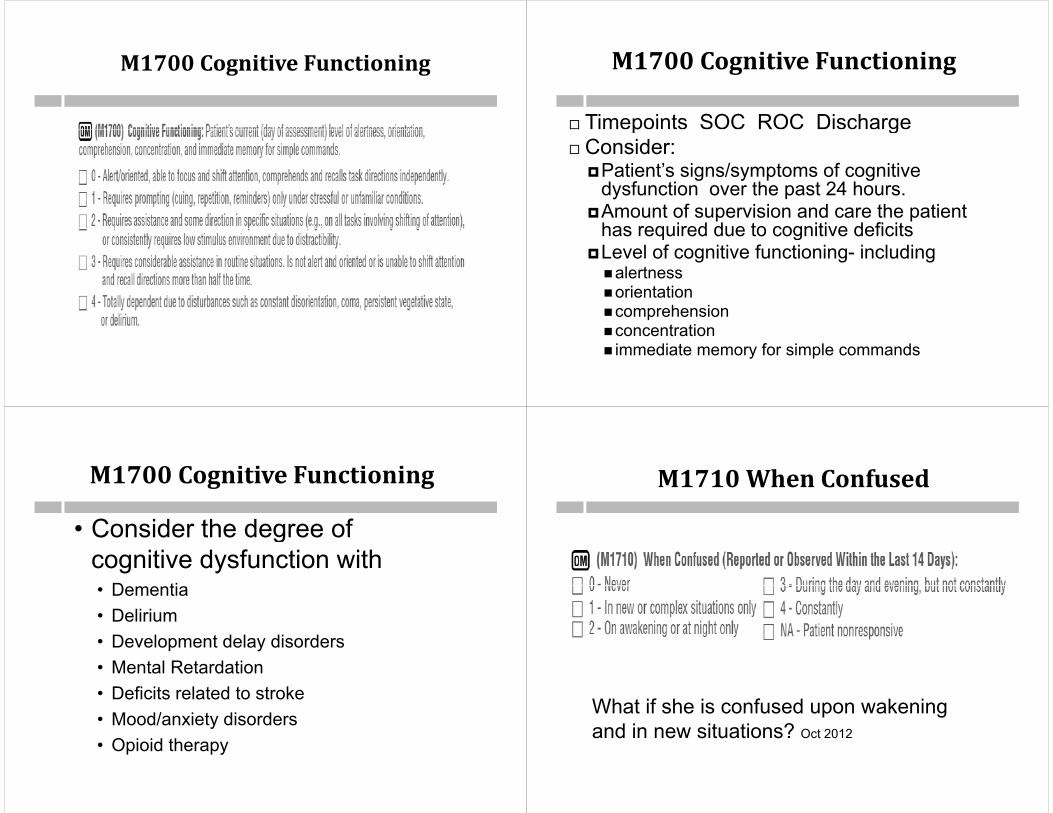
M1700CognitiveFunctioning M1700CognitiveFunctioning
Timepoints SOC ROC Dischargep g Consider:
Patient’s signs/symptoms of cognitive g y p gdysfunction over the past 24 hours.
Amount of supervision and care the patient has required due to cognitive deficitshas required due to cognitive deficits
Level of cognitive functioning- includingalertnessalertnessorientationcomprehension
concentrationconcentration immediate memory for simple commands
M1700CognitiveFunctioningg g
• Consider the degree ofConsider the degree of cognitive dysfunction with
D ti• Dementia• Delirium
D l d l di d• Development delay disorders• Mental Retardation• Deficits related to stroke• Mood/anxiety disorders• Opioid therapy
M1710When ConfusedM1710WhenConfused
What if she is confused upon wakening and in new situations? Oct 2012and in new situations? Oct 2012

M1710WhenConfused(ReportedorObservedWithin the Last 14 Days)ObservedWithintheLast14Days)
Timepoints SOC ROC Discharge May not relate directly to Item M1700 Assess specifically for confusion in the past 14 days. If it is reported that the patient is “occasionally” confused If it is reported that the patient is occasionally confused,
identify the situation(s) in which confusion has occurred within the last 14 days, if at all.Report any episodes of confusion that occurred during the Report any episodes of confusion that occurred during the past 14 days, without regard to the cause of potential relevance of the confusion to this episode of care“N i ” th t th ti t i bl t “Nonresponsive” means that the patient is unable to respond or the patient responds in a way that you can’t make a clinical judgment about the patient’s level of orientation Examples at 4b Q124 1orientation. Examples at 4b-Q124.1
MoreGuidanceonSelectingResponseResponse
Response 1 is selected when the patient's confusion is i l t d t l it ti th ti t
390
isolated to a new or a complex situation, e.g. the patient became confused when a new caregiver was introduced or when a complicated procedure was taught for the first time. Response 2 3 & 4 are selected when confusion occurs Response 2, 3, & 4 are selected when confusion occurs without the stimulus of a new or complex situation, or when confusion which initially presented with a new or complex situation persists days after the new or complex situation p y pbecome more routine. Responses 2, 3 & 4 differ from each other based on the time when the confusion occurred.
Response 2 is selected if the confusion only occurred p ywhen the patient was awakening from a sleep or during the night.
Response 3 is selected if the confusion occurs during the d d i b t i t t t If f i tday and evening, but is not constant. If confusion was not constant, but occurred more often than just upon awakening or at night, select Response 3.
WhatisthedifferenceinwhatismeasuredinM1700– CognitiveFunctioningandM1710‐
Wh C f d?WhenConfused?
M1700--Level of alertness, orientation, , ,comprehension, concentration, and immediate memory for simple commands on the day of assessment (at the time of the assessment and in the preceding 24 h )hours).
M1710, When Confused, is intended to id tif th ti f d it ti hidentify the time of day or situations when the patient experienced confusion, if at all during the past 14 days (Day ofall, during the past 14 days (Day of assessment and prior 14 days).
M1710‐WhenConfused
Confusion is defined in Mosby's Medical Confusion is defined in Mosby s Medical Dictionary as "a mental state characterized by disorientation regarding time, place, person or sit ation It ca ses be ildermentperson, or situation. It causes bewilderment, perplexity, lack of orderly thought, and inability to choose or act decisively and y yperform the activities of daily living. It is usually symptomatic of an organic mental disorder but it may accompany severedisorder, but it may accompany severe emotional stress and various psychological disorders."
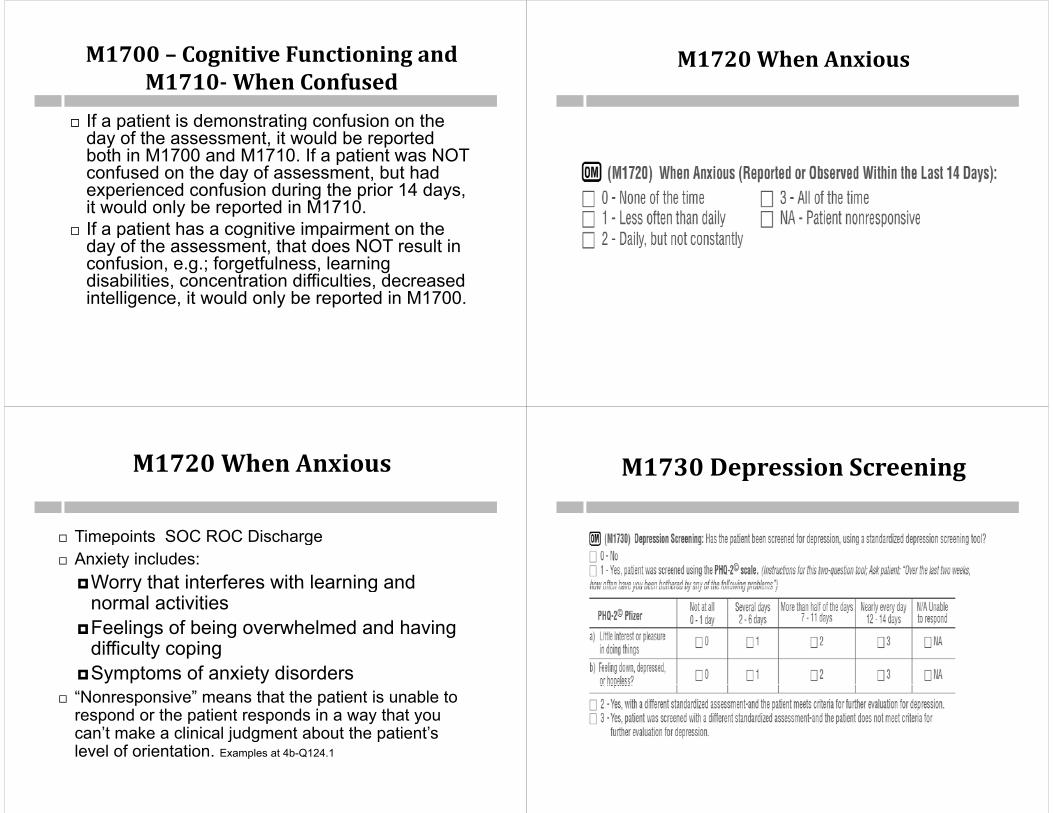
M1700– CognitiveFunctioningandM1710 When ConfusedM1710‐WhenConfused
If a patient is demonstrating confusion on the p gday of the assessment, it would be reported both in M1700 and M1710. If a patient was NOT confused on the day of assessment, but had y ,experienced confusion during the prior 14 days, it would only be reported in M1710.
If a patient has a cognitive impairment on the If a patient has a cognitive impairment on the day of the assessment, that does NOT result in confusion, e.g.; forgetfulness, learning disabilities concentration difficulties decreaseddisabilities, concentration difficulties, decreased intelligence, it would only be reported in M1700.
M1720WhenAnxious
M1720WhenAnxious
Timepoints SOC ROC Discharge Timepoints SOC ROC Discharge Anxiety includes:
Worry that interferes with learning andWorry that interferes with learning and normal activities
Feelings of being overwhelmed and having g g gdifficulty coping
Symptoms of anxiety disorders “Nonresponsive” means that the patient is unable to
respond or the patient responds in a way that you can’t make a clinical judgment about the patient’scan t make a clinical judgment about the patient s level of orientation. Examples at 4b-Q124.1
M1730DepressionScreening
M1730DepressionScreeningp g
Process Measure

M1730DepressionScreening
Timepoints SOC ROC p If using PHQ-2, then you must interview the patient.
4b-Q124.5
Depressive feelings, symptoms, and/or behaviors Depressive feelings, symptoms, and/or behaviors may be observed by the clinician or reported by the patient, family, or others, BUT another tool must be usedused.
If the patient is not cognitively able to respond then must answer 0-No, unless another tool can be
dused. If a standardized depression screening tool is used,
use the scoring parameters specified for the tool to g p pidentify if a patient meets criteria for further evaluation of depression
M1730DepressionScreening
Identifies if the agency screened the patient for depression using a standardized depression screeningdepression using a standardized depression screening tool
CMS does not mandate That patients are screened Use of the PHQ-2© or any other standardized tool
Process measures Process measures Capture the agency’s use of best practices following the
completion of the comprehensive assessment The best practices stated in the item are not necessarily The best practices stated in the item are not necessarily
required in the Conditions of Participation Note that patients who have been assessed as “unresponsive”,
based on M1710, When Confused and/or M1720, When A i ill t b i l d d i th fAnxious, will not be included in the process measure for depression screening.
M1730DepressionScreeningp g
Response 1 PHQ-2© is completed when responding to the question The results for rows a & b are for agency use only and will
not be encoded and transmitted with OASIS data If the patient/caregiver scores three points or more on the
PHQ-2©, then further depression screening is indicated. The PHQ-2 is only used for patients that appear to be
iti l d h i ll bl t th t i l d dcognitively and physically able to answer the two included questions. After determining the PHQ-2 is an appropriate tool, the patient may be unable to answer the questions, e g the patient may not be able to quantify how manye.g. the patient may not be able to quantify how many days they have experienced the problems. Answer 1 (NA)4b-Q124.5
If th ti t t t th ti t l d/ If the patient states the questions are too personal and/or refuses to answer, the answer is 0-No. Jan 2013
M2250PlanofCareSynopsisy p400
NO B t ti i t ti t i l d d i thNO: Best practice interventions not included in the POCYES: POC contains orders for treating depressionYES: POC contains orders for treating depression. Includes anti-depressant med on POC. 4b-Q172.9
NA: Patient has no diagnosis or the clinician gcompleted an assessment that indicated the patient has no symptoms of depression (or does not meet criteria for further evaluation or treatment if a standardized depression screening tool is used).
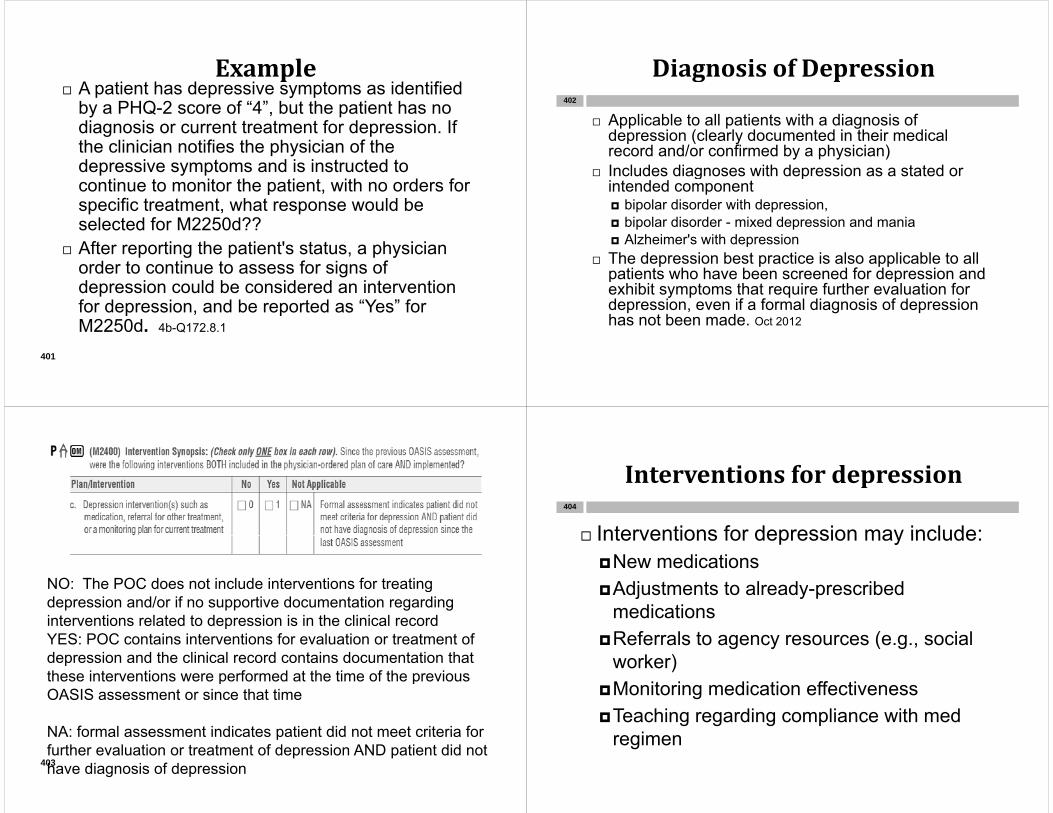
Examplep A patient has depressive symptoms as identified
by a PHQ-2 score of “4”, but the patient has no diagnosis or current treatment for depression Ifdiagnosis or current treatment for depression. If the clinician notifies the physician of the depressive symptoms and is instructed to
ti t it th ti t ith d fcontinue to monitor the patient, with no orders for specific treatment, what response would be selected for M2250d??selected for M2250d??
After reporting the patient's status, a physician order to continue to assess for signs of depression could be considered an intervention for depression, and be reported as “Yes” for M2250d 4b Q172 8 1M2250d. 4b-Q172.8.1
401
DiagnosisofDepressiong p
Applicable to all patients with a diagnosis of d i ( l l d d i h i di l
402
depression (clearly documented in their medical record and/or confirmed by a physician)
Includes diagnoses with depression as a stated or g pintended component bipolar disorder with depression, bipolar disorder - mixed depression and maniap p Alzheimer's with depression
The depression best practice is also applicable to all patients who have been screened for depression andpatients who have been screened for depression and exhibit symptoms that require further evaluation for depression, even if a formal diagnosis of depression has not been made. Oct 2012
NO: The POC does not include interventions for treatingNO: The POC does not include interventions for treating depression and/or if no supportive documentation regarding interventions related to depression is in the clinical recordYES POC t i i t ti f l ti t t t fYES: POC contains interventions for evaluation or treatment of depression and the clinical record contains documentation that these interventions were performed at the time of the previous p pOASIS assessment or since that time
NA: formal assessment indicates patient did not meet criteria forNA: formal assessment indicates patient did not meet criteria for further evaluation or treatment of depression AND patient did not have diagnosis of depression 403
Interventionsfordepressionp
Interventions for depression may include:404
Interventions for depression may include:New medicationsAdjustments to already prescribedAdjustments to already-prescribed
medicationsR f l t ( i lReferrals to agency resources (e.g., social worker)M it i di ti ff tiMonitoring medication effectiveness
Teaching regarding compliance with med iregimen
M1740Cognitive,behavioral,andpsychiatric symptomspsychiatricsymptoms
M1740Cognitive,behavioral,andpsychiatricsymptomssymptoms
Ti i t SOC ROC Di h Timepoints SOC ROC Discharge Behaviors can be observed by the clinician
t d b th ti t f il thor reported by the patient, family, or others
C id bl ti b h i Consider problematic behaviorsSevere enough to make the patient unsafe OR
cause considerable stress to caregivers ORcause considerable stress to caregivers OR require supervision or intervention
Consider frequency of behaviors
M1740Cognitive,behavioral,andpsychiatric symptomspsychiatricsymptoms
The time frame under consideration for M1740, 407
Cognitive, behavioral, and psychiatric symptoms that are demonstrated at least once a week, is defined in the wording of the item - "at least gonce a week". The phrase "at least once a week" means that a behavior was demonstrated multiple times in the recent relevant past andmultiple times in the recent, relevant past and the frequency of the occurrence was at least one time a week prior to and including the day of assessment The assessing clinician willof assessment. The assessing clinician will determine "recent, relevant past" based on the patient/caregiver interview, referral information, assessment findings diagnoses and recentassessment findings, diagnoses and recent history of medical treatment and its effectiveness. 4b-Q124.5.6
M1740
If a patient is alert and oriented but If a patient is alert and oriented, but decides not to use their cane because they think they don’t need it (they are unsafethink they don t need it (they are unsafe without it) or they decide they aren’t going to take their diuretic because they areto take their diuretic because they are going to the doctor and don’t want to have any accident would you select Responseany accident, would you select Response “2 – Impaired decision-making”?
4b-Q124.5.5
M1740
The intent of M1740, Cognitive, behavioral, and hi t i t i t t ifi b h ipsychiatric symptoms, is to capture specific behaviors
that are a result of significant neurological, cognitive, behavioral, developmental or psychiatric limitations or p p yconditions. It is not the intent of M1740 to report noncompliance or risky choices made by cognitively intact patients who are free of the aforementionedintact patients who are free of the aforementioned conditions. The assessing clinician will have to determine if the patient has a disorder that is causing her non-
li i th ti t ki h i t tcompliance or is the patient making a choice not to comply completely with physician's orders, cognizant of the implications of that choice.
Question 13
M1745FrequencyofDisruptiveBehavior SymptomsBehaviorSymptoms
Frequency of any behaviors that are disruptive or dangerous to the patient or the caregiversdangerous to the patient or the caregivers
Behaviors may or may not be listed in M1740
M1745FrequencyofDisruptiveBehaviorSymptomsSymptoms
Consider if the patient has any problematic behaviors – not just the behaviors listed in M1740 which jeopardize or couldthe behaviors listed in M1740 – which jeopardize or could jeopardize the safety and well-being of the patient or caregiver. Then consider how frequently these behaviors occur.
Include behaviors considered symptomatic of neurological, y p gcognitive, behavioral, developmental, or psychiatric disorders. Use clinical judgment to determine if the degree of the behavior is disruptive or dangerous to the patient or caregiver.
Disruptive/dangerous behaviors Disruptive/dangerous behaviors Sleeplessness “Sun-downing” Agitationg Wandering Aggression Combativeness
G i l i f ili l Getting lost in familiar places, etc.
M1745 - Frequency of Disruptive Behavior S t l b d di tiSymptoms, only based on disruptive behavior: physical, verbal or other di ti /d t ? O i thidisruptive/dangerous symptoms? Or is this item based on behaviors listed in M1740?
M1740 - Cognitive, behavioral, and psychiatric symptoms, and M1745 – Frequency of Disruptive Behavior Symptoms are not directly linked to one another.

M1740– M1745
There may be behaviors reported in M1740 413
y pthat are not reported in M1745 and vice versa.
F l ti tFor example, a patient may express excessive profanity or sexual references that cause considerable stress to the a cause co s de ab e s ess o ecaregivers and be reported in M1740, but in the clinician's judgment, the behavior does not jeopardize the safety and well being ofnot jeopardize the safety and well-being of the patient or caregiver, therefore is not reported in M1745.p
M1745
When completing M1745 - Frequency ofWhen completing M1745 - Frequency of Disruptive Behavior Symptoms, do we h t t k i t id ti if thhave to take into consideration if the patient has a fulltime caregiver to watch over her, or do we address it without including the caregiver's presence?g g p
M1745
The environment in which the patient lives and the pskills of the caregiver may impact the scoring of M1740 - Cognitive, behavioral, and psychiatric symptoms, and M1745 - Frequency of Disruptive y p , q y pBehavior Symptoms. For example, if a patient has dementia, they may exhibit a number of behaviors listed in M1740 but may not be reported in thelisted in M1740, but may not be reported in the OASIS item if they live in a setting specifically designed to care for patients with dementia. The same would be true for M1745 Look to thesame would be true for M1745. Look to the descriptors for the behaviors that are reportable for both M1740 and M1745 to determine if the behavior would be reportable 4b Q124 7would be reportable. 4b-Q124.7
M1750PsychiatricNursingServices
By home health not
M1750, Psychiatric Nursing Services, reports if the
By home health, not a different
community provider
M1750, Psychiatric Nursing Services, reports if the patient is receiving psychiatric nursing services in the home at the time of the SOC/ROC assessment. This is referring to qualified personnel of the home health agency, per physician orders,
ifi ll f th t d t t t fspecifically for the assessment and treatment of psychiatric conditions. When completing the SOC/ROC comprehensive assessment if an orderSOC/ROC comprehensive assessment, if an order exists on the plan of care for the agency to provide psychiatric services, then respond "Yes" to M1750.

M1750PsychiatricNursingServicesServices
If there are no orders on the referral for psych nursing i h ld th kill d M1750 “Y ” if
417
services, should the skilled nurse answer M1750 “Yes” if she identifies a psych issue on her initial assessment and plans to obtain physician’s orders for the agency’s Mental Health Nurse? Can she answer “Yes” even if the visit byHealth Nurse? Can she answer Yes even if the visit by the Mental Health Nurse will not be completed in the 5 day assessment window?
In order to select "Yes" for M1750, Psychiatric Nursing , y gServices, you must have a physician order for psychiatric nursing services on the Start of Care/Resumption of Care plan of treatment. It is not required that the clinician completing the comprehensive assessment be a qualifiedcompleting the comprehensive assessment be a qualified psychiatric nurse. The first visit by the qualified psychiatric nurse does not have to occur in the time frame allowed for completing the comprehensive assessment, but you must co p et g t e co p e e s e assess e t, but you usthave an order for the psychiatric nursing services to answer "Yes." 4b-Q126.1
ADL/IADL M1800 M1910ADL/IADLsM1800‐M1910418
ADL/IADLConventions
ADL questions assess the patient’s ABILITY, not ADL questions assess the patient s ABILITY, not necessarily actual performance
"Willingness" and "compliance" are not the g ess a d co p a ce a e o efocus of these items.
Items address the patient's ability to SAFELYp yperform ADLscurrent physical statusp ymental/emotional/cognitive statusActivities permitted/environmentActivities permitted/environment.
ADL/IADLConventions
• Ability can be temporarily or permanently y p y p ylimited byphysical impairments (e.g., limited range of
ti i i d b l )motion, impaired balance),emotional/cognitive/behavioral impairments
(e g memory deficits impaired judgment(e.g., memory deficits, impaired judgment, fear),
sensory impairments (e.g., impaired vision or i )pain),
environmental barriers (e.g., stairs, narrow doorways location of bathroom or laundry)doorways, location of bathroom or laundry).

ADL/IADLConventions
Patient’s ability yCondition improves or declinesMedical restrictions are imposed or liftedModification of environment
The clinician must consider what the ti t i bl t d th d f thpatient is able to do on the day of the
assessment. If ability varies over time, choose the response describing thechoose the response describing the patient’s ability more than 50% of the time period under consideration.
ADL/IADLConventions
While the presence or absence of a While the presence or absence of a caregiver may impact actual performance of activities, it does not p ,impact the patient’s ability to perform the task.
The patient is able to put her clothes on once laid out on the bed. The caregiver has been hospitalized. Is the patient now unable to dress herself?
Did the patient’s ability change?
ADL/IADLConventions
If the patient’s ability varies between the p ydifferent tasks included in a multi-task item, report what is true in a majority of the included tasks giving more weight to tasksincluded tasks, giving more weight to tasks that are more frequently performed.
The scales present the most independent e sca es p ese e os depe delevel first, then proceeds to the most dependent. R d h f ll t d t i Read each response carefully to determine which one best describes what the patient is able to do.; read from bottom to topis able to do.; read from bottom to top
BedfastDefined Ch. 3 of the OASIS-C Guidance Manual…defines bedfast.
"Bedfast refers to being confined to the bed, either per h i i t i ti d t ti t' i bilit t t l tphysician restriction or due to a patient's inability to tolerate
being out of the bed." If the patient can tolerate being out of bed, they are not bedfast unless they are medically restricted to the bed The patient is not required to be out ofrestricted to the bed. The patient is not required to be out of bed for any specific length of time. The assessing clinician will have to use her/his judgment when determining whether or not a patient can tolerate being out of bed. For example, p g p ,a severely deconditioned patient may only be able to sit in the chair for a few minutes and is not considered bedfast as she/he is able to tolerate being out of bed. A patient with M lti l S t At h b l h t iMultiple System Atrophy becomes severely hypotensive within a minute of moving from the supine to sitting position and is considered bedfast due to the neurological condition which prevents him from tolerating the sitting position 4b
424
which prevents him from tolerating the sitting position. 4b-Q151.14

M1800‐M1900
A patient may demonstrate that they can safely p y y yambulate while using a walker, but then as a matter of choice, decide to walk without it. Another patient may demonstrate that they can safely ambulate y y ywhile using a walker, but then consistently walk without it, forgetting that they have a walker.
For the purposes of OASIS scoring non conformityFor the purposes of OASIS scoring, non-conformity or non-compliance should not automatically be considered indicative of a deeper psychological impairment The assessing clinician will have toimpairment. The assessing clinician will have to use clinical judgment to determine if the patient’s actions are more likely related to impairment, or to
l h i d i f thpersonal choice made in awareness of the potential related risk.
M1800‐M1900
The response related to "assistance ofThe response related to assistance of another person" includes those
ti t ti l ti i ti ipatients, actively participating in performing a task, but needing assistance of one or more person(s) to safely complete included tasks. 4b-Q127.4y p
Service animal counts as a device, NOT as assistance 4b Q12 1as assistance. 4b-Q127.1
M1800Grooming M1800Grooming
Timepoints SOC ROC Dischargep g Grooming excludes
BathingShampooing hairToileting hygieneC id th f ith hi h l t d ti iti Consider the frequency with which selected activities are necessarywashing face and hands vs. fingernail care g g
Patients able to do more frequently performed activity should be considered to have more ability in groomingIf the patient requires a “spotter” for safety response 2 If the patient requires a spotter for safety, response 2.

M1810CurrentAbilitytoDressU B dUpperBody
M1820CurrentAbilitytoDressLower BodyLowerBody
M1810/M1820CurrentAbilitytoD U /L B dDressUpper/LowerBody
Timepoints SOC/ROC/FU/Discharge Timepoints SOC/ROC/FU/Discharge Identifies the patient’s ability toDress upper and lower bodyDress upper and lower bodyObtain, put on and remove upper and
lower body clothinglower body clothingPut on whatever clothing is routinely
(l k i th l t)worn (look in the closet). Specifically includes the ability to manage
i b tt d if thzippers, buttons, and snaps if these are routinely worn.
Prosthetic,orthoticandothersupport devicessupportdevices
Prosthetic, orthotic, or other support devices Prosthetic, orthotic, or other support devices applied to the upper body (e.g., upper extremity prosthesis, cervical collar, or arm li ) h ld b id d b dsling) should be considered as upper body
dressing items.Prosthetic orthotic or other s pport de ices Prosthetic, orthotic, or other support devices applied to the lower body (e.g., lower extremity prosthesis ankle/foot orthosisextremity prosthesis, ankle/foot orthosis[AFO], or TED hose) and including ace wraps should be considered as lower body dressing items. 4b-Q132.4

M1810/M1820CurrentAbilitytoDress
Observation/interview the patient or caregivercaregiver
Observe spinal flexion, joint range of motion, shoulder and upper arm strength, and manual dexterity g y
Ask the patient to demonstrate the body motions involved in dressingbody motions involved in dressing
Dressing
The patient’s clothes are hung over the p gchair in the bedroom, therefore he is safe getting his clothes? Is this his permanent solution? Is this his permanent solution? 4b-Q132.3
What if closets etc are adapted for your wheelchair bound patient? 4b-Q132 1wheelchair bound patient? 4b Q132.1
If a patient modifies the clothing they wear due to a physical impairment, the modified l thi l ti ill b id d ticlothing selection will be considered routine
if there is no reasonable expectation that the patient could return to their previousthe patient could return to their previous style of dressing.
M1810 & M1820. The guidance in M1810 & M1820 t t th t th ti t'M1820 states that you assess the patient's ability to obtain, put on and remove the clothing items usually worn Other guidance states thatitems usually worn. Other guidance states that items such as prosthetics, corsets, cervical collars, hand splints, Teds, etc. are considered , p , ,dressing apparel. Do we include the other items, like a splint, if the patient doesn't usually wear it? Our patient just injured their wrist and will only be wearing it for a week; he doesn't usually wear a splintusually wear a splint.
What response? 4b-Q132.4
M1830Bathing

M1830Bathing
Timepoints SOC ROC F/U Discharge Timepoints SOC ROC F/U Discharge Specifically excludes washing face and
hands and shampooing hairhands, and shampooing hair. If the patient requires standby
assistance to bathe safely in the tub orassistance to bathe safely in the tub or shower or requires verbal cueing/reminders, then selectcueing/reminders, then select Response 2 or Response 3, depending on whether the assistance needed is intermittent (“2”) or continuous (“3”).
M1830Bathing
Response 2--Intermittent Response 2--IntermittentPatient's ability to transfer into/out of the tub or
shower is the only bathing task requiring human y g q gassistance
Patient requires one, two, or all three of the types of assistance listed in Response 2 but not theof assistance listed in Response 2 but not the continuous presence of another person
Response 3--Continuous Response 3 Continuous If a patient requires one, two, or all three of the
types of assistance listed in Response 2 and the continuous presence of another person
M1830Bathing
Response 4 The patient must be able to safely p p yand independently bathe outside the tub/shower, including independently accessing water at the sink or setting up basin at thewater at the sink, or setting up basin at the bedside, etc.
Response 5 The patient must be unable to b th i th t b/ h ti i t ibathe in the tub/shower, can participate in bathing self but needs assistance (even if just to wash his back).)
Response 6 The patient is totally unable to participate in bathing and is totally bathed by another person regardless of where bathinganother person, regardless of where bathing occurs or if patient has a functioning tub or shower.
M1830Bathing
Response 4 or 5- If the patient does not p phave a tub or shower in the home, or if the tub/shower is nonfunctioning or not safe f ti t th ti t h ld bfor patient use, the patient should be considered unable to bathe in the tub or shower select based on the patient’sshower, select based on the patient s ability to bathe outside the tub/shower.
Note: The patient’s status should not be pbased on an assumption of a patient’s ability to perform a task with equipment they do not currently havethey do not currently have.

QuizQ
Shower/bath is non-functioning or not441
Shower/bath is non-functioning or not safe
Physician-ordered bed restFell getting out of the shower on 2 e gett g out o t e s o e o
previous occasions and is now afraid and unwilling to try againand unwilling to try again
Chooses not to navigate the stairs to h b/ hthe tub/shower. 4b-Q133
M1830Q&AApril2013Q p
Q5: Patient allowed to bathe, but medically restricted f i LE bl i
442
from getting LE cast wet; unable to put water protective sleeve on, but once someone applies the protective sleeve for him, he can get in/out of tub using transfer bench and wash entire body with hand held showerbench and wash entire body with hand-held shower. Does this medical restriction impact patient’s ability scoring M1830?A5 M di l t i ti th t i t OASIS i l d dA5: Medical restrictions that impact OASIS-included bathing tasks are considered, so the tasks required to allow compliance with medically prescribed precautions for bathing could impact patient’s ability Response 2 isfor bathing could impact patient s ability. Response 2 is appropriate since patient needs intermittent human assistance to bathe in tub/shower.
M1840ToiletTransferring M1840ToiletTransferring
Timepoints SOC/ROC/FU/Discharge• Timepoints SOC/ROC/FU/Discharge• Identifies patient’s ability to safely: Get to and from the toilet or commodeAnd transfer on and off the toilet or
bedside commode• Excludes personal hygiene and p yg
management of clothing when toiletingg

M1840ToiletTransferring
Response 0—Able…p Patient can get to and from the toilet during the day
independently, but uses the bedside commode at night for convenience 4b-Q143g
Response 1—When reminded… Patient needs assistance getting to/from the toilet or
with toileting transfer or both (even if they don’t havewith toileting transfer or both (even if they don t have a caregiver 4b-Q146)
Patient who can independently get to the toilet, but who requires assistance to get on and off the toiletwho requires assistance to get on and off the toilet
If the patient requires any degree of hands-on assistance and/or standby assistance and/or verbal cueing/reminders to get to/from the toilet and/orcueing/reminders to get to/from the toilet and/or transfer on/off the toilet safely
M1840 Toilet TransferringM1840ToiletTransferring
R 3• Response 3Patient who is unable to get to/from the
toilet or bedside commode, but is able to place and remove a bedpan/urinal independently
This is the best response whether or not pa patient requires assistance to empty the bedpan/urinal.p
BedpanandUrinalp
If the bedfast patient needs447
If the bedfast patient needs assistance to get on/off the bedpan, th i t M1840 R ithe appropriate M1840 Response is "4-Is totally dependent in toileting" even if they can place and remove the urinal. 4b-Q146.1
M1840ToiletTransferring
Observation and Interview Ask the patient if he/she has any difficulty
getting to and from the toilet or bedside commodecommode
Observe the pt during transfer and ambulation note:ambulation note:Difficulty with balanceStrengthDexterityPain, etc.
Determine the level of assistance needed to Determine the level of assistance needed to safely use the toilet or commode.

M1840. If my patient has a urinary catheter, does this mean he is totally dependent in toileting transferring?mean he is totally dependent in toileting transferring?
The item simply asks about the patient’s ability to get to and from the toilet or bedside commode and their ability to transfer on and off toilet/commode. This ability can be assessed whether or not the patient uses the toilet for urinary elimination 4b Q142toilet for urinary elimination. 4b-Q142
A patient with MS is transferred via a Hoyer. She is non weight bearing. She does not participate in the transfer g g p pprocess.
1- “when reminded, assisted or supervised…” requires th ti t t b ti i ti i th t k If th ti tthe patient to be participating in the task. If the patient cannot effectively participate in the effort required, she is scored a 4-”totally dependent in toileting” 4b-147.5
M1840. If a patient uses a bedside commode over the toilet, would this be considered “getting to the toilet” for the purposes of responding to M1840?responding to M1840?
Yes, a patient who is able to safely get to and from the toilet and transfer should be scoredfrom the toilet and transfer should be scored at response levels 0 or 1, even if they require the use of a commode over the toilet. Notethe use of a commode over the toilet. Note that the location of such a commode is not at the "bedside," and the commode is functioning much like a raised toilet seat. 4b-Q148
M1845ToiletingHygiene M1845ToiletingHygiene
Timepoints SOC ROC DischargeTimepoints SOC ROC DischargeToileting hygiene includes several
activities including pulling clothes upactivities, including pulling clothes up or down and adequately cleaning (wiping) the perineal area(wiping) the perineal area.
This item refers the patient’s ability to l h i dmanage personal hygiene and
clothing with or without assistive d idevices.

M1845ToiletingHygieneg yg
“Assistance” refers to assistance from Assistance refers to assistance from another person by verbal cueing/reminders, supervision, and/or stand-by or hands-on assistanceassistance.
Majority of tasks rule doesn’t apply. If they cant pull down their pants they cant be a ‘0’ orcant pull down their pants they cant be a 0 or ’1’
P ti t ti i t i h i Response 2--Patient can participate in hygiene and/or clothing management but needs some assistance with either or both activities or Patient requires standby assistance or verbal cueing.
M1850Transferring
M1850Transferring
Timepoints SOC/ROC/FU/Discharge Timepoints SOC/ROC/FU/Discharge Identifies the patient’s ability to safely transfer
from bed to chair (and chair to bed), or position self in bed if bedfastself in bed if bedfast.
For most patients, the transfer between bed and chair will include transferring from a supine g pposition in bed to a sitting position at the bedside, then some type of standing, stand-pivot, or sliding board transfer to a chair at the bedside. 4b-gQ151.7
If the patient does not sleep in a bed, assess the transfer from his usual sleeping place. (Recliner-p g p (4b-Q151.7.1
SittingSurfacenotatBedsideg
If the sleeping surface is in the bedroom and 456
p gthe sitting surface is down the hall in the bathroom and the patient is independent moving from the supine to sitting positionmoving from the supine to sitting position, sitting to standing, and then standing to sitting, but requires minimal human assistance or an assistive device to ambulate from the bed to the sitting surface, the appropriate M1850 score would be a "1"the appropriate M1850 score would be a 1 . If the patient requires more than minimal assistance or requires both minimal human
i t d i ti d i thassistance and an assistive device, the appropriate score would be a “2”. 4b-Q150.1
Definitions
“Minimum human assistance”-- Minimum human assistance --individual assisting the patient is
t ib ti l th 25% f th t t lcontributing less than 25% of the total effort required to perform the transfer
“Minimal human assistance” could include any combination of verbalinclude any combination of verbal cueing, environmental set-up, and/or actual hands on assistance 4b Q148 2actual hands-on assistance. 4b-Q148.2
M1850 TransferringM1850Transferring
• Response 1• Response 1Patient is able to transfer self from bed to
chair but requires standby assistance tochair, but requires standby assistance to transfer safely, or requires verbal cueing/ reminders
If the patient transfers either with minimal human assistance (but not device), or with ( )the use of a device (no human assistance)• “Minimal human assistance” could include any
bi ti f b l i i t lcombination of verbal cueing, environmental set-up, and/or actual hands-on assistance.
M1850Transferring
• Response 2pPatient requires both minimal human
assistance and an assistive device to transfer safelytransfer safely
Patient can bear weight and pivot, but requires more than minimal human assistrequires more than minimal human assist
Patient must be able to both bear weight and pivot
• Response 3Patient is unable to do one or the other and
is not bedfastis not bedfast
M1850Transferring
Response 4 or 5 (Depending on the patient’s ability p ( p g p yto turn and position self in bed)Patient is bedfast Bedfast refers to being confined to the bed,
either per physician restriction or due to a patient’s inability to tolerate being out of the p y gbed.
CMS is in the process of defining assistive devices and will provide guidance when the issue isand will provide guidance when the issue is clarified.
Service animals are ‘devices’

M1850. If a patient requires a little help from the f (caregiver to transfer (e.g., verbal cueing, stand by
assist, contact guard), would the score for M1850 Transferring be “1” (requires “minimal human g ( qassistance”) or a “2” (“unable to transfer self”)? Both seem to apply. 4bQ151.2
If the patient is able to transfer self but requires standby assistance or verbal cueing to safely y g ytransfer, response “1” would apply.
If the patient is unable to transfer self but is able to bear weight and pivot when assisted during the transfer process, then response “2” would apply.p , p pp y
M1850. A quadriplegic is totally dependent, cannot even turn self in bed however he does get up toeven turn self in bed, however, he does get up to a gerichair by Hoyer lift. For M1850, is the patient considered bedfast? 4b-Q151.3
A patient who can tolerate being out of bed is not “bedfast.” If a patient is able to be transferred to a chair using a Hoyer lift, response 3 is the option that c a us g a oye t, espo se 3 s t e opt o t atmost closely resembles the patient’s circumstance; the patient is unable to transfer and is unable to bear weight or pivot when transferred by another personweight or pivot when transferred by another person.
Responses 4 and 5 only apply for the patient who is bedfast according to CMS’s definition.
The frequency of the transfers does not change the response, only the patient’s ability to be transferred and tolerate being out of bedand tolerate being out of bed.
M1850. When scoring M1850, Transferring, the assessment revealed difficulty with transfers. The patient was toe-touch, y p ,weight bearing on the left lower extremity and had pain in the opposite weight bearing hip. The patient had a history of falls and remained at risk due to medication side effects, balanceand remained at risk due to medication side effects, balance problems, impaired judgment, weakness, unsteady use of device and required assistance to transfer. The concern is the safety of the transfers considering all of the above Would "2" or "3" be thethe transfers considering all of the above. Would 2 or 3 be the appropriate response? 4b-Q151.6
Safety is integral to ability, if your patient requires more than minimal h man assistance or the need minimal assistance andminimal human assistance or they need minimal assistance and an assistive device to safely transfer, and can bear weight and pivot safely, Response 2 should be reported. If you determine th b i i ht d i ti t f th t f i tthe bearing weight and pivoting component of the transfer is not safe even with assistance, then the patient is not able to bear weight or pivot and the appropriate selection would be Response 3 f f3 – Unable to transfer self and is unable to bear weight or pivot when transferred by another person.
M1860Ambulation/Locomotion

M1860Ambulation
Timepoints SOC/ROC/FU/DCp SOC/ OC/ U/ C Ambulatory, charifast, or bedfast? (majority rule
does NOT apply) Even and uneven surfaces defined at 4b Q155 2 Even and uneven surfaces defined at 4b-Q155.2 Observe the patient ambulating across the room or
to the bathroom and the type of assistance required. N if h i f i ll f Note if the patient uses furniture or walls for support
Assess if patient should use a walker or cane for safe ambulation
Observe patient’s ability and safety on stairs if used If chairfast, assess ability to safely propel wheelchair
independently whether the wheelchair is a poweredindependently whether the wheelchair is a powered or manual version.
M1860Ambulation
Response 1—one-handed device AND nophuman assistance ((This is true for blind patients utilizing a cane to ambulate safely, canes used for weight bearing and a whitecanes used for weight bearing, and a white cane used to detect objects in the path of the user.)) 4b-Q155.1.1
Response 2—two-handed device and/or intermittent human assistanceR 3 C ti h Response 3—Continuous human assistance or supervision at all times
What if they used a cane and also needed What if they used a cane and also needed assistance to get up stairs?
M1860 AmbulationM1860Ambulation What if a patient does not require human p q
assistance and is able to safely ambulate with a walker in some areas of the home, but must use a cane in other areas due to space plimitations, distances, etc.?
The clinician will select the response that reflects the device that best supports safereflects the device that best supports safe ambulation on all surfaces the patient routinely encounters.
F l l t R 2 if lk i For example select Response 2 if a walker is required for safe ambulation in the hallway and living room, even if there are some situations in the home where a cane provides adequatethe home where a cane provides adequate support.
M1860 AmbulationM1860AmbulationWhat if a patient does not have a walkingWhat if a patient does not have a walking device but is clearly not safe walking alone? The clinician will select Response 3, able to walk
only with the supervision or assistance-- unless theonly with the supervision or assistance-- unless the patient is chairfast. 4b-Q155.1
Responses 4 and 5 refer to a patient who is unable to ambulate even with the use ofunable to ambulate, even with the use of assistive devices and/or continuous assistance. A patient who demonstrates or reports ability to t k t t t l t t f b ttake one or two steps to complete a transfer, but is otherwise unable to ambulate should be considered chairfast, and would be scored 4 or 5, based on ability to wheel self.

M1860Q&AJan.2013Q J
Patient ambulates only with a gait belt with 469
y gtherapy assist and a device.
If the assessing clinician determines the patient If the assessing clinician determines the patient is safe ambulating with constant human assistance, they are ambulatory. This is true
h th th i t d d i b l iwhether the assistance needed is verbal cueing, reminders, contact guard, or any level of hands-on assistance. If the patient is not bedfast, and is not safe ambulating even with a combination of continuous assistance and a device, they are chairfast. If the patient can only take a couple of p y psteps safely, they are not ambulatory.
M1860Ambulation
We have a patient who is ambulating in the home. The li i i th t th ti t i t f b l ti
470
clinician assesses that the patient is not safe ambulating with an assistive device, even with the supervision of another person at all times. The patient does not have a wheelchair in the home What is the appropriatewheelchair in the home. What is the appropriate response to M1860, Ambulation/Locomotion, for this patient? 4b-Q155.3.1
A patient is considered chairfast if they cannot be made A patient is considered chairfast if they cannot be made safe ambulating even with the combination of a device and the assistance of another person at all times. They are not bedfast unless they are medically restricted to y ythe bed or cannot tolerate being out of bed. If there is no wheelchair in the home, the assessing clinician cannot make assumptions about their ability to propel it safely. Th i t M1860 i thi i “5The appropriate M1860 response in this case is “5-Chairfast, unable to ambulate and is unable to wheel self”.
M1870FeedingorEatingM1870 F di E tiM1870FeedingorEating
Timepoints SOC/ROC/Discharge Identifies the patient’s ability to feed
him/herself, including the process of eating, chewing, and swallowing food
Excludes prep of food and transport to the table
History of aspiration pneumonia, forgets to swallow, pockets food, what response? 4b-Q156.2

M1870 Feeding or EatingM1870FeedingorEating Assessing the assistance needed by the patient g y p
to feed himself once the food is placed in front of him. Assistance means human assistance by verbal Assistance means human assistance by verbal
cueing/reminders, supervision, and/or stand-by or hands-on assistance.
Meal "set-up" (Response 1) includes activities Meal set-up (Response 1) includes activities such as mashing a potato, cutting up meat/ vegetables pouring milk on cereal, opening a milk carton adding sugar to coffee or teamilk carton, adding sugar to coffee or tea, arranging the food on the plate for ease of access, etc. -- all of which are special adaptations of the meal for the patientadaptations of the meal for the patient.
M1880CurrentAbilitytoPlanandPrepare Light MealsPrepareLightMeals
M1880CurrentAbilitytoPlanandPrepareLi ht M lLightMeals
Timepoints SOC/ROC/Discharge Response 0 Patient has the consistent
physical and cognitive ability to plan and prepare mealsprepare meals
Response 1 Patient has inconsistent ability to prepare light meals (e.g., can’tability to prepare light meals (e.g., can t prepare breakfast due to morning arthritic stiffness, but can prepare other meals throughout day)throughout day).
Response 2 Patient does not have the ability to prepare light meals at any pointability to prepare light meals at any point during the day of assessment.
M1880CurrentAbilitytoPlanandPrepareLightMealsg
Consider any prescribed diet requirements (and related Consider any prescribed diet requirements (and related planning/preparation) when selecting a response 4b-Q158
May be physically able to heat meal or make a sandwich, but if the patient doesn’t know his therapeutic diet, then is 1-unable to p p ,prepare meals on a regular basis due to physical, cognitive or mental limitations.
Patient’s prescribed diet consists either partially or l t l f t l t iticompletely of enteral nutrition
Assess the patient’s ability to plan and prepare their prescribed diet P ti t’ k l d f f di t d bilit t Patient’s knowledge of feeding amount and ability to prepare the enteral feeding, based on product used
Note that the ability to set up monitor and change the Note that the ability to set up, monitor and change the feeding equipment is excluded from M1880, as it is addressed on row “e” of M2100.

M1890AbilitytoUseTelephone M1890AbilitytoUseTelephone
Timepoints SOC/ROC/Discharge Timepoints SOC/ROC/Discharge Ability to use telephone identifies the
patient’s ability to safelypatient s ability to safely Answer the phoneDial a numberResponse “1” Effectively use the telephone
to communicate If h i i d ti t l If a speech impaired patient can only communicate using a phone equipped with texting functionality, able to use a specially adapted telephone would be selectedadapted telephone would be selected.
Q&A#7April2013Q p
Q7: When should a patient’s ability to479
Q7: When should a patient s ability to access the location and/or implements
d d t l t ADL/IADL t k bneeded to complete ADL/IADL tasks be considered when scoring the OASIS items M1830, M1845, M1870, M1880, and M1890?
Q&A#7April2013Q p
A7: The OASIS ADL/IADL items480
A7: The OASIS ADL/IADL items consider the patient’s ability to access th d d it d/ l tithe needed items and/or locations where the task is performed unless item guidance specifically excludes these from consideration. There are 5 ADL/IADL items where there are exclusions:exclusions:
Q&A#7:ExclusionforM1830Q
Focus is on patient’s ability to access481
Focus is on patient s ability to access tub/shower, transfer in/out, and bathe
ti b d d d it ientire body once needed items are in reach. Ability to access bathing supplies and prepare water in tub or shower are excluded from consideration when assessing patient’s bathing abilitypatient s bathing ability.
Q&A#7:ExclusionforM1845Q
Focus is on patient’s ability to access482
Focus is on patient s ability to access needed supplies and implements, and manage hygiene and clothing once at themanage hygiene and clothing once at the location where toileting occurs. The ability to access the toilet or BSC transfer on/offto access the toilet or BSC, transfer on/off bedpan, and to use urinal are excluded from consideration when answering thefrom consideration when answering the patient’s toileting hygiene ability.
Q&A#7:ExclusionforM1870Q
Focus is on patient’s ability to eat chew483
Focus is on patient s ability to eat, chew, and swallow once the meal is placed in front of the patient and needed items are pwithin reach. The ability to access the location where the meal is prepared and consumed, and transporting food to the table are excluded from consideration
h i th ti t’ f diwhen assessing the patient’s feeding and eating ability.
Q&A#7:ExclusionforM1880Q
Focus is on patient’s ability to plan484
Focus is on patient s ability to plan and prepare meals once patient is in th l ti l ti Ththe meal preparation location. The ability to access the location where meals are prepared is excluded from consideration when assessing gpatient’s meal planning and preparation abilitypreparation ability.

Q&A#7:ExclusionforM1890Q
Focus is on patient’s ability to use a485
Focus is on patient s ability to use a phone once it is within reach. The
bilit t th l ti hability to access the location where the telephone is stored is excluded from consideration when assessing patient’s ability to use the telephone.p y p
M1900PriorFunctioningADL/IADL
M1900PriorFunctioningADL/IADL
Independent Can complete the activity by him/herself with or without assistive devices without physical or verbal assistance from a helper.
Needed some help Patient contributed effort but required help from another
person to accomplish the task/activity safely. Dependent
Patient was physically and/or cognitively unable to contribute effort toward completion of the task, and the helper must p , pcontribute all the effort.
If the patient was previously independent in any of the tasks, but needed help or was completely dependent in p p y pothers, pick the response that best describes the patient’s level of ability to perform the majority of included tasks.
M1900PriorFunctioningADL/IADL
•Refers specifically to grooming, dressing, bathing, and toileting hygienebathing, and toileting hygiene
• Medication management is not included in the•definition of self-care for M1900 as it is •addressed in a separate question (M2040)

M1900PriorFunctioningADL/IADL
•Refers to walking (with or without assistive device).
Wh l h i bilit i t di tl dd d i•Wheelchair mobility is not directly addressed in this item (wheelchair bound means dependent).
M1900PriorFunctioningADL/IADLADL/IADL
•Refers specifically to tub, shower, commode, and bed to chair transfers
M1900PriorFunctioningADL/IADLADL/IADL
•Refers specifically to light meal preparation, laundry, shopping, and phone use.
M1910FallRiskAssessment
Process Measure

M1910FallRiskAssessment
Timepoints SOC ROC Timepoints SOC ROC Process Measure
P i d h f 6 ill b Patients under the age of 65 will be excluded from the denominator of the publicly reported measure
Completed within specified time framesp p5 days after SOC48 hours for ROC48 hours for ROCBy the assessing clinician
M1910FallRiskAssessment
Multi-factor Falls Risk Assessment—one Multi factor Falls Risk Assessment one component must be a standardized tool appropriately validated for identifying falls risk in community dwelling elders
MAHC-10 Falls Risk Assessment Tool is now standardized and validated, therefore it may be used alone to satisfy the requirements of this item
CMS does not endorse any specific tool
M1910FallRiskAssessment
For Responses 1 and 2 (Yes) For Responses 1 and 2 (Yes)Fall risk assessment must have been completed
by the clinician completing the SOC or ROC Select Response 0 (No)
Multi-factor falls risk screening was not conductedMulti-factor falls risk screening was conducted but
NOT during the required assessment time frameMulti factor falls risk screening was conductedMulti-factor falls risk screening was conducted
during the assessment time frame, but by someone other than the assessing clinician
Multi-factor falls risk screening was conducted that was not appropriate for the patient
M2250PlanofCareSynopsisy p496
NO: If the plan of care does not include interventions for fall f fprevention, whether or not an assessment for falls risk was
conducted.
YES: If the physician-ordered plan of care contains specific interventions to reduce the risk of falls, select “Yes.”
NA: if the clinician completed an assessment that indicated the patient was at low, minimal, or no risk for falls.

NO: POC does not include interventions for fall prevention andNO: POC does not include interventions for fall prevention and /or there is no supportive doc in clinical record that interventions were performedYES l f t i ifi i t ti t d thYES: plan of care contains specific interventions to reduce the risk of falls and the clinical record contains documentation that these interventions were performed at the time of the previous p pOASIS assessment or since that time
NA: a formal multi-factor Fall Risk Assessment indicates theNA: a formal multi factor Fall Risk Assessment indicates the patient was at low, minimal or no risk for falls since the last OASIS assessment 497
ExamplesofFallPreventionInterventionsInterventions
498
Environmental changesEnvironmental changesStrengthening exercisesConsultation with the physician
regarding medication concerns
M di i M2000MedicationsM2000s499
Contactwithphysician‐ TermsDefined:
• Contact with physician is defined as communication by:TelephoneVoicemailElectronic meansFaxFax Or any other means that conveys the
message of patient statusmessage of patient status

Clinicallysignificantmedicationissues‐Terms Defined:TermsDefined:
Clinically significant medication issues that pose an actual or potential threat to patient health and safety:Drug reactionsDrug reactions Ineffective drug therapy Side effectsSide effects Drug interactionsDuplicate therapyDuplicate therapy Medication omissionsDosage errors gNon-adherence to prescribed medication regimen
MedicationInteractionDefined
The impact of another substance upon a medication. Substances include Other medication(s) Nutritional supplements Nutritional supplements Herbal products Food Food Substances used in diagnostic studies
The interactions may alter absorption, distribution, metabolism, or elimination. These interactions may decrease the effectiveness of the medication or increase the potential for adverse consequences.
AdverseDrugReactionDefinedg
• Adverse drug reaction (ADR)• Adverse drug reaction (ADR)Form of adverse consequencesMay be a secondary effect of a medicationMay be a secondary effect of a medication
that is usually undesirable and different from the therapeutic effect of the medicationthe therapeutic effect of the medication
Any response to a medication that is noxious and unintended and occurs innoxious and unintended and occurs in doses for prophylaxis, diagnosis, or treatment.
5TypesofAdverseDrugReactions
The categories of ADRsgSide effectsAn expected, well-known reaction that
occurs with a predictable frequency and may or may not constitute an adverse consequenceconsequence.
HypersensitivityIdiosyncratic responseIdiosyncratic responseToxic reactionsAdverse medication interactionsAdverse medication interactions.
M2000 DrugRegimenReview M2000DrugRegimenReviewg g
Timepoints SOC ROCTimepoints SOC ROC Include all medications / all routesPrescribed OTCOTC
Process MeasuresCaptures agency’s use of best practicesCaptures agency s use of best practicesThis one is required in CoPs
M2000DrugRegimenReview
Portions of the drug regimen review mayPortions of the drug regimen review may be completed by agency staff other than h i li i i id ifi ithe assessing clinician e.g., identification
of potential drug-drug interactions or potential dosage errors Review findings must be communicated toReview findings must be communicated to
the assessing clinician so that the appropriate response for M2000 may beappropriate response for M2000 may be selected
M2000DrugRegimenReview
This collaboration does not violate the ‘1 clinician’ requirement for the completion of the OASISof the OASIS Each Agency will need to create a workable
process to ensure complianceprocess to ensure complianceThe M0090 date (date assessment is
l t d) ld b th d t th tcompleted) would be the date the two clinicians collaborated and the assessment was completed.
M2000
In therapy only cases can an LPN in In therapy only cases, can an LPN in the office work cooperatively with the th i t t l t th Dtherapist to complete the Drug Regimen Review by performing elements of the drug regimen review that the therapist will not be pcompleting?
4b-Q160.3.1
M2000
No. Only registered nurses, physical therapists, speech language pathologists and occupational therapists are qualified to perform comprehensive assessments. LPNs are not qualified to performLPNs are not qualified to perform comprehensive assessments, so they may not work cooperatively with y p ytherapists in order to complete the drug regimen review.
Whataboutapharmacist?p
Current guidance states that only g yclinicians qualified to perform comprehensive assessments may
ll b t th D R icollaborate on the Drug Regimen Review. On therapy only cases, can the therapist collaborate with a pharmacisttherapist collaborate with a pharmacist when completing the Drug Regimen Review? 4b-Q160.3.2
Yes!! Agency policy and documentation requirements?
M2000DrugRegimenReviewg g
Response 1 No problems found Response 1 No problems foundMedication list from inpatient facility matches the
medications patient shows the clinician at the SOC/ROCSOC/ROC assessment
Assessment shows that diagnoses/symptoms are adequately controlled by meds as prescribedadequately controlled by meds as prescribed
Patient possesses all medications prescribedPatient has a plan for taking meds safely at the right p g y g
timePatient is not showing signs/symptoms that could be
d ti d b di tiadverse reactions caused by medications.

M2000DrugRegimenReview
Response 2 Problems found pMed list from the inpt facility does not match
the medications the patient shows the clinicianDiagnoses/ symptoms for which patient is
taking meds are NOT adequately controlledPt seems confused about when/how to take
meds indicating a high risk for med errors.Pt h t bt i d d i di t th tPt has not obtained meds or indicates that he/she will probably not take prescribed meds due to financial cultural or other issues withdue to financial, cultural, or other issues with medications.
M2000DrugRegimenReviewg g
R 2 P bl f d Response 2 Problems found Patient has signs/symptoms that could be adverse
reactions from medications. Patient takes multiple non-prescribed medications
(OTCs, herbals) that could interact with prescribed medsUse the timeframe to tr to resol e the problems Use the timeframe to try to resolve the problems found.
If a med related problem is identified and resolved If a med related problem is identified and resolved by the agency staff by the time the assessment is completed, the problem does not need to be reported as an existing clinically significant problemreported as an existing clinically significant problem. 4b-Q160.4
M2000DrugRegimenReviewg g
C id th t ti l f i d• Consider the potential for an increased risk due toimpairment or decline in an individual’s
mental or physical condition or functional p yor psychosocial status
Complex medication planComplex medication planMultiple physicians Multiple pharmaciesMultiple pharmacies
1 Is o gen considered a medication? (M2000 Dr g1. Is oxygen considered a medication? (M2000 - Drug Regimen Review) 4b-Q160.1
Yes, oxygen is included as a medication when answering M2000 - Drug Regimen Review.
2. In M2000 - Drug Regimen Review, are ALL drug interactions considered "potential clinically significant p y gmedication issues"? 4b-Q160.2
NoNo, the OASIS-C Guidance Manual states that potential clinically significant medication issues include serious drug-drug, drug-food and drug-disease g g, g ginteractions.
Notallpotentialmedsideeffectsareconsidered clinically significant med issuesconsideredclinicallysignificantmedissues
Problems found during review, should be selected if g ,the “Patient has signs/symptoms that could be adverse reactions from medications.” It further defines a side effect as "an expected well knowndefines a side effect as an expected, well-known reaction that occurs with a predictable frequency and may or may not constitute an adverse y yconsequence."
A side effect would be considered "a potential li i ll i ifi t di ti i " if it "clinically significant medication issue" if it "poses an
actual or potential threat to patient health and safety".safety .
4b-Q160.3
Notallpotentialmedsideeffectsareconsidered clinically significant med issuesconsideredclinicallysignificantmedissues
The determination of whether a medication issue meets this threshold should be based on the clinician's judgment in conjunction with agency guidelines and established standards for evaluating d ti id ff t i t ti t O lidrug reactions, side effects, interactions, etc. Online resources or these standards can be found in Chapter 5 of the OASIS C Guidance ManualChapter 5 of the OASIS-C Guidance Manual.
4b-Q160.2, 160.3
M2002MedicationFollow‐up M2002MedicationFollow‐up
Timepoints SOC ROC Timepoints SOC ROC Medication ‘issues’ Communicated with
physician (or designee) within one calendarphysician (or designee) within one calendar day
Someone else may communicate with the physician but who has to answer the data item?What about the on call physician who says to What about the on-call physician who says to call back Monday? 4b-Q160.5
Agency policy must define this process Agency policy must define this process Process Measure

M2002MedicationFollow‐up
Response “1” p Physician responds to the agency communication
with acknowledgment of receipt of information and/or further advice or instructionsand/or further advice or instructions
If the physician or physician designee responds within one calendar day and there is a resolution to the clinically significant medication issue or ato the clinically significant medication issue or a plan to resolve the issue
Two way communication AND reconciliation or plan by the end of the next calendar day 4b Q160 6plan by the end of the next calendar day. 4b-Q160.6
Response “0” Interventions are not completed as outlined in this
Citem and Clinician should document rationale in the clinical record
Example
• A clinically significant medication issue isA clinically significant medication issue is identified on day 5 after the SOC and the physician is notified. The physician doesn’t respond until the 6th day after SOC, what is the answer? 4b-Q160.5.1
X
M2002;M2004
Multiple clinically significant medications Multiple clinically significant medications issues were identified as I completed the SOC assessment Only one wasSOC assessment. Only one was resolved within one calendar day. How do I answer M2002 and then 2004?do I answer M2002 and then 2004?
4b-Q160.6.2
In order to select ‘yes’ on M2002/M2004 In order to select yes on M2002/M2004, ALL clinically significant issues must have been resolved (or plan to resolve)have been resolved (or plan to resolve) within one calendar day.
M2004MedicationIntervention

M2004MedicationIntervention
Timepoints Transfer Discharge Identifies if potential clinically significant p y g
problems such as adverse effects or drug reactions identified at the time of the most recent OASIS assessment or after that time were addressed with the physicianp y
Process measure
M2004MedicationIntervention
R 1 Y Response 1 – YesPhysician responds to the agency
communication with acknowledgment ofcommunication with acknowledgment of receipt of information and/or further advice or instructions within the specified timeframe.
Response 0 – No Interventions are not completed as outlined in
thi it d th li i i h ld d tthis item and the clinician should document rationale in the clinical record.
Collaboration between clinicians does not Collaboration between clinicians does not violate the ‘1 clinician’ rule
M2004MedicationIntervention
If the last OASIS assessment completed If the last OASIS assessment completed was the SOC or ROC, and a clinically significant problem was identified at that SOC or ROC visit, the problem (and/or related physician communication) would be reported at both the SOC/ROC (on M2002)reported at both the SOC/ROC (on M2002), and again at Transfer or Discharge (on M2004) since the time frame underM2004), since the time frame under consideration for M2004 is since OR AT the previous OASIS assessmentp
M2010Patient/CaregiverHighRiskDrug EducationDrugEducation

HighRiskDrugsDefined
High-risk medications are those identified by li i i h i id blquality organizations as having considerable
potential for causing significant patient harm when they are used erroneouslywhen they are used erroneously. Institute for Safe Medication Practices (High Alert
Med List)JCAHO t JCAHO, etc.
Examples of high risk meds that could have a severe negative impact on patient safety andsevere negative impact on patient safety and healthHypoglycemicsAnticoagulants
M2010Patient/CaregiverHighRiskDrug EducationDrugEducation
Timepoints SOC ROCEducate on high risk meds firstEducate on high risk meds firstUnrealistic to expect that pt education on
ll d d i iall meds can occur on admissionRemember the timeframeOthers can provide the education, but
who has to mark the data item? 4b Q161 4who has to mark the data item? 4b-Q161.4
M2010HighRiskDrugEducation
Response “0” p Interventions were not completed as outlined in
this item. Clinician should document rationale in the clinicalClinician should document rationale in the clinical
record, unless the patient is not taking any drugs Response “1”
Hi h i k d ib d d d tiHigh risk meds are prescribed and education was provided
ALF—staff are considered caregivers; may or g ymay not be appropriate to educate those administering medications 4b-Q161.3
Education can be over the phone 4b-Q161 4Education can be over the phone 4b Q161.4
M2015Patient/CaregiverDrugEducation InterventionEducationIntervention

M2015DrugEducationIntervention
Timepoints Transfer Discharge Identifies if clinicians instructed the pt/cg
(ALF—staff are considered caregivers; pharmacists are considered caregivers) 4b Q162 3pharmacists are considered caregivers) 4b-Q162.3, 162.4
Education can occur over the phone 4b-Q161.4
H t d ff ti l d f l th h How to manage meds effectively and safely throughKnowledge of effectivenessPotential side effectsPotential side effects Drug reactions When to contact the appropriate careWhen to contact the appropriate care
provider
M2015Patient/CaregiverDrugEducation InterventionEducationIntervention
Response No-- Response No Interventions are not completed as outlined in this
item Care provider should document rationale in the
clinical recordR Y Response Yes— Includes education by any agency staff Has to be all 4 components Has to be all 4 components
Note that just including written materials in the bag with the medications at the time the medication is dispensed may not provide the specified education.
M2015Patient/CaregiverDrugEducation InterventionEducationIntervention
Mr Walt’s ROC was completedMr. Walt s ROC was completed November 8th. The SN documented education on all (high risk and non higheducation on all (high risk and non high risk meds) of the patient’s meds was completed at that time The SN’scompleted at that time. The SN s documentation included how and when to report problems that may occurto report problems that may occur.
Mr. Walt is transferred to the hospital on N b 10th H ill l tNovember 10th. How will you complete M2015? 4b-Q162.2
M2015 - Patient/Caregiver Drug Education Intervention, reports if, at the time of or since the previous OASIS assessment, the patient and/or caregivers were educated regarding ALL theircaregivers were educated regarding ALL their medications (not just the high risk medications), including how and when to report problems thatincluding how and when to report problems that may occur. If this specified education was accomplished for all medications at the time of the previous OASIS assessment, the appropriate response for M2015 would be “Yes”.
M2015
When answering M2015 - Patient/CaregiverWhen answering M2015 Patient/Caregiver Drug Education Intervention, if you provide education intervention on all pmedications during the first episode, but no education in the second episode because the patient had no new medications and there was no need to re-t h ll di ti d h tteach on all medications, do you have to answer “No” for M2015 at Transfer/Discharge?Transfer/Discharge?
The Condition of Participation 484.55 requires a Drug Regimen Review (DRR) at every comprehensiveRegimen Review (DRR) at every comprehensive assessment time point. When performing the DRR, at the Recertification, if the assessing clinician evaluated the patient's retention of prior teaching and determined and documented that the patient possessed all the required knowledge related to allpossessed all the required knowledge related to all medications, then M2015 would be answered "Yes" at Transfer/Discharge. If the assessing clinician had not re-assessed the patient's medication knowledge and found the patient to be fully knowledgeable or not provided drug educationknowledgeable or not provided drug education related to all medications at the time of or since the previous OASIS assessment, the M2015 response
ld b "N " t T f /Di hwould be "No" at Transfer/Discharge
M2020ManagementofOralMedicationsMedications
M2020ManagementofOralMedicationsMedications
If patient’s ability to manage oral meds varies If patient s ability to manage oral meds varies from medication to medication, consider the medication for which the most assistance is needed when selecting a responseneeded when selecting a response.
If the medication is ordered prn, and on the day If the medication is ordered prn, and on the day of assessment the patient needed a reminder for this prn, then the patient would be a "2". If on the day of assessment the patient did not needthe day of assessment, the patient did not need any prn medications, therefore no reminders, then assess the patient's ability on all of the medications taken on the day of assessment Ch 3medications taken on the day of assessment. Ch 3

M2020ManagementofOralMedicationsMedications
Assess patient’s ability to take medications reliably and safely at all timesId ifi i ’ bili illi Identifies patient’s ability, not willingness or compliance or actual performance
Patient must be viewed from holistic perspective Patient must be viewed from holistic perspectiveMental EmotionalEmotional Cognitive status
A ti iti itt dActivities permitted Environment
M2020ManagementofOralMedicationsMedications
Abilit b t il tl li it d b Ability can be temporarily or permanently limited by:Physical impairments (e.g. limited manual
dexterity)dexterity)Emotional/cognitive/behavioral
impairments (e.g., memory deficits,impairments (e.g., memory deficits, impaired judgment, fear)
Sensory impairments, (e.g., impaired y p ( g pvision, pain)
Environmental barriers (e.g. access to kitchen or medication storage area, stairs, narrow doorways)
M2020ManagementofOralMedicationsMedications
Timepoints SOC/ROC/DCp Includes all prescribed and OTC oral meds
included on the POC Excludes topical, injectable and IV meds Excludes inhalation meds and sublingual meds
(Oct 2012)(Oct 2012)
Excludes swish and expectorate meds (Jan 2013)
Meds given per gastrostomy or other tube are Meds given per gastrostomy or other tube are not po 4b-Q167.8
Does not include filling/reordering 4b-Q166g g Meds swallow & absorbed through GI system!!
M2020ManagementofOralMedicationsMedications
Response 0 Patient sets up her/his own ‘planner Response 0 Patient sets up her/his own planner device’ and is able to take the correct med in the correct dosage at the correct time
Response 1 Patient is independent in oral med p
administration, but requiresanother person to prepare individual doses
(e.g., sets up a planner device) And/or if another person develops a drug
di h hi h h i lidiary or chart which the patient relies on to take meds appropriately

M2020ManagementofOralMedicationsMedications
Response 2P ti t i th tPatient requires another person to provide reminders
What about a device that provides reminders?Who sets up the device? 4b-Q167.5
ExamplesofResponse34b Q167 5 14b‐Q167.5.1
A patient who decided not to take her new pmedications, because the varying doses worried her, and she was unsure of the instructions. There had not been a medi-set up, nor reminders p,tried. The clinician would select Response 3 because it is unclear until reassessment if the interventions will be successfulinterventions will be successful.
A patient who, upon assessment, was not able to take prescribed medications at the correct time and doses even though remindedand doses even though reminded.
A patient who, on the day of assessment, was prescribed oral medications, but was unable to p ,safely swallow.
The patient is on multiple medications which span 3 times a day. Yesterday, the doctor started her on a varying dose of Prednisone. The patient admits to being confused about the directions and right dosage. The clinician observes that g gthe med box the patient set up is filled correctly with all usual medications, but not correctly with the prescribed Prednisone administration. The clinician also notes that the medication for last evening remained in the pill planner. Upon questioning, the patient admits to being tired and forgetting to take her evening medication. The nurse g g gdiscusses the use of an alarm clock to remind her to take her evening medication and fixes the Prednisone dosage for the rest of the week. Considering this patient needed g phelp with setting up one medication (Response 1) and a reminder for another (Response 2) in the last 24 hrs, what is the correct scoring with rationale for this situation? g
4b-Q167.9
"3-Unable to take medication unless administered by another person because on the day of theanother person because on the day of the assessment, the patient did not possess the ability to take the Prednisone at the correct time and dose and demonstrated that through her report and actions (required knowledge of the drug's dose and administration schedule )administration schedule ) Rationale: •Day of assessment•Do not report ability after skilled intervention, as this is not a reflection of what was true in the most dependent medication during the day of assessmentdependent medication during the day of assessment.
•The patient has to demonstrate success at taking p gmeds as ordered, at all times to move from a ‘3’.

M2020
If the patient does not have her If the patient does not have her prescribed medications in the home b h t ff d th dbecause she cannot afford them and she does not plan on getting them, what is the most appropriate response for M2020?p
4b-Q167.5.2
M2020
You are reporting the patient's ability to take all oralYou are reporting the patient s ability to take all oral medications reliably and safely at all times on the day of the assessment. If the patient did not take her
di ti th d f th t bmedications on the day of the assessment because they were not present in the home, you cannot make assumptions about a patient's ability to takeassumptions about a patient s ability to take medications she doesn’t have. If the medications were not in the home, you would not be able to determine if she could take each medication at the correct time and dose. The patient's status would be reported as “3-Unable to take medications unlessreported as 3 Unable to take medications unless administered by another person”.
QuizQ
Mrs. Wobble is unsteady while ambulating and i i i f b l i Sh
551
requires supervision for ambulation. She possesses the knowledge to take their medications reliably and safely if the bottles are placed near, or if she has supervision while ambulating to the medicationsupervision while ambulating to the medication storage area. Please advise how this patient would be scored for M2020, Management of Oral Medications. The item intent instructions include guidance relatedThe item intent instructions include guidance related to the patient’s ability to access the medication, how does this play into the question when the physical impairment causes the patient to require humanimpairment causes the patient to require human supervision or assistance and not the cognitive aspect (such as for reminders)?
4b-Q167.5.3
Answer
M2020 reports a patient's ability on the day of the k h l di i ll
552
assessment to take the correct oral medications at all the correct times. This would include the tasks of accessing the medications from the location where they are routinely stored in the home preparing thethey are routinely stored in the home, preparing the medications (including opening containers or mixing oral suspensions), selecting the correct dose and safely swallowing the medications typically involvingsafely swallowing the medications, typically involving having access to a beverage. If someone other than the patient must do some part of the task(s) that are required for the patient to access and/or take therequired for the patient to access and/or take the medication at the prescribed times, then the patient would NOT be considered independent (Response 0).

MoreScenarios
Scenario: Medications are routinely stored in the f i t l t d d t i Th ti t i
553
refrigerator located downstairs. The patient requires someone to assist them at medication administration time to walk to the location where the medications are routinely stored or someone must retrieve the medications andstored, or someone must retrieve the medications and bring them to the patient; Response "3" would apply. In this situation, just someone preparing the doses in advance did not enable the patient to self-administer their medications.
Scenario: The patient requires someone to prepare the medication doses in advance (e.g. visually they can't discern the appropriate dose) and to walk with them at all times to be safe Someone prepares the medi planner andtimes to be safe. Someone prepares the medi-planner and sets it within the patient's reach with the water they need to take the meds, the appropriate score is a "1", as the patient can access the medications from where they are routinely ca access t e ed cat o s o e e t ey a e out e ystored and has the water available to swallow the medication safely. 4b-Q167.5.3
MoreScenarios
If the medications were routinely stored in the kitchen d/ h il bl f h i
554
and/or the water was not available for the patient to self-administer and the patient required someone to assist them to the location where the meds were stored and or to water the appropriate score would bestored and or to water, the appropriate score would be a "3".
Scenario: Patient does not need doses prepared in d b t th di ti ti l t d iadvance, but the medications are routinely stored in a
location that the patient cannot access due to a physical, sensory, or environmental barrier. The patient is scored a "3" During the episode anpatient is scored a 3 . During the episode, an environmental modification was made, e.g. changing the medication storage and water supply to a location that the patient can access the patient could bethat the patient can access, the patient could be scored a "0" at the next OASIS data collection time point. 4b-Q167.5.3
M2030ManagementofInjectableMedicationsMedications
M2030ManagementofInjectableMedicationsMedications
Timepoints SOC/ROC/FU/Discharge Timepoints SOC/ROC/FU/Discharge Assess patient’s ability to take all injectable
meds reliably and safely at all timesmeds reliably and safely at all times Excludes
IV di tiIV medicationsInfusions (i.e. meds given via pump)Meds given in the physician’s office or
other settings outside the home 4b-Q168.3

M2030ManagementofInjectableMedsMeds
Response -0 p Patient sets up own meds with correct med, dose and
time Response -1 Response 1
Patient independent in injectable med administration except that another person must prepare doses and/or if another person must develop a drug diary or chartanother person must develop a drug diary or chart
Response -2 Reminders to take meds are necessary, regardless of
whether the pt is independent or needs assistance inwhether the pt is independent or needs assistance in preparing individual doses and/or developing a drug diary or chart.
Note: Reminders provided by a device that the patient Note: Reminders provided by a device that the patient can independently manage are not considered ‘assistance’ or ‘reminders’
M2030ManagementofInjectableMedsMeds
Response 3—Unable to take medication unless Response 3 Unable to take medication unless administered by another personThe physician orders the nurse to administer the
di ti ( t di l t i timedication (represents a medical restriction against self-administration) if not for convenience 4b-Q168.2, 168.3Q ,
If an injection is ordered but not administered the day of t th li i i ill th t f thassessment, the clinician will use the assessment of the
patient’s cognitive and physical ability and make an inference regarding what the patient would be able to do. 4b Q168 34b-Q168.3
M2030ManagementofInjectableMedications
If patient’s ability to manage injectable meds If patient s ability to manage injectable meds varies from medication to medication, consider the medication for which the most assistance is needed when selecting a response.
The patient administers his own insulin safely and reliably but his doctor has ordered B12 IM. What response? 4b-Q168.4
Wh if h d h i i hi What if the doctor wants the patient to come into his office for the IM injection?
The doctor orders that the patient receive a flu The doctor orders that the patient receive a flu vaccine?? 4b-Q168.5.1
WhatdoesM2030include?
M2030 requires an assessment of the patient's i i d h i l bili d h
560
cognitive and physical ability to draw up the correct dose accurately using aseptic technique, inject in an appropriate site using correct technique, and dispose of the syringe properly " My patient at the SOC wasof the syringe properly." My patient, at the SOC, was throwing his used needles and syringes into the trash. He stated he was never told how to properly dispose of them 4b Q168 3 1of them. 4b-Q168.3.1
If the patient lacked the knowledge regarding safe needle and syringe disposal on the day of the assessment the patient was unable to take injectableassessment, the patient was unable to take injectable medication unless administered by another person, Response 3. If the patient needed reminders regarding safe needle/syringe disposal they would beregarding safe needle/syringe disposal, they would be scored a "2".

M2030atDischargeg
Scenario 1: The first two weeks of the episode, the i h d L SQ d d Th i i b i
561
patient had Lovenox SQ ordered. The patient is being discharged 4 weeks later with no injectable medications currently ordered. At discharge, is the answer NA no injectable medications prescribed oranswer NA - no injectable medications prescribed or do we assess their ability from earlier in the episode?
Scenario 2: Is the order to administer the flu vaccine t th b i i f th i d i l d d hat the beginning of the episode included when
selecting a response for M2030 at the Discharge assessment?A t b th If th t i d Answer to both: If there are no current, ongoing orders for an injectable to be administered IM or SQ via needle and syringe in the home at the time of the assessment the appropriate response is NA 4b Q168 1 1assessment, the appropriate response is NA. 4b-Q168.1.1
M2040PriorMedicationManagement
•Timepoints SOC ROC•If patient’s ability varies from one med to another,If patient s ability varies from one med to another, consider the med that takes the most assistance when selecting your answer•Includes only those administered at home 4b-Q168.5.2
M2040 PriorMedicationManagementg
Independent Independent Patient completed activity by him/herself
(with or without assistive device)(with or without assistive device) Without physical or verbal assistance
from a helper or reminders from anotherfrom a helper or reminders from another personR i d id d b d i th t thReminders provided by a device that the pt can independently manage are not
id d i t i dconsidered assistance or reminders
M2040 PriorMedicationManagementManagement
‘Needed some help’ means that the patient Needed some help means that the patient required some help from another person to accomplish the task/activity.
‘Dependent’ means that the patient was incapable of performing any of the task/activity. p p g y yFor oral meds this means that the pt was capable only of swallowing meds that were given to him/her. For injectable meds, this g j ,means that someone else must have prepared and administered the meds.
NA There were no oral or injectable meds
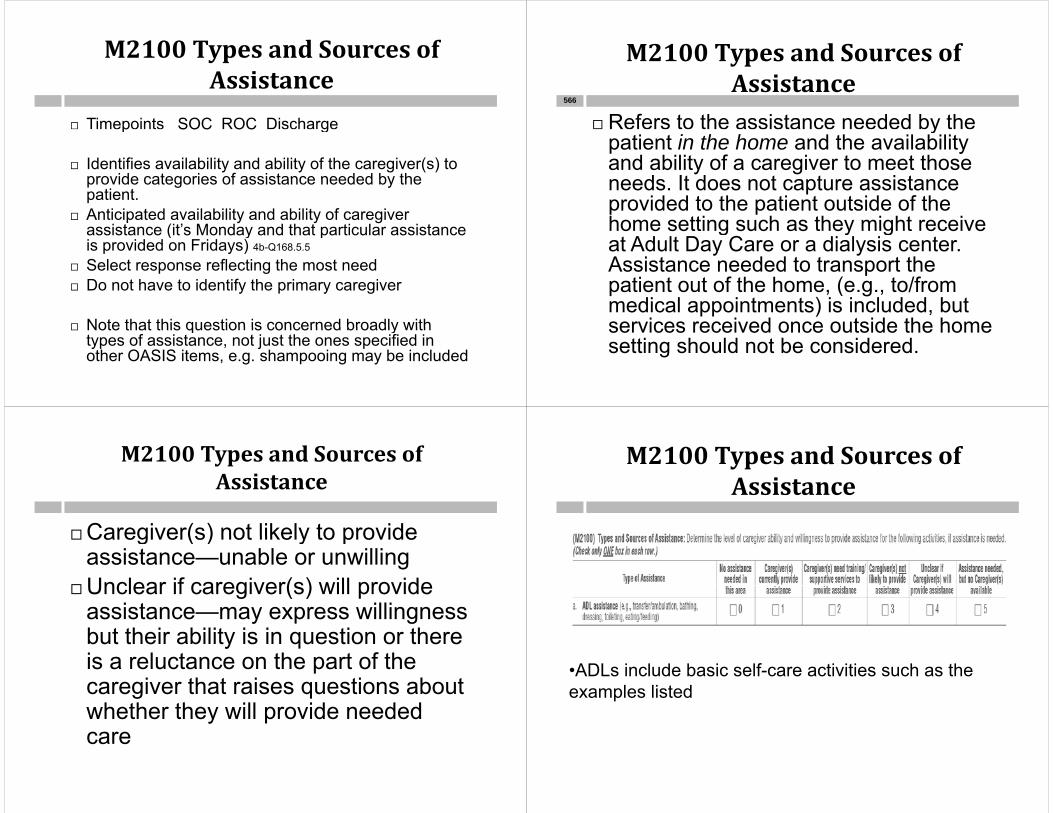
M2100TypesandSourcesofAssistanceAssistance
Timepoints SOC ROC Dischargep SOC OC g
Identifies availability and ability of the caregiver(s) to provide categories of assistance needed by theprovide categories of assistance needed by the patient.
Anticipated availability and ability of caregiver assistance (it’s Monday and that particular assistanceassistance (it s Monday and that particular assistance is provided on Fridays) 4b-Q168.5.5
Select response reflecting the most need Do not have to identify the primary caregiver
Note that this question is concerned broadly with Note that this question is concerned broadly with types of assistance, not just the ones specified in other OASIS items, e.g. shampooing may be included
M2100TypesandSourcesofAssistanceAssistance
Refers to the assistance needed by the 566
ypatient in the home and the availability and ability of a caregiver to meet those
d It d t t i tneeds. It does not capture assistance provided to the patient outside of the home setting such as they might receivehome setting such as they might receive at Adult Day Care or a dialysis center. Assistance needed to transport the
ti t t f th h ( t /fpatient out of the home, (e.g., to/from medical appointments) is included, but services received once outside the homeservices received once outside the home setting should not be considered.
M2100TypesandSourcesofAssistanceAssistance
Caregiver(s) not likely to provideCaregiver(s) not likely to provide assistance—unable or unwilling
Unclear if caregiver(s) will provideUnclear if caregiver(s) will provide assistance—may express willingness but their ability is in question or therebut their ability is in question or there is a reluctance on the part of the caregiver that raises questions aboutcaregiver that raises questions about whether they will provide needed carecare
M2100TypesandSourcesofAssistanceAssistance
•ADLs include basic self-care activities such as the examples listed

M2100TypesandSourcesofAssistanceAssistance
•IADLs include activities associated with independent living necessary to support the ADLs such as the examples listed. Determine the IADL with the most
dneed•Includes Meals on Wheels 4b-Q168.5.6
M2100TypesandSourcesofAssistance—ONLYincludemedsadministeredathomeCMSQ&A
July2010
Only meds received at home.•Medication administration refers to any type of y ypmedications (prescribed or OTC) and any route of administration including oral, inhalant, injectable, topical, or administration via g-tube/j-tube, etc.•C/G needs help to fill pill box—2 Oct 2012
M2100TypesandSourcesofAssistanceAssistance
•Medical procedures/treatments include procedures/ treatments that the physician or physician designee has ordered for the purpose of improving health status Some examples of thesepurpose of improving health status. Some examples of these procedures/ treatments include wound care and dressing changes (including change of the sponge of the wound vac),
f ti i i t itt t i th t i tirange of motion exercises, intermittent urinary catheterization, postural drainage, electromodalities, etc.
M2100
What is the appropriate response for M2100 What is the appropriate response for M2100, Types and Sources of Assistance, in cases where the physician has ordered the RN towhere the physician has ordered the RN to provide the treatment, e.g. a wound VAC procedure? p
Could fall under Medical procedures and management of equipment 4b-Q170.10
3-Caregivers not likely to provide. 5-if there is no caregiver involved 4b-Q170.11
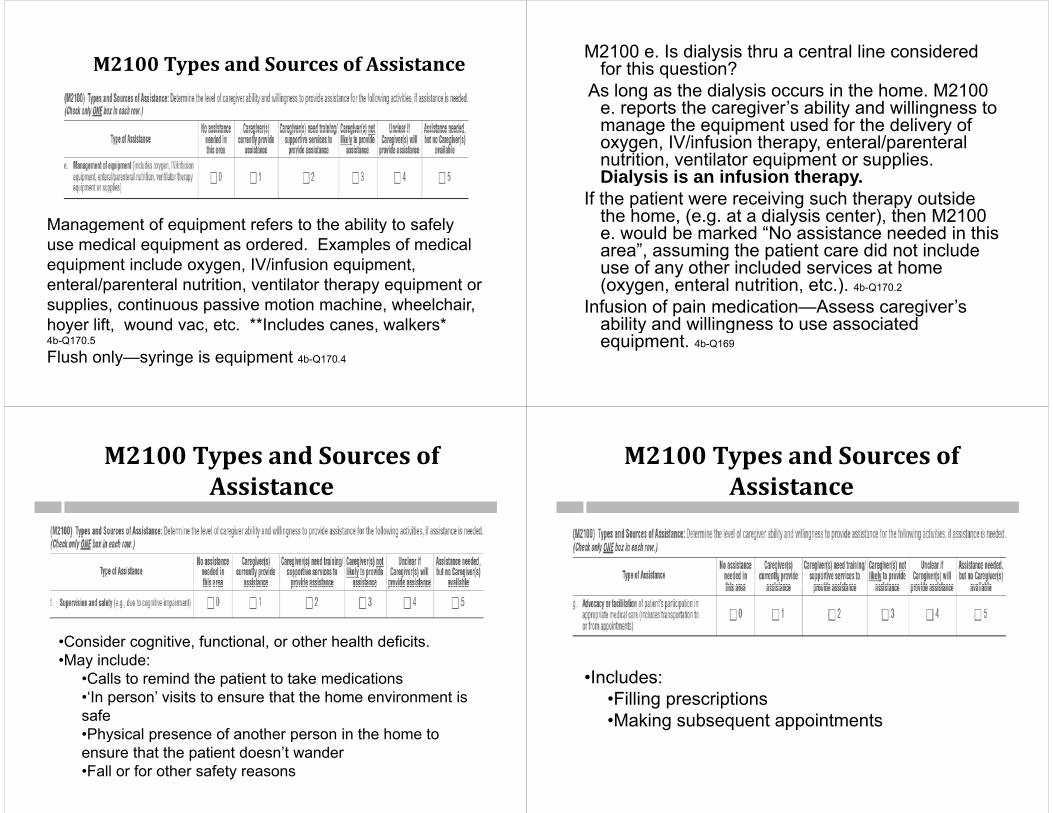
M2100TypesandSourcesofAssistance
Management of equipment refers to the ability to safelyManagement of equipment refers to the ability to safely use medical equipment as ordered. Examples of medical equipment include oxygen, IV/infusion equipment, enteral/parenteral nutrition, ventilator therapy equipment or supplies, continuous passive motion machine, wheelchair, hoyer lift wound vac etc **Includes canes walkers*hoyer lift, wound vac, etc. Includes canes, walkers 4b-Q170.5
Flush only—syringe is equipment 4b-Q170.4
M2100 e. Is dialysis thru a central line considered for this question?
As long as the dialysis occurs in the home. M2100 e. reports the caregiver’s ability and willingness to manage the equipment used for the delivery ofmanage the equipment used for the delivery of oxygen, IV/infusion therapy, enteral/parenteralnutrition, ventilator equipment or supplies. Dialysis is an infusion therapyDialysis is an infusion therapy.
If the patient were receiving such therapy outside the home, (e.g. at a dialysis center), then M2100
ld b k d “N i t d d i thie. would be marked “No assistance needed in this area”, assuming the patient care did not include use of any other included services at home ( l i i )(oxygen, enteral nutrition, etc.). 4b-Q170.2
Infusion of pain medication—Assess caregiver’s ability and willingness to use associatedability and willingness to use associated equipment. 4b-Q169
M2100TypesandSourcesofAssistanceAssistance
•Consider cognitive, functional, or other health deficits. •May include:
•Calls to remind the patient to take medicationsp•‘In person’ visits to ensure that the home environment is safe•Physical presence of another person in the home to•Physical presence of another person in the home to ensure that the patient doesn’t wander•Fall or for other safety reasons
M2100TypesandSourcesofAssistanceAssistance
•Includes:•Filling prescriptions•Making subsequent appointments

M2100TypesandSourcesofAssistanceAssistance
The types of assistance that a foley catheter The types of assistance that a foley catheter patient might need may be captured in multiple rows in M2100, Types and Sources of Assistance as described below:Assistance, as described below:
a- ADL assistance as part of toileting hygiene? - Examples: cleansing around the yg p gcatheter/peri care
d- Medical procedure? Examples: insertion/removal of catheter e g self cath orinsertion/removal of catheter, e.g. self cath or intermittent catheterization
e- Management of equipment? - Examples: t i th b h i th bemptying the bag, changing the bag
4b-Q170.7
M2100TypesandSourcesofAssistanceAssistance
How is "Assistance needed, but no Caregiver(s) available" defined? Would it apply to a son who is managing equipment and assists
578
Would it apply to a son who is managing equipment and assists with ADLs safely and independently, but is unwilling to assist with medication administration and is unable to take the patient to doctor's appointments?
"Response 5 - Assistance needed, but no Caregiver(s) available" means the patient has no one involved in providing any level of care to them at all. In your example, the patient has a son who is providing some level of caregiver assistance; therefore, Response 5 p g g pwould not be an appropriate response. If the son was willing and able to manage equipment and assist with ADLS, the appropriate responses for Row a and Row e would be "1-Caregiver currently provides assistance." If the son was unwilling to assist with p gmedication administration and unable to take the patient to doctor's appointments, the appropriate responses for Row c, Medication administration and Row g, Advocacy or facilitation would be "3-Caregiver not likely to provide assistance" because this response is g ydefined as including situations where the caregiver is unwilling or unable to provide the needed care.
4b-Q170.12
M2110Howoftendoesthepatientreceive ADL or IADL assistance…?receiveADLorIADLassistance…?
M2110HowoftendoesthepatientreceiveADL or IADL assistance ?ADLorIADLassistance…?
Timepoints SOC ROC Discharge Timepoints SOC ROC Discharge Question is concerned broadly with ADLs and
IADLs not just the ones specified in other j pOASIS items
In M2100 you report the response that represents the most need and the availabilityrepresents the most need and the availability and ability of the caregiver to meet that need. In M2110, simply report the frequency that the patient receives assistance with anypatient receives assistance with any ADLs/IADLs. Because of the different approaches with these items, a logical "tie" b t th t t l b tbetween the two may not always be apparent.
4b-Q171.5.1
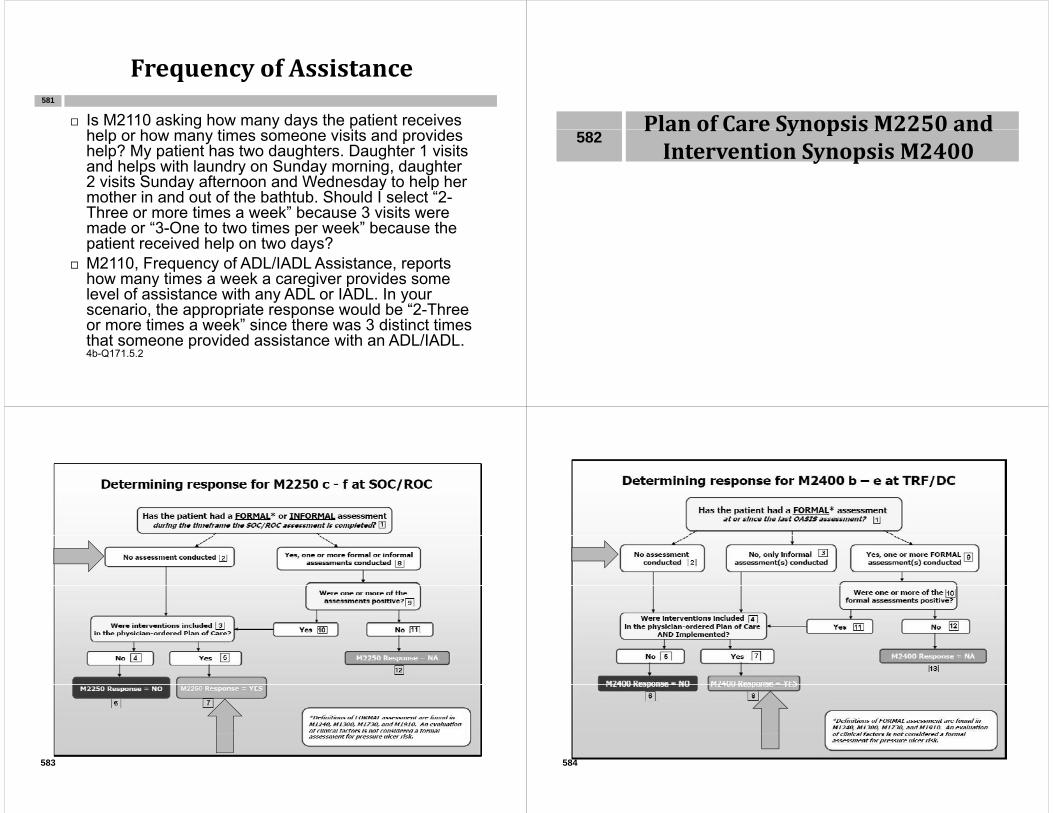
FrequencyofAssistanceq y
Is M2110 asking how many days the patient receives h l h i i i d id
581
help or how many times someone visits and provides help? My patient has two daughters. Daughter 1 visits and helps with laundry on Sunday morning, daughter 2 visits Sunday afternoon and Wednesday to help her2 visits Sunday afternoon and Wednesday to help her mother in and out of the bathtub. Should I select “2-Three or more times a week” because 3 visits were made or “3-One to two times per week” because themade or 3-One to two times per week because the patient received help on two days?
M2110, Frequency of ADL/IADL Assistance, reports how many times a week a caregiver provides somehow many times a week a caregiver provides some level of assistance with any ADL or IADL. In your scenario, the appropriate response would be “2-Three or more times a week” since there was 3 distinct timesor more times a week since there was 3 distinct times that someone provided assistance with an ADL/IADL. 4b-Q171.5.2
Plan of Care Synopsis M2250 andPlanofCareSynopsisM2250andInterventionSynopsisM2400
582
583 584
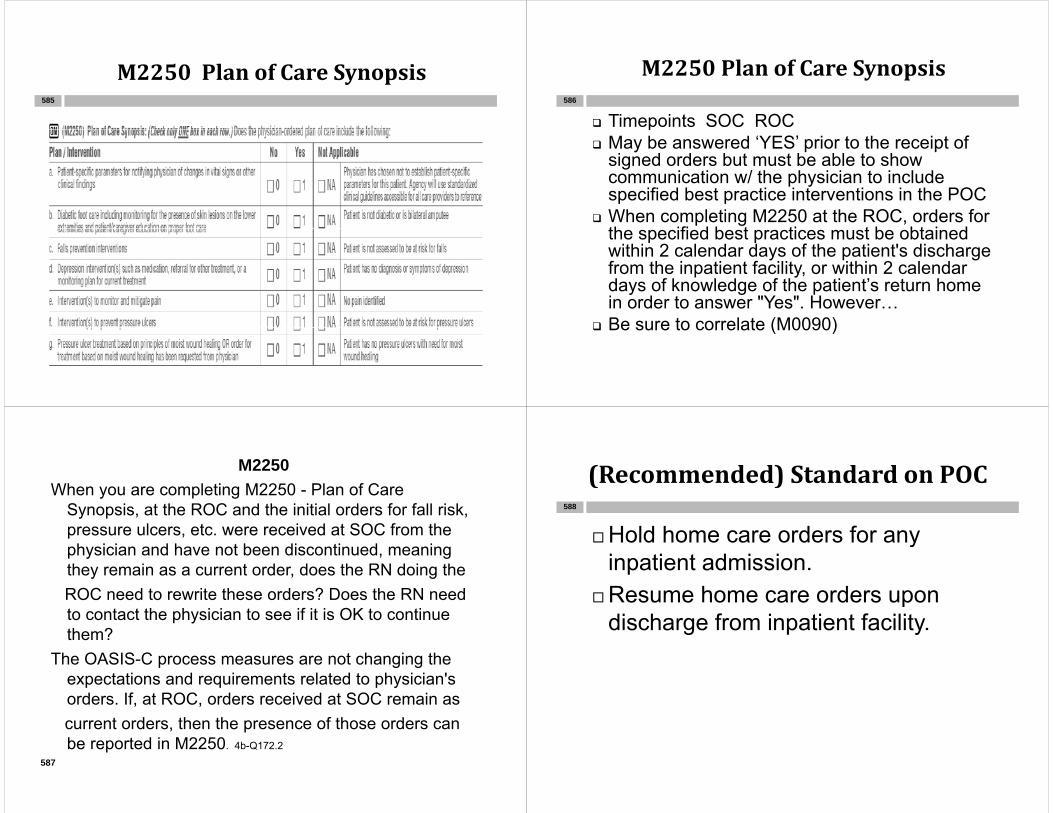
M2250PlanofCareSynopsisM2250PlanofCareSynopsis585
M2250PlanofCareSynopsisy p
Timepoints SOC ROC586
p May be answered ‘YES’ prior to the receipt of
signed orders but must be able to show communication w/ the physician to includecommunication w/ the physician to include specified best practice interventions in the POC
When completing M2250 at the ROC, orders for th ifi d b t ti t b bt i dthe specified best practices must be obtained within 2 calendar days of the patient's discharge from the inpatient facility, or within 2 calendar days of knowledge of the patient’s return home in order to answer "Yes". However…
Be sure to correlate (M0090) Be sure to correlate (M0090)
M2250Wh l ti M2250 Pl f CWhen you are completing M2250 - Plan of Care
Synopsis, at the ROC and the initial orders for fall risk, pressure ulcers, etc. were received at SOC from the p ,physician and have not been discontinued, meaning they remain as a current order, does the RN doing theROC need to rewrite these orders? Does the RN need to contact the physician to see if it is OK to continue them?them?
The OASIS-C process measures are not changing the expectations and requirements related to physician'sexpectations and requirements related to physician s orders. If, at ROC, orders received at SOC remain ascurrent orders, then the presence of those orders can
587
be reported in M2250. 4b-Q172.2
(Recommended)StandardonPOC( )
Hold home care orders for any588
Hold home care orders for any inpatient admission.
Resume home care orders upon discharge from inpatient facility.g y

M2250PlanofCareSynopsisy p
Yes POC contains orders for best practice 589
pinterventions as specified in each row, based on the patients needs. (Even though these are general interventions often performed without orders CMSinterventions often performed without orders, CMS expects orders. 4b-Q172.3)
No The best practice interventions specified in this fitem are not included in the plan of care that was
developed as a result of the comprehensive assessment, unless the plans/ interventions specified , p pin that row are not appropriate for this patient - see guidance on selecting NA for each row below.
Could it be determined that all these specific best practice orders were present if the communication with the o de s e e p ese t t e co u cat o t t ephysician were more general (like the patient's clinical findings are discussed with the physician and there is an agreement as to the general POC between the admitting clinician and the physician Then the formal detailed POC isclinician and the physician. Then the formal detailed POC is sent to the physician for signature, outlining the specific parameters and interventions)? 4b-Q172.9.2
The OASIS-C process measures are not changing the The OASIS C process measures are not changing the expectations and requirements for communicating with the physician to obtain verbal orders prior to providing services. The Medicare Benefit Policy Manual, defines clearly how orders can be obtained verbally if complete orders were not provided in thebe obtained verbally if complete orders were not provided in the referral. Chapter 7, Section 30.2.5 states: "Services which are provided from the beginning of the 60-day episode certification period based on a request for anticipated payment and before th h i i i th l f id d t bthe physician signs the plan of care are considered to be provided under a plan of care established and approved by the physician where there is an oral order for the care prior to rendering the services which is documented in the medical
590
rendering the services which is documented in the medical record and where the services are included in a signed plan of care."
M2400InterventionSynopsisy p591
M2400InterventionSynopsis
Timepoints Transfer Discharge592
Were there specific interventions that were ordered by the physician AND implemented as part of the plan of care? Used to calculate process measures to capture use of best
practices Problem specific interventions referenced in the item may
di l l d i i hor may not directly correlate to stated requirements in the CoPs
Included in the POC, but not implemented, then NO Every ‘NO” requires documentation for rationale Multiple interventions but only some or one implemented,
‘yes’ 4b-Q182.7
If not appropriate for this patient, then NA.

M2400InterventionSynopsisy p
You may say "Yes" to M2400 b - e, if the 593
y y ,specified clinical interventions were included in the physician ordered plan of care and implemented at the time of orcare and implemented at the time of or since the previous assessment whether or not a formal assessment was performed.
S fHowever, the Response Specific Instructions state that for Rows b-e, in order to select "NA-Not applicable" a formalto select NA Not applicable , a formal assessment must have been performed as defined in the relevant OASIS items. 4b-Q172.9.4, 172 9 5172.9.5
InterventionsPriortoSOC
For situations where best practices are provided during an initial assessment visit that is conducted BEFORE the SOC date would
594
assessment visit that is conducted BEFORE the SOC date, would those clinical assessments/interventions be considered as being provided "since or at the last OASIS assessment" or "within the outcome episode"? For example, in a situation of a Friday referral for a therapy only case the RN makes a non billable visit on a Saturdaya therapy only case, the RN makes a non-billable visit on a Saturday to meet the federal requirement that the initial assessment visit must occur within 48 hours of the referral. No nursing need existed and no billable service was provided, therefore Saturday was not the SOC date The patient was a diabetic but had no skilled nursing needsdate. The patient was a diabetic, but had no skilled nursing needs related to their diabetes, the nurse however, assessed the lower extremities for lesions, found no lesions, and verified the patient understood how to care for her feet. The PT did not assess the lower extremities for lesions and did not address the foot care education inextremities for lesions and did not address the foot care education in any way before discharge.
None of the interventions that the nurse provided on the initial assessment visit would be considered when responding to M2400, gIntervention Synopsis, even if orders existed, because the interventions were completed before the quality episode began on the SOC date.
M2250PlanofCareSynopsis595
"Yes" if the plan of care includes specific parameters ordered by the physician for this specific patient or after reviewing the agency's standardized parameters with the physician, s/he agrees they would meet the needs of this specific patient. • "No" if there are no patient specific parameters on the plan of care and the agency will not use standardized physician notification parameters for thisagency will not use standardized physician notification parameters for this patient. • "NA" if the agency uses their own agency standardized guidelines, which the physician has NOT agreed to include in the plan of care for this particularphysician has NOT agreed to include in the plan of care for this particular patient. The parameters must appear on the POC!! “Follow AHA guidelines” not acceptable! 4b-Q172.5.3
M2250PlanofCareSynopsis
NO: POC contains orders for only one (or none) of the interventionsYES: POC contains both orders for a) monitoring the skin of the patient’s lower extremities for evidence of skin lesions AND ppatient education on proper foot careNA: Patient does not have a diagnosis of diabetes or is a bilateral amputee **Note: This question does not apply tobilateral amputee Note: This question does not apply to diagnosis Diabetes Insipidus 4b-Q172.6
596

(M2400) I t ti S i(M2400) Intervention Synopsis
NO: If POC contains orders for only 1 of the interventions and/or only 1 type of intervention (monitoring or education) or th i ti d i li i l dthere is no supportive doc in clinical recordYES: POC must contain both orders for monitoring the skin AND patient education on proper care of lower extremities AND p p pthere is supportive clinical documentation that this was done at the time of the previous OASIS assessment or since that timeN/A: Patient does not have a diagnosis of diabetes or is a
597
N/A: Patient does not have a diagnosis of diabetes or is a bilateral amputee
M2250PlanofCareSynopsisy p598
NO: Best practice interventions not included in the POCYES: POC includes planned clinical interventions to reduce pressure on bony prominences or other areas of skin at risk for breakdownof skin at risk for breakdown. NA: Patient was not indentified as at risk for pressure ulcersulcers
NO: POC does not include interventions to prevent pressure ulcers and/or no interventions werepressure ulcers and/or no interventions were documented in the clinical record YES: POC contains interventions to reduce pressure on bony prominences or other areas of skin at risk for breakdown and the clinical record contains documentation that these interventions were performeddocumentation that these interventions were performed at the time of the previous OASIS assessment or since that time
599
that time . NA: Formal assessment indicates the patient was not at risk for pressure ulcers
PreventionofPressureUlcers
Planned interventions can include600
Planned interventions can include teaching on frequent position changes proper positioning to relieve pressure careful skin assessment and hygiene use of pressure-relieving devices such
as enhanced mattresses, etc. ,

M2250PlanofCareSynopsisy p601
NO: Best practice interventions not included in the POCYES: POC contains orders for pressure ulcer treatments based on principles of moist wound healing (e.g., moisture retentive dressings) OR if such orders have been requested from the physicianNA: Patient has no pressure ulcers needing moistNA: Patient has no pressure ulcers needing moist wound healing treatments (physician says ‘no’)4b-Q172.9.1
NO: POC does not include interventions for treatments based i i l f i t d h li d/ t t ton principles of moist wound healing and/or no treatments
based on principles of moist wound healing documented YES: POC contains interventions for pressure ulcer treatments pbased on principles of moist wound healing and there is supportive documentation in the clinical record interventions were carried out at the time of the previous OASIS assessmentwere carried out at the time of the previous OASIS assessment or since then. NA: dressings that support the principles of moist wound h li t i di t d f thi ti t’ l OR
602
healing were not indicated for this patient’s pressure ulcers OR patient has no pressure ulcers with need for moist wound healing.
Onlyoneulcerhasmoistwoundtreatmenttreatment
A patient has two pressure ulcers for which wet-to-dry d i d d Aft th SOC t thdressings are ordered. After the SOC assessment, the assessing clinician requests and receives an order for moist wound healing treatment for one of the pressure ulcers, without any discussion about appropriateness/inappropriateness of moist wound healing for the second ulcer. The moist wound healing treatment is provided and documented for the one g ppressure ulcer as ordered. How should 2400 be answered?
4b-Q172.9.3.1
There is no requirement that every pressure ulcer be treated There is no requirement that every pressure ulcer be treated with moist wound healing in order to mark "Yes" for M2250 (g) or M2400 (f). If the agency has orders for and implements
i t d h li t t t f t l t lmoist wound healing treatment for at least one pressure ulcer within the required time frames, then M2400 (f) should be "Yes".
MoistWoundHealingg
Principles of moist wound healing604
Principles of moist wound healing promote an optimal wound
i t d i l d filenvironment and includes films, alginates, hydrocolloids, hydrogels, collagen, negative pressure wound therapy, unna boots, medicated py, ,creams/ointments

If a clinician teaches Diabetic foot care, Prevention of f /falls, and/or pressure ulcers etc. on the discharge visit and then finds out that these were not included on the Plan of Care Synopsis, what would be the best way to y p , yanswer M2400 - Intervention Synopsis?
The response would have to be “No” if there were no orders for these best practices. In order to answer M2400 – Intervention Synopsis "Yes", the physician-y p , p yordered plan of care at the time of or since the previous OASIS assessment must have included the specified best practice intervention in addition tospecified best practice intervention, in addition to evidence that the interventions were implemented. Please remember that the physician plan of care includes the plan of care for certification/recertificationincludes the plan of care for certification/recertification in addition to all other addendum orders. 4b-Q182.5605
M2400andLongTermPatients
For example, foley catheter patient—all teaching has b d f h i i d hibeen done so further visits to do teaching are non-covered.
How is M2400 completed?p Since or at the last time OASIS completed If no orders on POC and/or no evidence of implementation,
then must mark ‘no’ (unless NA) During that time period, if specific orders were present,
and the clinician confirmed the patient/caregiver possessed the knowledge regarding the best practice th t t ht i i i d t th R tifi tithat was taught in a prior episode at the Recertification visit or on a subsequent visit, then upon confirmation that the patient/caregiver possessed the knowledge, the intervention may be considered implementedthe intervention may be considered implemented.
M2400andLongTermPatientsg
“Reviewed pressure ulcer prevention Reviewed pressure ulcer prevention, pain mitigation, and falls prevention with patient/caregiver. Patient/caregiver state
d di N f h i iunderstanding. No further intervention required.” (example note on recertassessment)assessment)
Adherence rate of 100% for the process measures???measures???
Note that none of the process measures for long-term episodes (those that include g p (a Recertification or Other Follow-up) are publicly reported
E C M2300EmergentCareM2300s608

M2300 Emergent CareM2300EmergentCare609
M2300 Emergent CareM2300EmergentCare610
Timepoints Transfer/Discharge Responses to this item include the entire Responses to this item include the entire
period since the last time OASIS data were collected, including current events.collected, including current events.
“Since the last time OASIS data were collected ” means “since or at the lastcollected… means since or at the last time” 4b-Q178.1
M2300 Emergent CareM2300EmergentCare
Excludes611
ExcludesUrgent care services not provided in a hospital
emergency department g y pDoctor's office visits scheduled less than 24
hours in advanceCare provided by an ambulance crew without
transportCare received in urgent care facilities
This item only includes holding and observation in the emergency department setting
M2300 Emergent CareM2300EmergentCare
Response 0—No 612
pNo emergent care in hospital emergency
dept ORdept ORPatient is direct admitted to the hospitalPatient was not treated or evaluated in thePatient was not treated or evaluated in the
emergency roomPatient had no other emergency departmentPatient had no other emergency department
visits since the last OASIS assessment.
M2300 Emergent CareM2300EmergentCare
Response 1 or 2 Yes613
Response 1 or 2--YesPatient went to a hospital emergency
fdepartment, regardless of whether the patient/caregiver independently made the d i i k ddecision to seek emergency department services or was advised to go the
d b h h i iemergency department by the physician, home health agency, or other health care
idprovider 4b-Q179
M2300 Emergent CareM2300EmergentCare
Response 2 Yes with admission614
Response 2—Yes with admissionPatient went to a hospital emergency
department and was subsequently admitted to the hospital
An OASIS transfer assessment is required (assuming the patient stay was for 24 hours or more for reasons other than diagnostic testing).
M2300 Emergent CareM2300EmergentCare
What if a patient went to a hospital emergency 615
p p g ydepartment, was “held” at the hospital for observation, then released?The patient did receive emergent care.
The time period that a patient can be "held" without p padmission can vary
An OASIS transfer assessment is not required if the patient was never actually admitted to an inpatient facility.
M2310ReasonforEmergentCareg616

M2310 Reason for Emergent CareM2310ReasonforEmergentCare
Timepoints Transfer/Discharge617
Timepoints Transfer/DischargeEmergency Room only If more than one reason contributed to the hospital
emergency department visit, mark all appropriate responses (include why even though not diagnosed)
Improper medication administration, regardless of h ( ti t i di l t ff)who (patient, caregiver, or medical staff)
administered the med improperly. 4b-Q181.5
M2310 Reason for Emergent CareM2310ReasonforEmergentCare
If the reason is not included in the choices, mark618
If the reason is not included in the choices, mark Response 19 - Other than above reasons.
If Pt received emergent care in a hospital ED multiple g p ptimes since the last time OASIS data were collected, include the reasons for all visits.
Include both the reasons care was sought and care received. 4b-Q181.5.1
Injury?j y
When answering M2310 (Reason for emergent g ( gcare) how is the term “injury” defined in Response 2-Injury caused by fall? I understand a fractured bone is an injury, but what about ecchymosis, j y, y ,increased edema, neurological changes (no confirmed neurological diagnosis as far as a bleed etc ) lacerations abrasions etc ? 4b-Q181 5 2bleed, etc.), lacerations, abrasions, etc.? 4b Q181.5.2
Injury means that hurt, damage or loss is sustained by the patient. The assessing clinician may use this definition and clinical judgment tomay use this definition and clinical judgment to determine whether or not the patient was "injured" when they fell.
M2410TowhichInpatientFacilityhas the patient been admitted?hasthepatientbeenadmitted?
620
R R l DCReRegular DC

M2410InpatientFacilityp y
Timepoints Transfer Discharge621
p g Special considerations:
• If admitted to more than one facilityI di t th f ilit t hi h th ti tIndicate the facility to which the patient was admitted first**
Patient dies in a hospital ED Patient dies in a hospital EDComplete a TRNSelect Response ‘1 Hospital’ for M2410
Nursing home admissionSkilled nursing facility (SNF) ICF/MR ICF/MR
M2410InpatientFacilityp y
Rehab Facility Admission622
Rehab Facility AdmissionFreestanding rehab hospitalCertified distinct rehab unit of a nursing homeCertified distinct rehab unit of a nursing homeDistinct rehab unit in a short stay acute
hospitalhospital Chemical dependency inpatient program of a
hospital whether it is a free-standing drughospital whether it is a free standing drug rehabilitation unit or a distinct drug rehabilitation unit that is part of a short-stay p yacute hospital is marked “1-Hospital”.
M2410. A patient receiving skilled nursing care from an HHA nder Medicare is periodicallfrom an HHA under Medicare is periodically placed in a local hospital under a private pay arrangement for family respite The hospitalarrangement for family respite. The hospital describes this bed as a purely private arrangement to house a person with no skilledarrangement to house a person with no skilled services. This hospital has acute care, swing bed, and nursing care units. The unit where thebed, and nursing care units. The unit where the patient stays is not Medicare certified. Should the agency do a transfer and resumption of care g y pOASIS? How should the agency respond to M0100 and M2410? 4b-Q183
623
Y if th ti t d itt d t i ti tYes, if the patient was admitted to an inpatient facility, the agency will need to contact the inpatient facility to verify the type of care that the pa e ac y o e y e ype o ca e a epatient is receiving at the inpatient facility and determine the appropriate response to M2410. If the patient is using a hospital bed response 1the patient is using a hospital bed, response 1 applies; if the patient is using a nursing home bed, response 3 applies. If the patient is using a swing-p pp p g gbed it is necessary to determine whether the patient was occupying a designated hospital bed (response 1 would apply) or a nursing home bed(response 1 would apply) or a nursing home bed (response 3 would apply). The hospital utilization department should be able to advise the agency
624
of the type of bed and services the patient utilized.

M2420DischargeDispositiong p625
M2420 Discharge DispositionM2420DischargeDisposition
Timepoints Discharge626
Timepoints Discharge
Patients who are in assisted living or Patients who are in assisted living or board and care housing are considered to be living in the community with formalbe living in the community with formal assistive services
Friends family neighbors who perform Friends, family, neighbors who perform services for free are considered informal assistive servicesassistive services
M2420DischargeDispositiong p
Formal assistive services include community based i
627
services:
Homemaking services under Medicaid waiver programsprograms
Home delivered mealsHome care or private duty care from another p y
agencyPaid services by an individual Other types of community based servicesOther types of community based services
Non institutional hospice is defined as the patient receiving p p ghospice care at home or a caregiver’s home, not in an inpatient hospice facility
Formal Assistive Service?FormalAssistiveService?
Formal assistive services are628
Formal assistive services are supportive community-based services provided through organizations or byprovided through organizations or by paid helpers and do not include medical or rehabilitative servicesmedical or rehabilitative services provided outside the home, e.g. outpatient therapy physician officeoutpatient therapy, physician office visits, dialysis, wound care clinic visits 4b Q184 1visits. 4b-Q184.1

M2430ReasonforHospitalizationp629
M2430ReasonforHospitalizationp
19--Examples of a scheduled treatment or630
19 Examples of a scheduled treatment or procedure include joint replacement surgery, non-emergency procedures to improve blood flow or heart function, such as angioplasty or pacemaker insertion, or cataract surgery. 4b-Q185.1
Does not include situation where patient’s health is deteriorating and the physician instructed to monitor the patient’s condition for 2 days andmonitor the patient s condition for 2 days and call 911 if the patient doesn’t improve. 4b-Q185.1
M2440ForwhatReason(s)wasthepatientAdmittedtoaNursingHome?p g
631
M2440ForwhatReason(s)wasthepatient Admitted to a Nursing Home?patientAdmittedtoaNursingHome?
Timepoints Transfer632
Timepoints TransferExcludes:Acute care facility Rehab facility admissionsyThese are both defined as admits to a
freestanding rehab hospital, a certified distinct rehab unit of a nursing home, or part of a general acute care hospital

M0903DateofLast(MostRecent) Home VisitRecent)HomeVisit
633
Timepoints Transfer/Death at Home/DC If the agency policy is to have an RN
complete the comprehensive assessment in a therapy-only case, the RN can perform the discharge assessment after the last visit b th th i t M0903 ill fl t thby the therapist. M0903 will reflect the nurse’s visit, even if non-billable. 4b-Q189.1
M0903. Do the dates in M0903 and M0090 always need to be the same? What situations might cause them tobe the same? What situations might cause them to differ?
When a patient is discharged from the agency with goals met, the date of the assessment (M0090) and the date of the last home visit (M0903) are likely to be the same. Under three situations however these dates are likely toUnder three situations, however, these dates are likely to be different. These situations are: (1) transfer to an inpatient facility; (2) patient death at home; and (3) the situation of an “unexpected discharge.” In these situations, the M0090 date is the date the agency learns of the event and completes the required assessmentof the event and completes the required assessment, which is not necessarily associated with a home visit. M0903 must be the date of an actual home visit. See M0100 Q&A f dditi l id “ t d
634
M0100 Q&As for additional guidance on “unexpected discharges.” 4b- Q188
PronouncementofDeath
When state law allows an RN to635
When state law allows an RN to pronounce death in the home, it is possible that the last visit to the home is pthe visit to pronounce death.
The visit to pronounce death is covered punder the home health benefit.
That visit date would be recorded in That visit date would be recorded in M0903.
This represents a change from the This represents a change from the answer 10/11. 4b-Q189.2
M0906Discharge/Transfer/DeathDischarge/Transfer/Death
636
M0906Discharge/Transfer/Deathg / /
Timepoints Transfer/Death at Home/DC637
Timepoints Transfer/Death at Home/DC
The date of discharge is determined byThe date of discharge is determined by agency policy or physician order. Th t f d t i th t l d t thThe transfer date is the actual date the patient was admitted to an inpatient f ilitfacility.
The death date is the actual date of the patient’s death at home
M0906 The Death DateM0906TheDeathDate
E l d d th i i i ti t
638
Exclude death occurring in an inpatient facility or in an emergency department, as both situations would result in Transferboth situations would result in Transfer OASIS collection and would report the date of transferof transfer.
Include death that occurs while a patient is being transported to an emergencybeing transported to an emergency department or inpatient facility (before being seen in the emergency department orseen in the emergency department or admitted to the inpatient facility).
M0903/M0906. When a speech therapist is the last service in a patient's home, our p ,agency has chosen to use an RN to complete the discharge assessment (with p g (OASIS) as a non-billable visit. If the patient meets the speech therapist's goals on day p p g y50 of the episode, but we cannot schedule an RN until day 51 of the episode, how do y p ,we respond to M0903 and M0906? 4b-Q190
639
If the agency policy is to have an RN complete the comprehensive assessment in a therapy only casecomprehensive assessment in a therapy-only case, the RN can perform the discharge assessment after the last visit by the SLP. This planned visit may be documented on the Plan of Care or not The RN visitdocumented on the Plan of Care or not. The RN visit to conduct the discharge assessment is a non-billable visit. M0903 (Date of Last/Most Recent Home Visit) would be the date of the last visit by the agency; inwould be the date of the last visit by the agency; in this case it would be the date of the RN visit. The date for M0906 (Discharge/Transfer/Death Date) would be determined by agency policy The date ofwould be determined by agency policy. The date of the actual agency discharge date would be entered here. When the agency establishes its policy regarding the date of discharge it should be notedregarding the date of discharge, it should be noted that a date for M0906 (Discharge/Transfer/Death Date) that precedes the date in M0903 (Date of Last/Most Recent Home Visit) would result in a fatal
640
Last/Most Recent Home Visit) would result in a fatal error, preventing the assessment from being transmitted.
M0906. My patient died at home 12/01 after the last visit of 11/30. I did not learn of her death until 12/04. How do I complete M0903 and M0906? What about M0090?
You will complete an agency discharge for the reason of death at home (RFA 8 for M0100). M0090 would be 12/04 -- the date you learned of her death and completed the assessment. M0903 (date of last home visit) would be 11/30, and M0906 (d h d ) ld b 12/01
641
M0906 (death date) would be 12/01. 4b-Q191
[email protected] [email protected] [email protected] comwww.selmanholmanblog.com
642