f ••.• 11 -. c)f cd - university of michiganioe481/ioe481_past_reports/w9604.pdfexecutive...
TRANSCRIPT
II
C‘4
’•r*
Q1
‘I-
’.
p.- cF
n(D
FF
•‘
F
FF
FF
r
11
IF
Cc
FF
FF
F
2.’
’;.
••.•
‘V
-:
—C
o(D
CD
c
_•:
Jc
C)
F
-.
(a••
F
FF
F
—
F
A•:
::
..,4
’.
..‘
I.
C)4)

TABLE OF CONTENTS
PageExecutive Summary1.0 Introduction and Background 12.0 Approach and Methodology 23.0 Current Situation 54.0 Inventory Replenishment Process 6
4.1 Ordering of Supplies 64.1.1 Special Ordering 64.1.2 General, Ordering 84.1.3 Ordering of Supplies Findings 8
4.2 Delivery of Supplies 104.2.1 Sepcial Orders 104.2.2 General Orders 114.2.3 Delivery of Supplies Findings 12
5.0 Service Scheduling Process 135.1 Service Scheduling Process Findings 15
6.0 Additional Findings 167.0 Recommendations 21
TABLE OF APPENDICES
APPENDIX A. Flow of Weekly Placement orders (Special Items)
APPENDIX B. Flow of General Material Ordering Process
APPENDIX C. Order Arrival Process (Special Items)
APPENDIX D. General Materials Receiving Flow
APPENDIX E. General Materials Replenishment Flow
APPENDIX F. Service Scheduling System Flow(Picking of first case only)
APPENDIX G. Service Scheduling System Flow (Day of Surgery)
APPENDIX H. NeuroSurgery Inventory Count Form
APPENDIX I. OR Equipment/Supply Requisition Form
APPENDIXJ. Sample Pick List
(
EXECUTIVE SUMMARY
The elimination of waste and inefficiencies of processes in the inventoryprocedure of the OR is important to improve the overall system. To evaluatethe inventory processes and general flow of items, it should first be noted thatthe key areas of inventory management are located in the OR and MaterielServices (MSE). The area is divided into three “cores”, named A, B, and Cand includes twenty-three operating rooms. Each department is allocated acertain amount of space within the cores to store its inventory. In addition,there is a main storeroom for MSE items in core A.
All stock items fall into one of two categories: general items from MSE andspecial orders from outside vendors. Some of the most expensive specialitems are also on consignment, which means that the item is not owned bythe OR until it is used. There are no special, designated areas for anyparticular item, as general items and special orders (and consignment items)are shelved together.
Implementation of the SSI Surgi-Server inventory software has resulted inthe program completely replacing the former preference card system in coreA. In cores B and C, the process of entering the preference cards into the SSIdatabase has already begun. Surgi-Server is used most frequently in theservice scheduling area. Surgeries are finalized approximately at 11:30 A.M.the day before, but an advanced schedule likely to change is generated a weekbefore.
Surgi-Server’s database is used to generate “pick lists” to indicate whichitems are needed for the next days surgeries. Pick lists are printed and sent tothe specific department at about 1:00 PM.
Key findings discovered during the inventory flow research include thefollowing:

• Dissimilarities between departments concerning the use of the Medical
Assistant
The job description for the Medical Assistant (M.A.) differed slightly
between departments. While all the departments allowed the C.N. ifi to train
the M.A., one department appeared to designate more responsibility to the
assistant. In this department, the M.A. is responsible for completely stocking
the items onto the shelves. Additionally, the M.A., upon receiving the SSI
generated pick list, picks supplies onto the bypods for the next day’s cases.
In another department, the stocking of items onto the shelves is a joint
effort between the M.A.’s and the R.N.’s. This department also had the M.A.
prepare the bypods, but it appeared that the R.N.’s took a more “hands-on”
approach with the items.
• Comparison of General Items vs. Special Items
General items and Special items are managed by different members of the
OR staff. General items are the responsibility of the stockkeepers, while
special items are the responsibility of the nurse coordinators or C.N. III. The
following table summarizes the differences among the two types of supplies.
Special Items General ItemsNumber of line 8,000 5,000
itemsPercentage on 80% 0%
ConsignmentNumber of Fed. -30/week 2/month
Ex. orders
Inventory on- 2 weeks 1-2 weeks
handTime to take 23 hours 20 min./ day
InventoryAverage orders 5 to 30 100
per weekNumber of —5 boxes 30
arrivals per dayAverage lead 3-7 days 5 days
time
C)
C
• Utilization of expensive equipment
One of the jobs of the circulating nurse is keeping track of items and price.
When an item of large expense comes into question, a discussion about its
use often arises. Nurses are often faced with a decision between using
supplies that a surgeon requests and the possibility of cutting costs for the
patient.
• Nurses spend. large amounts of time with inventory
There exists the theory that “nurses are on the forefront”. If nursing is
involved in the inventory process, they can talk directly to physicians.
Nursing knows and understands the intricate details involved in surgical
equipment. This is an argument used against adding departmental
stockkeepers to the staff.
• Relative independence between inventory replenishment and services
scheduling
Ideally, the ordering, pick list generation, and inventory replenishment
: processes should be tied together. Based on flow research, however,
inventory replenishment was found to be accomplished weekly through
comparison with par levels. With rio apparent approach to link the processes
together, goals of a perpetual inventory system are contradicted. A new
scheduling system is currently being implemented which has interface
capability with the SSI system being used. This interface will allow for more
of cooperation between the two processes.
• Apathy towards implementation of inventory software
The current attempt for implementation of the SSI Surgi-Server inventory
software program is the fifth in eight years. The program is not currently
used for inventory purposes, but is primarily used as a database capable of
generating pick lists. Ideally, the software should replace the time-consuming
equipment requisition process, and form the basis for a perpetual inventory
system. However, inadequate coordination in the past, and an aversion to
change have led to an apathetic view to the current implementation attempt.

1.0 Introduction and Background
Material requirements for the numerous surgical procedures are managed
by the Operating Room (OR) and Materiel Services (MSE). The operating
room deals with a total of 8000 products which are bought from outside
vendors, and 5000 general items which are bought from Materiel Services.
The high levels of inventory reflect the high values of supplies. The value of
OR supplies is estimated at around $2,000,000 in consignment orders only.
Both the special orders and the basic supplies (i.e., gloves, sutures, gauze, etc.)
which are common to every service are stored within each of the three cores
(A, B, and C) of the operating room. Each service has a designated location
and space within the cores to store its inventory.
Currently, nurses (R.N.’s), medical assistants (M.A.’s), and stockkeepers are
involved in the inventory ordering and replenishing processes. The number
of nurses responsible for the ordering varies depending on the size of the
service. Due to all the different people involved in the ordering and
managing of supplies, confusion occasionally arises. Because of the
numerous types of procedures and surgeon preferences, difficulties also have
been encountered in the effort to establish standards for surgical materials.
Situations such as backorders and Federal Express orders are ones which the
OR is would like to reduce, if not completely eliminate. The OR is aiming for
a perpetual inventory system. The SSI inventory software, Surgi-Server, is in
the process of being implemented to establish an on-line inventory system.
This implementation in addition to standardization, would result in a
reduction of money tied up in inventory due to a reduction of inventory
levels,, better coordination between the nurses and stockkeepers, and
improved organization of the overall system.
In order to ensure that all resources in the OR are effectively utilized and
that the number of items in inventory is accurate, a systematic materials
management system is required. The purpose of this project is to effectively
analyze and describe the system currently used at UH and identify possible
areas for improvement.
1
2.0 APPROACH AND METHODOLOGY
As the inventory handling process involves a large number of people, the
approach taken by the project team was to interview the relevant parties, as
well as to allocate substantial time to observe actual examples of the flow of
supplies within the cores and the operating rooms. The team treated the
interviewing process as an opportunity to understand the role and
responsibilities of the various people involved in the ordering, replenishing
and management of inventory. By observing the staff on a regular day in the
OR, the team was able to discover potential areas for improvements and
make suggestions for recommendations.
The first interview was conducted with the inventory coordinator. This
provided the team with a general description of the problematic issues and
main areas to concentrate on. The inventory coordinator exposed the team to
existingparadigms and prevalent attitudes among the staff. Many of the
nurses who have been responsible for the inventory system for many years
were very comfortable with the flow of the current system and expressed
resistance to any possible changes. The difficulty of learning a new
computerized inventory system was also noted as a concern by the nursing
staff. Also discussed were previous efforts made in addition to UH research
and studies conducted to improve the current system, such as the
establishment of a case cart system. With this information, the team was able
to understand the main areas of concern and the type of approaches already
considered. Subsequently, the team toured the three OR cores to get a more
accurate picture of how supplies are handled. This was the first opportunity
to see the equipment requisition forms, the shelving of stock, and the
preparing of bypods.
The stockkeeper was interviewed next. The responsibilities and work
sequence were described to the team. Correlation between the stockkeeper’s
ordering system and the nurses’ ordering system were identified. The
stockkeepers were determined to be responsible for ordering and replenishing
all the items bought from Materiel Services. In rare instances, special orders
were also placed by the stockkeeper.
2
Interviews were conducted with nurses (C.N. III) in charge of inventory to
gather information on the precise nature of the flow of materials. Three
C.N.’s III were interviewed, each from three different services (Neuro,
Cardiac, and ENT). The UH OR Head Nurse was interviewed so that a
standard inventory process could be determined. Issues discussed included
inter-departmental differences and current vs. proposed usage of the
computerized inventory software. The individual department nurses
provided a description of their department’s ordering and scheduling system.
The nurses were very cooperative in providing the most detailed
information on the inventory flow, from when supplies are ordered to when
they are stored and ultimately used and discarded. Issues regarding the
possibility of implementing a new “on-line” inventory system were
mentioned in the interviews in order to investigate on the nurses’
perspective about the effectiveness of the current system. The information
gathered from the department nurses was compared to the standard flow
provided by the Head Nurse in order to locate inconsistencies, if any.
Furthermore, the three specific departments were compared to determine the
consistencies and inconsistencies between the inventory control processes
because standardization of all departments was an issue of concern.
A tour of the operating room during a surgery further aided in analysis of
the inventory process. The team observed first-hand the responsibilities of
the nurse engaged in the preparation of a case. The circulating nurses were
observed bringing materials in and out of the operating room and keeping
track of all the extra supplies used in the case. Interviewing the circulating
nurse was also done at this time.
An OR ordering clerk was interviewed next to develop an understanding of
the ordering flow involved with material that is ordered from outside
suppliers. All of the items that are considered for ordering are listed within
the SSI Surgi-Server system. This includes detailed information about the
vendor and the expected cost of the items to be ordered. Some of these items
are purchased on blankets, which are estimated usage contracts with vendors
to help negotiate the price of the units. Further negotiating with the sales
representatives allow for discounts on early payments.
3

The team then interviewed a representative from the Med. Center
Information System department to understand previous attempts at SSI
implementation. The current state of the software and issues regarding
implementation were noted.
From the information received, an accurate overall flow was determined
and key issues were highlighted. Several of the staff members interviewed
also indicated what they felt were potential areas of improvements.
4

3.0 CURRENT SITUATION
Organization:
The inventory in the OR, including the ordering and storing process, is
managed by many people. For each department, multiple people such as the
C.N.’s III and medical assistants are involved in the OR materials
management program. Each staff member involved in the inventory process
has various responsibilities. This results in an intricate coordination and
organization among all the people involved . To analyze the current
situation, the flow of inventory should be separated into two independent
stages: the inventory replenishment process and the service scheduling
process.
5

4.0 INVENTORY REPLENISHMENT PROCESS:
The inventory replenishment process differs between special order items
and the general items. Special order items include all of those which are
ordered from an outside vendor and are specific to each service. General
items are those that are ordered in-house from Materiel Services and are
common to each service. These have different ordering, delivery, and storing
systems. Each department has a designated day of the week in which to take
inventory of all the supplies shelved in the core. The designated day is
consistent week after week. Through a system of checks and balances the
appropriate amounts of the specific items will be ordered.
4.1 Ordering of Supplies
General items and special items are managed by different staff members
and use different ordering systems.
4.1.1 Special Items
Specialty items are the responsibility of the nurse coordinators (C.N. III).
They are in charge of making sure that all supplies needed for each surgery
are on hand. Depending on the service, medical assistants also have
various responsibilities and aid the nurses on the day of inventory to
check which items are available and which are out of stock. The
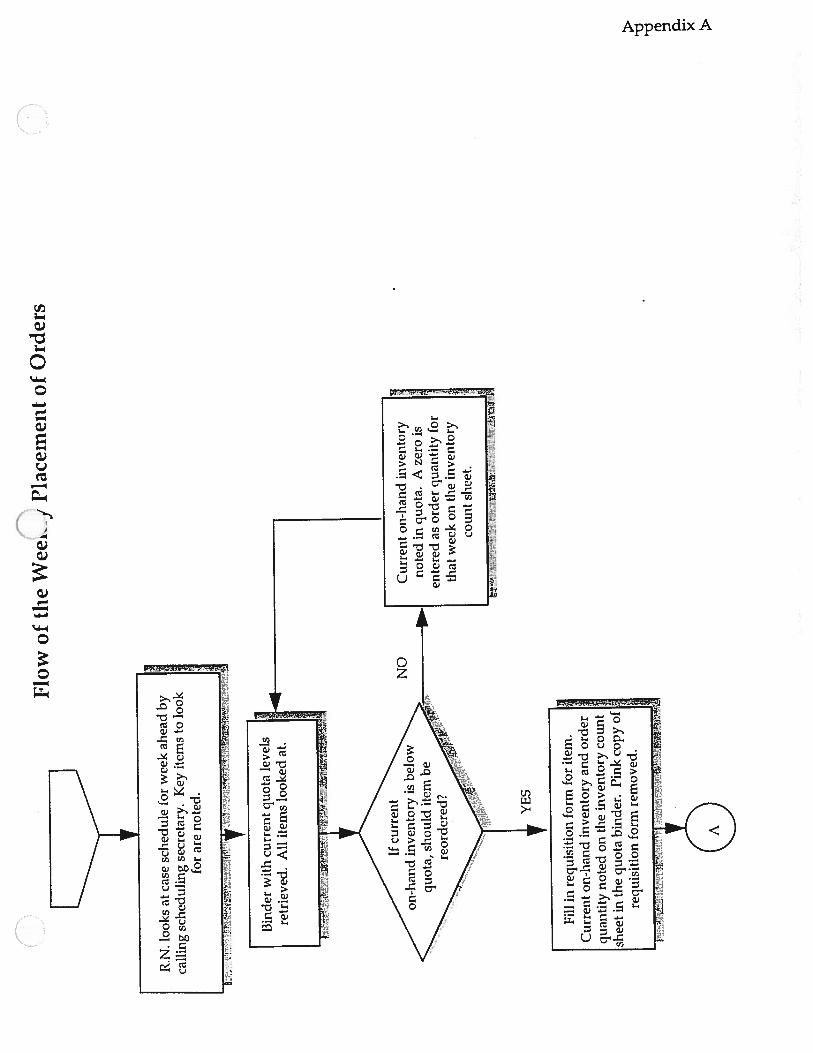
inventory flow is as follows (Appendix A):
• On the designated day of inventory the C.N. III will look at the case
schedule that has been proposed for the following week to determine
the key items to look for when taking a physical inventory.
• All the data regarding quota levels, changes in quota levels, and
placement of orders for each individual item are kept in a binder. This
binder is retrieved for taking the inventory. Depending on the service,
the nurse(s) or the medical assistant(s) check the inventory on a
qualitative basis to determine if the level on hand complies with the
quota of what should be kept on hand, usually a two week supply of
inventory is held. When an item reaches a level below the set quota a
6
requisition order form is filled out and the binder is updated to indicate
the amount that was ordered on that given date.
• The nurses record what they are ordering on an inventory count form
Appendix H). This form lists item name and current quota levels and
the date that inventory is taken. Typically, two months worth of
inventory ordering records can be tracked. In the date columns, two
numbers are written down. One represents current on-hand
inventory, and the other represents the amount ordered.
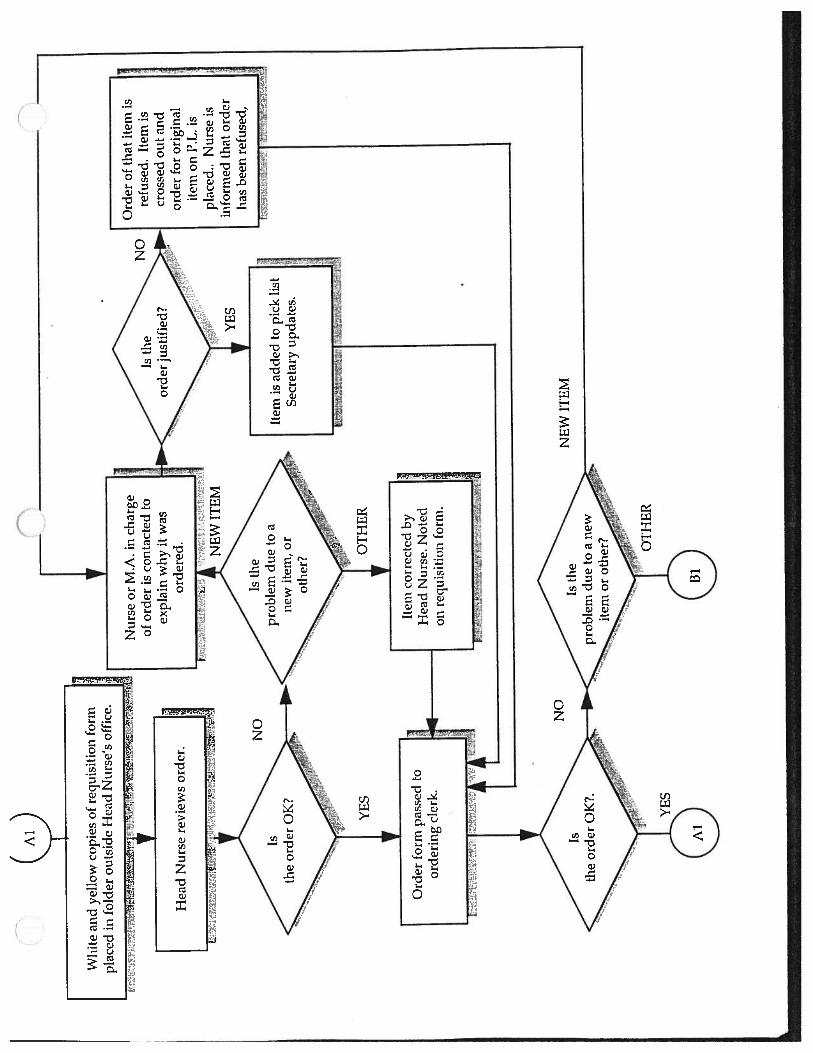
• The requisition form contains three copies (Appendix I) The top two of
these copies, one white and one yellow, are delivered to a folder
outside of the OR Head Nurse’s office for approval to verify that no
unusual or extremely expensive items are being ordered. The third, a
pink copy is kept in another binder by the C.N. Ill who placed the order.
In the case of a new or expensive item being ordered, the Head Nurse
inquires with the C.N. III or surgeon who proposed the item as to valid
reasons why such an item is necessary. If the item is new, justification
must be given for the item to be added to the pick list. Otherwise, the
Head Nurse will refuse the order of the new inventory and an order
will be placed for an equivalent existing item already on the pick list. If
there is another problem, such as quantity, the Head Nurse will make
notes on the copies of the requisition form and then pass the forms on
to the ordering clerk.
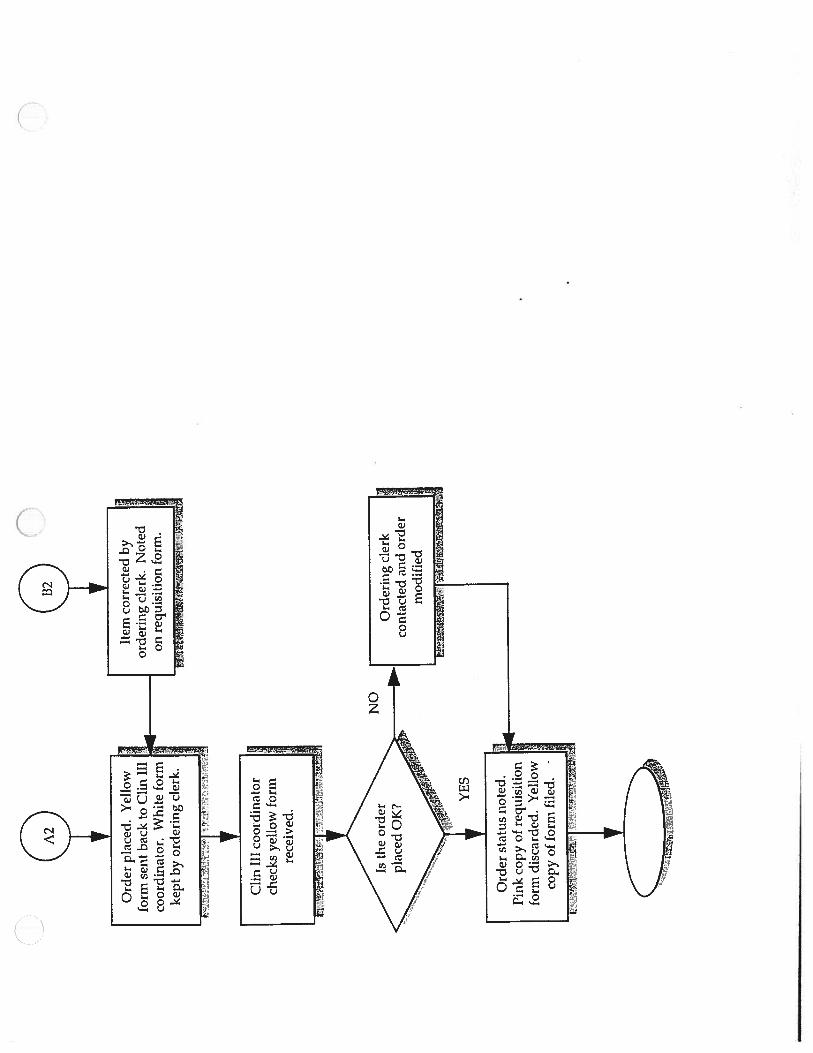
• Upon receiving the requisition forms the order is double checked. If
the item on the order form is not part of the existing pick list then the
C.N. III is contacted as mentioned above. Additional notes may be
added to the requisition form to indicate any changes that the ordering
clerk has made. If the order is correct it is placed and the yellow copy of
the form is sent back to the respective C.N. Ill. The white copy is filed
by the ordering clerk for later use.
• Upon receiving the yellow copy of the requisition form, the C.N. III
will check any noted changes in the order. If no changes were made or
if the changes are acceptable it is noted that the order has been placed.
7
However, if an incorrect change has been made on the ordering form,
the ordering clerk or Head Nurse will be approached to discuss these
changes and make the final appropriate order.
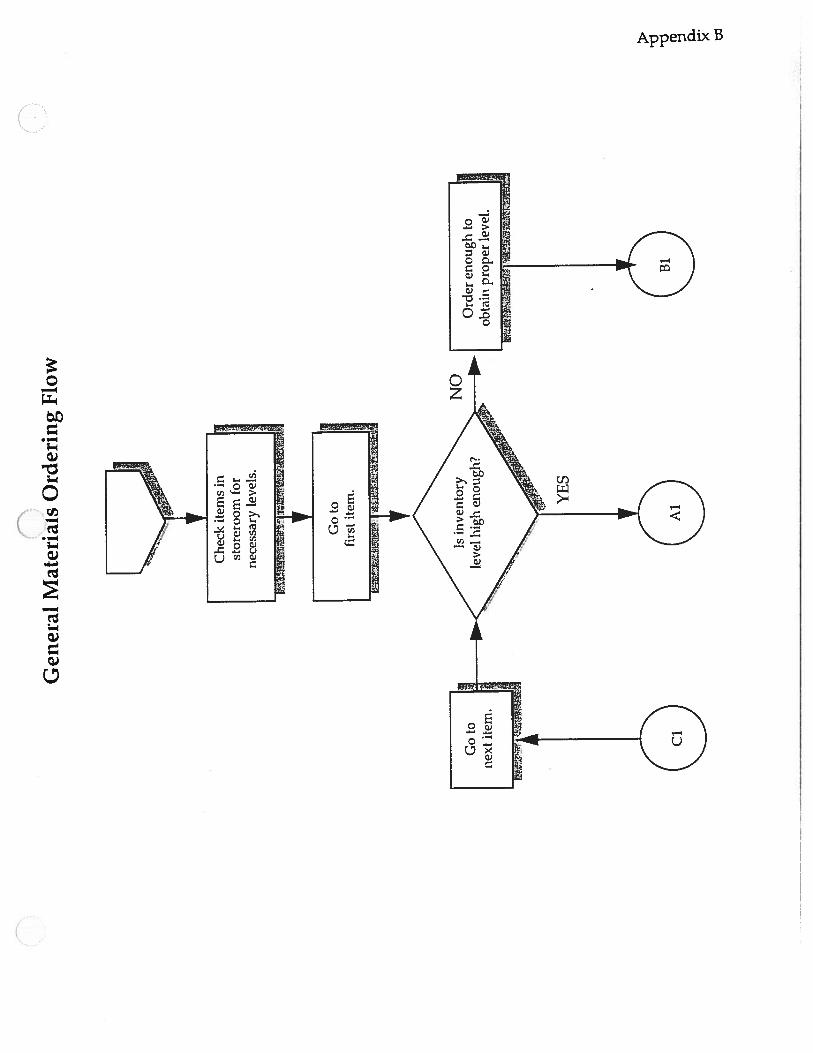
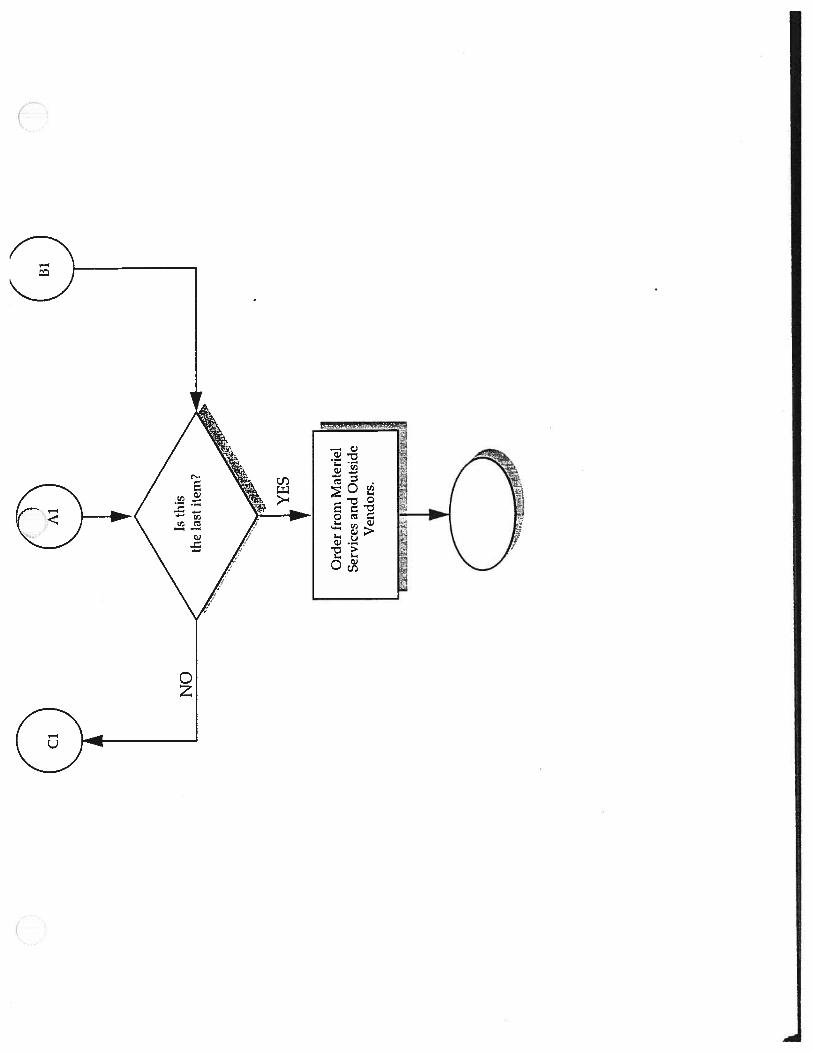
4.1.2 General Items
The stockkeepers are responsible for managing the general items. They
place orders daily from Materiel Services based on stock units which are
available for each item for each core. The flow is as follows (Appendix B):
• The stockkeeper checks the inventory levels within each of the
operating room cores. For each item, the stockkeeper approximately
checks the quantity and notes if the quantity is low and by how much.
The inventories within the cores are filled from both the main store
room and from Materiel Services.
• The stockkeeper next returns to the Operating Room storeroom. The
stockkeeper then checks the inventory levels within the storeroom to
ensure that they can satisfy the requirements obtained from the
previous search of the OR cores. If inventory levels are adequate, the
item(s) are loaded onto a cart for later distribution in the core. If
inventory levels are inadequate, the quantity available is stocked to the
cart and the remainder is noted to be ordered from Materiel Services or
an outside vendor.
• Once the carts have been filled the quantities in the main storeroom
are qualitatively checked. If the quantity of the designated item is
determined to be below that of the par level, it is noted to be ordered.
The stockkeeper will then call in the orders to Materiel Services and
the appropriate outside vendors. These orders are placed once per day
to Materiel Services and once per week to outside vendors.
4.1.3 Ordering of Supplies Findings:
• Several variances have been noted throughout each of the services
within the OR. In some of the departments the C.N. III takes the
inventory and decides what to order. In other departments the medical
8

assistant is trained and trusted to keep track of the inventory levels and
fills out the order requisition forms for the necessary orders. (• In some departments the C.N. Ill or the M.A. will look at the surgery
schedule in advance to get an idea and an estimate of what items will
be needed for the next two weeks. In some cases, the C.N. ifi will have
to contact the surgeon(s) secretary to request the schedule, and in other
services a schedule of cases for the following week is provided on the
day the take inventory.
• When the medical assistant takes the inventory on the designated day
of the week it is more likely to be an exact count as the M.A. is
instructed to count every item shelved in the core for that specific
service. In the circumstances where the C.N. III takes the inventory it
is more likely to be an educated guess by eyeballing what is on-hand on
the shelves.
• When a requisition form is filled it is delivered to the ordering clerk at
which point the order is checked (by the ordering clerk and/or Head
Nurse) before being placed. Occasionally, the ordering clerk will notice
an error on the requisition form (i.e. the quantity of the item being
ordered is too high), will make appropriate changes on the form, and
will then place the order. Occasionally, the yellow copy of the
requisition form is given back to the R.N. or M.A. after the order has
been placed or even after the shipment has arrived. This is mostly
because the lead time for an order is on average very short and papers
get lost in the shuffle. Unfortunately, this results in shipment errors or
creates confusion in keeping track of the ordering process.
• Errors in requisition forms may occur when the wrong code number is
written on the form. This also results in an incorrect shipment. Thirty
to fifty orders are placed per day. The ordering clerk and the Head
Nurse can not always catch such errors among all the orders that are
placed daily by each service.
9

• The stockkeeper replenishes the main store room with general items
that are delivered daily. From there, the cores are also replenished
from the items originally stored in the main store area. This creates
double handling of the materials.
4.2 Delivery of Supplies
The method in which supplies are brought into the OR also differs
between special items and general items. They have different arrival/drop-
off points and are followed by their own independent system of checks to
ensure that each delivery is correct. Deliveries of both of these types of
inventories are received on a daily basis.
4.2.1 Special Orders
Delivery of special items arrive on a daily basis in quantities of
approximately fifty cases per day. They are checked by the ordering clerk
and double checked by the C.N. III once they are delivered to the core to
help ensure that the order received is correct. However, no system is
currently being used to check that the correct prices are charged on these
deliveries. In addition, Federal Express and rush deliveries are received
on a daily basis. The flow for the delivery of Special items is as follows
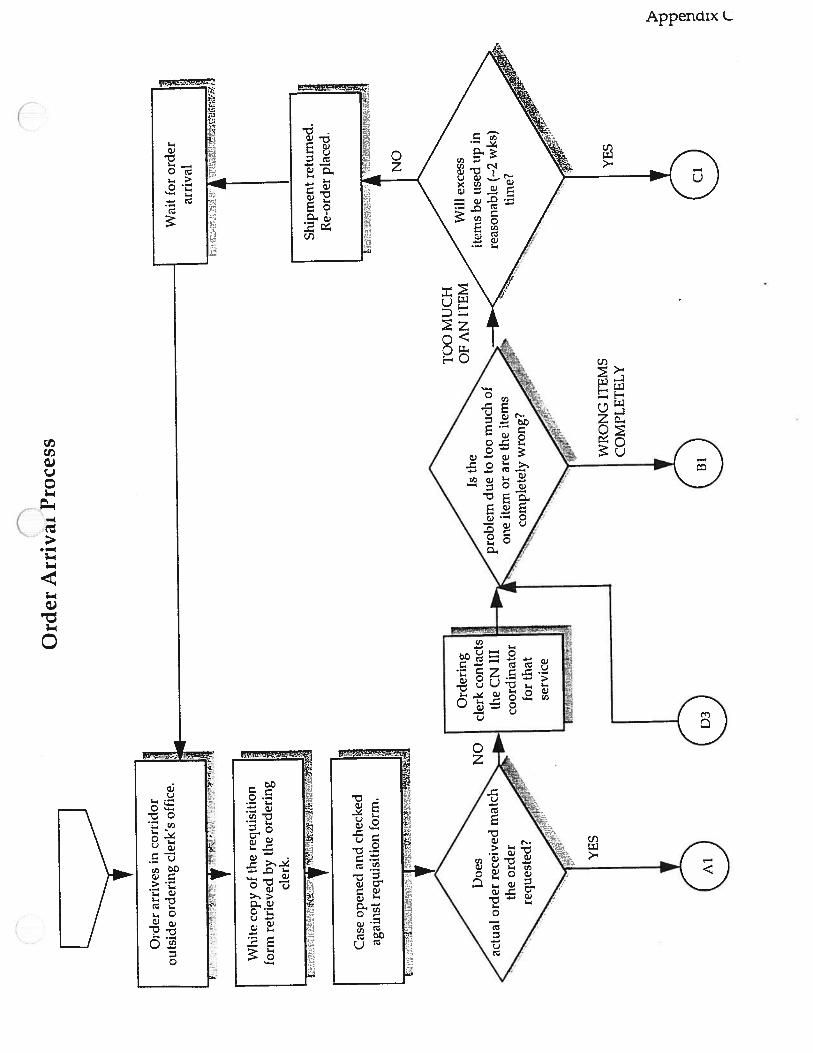
(Appendix C):
• Orders arrive on a daily basis into the OR. These orders are received by
the ordering clerk outside of their office. The white copy of the
requisition form (Appendix I) is then retrieved and the case is opened
and checked to insure proper delivery.
• If the order received matches the order placed, the white copy of the
requisition form is attached to the case and the stockkeeper will take
the order to the appropriate C.N. III in the designated core. Here, the
C.N. III or the M.A. will double check the order. If the shipment is
correct then the items are removed from the box and shelved.
Different services use different methods of storing their supplies in the
core. Some departments store the items in the cores alphabetically by
company name and some store them closely together according to the
10

cases for which they are used. If the order does not match, the C.N. III
is contacted. Upon being contacted, the C.N. III and the ordering clerk
will discuss what actions to take.
• If there is a problem with the quantifies of the items, (i.e.. excess is
received), it must be determined if the excess will be used up within
the allowable two week inventory limit. If not, the shipment is
returned and the original order is replaced. If the decision is yes, the
item will be kept and the C.N. III or stockkeeper will take the items to
the core and the binders will be updated.
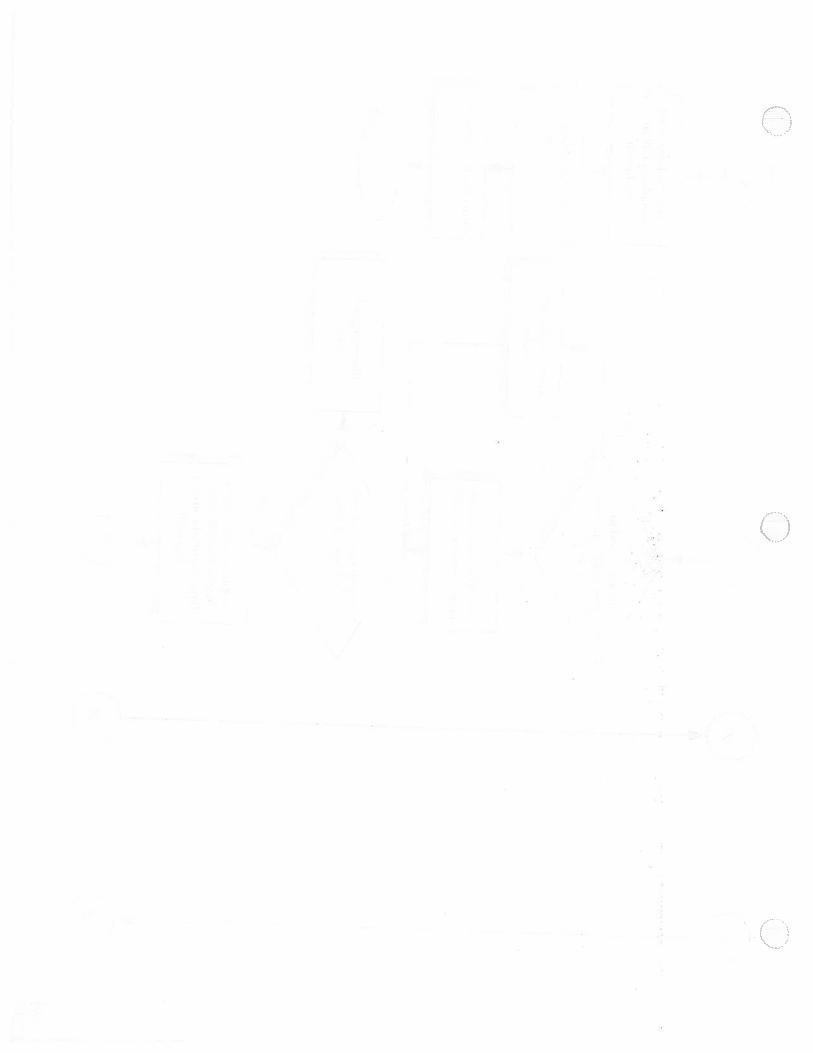
• If there is a problem such that an entire shipment of supplies is
incorrect, it must be determined if the item is one that can be used
within the OR. If the answer is no, the shipment is returned but if the
answer is yes the inventory will be kept and taken to the core. In either
case it must be determined if the original item that was ordered is
needed immediately or it the surgeon can use a similar item instead. If
the supply is not needed immediately, the original order will be placed.
However, if it is absolutely necessary then the search will begm The ()search will start within the cores of the OR. If the item is not found in
the core the stockkeeper will be contacted to search within the main
storage room. If it is still not found, resources will be checked with
Kellogg and/or Mott hospitals. If the item is still not found, the
vendor can be contacted to reveal the nearest location of a hospital that
has received the item. If the neighboring hospital has the item on
hand they will ship it over. In the worst case scenario, the overnight
courier service will be used.
4.2.2 General Orders
General items are delivered every morning at approximately 5:00 AM.
These orders are received by the stockkeeper outside of the main store
room in Core A. Quantities range from ten to fifty cases per day from
Materiel Services. Orders are received the day after an order is placed from
Materiel Services and according to delivery times from outside vendors.
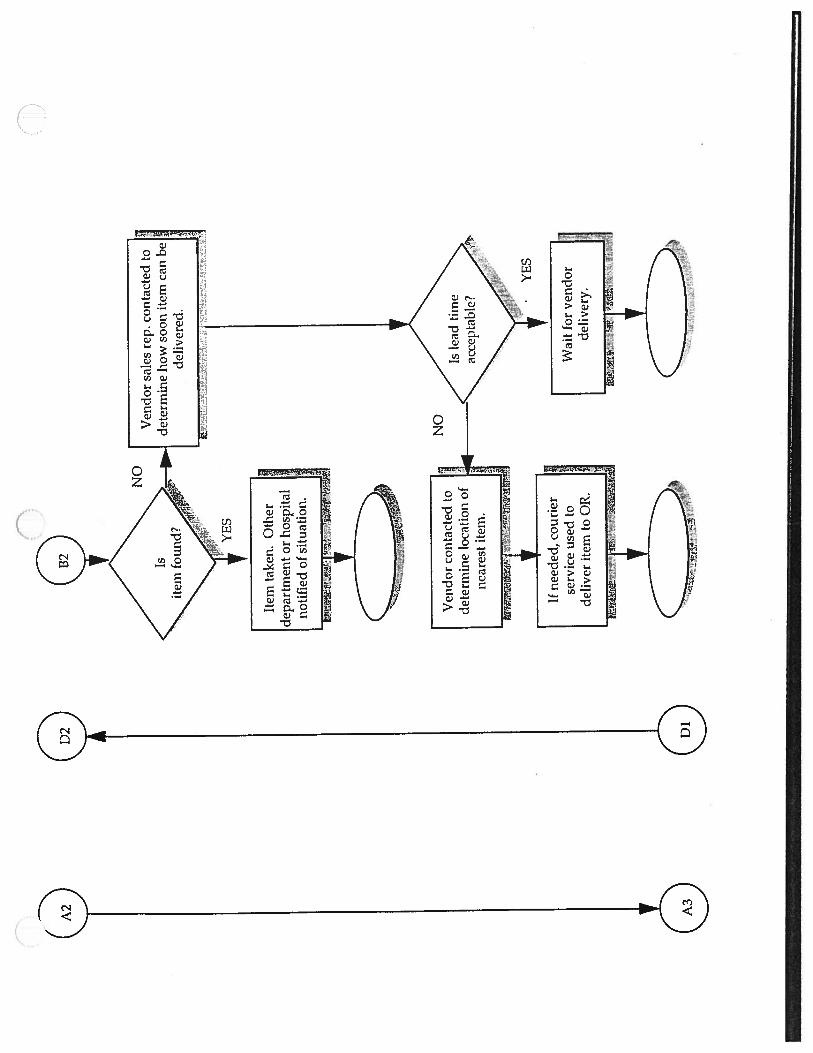
The flow is as follows (Appendix D):
11

• The stockkeeper will retrieve their note pad and the cases are checked
to insure proper delivery.
• If the order matches, the inventory is taken into and distributed
throughout the main store room. The remaining inventory that was
ordered is then brought to the designated location within the cores.
• When the inventory within the cores is checked the carts are filled
from the main store room as mentioned in the ordering process.
These carts are then taken from core to core to replenish the cores
inventories from the main store room. This process is usually
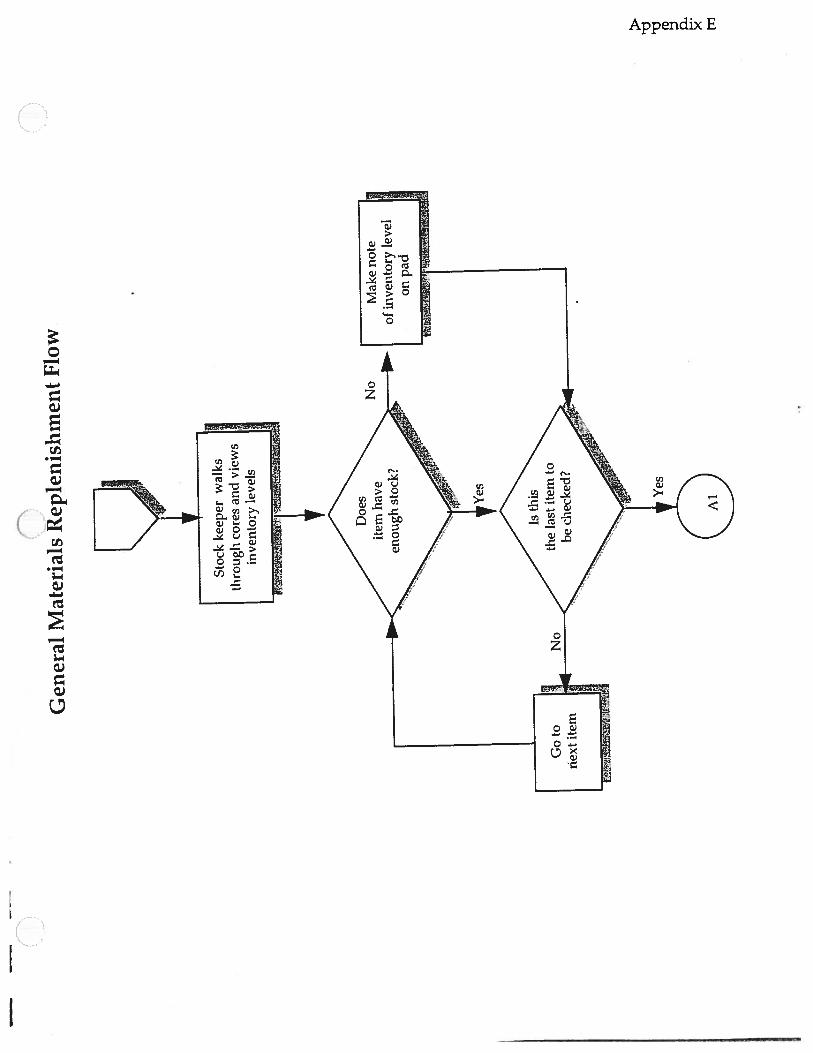
performed three times a day by the stockkeeper (Appendix E).
4.2.3 Delivery of Supplies Findings
• When an order is received and it is correct, it is not checked if the
correct price has been charged by the supplier for the items received.
The price listings are available on computer but are not displayed on
the requisition form. The original requisition form is the only thing
that the ordering clerk checks as the orders are delivered.
• Depending of the vendor, a wrong shipment will be taken back by the
company up to 30 days from the delivery date if the items are not
opened. However, if the supplier insists that the error was made by the
OR then the hospital has to pay for the excess re-shipment costs. A
wrong order is kept if it is less expensive to keep the items on stock
than to ship them back to the vendor, assuming that the inventory will
be used in the immediate future. This results in extra money being
tied up in inventory and in extra cost for Federal Express orders to
account for the item which was needed in the first place.
12

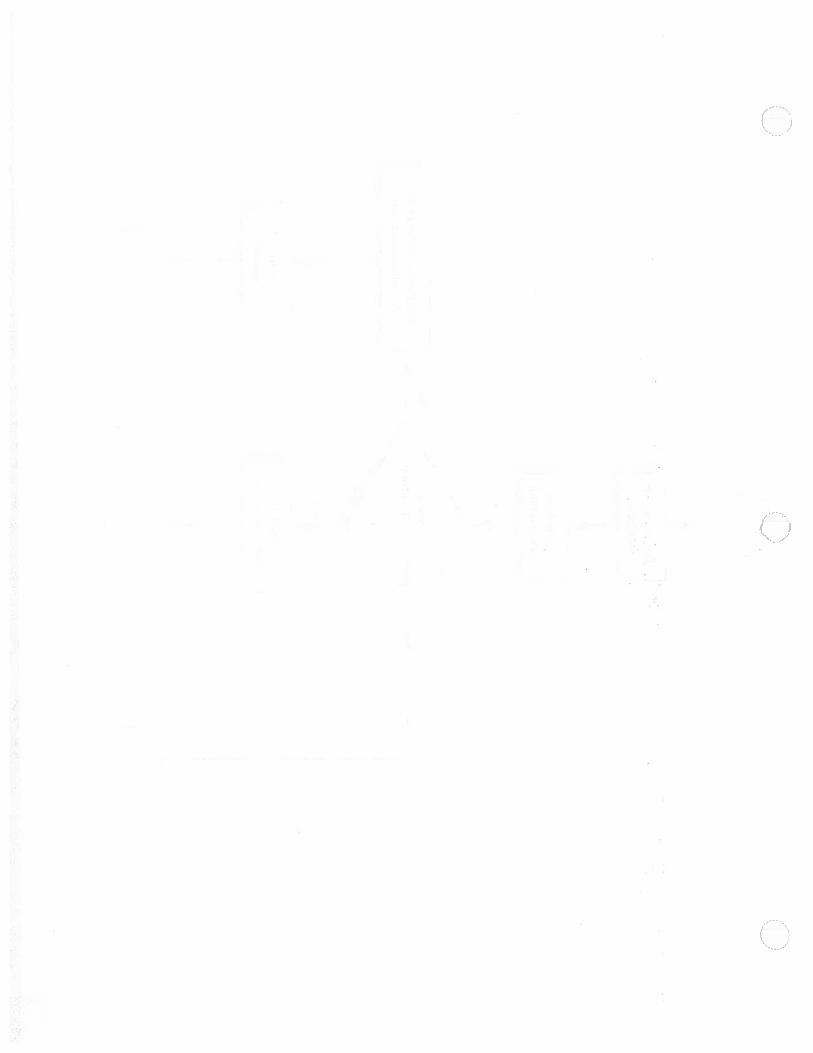
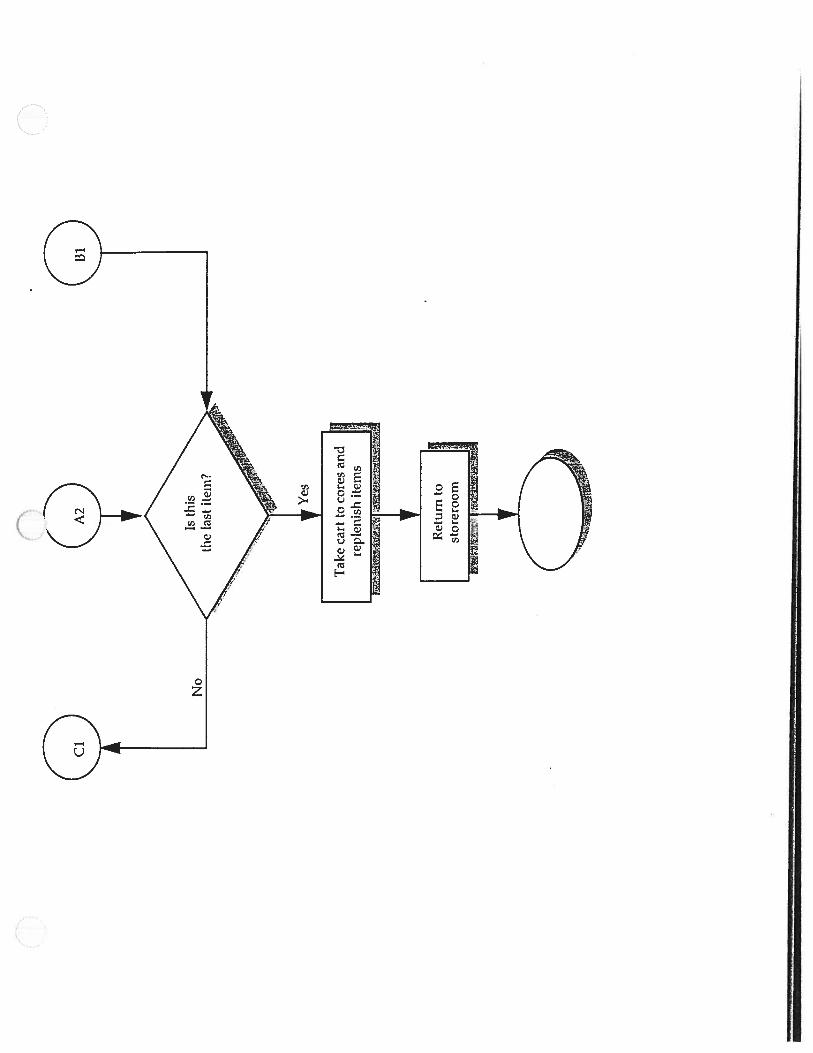
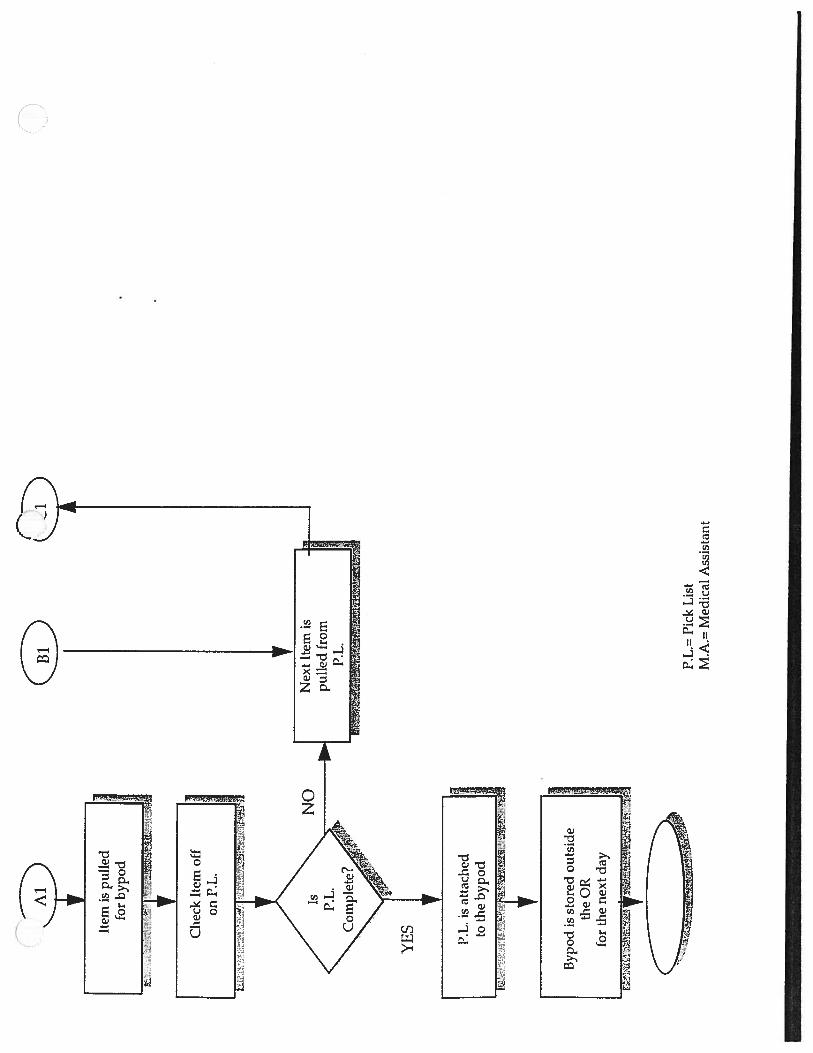
5.0 SERVICE SCHEDULING PROCESS:
The service scheduling process does not have any influence on the
materials ordering process. Ordering is based on quotas as mentioned above,
and it is not case generated. The service cheduling process is very involved
since there are many staff members engaged in the process. The Service
Scheduling Process is subdivided into two categories: The first cases of the
day which are picked the night before (Appendix F) and the following cases
picked the same day of the surgery (Appendix G).
Computerized pick lists are generated by Surgi-Server every day at
approximately 11:30 AM. The final schedule of surgeries for the day is
set only 24 hours in advance, but the schedules can be changed up to
the day of surgery due to such factors as cancellations. Once the
schedule is finalized, the pick lists that match the cases on the schedule
are printed and distributed to the nurses or medical assistants for each
department.
Pick lists are made available for the nurses at approximately 1 p.m. of ( )the day prior to the surgery. It takes on average 10 to 30 minutes to pick
a case. Depending on the department, either the M.A.’s or the Clin II
use the pick lists to gather all the items for the specific case. The
“hunt” for items begins, as items on the pick lists are not listed in any
particular order. Only the first case for the following day is picked for
each room because there are not.enough bypods and not enough space
in the cores to store them. All succeeding cases are picked during the
course of the same day in between surgeries. As an item is picked it is
checked off on the pick list and placed into an appropriate cart or bypod.
Bypods are sometimes difficult to locate since there is no specific
storage area for bypods only.
• If an item on the pick list is not available in the cores it is marked off
on the pick list as “missing”. If the case being picked is the first one of
the following day, then the missing items are hunted the next
morning, approximately 30 minutes before the case is set up.
Otherwise, the M.A. or the C.N. III will look for it right away. Usually,
13
the items not available are general items. This might occur either
because the item has not been restocked yet in the cores or because the
item is out of stock.
• Once all the available items are stored in the bypod, the bypod is placed
outside the designated operating room with the pick list attached to it.
If an item on the pick list is missing in the cores and it is out of stock,
then Federal Express orders are placed. Depending on the service,
orders are usually placed 2 to 3 times per week
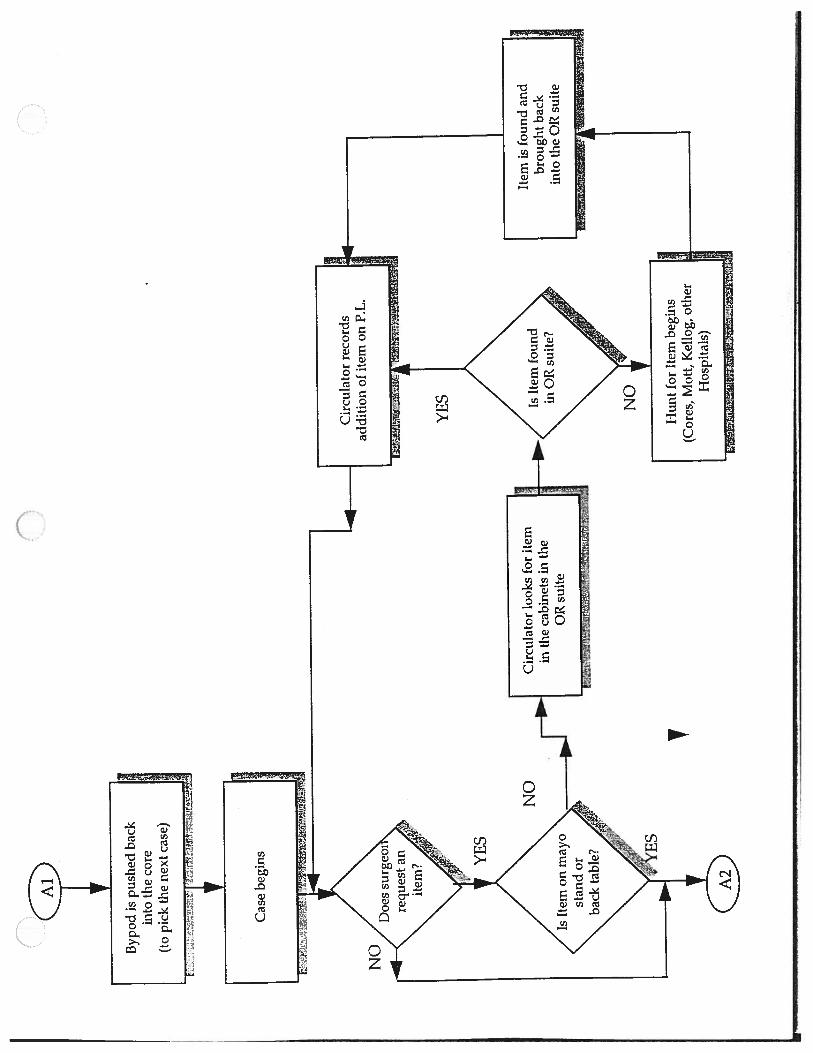
• The day of the surgery, the bypod already prepared is brought into the
operating room. As the scrub nurse and the circulating nurse(s) open
the supplies they double-check the pick list. In most of the cases, pick
lists are not complete. This is often because of surgeon preference. This
contributes to the number of products lines in the OR inventory
because different types of the same item can be used to perform the
same surgery.
• During the course of the surgery, the surgeon or the scrub nurse
request items that weren’t originally on the pick list. At this point, the
circulating nurses are in charge of gathering these items in the least
amount of time possible.
• The circulating nurse first looks for the item in the cabinets inside the
operating room. This is where the small quantities of supplies most
frequently used are also stored. If the item is not available, then the
circulating nurse will start hunting for the item in each of the three
cores, starting with the closest core first. If the item cannot be found
and the surgeon can not agree to use a substitute supply then the search
is extended, depending on the emergency, to Mott and Kellogg. Other
Hospitals will be contacted as well if necessary.
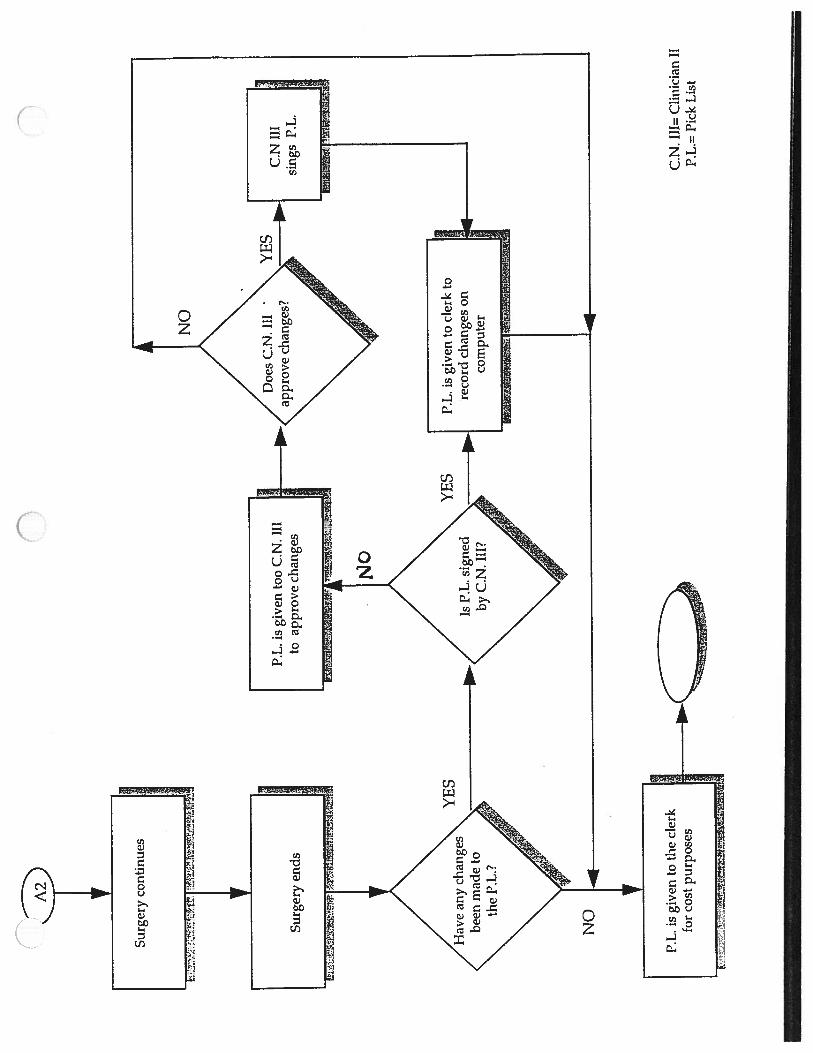
• When the item is found and brought into the operating room, the
circulating nurse records the change on the pick list and the additional
cost of the item on a separate sheet of paper. At the end of the surgery
14
the C.N. III must sign the pick list to approve the changes made during
surgery. (
The clerk will not add the new items onto the pick list without a
signature, but will return the pick list to the nurse coordinator for
approval. Occasionally, the nurse coordinator will not approve for the
changes to be permanently made on the pick list, but specifies the item
as “have available” only. This is because the extra item used was only
specific to that particular procedure and to that particular patient, hence
it is not necessarily required for the case. When the final signed pick
list is delivered to the scheduling department change will then be
recorded accordingly in the computer.
5.1 Service Scheduling Process Findings:
The surgery schedule is finalized only the day prior to the date of the
surgeries. Although this is necessary because of issues such as
cancellations, it doesn’t provide enough time to ascertain that all the
supplies needed for each case are available in the OR. Usually, each
department will keep a backup of a special order item in case of an
emergency. Occasionally the item needed for the surgery is out of
stock. This is the worst case scenario in the inventory process because
the hospital results in paying higher cost because of excessive Federal
Express orders or other means of immediate delivery for missing
items. Charges for such delivery services are estimated to range
between $20,000 to $30,000 per year.
• When the cases for the following day are picked, missing items are not
looked for right away. Nurses will search for them the following day
just before the surgery. This also contributes to the additional
immediate delivery charges that the hospital faces every year.
015

6.0 ADDITIONAL FINDINGS
• Summary of department differences
Data was gathered by interviewing nursing staff members from the
three different departments, Comparisons can be made among the
departments and the results are shown in Table 1.
Table 1. Comparison of Departmental Services
Each service deals with a different number of total line items and a
different percentage of on consignment items. Because of differences
in the way each service records their on-hand inventory and their
ordering, the time engaged in the inventory process slightly differs as
well.
V
Cardiac ENT Neuro
Number of line 200 409 240
items
Percentage on 0% (heart valves 47% 70% of. only) aneurysm clios
Consignment and 70% olimplants
Day to take Friday Wednesday Tuesday
inventory
Inventory on- 1 week 1-2 weeks 1 week
handdependingonitem
Time to take 3 hours 2 hours 3 hours
Inventory
Average orders 2-10 companies 15-20 —305-30 cases
per week
Average Fed EX 2 per week 2 per month 2-3 per week
orders
Number of 3-4 boxes 5-15 boxes 2-10 boxes
arrivals per day
Average lead 3-7 days 5 days —5 days
time
Advanced 1 week in advance 1 week in advance calls to find next
schedule?weeks schedule
16
• Consignment Items
Consignment items are items which are not charged to the department
until usage. There is no specific space allocated to store consignment
items. These are shelved together with the general supplies in the
designated space for each service. Consignment items are usually high-
ticket items negotiated by the Head Nurse. Currently, an estimated
$2,000,000 worth of supplies in storage are consignment items, and
some departments have a majority of their inventory as consignment.
There is no visual indication in the cores of an item being on
consignment, because it assumed that the nurses have proper
knowledge of all the supplies available. Should a consignment item be
used, special consignment forms are filled out by the nurse. A copy of
this form is sent to the vendor for billing purposes.
• Issues regarding Inventory Management during Surgery
The tour of the operating room during surgery provided a number of
findings. The surgery withessed was a removal of a cancerous thyroid
gland. First, the set-up time for the surgery witnessed took
approximately 70 minutes. This was an extremely long time in
contrast with the expected set-up times of about twenty minutes. The
nurses preparing the room were careful to point out that particular
surgery involved several departments. Indeed, the positioning of the
patient was a key issue between the ENT, Anesthesia and General
Surgery departments. In the time it took to prepare the room, a
number of additional supplies not on the bypod were brought not all at
once, but piece-by-piece over time. The supplies were requested by
surgeons from the different departments.
During the surgery, the circulating nurse took care to track all items
used. Upon interviewing this nurse, it was determined that it was the
nurse’s responsibility to look for potential areas to cut costs.
Specifically, this included considering the use of an alternate item if it
was more cost-effective and feasible.
C.17

• Responsibilities of Nursing Staff
In addition to finding potential for decreasing cost, nurses also act as
arbitrators in cases where not enough inventory is available for all
those who request it. In such a case, it is the nurses responsibility to
prioritize the use of the items based on knowledge of surgical
procedures.
Some concern was raised by members of the nursing staff that up to a
half day per week was spent in the reorder process. This is time which
should be spent in the OR assisting in the progress of surgeries.
A interesting finding about the nurses in charge of inventory was that
they knew little about the processes of other departments in the OR.
They assumed that the basic procedure of order and receiving were the
same, but expected that subtle difference existed throughout the flow.
• Responsibilities of Head Nurse
The Head Nurse is currently an integral and non-interchangeable piece
of the inventory process The Head Nurse is the major central figure
between departments because all decisions regarding adjustment of par
levels and ordering must get approval of this person Additionally, the
Head nurse is a key player in the negotiation for supplies. Price is
always the key issue, and higher costs must be justified.
• Duplicate System with Preference Cards
Although preference cards are in the process of being eliminated, they
are still referred to in some departments. Supposedly, only the pick
lists should be used to pick the cases but some M.A. or floaters still use
the preference cards as a backup since the pick lists are often not
completely accurate.
• Issues Regarding Standardization
The issue of standardizing processes is being examined. It appears as a
fundamental concept for the success of computerizing the inventory
process. The problem with the computer is that it does not perform
judgment-based decisions. Upon evaluation of the patient’s health and
18
condition, additional items may be requested, so a nurse may get a
particular supply even though it contradicts the pick list order.
Another issue which confronts standardization is the reluctance of the
surgeons. Each surgeon may have a different list of supplies for the
same surgery. These differences are based on preference or the
surgeon’s educational background. Thus, standardization will not be
easily implemented.
• Status of the Inventory Software Implementation:
The current attempt to implement the DOS-based Surgi-Server
software (SSI) is the fifth in eight years. A current goal is to remove the
DOS base of SSI. The software is primarily being used only to generate
pick lists, as that aspect only involves a simple database, but it is not
being utilized for inventory purposes. SSI is designed for a case cart
system which is not the system being used by UH. In addition there is
inadequate training for the use of SSI. Another system upgrade is due
in May, and implementation of a Pathways Healthier Scheduling.
U• Issues Regarding Implementation of Inventory Software
Implementation of the SSI Surgi-Server computer inventory software
has been a goal of UI-I for the past eight years. The ultimate goal of
computerizing the inventory process is to have a perpetual inventory
system. In such a system, the ordering process would be synchronized
with the service scheduling process as the software would decrement
inventory individually and trigger the ordering process when it
reaches a determined reorder point. This would ideally replace the
current requisition process and cut down the amount of paperwork.
Other goals for SSI include on-line receiving and shipping, which
would speed up the process even more.
To deal with the current dilemma of independent ordering and
scheduling processes, a new scheduling system called Pathways
Healthcare Scheduling is being considered. The advantage of this new
system is its direct interfacing with SSI.
19

A more intangible dilemma arising from SSI is its history of
implementation at UH. Many attempts have been made in the past for
implementation and an attitude exists in the OR that computerizing
the process does not effect the ultimate goal: the welfare of the patient.
Inadequate coordination in the past has also soured enthusiasm for thesystem. SSI is comprised of five main aspects, and previousimplementation attempts over zealously wanted to start up all five.
The current attempt has been more gradual, and the new scheduling
system forces the staff in the OR to look at the overall picture.
Concern was also raised that the success of SSI depended upon a
complete pick list. In the current early stage of implementation, many
pick list items in the computer database are not accurate. This is due to
the massive number of items which only the nurses have detailed
knowledge of.
• Potential for Bar-Coding to the Inventory Process
Currently being tested at the Kellogg Eye Center is a bar-code scanner to
increment and decrement items. A mandate is being considered to
standardize the bar coding for all medical products which is slowing
I down the process. The SSI program does not function with bar codes,
but use of the bar code for the tracking of inventory held in the system
is certainly under consideration.
20

7.0 RECOMMENDATIONS
• Standardize inventory count process
An exact physical count should be taken for each department on a
weekly basis. The problem with the current process of estimating the
inventory level is that it provides only an approximation of on-hand
inventory. By keeping an exact count, the system will be more accurate
and inventory levels will be kept closer to the par levels.
• Further training of Medical Assistant
The medical assistants should be comfortable with handling all aspects
of inventory control. The M.A. should have a broad and extensive
knowledge of all items. With this knowledge, they should be given the
responsibility of taking inventory and filling out requisitions for items
in order to allow nurses more time in the OR. Proper and quicker
training is possible by reorganizing the storage areas, and having
sufficient identification of items. One area of improvement could be to
label all consignment items, and to store items onto a shelf based on (surgical procedure.
• Encourage all C.N. III’s/M.A.’s to look at advanced surgery schedule
All departments should have the advanced schedule (for either one or
two weeks) available on the day they take inventory which is also the
day on which they place most of the orders. It should not be the
responsibility of the C.N. III to provide this advanced schedule for the
respective department. By doing this, the C.N. ifi or the MS. can have
a general idea of what it is expected to be used for the tentative
schedu1ed cases. The number of Federal Express or rush orders can be
reduced by having the item(s) on-hand in advance.
• Increase inter-departmental communication
If an order is sent to the wrong department, it should immediately be
sent to the correct department. This could be done by contacting the
stockkeeper to note that an incorrect order was received. The
stockkeeper should then deliver the inventory to the appropriate
21
department. This will reduce the amount of time spent searching for
an order.
• Encourage return of yellow requisition form immediately after order
The yellow copy of the requisition form indicates to the C.N. III or M.A.
in charge of inventory that the order has been placed. This yellow
form should be returned to the department before the order arrives, so
that the C.N. Ill or M.A. has the opportunity to confirm exactly what
items are in the order.
• Support mandate for standardized bar-coding of medical products
Standardization in any form aids in the implementation of software to
support computer-generated decisions. B ar-coding technology allows
for a highly efficient manner of tracking inventory quantities.
Through bar-coding, the process of filling inventory count forms can be
eliminated. This will reduce the time spent keeping track of the on
hand count to a minimum. Also, bar-coding helps reduce the effect of
human errors, where an item is ordered, but an incorrect product
number is entered.
22
C
Flo
wof
the
Weey
Pla
cem
ent
ofO
rder
srN
Bin
der
wit
hcu
rren
tqu
ota
leve
lsre
trie
ved.
All
item
slo
oked
at.
Ifcu
rren
ton
-han
din
vent
ory
isbe
low
quot
a,sh
ould
item
bere
orde
red?
NO
R.N
.lo
oks
atca
sesc
hedu
lefo
rw
eek
ahea
dby
call
ing
sche
duli
ngse
cret
ary.
Key
item
sto
look
for
are
note
d.
F
YES
Cur
rent
on—
hand
inve
ntor
yno
ted
inqu
ota.
Aze
rois
ente
red
asor
der
quan
tity
for
that
wee
kon
the
inve
ntor
yco
unt
shee
t.
I I
Fill
inre
quis
itio
nfo
rmfo
rit
em.
Cur
rent
on-h
and
inve
ntor
yan
dord
erqu
anti
tyno
ted
on[h
ein
vent
ory
coun
t
shee
tin
the
quot
abi
nder
.P
ink
copy
of
requ
isit
ion
form
rem
oved
.
Cn
Nur
seor
M.A
.in
char
geof
ord
eris
cont
acte
dto
expl
ain
why
itw
asor
dere
d.
-A
NE
WIT
EM
Ord
erof
that
item
isre
fuse
d.H
emis
cros
sed
out
and
orde
rfo
ror
igin
alit
emon
P.L.
ispl
aced
..N
urse
isin
form
edth
ator
der
has
been
refu
sed,
Item
corr
ecte
dby
Hea
dN
urse
.N
oted
onre
quis
itio
nfo
rm.
Item
isad
ded
topi
cklis
tS
ecre
tary
upda
tes.
()W
hite
and
yell
owco
pies
ofre
quis
itio
nfo
rmpl
aced
info
lder
outs
ide
Hea
dN
urse
’sof
fice
.
i•:
.:
S‘
‘7•
•-
•:•
-:-
C)
Item
corr
ecte
dby
orde
ring
cler
k.N
oted
onre
quis
itio
nfo
rm.
Th
Ord
erpl
aced
.Y
ello
wfo
rmse
ntba
ckto
Cli
nII
Ico
ordi
nato
r.W
hite
form
kept
byor
deri
ngcl
erk.
HC
lin
III
coor
dina
tor
chec
ksye
llow
form
rece
ived
.
Ord
erst
atus
note
d.P
ink
copy
ofre
quis
itio
nfo
rmdi
scar
ded.
Yel
low
copy
offo
rmfi
led.
--
F
Gen
eral
Mat
eria
lsO
rder
ing
Flo
w
Ct
4
Ord
eren
ough
toob
tain
prop
erle
vel.

fl
7-N
r
NO
Ord
erfr
omM
ater
iel
Serv
ices
and
Out
side
Ven
dors
.
(
0
Ord
erA
rriv
aiP
roce
ss
Ord
erar
rive
sin
coru
idor
outs
ide
orde
ring
cler
k’s
offi
ce.
Whi
teco
pyof
the
requ
isit
ion
form
retr
ieve
dby
the
ord
erin
gcl
erk.
Cas
eop
ened
and
chec
ked
agai
nst
requ
isit
ion
form
.
Shi
pmen
tre
turn
ed.
Re-
orde
rpl
aced
.
Ord
erin
g(s
the
CN
III
coor
dina
tor
for
that
serv
ice
Isth
epr
oble
mdu
eto
too
muc
hof
one
item
orar
eth
eit
ems
com
plet
ely
wro
ng?
TO
OM
UC
HO
FA
N1T
EMW
illex
cess
item
sbe
used
upin
reas
onab
le(—
2w
ks)
tim
e?
YES
WR
ON
GiT
EM
SC
OM
PLE
TE
LY


toke
epit
ems
ism
ade
byC
NIl
l
NO
CN
111
orst
ockk
eepe
rta
kes
item
sto
the
core
.
Isor
igin
alit
emor
dere
dne
eded
imm
edia
tely
?
Beg
inse
arch
for
item
.S
earc
hth
roug
hot
her
depa
rtm
ent’
sin
vent
ory
orM
oLt
OR
.
0
fTh
Ven
dor
sale
sre
p.co
ntac
ted
tode
term
ine
how
soon
item
can
deli
vere
d.
Item
take
n.O
ther
idep
artr
nent
orho
spit
alno
tifi
edof
situ
atio
n.
Ven
dor
cont
acte
dto
dete
rmin
elo
cati
onof
near
est
item
.
Ifne
eded
,co
urie
rse
rvic
eus
edto
deli
ver
item
toO
R.

11
:1
fl0
Whi
terc
qusi
tion
form
atta
ched
toor
der.
Sto
ckke
epcr
take
sor
der,
dete
rmin
esde
stin
edco
refr
omre
qusi
tion
form
and
deli
vers
toco
re.
Inco
re,
Cli
iiII
Ior
M.A
.lo
oks
atw
hite
rcc
1usit
ion
form
and
chec
ksor
der.
Ord
erin
gcl
erk
OS
conta
cte
dand
prob
lem
actu
alor
der
mat
chdi
scus
sed.
ieques
ted
ord
er
2
____
____
____
____
____
___
YE
S
A4

I
C)
Item
sre
mov
edfr
ombo
xan
dpl
aced
onsh
elve
sfo
rst
orag
e.
Pin
kan
dye
llow
copi
esof
requ
isit
ion
form
sdi
scar
ded.

n

Gen
eral
Mat
eria
lsR
ecei
ving
Flo
w
NO
NO
YES
YES
0

N
Ret
urn
item
toM
SEor
vend
or
NO

gt
I
CC
n)G
ener
alM
ater
ials
Rep
lenis
hm
ent
Flo
w
Stoc
kke
eper
wal
ksth
roug
hco
res
and
view
sin
vent
ory
leve
ls
C
(N
(J

Stoc
kav
aila
ble
quan
tity
todi
stri
buti
onca
rt
No
•t:
t•
••
•.•
£%!.
—:R
:A’’
t4t&
,rf”:
;‘‘)%
.‘ct-
‘?‘
••
.“““
•
/
No

—..
•%.—
._
.l
••
•4.
..
t.•—
00

4-N
n
Sch
edul
eis
fina
lize
d24
hour
spri
or
tosu
rger
yda
te
Ser
vice
Sch
edu
lin
gS
yste
m(P
icki
ngof
firs
tca
seon
ly)
M.A
.or
Flo
ater
uses
P.L
.to
pull
item
sfr
omsh
elve
s
••
p•I
•••
—..•.
••
••
••
•n
•-—
••...
•••I
•.•
•a;
•.•.
n
P.L
.=Pi
ckL
ist
M.A
.=M
edic
alA
ssis
tant

L:1
[3yp
odpr
epar
edth
eni
ght
befo
reis
chec
ked
for
com
plet
enes
sm
orni
ngof
surg
ery
Day
o.
urge
ry
Byp
odm
oved
into
the
OR
suit
ebe
fore
case
Scr
uban
dC
ircu
lato
rse
tup
for
case
(em
ptyi
ngby
pod)
Cir
cula
tor(
s)st
arts
sear
chin
gfo
rth
em
issi
ngit
em

V.
t•...
.r.
‘•
•..•;
••‘
:.%
aP
%f*’
,‘“•
‘T
C
l3yp
odis
push
edba
ckin
toth
ecore
(to
pick
the
next
case)

0•
C)
P.L
.is
give
nto
the
cler
kfo
rco
stpu
rpos
esC
.N.
liF
tC
lini
cian
IIP.
L.=
Pic
kL
ist
n
P.L
.is
give
nto
oC
.N.
III
toap
prov
ech
ange
s
YE
S
NO
P.L
.is
give
nto
cler
kto
reco
rdch
ange
son
com
pute
r
I1
•‘‘r
!”•.
.•.!F
F••‘
—.1
-.-
:
nn
..
—.
--V
.....
——
—,...
a._
i•
,.-
——
——
—
bAiT
tm)
fl6u
Ceak
NE
UR
OSU
RG
ER
YIN
VE
NT
OR
Y
QU
OTA
DA
TED
ATE
DA
TED
ATE
DA
TED
ATE
DA
TED
ATE
DA
TED
ATE
Dow
Cor
n!ng
Scie
ral
Spo
nge
:.•.
..
—V
.
kL
___
__
-3
each
_.
--____
TY
p!!_._.
--
#1
5-2
7005(1
_bx=
5)
QcriI
0.._
.--.-—
.—
-____
—____
-_____
#P
4412(l
bx=
20)
?:4
0.a
ch
..
-_____
—___
_
.—
-_
__
__
14m
mD
owel
c’__
____
____
__!
L_
Cru
shed
Can
ce!l
ou
s(lo
z4—
..-—
—..
.I
—.
PP
zP
Q9
c._
._.Z
c_
_I!cst.
We4e(_
•-
—
L(cL
__
_..
_?c
acp_
_II
iacC
resI
Wed
ge13
-15m
..-
---.
..—
—.—
---_____
#1
00
405
(eac
h).
?.c
h_
_L
c—
____
-—
._
lilac
Cre
stW
edge
18-?
Om
—____
?c.Z
2I___
Iliu
rnT
rico
rtS
trip
2.2c
mx4
5mm
—.-
-—--
-—--
-.-—
..-—
--.
—
#100
-500
(eac
h).-.?aL
/_
.-___
Ilium
Tri
cort
Stri
p2.
?crn
xQ
mr.
—
#100
-530
(eac
h)2c_
._.
._
__
__
.——
--
—-____
!!!
nm
__
__
_1P
(cL
__
_le
ach
(
Pat
ella
Wed
gel6
mm
xl8
mm
-—
.—
-_
--—
--.
.--_
__
_.-—
--—
-.—
-—
-—
#O
-5(é
ah)
Iea
ch2)/
CD
Pag
e1
h/uh
/adm
n/ne
uros
up.x
ls

NE
UR
OSU
RG
ER
YIN
VE
NT
OR
Y
-
QU
OT
AD
ATE
DA
TED
ATE
DA
TED
ATE
DA
TE
DA
TE
DA
TE
DA
TE
DA
TE
LIteysj
‘1I?
3?each
CQ
6rn
x8
crn
#D
G-0
60
8S
ç-_
__
-_
__
_
--_
_—
‘?‘P
?.._______
?x.
iiox
-____
1/2x
l/2
N#
80
4002boxes
-__
TL
1ux3
M11
8014
082
boxe
sV
/Z
Z-
ZZ
Cod
man
SundtK
eesC
Ips
—___
?x
?Q
10
—-
leach
-_
__
_
25x3m
m#2
017
62le
ach
-_
_
r#20
-17
63
leach
J3x
3m
rn#20-1
765
leach
-_
__
3x5m
m#
201766
leach
i7
ZZ
Z_
_m
_gJ___
-_
—
ZZ
ZZ
-
4x
7m
m#
20
17
17
—__
leach
5x5
rnrn
#20
1772
leach
T76
-_
_
Pag
e2 n
h/uh
/adm
ri/n
euro
sup.
xls
C

——
——
——
——
——
...‘-,—
..—
——
NE
UR
OSU
RG
ER
YIN
VE
NT
OR
Y
Aes
cula
pS
calp
Clip
s
icc.
codm
anL
eRoy
Ran
ey#2
0-10
34(1
bx=
20)
P!ering
c.c’”c
K!.
._
_.
-.
--.—
-.-----—
.
___—
____
__
__
__
__
_____
__
__
Nic
olet
Silic
onE
xten
sion
-—
___
....
Xom
ed-T
reac
eN
eedl
eE
lect
rode
s
Xom
ed-T
reac
eN
icol
etP
robe
_.
-
c!’
m9T
hbIi
1g
..
.____._
_._
_.
__._
#80-
1163
(1bx=
Pag
e3
h/uh
/adm
n/ne
uros
up.x
ls
IQU
OT
AD
AT
ED
AT
ED
ATE
DA
TED
ATE
DA
TE
DA
TE
DA
TE
DA
TE
DA
TE
25-3
0ea
ch
ichZ
1b
I7àZ
Zim
mer
Hal
lC
rani
Bla
de#50
59-2
22(1
bx=
5)
..____
.._._._
....
Zim
mer
Hal
lW
ire
Dril
l.
..
c0P
_--
._
_
gQ
g5
h—
____
10-1
5ea
ch
4-6
each
àead
h
5ea
chI
20-3
0ea
ch

TAV
AA
nale
dS
awB
lade
s
ATL
Ult
raso
und
Cov
ers
NE
UR
OSU
RG
ER
YIN
VE
NT
OR
Y
‘04
h/uh
/adm
nfr
rosu
p.xl
s
Cr
May
fiel
dSk
ull
-
Om
niM
edR
adio
lusc
ent
Skul
lP
ins
QU
OT
AD
ATE
DA
TED
ATE
DA
TE
3-4
boxe
sa
‘blc
DA
TE
.-...—
T-—
____
—-—
—
DA
TED
ATE
DA
TED
ATE
DA
TE
-.
.
1c:Q
c—
___
Lon
eS
tar
Med
ical
Pro
duct
s,In
c
?P
Jx
.
.._.
--
..
1--—
——
.—
—..—
-.---.....
...--.-.-.-
--.----.—
.-----
---.-----------—
--
---.-,-
—-...------
—-
----—
.—
—-
------
i.___
____
#622
-OO
O-1
7Oje
ach)
1P1c
c.M
orga
nZ
eiss
Opm
iS
cope
Cov
ers
-_____
—_
__
__
.,..
.._____
—.___
ffii.
?P
c._
__
_,.
.._
--
MED
TRO
NIC
mpcsP
rt
--
—.__
....
...
#86
15
S(e
ach
)-___
....
—.
.
Med
ical
Adh
esiv
e#0
8011
8(e
ach)
—-
1ea
ch—
__
__
_
Cat
hete
rA
cces
sP
ort
Kit
#85
40
(each
)__
leach
-—
--
-

.—.
——
.-.-
--
—i.
.-—
NE
UR
OSU
RG
ER
YIN
VE
NT
OR
Y
QU
OTA
DA
TED
ATE
DA
TED
ATE
DA
TED
ATE
DA
TED
ATE
DA
TEID
ATE
2ea
ch-___
_
P!i:cc1Y
1’t
-
#859
0-41
2ea
ch
Pis
ces
Qua
dP
lus
__
__
__
__
__
1each__
4&
Pis
ces
Qua
d
ffc’L
__
1cL
o.
ii(Ig
)_
#348
7A-3
3(e
ach)
l!re
!!__
Res
ume
TL
Itrel
IllIP
G
Itrel
IIE
xten
sion
Kit
Itrel
IIE
xten
sion
Kit
_____
74
96-5
1(e
ach)
-
1ea
ch-
Ref
illK
it
______
1(r)
-no
ne
Sym
mix
Lea
dK
it#3982-2
(each)
1each
__
__
__
__
__
__
__
__
__
__
__
__
__
_______________
__
__
__
__
__
__
__
Pag
e5
h/uh
/adm
n/ne
uros
up.x
ls
1ea
ch
1ea
ch
1ea
ch
1ea
ch

NE
UR
OSU
RG
ER
YIN
VE
NT
OR
Y
.--—
--—
-.—
--__
__
QU
OT
AD
ATE
DA
TED
ATE
DA
TED
ATE
DA
TED
AT
ED
AT
EID
AT
ED
AT
EB
oots
&A
nch
ors
—
.-.—
——
1ch_
--
——
--—
—--—
-—
-—
——
--—
-----------
--..
----
Wre
nche
s&
Scr
ews
#3
55
O-O
2ac
hj
leach
--
c!__.__
....
——
.
.
c)._____
1ac[!_._
.±Jö
.-—
-—
-—
—----
Pou
ch
..
c__
....___
.—
.
._
._
cc
Ijo
PS
Med
ical
oll
neO
penT
ipC
ath
.#81iO
iea2each
?ech_..I_
&—
_
.
PiA
iPE
1.c
L______,._
çt
.tQ
%2
...
.
Cod
man
Ric
kham
Res
ervo
ir#82
-l6
2le
ach
)5
each
Cod
man
15cm
Hot
ter
Ven
t.C
ath.
QcL
__._
_3J_
-_.
.__.
._.
.._
..
Cor
dis
15cm
Hot
ter
Ven
t.C
ath.
—
2ea
ch
Cor
dis
35cm
Ven
t.C
ath.
Acc
.K
it#9
51-3
03(e
ach)
4ea
chS
,Ic2
h/uh
/adm
nl36
)stJ
p.xI
sJ

.—
——
——
——
——
——
NE
UR
OSU
RG
ER
YIN
VE
NT
OR
Y
QU
OT
AD
ATE
DA
TE
2ea
ch
2ea
ch
Con
sV
alve
Uni
t-
Low
ciz
i_
_.
Co
rdis
VaL
veU
nht-
w)t
M
c9!Y
9Systcn..
fl9
03
-32
0{e
ach
-
c°c!
c!
Shun
tS
yste
m
Cor
dsH
V_l
Sys
tem
03-325jç_
Cor
dis
HV
Lum
bar
Val
veS
yste
m
-
Con
dis
Sid.
Inte
gra!
Shu
ntS
yste
m
h/u
h/ad
mn/
neur
osup
.xls
Cod
man
-H
igh
#82-
1600
(eac
h
Cod
mar
iH
olte
rV
alve
-M
ediu
m
Cod
mar
iH
olte
rV
alve
-L
ow#8
2-16
0?(e
ach)
DA
TED
ATE
DA
TED
AT
E.
DA
TE
IDA
TE
DA
TE
2ea
ch
i(chL
__
_
___._
DA
TE
each
4/c
,)I
1ea
chI
I_cL
Z
1 23
each
3,4
--
zzzz
zz:
1ea
ch-F
4ea
ch
2-3
each
Pag
e7

-—
——
——
NE
UR
OSU
RG
ER
YIN
VE
NT
OR
Y
______
QU
OT
AD
ATE
DA
TED
ATE
DA
TED
ATE
DA
TED
AT
ED
AT
ED
AT
ED
AT
E‘
Cor
dis
91cm
Per
iton
eal
Cat
h.#9
53-1
01(e
achj
2ea
ch—
____
--_____
Cor
dis
46cm
_Atr
ial
Cat
h.-
——
#953
-100
(eac
h)—
_______
__
•—
——
——
-—
——
—
Cod
man
Per
iton
eal
Cat
h.#8
2-16
82(e
ach)
leach
-_____
-—
-
Codrn
anA
tria
lCat
hJy
çeB
——
-____
#82-1g___
!t_
#82-1
501(e
ach)
4-8
each
—____
Cod
man
Sir.
Pla
stic
Con
nect
or#8
2-15
04(e
ach)
-1
each
-_____
Codm
anP
last
ic3w
ayC
onn.
-_____
#B2-l
52
O(c!’Ii
leach
cP
pcc!____
-___
#16-
1057
(1bx=
.3-5
Cor
dis
YC
onne
ctor
—
-__
#901
-410
(eac
h)1
ech____
Cod
man
TC
onne
ctor
?c_,7_
cord
isst
epD
own
Con
nect
o-
-
#901
-415
(eac
h)1
ech
I
Pi’
”’8
h/uh
Iadm
nlrn
up.x
ls

——
——
——
——
—w
——
——
——
—-
—
NE
UR
OSU
RG
ER
YIN
VE
NT
OR
Y
QU
OT
AD
ATE
DA
TED
ATE
DA
TED
ATE
DA
TE
DA
TE
DA
TE
DA
TE
DA
TE
Cor
dis
Bur
rH
ole
Res
ervo
ir#9
55-1
11ach)
Sid
earm
4ea
ch‘9
/c.__
—--—
----
——
—-.-
-—
..—
--_
..-.,.-..--.-
Cor
dis
Bur
rH
ole
Res
ervo
ir
icP
L______
i8cL
.!,
Z--___
-_
_
Cor
dis
Bur
rH
ole
Res
ervo
ir#9
55112eç
—tc[!_/
._.._
çgesç_
__
—___
-—
—.—
-_
__
_
L(cP
L.
.
Cor
dis
T’C
onne
ctor
#9O
1-4
(each)
_____
leach
.
—____
_.
....._
Cha
mbe
r-
Low
#850
-030
1(e
ach)
t.8
.c!.
_..2
_4
—-_
__
_.___
-.
--
—..._.
..
-.
....
—.
L_
__
.__
._..
cL
/b.
..
..
.
yercie
Ori-
Offr’ig
..—
—-—
.---—
—-—
-.
PceI-!ig
—.—
-—
—-—
.--—
#B
50
-0ea
ch)
1cL
._.___
._
__
__
y,c!!’iln
g.
-
._
.....
..
.._
_.
Dev
ice
-M
ediu
m
igic
)___
____
____
__.
Hey
erS
chult
eOn-O
tfF
ius[
ng
—._
——
--.
—.---—
-—
-—
—..
Dev
ice
ffo
gçah
j.._
-le
ach
--
•._____.
._
_—
.
Hey
erS
chul
teO
mm
aya
CS
F-
--
-.--—
—-—
#850
-127
2(e
ach)
•1
each
4.
h/uh
/adm
n/ne
uros
up.x
lsP
age
9
qic
-H
L.f
l(1ec)
NE
UR
OSU
RG
ER
YIN
VE
NT
OR
Y
Pv
10h/
uh/a
dmnl
ne’i
rosu
p.xl
S
__
__
_
QU
OT
AD
ATE
DA
TED
ATE
DA
TED
ATE
DA
TED
AT
ED
AT
EID
AT
ED
AT
E
Hey
ech
lteO
mm
ay
aC
SF
-._
__
-—
___
T
74
eac)_
__
lch
Bax
ter
Edw
ards
Bar
baro
____
_Sy
ring
oS
hunt
#800
-75S
01ach
)2
each
—_
__
__
—_
__
__
Cor
disO
rbis
-Sig
rna
Val
ve—
___
--___
#909
-612
(eac
h)-_
__
_le
ach
Bar
dJa
vid
Car
otid
Shu
ntle
ach
-_____
#00m
4(s
tocktr
om
rmii
)(ç)
—____
Rad
ioni
csG
utin
Rad
Nu
chd
e5each
_-_
__
--_
_-_
_
Cat
hete
r(l-_
2l-125________
-_
__
_
UR
NC
-6(ç
hj
-____
-_
__
_-
Ow
ens&
Min
orL
gPin
kK
eyho
les
-____
ta
-b
3t-
.h
—__
Co
rcsE
xte
maID
ran
aeK
-____
#910-1
09(e
ach
2each
3/j
Cod
man
Tw
ist
Dril
l
CN
S-E
xter
nalD
rain
age&
Mon
itor
ingS
yste
rn#S
P00
65(e
ach)
5each
-___
-_
__
Cod
man
ICP
Kit
#80-
1190
(eac
h)3
each
Cor
dis
Lum
bar
Cat
h.A
cc.
Kit
1?t(cP
L__._
_ch
-_
__
Cor
dis
Ven
t.D
rain
age
Bag
ss->
7/
/.
——
——
—
NE
UR
OSU
RG
ER
YIN
VE
NT
OR
Y
QU
OT
AD
AT
ED
ATE
DA
TED
ATE
DA
TED
ATE
DA
TE
IDA
TE
IDA
TE
DA
TE
cP
tL
_..-—
..—
.-..._..
Cod
man
Tita
nium
Mes
h#
43O
22
(eac
h)!çL
.i7
—_
__
_
Cord
is(r
oca
num
ber
)3-
15ea
ch
Cor
dis
Per
iton
eal
Intr
oduc
erS
heat
h
PE
___
-
9q
jp
t_____
—____
-____
-__
__
Clo
war
dFo
am#
NL
99
90
2(l
bx=
1?)
1ch
—._
__
_—
___
!cc!
----—
-—
---
-—
..—
--—
—--—
—-
.-—
—--.
---.—
----—
—----
—
8!4
i------
---------
-—
—--
-
US
Med
ical
CU
SAP
roce
dura
lP
acks
Cus
aC
anni
ster
s
OO
-O
O(L
cP
2,4
—___
----—
—
p!y_
._.
._-..-
-
#014
6570
0(e
ach)
1ea
ch..
TAV
A14
mm
Dis
trac
tion
Scr
ews.
4ech
_.
The
sem
ust
beord
ered
15at
ati
mel
itli
TAV
A16
mm
Dis
trac
tion
Scr
ews
..
?ech
......__
..___..
Thes
em
ust
be
ord
ered
15at
ati
mel
li
Pag
e11
h/uh
/adm
n/ne
uros
up.x
ls

NE
UR
OSU
RG
ER
YIN
VE
NT
OR
Y
__
__
—-
QU
OT
AD
ATE
DA
TED
ATE
DA
TED
ATE
DA
TED
ATE
DA
TE
IDA
TE
—---------
5ch
I7
—____
c7±
c_
fLL
—____
#505
6-17
05aC
h_
—--_-
--
-
codm
anM
ayne
idL
ockN
ut—
-___
9_________
?c’_
_?—
._____
Med
tron
lc
Mat
rix
Rec
eive
r#3
272
(eac
h)
Mat
rix
Tra
nsm
itte
rK
it#3
210
(achL
-
Mat
rix
Scr
eene
r#3
627
(eac
h)—
._____
Pis
ces
Qua
dL
ead
Kit
#348
7-A
(h)j
rere
guir
ed)
—_____
Eth
icon____
3-O
Chr
omic
FS
-2#6
36H
3ea
ch3
-
4O
Sd
kT
F4
#N
27
2H
3eac
h3
3-0
Plai
nG
ut_P
S-2
#163
0G2
each
3,
iaj1_fft1
44_
ii
--
Mid
asR
ex
kl_
__
__
3-_
_
-__
480
2ea
ch
ZZ
3z
AM
-i2e
ach
13
/-
At
iO
eachj
-—
AM
-8D
4each4/c2
-.____
-_
__
_
AM
-12
6ea
ch
q9eG
,a/
*Z
O-6
D/u
h/a
dm
n/n
’‘.s
up.x
is

AM
-32
____
BiiIL
__
__
.B
-38-5
__
__
BC
-i
____________
2ea
chC
-i
__
__
_
5ea
chM
-i2
each
Sal
ety
Sea
ls(1
bx=
20)
1-2
boxe
s
NIU
HU
SU
F-l
lihH
YIN
VIN
IOH
Y
2ea
ch8
each
QU
OT
AD
ATE
DA
TED
ATE
DA
TED
ATE
DA
TE
LA
I2
each
2ea
ch
DA
TED
AT
ED
AT
E
VL
D
DA
TE
MjN
T)
2ea
ch
‘kg.
___
—_
__
:_
_._
_
s*__
____
____
____
__37
c??ach_.3/
W-1_________
cL
,:;/
QW
H-2
2ea
ch
f10
Lub
ncan
t(e
ach)
14
each
7JZ
ZZ
ZZ
ZZ
ZA
irD
iffu
sers
(1bx
=8)
2bo
xes
31
Pag
e13
h/uh
ladm
n/ne
uros
up.x
ls
::.
:.‘.
:•‘•:•
:ç2
-•
4’et
f9.’
!”€?
?....
lq
fl*
n
Appendix I
UNiVERSiTY OF MICHIGAN HOSPITALS
OPERATING ROOMSEQUIPMENT! SUPPLY REQUISITION
DATE: / / REQUESTED BY:____________________________________ ROOM:
_____________
NAME OF COMPANY (ONE COMPANY ONLY!)
Y N
V N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
V N
Y N
V N
Y N
Y N
Y N
Y N
V N
________________
BE SURE AND CHECK IJNE IF ITEM IS PATIENTCHARGE IFOR OFFICE USE ONLY
SHIPPING: 1st DAY
po# 2ndDAY
RELEASE # NORMAL
CONFIRMING TO: DELIVERY ADDRESS VERIFIED? Y 0 N 0- fl1 ‘7ñ 4/01
()

Tye: STND Rn Time: 10:46am - 02/16/96 AppendixJSUPPLY REQUISITIONUniversity Michigan Medical Page
-Surgeon/Procedure
Suraecn: Deeb,G. Michael*
Procedure: CABG-IMA *CABG w/IMA
Prep:Gloves:Position:Drape:Sutures:Hints:Last Supply List Update: 02/13/96
Number ItemReq las Code H Description
U. HOSP. MEDICATIONS\SOLUTIONS2 5269 WATER FOR IRRIG BOTTLE 1000ML
q 6 5722 NACL 0.9% IRRIG BOTTLE 1000MLINSTRUMENT TRAYS
7GREYSEE EXTENDED PREFERENCE CARD
Location Charge Total
1 5000171 5000181 5000201 5000221 5000401 5006001 — 5006021 500654
I i 5006551 500656
U. HOSP. CORE A1 1005081 1005101 1001683 100654
I i 12351 2000411 300013
I1252
1 28501 4462
1 1001843 100187i 1001971 135400‘ 1 1502011 1850001 200182
1 1 200183
1 1 200185HOSP. CAUTERY
1 1231
1 2 1232U. HOSP. CORE A
PUMP IPUMP IIRETRACTOR MORRIS W/O SPRINGDR. DEEB CORONARY TRAYDR. DEEB SAPHENOUS VEIN TRAYIMA RETRACTORIMA BARICE PADDLE
DIUM INTERNAL PADDLESSTERNAL SAW
CARDIAC CART
TUBE CHEST 32FRTUBE CHEST 32FR CVDPUNCH VASCULAR PRECISION 4CLIP ATRAtJNAX SPRING 6TUBING ARTERIAL PRESSURE 72”RETRACT 0 TAPEBLADE BEAVER MINI #6500PLEURAVAC AUTOTRANSFUSION SYSTEM W/BAGCATHETER FOLEY TEMP SENSING 1SFRPLEUR-EVAC ADULTADAPTER MULTIPLE PERFUSION E1889CANNULA VESSEL DUCK BILL #30001TOURNIQUET ADULT COMPLETE SET 79006SYRINGE PRESSURE SENSING W/3000iVENT ADULT DLP #12002CANNULA CORONARY SINUS #94115 15FRCANNULA VENOUS 2 STAGE 36-46FR #164525SUCTION CARDIAC MINI SARNS 14991CANNULA AORTIC 8.0t #165264
SUPPLIESBOVIE PENCIL HANDSWITCHING DISPOSABLEBOVIE PAD ADULT
DRUG-U
DRUG - U
INSTU
INSTU
INSTU
INSTU
INSTU
INSTU
INSTU
INSTU
INSTU
INSTU
UCAC1O2
UCAC1O2
UCAC1O3
UCAC1O3
UCAC1O3
UCAC1O3
UCAC1O3
UCAC1O4
UCAC1O4
UCAC1O4
UCAC1O9
UCAC1O9
UCAC1O9
UCAC1O9
UCAC1O9
UCAC1O9
UCAC1O9
UCAC1O9
UCAC1O9
UCAUTERY
UCAUTERY
2.003.00
0.000.000.00
13.0016.00
23.0014.003.00
16.003.00
57.00
40.0043.00
31.00
6.00
6.0032.00
24.00
103.0023.00
21.00
32.00
5.005.00
4.00
18.00
0.000.000.00
0.000.000.000.000.000.000.00
13.0016.0023.00
42.003.00
16.003.00
0.0040.00
43.00
31.0018.00
5.00
32.00
24.00
103.0023.0021.0032.00
5.0010.00
SUPPLIES
Type: STND R,jn Time: 10:46am - 02/16/96
SUPPLY REQUISITIONUniversity of Michigan MedicalSurgeon/procedure
Location Charge
UCOA 37.00
Number ItemI Req Iss Code H Description
1 — 220234 BLADE SAW STERNAL
U. HQSP. CORE SUPPLIES
1 — 103486 MATTRESS HYPOTHERMIA LONG
1 138540 POUCH PACEMAKER #5409
2 — 150096 GEL POVIDONE IODINE TOPICAL PHARMASEAL
2 — 185331 BANDAGE ACE 6’
2 — 2560 STOCKINETTE 6” TUBULAR UNBLEACHED NS
1 300012 BLADE BEAVER MINI #6400
1 — 4441 CONTAINER SUCTION 1500CC
U. HOSP. BASIN SETS
2681 BASIN SET MAJOR CUSTOM
U. HOSP. DRAPES/LINEN
1 2147 GOWN SURGICAL XX LARGE-EXTRA PROTECTION
1 — 6132 GOWN PACK 4/PACK LARGE
6 T-841 TOWEL 4/PACK REPACK
1 1675 PACK DRAPE PUMP BASICU. HOSP. POSITIONING SUPPLIES
1 1239 FOAM KEYHOLE HEAD REST1 1600 FOAM PAD ELBOW/HEEL
U. CORE. SUTURE CART
UCOR
UCOR
tJCOR
UCOR
tJCOR
UCOR
UCOR
UCRBS
UCRDR
UCRDR
UCRDR
UCRDR117
UCRPT
UCRPT
UCSUT
UCSUT
UC SUT
UCSUT
UCSUT
UCSUT
UCSUT
UCSUT
UCSUT
UCSUT
(IC SUT
UCSUT
UCSUT
USRAAL
USRAAA4
USRABB2
USRAV1
USRAW1
USRAX3
USRAY2
USRAY3
USRAY4
USRAZ3
Page 2
Total
37.00
21.00
6.00
14.00
8.00
36.00
3.00
4.00
20.00
9.00
15.00
18.00
368.00
4 00
3.00
5.000.00
6.00
5.00
6 00
8.00
38.00
62.00
4.00
0.00
22.00
187.00
0.00
3.00
0.00
1.00
0.00
0.00
1.00
0.00
12.00
2.00
7.00
1,461.00 ()
21.00
6.00
7.00
4.00
18.00
3.00
4.00
20.00
9.00
15.00
3.00368.00
4.00
3.00
5.00
5.00
6.00
5.006.008.00
38.00
62.00
4.00
3.00
11.00
187.00
16.00
3.00
3.00
1.00
3.00
2.00
1.00
9.00
2.00
2.00
7.00
1 104234104234
1 125056
1 125112
1 125113
1 125114
1 125164
1 125174
1 125231
125394
2 125421
1 125548
125562
U. HOSP. STORE
1 150097
2781
1 1267
1737
1736
1 1063
2534
6 1744
1 1073
1 1753
LIGACLIP LT1O2 SMALL TITANIUMLIGACLIP LT1O2 SMALL TITANIUMSUTURE ETHIBOND 2-0 SH X523HLIGACLIP LT100 SMALL
LIGACLIP LT200 MEDIUM
LIGACLIP LT300 MED LARGESUTURE PROLENE 6-0 VBC M8307SUTURE PROLENE 7-0 VBBV M8304SUTURE PLEDGET PCP3O
SUTURE PDS 2-0 CT-i Z259HSUTURE STEEL MONO 5 CCS-1 M436GSUTURE E-PACK CARDIAC 3340ESUTURE PROLENE 7-0 VBBV 8304H
ROOM SUPPLIES
PAD INSTRUMENT* NEEDLE GUARD POP N COUNT
YANKAUER SUCTION W/O CONTROL VENT
SPONGE LAP 18Xl8 STER
SPONGE LAP 18X4 THORACIC
ALCOHOL ISOPROPYL
STAPLER SKIN DISPOSABLE 35W
SPONGE GAUZE DRESSING 4X8”
PREP SOLUTION POVIDONE IODINE 4 OZ
TAPE MICROFOAM 4”

Type: STND Run Time: 10:46am - 02/16/96SUPPLY REQUISITIONUniversity of Michigan Medical Page 3Surgeon/Procedure
Surgeon name: Deeb,G. Michael*Procedure: *CAB_G w/IMA
4edications: Vancomycin 500mgAlbumin 5% 50 ml x 2Papaverine 300mg = 10cc (2 amps if IMA)
dditional Supplies:
MA supplies: Small ligaclips x 3IMA RetractorIMA BarBovie at 30 for IMAStirrup attachment for IMA Bar
;uture: Cardiac E-Pack#5 Wire Ethicon 2/pkg x 22-0 Ethibond SI-i x 26-0 Prolene Multi C-i7-0 Prolerie Multi By-i2-0 Monocryl x 2
Large Pledgets x 1
ositioning: Supine, key hole foam, temp sensin foleyelbow pads.
rep: ETCH pre-wash, Gel prep x 2
ints: Bovie at 50Ether screen alwaysPicket fence to hold extremity for prepPillow x 2 under legs

tI..
•y..:
•.“*:.
-Jr.z,-a-•
.._r.._x:
,.tI
-Th 1