ez-blocker ® jan. 2010. ez-blocker ® a bronchoscope is mandatory bronchoscopic control for all...
TRANSCRIPT

EZ-Blocker®EZ-Blocker®
Jan. 2010
EZ-Blocker®EZ-Blocker®
A bronchoscope is mandatory
Bronchoscopic control for all in-, and deflations

EZ-Blocker®EZ-Blocker®
ETT Endotracheal tube
EZB EZ-Blocker®
DLT Double Lumen Tube
MPA Multiport Adaptor
PreparationsPreparations

PreparationsPreparations
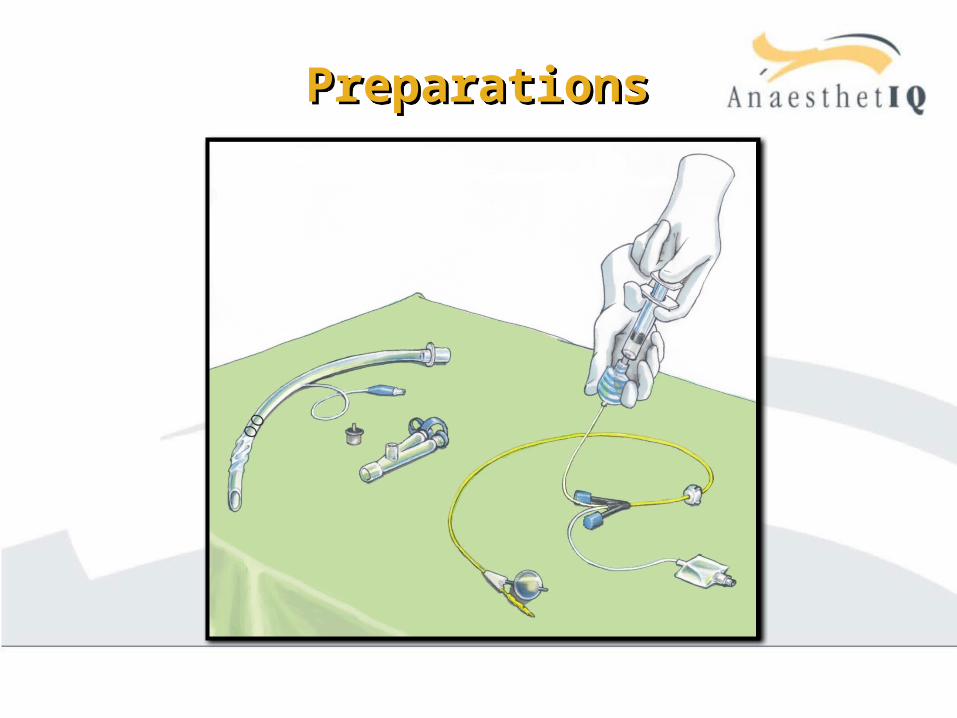
Sterile cloth
ETT Lubricant Syringe Marker EZ-Blocker® set
EZB Multiport Adaptor Closing caps CPAP connection piece

PreparationsPreparations
Inspect for damage Remove protection shaft of the
EZB carefully by pulling the labelat the top of the shaft
Fix 2 blue closing caps on CPAP ports
Inflate cuffs to check for leakage Deflate completely vacuum Lubricate
PreparationsPreparations
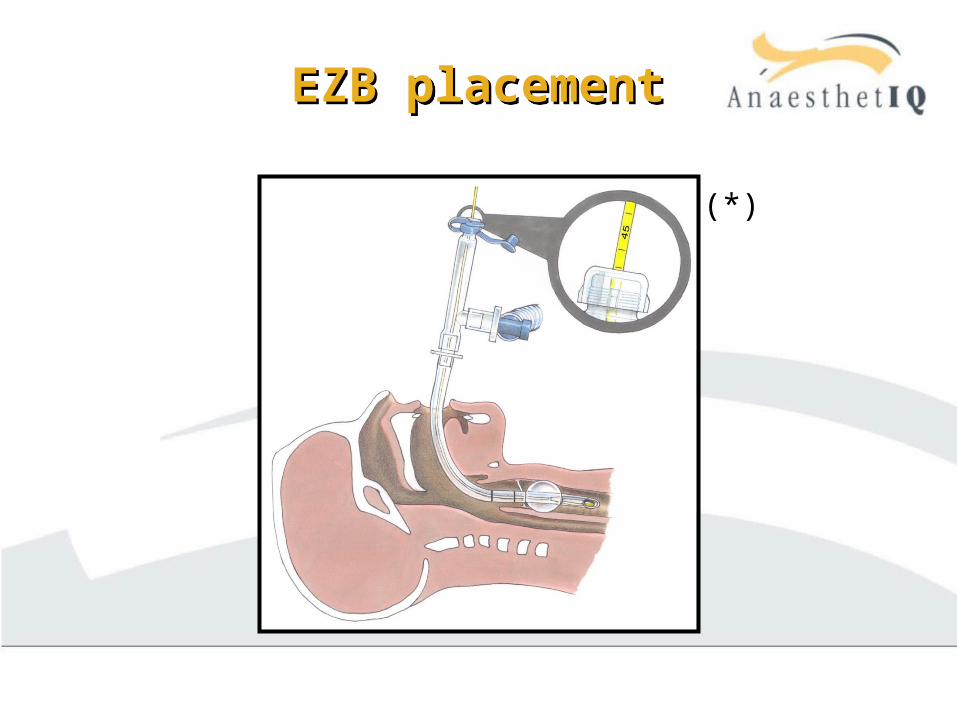
(*)
PreparationsPreparations
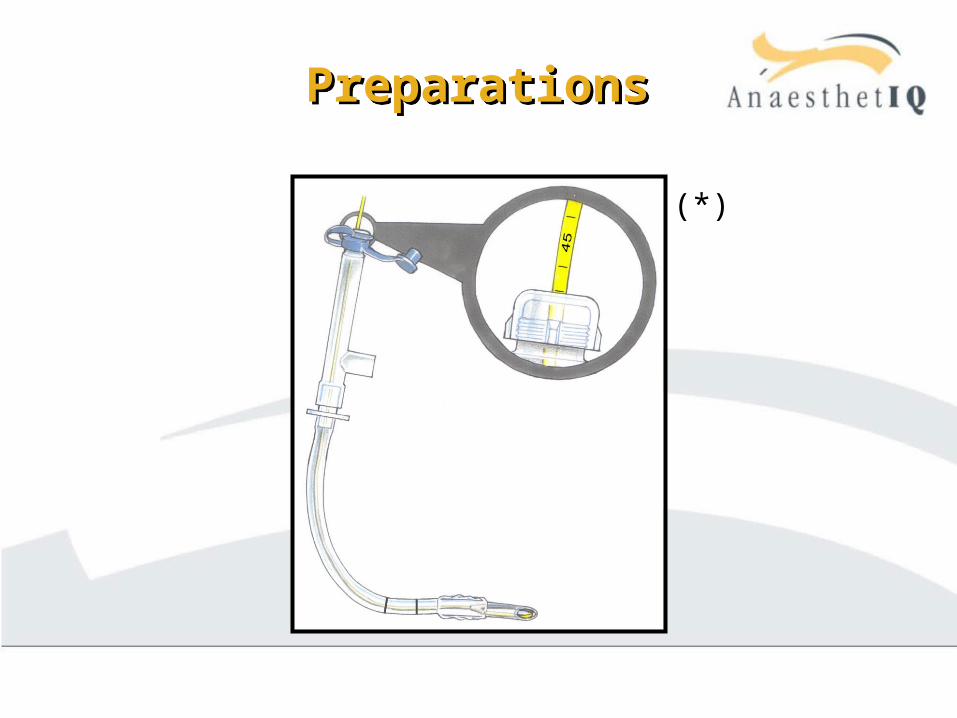
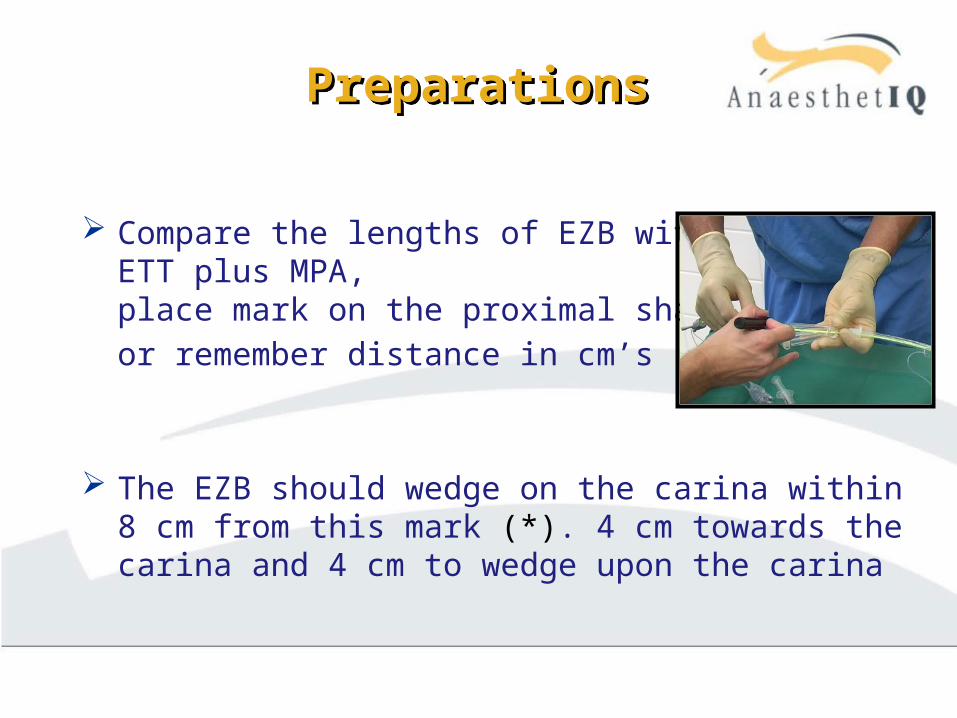
Compare the lengths of EZB withETT plus MPA,place mark on the proximal shaftor remember distance in cm’s
The EZB should wedge on the carina within 8 cm from this mark (*). 4 cm towards the carina and 4 cm to wedge upon the carina

IntubationIntubation
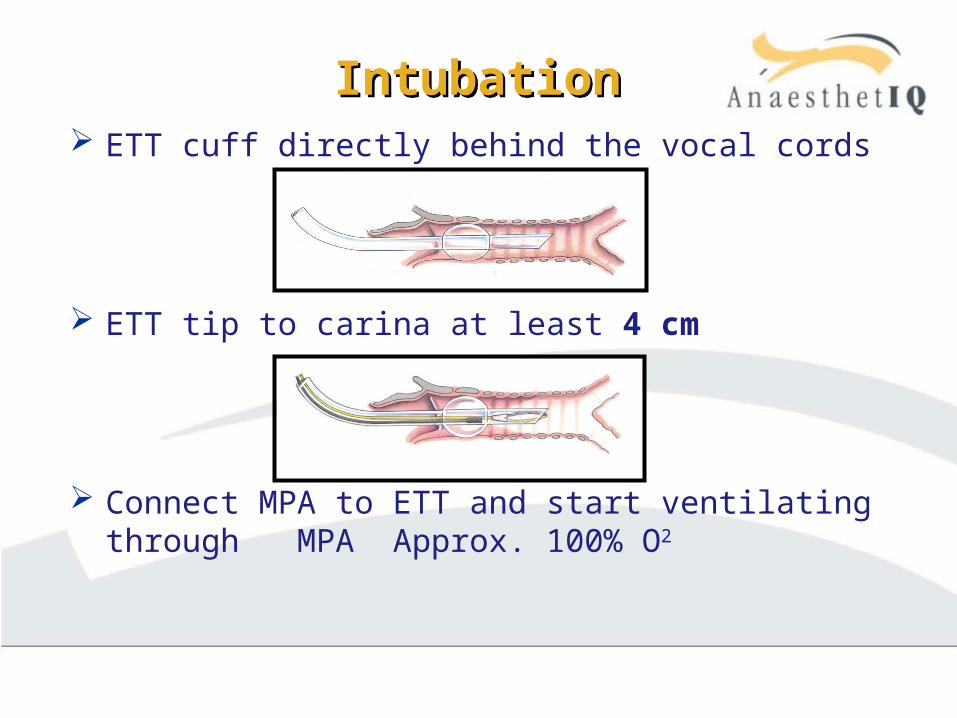
IntubationIntubation ETT cuff directly behind the vocal cords
ETT tip to carina at least 4 cm
Connect MPA to ETT and start ventilating through MPA Approx. 100% O2

IntubationIntubation
Distal end ETT
4 cm
Carina
EZB extensions need 4 cm to spread before wedging the carina
EZB placementEZB placement
(*)
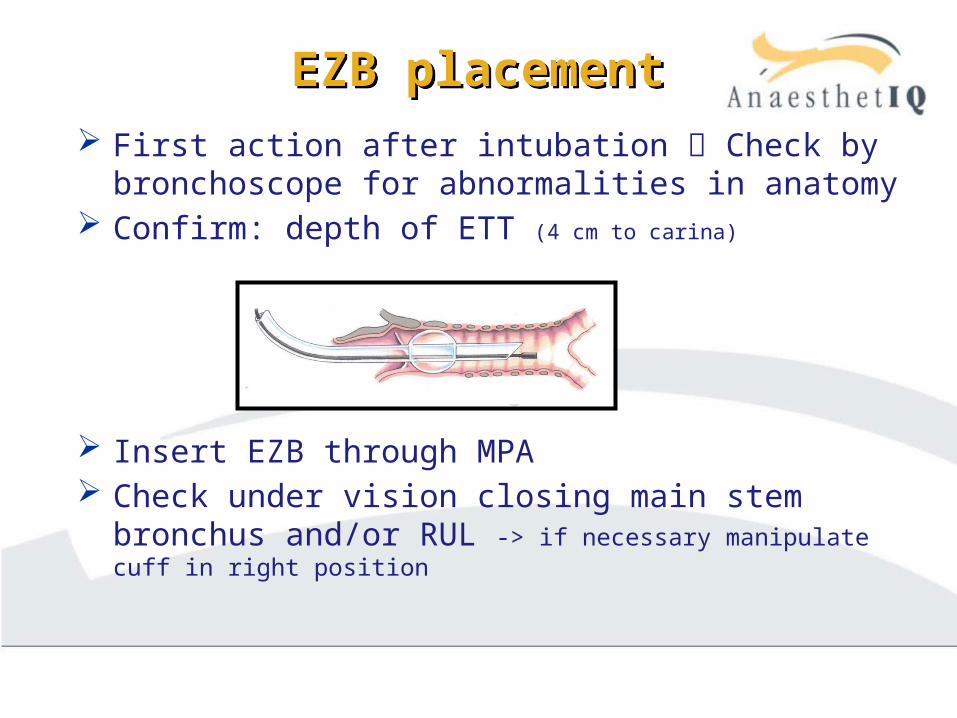
EZB placementEZB placement First action after intubation Check by
bronchoscope for abnormalities in anatomy Confirm: depth of ETT (4 cm to carina)
Insert EZB through MPA Check under vision closing main stem bronchus
and/or RUL -> if necessary manipulate cuff in right position

EZB placementEZB placement
Fiberscopic inspection of cuffs
Inflate the cuff in thetarget bronchus until Minimum Occlusive Volume (MOV) has been reached
Deflate the cuff vacuum



EZB Procedure lung collapseEZB Procedure lung collapse
Ventilate with deflated cuffs. Approx. 100% O2
Position the patient Disconnect ventilation from MPA as soon as the
surgeon enters the thoracic cavity Lung will collapse

EZB Procedure lung collapseEZB Procedure lung collapse If needed, the surgeon manipulates the lung to
the size of his desire After successful collapse, the cuff is inflated
under vision, start One Lung Ventilation Through resorption lung collapse will improve If collapsed lung starts ventilating again, deflate
cuff and disconnect ventilation -> re-collapse! When lung has the right size -> re-inflate cuff and
restart ventilation -> Always check with scope!
EZB removalEZB removal
End of operation deflate cuff. Vacuum!
Ventilate carefully to remove all atelectases
Block the other lung for bi-lateral procedure, or remove the EZB
The same ETT is used postoperatively

EssentialsEssentials

Essentials Essentials
ETT cuff must be introduced directly behind the vocal cords
EssentialsEssentials
First action after intubation Bronchoscopy
Confirm: Depth of ETT (4 cm from carina) and location of right upper lobe
If a cuff is not inflated, it should be deflated completely (vacuum)
Both cuffs should never be inflated at the same time †

EssentialsEssentials
After the EZB extends from the ETT, the EZB will wedge on the carina within ± 8 cm
After wedging the EZB on the carina, the ETT may be advanced a few cm for even more stability
No wedge? Both extensions situated in the same bronchus Check with scope, retry and/or withdraw ETT for
a few cm to provide space for spreading
EssentialsEssentials
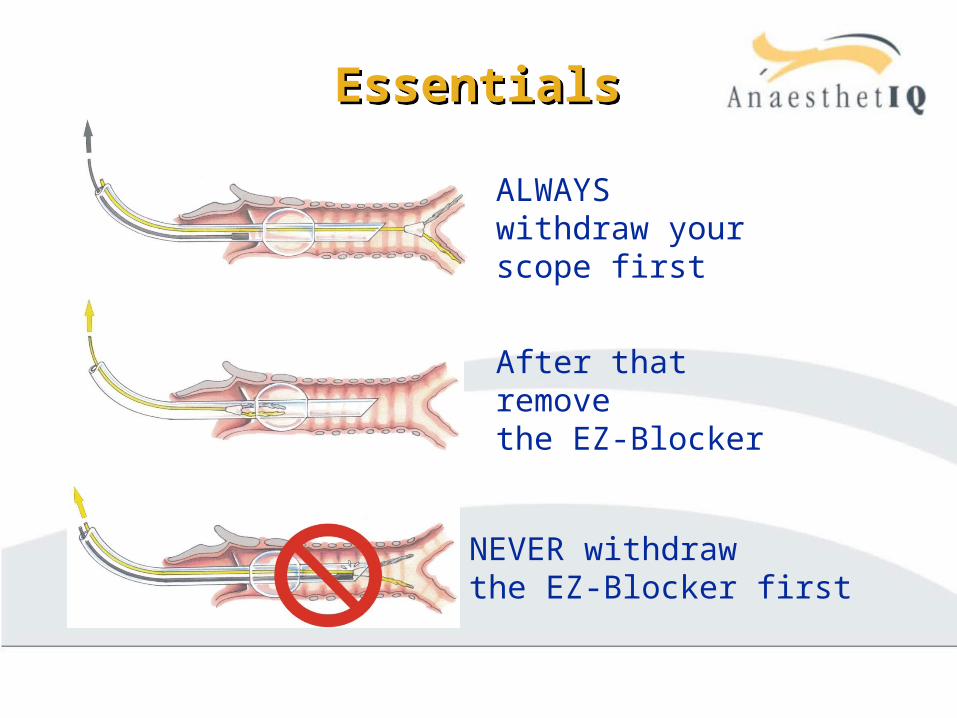
ALWAYS withdraw your scope first
After that removethe EZ-Blocker
NEVER withdrawthe EZ-Blocker first

EssentialsEssentials
Deflate cuffs completely (vacuum) Carefully ventilate until all atelectases are gone PEEP is needed before wound closure Check lung expansion Remove Bronchoscope first, then the EZB Never jet-ventilate a patient with a EZB in place
-> The lung could be damaged