experienced resource nurse: driving quality and decreasing ... resource_lawrie s provost.pdf ·...
TRANSCRIPT

Experienced Resource Nurse:
Driving Quality and
Decreasing Cost
Barb Lawrie
Sharon Provost
Vancouver Coastal Health June 2014
Q
C

Who are We?
•We serve over 1M people; 25% of
BC’s population
•Approx. 20,000 staff; Budget 3.18B
• Per year over 2.8M patient days of
care & 356,000 emergency visits
•4 Urban & 6 Rural Acute Care Sites
•Full continuum of care:
Acute/Community/MH/Residential

Our story...


Why a New Role & Why Now:

The Driving Forces
New Grads
needing unit
based instead of
float positions
Impact on
Quality of Care
Need
experienced
relief
Increasing OT
Costs and
working short

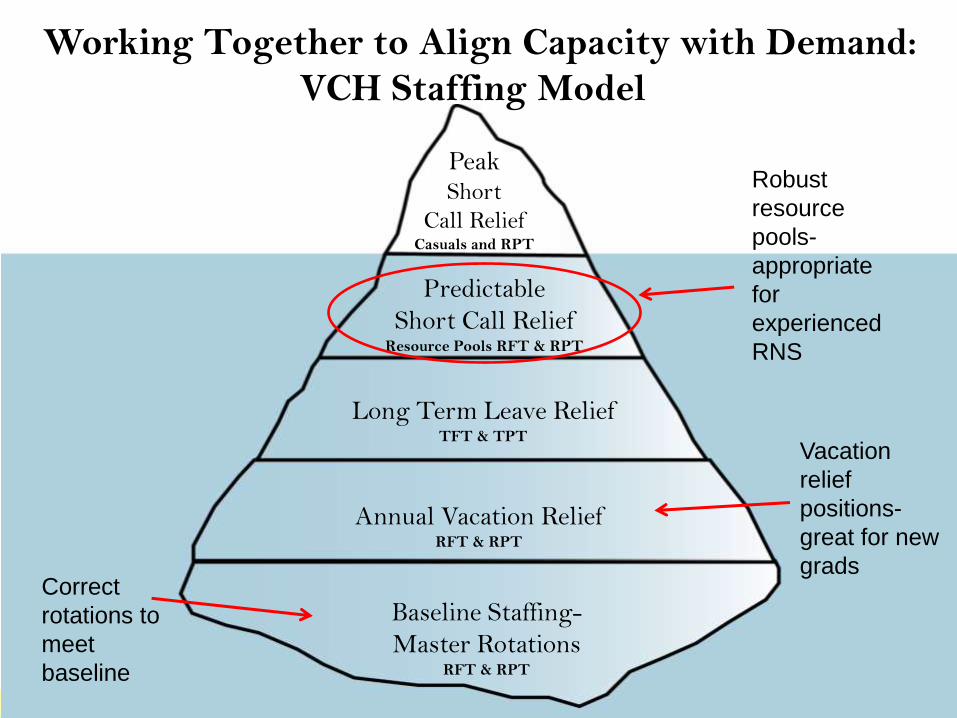
Working Together to Align Capacity with Demand:
VCH Staffing Model
Baseline Staffing-
Master Rotations RFT & RPT
Long Term Leave Relief TFT & TPT
Annual Vacation Relief RFT & RPT
Predictable
Short Call Relief Resource Pools RFT & RPT
Peak Short
Call Relief Casuals and RPT
Correct
rotations to
meet
baseline
Vacation
relief
positions-
great for new
grads
Robust
resource
pools-
appropriate
for
experienced
RNS


Experienced Resource Nurse Role
Why • Right level of experience in
roles
• Decrease reliance on casuals
• Make float pools attractive & part of a leadership career path
• Decrease OT
• Increase support & mentoring for new grads
What • Level 2 permanent relief
positions covering 4-5 units
• Work all shifts with a set master rotation
• 5% of shifts supernumerary for mentoring/ education
• Minimum 3-5 years experience

Direct
Care
RN
High
Acuity &
Specialty
RN
Critical
Care RN
Level 2
Clinician
Level 2
Educator
Level 3
Head
Nurse
Clinical
Nurse
Specialist
Nurse
Practioner
Level 2
ERN*
* Experienced Resource Nurse

How We Got There….
• Work with Unions over 2 years
• Focus groups with stakeholders
• Clear Job Description
• Pilot
• Communication plan

What We Did • Sized the need using relief data from
previous year
• Created master rotations providing smooth
coverage
• Aligned the new grad nurse educator and
program with supporting the ERN team
who then supported new grads

We Measured
Turnover/Retention
Mentorship
Leadership Education
Experience level of relief
Cost of relief
Overtime
Satisfaction
Perception of impact on quality of care

1 year 9+ years
ERNP 2
Reg Pool
Turnover
Experience
Level ERNP 1

New Grad Nurses Hired by Calendar
Year: All VCH by Status

New Grad Nurses hired by calendar year:
Regular Positions for ERN sites

“They travel throughout the hospital and share best
practice with our staff-and what’s going on with other
units.”
“They have really stepped up to the plate with new
projects. They are often willing to help initiate new
projects and get staff engaged. They now know the
units and the idiosyncrasies of the nurses and units
and how to sell things.”
“…often are a good resource on units, especially at night if the team leader is not there. They can often intervene and diffuse potentially volatile situations…”
Fo
cus
Gro
up
Co
mm
en
ts

“We’ve been getting busier and busier on the units. They
may have a very heavy patient workload and can’t
provide much support—it’s a balance.”
“There was a rocky start because there was a lot of
misunderstanding about the role when it first started. There
were misconceptions about what they were doing here. Some
people felt disrespected by the process of bringing in others.”
“I see the value in the ERNPs-but I need to see the results
now. When they were put in place, we wanted them to
reduce overtime by helping to fill short-term needs-not
chronic vacancies. I will be very eager to see the results
financially.”
Fo
cus
Gro
up
Co
mm
en
ts

“The 1st group we hired had 3 years, but it turned out that was
probably not enough-or too narrow, too specialized. It would
have to be a broader background, higher acuity programs”
“They have to be able to think critically and
communications a big thing-especially on nights..and
conflict management.”
“ We need to integrate all the DC2s and ERNs in the hospital so that
they have common goals and common times for coming together to
strategize what we would like them to do.”
Fo
cus
Gro
up
Reco
mm
en
dat
ion
s

Lessons Learned
Involve
Communicate
Ensure Support
Find Champions
Evolve
**Manage Change**


# 1 Issue

Lesson 1: Never Underestimate the Challenge of Change Management in Healthcare


# 2 Issue

Status Relative importance to others; ‘pecking
order’
Certainty Concerns being able to predict the future
Autonomy Provides a sense of control over events
Relatedness A sense of safety with others, of friend
rather than foe
Fairness Perception of fair exchanges between
people
SCARF – brain based model for collaborating with and influencing others (David Rock)
27
Reward Threat


