expanding opportunities caring for older adults kenneth brubaker md, cmd medical director of masonic...
TRANSCRIPT

Expanding Opportunities Caring for Older Adults
Kenneth Brubaker MD, CMD
Medical Director of Masonic Village

Learning Objectives
1. How will the Patient Protection and Affordable Care Act (PPACA) impact your mission?
2. How can you expand your nursing home without walls?
3. Will quality of care and cost of care be the trump cards that dictate your future caring for older adults?
4. What opportunities will you have to improve your bottom line in a competitive market place?

Where are Medicare/Medicaid dollars spent?
• $101 billion dollars are spent on long term care services and supports (about 1/3 of Medicaid spending)
• A decline in three or more ADLs cost 4.5 times more in Medicare spending
• 35% of LTC is privately financed

SCAN Foundation National Poll
• 8 out of 10 Americans support health care reform that includes improved coverage for home and community based long term care services
• 8 out of 10 Americans indicated that health care reform would benefit them
• 8 out of 10 Americans fear that they will not be able to pay for LTC services

Patient Protection and Affordable Care Act (PPACA)
• National insurance for LTC services
• Medicaid options and incentives to expand long term services and supports (LTSS)
• Chronic care coordination
• Nursing home reform

Community Living Assistance Services and Supports (CLASS) ACT
• New voluntary LTSS insurance program federally administered
• Financed by individual enrollees through payroll deductions
• Eliminates pre-existing conditions

Community Living Assistance Services and Supports (CLASS) ACT
• Participation by employers is voluntary
• Employees must participate at least 5 years to be eligible for benefit
• Premiums set by DHHS
Medicaid Options and Incentives to Expand
• Expand Medicaid 1915(c) Home and Community Based Services (HCBS) waivers
• Expand PACE programs (LIFE in PA)
• Other home health and personal assistance under the Medicaid state funding plan

Qualifying for Federal Matching Payments
• Describe state approach to make 3 structural changes in its delivery systems
1. Establish a Single Entry Point System
2. Adopt conflict-free case management
3. Adopt standard assessment tools to
determine eligibility for non-institutional
LTSS
Other Requirement for Federal Participation
• Collect data on service utilization
• Develop core quality measures
• Maintain data on consumer outcomes
• Restricted to eligibility determinations that were in effect in December 31, 2010

The Bottom Line to States
• States that spend less than 25% of their fiscal year 2009 Medicaid LTSS expenditures on non-institutional LTSS will:
• Receive a 5 percentage point increase in Federal Medicaid Assistance Payments (FMAP) between 2011-2015; and
• Are expected to achieve a target of 25% or more Medicaid spending in HCBS by 2015

Community First Choice Option
• Aims to provide financial assistance to Medicaid eligible persons with declines in ADLs/IADLs and require institutional LTSS
• Less restrictions in financial support (i.e. may cover one month’s rent, utility deposits, furniture, etc)
• Help individuals transition from institutional care to the community

Community First Choice Option
• More generous eligibility criteria of up to 300 percent of income threshold for Supplemental Security Income (SSI)
• Option becomes effective on October 1, 2011 for participating states
• States receive 6% increase in the Federal Medicaid Assistance Payments (FMAP)
• States cannot set ceilings on number of persons served.

The Money Follows the Person• Established by the Deficit Reduction
Act in 2005 and to end in 2011
• Extended to 2016
• Reduced institutional length of stay 90 days rather than 180 days

The Money Follows the Person
• July 2010 CMS released 2.25 billion dollars in grant money for Community-based Long-term Care service program in MFP

Other Provisions in the PPACA
• LTSS Workforce
• Aging and Disability Resource Centers
• Chronic Care Coordination (PCP/Transitions of Care)

Other Provisions in the PPACA
• Encourage the concept of Medical Homes
• Pilot Program on Payment Bundling (payment includes cost of care three days before admission and 30 days after the discharge) - begins in 2013

Accountable Care Organizations (ACO)
• Financial incentives to reduce the growth of Medicare expenditures and improve outcomes
• Participants of ACO must be accountable for quality, cost, and overall care of the Medicare fee-for-service beneficiaries assigned to them

Accountable Care Organizations (Cont)
• Should be ready by 2012
• Considered the backbone of the new health care system
• Large health care systems are organizing
• Requires 5000 residents

Nursing Home Reforms• Transparency by increasing availability of
information about the operation of individual nursing homes
• Medicare requirements for cost reports:
1. Number of direct and indirect care staff employed in each position
2. Employee tenure and turnover
Nursing Home Reforms
3. Hours of care provided per resident per day
4. Resident census and case mix data
5. Administrative costs

PPACA - Opportunities & Challenges
• Improving quality of services for the dually eligible (Medicare/Medicaid) community residents
• Expanding services beyond our institutional walls
• Expanding needs for medical services with shrinking reimbursements for care
PPACA-Opportunities & Challenges
• Declining nursing home beds and occupancy of beds
• Hospitals will have a financial penalty for high readmission rates starting 2013
• Hospitals experience longer lengths-of-stays due to nursing homes inability to accept dually eligible (Medicare/Medicaid) residents

STAR Ratings of Not-For-Profit Nursing Homes in Lancaster County
Not-For Profit Rating
3 3 3
4 4 4 4 4 4 4 4 4 4
5 5 5 5 5
0
1
2
3
4
5
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
Rat
ing
Facility

STAR Ratings of For-Profit Nursing Homes in Lancaster County
For Profit Rating
1 1 1 1 1
2
3 3
4 4 4
0
1
2
3
4
5
1 2 3 4 5 6 7 8 9 10 11
Rat
ing
Facility

For Profit Rating
1 1 1 1 1
2
3 3
4 4 4
0
1
2
3
4
5
1 2 3 4 5 6 7 8 9 10 11
Rat
ing
Facility
Not-For Profit Rating
3 3 3
4 4 4 4 4 4 4 4 4 4
5 5 5 5 5
0
1
2
3
4
5
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
Rat
ing
Facility

Percent of Medicaid Beds in Lancaster County in 2008
• Not-for-Profits (19) averaged 40% (range was 28% to 82%)
• For-profits (12) averaged 73% (range was 59% to 91%)

Percent Medicaid Beds for Not-For-Profits and STAR Ratings
Star Rating & Percentage of Not-For-Profit Medicaid Beds 2008
82.0%
64.0%
53.1%51.2%50.2%48.1%45.6%44.5%43.7%43.3%41.2%35.2%33.0%31.0%
28.2%
0.0% 0.0% 0.0%
3
4 4 4
5
4
5
3
4
5
4
5
4
3
5
4 4 4
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
Facility
Per
cen
tag
e
0
1
2
3
4
5
6
Sta
r R
atin
g
% of Medicaid Beds Star Rating
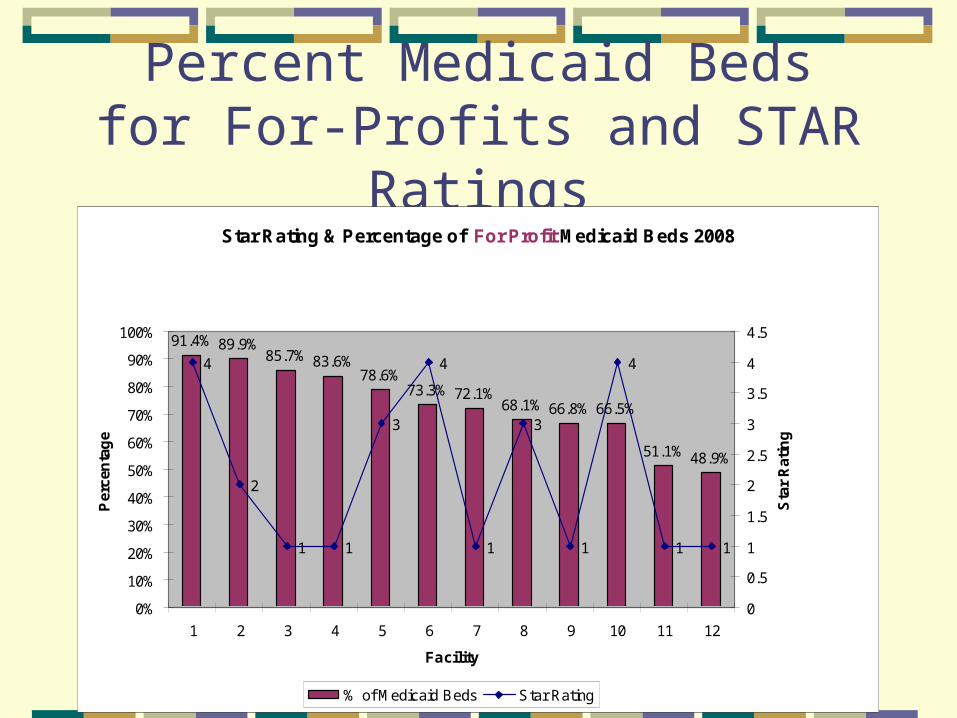
Percent Medicaid Beds for For-Profits and STAR Ratings
Star Rating & Percentage of For Profit Medicaid Beds 2008
91.4% 89.9%85.7% 83.6%
78.6%73.3% 72.1%
68.1% 66.8% 66.5%
51.1% 48.9%
4
2
1 1
3
4
1
3
1
4
1 1
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1 2 3 4 5 6 7 8 9 10 11 12
Facility
Per
cen
tag
e
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
Sta
r R
atin
g
% of Medicaid Beds Star Rating

Star Rating & Percentage of Not-For-Profit Medicaid Beds 2008
82.0%
64.0%
53.1%51.2%50.2%48.1%45.6%44.5%43.7%43.3%41.2%35.2%33.0%31.0%
28.2%
0.0% 0.0% 0.0%
3
4 4 4
5
4
5
3
4
5
4
5
4
3
5
4 4 4
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
Facility
Per
cen
tag
e
0
1
2
3
4
5
6
Sta
r R
atin
g
% of Medicaid Beds Star Rating
Star Rating & Percentage of For Profit Medicaid Beds 2008
91.4% 89.9%85.7% 83.6%
78.6%73.3% 72.1%
68.1% 66.8% 66.5%
51.1% 48.9%
4
2
1 1
3
4
1
3
1
4
1 1
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1 2 3 4 5 6 7 8 9 10 11 12
Facility
Per
cen
tag
e
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
Sta
r R
atin
g% of Medicaid Beds Star Rating

Low Costs and High Quality Will Determine Your Future Success
• “Innovator’s Prescription” (A Disruptive solution for Health Care) by Hwang, Christensen, and Grossman
• “The Cost Conundrum” published in The New Yorker June 2009 by Atul Gawande

As the Hospitals Go, So go the Nursing Homes
• Requiring regular surveys by outside organizations
• Reporting health facility acquired infections
• Reporting Preventable Serious Adverse Events (PSEA)
• Reporting quality indicators/measures
• Reporting cost of care in the future

Opportunities to Improve Your Margins
• Critical mass by local collaborative business models
1. Home care services
2. Hospice services
3. Limited medical staff
4. At risk contracts with dually eligible Medicare/Medicaid

Opportunities to Improve Your Margins (cont)
5. Pharmacy
6. Physical Therapy
7. Expanding your endowment

Masonic Village Home Care ServicesProjected vs Actual Billable Hours
Projected vs Actual Billable Hours
0
500
1000
1500
2000
2500
Ho
urs
Projected Hours
Actual Hours
Masonic Village Home Care ServicesQuality
• First year satisfaction surveys showed 88 respondents rated services excellent or above average, and 11 respondents rated service average. No question was rated poor or very poor, and all feedback was positive.

Masonic Village Home Care ServicesFinancials
• Projected to show revenue over expenses in 12th month, break even in 19th month
• Showed revenue over expenses in 7th month, broke even in 11th month

Hospice Services
• Critical mass for hospice care in your facility/community
• Excellent family satisfaction
• Continuum of care for residents
• Recover your costs of quality end-of-life care

Hospice Services
• Opportunity to generate gifts of appreciation by families
• Expertise in end-of-life care

Figure 1. COMPARISON OF SCORES
8.609.05 9.00
9.47
8.60
9.30
8.73
9.36 9.28 9.46
8.939.30
0.00
1.00
2.00
3.00
4.00
5.00
6.00
7.00
8.00
9.00
10.00
Communication Respect Symptom Control Die w ith Dignity Family Emotional Support Overall Satisfaction
Note: No statiscally significant difference in any area of satisfaction
Fig
ure
1
Nsg. Home Pallative Care Nursing Home & Hospice
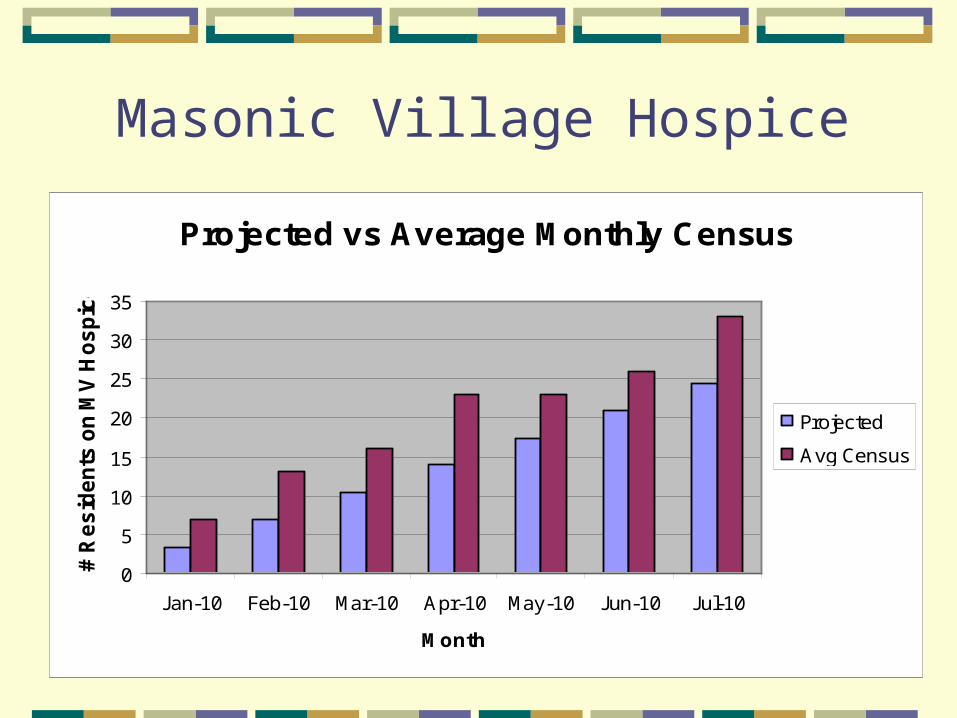
Masonic Village Hospice
Projected vs Average Monthly Census
0
5
10
15
20
25
30
35
Jan-10 Feb-10 Mar-10 Apr-10 May-10 Jun-10 Jul-10
Month
# R
es
ide
nts
on
MV
Ho
sp
ice
Projected
Avg Census

Masonic Village Hospice Financials
• Projected to show revenue over expenses in 9th month, break even in 19th month
• Showed revenue over expenses in 6th month, broke even in 10th month

Masonic Village Hospice Gifts
• To date we have received 75 hospice gifts totaling $8,650 in donations
• Planning 2 gift giving programs around the holiday season
• Volunteer additions account for 13% total hospice staff

Limited Provider Staff Model
• Improve quality of care
• Reduce cost of care
• Require core competencies of care
• Better resident satisfaction
• Increase availability
• Reduction of readmissions to hospital

At risk Medicare/Medicaid Contracts
• Increased reimbursement for caring for residents in their home
• Decreased emergency room visits and hospitalization
• Improved quality of care
• Increase availability of provider staff


“Never doubt that a small group of thoughtful, committed citizens can change the world; indeed, it’s the only thing that ever has.”
- by Margaret Mead

The Parable of the Talents in Matthew 25
“The master replied to the servant who received 5 talents and brought back 5 more, ‘Well done, good and faithful servant! You have been faithful with a few things; I will put you in charge of many things’.”