expanding health coverage to informal workers in usaid priority countries
TRANSCRIPT

Abt Associates Inc.In collaboration with:
Broad Branch Associates | Development Alternatives Inc. (DAI) | Futures Institute | Johns Hopkins Bloomberg School of Public Health (JHSPH)| Results for Development Institute (R4D) | RTI International | Training Resources Group, Inc. (TRG)
January 29, 2017
Sharon Nakhimovsky, Onaopemipo Abiodun,
Adam Koon (presenter), and Altea Cico
Expanding Health Coverage toInformal Workers in USAID PriorityCountries

Ending Preventable Child and MaternalDeaths (EPCMD) countries
2
EPCMD Countries
Afghanistan Mozambique
Bangladesh Myanmar
Democratic Republic of the Congo Nepal
Ethiopia Nigeria
Ghana Pakistan
Haiti Rwanda
India Senegal
Indonesia South Sudan
Kenya Tanzania
Liberia Uganda
Madagascar Yemen
Malawi Zambia
Mali
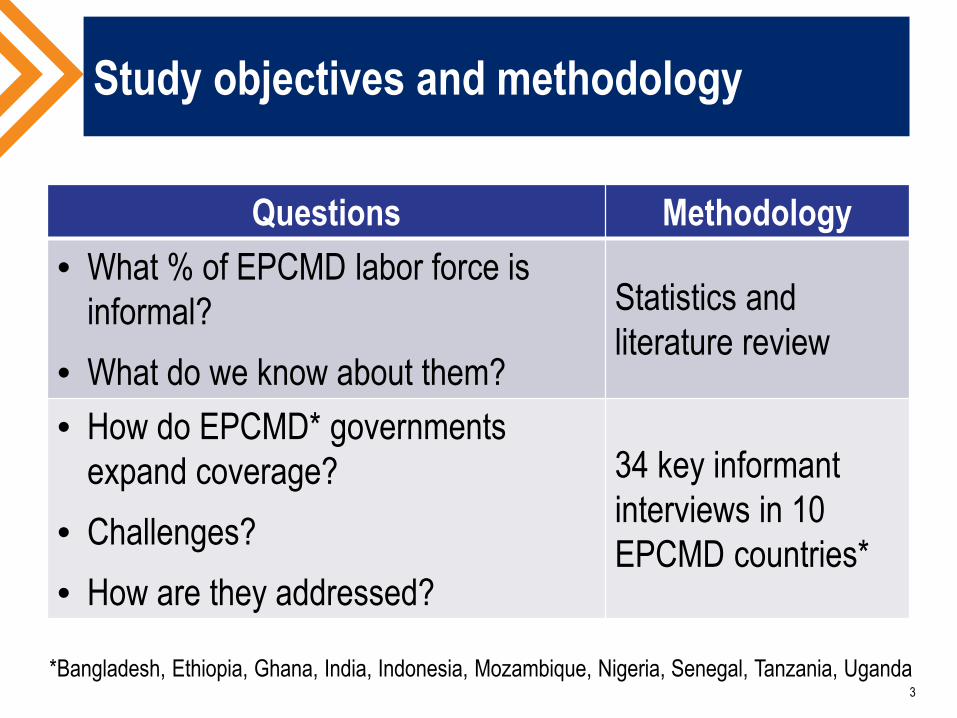
Study objectives and methodology
Questions Methodology
• What % of EPCMD labor force isinformal?
• What do we know about them?
Statistics andliterature review
• How do EPCMD* governmentsexpand coverage?
• Challenges?
• How are they addressed?
34 key informantinterviews in 10EPCMD countries*
3
*Bangladesh, Ethiopia, Ghana, India, Indonesia, Mozambique, Nigeria, Senegal, Tanzania, Uganda
Who are informal workers?
4
People of working age whose job does not provide them withlegal social protection.
Source: International Labor Organization 2003
Ho
useh
old
inco
me
Poo
rV
ulne
rabl
eN
on-p
oor,
non-
vuln
erab
le
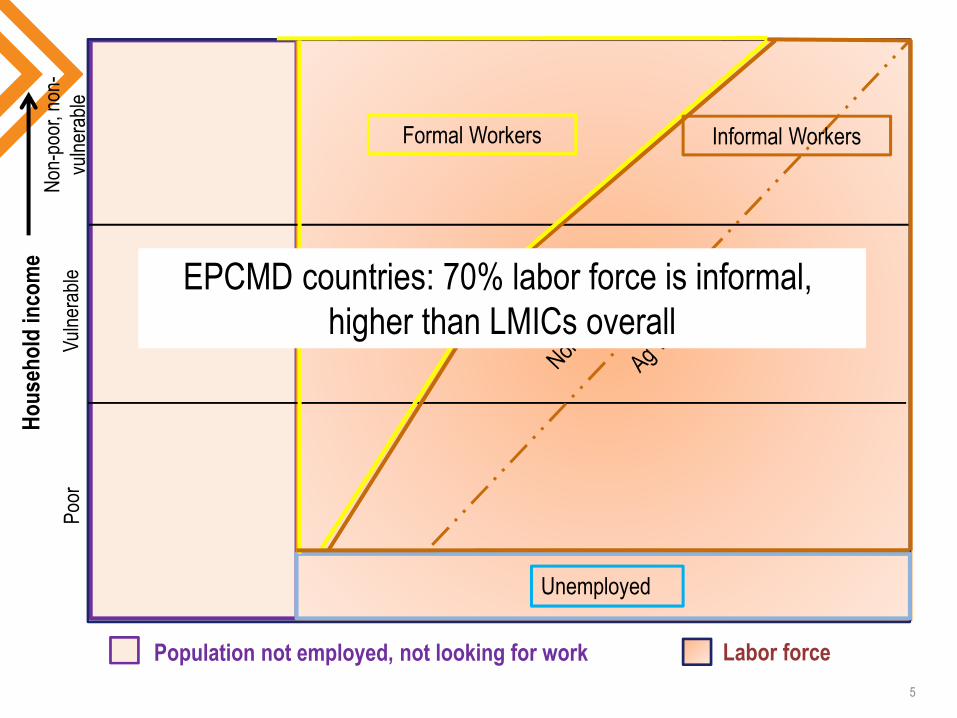
Unemployed
Formal Workers Informal Workers
Labor forcePopulation not employed, not looking for work
5
EPCMD countries: 70% labor force is informal,higher than LMICs overall
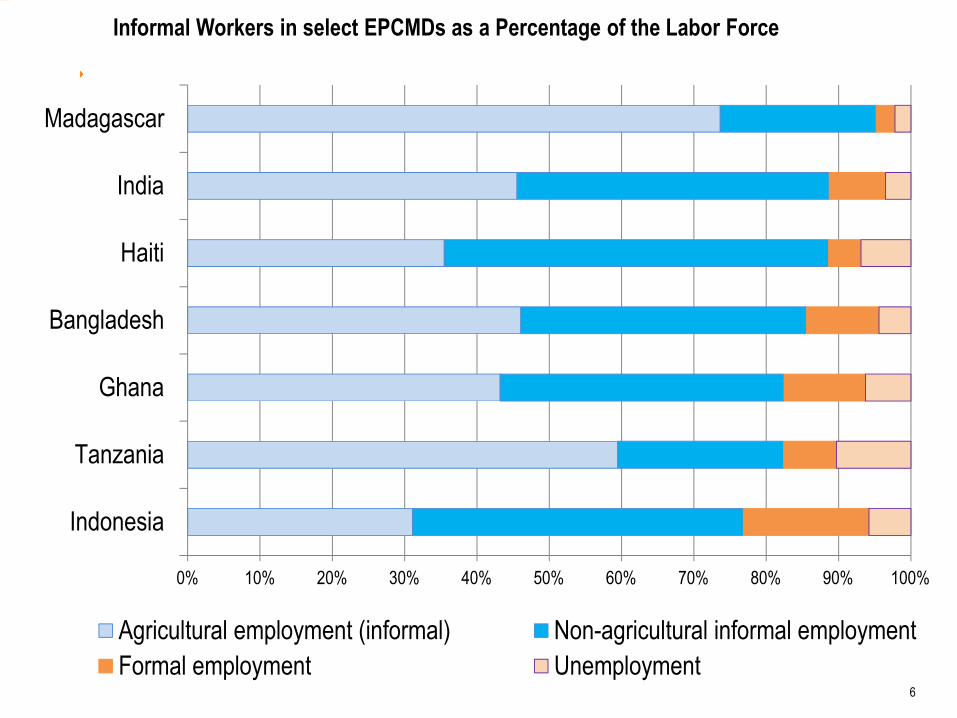
Informal Workers in select EPCMDs as a Percentage of the Labor Force
6
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Indonesia
Tanzania
Ghana
Bangladesh
Haiti
India
Madagascar
Agricultural employment (informal) Non-agricultural informal employment
Formal employment Unemployment

Improving micro-level operations to expandcoverage for informal workers
Demand-side:
Use labor groups to reachmembers
Easier payment options
Supply-side:
Keep health facilities open later
More facilities in rural areas
Expanded outreach
7

Good governance builds on small schemes
Isolated “grassroots”community schemes notsustainable or scalable
Policy actions
Tax subsidy
Consolidated beneficiarycontributions
Professionalizing schememanagement
8
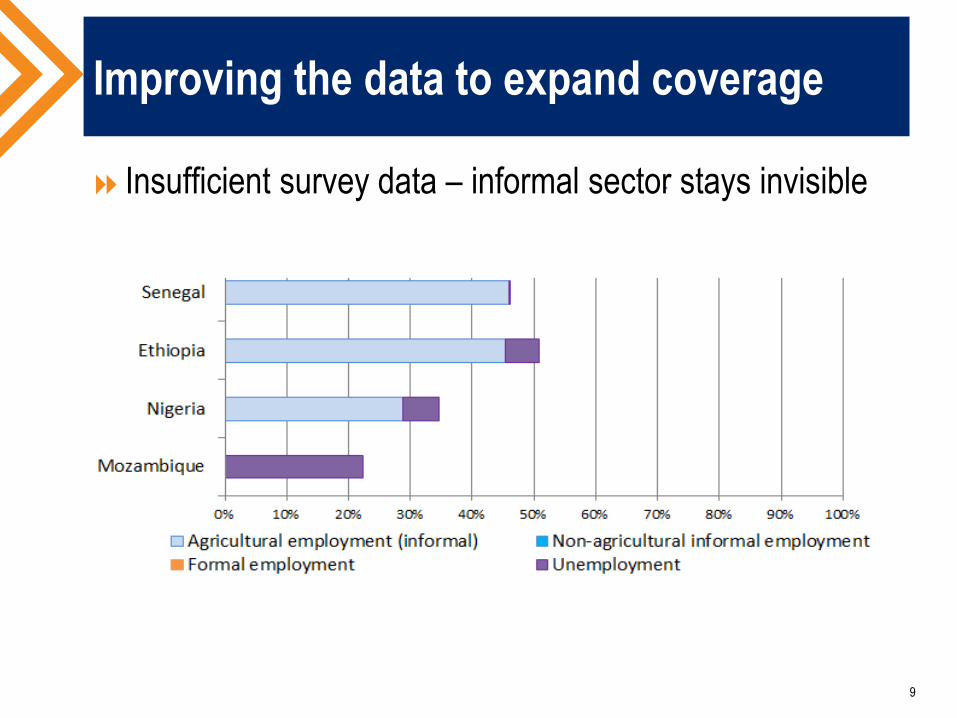
Improving the data to expand coverage
9
Insufficient survey data – informal sector stays invisible

Informal/formal dichotomy in UHC dialogue
Moving beyond ‘informality’
SHI legacy countries
Free care legacy countries
Incremental approachesbeginning with the poor
10

Key takeaways
Progress towards UHC requires covering informal workers
EPCMD countries have MORE informal workers
No silver bullet
Policy solutions shaped by the past
Informal workers less visible and influential on public policy
Looking ahead
Better data on informal workers
Informed long term policy
Micro-level operational improvements
Targeting subgroups to expand coverage incrementally
11
THANK YOU!
12
All Study Participants, Laurel Hatt, RicardoBitran, USAID: Scott Stewart and Jodi Charles
Photos courtesy of Photoshare and A. Koon
Please see full report on our website:
www.hfgproject.org