exercise prescription for obese patient - fms conference...exercise prescription for obese patients....
TRANSCRIPT
EXERCISE PRESCRIPTION FOR OBESE PATIENT
ASSOC. PROF. DR. MOHD NAHAR AZMI MOHAMED
HEAD,
SPORTS MEDICINE DEPARTMENT
SENIOR MEDICAL LECTURER / CONSULTANT SPORTS PHYSICIAN
UNIVERSITI MALAYA MEDICAL CENTER

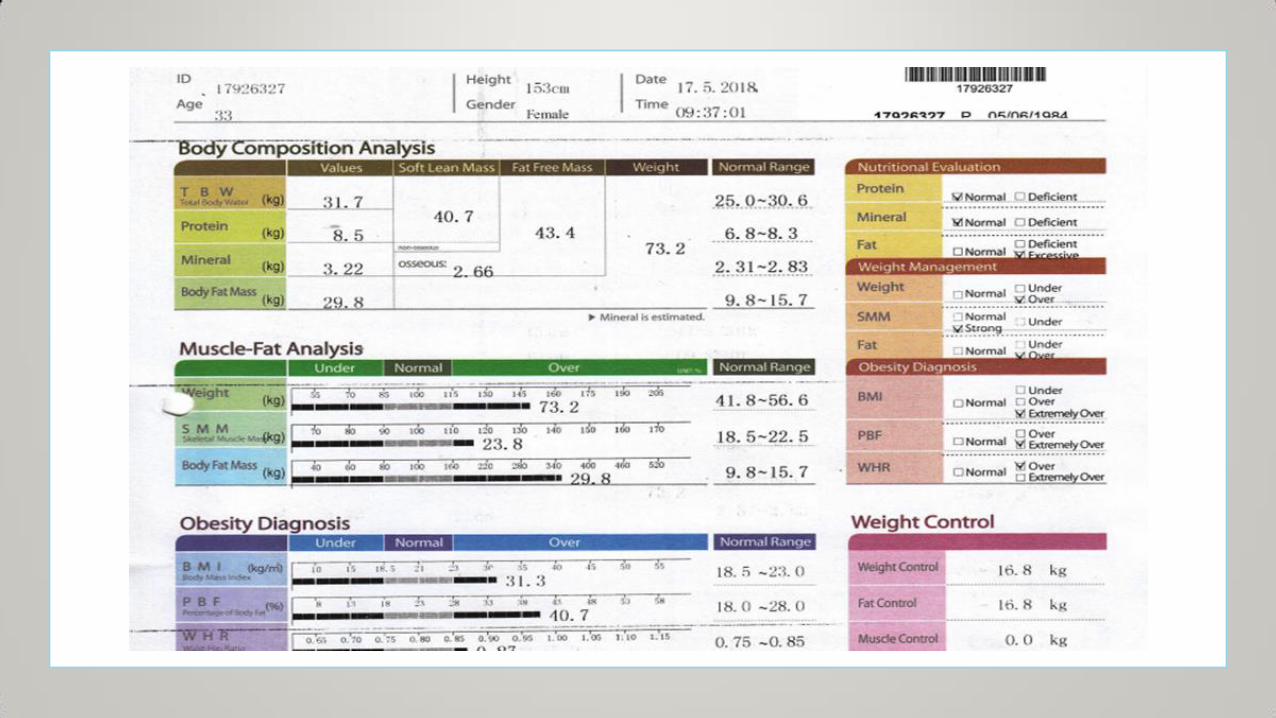
OBESITY AND EXERCISE
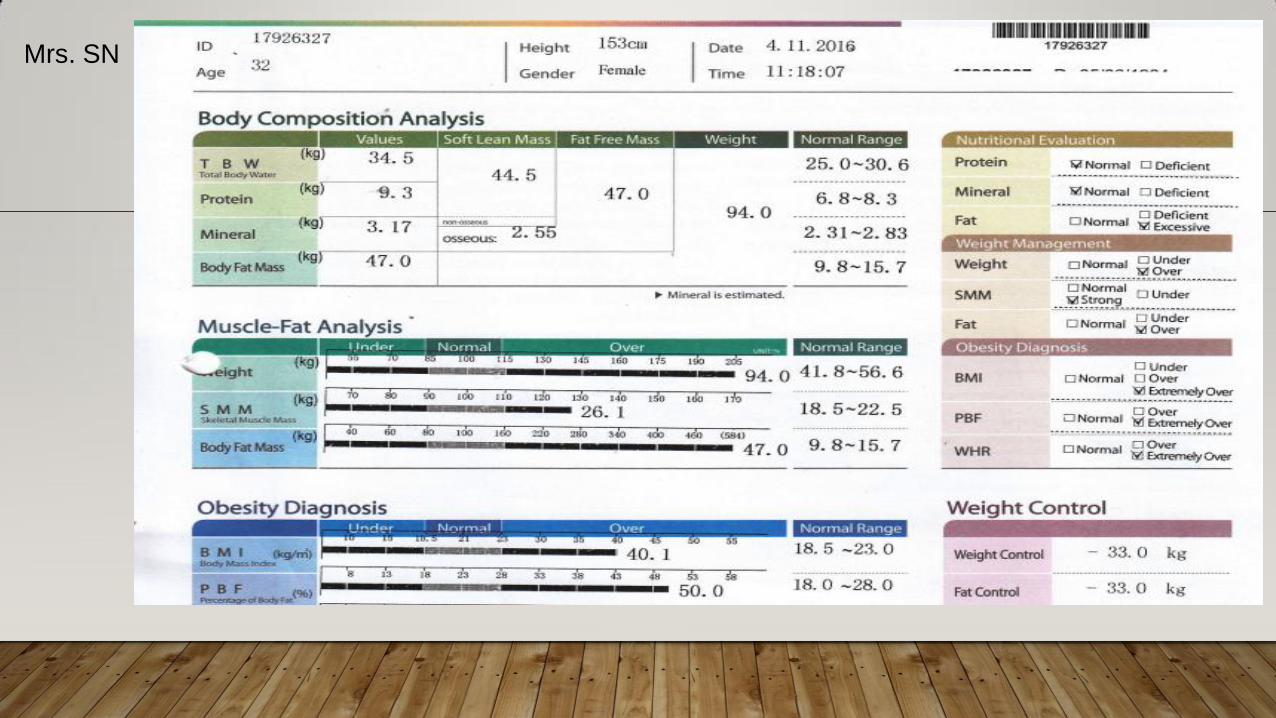
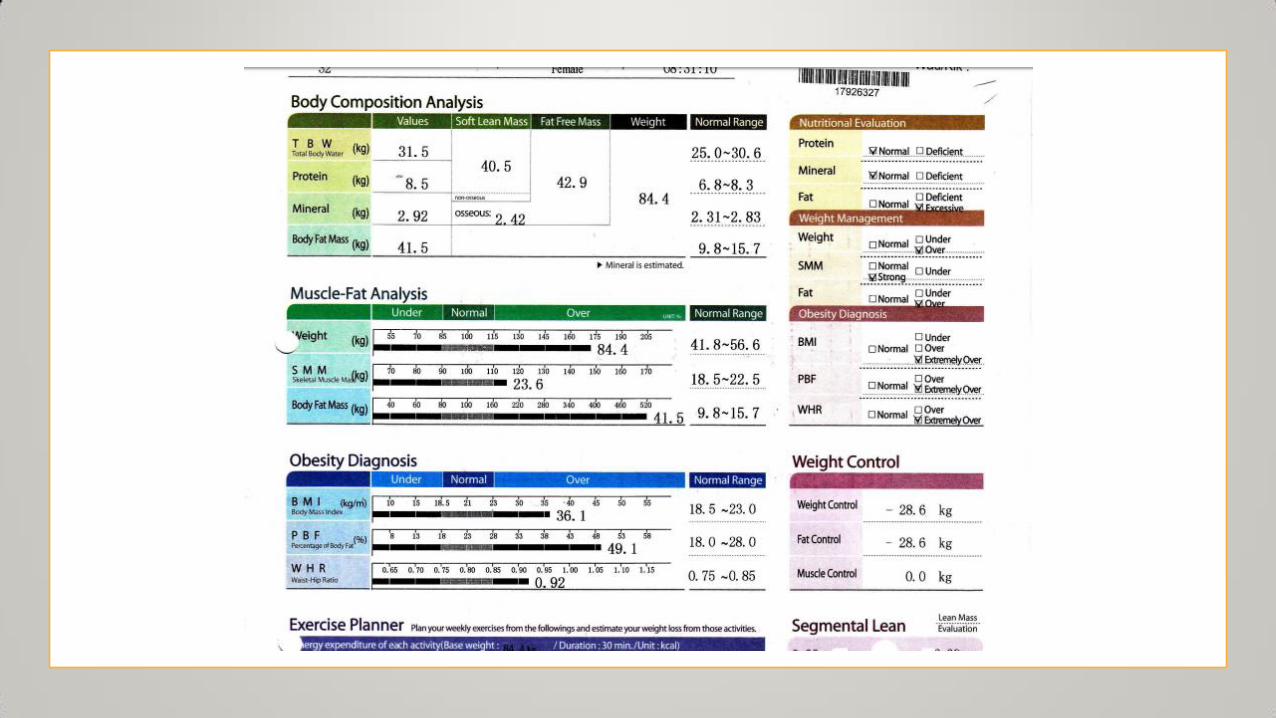
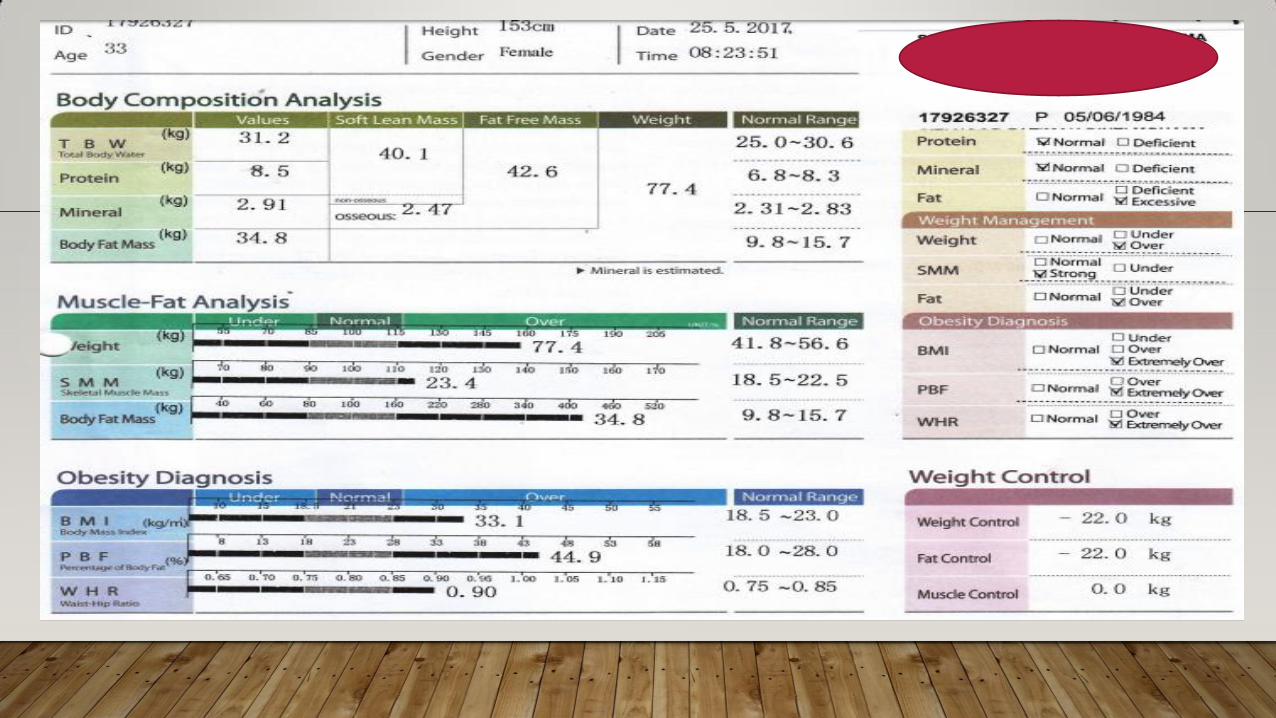
Mrs. SN
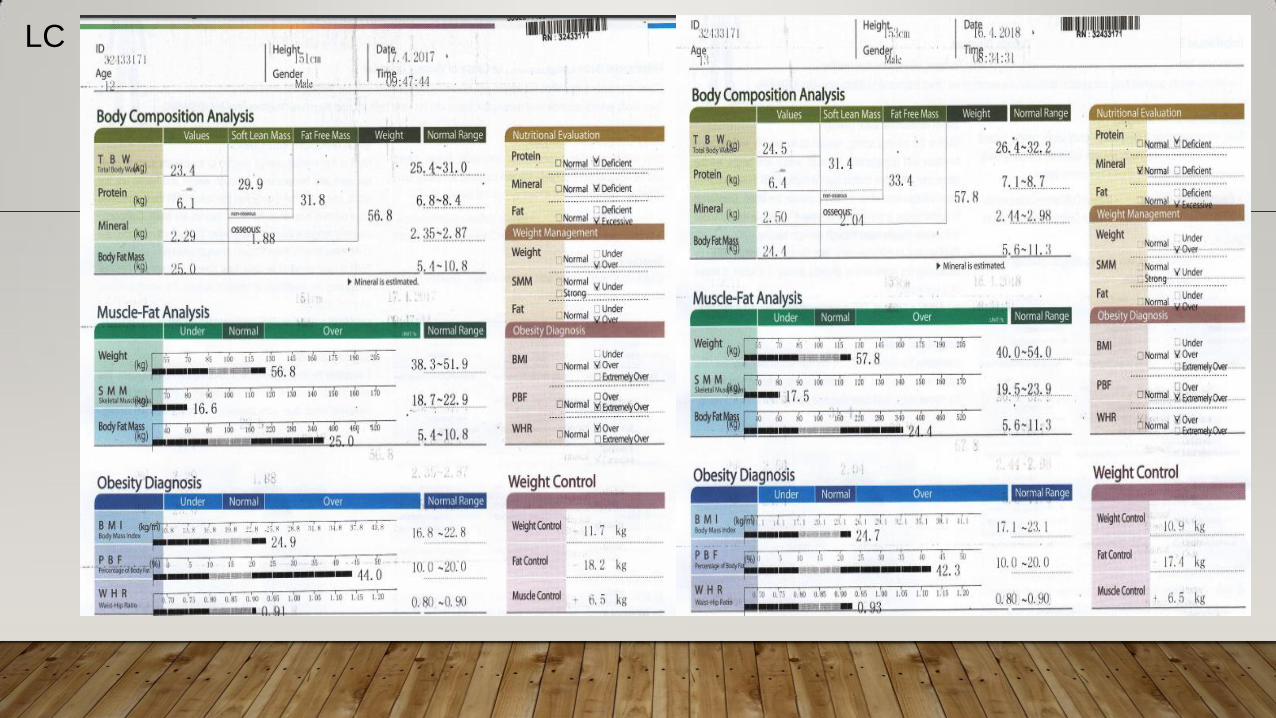
LC
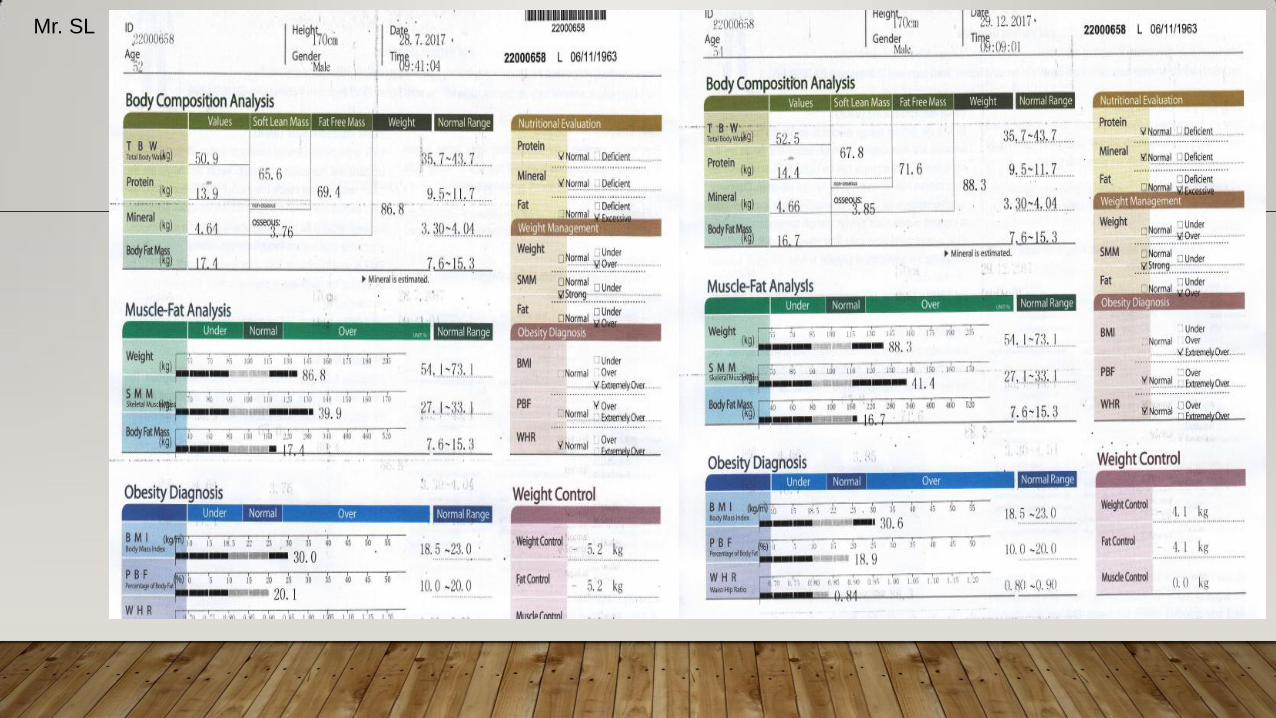
Mr. SL
EXERCISE METABOLISM
EXERCISE METABOLISM
• Skeletal muscle comprises ∼40% of total body mass in mammals and
accounts for ∼30% of the resting metabolic rate in adult humans
(Zurlo et al., 1990).
• Skeletal muscle has a critical role in glycemic control and metabolic
homeostasis and is the predominant (∼80%) site of glucose disposal under
insulin-stimulated conditions
(DeFronzo et al., 1981).
10
EXERCISE METABOLISM
• Skeletal muscle is the largest glycogen storage organ, with/having ∼4-fold the
capacity of the liver.
• A single bout of acute exercise improves whole-body insulin sensitivity for up
to 48 hr after exercise cessation
(Mikines et al., 1988; Koopman et al., 2005)
11
EXERCISE METABOLISM
• Skeletal muscle is the principal contributor to exercise-induced changes in metabolism.
• Maximal exercise can induce a 20-fold increase in whole-body metabolic rate over resting
values, whereas the ATP turnover rate within the working skeletal muscle can be more
than 100-fold greater than at rest.
(Gaitanos et al., 1993)
12
EXERCISE METABOLISM
• Skeletal muscle is richly endowed with mitochondria and heavily reliant on oxidative
phosphorylation for energy production.
• During strenuous exercise, dramatic (>30-fold) increases in intramuscular oxygen consumption
and local blood flow occur
(Andersen and Saltin, 1985; Gibala et al., 1998)
• Skeletal muscle is the primary site for CHO and lipid metabolism for energy production.
13
EXERCISE METABOLISM
• At low-to-moderate intensities of exercise, the primary fuel sources supplying skeletal muscle
are glucose, derived from hepatic glycogenolysis (or gluconeogenesis) or oral ingestion, and
free fatty acids (FFAs) liberated by adipose tissue lipolysis.
(van Loon et al., 2001).
14
EXERCISE METABOLISM
• Exercise intensity increases, muscle utilization of circulating FFAs declines modestly, whereas
utilization of circulating glucose increases progressively up to near-maximal intensities
(van Loon et al., 2001).
• This coincides with increasing absolute rates of CHO oxidation and relative contribution to
energy provision, with a majority of energy at high intensities of exercise being provided by
muscle glycogen
15
EXERCISE METABOLISM
• Muscle glycogen is the predominant CHO source during moderate to intense exercise,
and the rate of degradation (glycogenolysis) is proportional to the relative exercise
intensity
(Romijn et al., 1993).
16
EXERCISE METABOLISM
• After the cessation of exercise, the metabolic rate declines but remains slightly elevated (<10%) for
up to 24 hr.
Børsheim and Bahr, 2003
17
VO2 Peak/VO2max
Cardio Pulmonary Exercise Test
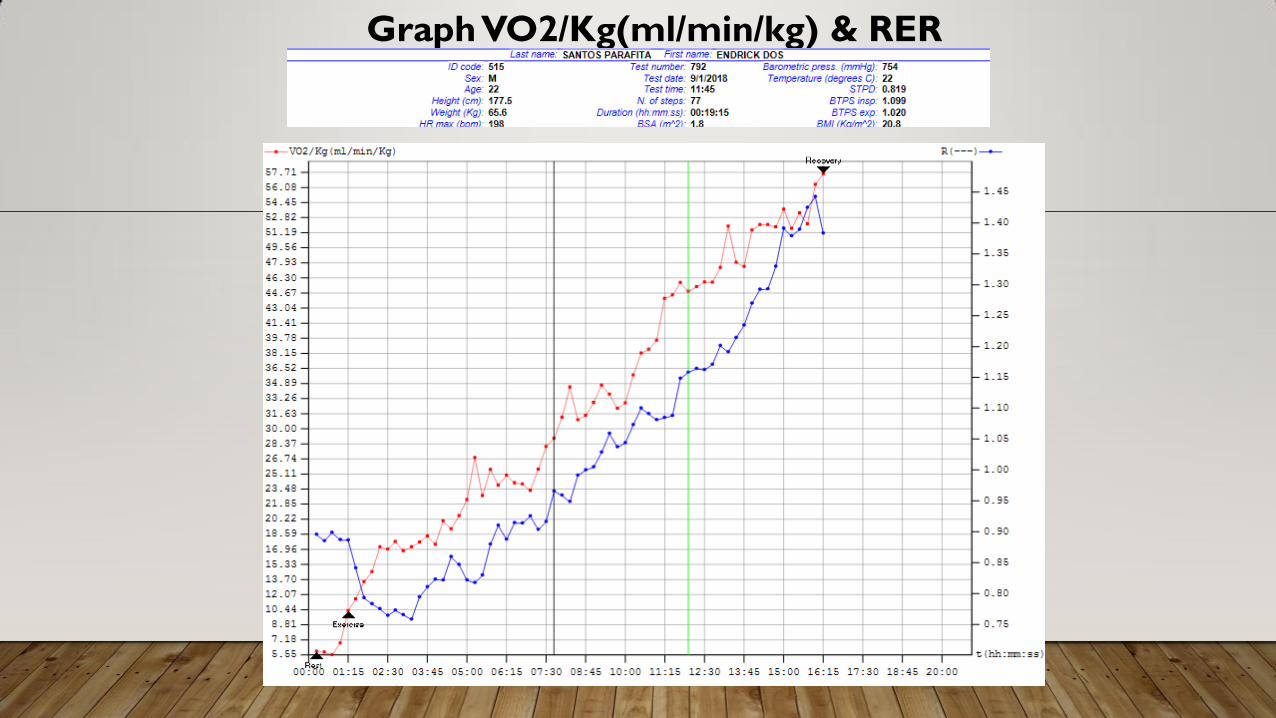
Graph VO2/Kg(ml/min/kg) & RER
/ t
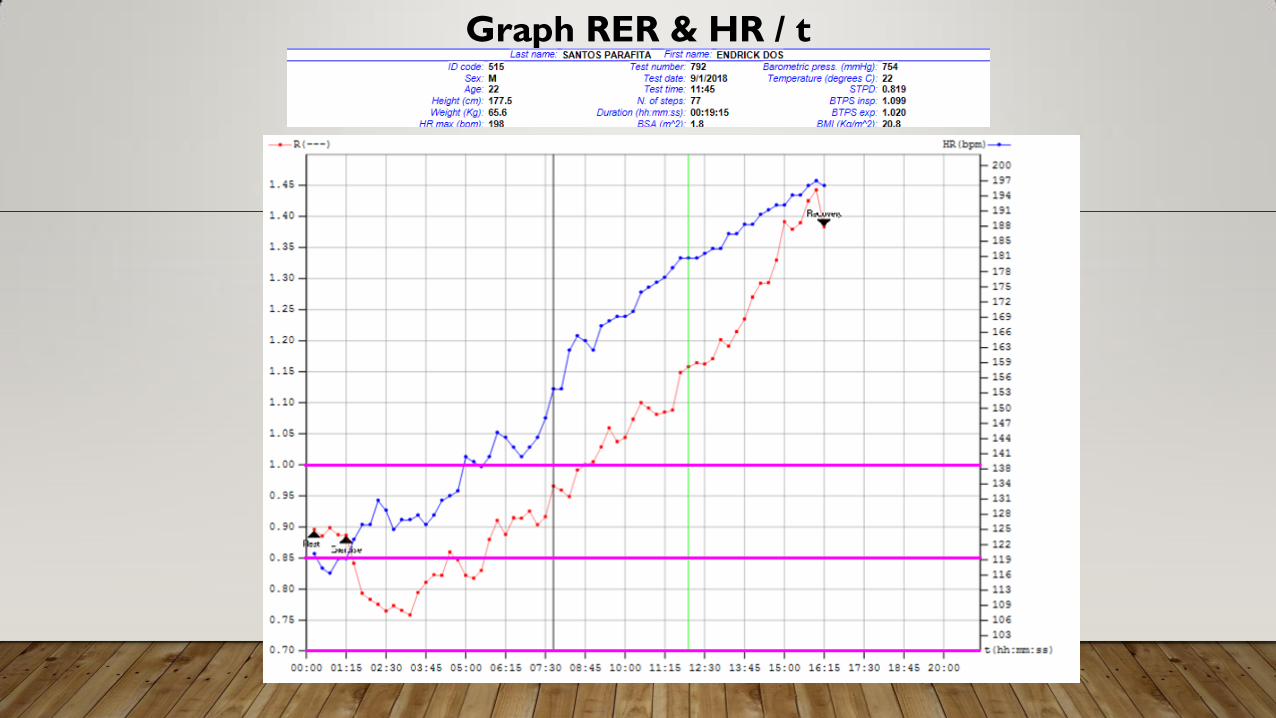
Graph RER & HR / t
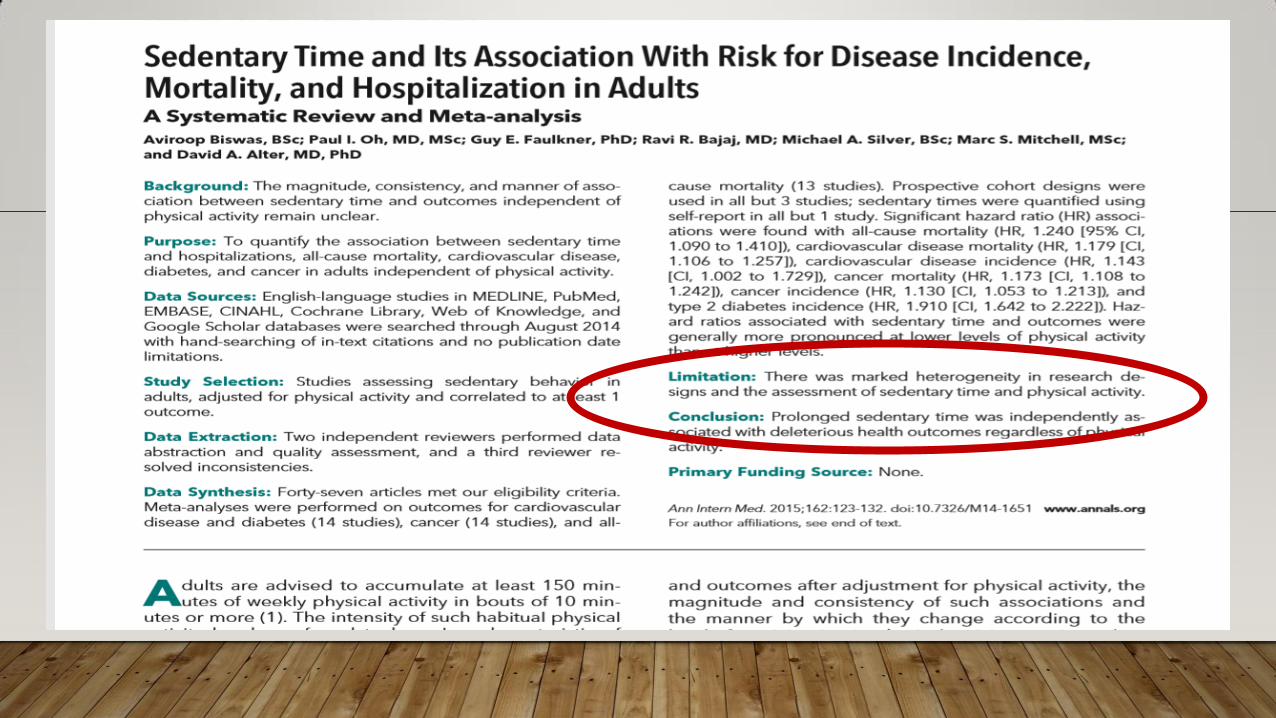
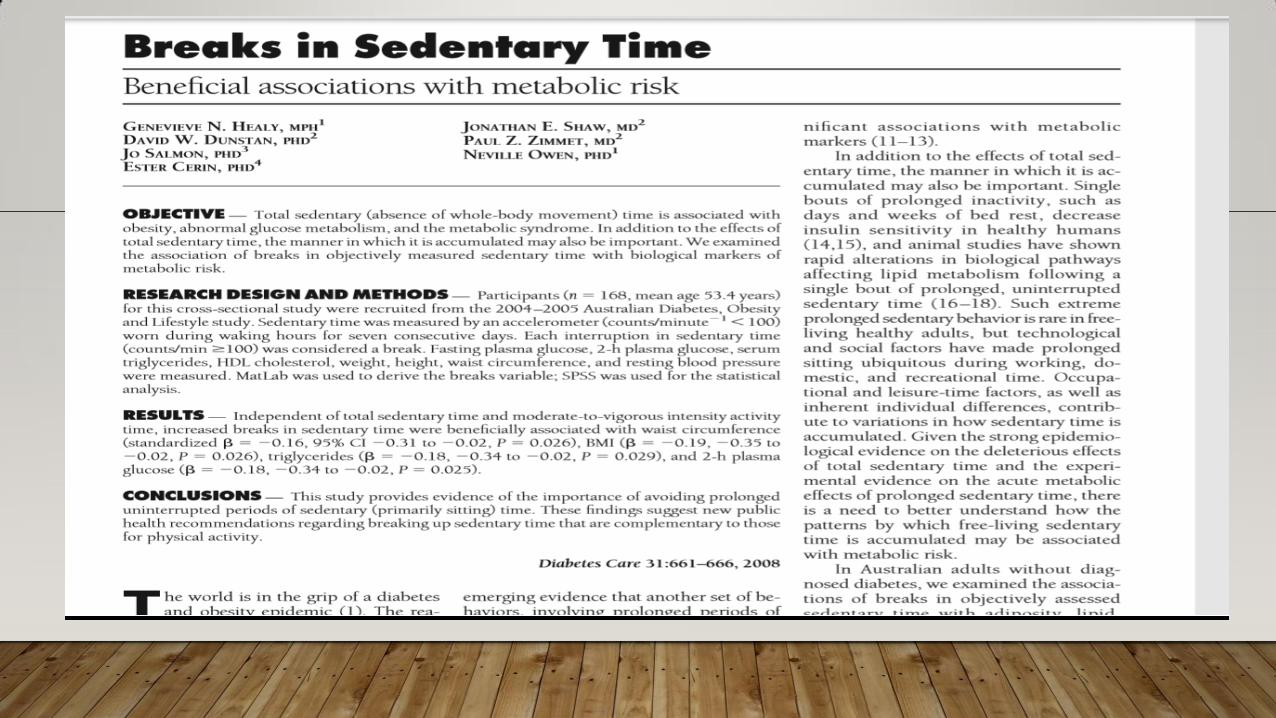
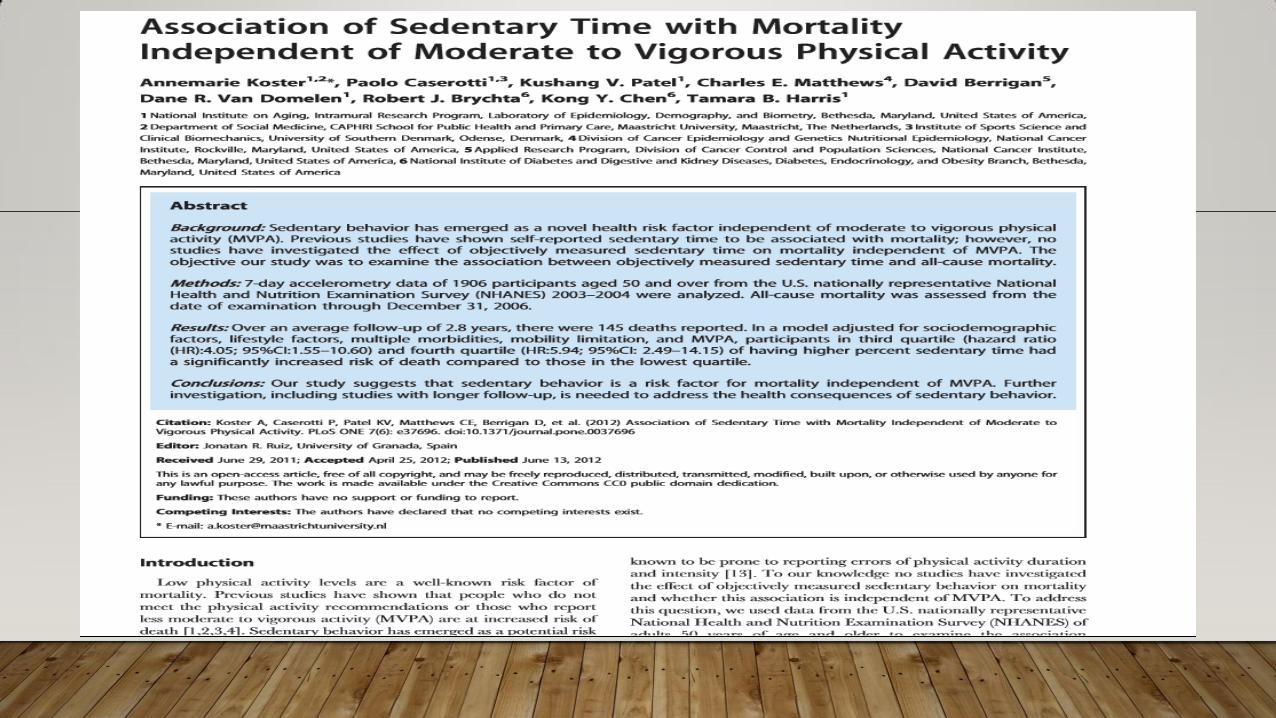
SEDENTARY BEHAVIOUR AND HEALTH
• Prolonged periods of sitting or sedentary behaviour are
associated with deleterious health consequences independent
of Physical Activity level.
• Sedentary time was also associated with a 30% lower relative
risk for all cause mortality among those with high level of PA with
those with low level of PA.
Balady GJ et. al. Circulation 2004; 110(14):1920-5
THE GENERAL PRINCIPAL OF F.I.T.T.
•F – Frequency
• I – Intensity
•T – Type
•T – time
•E - Enjoyment
•P - Progression
• One of the most important components of a properly designed training
program is that it must be
Enjoyable.
ENJOYMENT
• The amount of pleasure derived from the activity by the person.
• Often overlooked component of program
• The program and its activities must coincide with the personality, likes, and
dislikes of the person.
• This ultimately translates into compliance.
Modified according to an individual’s habitual physical activity, physical function,
health status, exercise responses, and stated goals.
EXERCISE PRESCRIPTION FOR OBESE PATIENTS
EXERCISE PROGRAM FOR THE OBESE
• A weight loss of 5%–10% provides significant health benefits,
and these benefits are more likely to be sustained through
the maintenance of weight loss and/or participation in
habitual physical activity.
• Weight loss maintenance is challenging, with weight regain
averaging approximately 33%–50% of initial weight loss
within 1 yr of terminating treatment.
ACSM, 2014
• Lifestyle interventions for weight loss that combine reductions in energy
intake with increases in EE through exercise and other forms of physical
activity typically result in an initial 9%–10% reduction in body weight.
• Physical activity appears to have a modest impact on the magnitude of
weight loss observed across the initial weight loss intervention compared
with reductions in energy intake.
• The combination of moderate reductions in energy intake with adequate
levels of physical activity maximizes weight loss in individuals with
overweight and obesity.
ACSM, 2014
• Pre-participation assessment needed,
• Current level of fitness,
• Blood pressure and other observations,
• ECG was requested as a baseline.
• Exercise stress test.
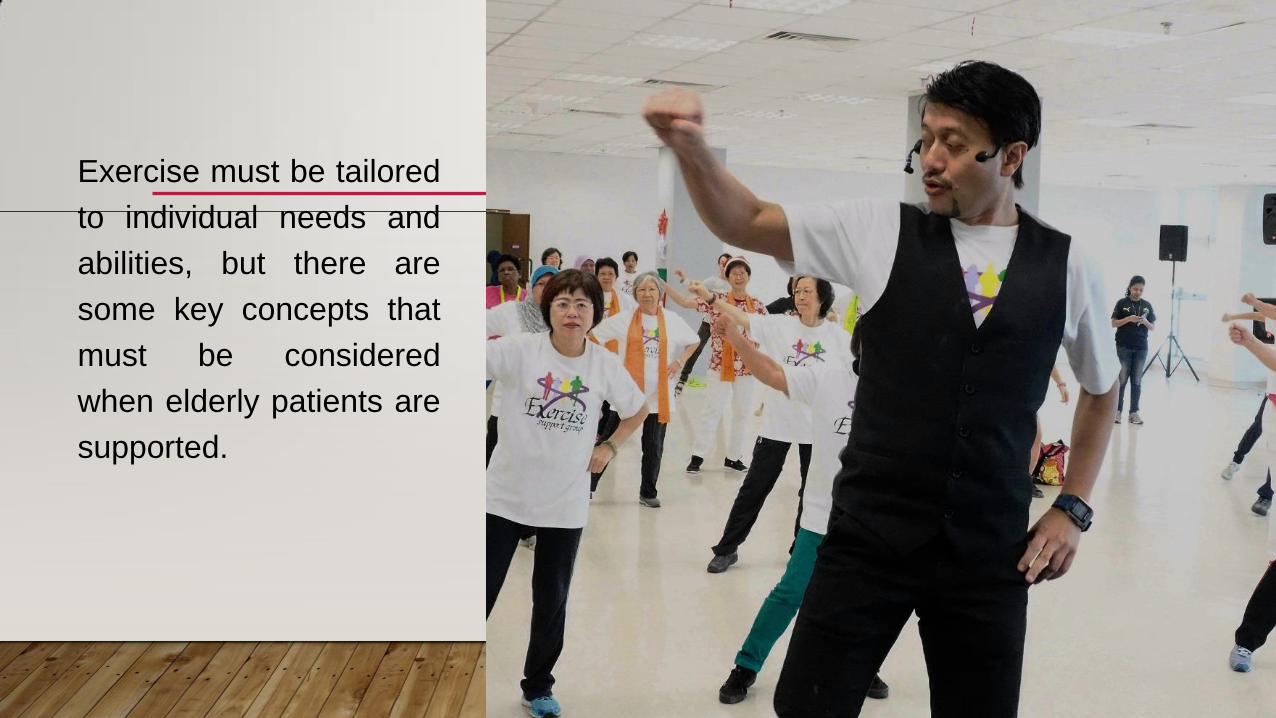
Exercise must be tailored
to individual needs and
abilities, but there are
some key concepts that
must be considered
when elderly patients are
supported.
THE TYPE OF EXERCISE
• Aerobic exercise
• Muscle function and strength training
• Balance and flexibility
EXERCISE PRISCRIPTION FOR THE OBESE PATIENTS
Physical activity obviously boosts the energy expenditure. However, the human body is extremely energy
efficient. Losing weight by merely increasing physical activity is very difficult in practice. Many overweight
and obese individuals also find it difficult to move around because of the mechanical load, risk of injury.
One important positive effect of physical activity is an increase in muscle mass and subsequent
improvement in the basal metabolic rate. A large muscle mass improves the chances of maintaining a
high level of energy expenditure. The muscle mass can only be increased through physical activity while
the volume of fatty tissue can grow without limit through constant overconsumption
44
• Education into the benefits of physical activity should be commenced from the initial
consultation
• Education should also include red flags and when to seek help
• Allowing time between consultations can be useful to help understanding
• Screening for red flag symptoms is important to ensure safety and tailor physical activity
to ability
EXERCISE PROGRAM FOR THE OBESE
• Understand the level of Physical Activity/Exercise
• No matter how small, is better than sitting
• The good news is that accumulated daily physical activities count
towards our overall energy expenditure.
46
EXERCISE PROGRAM FOR THE OBESE
• 1) There is clear evidence for a dose-response relationship between physical activity and weight loss.
The more you put in the more you will “get out”.
• 2) Obesity is one of only a few medical conditions that can be completely reversed by undertaking
physical activity
James Thing, Exercise Prescription in Health and Disease
47
Considerations
• when helping patients take up physical activity are the frequency, intensity, type and duration of the training. Patients with joint pathologies may experience pain due to their weight and the sudden change in activity levels; this may feedback negatively on their ambitions.
• Therefore it is sensible to commence with non-weight bearing activity initially and minimise the impact on joints.
EXERCISE PROGRAM FOR THE OBESE 49
• F – Frequency
• I – Intensity
• T – Type
• T – time
• E - Enjoyment
• P - Progression
FITT RECOMMENDATIONS FOR INDIVIDUALS WITH OVERWEIGHT AND OBESITY
Frequency: ≥5 d ∙ wk−1 to maximize caloric expenditure.
Intensity: Moderate-to-vigorous intensity aerobic activity should be encouraged. Initial exercise training intensity should be moderate
(i.e., 40%–<60% VO2R or HRR). Eventual progression to more vigorous exercise intensity (i.e., ≥60% VO2R or HRR) may result in
further health/fitness benefits.
Time: A minimum of 30 min ∙ d−1 (i.e., 150 min ∙ wk−1) progressing to 60 min ∙ d−1 (i.e.,
300 min ∙ wk−1) of moderate intensity, aerobic activity.
Incorporating more vigorous intensity exercise into the total volume of exercise may provide additional health benefits. However,
vigorous intensity exercise should be encouraged in individuals who are both capable and willing to exercise at a higher than moderate
intensity levels of physical exertion with recognition that vigorous intensity exercise is associated with the potential for greater injuries.
Accumulation of intermittent exercise of at least 10 min is an effective alternative to continuous exercise and may be a particularly
useful way to initiate exercise.
Type: The primary mode of exercise should be aerobic physical activities that involve the large muscle groups. As part of a balanced
exercise program, resistance training and flexibility exercise should be incorporated
. .
ACSM, 2014
WEIGHT LOSS MAINTENANCE SPECIAL CONSIDERATIONS
• Adults with overweight and obesity may benefit from progression to
approximately >250 min ∙ wk−1 because this magnitude of physical
activity may enhance long-term weight loss maintenance.
• Adequate amounts of physical activity should be performed on 5–7 d ∙
wk−1.
• The duration of moderate-to-vigorous intensity, physical activity should
initially progress to at least 30 min ∙ d−1 and when appropriate progress
to >250 min ∙ wk−1 to enhance long-term weight management.
ACSM, 2014
WEIGHT LOSS MAINTENANCE SPECIAL CONSIDERATIONS (CONT.)
• Individuals with overweight and obesity may accumulate this
amount of physical activity in multiple daily bouts of at least 10
min in duration or through increases in other forms of moderate
intensity lifestyle physical activities.
• Accumulation of intermittent exercise may increase the volume
of physical activity achieved by previously sedentary individuals
and may enhance the likelihood of adoption and maintenance
of physical activity.
ACSM, 2014
WEIGHT LOSS MAINTENANCE SPECIAL CONSIDERATIONS
• The addition of resistance exercise to energy restriction does not
appear to prevent the loss of fat-free mass or the observed
reduction in resting EE.
• However, resistance exercise may enhance muscular strength and
physical function in individuals with overweight and obesity.
Moreover, there may be additional health benefits of participating in
resistance exercise such as improvements in CVD and DM risk
factors and other chronic disease risk factors.
ACSM, 2014
WEIGHT LOSS PROGRAM RECOMMENDATIONS
• Target a minimal reduction in body weight of at least 5%–10% of
initial body weight over 3–6 mo.
• Incorporate opportunities to enhance communication between
health care professionals, dietitians, and health/fitness and clinical
exercise professionals and individuals with overweight and obesity
following the initial weight loss period.
• Target changing eating and exercise behaviors because sustained
changes in both behaviors result in significant long-term weight loss.
ACSM, 2014
WEIGHT LOSS PROGRAM RECOMMENDATIONS
• Target reducing current energy intake by 500–1,000 kcal ∙ d−1 to
achieve weight loss. This reduced energy intake should be
combined with a reduction in dietary fat to <30% of total energy
intake.
• Progressively increase to a minimum of 150 min ∙ wk−1 of
moderate intensity, physical activity to optimize health/fitness
benefits for adults with overweight and obesity.
WEIGHT LOSS PROGRAM RECOMMENDATIONS
• Progress to greater amounts of physical activity (i.e., >250 min ∙
wk−1) to promote long-term weight control.
• Include resistance exercise as a supplement to the combination of
aerobic exercise and modest reductions in energy intake to lose
weight.
• Incorporate behavioral modification strategies to facilitate the
adoption and maintenance of the desired changes in behavior
57 EXERCISE PROGRAM FOR THE OBESE

EXERCISE PROGRAM FOR THE OBESE
• Special Consideration
• The presence of other comorbidities may increase the risk stratification for obese
individuals, resulting in the need for additional medical screening before exercise
• The presence of musculoskeletal and/or orthopedic conditions may require
modifications to the exercise program that may require the need for non weight
bearing exercise (leg or arm ergometry), or other form of upper body
resistance/endurance type of exercise.
59
OBESE WITH COMORBIDITY SPECIAL CONSIDERATIONS.
• Alternatively, begin with the FITT that is the most conservative FITT prescribed for the
multiple diseases, health conditions, and/or CVD risk factors the client and patient
present with.
• Know the magnitude and time course of response of the various health outcome(s) that
can be expected as a result of the FITT principle of Ex Rx in order to progress the client
and patient safely and appropriately.
• Frequently monitor signs and symptoms to ensure safety and proper adaptation and
progression.
TAKE HOME MESSAGE
• Exercise Program for Obese
• Physical Activity/Exercise History
• Understand individual Comorbidities
• Exercise is tailored for each individual
• Do it within individual limits
• Gradually progress the level of intensity.
• A combination of cardiovascular, resistance and proprioceptive exercises are suitable when
addressing confidence in physical activity
• Regular contact supports the patient and enables monitoring of progress
• Community based interventions are useful for adherence and there are additional benefits
to be gained from social interaction with peers
61
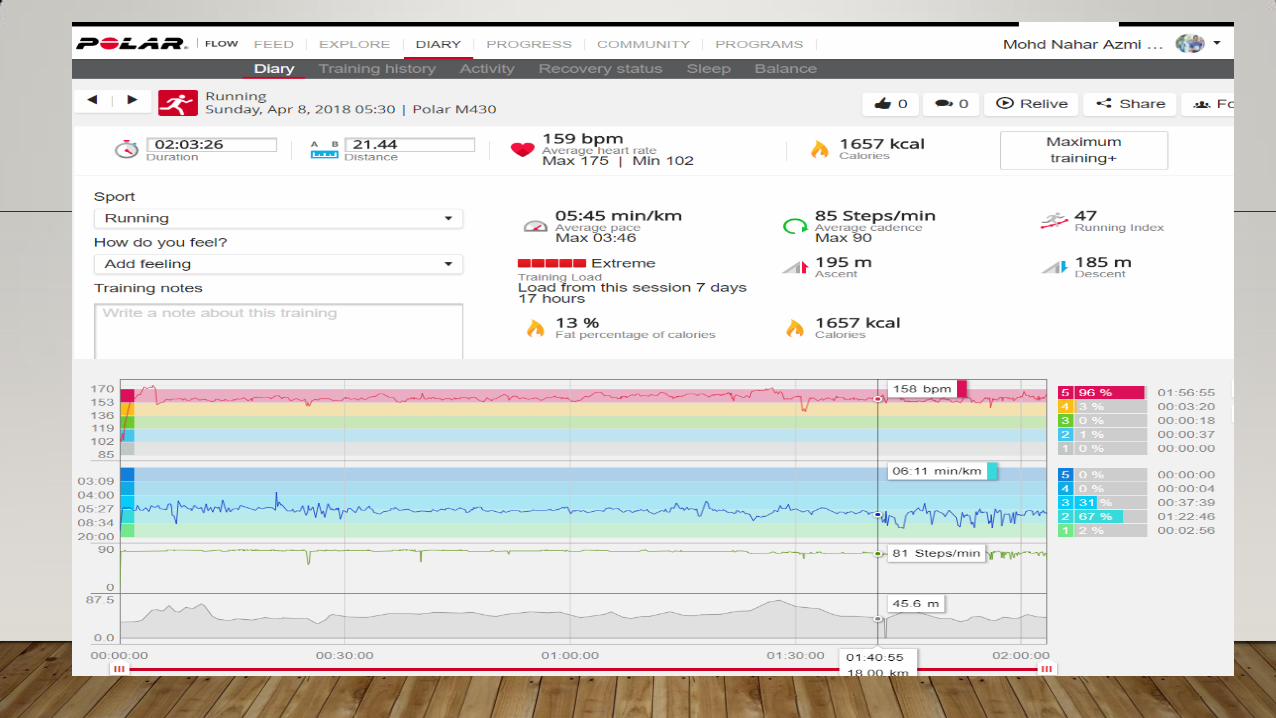
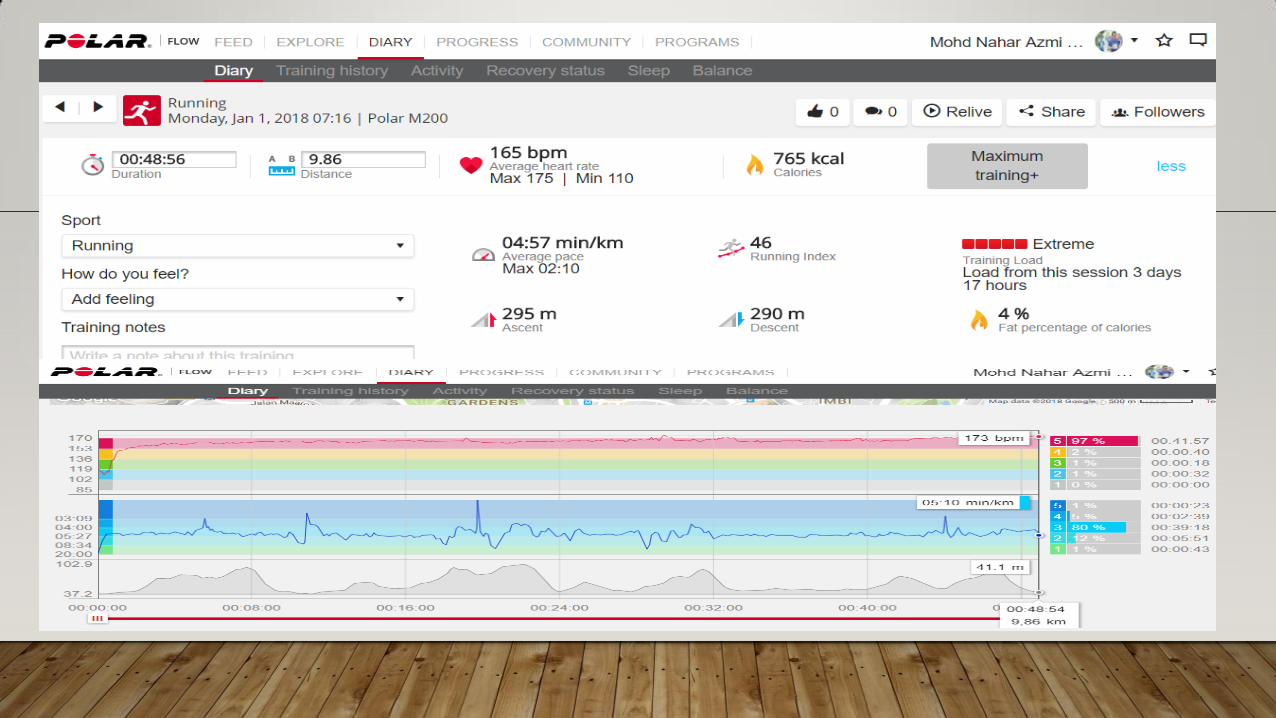
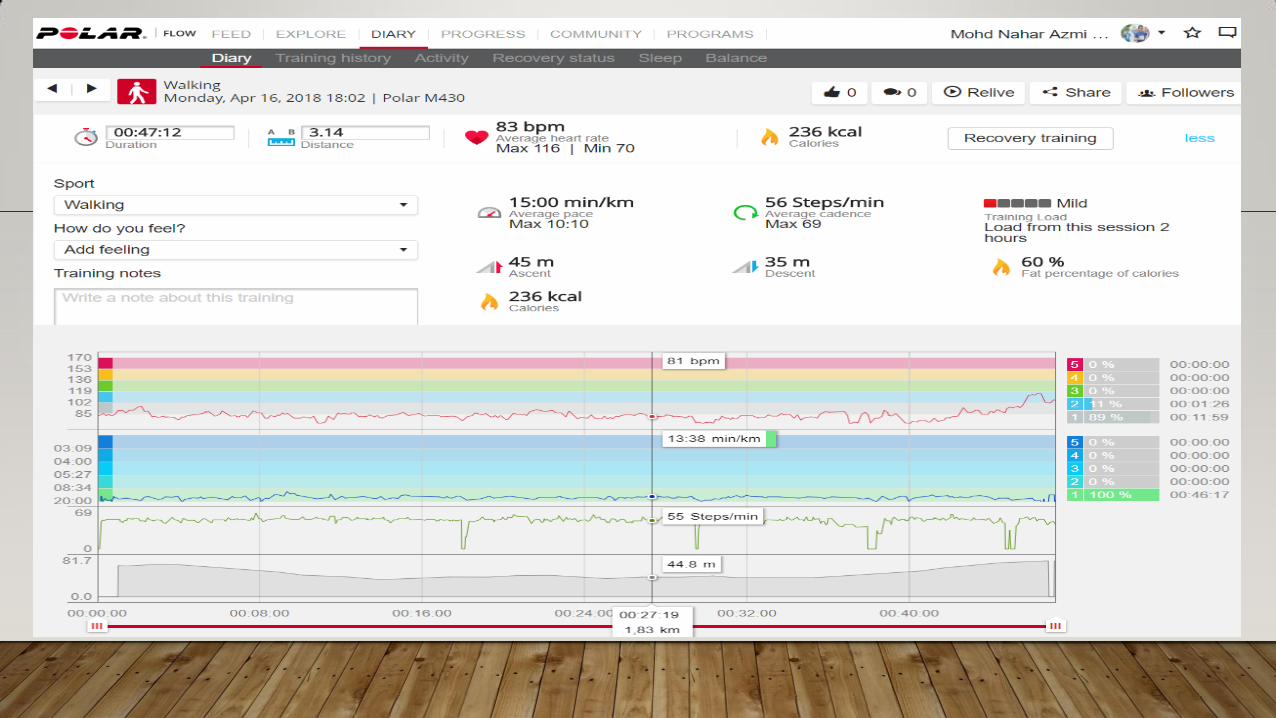
MY JOURNEY

MY WAY TO AN IDEAL BMI, WAIST LINE AND FAT%
• < 2007 = 80kg 2008 – August 2009
• Waist = 90 cm 72-74 kg, W = 86
Waist = 76
THANK YOU

THANK YOU