exercise physiology exam 1 - kupt2013comps -...
TRANSCRIPT

Exercise Physiology Exam 1
Introduction to Ex Phys- Metabolism- all chemical reactions in the body
o Catabolism- breakdown (digestion)o Anabolism- buildup (muscle hypertrophy)
- Bioenergetics- chemical conversion of food into energy- Thermodynamics
o 1st law- energy is neither created or destroyedo 2nd law- process goes from higher to lesser order
Entropy- randomness is favored since takes less energy to spread out 60-70% of energy in body is released as heat—inefficient
- Cellular Energyo At rest body uses mix of fats and carbs, with high intensity switches to carbso Protein doesn’t really provide any energy but is the building blocks for tissue
- Carbohydrateso Advantages- available and easy for muscles to useo Disadvantages- stored with water so takes up a lot of space so don’t store a lot of
glycogen, if used anaerobically is results in lactateo Stored as glycogen in the liver and converts to glucose as neededo Use for both anaerobic and aerobic activityo Yields 4 kcal/gram
- Fato Advantages- lots of energy for long low intensity, stored in large amountso Disadvantages- slower transport to muscle, not an energy source for anaerobic o Yields 9 kcal/gram
- Proteins o Contributes very little energy since can’t oxidize nitrogeno Can be used as energy if converted through glucogenesis- costs a lot of ATPo Large stores in the body as muscles
Basics of Metabolism—energy systems- Immediate sources
o Stored ATP- breaks down through hydrolysiso ATP-PCR system- quick and explosive—5-15 sec
No oxygen required, regenerates ATP PCr + ADP ATP + Cr (enzyme is creatine kinase)
o Adenylate Kinase ADP + ADP ATP + AMP (enzyme is adenylate kinase)- Glycolytic- short and high intensity- 15sec- 2 min
o Glycolysis- glucose is broken down into pyruvate which may be converted to lactic acid
Breakdown of glucose yields 2 ATP, breakdown of glycogen yields 3 ATP o REVIEW diagram of glycolysis and enzymes involved from Ex Phys noteso If need energy fast pyruvate is converted to lactate, if need energy slower than
converted to Acetyl CoA
Lactate dehyrogenase converts pyruvate to lactate Lactate regenerates NADH to NAD+ by taking H+ so rapid glycolysis can
continue Lactate can shuttle electrons to the mitochondria Training improves ability to transport and use lactate so it doesn’t
accumulate causing a decrease in pH Cori cycle- can produce glucose from lactate in the liver with the use of 6
ATP (high ATP expense) if need to maintain blood glucose while fasting- Oxidative system- aerobic energy production- beyond 2-3 min
o Glycolysis (CHO) or Beta-oxidation (Fat) With O2 pyruvate is converted by pyruvate dehyrogenase to Acetyl CoA
(instead of lactic acid) to enter Krebs o Krebs cycle
Each molecule of glucose results in 2 Acetyl CoA 2 ATP, 6 NADH, 2 FADH2
Mitochondria is site for Krebs and ETCo Electron Transport chain
NADH and FADH2 prevent the accumulation of H+ in muscle and blood and carries it to ETC in mitochondria to form ATP
H+ is used to phosphorylate ADP to ATP 1 NADH = 3 ATP 1 FADH2 = 2 ATP End products of oxidative metabolism are CO2 and H2O Oxygen in the final electron acceptor and becomes H2O, if no O2 then
system backs up and slows down (O2 is important since aerobic metabolism)
Oxidation of CHO = 38 ATP (glucose), 39 ATP (glycogen)o Beta oxidation of fat
Free fatty acids in blood travel to muscles and converted to Acetyl CoA to enter Krebs and ETC
1 16-C fat results in 8 Acetyl CoA, 7 NADH, 7 FADH2 = 129 ATP (131-2 ATP for activation)
Lipid Metabolism1. Mobilization- lypolysis is the breakdown of triglyceride to FFA by hormone sensitive
lipase2. Circulation- FFA bound to albumin in the blood3. FFA Uptake- FFA released from albumin and binds to fatty acid binding protein
(increase in this protein with endurance training and in red muscles)4. Activation- invest ATP to attach FFA to coenzyme A Fatty acyl CoA5. Translocation- carnitine acyltransferase enzyme moves fatty acyl CoA into mitochondria
(this enzyme increases with training and increase in # of mitochondria)6. Beta oxidation- faaty acyl CoA results in Acetyl CoA and NADH and FADH27. Mitochondrial oxidation – Acetyl CoA from Beta oxidation enters Kreb’s cycle and ETC
a. 129 net ATP- Red Type 1 muscles are better at using fat as a fuel source

o Better blood supply to transport FFAo High mitochondria contento Endurance training increases mitochondrial capacity to use fat— prolongs time
before glycogen stores are depletedo Fat vs CHO crossover with exercise- Low intensity exercise uses more fats and
fat uses decreases with higher intensity- Ketone Bodies
o Byproduct of lipid metabolismo Seen in hypoglycemic conditions (fasting, starving, diabetes, endurance exercise)o Ketones can be used for fuel in nerves, brain, liver, and hearto If too many ketones accumulate then it is detrimental drop in pH causing
ketoacidosis and are excreted in urine- hard on kidneys
Protein metabolism- Proteins are usually used for structures or enzymes—building blocks of the body- Not use much for energy since nitrogen can’t be stored or oxidized so must be degraded
firsto Degradation- removal of nitrogen so left with a carbon skeleton which can feed
into Kreb’s cycle as pyruvate or Kreb cycle intermediates (occurs in liver) Gluconeogenic amino acids- AAs used in gluconeogensis is glucose levels
are very low (starving or fasting) to keep glucose to the brain These AAs are converted to PEP which can be converted to
glucose but it is an expensive processo Transamination- removes nitrogen and exchange of amine groups to amino and
keto acids Branched chain AA are metabolized by muscle primarily End up with alanine which can be used in gluconeogenesis
Risk Stratification for exercise testingHigh risk- known cardiovascular, pulmonary, or metabolic disease or symptoms—need physician present to supervise sub or max testing
- cardiovascular- cardiac, peripheral vascular (DVT or claudication), cerebrovascular (stroke)
- pulmonary- COPD, asthma, lung disease, cystic fibrosis- metabolic- diabetes (type 1 or 2), thyroid, renal or liver disease- Symptoms
o Pain or discomfort in chest, neck, jaw, arms from ischemiao Shortness of breath at rest or mild activity, fatigueo Dizziness or syncopeo Ankle edemao Palpitation or tachycardiao Intermittent claudicationo Heart murmur
Moderate risk- Asymptomatic with 2 or more risk factors- Physician recommended for max testing, recommend to see physician before vigorous training
Low risk- Asymptomatic with 1 or less risk factors
Risk factors- Age- men 45 yo and older, women 55 and older- Family history- first degree relative (immediate family or grandparents) with MI or
bypass before the age of 55 for men or 65 for women- Current cigarette smoking (still smoking or stopping in the last month)- Sedentary lifestyle- less than 30 min of moderate intensity activity for 3 day/wk for less
than 3 months- Obesity- BMI over 30- Hypertension – 140/90- Dyslipidemia- on cholesterol meds, LDL >= 130 mg/dL, HDL < 40mg/dL- Pre-diabetes- fasting glucose of 100mg/dL or greater (greater than 126 is diabetes) or
OGTT (oral glucose tolerance test) between 140 and 200 (over 200 is diabetes)
Exam 2Energy Expenditure and Fatigue
Basal Metabolic Rate – BMR – Measurement takes place while the subject rests, no food within the past 12 hours, no physical activity within 2 hrs
Resting metabolic rate – RMR – measure 3-4 hours post eating without prior exercise – refers to the sum of metabolic processes of active cells mass required to maintain normal regulatory balance. This accounts for 60-75% of daily energy expenditure.
Resistance training increases BMR by increasing free fat mass. Endurance training increases BMR without increasing free fat mass
Direct Calorimetry – Measures the body’s heat production to calculate energy expenditure. Indirect Calorimetry – Calculates energy expenditure from the respiratory exchange ratio (RER)
of VCO2 and VO2
RER estimates the amount of energy used by the body. RER=0.80 (fats). RER=1.05 (CHO). RER calculation: VCO2/ VO2
MET = metabolic equivalent. 1 MET = 3.5 mL × kg−1 × min−1 . Used to guide or prescribe exercise intensity
VO2 max: Oxygen consumption plateaus with increase in intensity. Absolute O2 uptake (mL min∙ -
1) is divided by body weight (kg) to yield a relative VO2max Oxygen deficit – difference between the oxygen required for a given rate of work and that
actually consumed. Endurance trained individuals have smaller oxygen deficits and reach steady state more quickly
EPOC- excess post exercise oxygen consumption. Lactate threshold- point at which lactate is produced more quickly than can be cleared. Lactate dissociates into lactate anion and H+ ion. Accumulations of H ions causes performance to
decline. Slows glycogen breakdown (remember PFK is sensitive to H ion concentration.). Active recovery helps reduce lactate.
Fatigue: Inability to maintain required power for work at a given intensity and can be reversed by rest. Causes: Energy delivery (ATP-PCr, anaerobic glycolysis and oxidation), Accumulation of
metabolic by-products (lactate and H+), Failure of muscle fiber’s contractile mechanism, Alterations in nervous system

Rhabdomyolysis: breakdown of muscle fiber, releases myoglobin into bloodstream, kidney failure.
Metabolic Control During Exercise
Body has a huge energy demand during exercise. Endocrine system maintains the homeostatic control. Diabetes and kidney disease greatly limit the function of this system
CNS produces quick, short lasting effects while the endocrine system produces slow, long lasting effects.
Hypothalamus and Pituitary gland ”talk” to each other Steroid hormones: soluble in lipids- can cross the cell membrane very easily and to act directly on
the cells DNA. Secreted by the adrenal cortex, ovaries, testes, and placenta. Non-steroid hormones: Not soluble in lipids and can’t cross cell membrane (need a transporter),
react with receptor sites on the cell membrane. *See table in Angel (pdf files) for a list of hormones and what happens to them in response to
exercise. Catecholamines : increase at exercise intensities above 50-70% VO2 Max. With training, the
blood concentrations are decreased (when compared to non-trained) and are increased at maximal exercise (when compared to non-trained)
The pancreas releases insulin (during high blood glucose) and glucagon (during low blood glucose).
Insulin: promotes glycogenesis and inhibits gluconeogenesis. Levels usually decline with exercise. Attenuated response with same work rate ( with training).
Glucagon: promotes glycogenolysis and gluconeogenesis. Increases with increased exercise. Attenuated response with same work rate (with training).
Lose plasma volume during exercise. Endocrine system monitors fluid levels and excretes ADH and aldosterone in response.
ADH: targets kidneys. Promotes water conservation. Causes kidneys to “hold on” to water. Aldosterone (mineralocorticoids): promotes renal reabsorption of Na (causes water retention).
Secreted in response to low blood volume, decreased plasma Na concentration, or increased plasma K condnetration. Increases acutely with exercise.
Neural Control of Movement
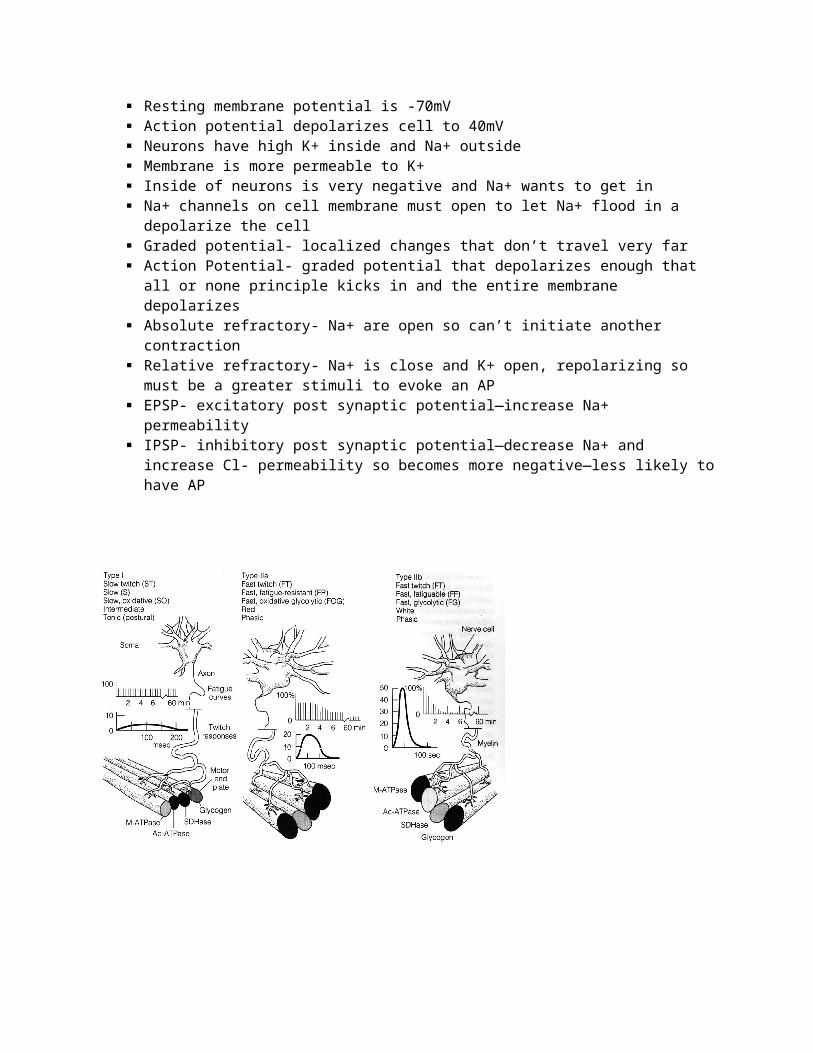
Resting membrane potential is -70mV Action potential depolarizes cell to 40mV Neurons have high K+ inside and Na+ outside Membrane is more permeable to K+ Inside of neurons is very negative and Na+ wants to get in Na+ channels on cell membrane must open to let Na+ flood in a depolarize the cell Graded potential- localized changes that don’t travel very far Action Potential- graded potential that depolarizes enough that all or none principle kicks in and
the entire membrane depolarizes Absolute refractory- Na+ are open so can’t initiate another contraction

Relative refractory- Na+ is close and K+ open, repolarizing so must be a greater stimuli to evoke an AP
EPSP- excitatory post synaptic potential—increase Na+ permeability IPSP- inhibitory post synaptic potential—decrease Na+ and increase Cl- permeability so becomes
more negative—less likely to have AP
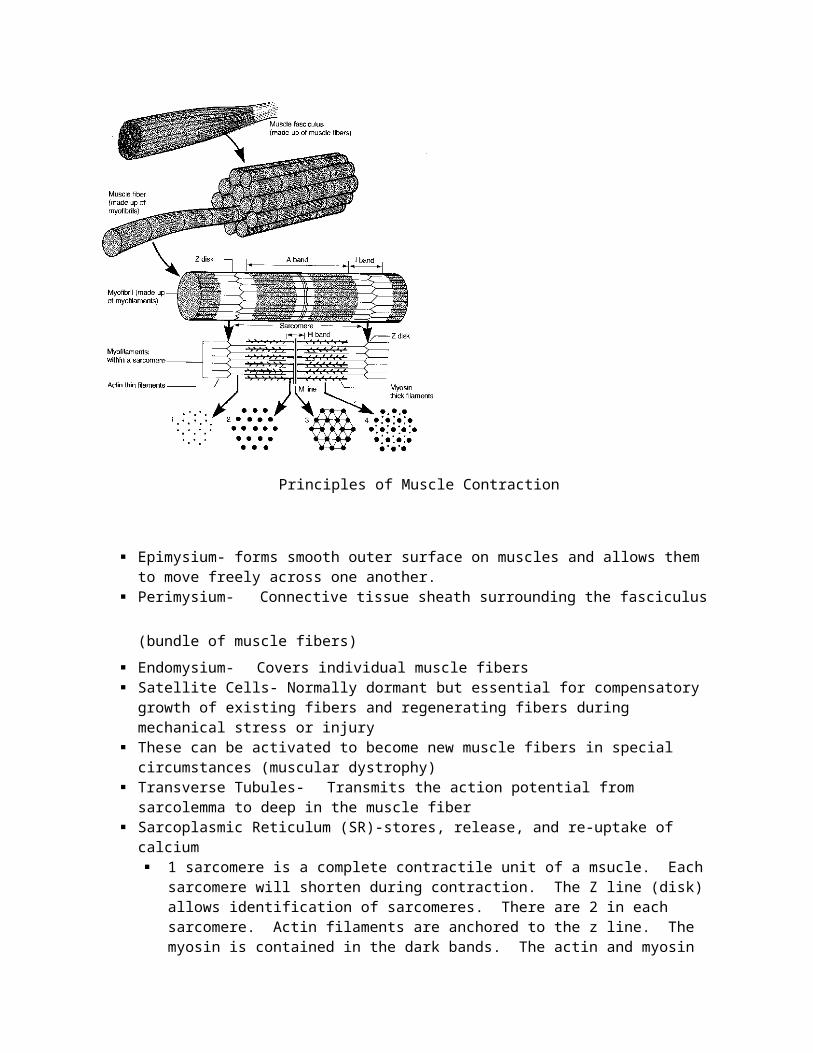
Principles of Muscle Contraction

Epimysium- forms smooth outer surface on muscles and allows them to move freely across one another.
Perimysium- Connective tissue sheath surrounding the fasciculus (bundle of muscle fibers) Endomysium- Covers individual muscle fibers Satellite Cells- Normally dormant but essential for compensatory growth of existing fibers and
regenerating fibers during mechanical stress or injury These can be activated to become new muscle fibers in special circumstances (muscular
dystrophy) Transverse Tubules- Transmits the action potential from sarcolemma to deep in the muscle
fiber Sarcoplasmic Reticulum (SR)-stores, release, and re-uptake of calcium
1 sarcomere is a complete contractile unit of a msucle. Each sarcomere will shorten during contraction. The Z line (disk) allows identification of sarcomeres. There are 2 in each sarcomere. Actin filaments are anchored to the z line. The myosin is contained in the dark bands. The actin and myosin overlap but do not go all the way to the next band (A Band or Z band). A band is where acting and myosin overlap. Myosin heads grab onto actin and will pull the Z lines closer together, shortening the sarcomere. The H zone is the light part in the middle. The middle line is the M line and this is where the myosin is anchored. A bands are composed mainly of thick filaments (but the thin filaments run between them). H bands are composed only of thick filaments
Events leading to a muscle fiber action: Action Potential (AP)- release of neurotransmitter
(acetylcholine-ACh) at neuromuscular junction (NMJ). Ach binds to receptors causing AP to “spread” over the muscle fiber into the T-tubules and stimulate the SR. AP stimulates the
release of calcium from SR Calcium binds to troponin which causes a shift in the tropomyosin revealing active sites on actin. Breakdown (hydrolysis) of ATP “cocks” myosin
head. “Cocked” myosin attaches to actin and movement/muscle contraction occurs. Cross-bridge attachment requires new ATP. In the absence of AP, SR takes up calcium from the intracellular space. Troponin and tropomyosin shift back to resting position (no contraction occurs).
Adaptations to Resistance Training
Factors involved in muscle adaptations to resistance exercise: Specificity, Reversibility, Overload, Individuality.
When designing a program, need to consider components of strength:, Neural adaptations: motor unit activation and frequency, Contractile adaptations: cross section increases, Elastic adaptations: stretch-shortening cycle increased the force (stretch, recoil)
Muscle hypertrophy: Hypertrophy occurs as additional protein is added in the muscle (actin and myosin added). Fiber hyperplasia-does not occur in humans
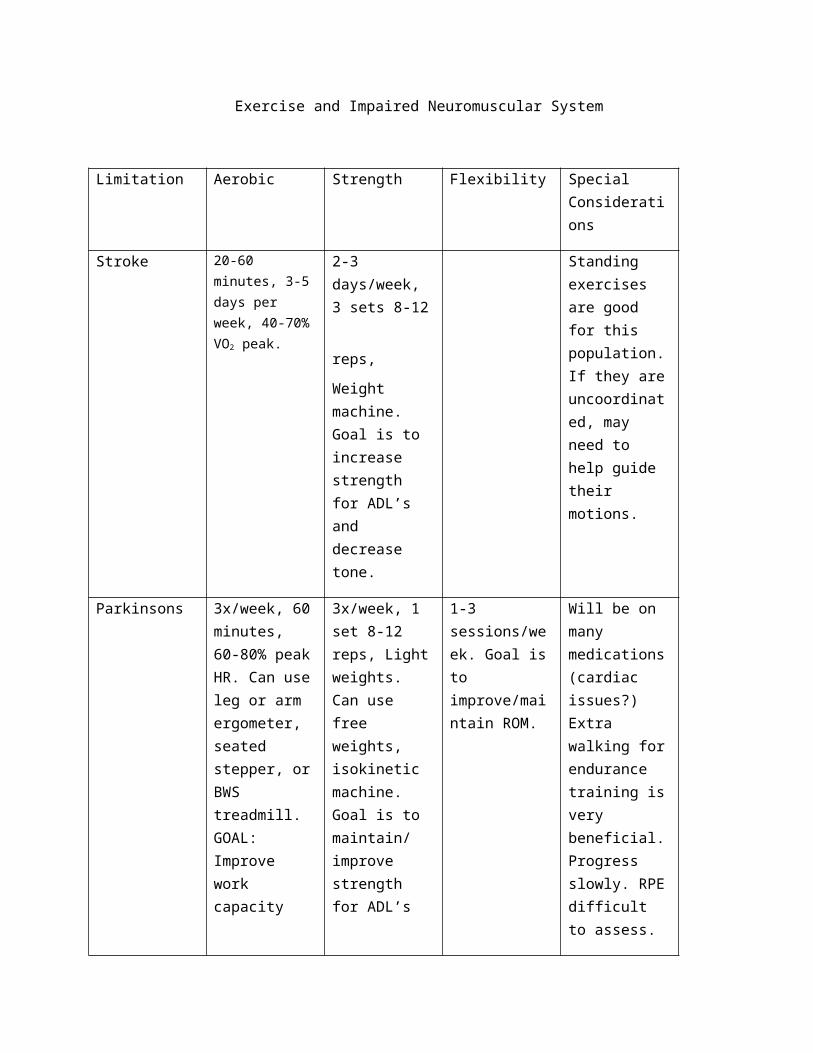
Exercise and Impaired Neuromuscular System
Limitation Aerobic Strength Flexibility Special Considerations
Stroke 20-60 minutes, 3-5 days per week, 40-70% VO2 peak.
2-3 days/week, 3
sets 8-12 reps, Weight machine. Goal is to increase strength for ADL’s and decrease tone.
Standing exercises are good for this population. If they are uncoordinated, may need to help guide their motions.
Parkinsons 3x/week, 60 minutes, 60-80% peak HR. Can use leg or arm ergometer, seated stepper, or BWS treadmill. GOAL: Improve work capacity
3x/week, 1 set 8-12 reps, Light weights. Can use free weights, isokinetic machine. Goal is to maintain/ improve strength for ADL’s
1-3 sessions/week. Goal is to improve/maintain ROM.
Will be on many medications (cardiac issues?) Extra walking for endurance training is very beneficial. Progress slowly. RPE difficult to assess.
MS 3x/week, 30 min/session, 50-70% VO2 peak or 60-85% HR. Can do cycling, walking, or aquatics. Goal is to improve/maintain CV function.
Don’t do on days of aerobic training. Can use free weigts, isokinetics, weight machines. Goal is to increase functional capacity.
Perform before strength/ endurance training. 5-7 days/ week. Goal is to increase/maintain ROM.
Heat sensitivity.
Morning is optimal time for exercise. Hydration is critical.
Exam 3
PTRS 825 Ex phys Exam 3
EKG
Rate SA node 60-100 bpm
Bradycardia < 60bpm (athletes < 60 bpm still considered bradycardia)Normal bradycardia: Heart is pumping too slow- medications to ↑ HR
Tachycardia > 100 bpm AV node 40-60 bpm
Axis Limb lead placement (most activity from apex of heart)
Right arm, left arm, right leg, left leg (cannot be on trunk)
Einthoven’s triangle (seen from + to -)
I. Depolarizing from L arm (+) to R arm (-)
II. Depolarizing from L leg (+) to R arm (-)
III. Depolarizing from leg (+) to L arm (-)
AVR: augmented voltage R (always -)
AVL: augmented voltage L
AVF: augmented voltage foot
Precordial leads- V1-V6V1-V2: Septal; V1-R of sternum 4th intercostal space,
V2-L of sternum 4th intercostal space
V3-V4: Anterior; V3-between V2&4,
V4-L mid clavicular line & 5th intercostal space
V5-V6: Lateral; V5-level with V4 &L ant axillary line
V6-level with V4 & L mid axillary line
Multilead assessment

o Inferior: II, III, aVFo Septal: v1, v2o Lateral: I, aVL, v5, v6o Anterior: v3, v4
Intervals/rhythm SA node fires prior to P wave
Sinus rhythm: SA node is the source of HR= Always a P-wave for every QRS (both upright)
P wave (atrial myocardium depolarization)
Not wider than 0.11s (<3 small boxes)
Not taller than 3mm (<3 small boxes)
Rounded, not notched or peaked
If notched=atria depolarizing separately
+ in I,II, aVF, - in aVR
+/-/biphasic in III, aVL, v1, v2, v3
PR interval (atrial depolarization + delay of AV node- time for atria empty/ventricles fill)
Normal 0.12-0.20s (<1 large box)
If longer, AV conduction is prolonged-1st degree AV block
PR segment (after P wave to before QRS)
Isoelectric (flat)
Elevated with atrial infarction or pericarditis, Not flat with A-fib
QRS-ventricular (myocardium)depolarization & atrial repolarization
All + waves=R, R’ (ventricles depolarize at different times=bundle branch block)
Normal QRS 0.07-.11s, the widest lead measurement is correct (usually 1 & v1)
Leads I, II, III > 6mm, v5, v6 < 25-30mm
Tall waves=hypertrophy
QRS gets bigger as you get closer to the heart
R waves should progress from V1 (-) and gradually become +, with v5 & v6 being tallest
Most progression should occur v3-v4 (if v5-v6=infarction of anterior L ventricle)
Q wave (-, represents septal depolarization)
Not recorded in all leads-present in I, aVL, v, v6, small in aVF & v5
Normal Q wave <1/3 QRS, < 0.04s (<1 small box)
Large= altered electrical activity in myocardium
ST segment- absolute refractory period (heart cannot contract ventricles have not repolarized)
Ventricle cells are in the plateau phase, should be flat (isoelectric)
Elevation/rounds out= vessel occlusion
Down slope= ischemia
T wave- ventricular repolarization (occurs backwards in cardiac tissue)
Should be same direction as QRS- if opposite big problem!
Ventricles can depolarize again at apex of T wave
EKG paper1 Small box (1mm) = 0.04 sec
1 large box = 5 small boxes = 0.2 sec
Amplitude: 1 small box = 0.1mV
Count the rate:a. Count QRS complexes in 10s rhythm strip X 6 = bpm (for normal rhythm)b. 60 ÷ R to R interval (in seconds)c. Find QRS on a heavy line & count large boxes until next Rwave
1 box = 300 bpm (has to be a regular HR = distance between)
2 boxes = 150 bpm
3 boxes = 100 bpm
4 boxes = 75 bpm
5 boxes = 60 bpm
6 boxes = 50 bpm
d. For irregular HR: Count cycles over 6 sec period X 10 Axis deviation
Axis= direction of ventricle depolarization (Vector) of the QRS complex
Abnormal axes are suggestive of disease states:

Emphysema, Hyperkalemia, Lead transposition, Artificial cardiac pacing, Ventricular tachycardia
Examine limb leads I, II, III, & aVR, aVF, aVL
Upward deflection: + charge towards + electrode
Downward deflection: + charge away from + electrode
Normal (+90 to -30) Left axis deviation (>-30 to -90)
Can be caused by left ant hemiblock, Q waves of inferior myocardial infarction, artificial cardiac pacing, emphysema, hyperkalaemia
Right axis deviation (>+90 to 180)Normal in children & tall adults, can be caused by R ventricular hypetrophy, chronic lung
disease, L post hemiblock, pulmonary embolus, atrial septal/ventricular septal defect
Extreme right axis deviation (>-90 to <180) Methods of axis deviation determination
o Mean QRS axis is midway between the 2 leads with tall R waves of = amplitudeo Mean QRS axis is at a right angle to lead with a biphasic isoelectric complex
1. Find biphasic isoelectric R=S2. Find right angle lead using diagram3. Identify +/- using EKG4. Find correlating angle on diagram= mean QRS axis
CARDIOVASCULAR SYSTEMCellular activity: ↑O2 demand, ↑CO2 production
Circulation: ↑stroke volume, ↑HR
Ventilation: ↑RR, ↑tidal volume
Heart receives blood flow from cardiac capillaries during diastole (ventricles filling/relaxed)
Cardiac cycle: ≈0.9s (67bpm)Ventricular Diastole- relaxation phase: Chambers fill with blood ≈0.50s
T wave to QRS Inlet valves open (bi-/tricuspid) Outlet valves closed (aortic/pulmonary) Passive rapid filling phase → diastasis → atrial contraction(15-20% Q) End diastolic volume (in ventricle)
Isovolumetric contraction ≈0.05s
LAD
RAD
X-RAD

wall tenses → ventricles change shape (wringing) → increasing pressure All valves closed: bi-/tricuspid valves close when ventricle pressure > atrial
pressure (S1 or “lub” sound) ventricle is a closed chamber
Ventricular Systole- contraction phase (ejection phase): Chambers expel blood ≈0.30s
QRS to T wave Ventricle pressure >>>atrial pressure Inlet valves closed, outlet (aortic/pulmonary)valves forced open ¾ stroke volume ejected in rapid phase (≈0.15s)
Isovolumetric relaxation ≈0.8s
All valves closed, outlet valves closing cause S2 or “dub” sound Ventricle is a closed chamber Elastic recoil of myocardium → ventricle pressure falls rapidly Ventricle pressure < atrial pressure inlet (AV) valves open
Atrial diastole ≈0.65s, immediate filling when atria open (during ventricular systole)
Atrial systole ≈0.15s, push blood completely into ventricles
Sinoatrial (SA) Node: Pacemaker of the heart (Intrinsic rate ≈72bpm)Bundle of nerves located in the R atrium
Highest concentration of intrinsic rhythm-> dominant heart pace
Parasympathetic Nervous System Vagus Nerve (CNX)-innervates heart, GI SA node, resting HR
Sympathetic nervous system Responds to various stimuli “fight or flight” Catecholamines: epinephrine & norepenephrine
↑contractility, HR, & speed of contraction (adrenergic receptors) Periphery effects: ↑vasoconstriction (- adrenergic receptors)
Epinephrine ↓vasoconstriction (- adrenergic receptors) Homeostasis
Atrioventricular (AV) node (intrinsic rate 40-60bpm)AV node is part of the neuromuscular conduction system->Bundle of HIS->L/R bundle branches
Can become dominant under certain circumstances
Cardiac functions
Delivery: O2, nutrients; Removal of waste,
Transport: hormones, insulin, glucose, catecholamines
Maintenance of pH

Cardiac output (Q) amount of blood pumped out of the heart per unit time
Q = SV x HR
Rest ≈ 5 L/min, exercise ≈ 20-25 L/min,
increases linearly with workload
SV & HR responsible up to 50% max capacity,
>50% HR (SV plateaus-↓ fill time)
Training increased make Q (↑SV)
At sub max untrained Q ≈ trained Q
training ↑SV & ↓HR=same Q
Greatest with running vs cycling or swimming- greatest weight bearing
Stroke Volume (SV) = end diastolic-end systolic volume=the amount pumped out (≈100-200ml)
Increases curvilinear with work, reaches max at approx 50% aerobic capacity
SV is higher in trained individuals at any workload (can work at lower HR)
Important in determining VO2 max, greatest difference in trained vs. sedentary individuals
Frank-Starling Mechanism: ↑blood in ventricle causes greater stretch & ↑ contractility
Will reach max EDV fill (max effectiveness) more effect at lower work rates
At rest: SV higher in supine than upright (↑ EDV-easier for blood to return to heart)
Ejection fraction (EF): proportion of blood pumped out of L ventricle with each beat
EF= SV/EDV = EDV-ESV/EDV (≈ 60%)
EF<40-50: is a concern, 15-20%: indicative of death
Resting HR ≈ 60-80 bpm, can range from 30-100bpm
Decreases with age & cardiovascular fitness (endurance training)
Training sedentary individuals may see ↓ HR by 1bpm/week
Fluctuation of 10bpm indicative of over training (overstressing the heart)
Affected by environment: temp (cold ↓ HR) & altitude
Max HR: can be estimated 220-age (yrs), will decrease with age
Remains unchanged or slightly decreases with training (allows for optimal SV)
HR recovery: time after ex for HR to return to resting rate (faster with training)
Can be affected by altitude or heat
Steady-state HR: plateau during sub-max work
Lower steady-state HR, more efficient the heart
May decrease by 10-30bpm after 6 months of moderate training
Karvonen formula: [training range % (max HR-resting HR)] + resting HR
Used if pt is taking meds that increase HR: train them at % of their available HR range
Anaerobic threshold: level of activity that can no longer be supported solely by aerobic metabolism
Above AT: rise in CO2-increased anaerobic metabolism->lactic acid (buffer= HCO3)
Cannot sustain prolonged workout
Below AT can maintain exercise
Will increase with training (intervals)
RER > 1.0 indicates anaerobic metabolism (CO2 production> O2 consumption)
RER>1.09-1.29 = max effort (normal population)
↑ with anxiety, ↑ with eating
VO2max: maximal O2 consumption, VO2max = SV x HR x arteriovenous O2 difference
Measure of cardiorespiratory fitness via direct or indirect calorimetry
Improves with training (10-30%), can work longer & at greater loads
Decreases with age, training can maintain VO2max or decrease downward slope
Males have higher VO2max than females with similar training levels
Arteriovenous difference: how well cells pull O2 from blood
Difference between [O2] of arterial & venous blood
Normal resting ≈ 5ml O2/100ml blood, exercise ≈ 15ml O2/100ml blood
Can increase with training

Minute ventilation: RR x tidal vol (L/min)
snapshot of how pulmonary system is doing
Blood volume: increased with endurance training (primarily increased plasma volume)
RBC volume ↑, but plasma volume is higher: hematocrit ↓ (44% to 42%)
Blood flow increases at exercise onset, linear increase with workload
Blood flow stabilized at constant workload
Blood pressure (BP): intra-arterial pressure during systole and diastole
BP = Q x total peripheral resistance (TPR)
Systolic increases linearly with exercise intensity (failure to ↑ signifies heart failure)
Diastolic remains unchanged or decreases slightly (mm pump helps drive blood back)
Training lowers resisting & submax systolic/diastolic BP, max is unchanged
Nervous control of BP
Long term: kidneys (fluid balance)-important in running for hours
Short term: cardiovascular system
Sensors monitor pressure and adjust the Q and TPR accordingly
Stretch receptors: pulmonary & cardiac (carotid & aortic arch)
Sense atrial stretch & preload- ↓ BP (vasodialation=↓TPR) and ↑ ADH
Vasomotor center (medulla) receives input from sensors (chemo, baro, mm afferents), cortex, hypothalamus -> communicates with sympathetic neurons in spinal cord
Pressor stimulation: ↑HR, ↑contractility, ↑constriction of vascular smooth mm
↑sympathetic tone (constriction of mm vessels are overridden by ↑CO2 in blood)
Depressor stimulation: ↓HR, ↓contractility, ↓constriction of vascular smooth mm
Parasympathetic tone
Aging: tend to be more sedentary, lose mm, medical problems resulting in functional impairment, ↓independence, ↑need for healthcare services
Negative changes: Vascular, BP, Cardiac, coronary arteries, ANS, pulmonary, musculoskeletal
Training: ↑VO2max (endurance), ↑strength (resistance), ↓BP, ↓HR, ↓body weight, ↓%fat, ↑insulin sensitivity, ↓cholesterol
RESPIRATORY SYSTEM
Respiration-delivery of O2 & removal of CO2 from tissueo Internal respiration: exchange of gasses btn blood & tissue (capillary gas
exchange)o External respiration: ventilation & gas exchange in lungs
Pulmonary ventilation (inspiration & expiration) Inspiration is active- diaphragm & external intercostals Expiration is passive- relaxation of inspiratory mm & lung elastic
recoil controls blood acidity: CO2+ H2O ->H2CO3->H+ + HCO3-
Pulmonary diffusion: Exchange of O2 & CO2 btn alveolar sacs & pulmonary capillaries
1. Replenishes blood O2 after used for oxidative energy production2. Removes CO2 from venous blood
o Conducting zone (anatomical dead space ≈ 159mL) Trachea, primary bronchioles, bronchus, bronchi, bronchioles Humidification, warming, filtration (nose, cilis, swallowed), vocalization
o Respiratory zone (gas exchange) Respiratory bronchioles, alveolar ducts, alveolar sacs ↑ surface area slows airflow, surfactant production, endocrine function
o Partial pressures: ↑ pressure gradient = ↑ O2 diffusion Dalton’s law of partial pressures (each gas contributes to total pressure) O2 21%, CO2 0.03% , N2 79% of air
Partial pressures create pressure gradient (facilitate gas exchange) Gases move from high to low concentration
Fick’s law of diffusion: gas diffusion rate across tissue sheet is proportional to surface area & inversely proportional to thickness of tissue
CO2 20x faster than O2 (CO2 has higher solubility) Measuring pulmonary ventilation
o Vol of gas exchange will change with temperatureo Ventilation (VE) = tidal volume (TV) * breathing frequency (f)
Mild-mod exercise VE is increased by ↑TV, max exercise VE is increased by ↑f
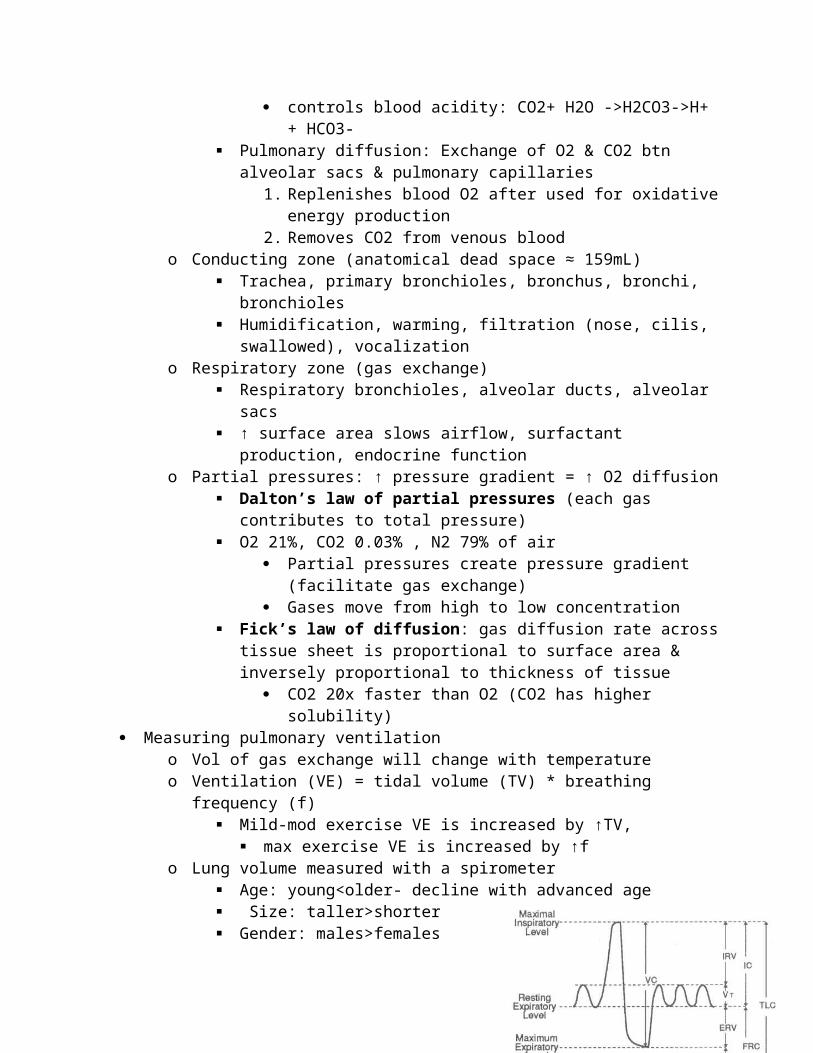
o Lung volume measured with a spirometer Age: young<older- decline with advanced age Size: taller>shorter Gender: males>females
o Tidal volume (TV)~0.4-1 L o Inspiratory reserve volume (IRV)~2.5-3.5 Lo Inspiratory capacity (IC): TV + IRV
o Expiratory reserve volume (ERV)~1.0-1.5 Lo Forced vital capacity (FVC=IRV + ERV)~3-5Lo Residual lung volume (RLV)~ 0.8-1.4 L (↑ with age, ↓ elasticity)o FEV1: forces expiratory volume in 1 secondo FEV1/FVC indicated pulmonary airflow capacity (≈85%)
Ventilatory response to exerciseo Maximum exercise is not limited by pulmonary ventilationo Respiratory mm uses > 15% of total O2 consumed during heavy exercise o Minute ventilation: volume breathed out each minute
Increases dramatically during exercise TV rarely exceeds 60% vital capacity
o Ventilation-perfusion ratio (Alveolar ventilation:pulmonary blood flow) Light exercise ≈0.8, strenuous exercise ≈5.0
o Respiration rate (RR) increases 1-3X in normal adults (6-7X in athletes)o Dyspnea (shortness of breath) poor conditioning of respiratory mm (shallow,
ineffective breathing)-> inability to readjust blood PCO2& H+ o Hyperventilation (ventilation exceeds metabolic O2 need) ↓ ventilator drive by
↑blood pH (↓ blood CO2)o Valsalva maneuver (trap air pressure in lungs) ↑ intrathoracic pressure, can ↓
cardiac output, can be dangerous (↓venous return, ↓blood to brain- causes dizziness/fainting)
o Cold-weather exercise: air is warmed in conducting zone Moisture lost if air is cold & dry (dehydration, dry mouth, bronchospasm)
o Anaerobic threshold: ventilatory breaking point Work rate > 55-50% VO2max- energy must come from anaerobic ↑ CO2 -> ↑ ventilation
o Lactate accumulation Untrained: 55% VO2max,enduranced trained: 80-90% VO2max Active recovery reduces lactate levels faster
o Excess H+ impairs mm contractility & ATP formation CO2 or lactate accumulation (bicarbonate ions buffer H+) ↑ RR to ↑ CO2 released in blood (bound to bicarbonate)->to lungs &
exhaled (carbonic anhydrase catalyzed dissociation) Haldane effect: hemoglobin binds to O2 & ↓affinity for CO2 Extracellular buffers: bicarbonate, release CO2 in lungs, H+ excretion in
kidneyso 60-80% VO2 max >5-10 min
↓PO2 in arterial & mixed venous blood ↑PO2 in alveolar air ↑PCO2 in mixed venous blood (↓pH)
o 80-90% VO2max ↑Ventilation, arteriol H+, VO2 (degree dependent on fitness level)
o Altitude: can cause ventilation to be a limiting factor during exercise Acclimation:

right shift of O2 dissociation curve (↑ O2 unloading, ↑2,3-DPG) ↑max breathing capacity (air is less dense) Pulmonary vasoconstriction due to hypoxia
o ↑pulmonary arterial pressureo ↑work of right heart ventricle (hypertrophy)
↑viscosity (polycythemia-↑RBC) Ventilatory control: adjust rate & depth of breathing in response to metabolism
o Receptors in various tissues (monitor blood pH, PCO2, PO2, temp)o Ventilatory threshold: ventilation↑ disproportionately to O2 consumption
Lactate is buffered by sodium bicarbonate->CO2 (stimulates ventilation)o Pulmonary ventilation during exercise regulates arterial blood gas (try to
maintain normal levels) & maintains acid/base balance ↑intensity, ↑ventilatory response
Bohr effect: R shift of O2 dissociation curve (↑ O2 dissociation from hemoglobin)o ↑PCO2, ↓pH, ↑temp, ↑2,3-DPG (byproduct of glycolysis)o Hopes to deliver more O2 to working tissue
CARDIORESPIRATORY RESPONSE TO EXERCISE
Exercise to VO2 maxo ↑O2 deliveryo ↑max mm flood flow (↑cardiac output & ↑mm capillary density*)o ↑Cardiac output (Q)o ↑Stroke volume (↓HR)o ↑End diastolic volume (↑Venous return & ↑ventricular volume*)o ↑Blood volume (↑ plasma volume* & ↑ RBC mass*)
*affected by training for long-term endurance (improves peripheral focus)
Submax Steady state exercise o ↑HR (↑Stroke volume & ↓sympathetic stimulation*)o ↑End diastolic volume (↑Venous return & ↑ventricular volume*)o ↑Blood volume (↑ plasma volume* & ↑ RBC mass*)
*affected by training for long-term endurance (improves peripheral focus)
Body is a closed loop system: blood pressure (BP) gradient moves blood through system Total blood volume ≈ 5L (64% in veins, 16% in arteries/arterioles, 4% in capillaries) Hemodynamics
o Pressure 80->35mmHg along arterioles: highest vascular resistance
Thick walls ≈6m (allows for variation in blood flow) Darcy’s law: Q = (P1-P2)/R (inversely related: ↑ P, ↓ resistance)
o Velocity (rate) Capillaries have lowest velocity: facilitates exchange btn blood & tissue Velocity is inversely proportional to diameter: Smaller vessel->faster rate
o Flow (volume) Poiseulle’s equation: Blood flow = change in P*π R4 / 8*viscosity*length

Length: length x 2 => ↓ flow 50% Radius: radius x 2 => ↑ flow x 16 Viscosity: viscosity x 2 => ↓ flow 50%
laminar flow: uniform, in 1 direction travels in concentric fluid layers little energy loss to viscous interactions disruption results in turbulence
turbulent flow: not uniform, a lot of movement-high shear on endothelial wall (can form plaques)
occurs at narrowed vessels, branches, aortic arch at high velocities Greater pressure required to propel blood Can be heard through stethoscope (Bruit)
Sheer stress: friction on endothelial wall (blood rate & viscosity) Cause HTN, Marfan’s syndrome Release NO (vasodialator)
o Resistance (of vessels) Total peripherial resistance (TPR)= sum of all systemic vascular resistance
=Resistance from aorta to rightR atrium arteriole R is a major part: arterioles dilate/constrict-TPR changes Venoconstriction does not sig. change radius & little change in R (veins
have large diameter with low R) o ↑Pressure in peripheral veins without change in resistance = ↑
venous compliance In series: resistances will be added together -> total R will be higher
TPR = Rarteries + Rarterioles + Rcapillaries + Rvenules + Rveins
In parallel: resistance is split among vessels -> total R is reduced 1/TPR =1/Rbrain + 1/Rcoronary + 1/Rrenal + 1/Rmuscle + 1/Rskin + 1/Rother
Blood flow regulationo Neural control: change in position, exercise, injury to brain (autonomic control)o Vasodilator metabolites are produced by cells (mm requires K+)
Concentration of metabolites determined by rate of formation: proportional to metabolic rate rate of removal: proportional to blood flow to organs
Vasodilator metabolites: ↓ Ca++ within vascular smooth mm ↑Relaxation, ↑arteriolar radius, ↓vascular resistance, ↑blood flow ↑Metabolic activity-> ↑release of adenosine (vasodilator) K+: regulates electrically excitable organ blood flow (brain & heart),
↑action potential ↑interstitial K+->↓Ca++ influx->causes mm relaxation
↑La+, H+, CO2 when O2 demand > availability =>vasodilation ↓ATP levels (↑ ADP levels) activate K channels -> ↑K+ efflux (local hyperkalemia) ->vasodilation
Active hyperemia: ↑metabolic activity->↓O2 -> ↑local arteriolar dilation from metabolites -> ↑blood flow
Reactive hyperemia: blood flow transiently ↑ (excess of normal) after brief ischemia
o Vascular tone is the degree of blood vessel constriction relative to its max dilation Heart, muscle, skin have ↑vascular tone (due to vasodilation capacity) vs.
cerebral & renal circulation (maintain same flow)

Balance of competing vasoconstriction & vasodilation influences Extrinsic factors:
o Neurohumoral: sympathetic n, angiotension II ↑ vascular tone (vasoconstriction)
o Some circulating factors ↓ vascular tone Intrinsic factors
o Myogenic mechanisms: originate from vascular smooth mm (↑ vascular tone)
o Endothelial factors: NO, endothelin can ↑ or ↓ toneo Local hormones/chemical substances: arachidonic acis
metabolites & histamine can ↑ or ↓ toneo Metabolites generally ↓ toneo Hypoxia ↓ tone
Hormones: released at 1 site & effect another siteo Bradykinin (dilation)o Norepinephrine (constriction)o Angiotensin II (constriction)o Vasopression/ AHD (constriction)
o Blood flow increases with training ↑ capillary formation, ↑ opening of existing capillaries More effective blood redistribution (goes where it is needed)
Exam 4
AgingIs the accumulated effects of the interaction of the self and the environment over time.
Theories of Aging:Hayflick Limit: cells can only divide so many times.Free Radical Damage: electron deficient molecules stealing electrons from other proteins. Ie Oxidative stress.
Age Related Changes in the BrainAtrophy- loss of neurons, axon diameter decreases, reduced thickness of myelin sheath.
FunctionDecline in inhibition, speed, accuracy and reliability of neural coding, neural noise may increase.
Cognition & PerformanceAge-Related Cognitive Slowing Theory-through various physiological processes, older adults’ cognitive processes slow and deteriorate. Older adults struggle with learning more complex tasks, but can still learn new motor skills. Exercise has been shown to reduce cognitive decline
Exercise and Alzheimer’s Disease
Alzheimer’s Disease is the most common cause of dementia. Early cognitive changes include:
Memory Loss: forgetfulness, repetition of questions, misplacing items.Executive Dysfunction: Managing finances, driving, meal prep, operating appliances.
Noncognitive changes include:Bone mineral loss, sleep disturbances, behavioral disturbances,
PreventionPhysical activity is associated with lower risk of cognitive impairment, Alzheimer’s disease and dementia.
Exercise in Chronic Disease and Disability
HIV- selective infection of CD4 or T-helper cells results in immunosuppression. Stage 1: Asymptomatic HIV seropositive.Stage 2: Early symptomatic HIVStage 3: AIDS- fatigue, chronic diarrhea, anemia, muscle wasting, pneumocystis pneumonia
Exercise in individuals with AIDSAerobic Exercise:Frequency: 3-5x/week
Duration: 20-60min/sessionIntensity: 50-60% VO2 peak or 60-75% HR
Strength Training: Frequency: perform on non-aerobic daysExercise considerations: strict universal precautions, medications can cause tachycardia, anemia, hypertension.
Spinal Cord Injury Aerobic Exercise:
Frequency: 3-5x/weekDuration: 20-60min/sessionIntensity: 50-80% VO2 peak
Strength Training:Frequency: 2-4 days/weekIntensity: 2-3 sets of 8-12 reps
Exercise considerations: hypotension->no exercise <3 hrs after eating, hypertension, limited forced expiration, thermoregulation.
DiabetesIs a chronic metabolic disease with absolute or relative deficiency of insulin->hyperglycemia. Complications include: retinopathy, nephropathy, neuropathy-peripheral & autonomic.
Aerobic Exercise:Frequency: 3-4x/weekDuration: 20-60 min/sessionIntensity: 50-70% max HR
Strength Training:Frequency: 3 days/week
Monitor glucose pre & post exercise. No exercise if glucose>250 or < 70.
Chronic Kidney DiseaseIs a permanent loss of kidney function. Diagnosed by markers of injury in blood, urine or imaging. Glomerular filtration rate <60 ml/min per 1.73m² for more than 3 months. Management: Hemodialysis, peritoneal dialysis, renal transplantation, Meds-anti-hypertensives, anemia meds (EPO), hyperparathyroidism(phosphate binding agents).
Aerobic Exercise:Frequency: 4-7x/weekDuration: 15-60 min/session as toleratedIntensity: 40-80% max HR
Exercise considerations: Patients will have low exercise tolerance, blunted HR 220-age is not appropriate to use, high blood pressure, anemia, exercise or therapy may not be tolerated after dialysis, renal bone disease in patients on dialysis > 5 years.
Cancer is a collection of diseases caused by excessive, uncontrolled cellular proliferation->Metastasis.
Aerobic Exercise:Frequency: every other day
Duration: 20-40min/sessionIntensity: symptom limited or moderate intensity
Strength Training:Frequency: 2-3 days/weekIntensity: 2-3 sets of 3-10 reps @50% 1RM
Exercise considerations: Anemia, loss of lean muscle.
Pediatric Exercise Testing
Cardiovascular Response to Exercise in ChildrenQ for children can increase 3-4 times above resting levels, mostly due to increased heart rate.
Children have lower stroke volumes and higher hear rates.Maximal HR ranges from 195-205-210bpm, starts to decline in late teens-early 20’s.High temp & humidity can increase HR 10-20bpm at a standard workload.SBP >220mmHg is of increased concern.DBP should only vary 6-10 mmHg.
Pediatric Chest Pain & Shortness of BreathCategories of Chest Pain
Acute Onset: Cardiac or noncardiac in nature. Pts seen in ER.Causes of Chronic/Reoccurring Chest pain
NonCardiac:Pulmonary: pneumothorax, pneumonia, pleurodyniaEsophageal: acute esophagitis, foreign body
Cardiac CausesPericarditis, trauma, arrhythmia
Exercise Induced AsthmaSymptoms: coughing, wheezing, chest tightness, shortness of breath.Symptoms typically begin 15-20 min after starting exercise. Exacerbated by cold dry air. About 2/3 of pts with asthma have GERD. Treatment of reflux may alleviate asthma symptoms.Management: Quick acting Beta-agonists- fast acting bronchodialators: albuterol, Proventil.
Bronchodialator Response w/ treatment using short acting acting beta-agonistFEV1- increase of 200ml or 12% is considered a positive response.FVC- increase of 10% or more.FEF 25-75%- an increase >29%.If 2 or more of these are met= reversible airway obstruction.
Vocal Cord DysfunctionVCD s a paradoxical closure or adduction of the vocal cords during inspiration. This causes partial to severe airflow obstruction with sensation of throat tightness, suffocation and/or chocking.

Symptoms of VCD: stridor, chest or throat tightness, difficulty w/ inspiration, abrupt onset and resolution, chronic cough or hoarseness, tingling in arms/legs, felling faint, hyperventilation.
Treatment of VCD- education, correct diaphragmatic breathing techniques, upper body relaxation techniques.
Lung FunctionForced Vital Capacity- maximum volume of air that can be forcefully exhaled after the deepest possible inspiration.FEV1- indicator of large airway obstruction. Should be >80% of predicted.FEV1/FVC- Best predictor of obstruction. If below 80% think obstruction.FEF 25-75%- forced expiratory flow. Mean expiratory flow during middle half of FVC. Decrease represents small airway obstruction. Should be between 60-70% of predicted.
Airway ObstructionDisease that affects the diameter of the airways. Low flow rates relative to lung volumeMucous production, inflammation, bronchoconstrictionAirway Restriction
Restriction of lung tissue or capacity of lungs to expand and hold the predicted volume of air. Low volume with normal flow rate. Secondary to scarring, fibrosis or deformity--Sarcoidosis, interstitial fibrosis, scoliosis
Combined Restrictive/ObstructiveCystic Fibrosis- excessive mucous and damage to lung tissue
Congenital Heart DiseasesAortic StenosisAortic Coarctation- constricted or pinched aorta.Hypertrophic Cardiomyopathy- large dilated left ventricle.Kawaski Disease- transposition of coronary vessels and other coronary defects.Single Ventricle- will see blunted HR, low functional capacity, ECG abnormalities, decreased O2 sat, pt will look purple esp. in lips and fingernails.Pulmonary Atresia & tetralogy of Fallot- malformed pulmonary valve.
Ergogenic AidsAny substance or technique used to improve athletic performance.
Hormonal AgentsAnabolic steroids- resemble androgenic hormones such as testosterone and nandroloneAccelerate growth by increasing the rate of bone maturation & increase muscle mass

Prescribed to children with delayed growth patterns to normalize growth curve Effects of Anabolic Steroid Use:
Increased body mass and fat free mass Increased total body potassium and nitrogen Increase muscle size and strength May facilitate recovery from intense exercise by reducing muscle fiber
damage and increased protein synthesis
Risks of Anabolic Steroids
Cardiovascular; CAD, HTN Tendon ruptures Liver tumors Psychiatric complications Reproductive side effects
o Males: testicular atrophy, infertility, gynecomastia, impotence, prostate CA,
o Females: amenorrhea, infertility, acne, hirusitism (excess body hair)
Human Growth FactorSecreted by anterior pituitary gland. Prescribed for hypopituitary dwarfism
Potential Effects of HGH
Stimulation of protein and nucleic acid synthesis in skeletal muscle Stimulation of bone growth (elongation) if bones have not fused Increase in lipolysis -> reduction in body fat Increase in blood glucose levels Enhanced healing after musculoskeletal injuries
Risks & Side Effects of HGH
Gigantism & acromegaly Weakness in proximal muscle attachments in thighs and upper arms Damage to myocardium Organ enlargement (liver, spleen) Osteoporosis and sexual dysfunction Hypertension and diabetes
Physical AgentsAgents normally found in the body. Ie Vitamins & Minerals
Pharmacological Agents
Amphetamines- used to combat fatigue and improve endurance.
Increase concentration, decrease reaction time, weight loss, mask fatigue Increase max HR, BP and muscle glycolysis VO2 max and RER are unaffected
Risks or Side Effects of Amphetamines
Psychological and physical addiction Restlessness, anxiety, euphoria, paranoia, insomnia, aggressive behavior Cardiac arrhythmias, death
Beta Blockers- block beta-andrenergic receptors preventing norepinephrine binding
Reduces the effects of stimulation by the sympathetic nervous system Reduces maximal heart rate Reduces resting and submaximal heart rate
Risks or Side Effects of Beta Blockers
Bradycardia-> may lead to heart block Hypotension, Bronchospasm, Fatigue, Decreased motivation Most are associated with prolonged use
Caffeine
Effects of Caffeine
CNS: Stimulates adrenal medulla to release epinephrine CV: Increased HR and contractility at rest, peripheral vasodialation,
diuretic Stimulated glycogenolysis, increased FFA mobilization
Side Effects of Caffeine
Diuretic, increased risk of arrhythmias, insomnia, tremors, addiction
Diuretics
Effects of Diuretics
Weight loss due to decreased extracellular fluid and plasma No evidence of potential ergogenic effect
Risks and Side Effects of Diuretics
Altered thermoregulation, electrolyte imbalances, fatigue, muscle cramps

Cardiac arrhythmias, death
Physiological AgentsBlood Doping- transfusion of red blood cells in order to increase oxygen carrying capacity, increase hemoglobin content, increase VO2 max, increase time to exhaustion
Risks of Blood Doping--Blood clotting, heart failure, transfusion rxn, disease transmission
Erythropoietin (EPO)- hormone produced by kidneys. Stimulates RBC production. Risks of EPO--Overproduction of RBC can cause thrombosis, MI, HTN, stroke
Oxygen Supplementation- increase in VO2 max, decrease in submax HR,↑ work capacity
Bicarbonate Loading- enhances the pH gradient in blood and creates a lactate efflux that decreases fatigue. Risks of Bicarbonate Loading
GI distress, cramping, bloating, diarrhea
ThermoregulationMetabolic heat production- 75% of energy produced is converted to heat.
Heat Related Disorders- acclimatization takes 9-14 days.
Heat Cramps- due to sodium loss in sweat Heat Exhaustion- thermoregulation still intact, body can’t compensate for
dehydration. Fatigue, dizziness, nausea, vomiting, fainting, weak rapid pulse Heat Stroke- thermoregulation not intact, core temp >104⁰, confusion,
disorientation, death
Cold Related Disorders
Hypothermia- hypothalamic regulation lost below 94.1⁰, decreased HR and respiration
Frostbite- occurs at 32⁰, severe vasoconstriction, tissue death.
Body CompositionObesity- excess amounts of adipose tissueBMI=Kg/m²
Normal BMI: 18.5-24.9 Overweight BMI: 25-29.9 Class I Obesity BMI: 30-34.9

Class II Obesity BMI: 35-39.9 Class III Obesity BMI: > 40
Body Composition Assessment Techniques
Waist/Hip ratio- increased abdominal fat=increased risk for HTN, diabetes, dyslipidemia. High Health Risk: Men>.95, Women>.86
Skinfold- abdominal, triceps, biceps, chest, med. calf, midaxillary, subscapular, suprailiac, thigh. Men & Women any seven sites. If using 3 sites: women use-tricep, suprailiac & thigh. Men use chest abdomen & thigh.
Bioectrical Impedance- estimates total body water and uses equations to measure body fat.
DEXA- provides regional estimates of bone, fat & lean tissue.
Exercise Testing & Prescription
Exercise PrescriptionMuscular Strength- maximal force that muscle can generate. 1RM, or isokineticallyMuscular Power- rate of work performanceMuscular Endurance- capacity to sustain repeated muscle contractionsAerobic Power- rate of energy released through aerobic metabolism, assed by VO2 maxAnaerobic Power- assessed with Wingate, shuttle tests
General Training PrinciplesIndividuality- who you’re working withSpecificity- train what you want to improveReversibility- gain can be lostProgressive Overload- increase intensity needed for improvementHard/Easy- high intensity followed by easy daysPeriodization- gradual cycling of specificity, intensity and volume of training
Comparison of the Effects of Endurance Training and Strength Training on Health and Fitness Variables
Variable Aerobic Exercise Resistance ExerciseBone mineral density ↑↑ ↑↑
(%Fat) ↓↓ ↓Lean Body Mass ↔ ↑↑
Strength ↔ ↑↑↑Insulin Response to Glucose
Challenge↓↓ ↓↓
Basal Insulin Levels ↓ ↓Insulin Sensitivity ↑↑ ↑↑

HDL-C ↑↔ ↑↔LDL-C ↓↔ ↓↔
Resting Heart Rate ↓↓ ↔Stroke Volume ↑↑ ↔
Blood Pressure at Rest –Systolic
↓↔ ↔
Blood Pressure at Rest –Diastolic
↓↔ ↓↔
VO2 Max ↑↑↑ ↑Endurance Performance ↑↑↑ ↑↑
Basal Metabolism ↑ ↑↑