exercise and disease ii urho kujala professor of sports & exercise medicine department of health...
Post on 21-Dec-2015
216 views
TRANSCRIPT

Exercise and Disease II
Urho Kujala
Professor of Sports & Exercise Medicine
Department of Health Sciences, University of Jyväskylä
Contents
• Musculoskeletal disease• Neurologic disease• Renal disease –bladder problems• GI-tract• Cancer• Infections• + Pulmonary disease (separate presentation)

Exercise and musculoskeletal disease
• Relations to other diseases
• Relations to functioning and disability
• Immobilization
• Sports and exercise in the prevention
• Exercise in the treatment and rehabilitation

Wang et al. www.plosbiology.org;
Oct 2004;vol 2; Issue 10; e294
(WT=wild typeTG=transgenic)
The role of interspecies differences has to be taken into accountwhen attempting to extend the results of animal experiments to humans!
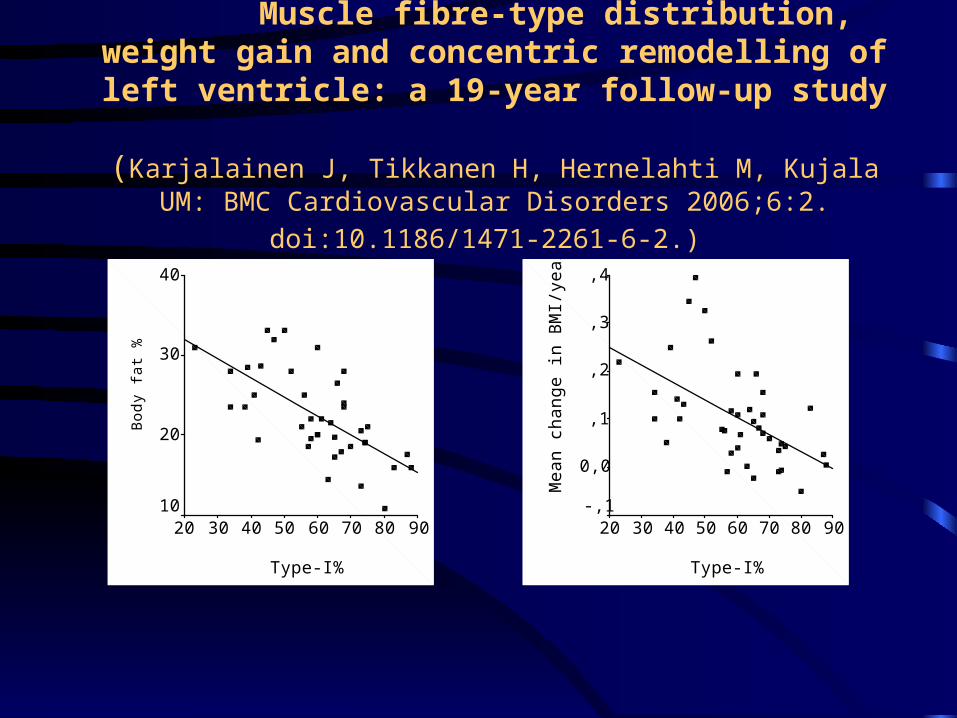
Muscle fibre-type distribution, weight gain and concentric remodelling of left ventricle: a 19-year follow-up study
(Karjalainen J, Tikkanen H, Hernelahti M, Kujala UM: BMC
Cardiovascular Disorders 2006;6:2. doi:10.1186/1471-2261-6-2.)
Type-I%
9080706050403020
Bod
y fa
t %
40
30
20
10
Type-I%
9080706050403020
Mea
n ch
ange
in B
MI/
year
,4
,3
,2
,1
0,0
-,1

Basics on functions of skeletal muscle
• Movement, posture, stability• Communication• Heat production, cold tolerance• Important role in metabolism/energy balance • Endocrine organ; ”myokines”(IL-6, -8, -15) and
myostatin partly control/regulate inflammation, energy expenditure, muscle growth and fat deposition.
NOTE: Skeletal muscle is a major mass peripheral tissue (about 36% for females and 42% for males)

Functions of bone
• Support
• Production of cells to circulation
• Calcium reserve/metabolism
• Associations to fat etc. Metabolism
• Endocrine functions

Sarcopenia
• Decrease in muscle mass is an important age-related change• Degreases in number and size of muscle cells and infiltration of fat
into muscle• Associated with increased risk of disability and death• Risk factors for sarcopenia; aging, nutrition, hormonal balance,
different diseases• Physical activity is the best preventive means• Muscle is important not only for producing work but olso for
metabolism, body temperature maintenance, and protein source• Muscle training among older people important for maintaining
mobility
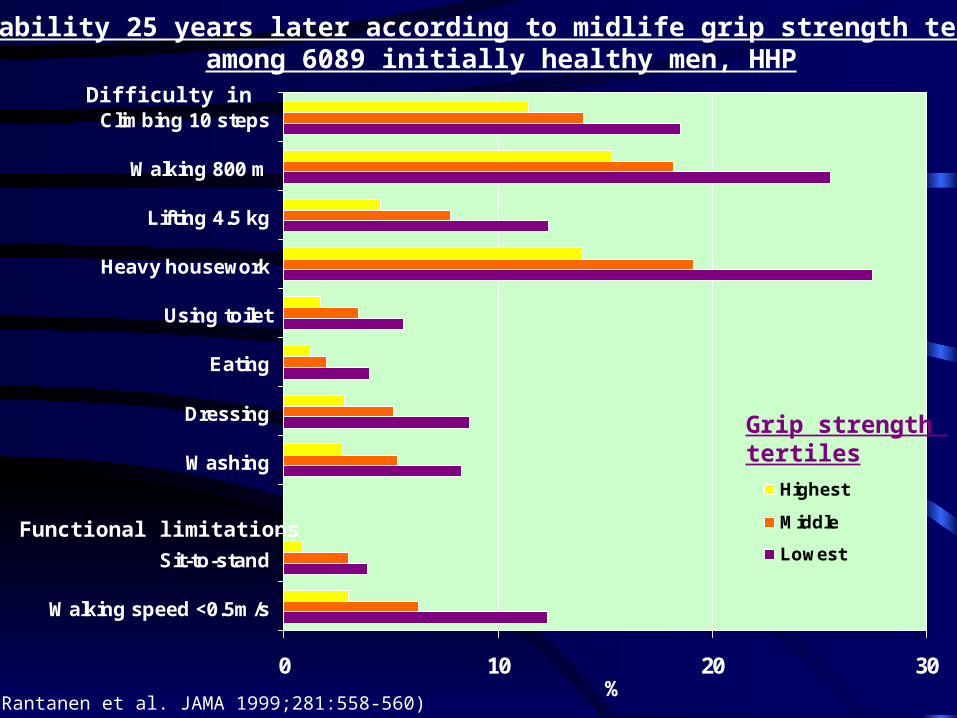
Disability 25 years later according to midlife grip strength tertilesamong 6089 initially healthy men, HHP
0 10 20 30
Walking speed <0.5m/s
Sit-to-stand
Washing
Dressing
Eating
Using toilet
Heavy housework
Lifting 4.5 kg
Walking 800 m
Climbing 10 steps
Highest
Middle
Lowest
Grip strength tertiles
%(Rantanen et al. JAMA 1999;281:558-560)
Difficulty in
Functional limitations

Biological Change Risk of Injury
Intensity of Exercise
Light Medium High
Risk of injury; profile A
Risk of injury; profile B
Benefit profile A
Benefit profile B
Net health benefit
What kind of evidencedo we need?
• Prevention; Observational studies to give general advice for healthy people?
• Treatment of patients with chronic disease using resourches of health care; RCTs are needed?
• Studies on the effects of exercise on the mechanisms of disease
Exercise recommendations and how to follow the recommendations
• Recommendations for the prevention of disease
• Recommendations in the treatment and rehabilitation of disease
• Contraindications/safety rules

Reduction of maxVO2 during bed rest (Greenleaf et al. J Appl Physiol 1989;67:1820-1826.)
-14
-12
-10
-8
-6
-4
-2
0
Day 0 Day 7 Day 14 Day 21
No exercise
Bicycle 30 min x 2 perdayMax leg ext and flex10 x 5 x 2 per day
Effects of immobilization on musculoskeletal system
• Bone• Cartilage• Muscle• Tendon(See: Bloomfield et al. Changes in
musculoskeletal structure and function with prolonged bed rest. Med Sci Sports Exerc 1997; 29: 197-206)
Osteoarthritis and exercise
• Osteoarthritis causes long-lasting physical activity limitations more than any other disease
Factors predisposing to osteoarthritis
• Overweight
• High work-related loading
• Joint injuries (leisure/sports and work)
• Genetic factors
• Other diseases (diabetes etc.)

HERITABILITY: TWIN STUDIES
• The genetic influence explains 39-65% of the variance in the occurrence of radiographic hand or knee OA in women
• OA-score; MZ - r=0.64 vs. DZ - r=0.38
• (Spector et al. BMJ 1996;312:940-3)

Kujala et al. British Medical Journal 1994;308:231-234.
Hospital discharge reportsICD 8 (1970-1985)ICD 9 (1986-1990)
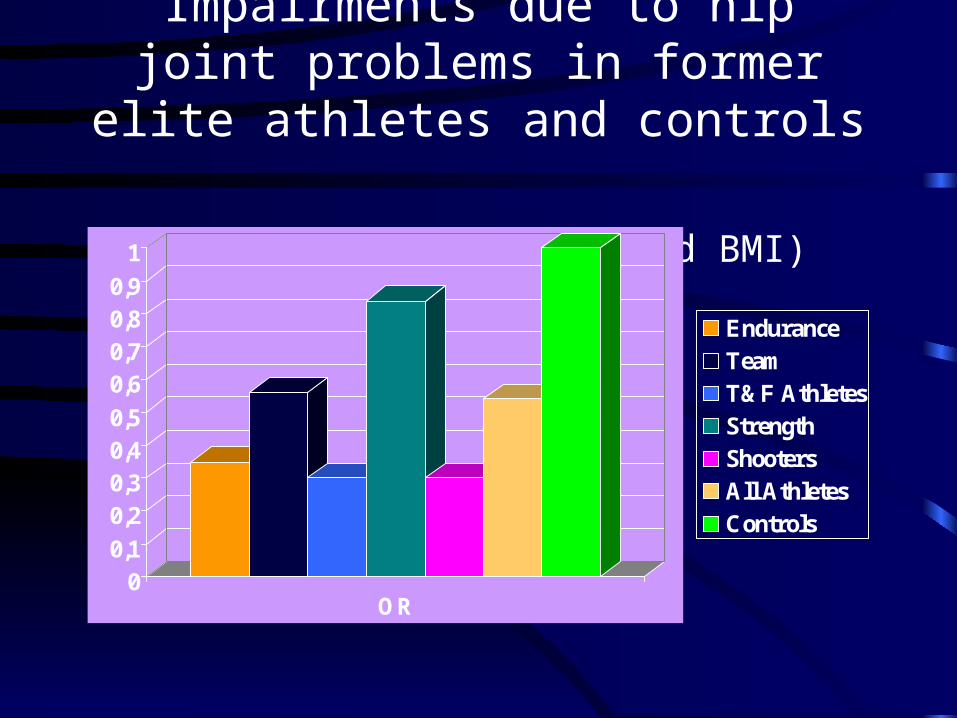
Impairments due to hip joint problems in former elite athletes and controls
(adjusted for age, SES and BMI)
00,1
0,20,30,40,5
0,60,70,80,9
1
OR
EnduranceTeamT&F AthletesStrengthShootersAll AthletesControls
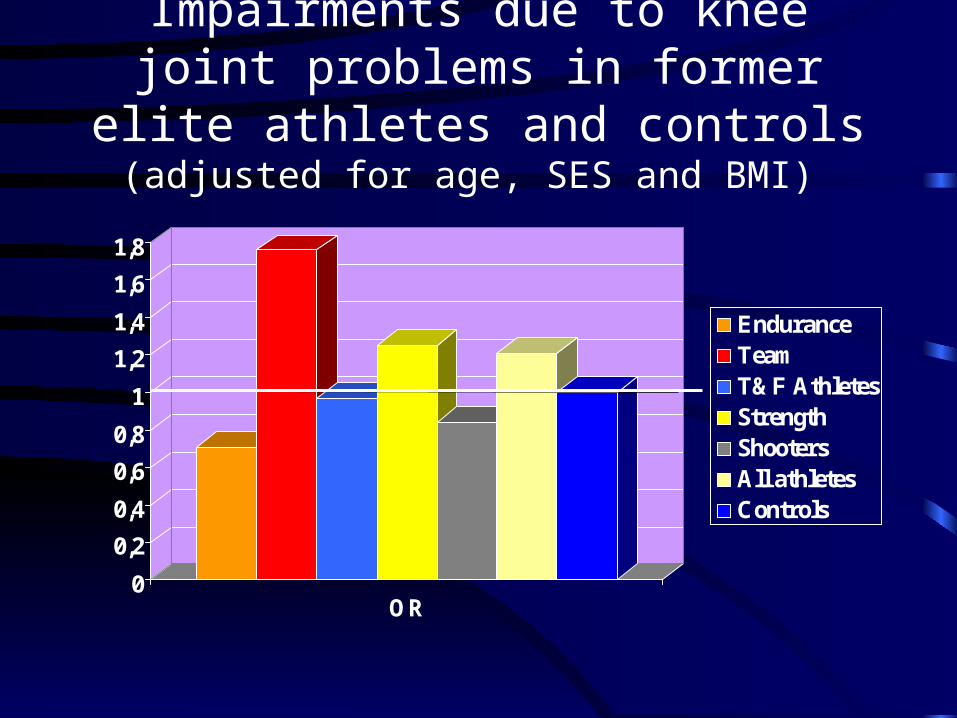
Impairments due to knee joint problems in former elite athletes and controls
(adjusted for age, SES and BMI)
0
0,2
0,4
0,6
0,8
1
1,2
1,4
1,6
1,8
OR
EnduranceTeamT&F AthletesStrengthShootersAll athletesControls

Sports or physical activity in the prevention of osteoarthritis
• Sports including high risk of joint injuries and very high impact loads increases the risk of osteoarthritis
• Low to moderate leisure physical activity without joint injuries does not increase the risk
• High work-related loading increases the risk of osteoarthritis
• Physical activity maintains function
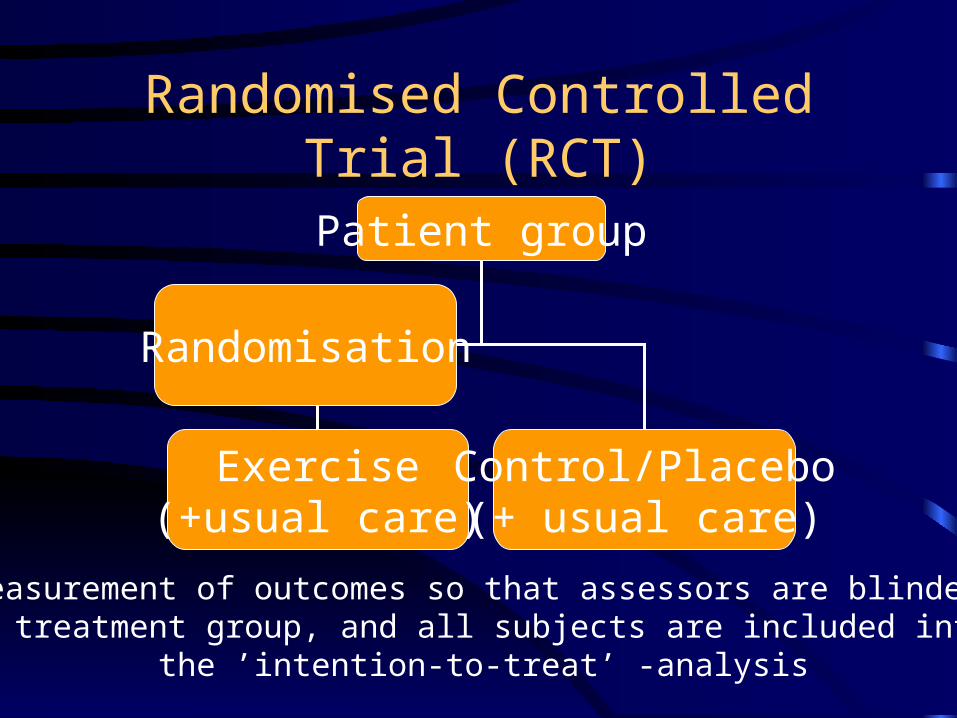
Randomised Controlled Trial (RCT)
Patient group
Exercise(+usual care)
Control/Placebo(+ usual care)
Randomisation
Measurement of outcomes so that assessors are blinded to treatment group, and all subjects are included into
the ’intention-to-treat’ -analysis

KNEE OA & EXERCISE• Randomized 18 mo trial; aerobic exercise vs.
resistance exercise vs. education• N = 439 subjects, age 60+• Conclusion: Older disabled persons
participating in aerobic or resistance exercise programs had modest improvements in measures of disability, performance and pain
• (Ettinger et al. JAMA 1997;277:64-66)
Statistical methods of meta-analyses
• Dichotomous (or binary) data; odds ratios (OR), relative risks (or relative effects), risk differences as well as absolute measures, such as the number needed to treat (NNT).
• For continuous data; weighted mean difference (WMD) is preferable when outcomes measured in a standard way. In case continuous outcomes are conceptually the same but measured in different ways, standardized mean differences (SMD).
• Heterogeneity between different studies; fixed effect vs. random effects analysis methods

Osteoarthritis – Contrast; ExerciseOutcome; Pain (Fransen et al.)

Osteoarthritis – Contrast; ExerciseOutcome; Physical function

Osteoarthritis
• Based on RCTs, land-based therapeutic exercise (with manual therapy or balance training in some studies) improved self reported pain and self-reported physical function in patients with knee osteoarthritis (Fransen et al., 2007).
• Both aerobic walking and home based quadriceps strengthening exercise reduce pain and disability but no difference between them was found on indirect comparison (Fransen et al. 2008, Roddy et al. 2005, Lange et al. 2008).
• The effect size of exercise in alleviating pain in hip OA has been shown to be compareable to that in knee osteoarthritis (Hernandez-Molina et al. 2008).
Osteoarthritis
• Aquatic exercise gives rather similar benefits as land-based exercise (Bartels et al. 2008). The effect of exercise on the progression of osteoarthritis is unclear.
• On the basis of 11 RCT:s Pisters et al. (2007) have analyzed long-term effects of exercise therapy in hip or knee osteoarthritis patients. The analysis showed that there is no long-term effectiveness on pain and self-reported physical function 6+ months after the treatment ended.
• Additional booster sessions seem to maintain some of the benefits and some benefit on patient global assessment of effectiveness may remain without booster sessions.
EXERCISE WITH OA:TRAINING PRINCIPLES
• Individual programmes and group-based programmes are equally effective; long-term compliance is a key factor. Utilise local resources.
• Remember: Movement, progressive muscle strengthening, ROM, aerobic training.
• Avoid: Injuries, high impact loads.

TAKE-HOME MESSAGE:EXERCISE AND OA
• Exercise associated injuries may lead to degenerative changes and OA
• Different types of training may help in the prevention or treatment of disability
• Can exercise help in the prevention of degenerative changes? No final evidence.
Yleinen liikuntasuositus
• Alaraajojen nivelrikkoa potevalle sopivat hyvin esim. uinti, pyöräily (huom. erit. ylipainoiset; ei kehon paino kipeän nivelen päällä), kävely
• Huonommin sopivat juoksu, pallopelit yms.
• Yläraajojen nivelrikkoa poteville sopii myös juoksu ym. esim. mailapelit huonommin

Vasta-aiheet ja varoitukset
• Yleensä kyseessä iäkkäät henkilöt, aina vähintään kardiovaskulaarianamneesi
• Kysytään kipeytymisistä, muunnetaan ohjelmaa
• Jos nivelen lukkiutumisia, pahenevaa nivelturvotusta ym. arvioidaan kliininen tilanne ja harjoituskelpoisuus uudelleen
Ryhmäohjelman toteutus• Aluksi esim. 3 x viikko x 1 tunti, myöhemmin
käyntejä harventaen ja kotiohjelmaa opastaen
• Nousujohteinen
• Sisätö: Lämmittely (esim. kuntopyörä, kävely), venyttely, kuntopiiri 2 x (2x10 liikettä) sisältäen mm. polven ojentajien ja koukistajien harjoituksia + esim istumasta ylös nousu, verryttely/venyttely

Exercise and the prevention of rheumatoid arthritis
• There is no clear evidence on that exercise pedisposes to or prevents from rheumatoid arthritis

Rheumatoid arthritis
• On the basis of more than 10 RCTs exercise therapy seems to be effective at increasing aerobic capacity and muscle strength in patients with rheumatoid arthritis though good meta-analyses are lacking (Kettunen and Kujala 2004, Van den Ende et al., 2004, Metsios et al. 2008).
• Also on the basis of 3 RCTs in patients with juvenile idiopathic arthritis under 18 years of age the functional ability tended to be better after exercise therapy (Takken et al. 2008).
• No detrimental effects on disease activity and pain were observed in these trials.
• The effects of dynamic exercise therapy on radiological progression and cardiovascular disease need further studies (Kettunen and Kujala 2004, Van den Ende et al., 2004, Metsios et al. 2008).
• Disease activity?

EXERCISE WITH RA:TRAINING PRINCIPLES
• Individual programmes and group-based programmes are equally effective; long-term compliance is a key factor. Utilise local resources.
• Remember: Movement, progressive muscle strengthening, ROM, aerobic training.
• Avoid: Injuries, high impact loads.

TAKE-HOME MESSAGE:EXERCISE AND RA
• Different types of training may help in the prevention or treatment of disability
• Aerobic exercise helps in maintaining cardiovascular function (remember co-morbid conditions)
• Can exercise help in the prevention of degenerative changes? No final evidence.
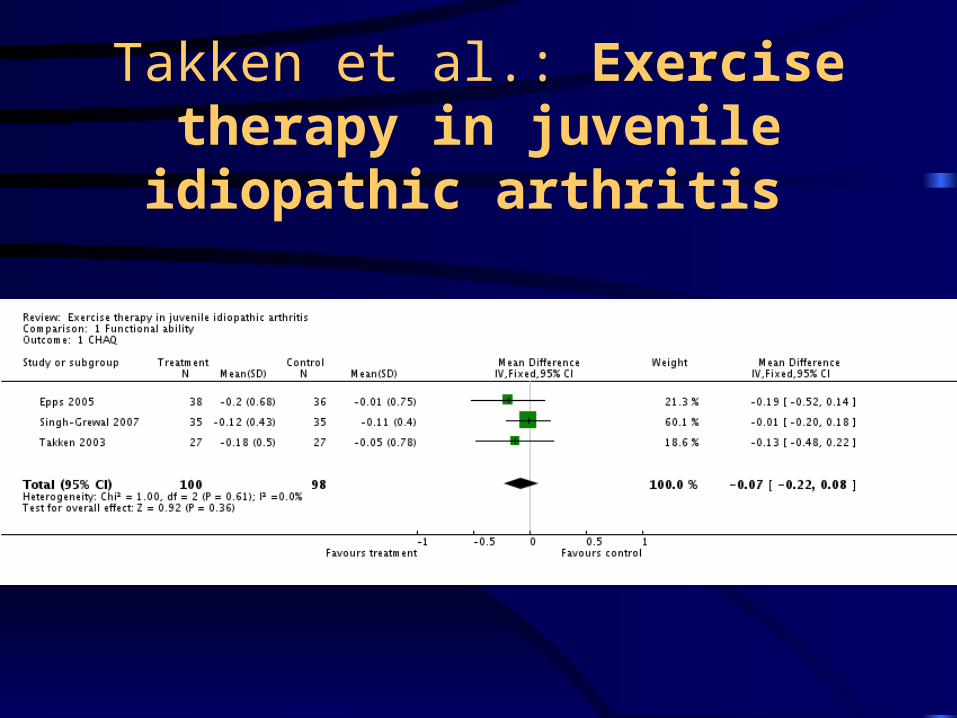
Takken et al.: Exercise therapy in juvenile idiopathic arthritis
Exercise after total joint replacement
• There is some evidence based on RCTs that perioperative (Gilbey et al. 2003) and postoperative (Maire et al. 2003) exercise therapy improves early functional recovery after total hip arthroplasty.
Exercise after total joint replacement
• Consensus statements say that participation in no-impact or low-impact sports (swimming, cycling etc.) can be encouraged, but participation in high-impact sports (running, ball games, racquetball etc.) should be prohibited after TJR (McGrory et al. Mayo Clin Proc 1995;75:342-348).
• There is some evidence of increased surface wear rate (Dubs et al. Arch Orthop Trauma Surg 1983;101:161-169) and of increased aseptic loosening rates (Kilgus et al. Clin Orthop 1991;269:25-31) in active patients.
Ankylosing spondylolitis
• Four RCTs compared exercise program with no intervention and reported some increases in spinal mobility and physical function (Dagfinrud et al., Cochrane Review 2008).
• Training of ROM and muscle strength are effective.

Low back pain

Exercise in the prevention of low back pain
• Leisure physical activity does neither predispose to nor prevent from LBP
• Good muscle function does neither predispose to nor prevent from LBP
• High work-related loading predisposes to LBP• Traumatic sports predisposes to degenerative
changes and pain episodes• Physically active have better function
Low back pain
• Acute back pain – Exercise does not help (strong evidence); subacute back pain – no help
• Chronic low back pain; effect on pain based on 8 RCTs -10.2 units (95% CI; -19.09, -1.31) on a scale from 0 to 100.
• Effect on function is smaller (target group has an effect) • Exercise may be helpful for chronic LBP patients to
increase return to normal daily activities and work.(Hayden et al. Cochrane Database Syst Rev)

LBP- Hayden et al. Updated review
EXERCISE WITH CHRONIC LBP:TRAINING PRINCIPLES
• Non-traumatic exercise that helps in increasing ordinary activity.
Best exercise programme?
• Indirect comparisons using Bayesian multivariable random-effects meta-regression (Hayden et al. Ann Intern Med 2005;142:776-786)
• Compared to non-supervised home exercises the improvements were higher for:
Individually designed programs 5.4 points Supervised home exercise 6.1 p. Group and individually supervised program 5.9 p.
TAKE-HOME MESSAGE:EXERCISE AND LBP
• Exercise associated injuries may lead to degenerative changes
• Different types of training may help in the prevention or treatment of disability
• Can exercise help in the prevention of degenerative changes? No final evidence.

Neck and shoulder pain
Chronic non-specific neck-shoulder pain syndrome
• 5% of Finnish men and 7% of Finnish women (Mini-Finland health survey)
• Patholic-anatomic causes can be determined in only a small proportion of cases; imaging methods focus on excluding severe underlying causes
• Pain originates from muscles?, other soft tissues?, facet joints?, intervertbral discs?
Classification
• Neck vs shoulder• Neck pain:
1. Local
2. Radiating
3. Whiplash
4. Myelopathy
5. Others: generalized diseases, neoplasms, fractures etc.
Neck pain and exercise/loading
• Severe neck pain is often associated with mood problems and fear of exercising and loading; choose activities that do not provocate problems
• Risk-factors: static loading of upper extremities (in upward positions), high wrk-related loading, low socio-economic position etc.

Physical activity and prevention of neck pain
• No clear associations
Neck pain - treatment
• Avoid bed rest at acute phase – normal daily activities if tolerated
• Associated symtoms such as headache may be provocated/increased by exercise
• Training has been shown to be effective in the treatment of chronic neck pain and whipplash injury in case it focuses specifically on neck and is repeated often and long enough

New Finnish RCTs on the effects of training on chronic neck pain
• Viljanen et al. BMJ 2003; no effect (training of upper extremities with low frequency)
• Ylinen et al. JAMA 2004; training beneficial (specific training for neck musculature with higher frequency; strength training and endurance type training equally effective on pain)
Fibromyalgia
• Fibromyalgia manifests as chronic pain and fatigue/tiredness
• Symptoms are non-specific and the patophysiology is unknown
• Peripheral muscles are normal• The abnormality may be related to experiencing pain at the
level of CNS• Diagnosis: rule out other specific diseases, no diagnostic
tests - typical symptoms and signs; wide-spread, continuous, symmetrical pain symptoms – tender point palpation often used
Exercise in the prevention of fibromyalgia
• Exerise does not prevent from fibromyalgia
• Young athletes usually do not have fibromyalgia?
• Explanation: Central mechanisms
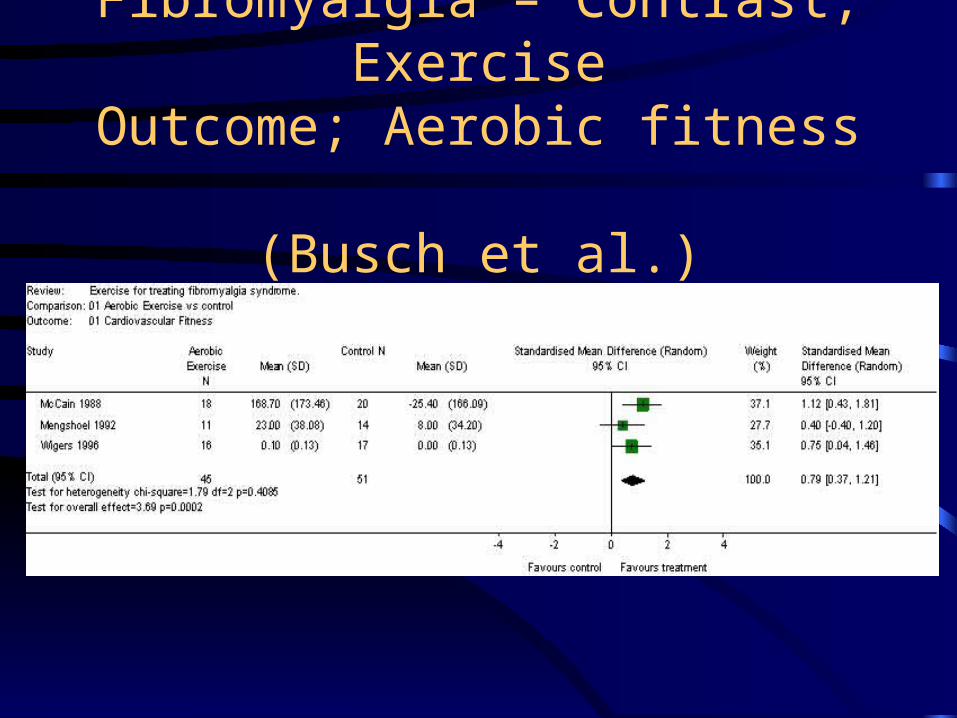
Fibromyalgia – Contrast; ExerciseOutcome; Aerobic fitness
(Busch et al.)
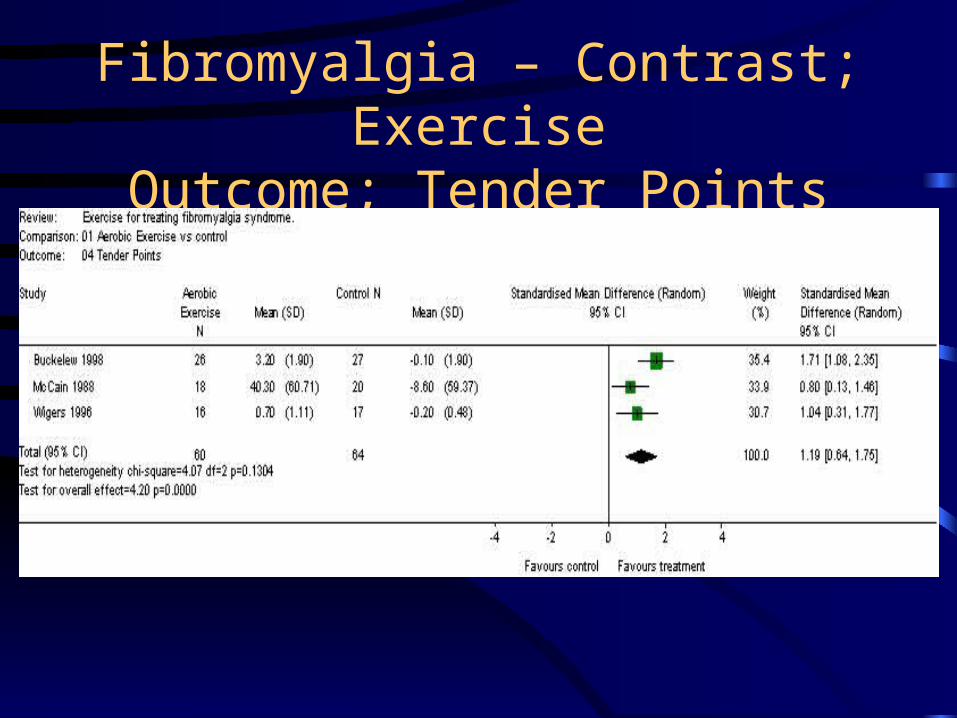
Fibromyalgia – Contrast; ExerciseOutcome; Tender Points
Fibromyalgia
• Based on RCTs aerobic exercise improves
• Function• Global well-being• Pain • Possibly tender-point pressure threshold(Busch et al. Cochrane Database Syst
Review 2008)
EXERCISE WITH FIBROMYALGIA:TRAINING PRINCIPLES
• Training is important for preventing disability
• Different types of non-exhaustive aerobic or strength training which is tolerated by the patient, there may be daily variation in what the patient tolerates
• Aerobic and muscular training response is normal
Training program for fibromyalgia
• Regular frequency is preferred: daily 15-60 min (an inactive day after exercise day may be difficult)
• More than 3 hours per week• Low to moderate intensity (HR 110-130/min)• Strength training max 2-3 times weekly with max 50%-
65% of one repetition maximum, 10-12 repeats, total session duration may have daily variation, warm-up necessary
• Exercise types: walking, swimming, strength training
TAKE-HOME MESSAGE:EXERCISE AND FIBROMYALGIA
• Different types of training may help in the prevention or treatment of disability.
EXERCISE AND OSTEOPOROSIS
• Exercise helps in the prevention and treatment of osteoporosis.
• Exercise may both predispose to or prevent from falls and fractures.
• High activity level delays the occurrence of hip fractures based on observational studies

Neurologic disease
MS
Parkinson
Impairment of congnitive function and dementia
Epilepsy
CP
Myopathies
Pheripheral nerve diseases

Headache
• Subjective symptom; primary vs. secondary
• Dynamic aerobic exercise seems to prevent tension type headache. Low to moderately intensive dynamic exercise without static loading to neck-shoulder-upper extremities
Headache
• Postexercise headache (after static loading/strength training exercise; 5 min – one day)
• Effort headache (during running etc., 4-6 hours)
• Headache after contacts (soccer, boxing etc.), prevalence ad 50%

MS
• Autoimmunologic demyalinization disease (CNS); a) ralapsing intermittent, b) progressive
• Spasticity, balance and motor ability problems, muscular weakness, fatique
• Exercise in the prevention of MS: no role• Recommend: Dynamic aerobic exercise – interval
type in case of fatique• Avoid: Contact sports, warm environments,
training during infection• Morning is better

Exercise and MS – the evidence
• Based on six RCTs (157 patients) best evidence synthesis showed strong evidence in favour of exercise therapy compared to no exercise therapy in terms of muscle power function, exercise tolerance functions and mobility related activities in patients with multiple sclerosis
• Moderate evidence - improving mood. • No evidence - fatigue and perception of handicap.
Rietberg et al. Cochrana Database Syst Rev 2005).

Parkinson’s disease
• Chronic progressive degenerative disease of CNS; dopaminergic tract between substantia nigra – striatum
• Tremor, rigidity, hypokinesia, fatique, disturbances in proprioception and balance
• Exercise in the prevention: no role• Treatment and rehabilitation: Regular daily
activities/exercises according to indiviual health status + stretching
• Avoid: Sports and exercise with injury risk (hip fracture risk!)
Parkinson’s disease
• According to meta-analysis exercise therapy/exercise-based physiotherapy improved physical functioning (7 trials; SMD -0.47 (-0.82, -0.12) ) and health-related quality of life (4 trials; SMD -0.27 (-0.51, -0.04) ) in patients with Parkinson’s disease (Goodwin et al. 2008). In addition,exercise groups had improvements in balance in 4 of 5 trials and in walking speed in three of four trials (Goodwin et al. 2008).
Impairment of congnitive function and dementia
• Based on RCT:s Exercise training increases congnitive performance in elderly persons with congnitive impairment and dementia (Heyn et al. Arch Phys Med Rehabil 2004;85:1694-704)
• In observational cohort studies an association betfeen high physical activity and low incidence of dementia (Larson EB et al. Ann Intern Med 2006;144:73-81)
Epilepsy
• Convulsions• Side effects of medical treatment: tiredness,
hyponatremia• Exercise does not provocate convulsions• Normal health enhancing and school
exercises/sports• Not recommended: contact sports, sports
with injury risk
Cerebral palcy (CP)
• CNS injury before birth or until the age of 2 years
• Spastic or dyskinetic-dystonic or atactic
• Physical exercise capacity usually lowered
• Rehabilitaion: exercise, physiotherapy, surgery
Muscle diseases
• Different types of dystrophias and myopatias
• Exercise has no role in prevention
• Exercise and physiotheraphy are the best ways in maintaining motor abilities

Neuro-muscular synapse
• Myastenia gravis most common (antibodies for acethylcholine receptors)
• Cholinergic medications: exercise optimally 1-2 hours after taking medicine, 10 mg pyridostigmin if necessary
• Exercise important in rehabilitation but avoid fatique
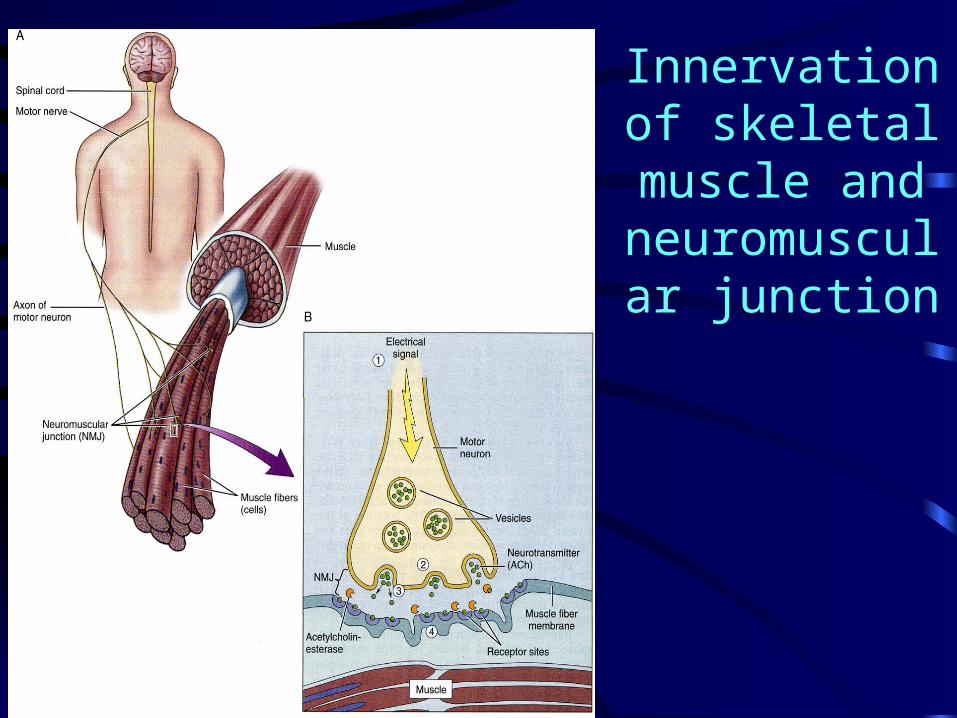
Innervation of skeletal muscle
and neuromuscular
junction

Disorders of the neuromuscular junction

Neuropathias
• Mechanical nerve injury (entrapment, vulnus, fracture etc.); functional deficiencies
• Polyneuropathy (common reasons: alcoholism, diabetes); scin injuries

Renal diseases and exercise
• Exercise proteinuria – benign
• Exercise haematuria
• Rhabdomyolysis
• Chronic renal insufficiency and lowered exercise capacity
Exercise and renal function
• Exercise -> sympathicus activation -> contraction of renal artery -> lowered renal blood flow (ad 75%)
• Lowering of glomerular filtration rate (GFR) (ad 50%), increase in filtration fraction
• Increased antidiuretic hormone (ADH) – lowered excretion of urine
• Increased aldosterone -> Na retention• Incresed number of cells in urine
Exercise proteinuria
• Plasmaproteins • Glomerular permeability increases• Tubular reabsorption decreases• Last maximally 24-48 hours after exercise• Normal 150 mg/day – exercise proteinuria usually less
than 500 mg/day. • Test sensitivity 200 mg/l; wrong positive findings:
concentrated urine (ex), blood in urine (ex), alcalic urine (infection).
• Among young; orthostatic protinuria (max 1.5 gr/day)• => Overnight urine collection after a day without exercise

Exercise haematuria
• Microscopic or macroscopic• Disappears usually within two days after exercise• From kidney or bladder• Hypoxic damage in nefrons -> increse in
glomerular permeability• Contact sports – mechanical injuries• Running etc. -> injury due to microtrauma,
epithelial bladder injury after marathon run• Control sample 24-72 h after exercise -> in case +
rule out other reasons, such as glomerulonefritis
Acute renal insufficiency
• Rhabdomyolysis; common reasons are alcohol and medications, exercise may cause alone or more commonly contribute together with others
• Exercise -> swelling of muscle -> cell death -> myoglobin out of muscle -> ferrihematin in acidic urine -> tocsic for tubular cells -> tubular necrosis (-> anuria -> death)
• Diagnosis; increase of creatine kinase (CK)• Treatment; correction of dehydration +
alcalisation (natriumbicarbonate), sometimes dialysis or fasciotomies

Chronic renal insufficiency
• Lowered physical capacity• Reasons: accumulation of uremic toxins and
cardiovascular, endocrinic, metabolic, musculoskeletal, neurologic, haematologic complications.
• Hypertension, left ventricular hypertrofy and function abnormality, myocardial fibrosis, heart valve calcifications, hyperlipidemia, glucose intolerance, hyperinsulinemia, abnormalities in androgens tiredness, headache, muscular cramps, pericarditis, pleuritis, oedems, coronary heart disease, secondary anemia, hyperkalemia, metabolic asidosis, muscular athrophy
• Physical activity may delay occurrence of diasbility
Stress urinary incontinence
• More common in females (about 20% of adults, among older people even more common)
• Endurance running (38%), aerobic (22-36% depending on the number of jumps)
• Other risk factors: age, number of children (normal labours)
Stress urinary incontinence
• Problems in: aerobic, running, basket ball, wolley ball, squash, badminton, hand ball, tennis, dance, gymnastics, trambolin
• Recommend: walking, golf, joga, biking, swimming

Urinary incontinence and PFMT
• Women who did pelvic floor muscle training (PFMT) were more likely to report they were cured or improved than women who did not. PFMT women also experienced about one fewer incontinence episode per day (Hay-Smith & Dumolin, Cochrane Database Syst Rev, 2007)
• PFMT + bladder training consistently increased continence rates (see meta-analysis by Shamliyan et al. Ann Intern Med 2008;148:459-473)

Urinary incontinence - Treatment
• Stress incontinence: prevention, pelveo-building, medications (contracting urethra), operative treatment (TOT), equipments
• Urge incontinence: medications relaxing bladder muscles (anticholinergic)
Gastro-intestinal tract
• Reflux-esophagitis
• Gastro-duodenal function
• Colon function
• Exercise is associated with lower incidence of: colon cancer, biliar stones, obstipation

Exercise and reflux/esophagitis
• Mild symptoms common, ad 50% of endurance athletes; more common when exercise less than 3 hours after meal, risk 3 times higher 45 min after meal.
• Other risk sports; weight lifting• Causes: mechanical, gi-tract motor disturbances,
decrease in blood circulation• Diagnostics: problems at rest or not?• Note: Association with asthma
Exercise and gastroduodenal function
• 70% of maximal oxygen uptake; delayed emptying of ventricle; symptoms during exercise (nausea, vomiting, pain)
• Acid secretion decreases during maximal exercise
• Low to moderate exercise may increase motility
Exercise and colon function
• Normal passing time 20-60 hours
• Exercise shortens
• Runners diarrea
• Sympathicus –parasymphaticus balance?
• Changes in circulation; ischemic colitis;
(->anemia)
Cancer
• Colon
• Breast
• Prostata
• Lungs
Exercise and colon cancer; prevention
• Based on epidemiologic observational follow-ups risk for colon cancer is 30-40% lower in physically active males and females compared to sedentary
• Mechanism(s): (?) passing time, immune system, lower insulin and insulin like growth factors, lower obesity, etc.
Exercise and breast cancer; prevention
• Risk of breast cancer in physically active (at least two hours/week moderate to vigorous activity) women is 30-40% lower compared to sedentary
• Mechanisms (?): lower estrogen levels, lower obesity, lower insulin and insulin like growth factors, immune system, etc.
Exercise and other cancers; prevention
• Prostata ca: Lower testosterone helps in prevention; contradictory evidence on the association between ca and exercise
• Exercise and cancer of endometrium, ovaria, testis, pancreas, kidney, bladder and blood insufficiently studied
Exercise after ca-diagosis
• No evidence on that exercise has an effect on the prognosis of cancer; other treatments of prmary importance
• Physical activity can improve fitness, decrease depression and disability
• Problems: tiredness, weight changes, anemia, ca-treatments have effects on fitness and side-effects, risk of infections, etc.
• Exercise: low intensity, low progression, individual problems
Exercise and breast cancer
• Improvements in quality of life parameters (FACT-G and FACT-B scales)
• Improvements in aerobic fitness
McNeely et al. CMAJ 2006;175:34-41
Exercise and depression
• Patients with depression are less physically active; regular exercise may prevent from depression (observational data)
• Physical activity has a role in the treatment of depression, can be combined with medical treatment, effect compareable to psychotherapy, combination of exercise and light, long-term compliance is important

Depression
• Based on 9 low quality RCTs exercise treatment decreased Beck depression inventory score (weighted mean difference -7.3 (95% CI -10.0 to -4.6)
(Lawlor and Hopker. BMJ 2001;322:763-767)
Depression and exercise – Study example: Dunn et al. Am J Prev Med 2005;28:1-8.
Exercise treatment for depression. Efficacy and dose response.
• Mild to moderate major depressive disorder• Randomized 2x2 factorial design; 5 groups: (1) low dose/3
x wk; (2) low dose/5 x wk; (3) public health dose/3 x wk; (4) public health dose/5 x wk; (5) control/3 x wk flexibility exercise
• 12 wk supervised laboratory (treadmill/bicycle) exercise program
• 17-item Hamilton Rating Scale for Depression• Public health dose exsercise was effective treatment, but
low dose was compareable to placebo. Frequency played no role.
Exercise and anxiety
• Anxiety decreased during exercise and two hours after exercise
• Regular long-lasting aerobic exercise has long-term benefits
• Panic is first decreased more effectively using medication but in long term (10 weeks) exercise is as good as medication

Chronic fatigue syndrome
• Illness characterized by persistent medically unexplained fatigue of at least 6 months
• Exercise therapy vs. control (Edmonds et al. Cochrane review):
Based on 5 studies (286 participants) those receiving 12 we exercise therapy were less fatigued than controls (Chalder fatigue scale; SMD -0.77; 95% CI -1.26,-0.28)
Based on 3 studies (162 participants) physical functioning improved (Quality of life – SF-36 physical functioning subscale; SMD -0.64; 95% CI -0.96, -0.33)
Dependence
• Compulsory exercise despite of tiredness -> predisposes to social problems, fatique, injuries and even death when older people or patients with infections exercise too intensively
• Endorphins may contribute• Exercise may be a means to handle with negative feelings• Specific personality characteristics (demanding) may
predispose to exercise dependence• Exercise seems to stimulate different pathways in CNS
some of which lead to positive feelings
Infections and exercise
• Fever: no exercise• Generalized symptoms (muscle ache or pain,
headahe etc.): no exercise• First 1-3 days of an infecton: be careful, follow
what is the course of infextion• Cold; take it easy for three days, gradual start of
exercise (dd: allergic symptoms)• Cold, sore throath, cough; follow the progression
of symtoms then as cold
Infections and exercise
• Sore throath alone: rest; in case of angina antibiotics 10 days, rest 7 days
• Sinuitis, bronchitis, pneumonia; rest• Mononucleosis; avoid strenuous exercise 1
month• Lower urinary tract infection; rest until
symptoms are away• Gastroenteritis; avoid strenuous exercise

Infections and exercise
• Scin infections: according to severity• Erythema migrans/borreliosis: antibiotics 10 days, rest 7
days• Herpes: no sports where skin contacts, in case of general
symptoms and enlarged lympho nodes – rest• Genital infections; evoid strenuous exercise, during
antibiotic treatment of non-symptomatic clamydia infection –rest
• HIV, hepatitis B and C positive; exercise allowed, recommend non-contact sports (in case of wounds sports not allowed for anybody)

Genetic/Social/Environmental FactorsGenetic/Social/Environmental Factors
FitnessBehavior Outcome
Smoking/Alcoholconsumption
Stress Management
Physical Activity
Diet
Morphologic Components
Health Outcome
Muscular Component
Metabolic component
Cardiorespiratory Component
Motor Component