examination skills masterclass hughes exam skills...staff development programme 2010 5 precordium...
TRANSCRIPT

Examination Skills
Masterclass Royal Blackburn Hospital Wednesday 10th March 2010
Dr Richard Hughes
Staff Development Programme 2010
2
Contents
INTRODUCTION
3
CVS EXAMINATION – CRIB SHEET
4
CVS EXAMINATION – DETAILED LIST
7
RESPIRATORY EXAMINATION – CRIB SHEET
12
RESPIRATORY EXAMINATION – DEATILED LIST
14
ABDOMINAL EXAMINATION – CRIB SHEET
19
ABDOMINAL EXAMINATION – DETAILED LIST
21
ACKNOWLEDGEMENTS
27
Staff Development Programme 2010
3
Introduction
This booklet is designed to aid in clinical examination skills.
The aim is to outline a systematic approach to clinical examination that is valid
for both students and doctors sitting post-graduate examinations.
Each section is laid out in a similar manner, with a ‘crib sheet’ that can be used as
an aide memoire followed by a more detailed explanation of the examination
technique.
I hope you find the booklet useful and enjoyable.
Dr Richard Hughes MBChB MRCP MCEM
SpR in Emergency Medicine
Sub-specialty Acute Medicine
Staff Development Programme 2010
4
Cardiovascular Examination – Crib Sheet
• Introduce yourself
• Wash hands
• Position patient supine at 450
• Expose patient above the waste and also below the knees
• General Inspection
o Scars (sternotomy, scars from saphenous vein donation to CABG)
o SOB
• Hands
o Clubbing
o Splinter haemorrhages
o Quincke’s sign
o Osler’s nodes
o Janeway lesions
o Xanthomata on extensor tendons
• Radial pulses (both at same time)
• Brachial pulse
• Check for collapsing pulse
• Eyes
o Anaemia
o Xanthelasmata
o Corneal arcus
• Face
o Malar flush
• Mouth
o Central cyanosis
• JVP and hepatojugular reflex
• Carotid pulse for character
o Slow-rising (aortic stenosis)
o Collapsing (aortic regurgitation)
o Jerky (hypertrophic cardiomyopathy)
Staff Development Programme 2010
5
Precordium
• Inspection
o Scars
o Breathing
o Visible apex
• Palpation
o Apex beat (normally 5th IC space, mid-clavicular line)
o Parasternal heave
o Aortic thrill
Auscultation
• Left-sided heart murmurs are heard best in expiration
• Right sided heart murmurs are heard best in inspiration
• Palpate the carotid whilst listening over precordium to enable timing of
any murmur
• Listen over the four valve areas with the diaphragm to see if any murmurs
are heard:
o Mitral valve - apex
o Tricuspid valve – 4th IC space, left sternal edge
o Pulmonary valve – 2nd IC space, left sternal edge
o Aortic valve – 2nd IC space, right sternal edge
• Go back to apex and listen for:
o Mitral regurgitation
� Pansystolic murmur
� Heard best over apex
� Radiates to axilla (demonstrate this by listening here)
o Mitral stenosis
� Listen with bell
� Mid-diastolic murmur
� Heard best:
• Over apex
• In expiration
• With patient rolled onto left side
Staff Development Programme 2010
6
• Go back to aortic valve region and listen for:
o Aortic stenosis
� Ejection systolic murmur
� Radiates to carotids (demonstrate this by listening here –
also listen for carotid bruits)
o Aortic regurgitation
� Early diastolic murmur
� Heard best:
• In 2nd aortic area (3rd or 4th intercostal space, LSE)
• With patient lent forwards
• In expiration
• Keep patient sat forwards and:
o Listen for crackles at lung bases
o Palpate for sacral oedema
• Lay patient back to 450
• Palpate for ankle oedema
• To complete
o Blood pressure in both arms
o Look at obs chart
o Palpate all peripheral pulses
Staff Development Programme 2010
7
Cardiovascular Examination – Detailed List
General
Compared with the respiratory examination and abdominal examination, there is
probably more variation in the way a ‘textbook’ cardiovascular examination is
conducted.
Also, the examination should take on a different emphasis depending on what is
found. For example, if I saw giant 'cV' waves in the JVP, I would:
• Listen carefully over the 4th IC space left sternal edge with the breath held
in inspiration to listen for tricuspid regurgitation
• Feel for pulsatile hepatomegaly
I do neither of theses as part of my routine examination. Therefore, the list
below is not exhaustive, but forms a framework to cover most common ‘PACES-
style’ cardiology patients and forms a good baseline examination to teach
students.
It is clearly important to check the blood pressure as part of a cardiovascular
exam. Some people say “I would now check the blood pressure” as they palpate
the brachial pulse. Some people (like me) leave it until the end. I don’t think it
matters as long as you say you would do it.
There are many, many signs associated with cardiac disease (for example, with
aortic regurgitation). I make no apology for not including them all!
Introduce yourself
Wash hands
Position patient supine at 450
Expose patient above the waste and also below the knees
General Inspection
• Scars
o The saphenous veins are the most commonly used vessels for
coronary artery bypass grafts
o The presence of a midline sternotomy scar in the absence of scars
on the legs should alert the examiner to the likely diagnosis of a
prosthetic valve replacement
Staff Development Programme 2010
8
o Things often aren’t that easy, though, as many patients have a
CABG and valvular replacement at the same time and so will have
both types of scar
• SOB
Hands
• Clubbing
o Congenital cyanotic heart disease
o Subacute bacterial endocarditis
• Splinter haemorrhages
o Infective endocarditis
• Quincke’s sign
o Alternate flushing and paling of the nail bed when pressure is
applied to the tip of the nail. Seen in aortic regurgitation.
• Osler’s nodes
o Small, painful, purplish nodules at finger pulps. Seen in infective
endocarditis.
• Janeway lesions
o Pink palmar macules. Seen in infective endocarditis.
• Xanthomata on extensor tendons
o Familial hypercholesterolaemia
Radial pulses (both at same time)
• Radial-radial delay may be felt with coarctation of the aorta
Brachial pulse
Check for collapsing pulse
• Also called ‘water hammer’ pulse
• With aortic regurgitation
• Best felt by raising patient’s arm and feeling the radial pulse ‘slap’ against
your fingertips or palm
Eyes
• Anaemia
• Xanthelasmata
• Corneal arcus
o White deposit in the cornea near the periphery - indicative of
hypercholesterolemia among those under the age of 60
Face
• Malar flush. This may be a sign of pulmonary hypertension, of which
mitral stenosis is a cause.
Staff Development Programme 2010
9
Mouth
• Central cyanosis. Seen with cyanotic heart disease.
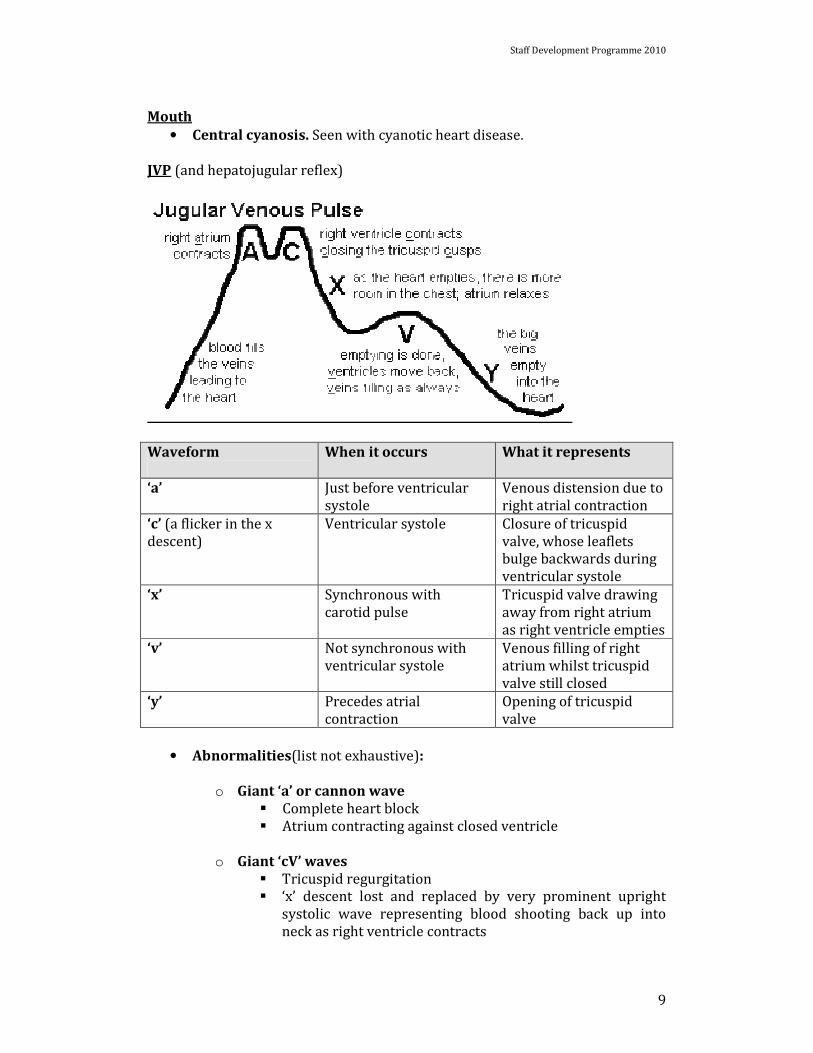
JVP (and hepatojugular reflex)
Waveform
When it occurs What it represents
‘a’ Just before ventricular
systole
Venous distension due to
right atrial contraction
‘c’ (a flicker in the x
descent)
Ventricular systole Closure of tricuspid
valve, whose leaflets
bulge backwards during
ventricular systole
‘x’ Synchronous with
carotid pulse
Tricuspid valve drawing
away from right atrium
as right ventricle empties
‘v’ Not synchronous with
ventricular systole
Venous filling of right
atrium whilst tricuspid
valve still closed
‘y’ Precedes atrial
contraction
Opening of tricuspid
valve
• Abnormalities(list not exhaustive):
o Giant ‘a’ or cannon wave
� Complete heart block
� Atrium contracting against closed ventricle
o Giant ‘cV’ waves
� Tricuspid regurgitation
� ‘x’ descent lost and replaced by very prominent upright
systolic wave representing blood shooting back up into
neck as right ventricle contracts

Staff Development Programme 2010
10
Carotid pulse for character
• Slow-rising (aortic stenosis)
• Collapsing (aortic regurgitation)
• Jerky (hypertrophic cardiomyopathy)
Precordium
• Inspection
o Scars
o Breathing
• Palpation
o Apex beat (normally 5th IC space, mid-clavicular line)
� Tapping apex – mitral stenosis
� Sustained apex beat – aortic stenosis
� Thrusting apex – aortic regurgitation
o Parasternal heave (right ventricular hypertrophy)
o Aortic thrill (aortic stenosis)
Auscultation
• Left-sided heart murmurs are heard best in expiration
• Right sided heart murmurs are heard best in inspiration
• Palpate the carotid whilst listening over precordium to enable timing of
any murmur
• Listen over the four valve areas with the diaphragm to see if any murmurs
are heard:
o Mitral valve - apex
o Tricuspid valve – 4th IC space, left sternal edge
o Pulmonary valve – 2nd IC space, left sternal edge
o Aortic valve – 2nd IC space, right sternal edge
• Go back to apex and listen for:
o Mitral regurgitation
� Pansystolic murmur
� Heard best over apex
� Radiates to axilla (demonstrate this by listening here)
o Mitral stenosis
� Listen with bell
� Mid-diastolic murmur
� Heard best:
• Over apex
• In expiration

Staff Development Programme 2010
11
• With patient rolled onto left side
• Go back to aortic valve region and listen for:
o Aortic stenosis
� Ejection systolic murmur
� Radiates to carotids (demonstrate this by listening here –
also listen for carotid bruits)
o Aortic regurgitation
� Early diastolic murmur
� Heard best:
• In 2nd aortic area (3rd or 4th intercostal space, LSE)
• With patient lent forwards
• In expiration
Keep patient sat forwards and:
• Listen for crackles at lung bases
• Palpate for sacral oedema
Lay patient back to 450
Palpate for ankle oedema
To complete
• Blood pressure in both arms
• Look at obs chart
• Palpate all peripheral pulses
Staff Development Programme 2010
12
Respiratory Examination – Crib Sheet
• Introduce yourself and ask permission
• Wash hands
• Position patient supine at 450
• General inspection from end of bed
o ‘Wide-angle lens’
� Inhalers
� Oxygen
� PEFR
� Nebulisers
� Sputum pot (look in it)
o Patient
� Respiratory distress?
� Accessory muscle use?
� Cyanosis?
� Chest shape
• Hands
o Clubbing
o Peripheral cyanosis
o Tar staining
o Fine tremor (β-agonist)
o Coarse tremor (CO2 retention)
• Pulse
• Respiratory rate
• Eyes
o Anaemia
o Horner’s syndrome
• Mouth
o Central cyanosis
o Inspect JVP
• Check for mediastinal shift
o Palpate trachea
o Palpate apex beat
• Sit patient forwards
• Palpate head and neck lymph nodes
Staff Development Programme 2010
13
• Posterior chest
o Chest expansion
o Percussion
o Auscultation
o One of:
� Vocal resonance
� Tactile vocal fremitus
� Whispering pectoriloquy
• Lie patient back to 450
• Anterior chest
o Chest expansion
o Percussion
o Auscultation
o One of:
� Vocal resonance
� Tactile vocal fremitus
� Whispering pectoriloquy
• Palpate for ankle oedema
• To complete:
o Check oxygen sats
o Measure peak flow
Staff Development Programme 2010
14
Respiratory Examination – Detailed List
General
There is always debate about whether the examiner should examine the front of
the chest before the back of the chest or vice versa. I don’t think it really matters,
as long as the whole of one side is done before the whole of the other, to avoid
sitting the patient backwards and forwards repeatedly. Personally, I prefer to
examine the posterior chest first, as you are more likely to find clinical signs at
the back.
Vocal resonance, tactile vocal fremitus and whispering pectoriloquy can be used
to help differentiate between consolidation and pleural effusion. Sound /
vibration is increased through an area of consolidation and decreased if there is
a pleural effusion between the lung and the stethoscope / hand. I do not think
there is a need to use all three as part of a routine examination – I think one is
adequate. I use vocal resonance.
Introduce yourself and ask permission
Wash hands
Position patient supine at 450
General inspection from end of bed
This is especially important for the respiratory examination, as many useful
things can be picked up from simple careful observation.
• ‘Wide-angle lens’
You are looking around for clues as to what the underlying diagnosis may be.
Look for:
o Inhalers
o Oxygen
o PEFR or PEFR chart
o Nebulisers
o Sputum pot (look in it)
• Patient
o Respiratory distress? Accessory muscle use? Cyanosis?
o Chest shape
� ‘Big chest’ with large anteroposterior diameter, little lateral
expansion, lifting of rib cage on inspiration – suggests
hyperinflation. Likely underlying COPD.
� ‘Small chest’ – possible fibrotic lung disease
� Pectus excavatum (‘funnel chest’) – common congenital
abnormality. Can occur on its own or with Marfan’s
syndrome
Staff Development Programme 2010
15
� Pectus carinatum (‘pigeon chest’) – can occur congenitally
or during adolescent growth spurt. Can occur in isolation or
as part of genetically inherited syndromes
Hands
• Clubbing. Causes:
o Bronchial carcinoma
o Chronic pulmonary infection:
� Empyema
� Bronchiectasis
� Lung abscess
� Cystic fibrosis
o Idiopathic pulmonary fibrosis
o Asbestosis
• Peripheral cyanosis
• Tar staining
• Fine tremor (β-agonist use)
• Coarse tremor (CO2 retention) – ‘asterixis’
Pulse
Respiratory rate
• Do this whilst palpating pulse so that patient is not aware that you are
counting their respiratory rate (may cause them to become
subconsciously tachypnoeic!)
Eyes
• Anaemia
• Horner’s syndrome – four potential features:
o Miosis
o Partial ptosis
o Anhydrosis on affected side of face
o Apparent enopthalmus
o Usual cause is Pancoast’s tumour – tumour of thoracic inlet
infiltrates sympathetic chain and T1 nerve root
Mouth
• Central cyanosis
Inspect JVP
Check for mediastinal shift
• Palpate trachea
• Palpate apex beat
• Mediastinum moves away from affected side in tension pneumothorax
• Mediastinum moves towards affected side in lung collapse or focal
fibrosis
Staff Development Programme 2010
16
Sit patient forwards
Palpate head and neck lymph nodes
No hard and fast rules as to which should be examined. Could do all. Must do the
ones in bold:
• Submental
• Submandibular
• Tonsillar
• Pre-auricular
• Post auricular
• Occipital
• Cervical
• Supraclavicular
• Axillary
Posterior chest
• Chest expansion
o Use ‘bucket handle’ approach with fingers in intercostal spaces
either side of chest and thumbs floating in midline – allows ribs to
move outwards
• Percussion - compare sides
o Stony dullness
� Effusion
o Dullness
� Consolidation
� Collapse
o Resonant
� Normal
o Hyper-resonant
� Tension pneumothorax
Staff Development Programme 2010
17
• Auscultation
o Compare sides
o Breath sounds can be normal or bronchial
o The volume can be normal or reduced
o There may be added breath sounds
Sounds What they sound like When they
are heard
Breath sounds
Normal (vesicular) Louder and longer in
inspiration than expiration
No gap between inspiratory
and expiratory sounds
Normally
Bronchial Hollow, blowing
Resemble sound when
stethoscope applied to neck
(but quieter)
Over an area
of
consolidation
Added sounds
Crackles Early and
mid-
inspiratory
Tend to be coarse
If clear on coughing and occur
in expiration are probably
result of airway secretions
Pneumonia
Bronchiectasis
Late
inspiratory
Tend to be fine Pulmonary
fibrosis
Pulmonary
oedema (may
be coarse)
Wheeze Expiratory
Polyphonic
COPD
Asthma
Pleural rub Scratching or grating sound on
deep inspiration, like leaves
underfoot or snow underfoot
Pulmonary
embolism
Pneumonia
• One of:
o Vocal resonance– say “99”
o Tactile vocal fremitus – say “99”
o Whispering pectoriloquy – whisper “99”
• Lie patient back to 450

Staff Development Programme 2010
18
Anterior chest
• Chest expansion
• Percussion
• Auscultation
• One of:
o Vocal resonance
o Tactile vocal fremitus
o Whispering pectoriloquy
Palpate for ankle oedema
To complete:
• Check oxygen sats
• Measure peak flow
Staff Development Programme 2010
19
Abdominal examination – Crib Sheet
• Introduce yourself, ask permission
• Wash hands
• Position patient
o Supine
o 1 pillow
o Exposed from xiphisternum to pubic symphysis
• Inspection from end of bed
o Jaundice
o Pigmentation
o Spider naevi
o Excoriations
o Abdominal distension
o Distended abdominal veins
• Hands
o Clubbing
o Koilonychia, leuconychia
o Palmar erythema
o Dupuytren’s contracture
o Asterixis
• Check radial pulse
• Eyes
o Anaemia
o Icteric sclera
o Xanthelasmata
• Mouth
o Apthous ulcers
o Telengiectasia
o Glossitis
o Angular stomatitis
• Palpate for supraclavicular lymphadenopathy
• Inspect for gynaecomastia (if male)
• Inspect for spider naevi
Staff Development Programme 2010
20
• Examine the abdomen
o Inspect
� Swelling
� Distended veins (? Caput medusa)
� Scars
o Palpation – look at patient’s face whilst doing this to check for
pain
� All 9 areas of abdomen, starting away from tenderness
� Superficial initially followed by deep
� Palpate for liver, starting in RIF
� Palpate for spleen, starting in RIF
� Bimanual palpation for each kidney
o Percussion
� Liver
� Spleen
� Flank dullness +/- shifting dullness
o Auscultation
� Bowel sounds
� Renal artery bruits
o To complete - offer
� External genitalia
� Hernial orifices
� PR examination
� Generalized lymphadenopathy (esp. if organomegaly)
� Urine dipstick
Staff Development Programme 2010
21
Abdominal examination – Detailed List
General
Some doctors, for patient comfort, begin with the patient positioned supine at
450 for the first part of the examination (hands, face etc). They then lay the
patient flat with one pillow for the ‘abdominal’ part of the examination.
Personally, I lay the patient flat with one pillow from the beginning – I think
either technique is acceptable.
Classically, optimal patient exposure is described as ‘nipples to knees’. This is
clearly inappropriate for the examination setting, and I believe xiphisternum to
pubic symphisis is adequate exposure.
Palpating the abdomen is easier and more comfortable for the patient if the
examiner is sat on a chair next to the bed.
The terms ‘jaundice’ and ‘icterus’ are interchangeable. Icterus is a more ‘medical’
word.
Introduce yourself, ask permission
Wash hands
Position patient
• Supine
• 1 pillow
• Exposed from xiphisternum to pubic symphysis
Inspection from end of bed
The following things can be looked for as part of a ‘visual survey’:
• Jaundice
Yellowing of the skin / sclera can be seen when serum bilirubin is above twice
the normal level (normal level 3-17µmol/l). Causes:
o Pre-hepatic: Usually haemolysis
o Hepatic: Gilbert’s syndrome / other enzymopathies
Acute liver disease (viral, drugs, alcohol)
Chronic Liver Disease
o Post-hepatic: Cholelithiasis
Ca pancreas
Cholangiocarcinoma
Drugs
Staff Development Programme 2010
22
• Pigmentation
o ‘Slate-grey’ or ‘dusky’ pigmentation with haemochromatosis.
• Spider naevi
o A central arteriole that radiates to numerous smaller vessels - said
to look like spider’s legs.
o Blanch when pressure applied and then refill from the centre
o In area supplied by SVC
o Traditionally attributed to excess oestrogen
o 5 or more are probably abnormal
o Sign of chronic liver disease
• Excoriations
o Associated with jaundice
• Abdominal distension
• Distended abdominal veins
o Flow always towards head – suggests IVC obstruction
o Flow away from umbilicus (‘Caput Medusae’) – portal
hypertension
Hands
• Clubbing – causes:
o Cirrhosis
o Crohn’s
o Ulcerative Colitis
• Koilonychia – spoon-shaped nails – iron-deficiency anaemia.
• Leuconychia – nail beds opacify leaving only a rim of pink nail at the
distal end (i.e. gives appearance of white nails). Seen with
hypoalbuminaemia
• Palmar erythema– causes:
o Chronic liver disease
o Pregnancy
o Thyrotoxicosis
o Rheumatoid Disease
o Polycythaemia
o Chronic leukaemia
• Dupuytren’s contracture
Visible and palpable thickening of palmar fascia – causes flexion deformity of one
or more fingers. Causes:
Staff Development Programme 2010
23
o Alcohol dependence
o Anticonvulsant therapy
o Diabetes
o Retroperitoneal fibrosis
o Manual workers
o Idiopathic familial
o Named after Baron Dupuytren (1777-1835) – Napoleon’s Surgeon
o Famous sufferers
� Margaret Thatcher
� JM Barrie – his contracture thought to have been
inspiration for Captain Hook
� Papal Benediction sign may have started with a Pope with
the condition
• Asterixis
o Jerky, irregular flapping at MCP joints and wrist.
o Seen commonly with:
� Hepatic encephalopathy
� CO2 retention
Check radial pulse
Eyes
• Anaemia?
• Icteric sclera?
• Xanthelesmata – associated with primary biliary cirrhosis
Mouth
• Ulcers - causes
o Trauma
o Drugs
o Apthous ulcers
o Herpes simplex
o GI disease – inflammatory bowel disease, celiac
o Rheumatological disease – Behcet’s disease, Reiter’s syndrome
o Erythema multiforme
• Telengiectasia
o Chronic liver disease
o Hereditary hemorrhagic telengiectasia
• Pigmented lips
o Peutz-Jeghers syndrome
• Angular stomatitis
o Iron deficiency
o Vitamin B deficiency

Staff Development Programme 2010
24
o Folate deficiency
• Glossitis
o Iron deficiency
o Vitamin B deficiency (esp. B12)
• Gum hypertrophy
o Phenytoin, nifedipine, OCP, cyclosporin
o Pregnancy
o Scurvy
o Gingivitis
Palpate for supraclavicular lymphadenopathy
• Virchow’s node (gastric carcinoma)
Inspect for gynaecomastia (if male)
Inspect for spider naevi
• 5 or more probably abnormal
Examine the abdomen
• Inspect
o Swelling
o Distended veins (? Caput medusae)
o Scars
• Palpation
o All 9 areas of abdomen, starting away from tenderness
o Superficial initially followed by deep
• Lumbar area also referred to as
flank or loin
• Hypogastric area also referred to as
suprapubic area
Staff Development Programme 2010
25
o Palpate for liver, starting in RIF
o Common causes of hepatomegaly – the three ‘C’s
� Cirrhosis (early)
� Cancer – liver often hard, nodular edge
� Cardiac (right-sided heart failure) – liver firm, smooth,
tender edge; may be pulsatile if tricuspid regurgitation
present
o Palpate for spleen, starting in RIF
o Causes of splenomegaly (similar to causes of
hepatosplenomegaly, but an important additional causes are
infective endocarditis and Felty’s syndrome (Rheumatoid
arthritis and hypersplenism)
o Causes of hepatosplenomegaly
� Cirrhosis with portal hypertension
� Lymphoproliferative disorders
• CLL
• ALL
• Myeloma
• Lymphoma
• Waldenstrom’s macroglobulinaemia
� Myeloprolifertive disorders
• CML
• Myelofibrosis
• Polycythaemia Rubra Vera
• Essential thrombocythaemia
� Infection / infiltration
• Glandular fever
• Brucellosis
• Leptospirosis
• Sarcoid
• Amyloidosis
• Glycogen storage disorders
o Bimanual palpation for each kidney
� Causes of a palpable kidney
• Polycystic kidney disease
• Renal cell cancer
• Renal transplant
• Hydronephrosis
Staff Development Programme 2010
26
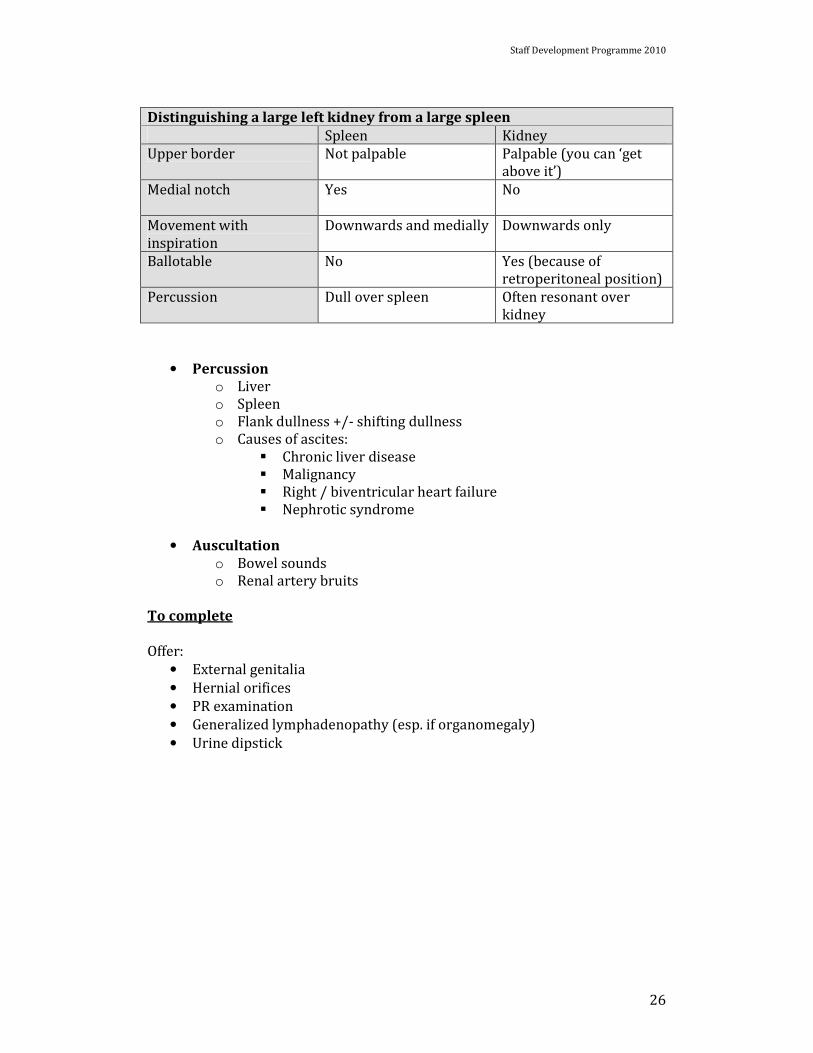
Distinguishing a large left kidney from a large spleen
Spleen Kidney
Upper border Not palpable Palpable (you can ‘get
above it’)
Medial notch Yes
No
Movement with
inspiration
Downwards and medially Downwards only
Ballotable No Yes (because of
retroperitoneal position)
Percussion Dull over spleen Often resonant over
kidney
• Percussion
o Liver
o Spleen
o Flank dullness +/- shifting dullness
o Causes of ascites:
� Chronic liver disease
� Malignancy
� Right / biventricular heart failure
� Nephrotic syndrome
• Auscultation
o Bowel sounds
o Renal artery bruits
To complete
Offer:
• External genitalia
• Hernial orifices
• PR examination
• Generalized lymphadenopathy (esp. if organomegaly)
• Urine dipstick
Staff Development Programme 2010
27
Acknowledgements
The two main texts consulted for reference whilst producing this booklet were:
1. Tim Hall. ‘ PACES for the MRCP’. Churchill Livingstone.
2. Epstein, Perkin, de Bono, Cookson. ‘Clinical Examination – Second
Edition’. Mosby.
Special thanks to the following people:
• Dr Katherine Bowering (SpR in Gastroenterology)
• Dr Richard Lee (Consultant in Gastroenterology)