evidence based medicine in peri-operative care wimonrat sriraj m.d. department of anesthesiology,...
TRANSCRIPT

Evidence Based Medicine Evidence Based Medicine in in
Peri-operative CarePeri-operative Care
Wimonrat Sriraj M.D.Wimonrat Sriraj M.D.Department of Anesthesiology, Department of Anesthesiology,
Faculty of Medicine, Faculty of Medicine,
Khon Kaen UniversityKhon Kaen UniversityPhuket 17/07/2008

OutlineOutline
What What WhenWhen WhichWhich Where Where How toHow to ExampleExample
Evidence-based medicineEvidence-based medicine
Phuket 17/07/2008

What evidence-based medicine is What evidence-based medicine is ??
““Evidence-based medicine is the Evidence-based medicine is the integration of integration of best research best research evidenceevidence with with clinical expertiseclinical expertise and and patient valuespatient values” ”
Sackett, et al 2001Sackett, et al 2001
Phuket 17/07/2008

Peri-operative anesthesia Peri-operative anesthesia carecare
Preanesthetic evaluationPreanesthetic evaluation Preanesthetic preparationPreanesthetic preparation Anesthetic managementAnesthetic management
Choice of AnesthesiaChoice of AnesthesiaMonitoring during anesthesiaMonitoring during anesthesiaPrevention & management of anesthetic-Prevention & management of anesthetic-
related related
complicationcomplication Postanesthesia carePostanesthesia care Postoperative pain managementPostoperative pain management
Phuket 17/07/2008

Best evidenceBest evidence
Research, Practice guideline Research, Practice guideline Type of research eg. Systematic review, RCT, etc.Type of research eg. Systematic review, RCT, etc.
Source eg. Journal, OrganizationSource eg. Journal, Organization
Critical appraisal Critical appraisal Internal validity : Appropriate methodologyInternal validity : Appropriate methodology
Minimal biasMinimal bias
Result : Magnitude, PrecisionResult : Magnitude, Precision
Clinical Clinical VSVS Statistical significance Statistical significance
External validity : Generalizability , ApplicabilityExternal validity : Generalizability , Applicability
Phuket 17/07/2008

American College ofPhysicians
BMJPublishing Group
Pre-filtered Journal
Phuket 17/07/2008

Level of evidence for recommendation
Phuket 17/07/2008

Searching for systematic Searching for systematic reviewreview
PubMed, At PubMed, At www.pubmed.comwww.pubmed.com restrict to : Meta-analysis [pt]restrict to : Meta-analysis [pt]
Review [pt]Review [pt]
Phuket 17/07/2008



Searching for systematic Searching for systematic reviewreview
PubMed, At www.PubMed.comPubMed, At www.PubMed.com restrict to : Meta-analysis [pt]restrict to : Meta-analysis [pt]
Review [pt]Review [pt]
The Cochrane library, The Cochrane library, At At www.thecochranelibrary.comwww.thecochranelibrary.com
Search by review group/ topicSearch by review group/ topic- - Anesthesia groupAnesthesia group- Pain, palliative and supportive care group- Pain, palliative and supportive care group- Others eg. Pregnancy and childbirth group- Others eg. Pregnancy and childbirth group
Phuket 17/07/2008








Choice of AnesthesiaChoice of Anesthesia
““Caesarean section”Caesarean section”
Efficacy, safetyEfficacy, safetyMaternal & Neonatal effectMaternal & Neonatal effect
Feasibility, practicalityFeasibility, practicality Patient preference Patient preference
Phuket 17/07/2008
RARAVS VS GA for C/SGA for C/S
Anaesthesia for Caesarean section and neo Anaesthesia for Caesarean section and neo - - natal acid base status: a meta analysis. An - - natal acid base status: a meta analysis. An
aesthesia aesthesia 2005;60(7):636-532005;60(7):636-53 . .
Regional versus general anaesthesia for ca Regional versus general anaesthesia for ca esarean section esarean section.. Cochrane Database Syst R Cochrane Database Syst R
evev. . 2006 2006 Oct Oct 18(4):18(4): CD CD 004350 004350
Spinal versus epidural anaesthesia for caes Spinal versus epidural anaesthesia for caes arean section arean section. . Cochrane Database Syst Re Cochrane Database Syst Re
vv. . 2004 2004 Oct Oct 16(2):16(2): CD CD 003765 003765
Phuket 17/07/2008

Choice of AnesthesiaChoice of Anesthesia
Phuket 17/07/2008

Maternal effect 1Maternal effect 1
Phuket 17/07/2008

Maternal effect 2Maternal effect 2
Phuket 17/07/2008

Neonatal effect 1Neonatal effect 1
Phuket 17/07/2008

Neonatal effectNeonatal effect 22
Phuket 17/07/2008

Reynolds F, Seed PT. Anaesthesia for Caesar Reynolds F, Seed PT. Anaesthesia for Caesar - ean section and neonatal acid base status: a - ean section and neonatal acid base status: a
- meta analysis.- meta analysis.AnaesthesiAnaesthesia a 2005; 60(7): 636-2005; 60(7): 636-
53.53.
More neonatal acidosis in Regional More neonatal acidosis in Regional anesthesiaanesthesia
Umbilical pH difference -0.015 ( 95% CI -0.029, -0.001)Umbilical pH difference -0.015 ( 95% CI -0.029, -0.001) Base deficit difference 1.109 ( 95% CI 0.434, 1.784 Base deficit difference 1.109 ( 95% CI 0.434, 1.784
mEq/l) mEq/l)
Neonatal effectNeonatal effect 33
Phuket 17/07/2008

Patient valuePatient value
Phuket 17/07/2008
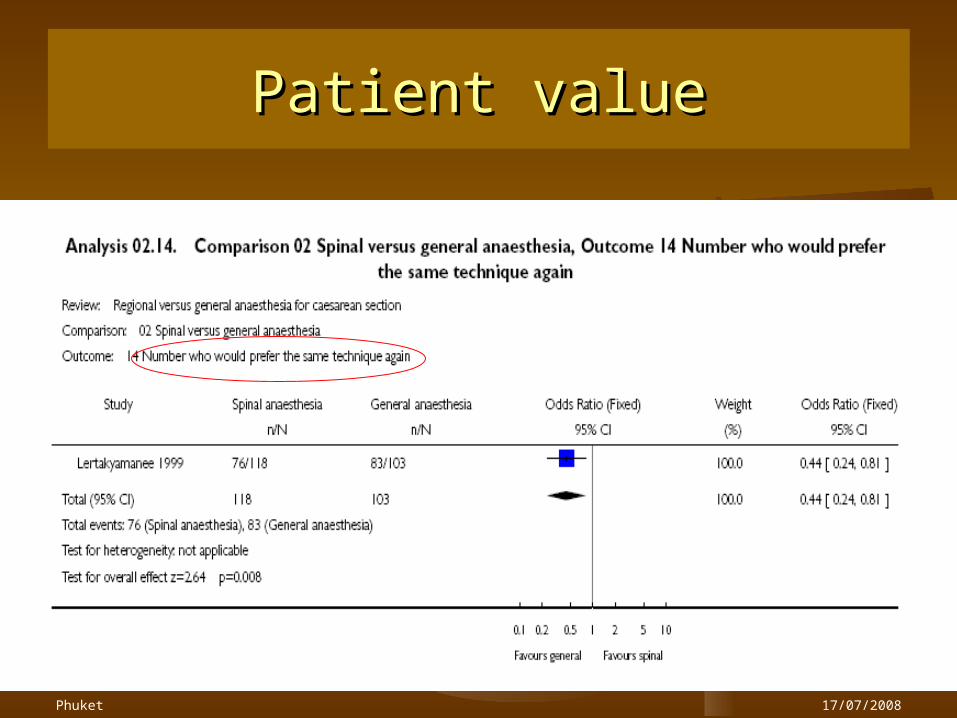
Patient valuePatient value
Phuket 17/07/2008

Authors’ conclusionAuthors’ conclusion
In terms of In terms of majormajor maternal & maternal & neonatal outcomes : Not enough neonatal outcomes : Not enough evidence to show that either RA or evidence to show that either RA or GA is superior to each otherGA is superior to each other
In low to intermediate income In low to intermediate income countries, the least expensive countries, the least expensive method should be chosenmethod should be chosen
Phuket 17/07/2008

Evidence-based Practice Evidence-based Practice (EBP)(EBP)
ASK
ACQUIRE
APPRAISE
APPLY
ASSESS
Decision making
Professional experience
Clinical expertise
Clinical circumstance
Patient preferences
Costs
Organizational issues
Politics
etc.
Professional experience
Clinical expertise
Clinical circumstance
Patient preferences
Costs
Organizational issues
Politics
etc.
The right
question
Systematically search for
the best evidences
Critically appraised for
validity & applicability
Judiciously applied to
the appropriate
patients

Choice of regional Choice of regional anesthesiaanesthesia
Phuket 17/07/2008
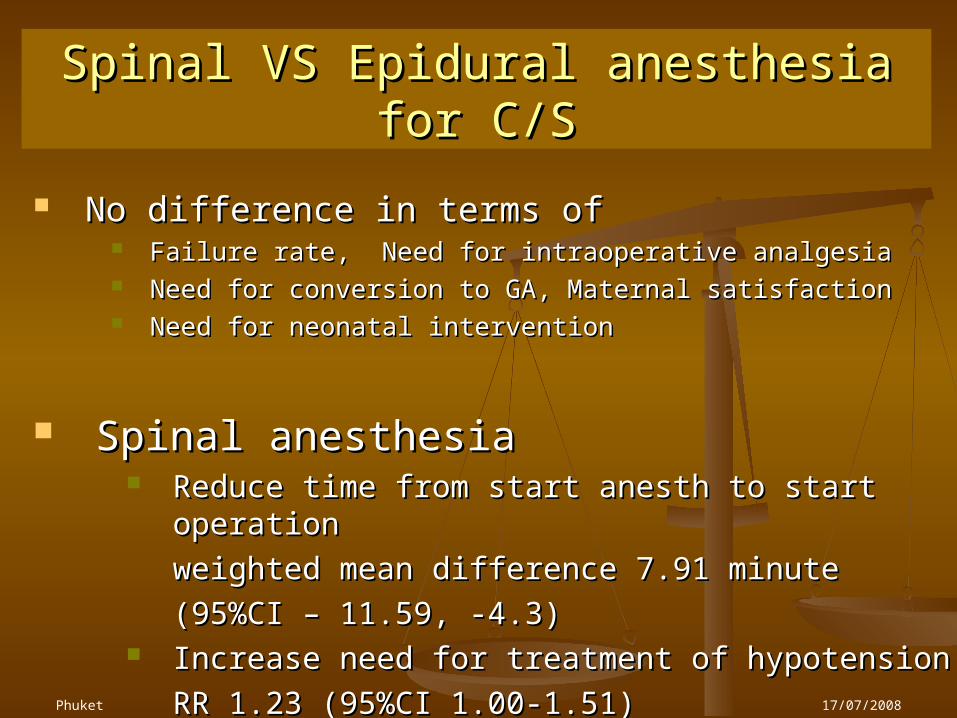
Spinal VS Epidural anesthesia for C/SSpinal VS Epidural anesthesia for C/S
Phuket 17/07/2008
No difference in terms of No difference in terms of Failure rate, Need for intraoperative analgesiaFailure rate, Need for intraoperative analgesia Need for conversion to GA, Maternal satisfactionNeed for conversion to GA, Maternal satisfaction Need for neonatal interventionNeed for neonatal intervention
Spinal anesthesia Spinal anesthesia Reduce time from start anesth to start operationReduce time from start anesth to start operation
weighted mean difference 7.91 weighted mean difference 7.91 minuteminute
(95%CI – 11.59, -4.3)(95%CI – 11.59, -4.3) Increase need for treatment of hypotensionIncrease need for treatment of hypotension
RR 1.23 (95%CI 1.00-1.51)RR 1.23 (95%CI 1.00-1.51)

Rapid recoveryRapid recovery Less nausea & vomitingLess nausea & vomiting Good postoperative painGood postoperative pain
Ambulatory anesthesiaAmbulatory anesthesia
Regional Regional VSVS General anesthesia General anesthesia

Ambulatory anesthesiaAmbulatory anesthesia
Anesthesia Analgesia 2005; 101(6): 1634-42

Outcome of interestOutcome of interest
Induction timeInduction time Incidence of nausea & vomitingIncidence of nausea & vomiting Postop pain : VAS, rescue analgesicsPostop pain : VAS, rescue analgesics Ability to bypass PACUAbility to bypass PACU Time in PACU, Time until dischargeTime in PACU, Time until discharge Patient satisfactionPatient satisfaction

FindingFinding
RA RA Need more induction time ~ 8.1 minuteNeed more induction time ~ 8.1 minute Less postop painLess postop pain PONV : PNB less but not with CNBPONV : PNB less but not with CNB More ability to bypass PACU More ability to bypass PACU
Time for ambulatory unit stay : not Time for ambulatory unit stay : not reducereduce
CNB associate with delay discharge time ~ 35 CNB associate with delay discharge time ~ 35 minute minute

Implication for practiceImplication for practice
RA : Advantage but need more timeRA : Advantage but need more time
Busy ambulatory unit : ???Busy ambulatory unit : ???
GA : Techniques, anesthetic drugs, GA : Techniques, anesthetic drugs,
Prevention of PONV , severe P/O painPrevention of PONV , severe P/O pain
Cost effective, Policy, Patient Cost effective, Policy, Patient valuevalue

Decision makingDecision making
Efficacy & safety Efficacy & safety Evidence based medicineEvidence based medicine
(Best) Evidence , Expertise, Patient (Best) Evidence , Expertise, Patient valuevalue
Clinical circumstanceClinical circumstance PolicyPolicy Etc.Etc.

Thank YouThank You