evaluation of poisoning and drug overdose
TRANSCRIPT

Evaluation of Poisoning and Drug Overdose
Kara Lynch, PhD, DABCC University of California San Francisco
San Francisco, CA

Learning Objectives
• Understand the laboratories role in the diagnosis and treatment of toxicology cases
• Review the pathophysiology of toxic exposures • Identify the common toxidromes • Calculate the osmolar gap and anion gap • Be able to recognize drug overdoses

Paraclesus – “father of toxicology”
• “All things are poison, and nothing is without poison; only the dose permits something not to be poisonous.”
• “The dose makes the poison.” • substances considered toxic
are harmless in small doses, and an ordinarily harmless substance can be deadly if over-consumed
Paraclesus, 1490 - 1541

• A poisoning occurs when a person’s exposure to a natural or manmade substance has an undesirable effect - CDC
• Poisonings can be classified as: – Self-harm or suicide – Assault or homicide – Unintentional or accidental, when no harm was
intended – includes overdoses resulting from drug misuse, drug abuse or taking too much of a drug for medical reasons
Definition of “Poisoning”

• AAPCC – American Association of Poison Control Centers – – National poison data system (NPDS) annual report
• DAWN – Drug Abuse Warning Network • SAMHSA World Drug Report – Substance
Abuse and Mental Health Services Administration
• CDC – Center for Disease Control – National Vital Statistics System (NVSS)
Monitoring Poisonings

Poisoning / Overdose Trends

Poisoning / Overdose Trends

AAPCC: Top 25 human exposures

AAPCC: Top 25 pediatric exposures

Increase in Exposure – Top 4

• ABCs (airway, breathing, circulation) • Supportive Care • Antidote if available and indicated • Decontamination (surface and gastrointestional)
– Wash skin and irrigate eyes, emesis or gastric lavage, activated charcoal or cathartic, whole-bowel irrigation
• Enhanced Elimination – Hemodialysis – Hemoperfusion – Repeat-dose charcoal
Poisoning: Treatment Approach

• Airway → Endotracheal intubation – Check gag/cough reflex – Position patient – Clear/suction airway
• Breathing → ventilatory failure, hypoxia, bronchospasm – Obtain arterial blood gases – Assist with bag/mask device – Give supplemental oxygen
• Circulation → bradycardia, tachycardia, prolonged QRS interval, arrhythmias, hypotension, hypertension – Measure blood pressure/pulse – Monitor electrocardiogram – Start 1-2 IV lines – Obtain routine bloodwork
Treatment: ABC’s or CAB

Antidote or Specific Treatment Toxin Antidote/Treatment Acetaminophen N-Acetylcysteine (NAC, Mucomyst)
Aluminum or Iron Deferoxamine
Anticholinergic agents Physostigmine
Arsenic and Mercury Unithiol, Dimercaprol (BAL), oral succimer (DMSA)
Benzodiazepines Flumazenil
Beta-blockers Glucagon
Calcium channel blockers Calcium
Carbon monoxide Oxygen (normobaric or hyperbaric)
Cyanide Amyl nitrite, sodium nitrite, sodium tiosulfate
Digoxin Digibind (Fab fragments)
Ethylene glycol, methanol Ethanol, fomepizole (5-methylpyrazol), hemodialysis
Isoniazid Pyridoxine (Vitamin B6)
Lead Calcium EDTA, Dimercaprol (BAL), oral succimer (DMSA)
Nitrites, nitrates Methylene blue
Opioids Naloxone
Salicylates Bicarbonate, hemodialysis, alkaline diuresis

Poisoning Evaluation: toxidromes
• Toxidrome = A collection of symptoms and signs that consistently occur after ingestion of a particular toxin or drug class
• Often identified with a basic history and physical examination
• Rapid identification of the toxidrome saves time in evaluating and managing a poisoned patient

Poisoning Evaluation: toxidromes
Kinetic Anatomy with Web Resource, 3rd Edition
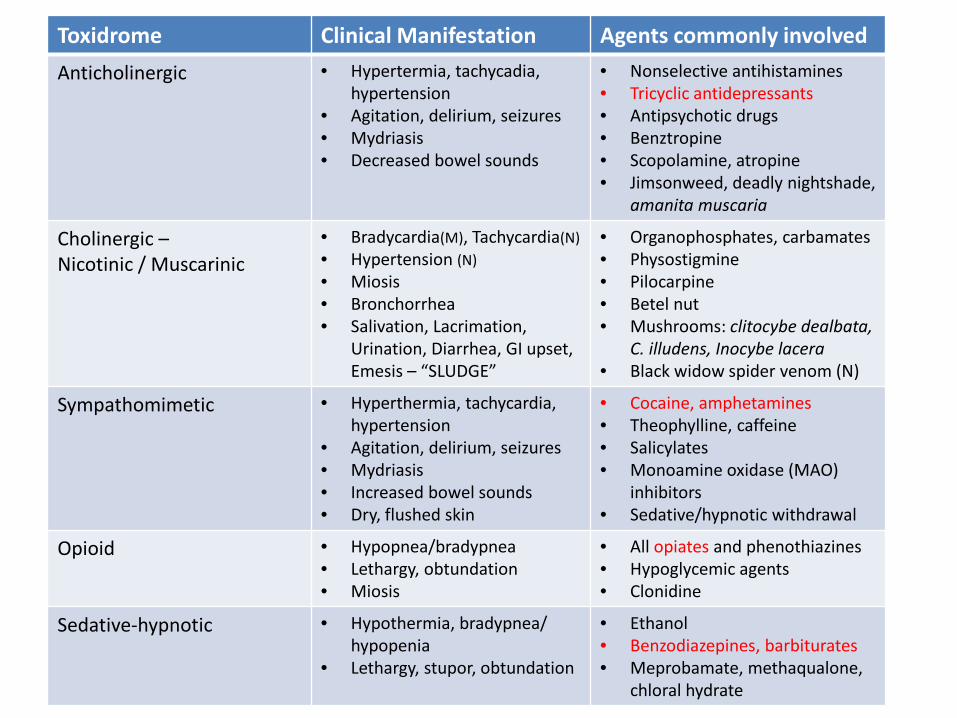
Toxidrome Clinical Manifestation Agents commonly involved Anticholinergic • Hypertermia, tachycadia,
hypertension • Agitation, delirium, seizures • Mydriasis • Decreased bowel sounds
• Nonselective antihistamines • Tricyclic antidepressants • Antipsychotic drugs • Benztropine • Scopolamine, atropine • Jimsonweed, deadly nightshade,
amanita muscaria
Cholinergic – Nicotinic / Muscarinic
• Bradycardia(M), Tachycardia(N) • Hypertension (N) • Miosis • Bronchorrhea • Salivation, Lacrimation,
Urination, Diarrhea, GI upset, Emesis – “SLUDGE”
• Organophosphates, carbamates • Physostigmine • Pilocarpine • Betel nut • Mushrooms: clitocybe dealbata,
C. illudens, Inocybe lacera • Black widow spider venom (N)
Sympathomimetic • Hyperthermia, tachycardia, hypertension
• Agitation, delirium, seizures • Mydriasis • Increased bowel sounds • Dry, flushed skin
• Cocaine, amphetamines • Theophylline, caffeine • Salicylates • Monoamine oxidase (MAO)
inhibitors • Sedative/hypnotic withdrawal
Opioid • Hypopnea/bradypnea • Lethargy, obtundation • Miosis
• All opiates and phenothiazines • Hypoglycemic agents • Clonidine
Sedative-hypnotic • Hypothermia, bradypnea/ hypopenia
• Lethargy, stupor, obtundation
• Ethanol • Benzodiazepines, barbiturates • Meprobamate, methaqualone,
chloral hydrate

Blood Pressure
Heart Rate
Resp. Rate
Temp. Pupil size
Bowel sounds
Diaph-oresis
Anticholinergic ↑ ↑ ↑ ↓ ↓
Cholinergic ↓ ↑ ↑
Opioid ↓ ↓ ↓ ↓ ↓ ↓ ↓
Sympathomimetic ↑ ↑ ↑ ↑ ↑ ↑ ↑
Sedative-hypnotic ↓ ↓ ↓ ↓ ↓ ↓
Poisoning Evaluation: toxidromes

psychiatryonline.org
Illicit Drugs: Mechanism of Action
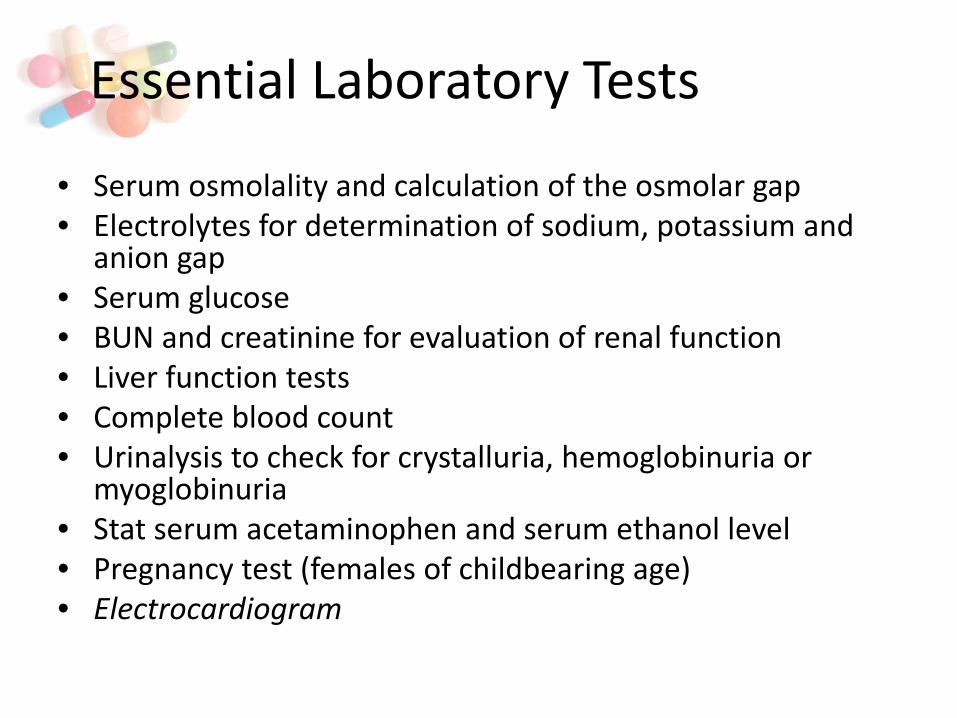
• Serum osmolality and calculation of the osmolar gap • Electrolytes for determination of sodium, potassium and
anion gap • Serum glucose • BUN and creatinine for evaluation of renal function • Liver function tests • Complete blood count • Urinalysis to check for crystalluria, hemoglobinuria or
myoglobinuria • Stat serum acetaminophen and serum ethanol level • Pregnancy test (females of childbearing age) • Electrocardiogram
Essential Laboratory Tests
Toxic Alcohols
• Ethanol • Methanol • Isopropanol • Acetone • Ethylene glycol

• First-order kinetics – rate of elimination is proportional to the amount of drug present
• Zero-order kinetics – rate of elimination is constant regardless of the amount of drug present in the system
• Capacity-limited kinetics – occurs when the rate of elimination shifts from first-order to zero-order based on the saturation of the elimination processes (overdoses)
• Serum half-life – time required for serum concentrations to decrease by one half
• First-pass effect – applies to drugs cleared by the liver before reaching systemic circulation
• Steady-state – applies to repeated dosing; reached in about 4 half-lives
Pharmacokinetics: Review

Toxic Alcohols: Ethanol
• Ethanol or ethanol combined with other drugs accounts for the highest number of toxic exposures
• Potent central nervous system depressant • Effects vary with concentration • Common cause of hyperosmolality in the ED • Metabolism follows zero-order kinetics

Ethanol
Acetate
Acetaldehyde
UGT 1A1 UGT 2B7 SULTs
Ethylsulfate (EtS) Ethylglucuronide (EtG)
ADH1B ADH1C
ALDH2
CYP2E1
Urine ~ 80 hours Urine ~ 80 hours
Serum ~ 3.5 hours
Ethanol Metabolism

Ethanol Measurement
• Enzymatic methods – alcohol dehydrogenase • CH3CH2OH CH3CHO
• ADH is selective but not specific for ethanol, although current assays have minimal reactivity with non-ethanol alcohols
• Other enzymes that involve NADH can potentially interfere (ie: lactate, LD)
• Other methods - Headspace GC-MS
NAD+
ADH
NADH 340 nm
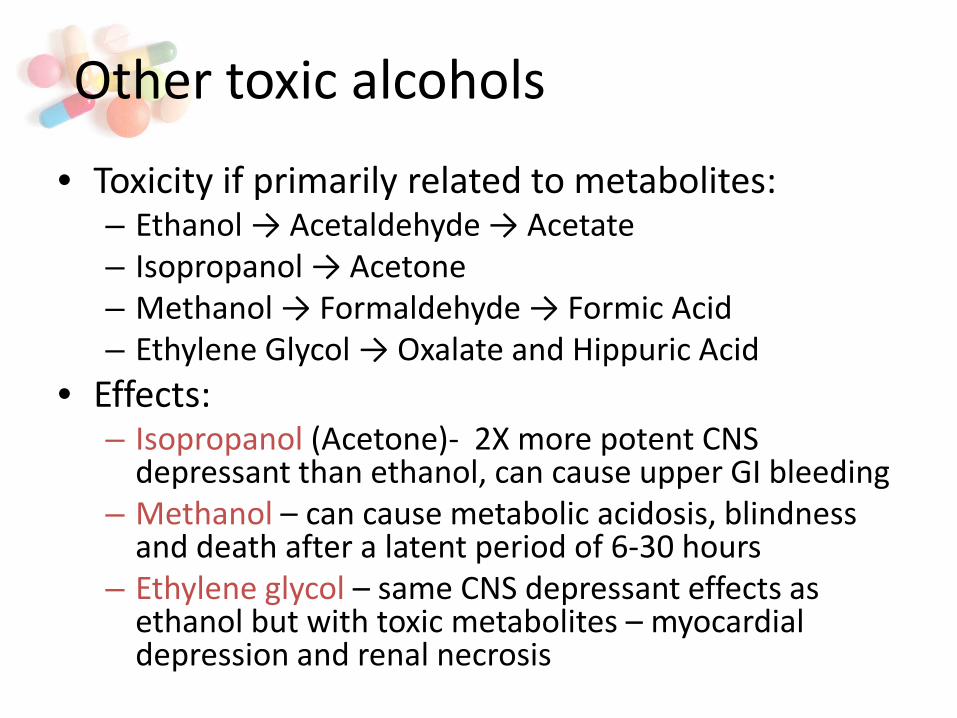
• Toxicity if primarily related to metabolites: – Ethanol → Acetaldehyde → Acetate – Isopropanol → Acetone – Methanol → Formaldehyde → Formic Acid – Ethylene Glycol → Oxalate and Hippuric Acid
• Effects: – Isopropanol (Acetone)- 2X more potent CNS
depressant than ethanol, can cause upper GI bleeding – Methanol – can cause metabolic acidosis, blindness
and death after a latent period of 6-30 hours – Ethylene glycol – same CNS depressant effects as
ethanol but with toxic metabolites – myocardial depression and renal necrosis
Other toxic alcohols

Other toxic alcohols
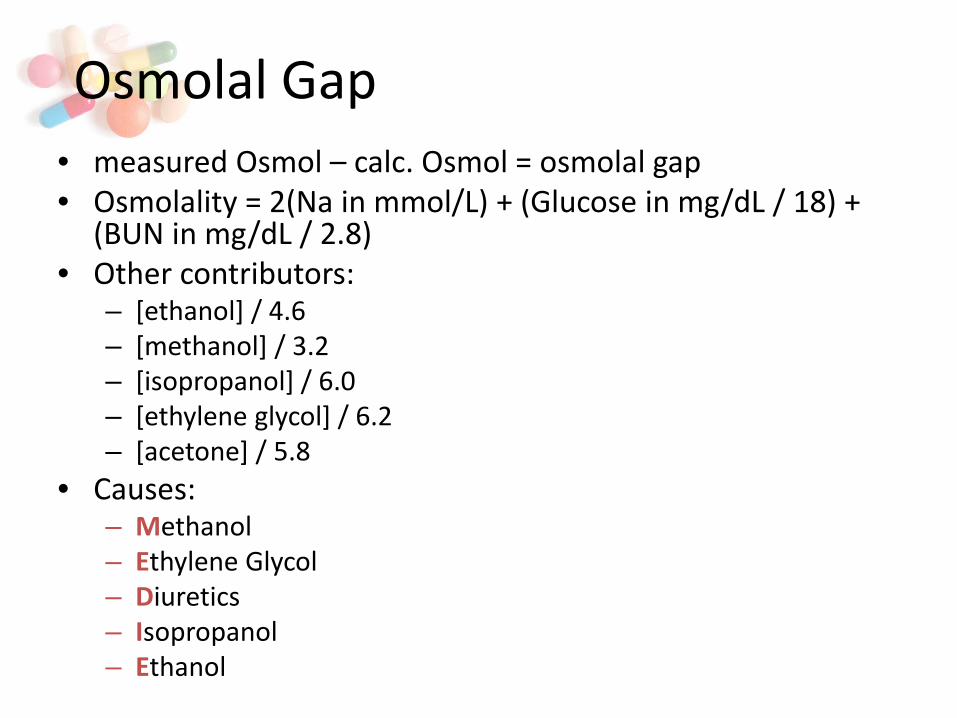
• measured Osmol – calc. Osmol = osmolal gap • Osmolality = 2(Na in mmol/L) + (Glucose in mg/dL / 18) +
(BUN in mg/dL / 2.8) • Other contributors:
– [ethanol] / 4.6 – [methanol] / 3.2 – [isopropanol] / 6.0 – [ethylene glycol] / 6.2 – [acetone] / 5.8
• Causes: – Methanol – Ethylene Glycol – Diuretics – Isopropanol – Ethanol
Osmolal Gap
Anion Gap
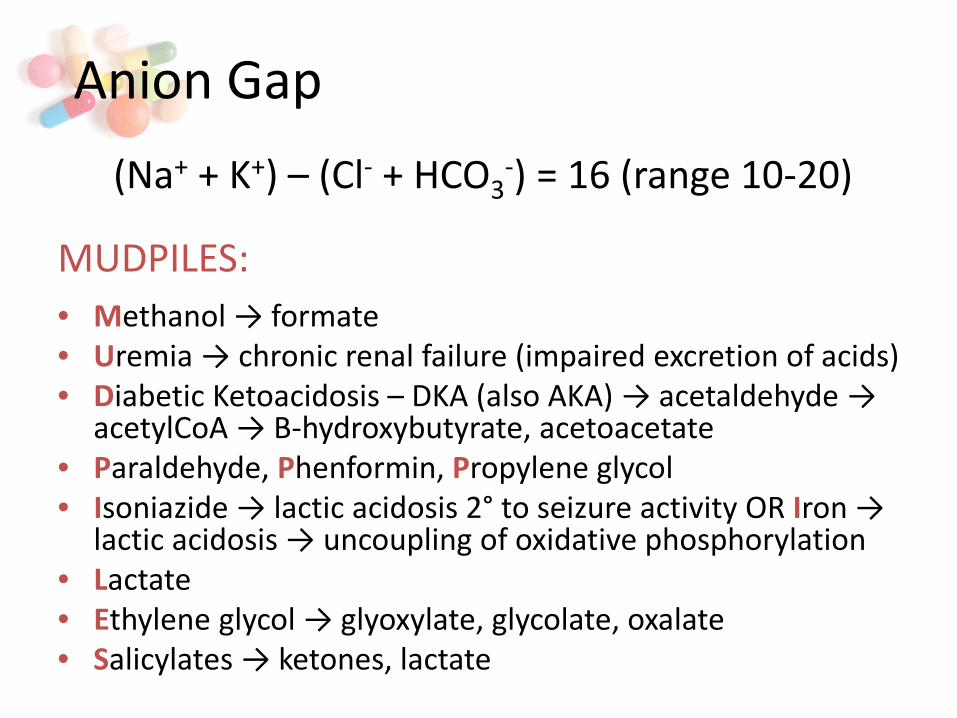
MUDPILES:
• Methanol → formate • Uremia → chronic renal failure (impaired excretion of acids) • Diabetic Ketoacidosis – DKA (also AKA) → acetaldehyde →
acetylCoA → B-hydroxybutyrate, acetoacetate • Paraldehyde, Phenformin, Propylene glycol • Isoniazide → lactic acidosis 2° to seizure activity OR Iron →
lactic acidosis → uncoupling of oxidative phosphorylation • Lactate • Ethylene glycol → glyoxylate, glycolate, oxalate • Salicylates → ketones, lactate
(Na+ + K+) – (Cl- + HCO3-) = 16 (range 10-20)

Ingestion of Alcohols: Lab Findings
Alcohol Osmolal Gap
Metabolic Acidosis with anion gap
Serum Acetone
Urine Oxalate
Ethanol + - - -
Methanol + + - -
Isopropanol + - + -
Ethylene glycol + + - +

• Healthy 50 year-old man was found unconscious in this home, believed to be down for ~24 hours
• Emergency response – GCS 3, vitals normal, oxygen saturation 80%, patient intubated and brought to UCSF ED
• Remarkable lab findings: HCO-3 5, osmolol gap and
anion gap >35, pH 6.7, lactate above the ULOQ, creatinine 2.4
• LFTs, tox screen, APAP and salicylate normal • Normal head and abdominal CT, all cultures negative
no vasopressors required • Patient received IVFs and died before they could start
dialysis
Case Study

Case Study
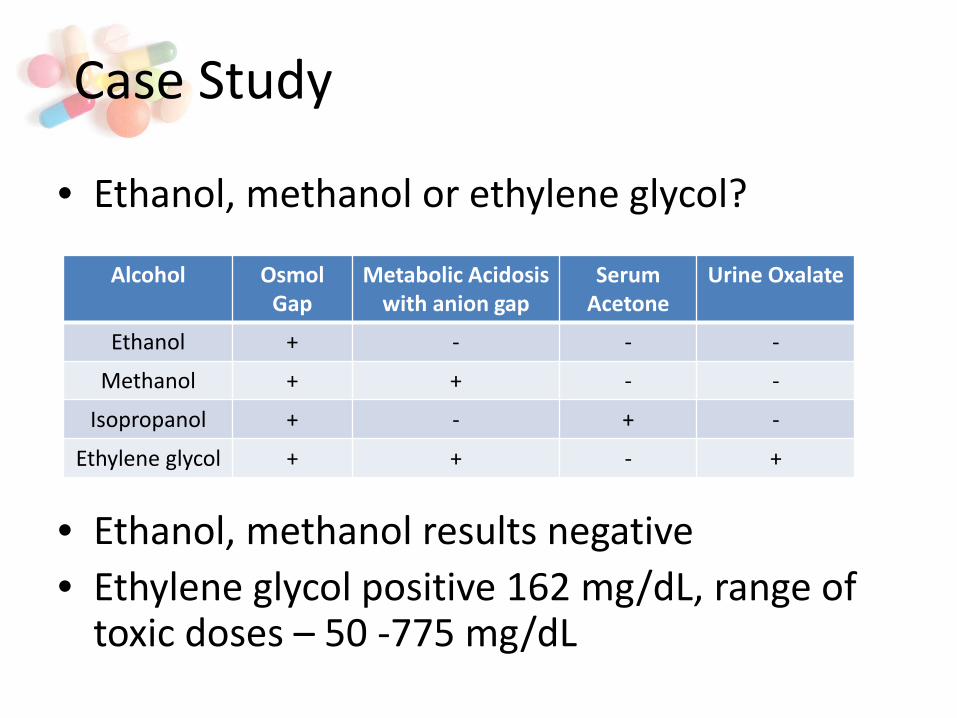
• Ethanol, methanol or ethylene glycol?
• Ethanol, methanol results negative • Ethylene glycol positive 162 mg/dL, range of
toxic doses – 50 -775 mg/dL
Case Study
Alcohol Osmol Gap
Metabolic Acidosis with anion gap
Serum Acetone
Urine Oxalate
Ethanol + - - -
Methanol + + - -
Isopropanol + - + -
Ethylene glycol + + - +
• Analgesic and antipyretic • Peak concentrations – 4 hours post-ingestion • Normal half-life 2-3 hours; >4 hours hepatic
toxicity; >12 hours hepatic coma likely • Acute liver damage threshold; adults 150-250
mg/kg • Children under the age of 10 more resistant to
toxicity • Measured by enzymatic / colorimetric methods • Antidote is N-acetylcysteine
Acetaminophen (Tylenol)
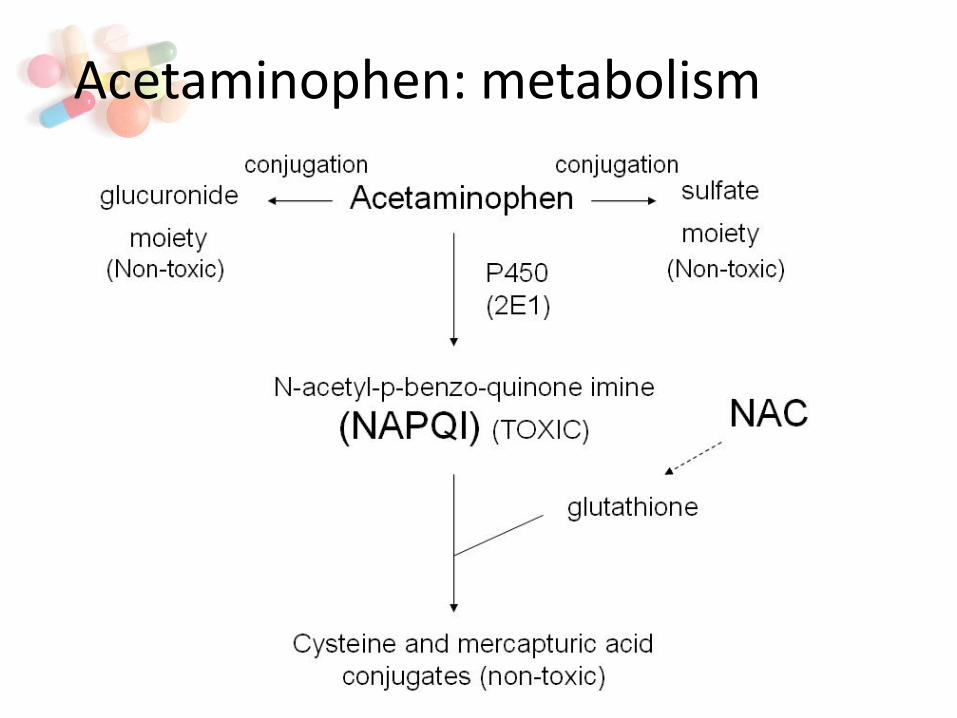
Acetaminophen: metabolism

Acetaminophen: hepatic toxicity
Salicylate (Aspirin) • Analgesic, antipyretic and anti-inflammatory • Therapeutic dose – single dose – 10 mg/kg; daily dose
– 40-60 mg/kg • Mild intoxication – 150-200 mg/kg; severe intoxication
– 300-500 mg/kg; chronic toxicity - >100 mg/kg/day • Lab results reveal mixed metabolic acidosis /
respiratory alkalosis • Tinnitus, hyperthermia, hyperventilation, CNS • Measured by enzymatic / colorimetric methods • Treatment of salicylate overdose
– Hydration, glucose, K+ supplements, bicarbonate, hemodialysis

• Most common cause of fatal poisonings – smoke inhalation
• Colorless, odorless, tasteless gas • Has 240x the affinity for hemoglobin than oxygen
→ carboxyhemoglobin (COHb) • Symptoms begin at COHb levels of 10-20% and
50% can be fatal • Nonsmokers – 1-2% COHb, smokers 5-6% COHb • Treatment: fresh air, 100% O2 or hyperbaric
oxygen may be indicated
Carbon Monoxide

Wavelength (nm)
Abso
rban
ce →
methemoglobin
oxyhemoglobin
reduced hemoglobin
carboxyhemoglobin
UV Absorption of Hb forms
Comparison of absorbencies at different wavelengths allows estimation of the relative concentrations of different forms of hemoglobin beer-lambert law – A = ɛbc or A = ɛ1bc1 + ɛ2bc2 + ɛ3bc3 ….
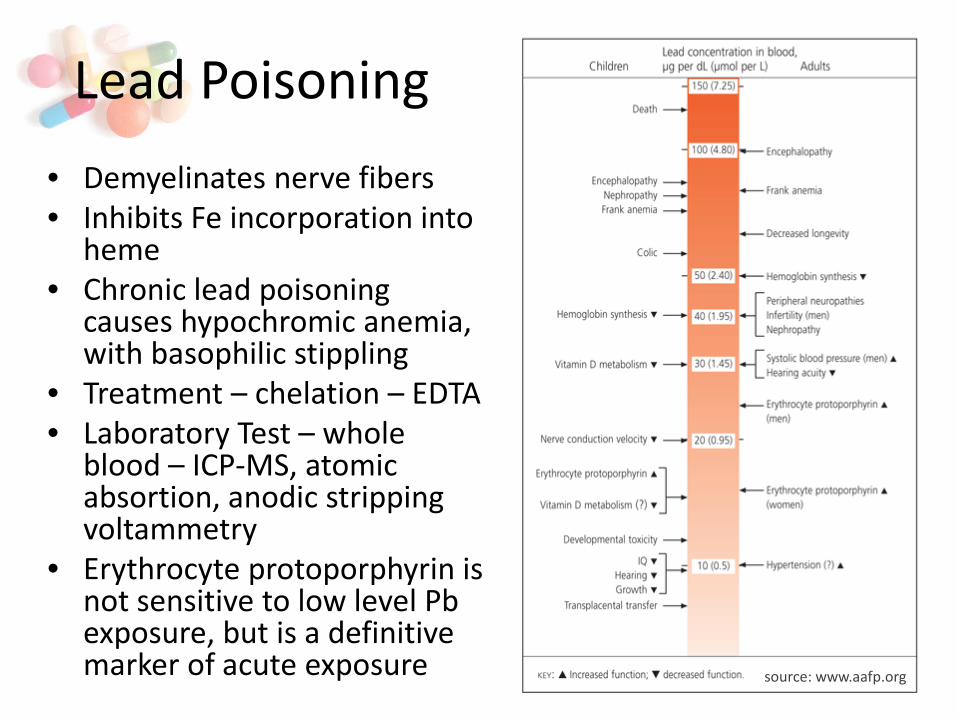
Lead Poisoning • Demyelinates nerve fibers • Inhibits Fe incorporation into
heme • Chronic lead poisoning
causes hypochromic anemia, with basophilic stippling
• Treatment – chelation – EDTA • Laboratory Test – whole
blood – ICP-MS, atomic absortion, anodic stripping voltammetry
• Erythrocyte protoporphyrin is not sensitive to low level Pb exposure, but is a definitive marker of acute exposure source: www.aafp.org

Iron Poisoning • Approximately 5,000 case per year – mostly children • Toxicity of related to the dose of elemental iron • Treatment:
– Serial monitoring of serum iron – Obtain creatinine, electrolytes, hemoglobin, PT, LFTs and arterial
blood gases – Calculate elemental iron dose ingestion; 20-60 mg Fe/kg
moderate risk; >60 mg/kg high risk – <350 μg/dL and no symptoms – supportive care – >300 μg/dL and symptoms – deferoxamine infusion
Compound Elemental Iron
Ferrous sulfate (hydrate) 20%
Ferrous fumarate 33%
Ferrous gluconate 12%
Ferrous chloride (hydrate) 28%
Ferric chloride (hydrate) 20%

1. Which toxidrome is characterized by Salivation, Lacrimation, Urination, Diarrhea, GI upset, Emesis – “SLUDGE”?
a) Anticholinergic b) Cholinergic c) Sympatomemetic d) Sedative-hypnotic
2. A blood ethanol concentration of 130 mg/dL will contribute how much to a serum osmolality?
a) 2.8 mOsm/kg b) 3.5 mOsm/kg c) 28 mOsm/kg d) 35 mOsm/kg e) 280 mOsm/kg
3. By what mechanism does N-acetylcystine help prevent hepatic damage in acetaminophen overdose?
a) Blocks absorption of acetaminophen b) Provides a source of glutathione c) Prevents hepatic conjugation of acetaminophen d) Blocks acetaminophen receptors on hepatocytes e) Forms an in active complex with acetaminophen
Self-Assessment Questions