evaluating the landscape of statin drug interactions with ... · evaluating the landscape of statin...
TRANSCRIPT

Evaluating the Landscape of Statin Drug Interactions with Select Cardiovascular Medications: What you need to know
Barbara S. Wiggins, Pharm.D., FCCP, FAHA, FNLA, AACC, BCPS (AQ Cardiology), CLSClinical Specialist‐ Cardiology, Medical University of South CarolinaAdjunct Professor, South Carolina College of PharmacyCharleston, South Carolina

Disclosures
No Conflicts of Interest

Objectives• Review the various type of pharmacokinetic interactions that can occur with medications
• Describe drug interactions that occur with the CYP 450 enzymes and P‐glycoprotein.
• Discuss specific drug interactions with statins and other lipid lowering agents as well as clinical management
• Review drug interactions with select cardiovascular agents and statins as well as clinical management

Metabolism of Select Statins
Copyright to PharmGKB, with permission by PharmGKB and Stanford University. https://www.pharmgkb.org/pathway/PA145011109
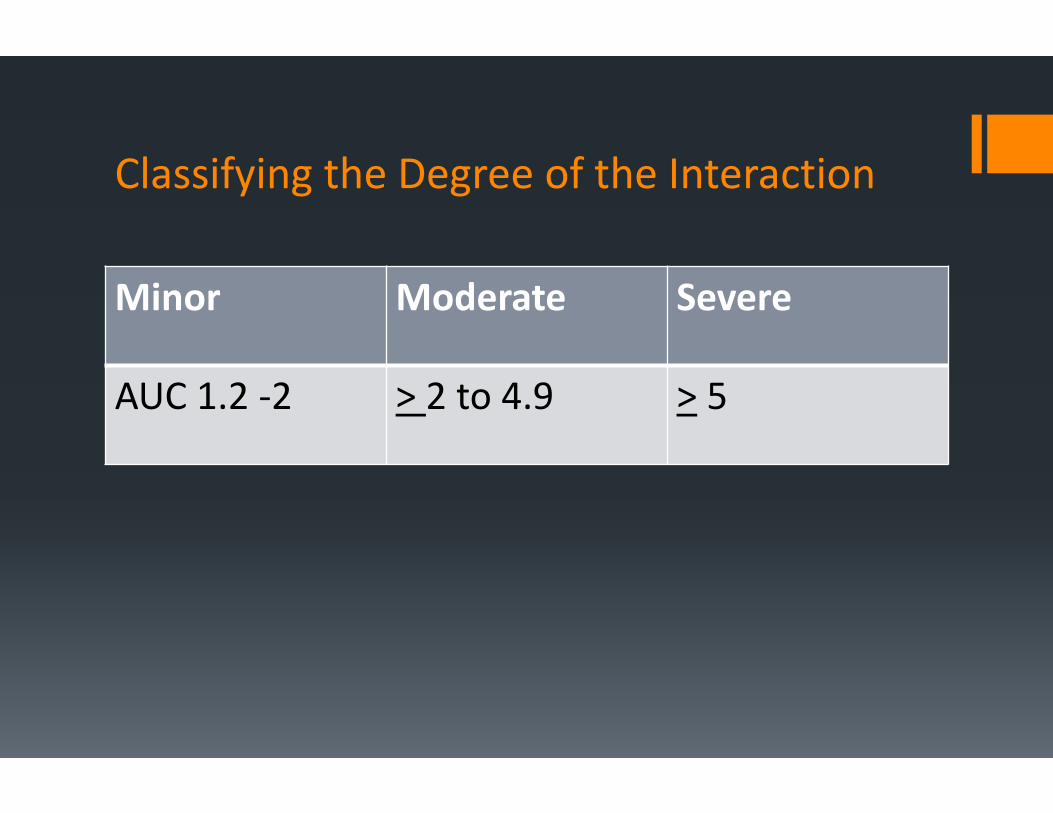
Classifying the Degree of the Interaction
Minor Moderate Severe
AUC 1.2 ‐2 > 2 to 4.9 > 5

Metabolism of Select Statins (CYP 450 Enzymes and P‐glycoprotein)
Statin Bioavail T ½ (hours) Metabolism Pro‐drug P‐Glycoprotein
Pravastatin 17% 1.5‐2 n/a No
Fluvastatin 24% 1 CYP 2C9 No
Lovastatin <5% 2‐3 CYP 3A4 Yes ? Substrate and inhibitor
Simvastatin <5% 2 CYP 3A4 Yes ? Substrate and inhibitor
Atorvastatin 12% 14 CYP 3A4 No ? Substrate and inhibitor
Rosuvastatin 20% 20 Limited 2C9 No
Pitavastatin 51% 12 CYP 2C9,2C8 Yes ? Substrate and inhibitor

Adapted from Corsini et al. Pharmacol Ther 1999;84: 413-428.White CM. J Clin Pharmacol 2002;42:963-970.
N.A. = not availableLog D class = distribution of drug into octanol:water
Clinical Pharmacokinetics of Statins
Parameter Atorva Rosuva Fluva Lova Prava Simva
DistributionFraction bound(%)
80 - 90 88 > 99 > 95 43 - 55 94 - 98
Lipophilic YES NO YES YES NO YES
Log D class 1 to 1.25 -0.25 to -0.5 NA -0.75 to -1.0 1.5 to 1.751 to 1.25

Clinical Pharmacokinetics of Statins
Parameter Atorva Rosuva Fluva Lova Prava Simva
Metabolism
Hepatic extraction (%)
> 70 63 > 68 > 70 46 - 66 78 - 87
Metabolism CYP3A4 CYP2C9, 2C19 (minor)
CYP2C9 CYP3A4 Sulf/Gluc CYP3A4
Systemic metabolites
Active Active Inactive Active Inactive Active
Clearance (L/hr/kg)
0.25 0.63 0.97 0.26 – 1.1 0.81 0.45
Adapted from Corsini et al. Pharmacol Ther 1999;84: 413-428.White CM. J Clin Pharmacol 2002;42:963-970.

Clinical Pharmacokinetics of Statins
Parameter Atorva Rosuva Fluva Lova Prava Simva
Excretion
t ½ (hr) 15 - 30 20.8 0.5 – 2.3 2.9 1.3 – 2.8 2 - 3
Urinary excretion (%)
Negligible 10 6 10 20 13
Fecal excretion (%)
Major route
90 90 83 71 58
Adapted from Corsini et al. Pharmacol Ther 1999;84: 413-428.White CM. J Clin Pharmacol 2002;42:963-970.

Fibrates

Which of the following statins levels is increased the most when combined with Gemfibrozil?
A. Fluvastatin
B. Atorvastatin
C. Pravastatin
D. Rosuvastatin

Statin/Fibrate Combination Therapy: Pharmacokinetic Interactions
GEMFIBROZIL FENOFIBRATEAtorvastatin in Cmax 1.4 fold No effect
Simvastatin in Cmax 2‐3 fold No effect
Pravastatin in Cmax 2.02‐fold No effect
Rosuvastatin in Cmax 1.56‐1.88‐fold No effect
Fluvastatin No effect No effect
Lovastatin in Cmax by 2‐3‐fold Not available
Pitavastatin in Cmax by 1.45–fold No effectTriCor [package insert]. Abbott Laboratories. 2004; Kyrklund C et al. Clin Pharmacol Ther. 2001;69:340‐345;Pan WJ et al. J Clin Pharmacol. 2000;40:316‐323; Backman JT et al. Clin Pharmacol Ther. 2000;68:122‐129;
Backman JT et al. Clin Pharmacol Ther. 2002;72:685‐691; Abbott Laboratories. Data on file. 2005;Davidson MH. Am J Cardiol. 2002;90:50K‐60K; Prueksaritanont T et al. Drug Metab Dispos. 2002;30:1280‐1287;
Martin PD et al. Clin Ther. 2003;25:459‐471; Bergman AJ et al. J Clin Pharmacol. 2004;44:1054‐1062
Davidson MH. Am J Cardiol. 2002;90(suppl):50K‐60K.Kyrklund C, et al. Clin Pharmacol Ther. 2001;69:340‐345.
Glucuronidation: Possible Explanation for Fibrate/Statin Interaction
Glucuronidation is a pathway for the elimination of the active hydroxy acid metabolites of atorvastatin, lovastatin, simvastatin, and cerivastatin
Clinical and preclinical studies indicate that gemfibrozil inhibits statin glucuronidation
Fenofibrate appears to have significantly less inhibitory effect on statin glucuronidation, and this may explain the lack of significant drug interaction between fenofibrate and statins

Niacin
Increased risk of skeletal muscle effectsDose of niacin > 1 gram in combination with statins should be avoided
Clinical ImplicationsPertains to “immediate release” niacinER‐ Niacin can be used up to 2 grams daily

Calcium Channel Blockers

Which of the following in correct regarding diltiazem/verapamil and why they interact with statins?A. They are strong inhibitors of CYP3A4 and inducers of P‐glycoproteinB. They are substrates for CYP3A4 and substrates and inducers of P‐glycoproteinC. They are moderate‐to‐weak inhibitors of CYP3A4 and substrates for CYP3A4 and P‐glycoproteinD. They are strong inhibitors of CYP3A4 and substrates for CYP3A4 and P‐glycoprotein

Diltiazem/VerampamilDiltiazem co‐administered with simvastatinC‐max of simvastatin increasedAUC of simvastatin increased by 5 foldElimination t1/2 increased by 2.3 foldDiltiazem co‐administered with lovastatinAUC increased 3.6 foldNo effect of half‐life

Amlodipine
Substrate of CYP3A4Amlodipine 10 mg co‐administered with 80 mg of simvastatin‐ 77% in simvastatin exposure

Calcium Channel Blockers
Statin CCB Increase in AUC
Simvastatin Diltiazem 3.7 fold
Lovastatin Diltiazem 3.6 fold
Simvastatin Verapamil 2.5 fold
Lovastatin Diltiazem 3.6 fold
Simvastatin Amlodipine 1.76 fold
Lovastatin Amlodipine 1.76 fold

Anti‐arrhythmics

Amiodarone/DronedaroneAmiodaroneMetabolized by CYP3A4 and CYP2C8Inhibitor of CYP3A4 and P‐glycoproteinSome level of inhibition of CYP1A2, CYP2C9, CYP2D6DronedaroneMetabolized extensively by CYP3A4Moderate inhibitor of CYP3A4 and CYP2D6Also inhibits P‐glycoprotein

Amiodarone/Dronedarone
AmiodaroneAUC increase of simvastatin by 75%Cmax increase of 75%DronedaroneAUC increase of simvastatin by 4 foldAUC increase of simvastatin acid by 2 fold

Antiarrhythmics
Statin Interacting Agent Increase in AUC
Simvastatin Amiodarone 1.76 fold
Lovastatin Amiodarone 1.76 fold
Simvastatin Dronedarone 3.9 fold
Lovastatin Dronedarone 3.9 fold

Ranolazine
Which of the following in true regarding ranolazine?
A. Inhibitor of CYP3A4 and CYP2D6 and inhibitor of P‐glycoproteinB. Metabolized by CYP3A4 and CYP2D6 and weak inhibitor of CYP3A4C. Metabolized by CYP3A4 and CYP2D6 and weak inhibitor of CYP2D6D. Inhibitor of CYP3A4 and CYP2D6 and substrate for P‐glycoprotein

Ranolazine
Metabolized predominately by CYP3A4 and to a lessor extent by CYP2D6Weak inhibitor of CYP3A4Co‐administration with simvastatinApproximately a 50% increase in AUC of simvastatinDoubles Cmax

Anti‐Anginals
Statin Interacting Agent Increase in AUC
Simvastatin Ranolazine 1.86 fold

Antiplatelet Agents

TicagrelorPredominantly metabolized by CYP3A4 and to a lesser extent by CYP3A5Substrate for P‐glycoprotein Weak inhibitor of CYP3A4 and P‐glycoprotein

Ticagrelor
23% increase in AUC of atorvastatin35% increase in Cmax with atovastatin81% increase in Cmax with simvastatin56% increase in AUC of simvastatin

Antiplatelet Agents
Statin Interacting Agent Effect on AUC
Simvastatin Ticagrelor 2‐3 fold
Atorvastatin Ticagrelor 1.36 fold
Lovastatin Ticagrelor 2‐3 fold

Immunosupressive AgentsCyclosporine/TacrolimusExtensively metabolized by hepatic and intestinal CYP3A4Inhibitor and substrate of P‐glycoprotein and OATP‐1B1
SirolimusExtensively metabolized by hepatic and intestinal CYP3A4 and P‐glycoprotein

Immunosupressive AgentsStatin Interacting Agent Effect in AUC
Simvastatin Cyclosporine/everolimus/sirolimus 6‐8 fold
Atorvastatin Cyclosporine/everolimus/sirolimus 6‐15 fold
Lovastatin Cyclosporine/everolimus/sirolimus 5‐10 fold
Fluvastatin Cyclosporine/everolimus/sirolimus 2‐4 fold
Pitavastatin Cyclosporine/everolimus/sirolimus 5 fold
Rosuvastatin Cyclosporine/everolimus/sirolimus 5‐10 fold
Pravastatin Cyclosporine/everolimus/sirolimus 5‐10 fold
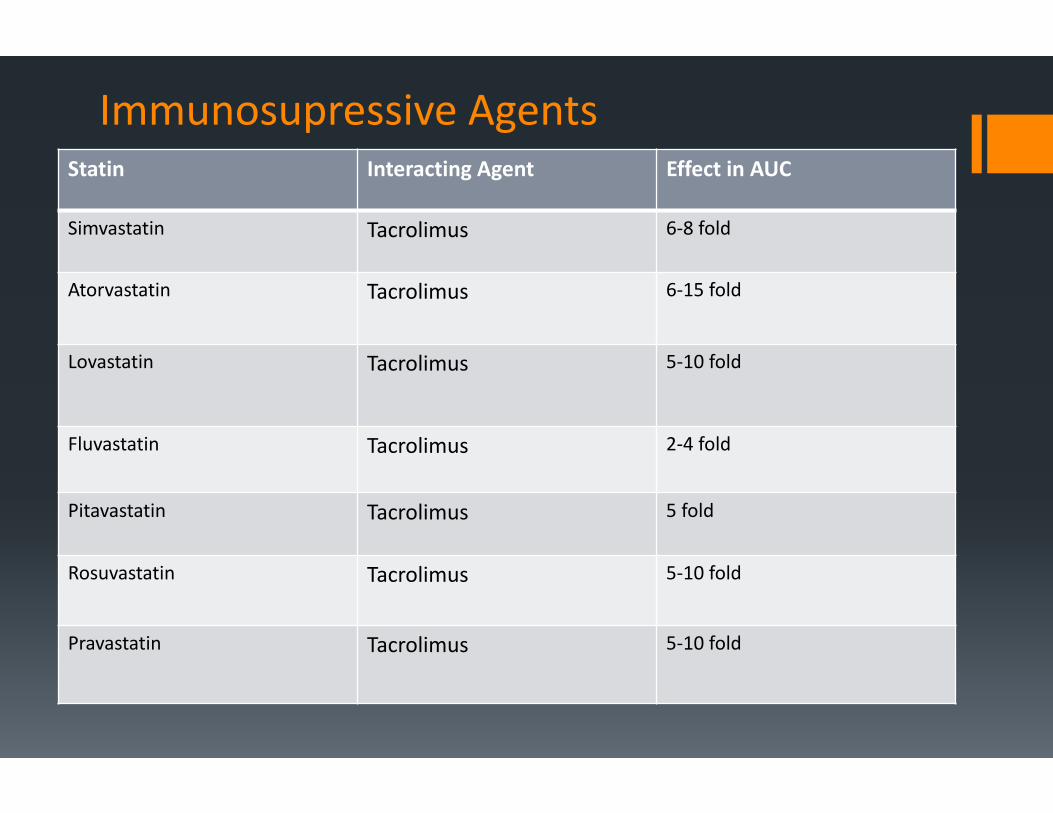
Immunosupressive AgentsStatin Interacting Agent Effect in AUC
Simvastatin Tacrolimus 6‐8 fold
Atorvastatin Tacrolimus 6‐15 fold
Lovastatin Tacrolimus 5‐10 fold
Fluvastatin Tacrolimus 2‐4 fold
Pitavastatin Tacrolimus 5 fold
Rosuvastatin Tacrolimus 5‐10 fold
Pravastatin Tacrolimus 5‐10 fold

Summary
Many cardiovascular agents have significant interactions with statinsUnderstanding the magnitude can assist with clinical decision makingHigh intensity statin may not be an option for all patients

Take Home Message
Varying degrees of interactions with statinMost significant occur with simvastatin and lovastatinClinical practice may dictate combinations that are not ideal