eun-ran kim - smcgismcgi.co.kr/lecture/infectious_colitis.pdf · most cause of infectious colitis :...
TRANSCRIPT

Eun-Ran Kim
Division of Gastroenterology, Department of Medicine
Samsung Medical Center

Colitis
– an inflammation of the colon
– diagnosed when the patient has diarrhea (≥ 3 unformed stools/day)
and has evidence of colonic inflammation of the following:
• Positive fecal markers
: numerous leukocytes, positive lactoferrin, or calprotectin
• Passage of many small volume stools containing gross blood
• Endoscopy revealing mucosal inflammation
Acute, chronic and persistent
– Acute : develops within 14 days of diarrhea onset
– Chronic : 30 or more days after development of diarrhea
Colitis (Colitides)

Differential diagnosis

The cause of infectious colitis

Common microbial cause
Emerg Infect Dis 2011 Jan;17(1):7-15
Journal of Infect ion (2012) 64,374-386
(2000-2008)

Most cause of infectious colitis : bacterial enteropathogens
Symptoms
: diarrhea with or without dysentery, abdominal pain, fever
Important microbial pathogens
– All regions : Salmonella, Shigella, Campylobacter
– Developing tropical & semitropical regions : Entamoeba histolytica
– Industrialized : Shiga toxin-producing Escherichia coli (STEC)
– Hospitalized : C. difficile infection (CDI)
≥ 30 days : consider IBD, or in endemic area, Entamoeba
histolytica or Schistosoma mansoni (africa)
Infectious colitis

Pathogenesis
– Invaded colonic mucosa
• Systemic sign and symptoms including fever, chill, toxicity
• Salmonella, Shigella, Campylobacter
– Non-invasive
• Attach to colonic mucosa, localozed inflammation
• Clostridium difficile, enteroaggregative, or STEC
Regardless of the etiology, clinical symptoms are quite similar.
Infectious colitis

the most important diagnostic test
: a single stool culture for bacterial causes of colitis
It is hard to prove the existence of pathogens.
: In more than 50% of cases of dysentery, an etiologic agent is not
identified despite using optimal diagnostic methods.
Patients whose symptoms have not improved within 1 week should
undergo a sigmoidoscopy or colonoscopy.
Infectious colitis


Endoscopy is not warranted for the initial evaluation.
Should be considered for patients with
– persistent symptoms
– inconclusive diagnosis after routine blood & stool tests
– failure to respond to empirical therapy
Suitable initial investigation : Flexible sigmoidoscopy with biopsy
– Acute diarrhea : suspected diffuse colitis (C. difficile )
– Chronic diarrhea : pregnant, significant comobidity, symptoms
characteristics of left sided colonic disease (tenesmus, urgency)
Colonoscopy : if the findings at sigmoidoscopy are inconclusive
The role of endoscopy

Prominent endoscopic features
– patchy or diffuse mucosal edema, mucosal erythema, focal or
coalescent haemorrhagic spots
– a variety of ulcerations occasionally with cobblestone appearance,
and spontaneous bleeding
Duration
– Acute : UC or ischemic colitis-like
– Subacute or chronic : CD-like
Location
– Shigella : intense involvement of the rectosigmoid
– Salmonella, Yersinia, Amoeba : cecum and ascending colon
Endoscopic findings

Endoscopic similarities

UC (ulcerative colitis) –like
– Shigella, Salmonella, Campylobacter, Amoeba, CMV
CD (Crohn’s disease)-like
– Salmonella, Campylobacter, Yersinia, Amoeba, intestinal Tbc,
CMV
Endoscopic findings

Shigella
UC-like
Yersinia
CD-like

Case
69 yrs old man
3 days ago, lower abdominal pain, diarrhea with fever
1 day ago, hematochezia
WBC 15240/L, CRP 24.08 g/dL

Stool Culture :
Shigella sonnei

Stool Culture :
Shigella sonnei

Histologic findings : Chronic inflammatory changes
– crypt architecture distorsion, crypt atrophy, basal lymphoid
aggregates
Differential diagnosis

Shigellosis
UC-like
Involvement : Rectosigmoid
15% : pancolitis
Prominent endoscopic findings
- erythema, severe edema
- irregular ulcers
- spontaneous bleeding

UC-like CD-like
Salmonellosis Involvement: terminal ileum, right side colon
Erythema, edema, granularity, loss of the normal vascular pattern
More severe : diffuse erythema, pitting edema, ulceration
(punctuate, aphthoid, aphthae, irregular (stellate), deep)
occasionally, denuded extensive areas of colonic mucosa

CD-like
Yersinia
Involvement : Right side colon
Endoscopic findings
- erosions, various forms of
ulcerations (usually punctuate)
- on other occasions,
mimics ulcerative colitis

Amebic colitis
UC-like CD-like
Involvement: cecum and Rt. Colon (70%), rectum and S colon
Acute: Diffuse erythema, granularity, friability resembling UC.
Chronic form : discrete or localized mucosal ulcers with a
characteristic pounched-out appearance (rolled edges) helps the
differential diagnosis from CD. (A flask shaped ulcer)

Usually non-specific but includes discrete ulcerations, varying
from punctate and superficial erosions to deep ulcers .
Histology
: typical inclusions which confirm the diagnosis
CMV colitis

Intestinal tuberculosis

Intestinal tuberculosis
CD : anorectal lesions, longitudinal ulcers, aphthous ulcers
and cobblestone pattern
Tbc : involvement of less than 4 segments, a patulous IC valve,
transverse ulcers, and scars or pseudopolyps

Distal or Left side colon
white yellow mucosal lesions including pseudomembranous
1/3 : non-specific erosions or erythemas
Clostridium difficile

Treatment
Empiric antibiotic therapy
– oral fluoroquinolone for 3-5 days
(in the absence of suspected EHEC or fluoroquinolone-resistant campylobacter infection)
• ciprofloxacin 500 mg twice daily
• norfloxacin 400 mg twice daily
• levofloxacin 500 mg once daily
Consideration
– with moderate to severe travelers' diarrhea as characterized by more
than four unformed stools daily, fever, blood, pus, or mucus in the stool
– with more than eight stools per day, volume depletion, symptoms for
more than one week, those in whom hospitalization is being
considered, and immunocompromised hosts


Eun-Ran Kim
Division of Gastroenterology, Department of Medicine
Samsung Medical Center

51 yrs old man
Previously healthy
1 day ago, sudden onset of abdominal pain, followed by
hematochezia
Case


Old age
Sudden onset of abdominal pain & hemtochezia
Endoscopy
– hyperemia, edema, ulceration
– rectal sparing
– resolved within 1-2 weeks
– Bx : coagulation necrosis
Ischemic colitis

29 yrs old female
2001.1. cervix ca -> radiation + chemotherapy
2001.8. hematochezia
Case


Radiation history due to cervix ca. or prostatic ca.
Endoscopy
– proximal rectum & distal sigmoid colon
– mucosal friability
– granularity with spontaneous bleeding
– multiple telangiectasia
Radiation colitis

48 yrs old female
10 years ago, constipation with straining
Anal bleeding, mucoid stool, tenesmus, lower abdominal pain
Case
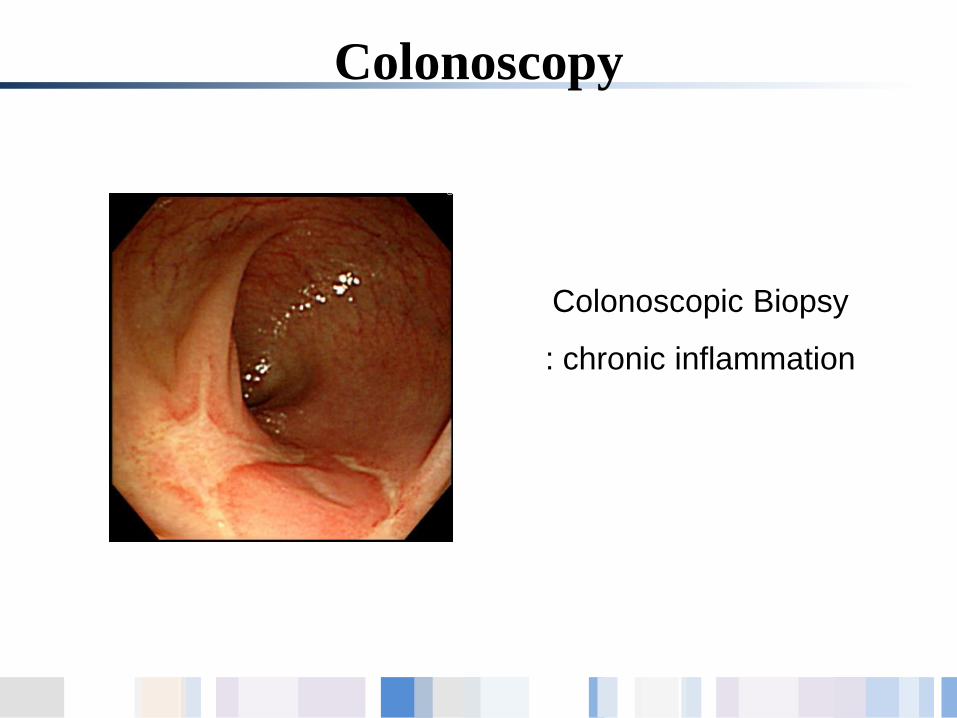
Colonoscopy
Colonoscopic Biopsy
: chronic inflammation

Defecography

A chronic course characterized by rectal bleeding,
disordered defecation, tenesmus and mucorrhea
Endoscopy
– anterior wall, 4 to 15 cm from the anal verge
– shallow ulcers with white, sloughy base surrounded by
a thin rim of erythematous mucosa
Solitary rectal ulcer syndrome

Histology
– characteristic
– obliteration of lamina propria by fibromuscular
proliferation of the muscularis mucosa
– streaming of fibroblasts and muscle fibers up between
crypts
– thickening of muscularis mucosa
– branching, distorted glandular crypts
– diffuse collagen infiltration of lamina propria
Solitary rectal ulcer syndrome

Sodium phosphate
– aphthous ulcers
– focal cryptitis
Bisacodyl suppository
– mucosal hyperemia
– obliteration of vascular pattern
Bowel preparation

Bowel preparation

Non specific colitis

중년 남성
Low abdominal discomfort
Bx : focal active inflammation, terminal ileum

Diarrhea (-) Hematochezia (-) Wt loss (-) Oral ulcer (-)
ESR/CRP : normal
“복통이나 설사가 심해지거나 혈변이 생기면 들리세요”
Colonoscopy, 1 year later

Gastrointest Endosc 2010;72:1226

2개월 전 외부 병원에서 건강 검진으로 대장내시경 시행
Young female

현재 특이 증상 없음
건강 검진 1주일전 발열, 복통, 설사
Colonoscopy 6 months later

Conclusions
장염의 정확한 진단을 위해서는 자세한 병력청취가 중요하다.
대장내시경 소견의 이해도 중요하다.
그러나 환자의 병력과 여러 가지 검사 소견을 종합적으로
검토하여야 한다.
때로는 경과 관찰로 환자의 변화를 파악하는 것도 중요하다.