establishing medical operations coordination cells …...2020/04/24 · patient transfer...
TRANSCRIPT

UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Establishing Medical Operations Coordination Cells (MOCCs) for COVID-19
April 24 2020
1 UnclassifiedFor Public Use
Access the recorded webinar here httpsattendeegotowebinarcomrecording256769356898835472
Access speaker bios herehttpsfilesasprtraciehhsgovdocumentsestablishing-mocc-for-covid-19-webinar-speaker-biospdf
Access Q and A here httpsfilesasprtraciehhsgovdocumentsaspr-tracie-ta-mocc-webinar-qa-finalpdf
UnclassifiedFor Public Use
llirL TECHNICAL IIPr RESOURCE$
__II_ ASS ISTANCE CENTER
J ~ INFORMATION ~ EXCHANGE
asprtraciehhsgov
1-844-5-TRACIE
askasprtraciehhsgov
ASPR AUIS1ANT bulllCUTtamp~ ~00
UIPAUDgt1111 ~gtIC UfPO~H HUtTHCdl h oUGpound NC1 HpoundhH0Npound~~
I NfORMAT IONGAIEWAf
ASPR TRACIE Three Domains
bull Self-service collection of audience-tailored materials
bull Subject-specific SME-reviewed ldquoTopic Collectionsrdquo bull Unpublished and SME peer-reviewed materials
highlighting real-life tools and experiences
bull Personalized support and responses to requests forinformation and technical assistance
bull Accessible by toll-free number (1844-5-TRACIE)email (askasprtraciehhsgov) or web form (ASPRtraciehhsgov)
bull Area for password-protected discussion amongvetted users in near real-time
bull Ability to support chats and the peer-to-peerexchange of user-developed templates plans andother materials
2
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Resources
3
bull
bullbullbull
ASPR TRACIE COVID-19 Page
ndash Critical Care Surge Resourcesndash Hospital Triage Screening Resourcesndash Regional Support Resources
ASPR COVID-19 PageCDC COVID-19 PageCoronavirusgov
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Moderator Meghan Treber MS ASPR TRACIE
UnclassifiedFor Public Use 4
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Melissa Harvey RN MSPH Hospital Team Lead Healthcare Resilience Task Force Director Health System Management Office of the Chief Medical Officer US Department of Homeland Security
5 UnclassifiedFor Public Use
6Saving Lives Protecting Americans
Executive Summary
Some hospitals areoverwhelmed with
COVID-19 patients while successful mitigation has
created excess capacity in nearby hospitals creating
an opportunity to transferpatients
MOCCs are a strategy to optimize patientdistribution by
augmenting EOCs withclinical experts that
synthesize and coordinate healthcare capacity
The MOCC strategy can beimplemented nationwide (at sub-state state- and
regional levels) through amodifiable toolkit technical
assistance and federal funding permitting
flexibility for states while optimizing patient
distribution
6
7Saving Lives Protecting Americans
bullbull
--
MOCCs | Problem Statement COVID-19 has resulted in asymmetrical hospital utilization certain regionsrsquo healthcare systems have experienced a surge in patients while others have excess capacity
What are we seeing
Hospitals are the preferred location for seriously ill Facilities with 50+ Beds COVID-19 patients due to existing patient care expertise and resources
Most hot spots are geographically localized overwhelming local healthcare facilities
While some facilities are overwhelmed successfulmitigation in neighboring areas has created excesscapacity in nearby hospitals creating an opportunity to transfer patients
bull bull bull bull
bull middott middot
bull t
bull
D
bull
middot~middotmiddotmiddot
bull le bull l bull bull bull bullt + bull_ I bull bull bull bull bullbull bull bull bull + bull middotmiddot middot middot ~ bullmiddot middotmiddotJ~
-i bullbull bullbullbullbull -ii bull ~ bull ~ bull ~bull bull bull Abull~
bull bullbull i bullbull bullbull middotr bullbullbull bull bullbull bull middotmiddot
i l _
Number of ICU Beds
above 90 control limit of national average below 90 control limit of national average within 90 control limit of national average
Patient transfer coordination through dedicated staffing and data collectionanalysis can improve patient allocation at the sub-state state and federal levels
bull
bullbull
0
7
8Saving Lives Protecting Americans
bull
A MOCC AIMS TO
Move patients to the at the right to improve staff and right time in the patientsupplies provider right way well-being
8
9Saving Lives Protecting Americans
MOCCs | Concept MOCCs can be activated at the Sub-State Regional State and Federal levels to facilitate patient movement and resource allocation during a surge event There are three types of MOCCs included in the concept sub-state Regional Medical Operations Coordination Centers (RMOCCs) State Medical Operations Coordination Centers (SMOCCs) and Federal Medical Operations Coordination Centers (FMOCCs)
RMOCC Sub-State Level
SMOCC State Level
FMOCC Federal Level
HHS Region A HHS Region B
RegionA
State A
RegionB
State A
RegionC
State A
State D HHS Region B
State E HHS Region B
State A HHS Region A
State B HHS Region A
State C HHS Region A
RegionD
State B
RegionE
State B
RegionF
State C
RegionG
State C Region
H State D
RegionI
State D
RegionJ
State D
RegionK
State E
RegionL
State E Region
M State E
State F HHS Region B
RegionN
State F
RegionO
State F
Patient transfer coordination activity originates with the RMOCC The SMOCC can help transfer patients to a facility in a neighboring sub-state region The FMOCC can transfer patients to a neighboring state or Federal
HHS Region if that is closer 9
MOCCs | General Activity Summary
MOCCs are cells within emergency operations centers (EOCs) at the sub-state regional state and federal levels (FEMAHHS regions) that facilitate patient movement and resource allocation
MOCC PRIORITIES
bull Adding clinical staff to existing EOCs and RRCCsbull Establishing stakeholder agreements that allow for collecting data regarding health system capacity synthesizing the data to
understand the needs of the system and determining areas of the system that may be overwhelmedbull Facilitating movement of patients staff and supplies between healthcare facilities andor states
MOCC ROLE
bull Acting as a single point of contact (POC) for requests from multiple stakeholders such as healthcare facilities RMOCCs and SMOCCsbull Reviewing facilitating and processing patient movement staffing and supply requests and providing medical consultation to
facilitate the decompression of health systems
MOCC DATA ACTIVITIES
bull Collecting analyzing and disseminating information to and from stakeholders to develop comprehensive situational awarenessbull Establishing protocols systems and triggers to inform operational planning stakeholder communications and transfer decision
making
10
~ - ~--~- ----- -
MOCCs | Toolkit
The MOCCs Toolkit contains information on funding a MOCC standard operating procedures for each type of MOCC including integration with ESF-8 roles and responsibilities staffing and transport coordination
FUNDING
bull FEMA Public Assistancebull FEMA Mission Assignmentbull ASPR Hospital Preparedness
Programbull CDC Public Health Emergency
PreparednessCrisis Agreement
STANDARD OPERATING TRANSPORT PROCEDURES COORDINATION
bull RMOCCSMOCC
bull FMOCC
bull Transportation workflows andbull transfer checklists
Each MOCC SOP includes details on bullbullbullbullbull
MOCC Integration with ESF-8Roles and ResponsibilitiesStaffingOperationsPatient MovementMedical Resource Sharing
The MOCCs Toolkit will be located on ASPR TRACIE
11
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Steven Mitchell MD FACEP Medical Director Western Washington Regional COVID Coordination Center Medical Director Emergency Department Harborview Medical Center
12 UnclassifiedFor Public Use
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Western Washington MOCC
bull
bull
bull
First US COVID-19 case Jan 21ndash Snohomish County WA
First US COVID-19 death Feb 29ndash King County WA
First major outbreak late FebMarch1
ndash 167 cases at Long-Term Care Facilitybull 101 residents 50 staff and 16 visitorsbull 43 deaths
1 Epidemiology of Covid-19 in a Long-Term Care Facility in King County Washington N Engl J Med 2020 Mar 27
13
UnclassifiedFor Public Use
THE WALL STREET JOURNAL
One Nursing Home 35 Coronavirus Deaths Inside the Kirkland Disaster
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
King County LTCF Outbreak
~be ~cu Uork ~itnes
Its Pure Panic A Wrenching Wait at Nursing Home Where Coronavirus Took Hold Cut off from their relatives inside a virus-stricken nursing center families are frantically searching for help and basic information
14
UnclassifiedFor Public Use
Characteristics and Outcomes of 21 Critshyically Ill Patients With COVID-19 in Washshyington State Matt Arentz MD1 Eric Yim MD2 Lindy Klaff MD2 et al
Author Affiliations I Article Information
JAMA Published online March 19 2020 doi101001jama20204326
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Single LTCF - Single Hospital
bull Overwhelmed bull No coordination bull Not isolated example
15
UnclassifiedFor Public Use
~) NORTHWEST HEALTHCARE HARBORVIEW MEDICAL CENTER
UW Medicine [f]KingCounty
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Medical Operations Coordinating Cell
bull Disaster Medical Coordination Center
bull Regional COVID Coordination Center (RC3) ndash Harborview Medical CenterKing County ndash Northwest Health Response Network
16
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Regional COVID Coordinating Center ndash Western Washington
17
UnclassifiedFor Public Use
Staffing
Impacts
Resource
Impacts
Ventilators PPE
urveillance of Hospitals
Health
Surveillance of Congregant
Settings
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Two Surveillance Pillars of the RC3
18
UnclassifiedFor Public Use
Health System __-1
Level Loadin
ealth System
Coordination of Resources
ASPR AUIS1ANT bulllCUTtamp~ ~00
UIPAUDgt1111 ~gtIC UfPO~H HUtTHCdl h oUGpound NC1 HpoundhH0Npound~~
I NfORMAT IONGAIEWAf
Two Coordination Pillars of the RC3
19
UnclassifiedFor Public Use
WA HEALTH G) About f) Stevo Mltchell
E-- Home
Q~ _ (WIJ - _uw_ 0
COVIDbulllltl1-t1 ltD _
ltD _
ltD AvilfllHlty - ~c_
44
J -(--
8 j ((MON_
36 j
--0 18 22 0 42 2~
jll 4Jtbull
r 11H -middot- __ ~ -- I 1rA
I --- --J - 353 600 500 1000 806 00 -- -- --
8 J _
101 25
fj)
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH hoUGpoundNC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Emergency Response Platform - Microsoft
bull Constrained Resources ndash Staffing ndash Beds bull Critical Care bull Acute Care
ndash Equipment bull Ventilators bull PPE
ndash COVID-19 patients
20
UnclassifiedFor Public Use
WA HEALTH C) About - Steve
~ Homo
6-hiyenHiiii+MF _ _ a
KING
43 COVID JM1Q
267
55 CD IDlnn1bned
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Emergency Response Platform - Microsoft
bull Next Releasendash Long Term Care Facilitiesbull COVID-19 Impactsndash Positive Patientsndash Positive Health Care
Workers raquo of staff impacted
bull PPE availability
21
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
William Fales MD FACEP FAEMS Medical Director Division of EMS and Trauma Michigan Department of Health and Human Services
22 UnclassifiedFor Public Use
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michiganrsquos Healthcare Preparedness Program bull Michigan Department of Health and Human Services ndash Bureau of EMS Trauma and Preparedness
bull 8 Regional Healthcare Coalitions ndash Hospitals EMS LPH EM LTC Tribal Health ndash Regional Coordinator Assistant Coordinator
Medical Director (25 FTE) ndash Regional Medical Coordination Center bull Multi-Agency Coordination Center bull Statewide use of EMResource by hospitals EMS
23
UnclassifiedFor Public Use
p ror
~ SC ON5
Sault Ste Marie
N
bull
Huron
Madison Milwa uk ee Graed Rapids bull bull e bull ~ 3rnia
L~nsi~ g bull - It bull
bullbullbullbull bull bull bull bull De troi t
bull Glwcago bull bull bull
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Michigan COVID-19 bull bull
bull
First 2 cases ndash March 10 Asymmetric epidemiology ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
24
UnclassifiedFor Public Use
Barrie
Toronto
Hamilton
bull bull
bull
Lake Ontario
bull Ro~besterbull
bull
bull
Brockville bull Kingston
~~w voRK
bull bull bull
bull
bull Pt0NfV VAN1A bull
bull
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H I NfOR MATION GATEWAY
bull
bull bull ~ ba riy
bull bull
Michigan COVID-19 bull First 2 cases ndash March 10
Asymmetric epidemiology bull ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
bull Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
25
UnclassifiedFor Public Use
I I I I I I I I I I I I I
ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City COVID-19 Daily Hospital Admissions
New York City vs Detroit 1800 1600 1400 1200 1000 800 600 400 200 0
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 26
UnclassifiedFor Public Use ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City
1 1 I 11111 111 11 11 1111 1 II II 1 1 1
400
300
200
COVID-19 Daily Hospital Admissions Per 1 Million PopulationNew York City vs Detroit
40-Day Post-Outbreak Mortality bull NY City 646 deaths per million bull Detroit 919 deaths per million
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 27
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Goal bull Save lives and reduce pain and suffering by optimizing
the use of the statersquos healthcare resources ndash Extend conventional standards of care to as many
patients as possible ndash Minimize the need for crisis standards of care bull Especially while conventional capacity exists
28
UnclassifiedFor Public Use
--
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Components bull Relief Hospitals
bull Alternate Care Sites EMS
ndash Home Care Sites
ndash Relief Personnel
29
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals vs Alternate Care Sites bull Relief Hospitals The objective is to extend the
conventional standard of care to as many citizens in need as possible (ie minimize the need to move intocrisis standards of care)
bull Alternate Care Sites (ACS) The objective is to delivercrisis standards of care (as close to the conventional standard of care as possible) in extreme conditions in which the conventional standard of care can not be provided at overloaded hospitals
30
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital ldquoAskrdquo bull Hospitals have been previously asked to be able to
surge an additional 20 above average daily census ndash Increased to 50 ldquosuper surgerdquo
bull Relief Hospitals provide 10 of their expanded capacity to assist severely impacted hospitals ndash While preserving 50 of super-surge capacity bull Many hospitals at very low census
31
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals and Patient Redistribution
bull Intra-Health System Transfer ndash Coordinated by specific health system
bull Intra-Regional Transfer ndash Coordinated by Regional Medical Coordination Center
bull Statewide Transfer ndash Coordinated by Inter-Hospital Coordination Unit bull AKA Medical Operations Coordination Cell (MOCC)
32
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Statewide Inter-Hospital Coordination Unit State EmergencyOperations Center
Planning Finance Operations
Health Branch
Inter-HospitalCoordination Unit
Physician Consultant
EMS Coordination Group
Logistics
MDHHS Health Emergency Operations
Center
Medical Operations
Coordination Cell
33
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs and Patient Redistribution Regional Medical
Coordination Center bull Relief hospitals declare status on
EMResource bull RMCC receives request from
transferring hospital bull RMCC identifies Relief Hospital(s) bull Transferring hospital contacts
Relief Hospital directly bull Relief Hospital accepts patient(s) bull RMCC coordinates EMS PRN
Statewide Inter-Hospital Coordination Unit
Relief hospitals declare status on EMResource
IHCU receives request from RMCC on behalf of transferring hospital
IHCU identifies Relief Hospital(s) Transferring hospital contacts Relief
Hospital directly Relief Hospital accepts patient(s) IHCU coordinates EMS PRN
34
UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use
llirL TECHNICAL IIPr RESOURCE$
__II_ ASS ISTANCE CENTER
J ~ INFORMATION ~ EXCHANGE
asprtraciehhsgov
1-844-5-TRACIE
askasprtraciehhsgov
ASPR AUIS1ANT bulllCUTtamp~ ~00
UIPAUDgt1111 ~gtIC UfPO~H HUtTHCdl h oUGpound NC1 HpoundhH0Npound~~
I NfORMAT IONGAIEWAf
ASPR TRACIE Three Domains
bull Self-service collection of audience-tailored materials
bull Subject-specific SME-reviewed ldquoTopic Collectionsrdquo bull Unpublished and SME peer-reviewed materials
highlighting real-life tools and experiences
bull Personalized support and responses to requests forinformation and technical assistance
bull Accessible by toll-free number (1844-5-TRACIE)email (askasprtraciehhsgov) or web form (ASPRtraciehhsgov)
bull Area for password-protected discussion amongvetted users in near real-time
bull Ability to support chats and the peer-to-peerexchange of user-developed templates plans andother materials
2
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Resources
3
bull
bullbullbull
ASPR TRACIE COVID-19 Page
ndash Critical Care Surge Resourcesndash Hospital Triage Screening Resourcesndash Regional Support Resources
ASPR COVID-19 PageCDC COVID-19 PageCoronavirusgov
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Moderator Meghan Treber MS ASPR TRACIE
UnclassifiedFor Public Use 4
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Melissa Harvey RN MSPH Hospital Team Lead Healthcare Resilience Task Force Director Health System Management Office of the Chief Medical Officer US Department of Homeland Security
5 UnclassifiedFor Public Use
6Saving Lives Protecting Americans
Executive Summary
Some hospitals areoverwhelmed with
COVID-19 patients while successful mitigation has
created excess capacity in nearby hospitals creating
an opportunity to transferpatients
MOCCs are a strategy to optimize patientdistribution by
augmenting EOCs withclinical experts that
synthesize and coordinate healthcare capacity
The MOCC strategy can beimplemented nationwide (at sub-state state- and
regional levels) through amodifiable toolkit technical
assistance and federal funding permitting
flexibility for states while optimizing patient
distribution
6
7Saving Lives Protecting Americans
bullbull
--
MOCCs | Problem Statement COVID-19 has resulted in asymmetrical hospital utilization certain regionsrsquo healthcare systems have experienced a surge in patients while others have excess capacity
What are we seeing
Hospitals are the preferred location for seriously ill Facilities with 50+ Beds COVID-19 patients due to existing patient care expertise and resources
Most hot spots are geographically localized overwhelming local healthcare facilities
While some facilities are overwhelmed successfulmitigation in neighboring areas has created excesscapacity in nearby hospitals creating an opportunity to transfer patients
bull bull bull bull
bull middott middot
bull t
bull
D
bull
middot~middotmiddotmiddot
bull le bull l bull bull bull bullt + bull_ I bull bull bull bull bullbull bull bull bull + bull middotmiddot middot middot ~ bullmiddot middotmiddotJ~
-i bullbull bullbullbullbull -ii bull ~ bull ~ bull ~bull bull bull Abull~
bull bullbull i bullbull bullbull middotr bullbullbull bull bullbull bull middotmiddot
i l _
Number of ICU Beds
above 90 control limit of national average below 90 control limit of national average within 90 control limit of national average
Patient transfer coordination through dedicated staffing and data collectionanalysis can improve patient allocation at the sub-state state and federal levels
bull
bullbull
0
7
8Saving Lives Protecting Americans
bull
A MOCC AIMS TO
Move patients to the at the right to improve staff and right time in the patientsupplies provider right way well-being
8
9Saving Lives Protecting Americans
MOCCs | Concept MOCCs can be activated at the Sub-State Regional State and Federal levels to facilitate patient movement and resource allocation during a surge event There are three types of MOCCs included in the concept sub-state Regional Medical Operations Coordination Centers (RMOCCs) State Medical Operations Coordination Centers (SMOCCs) and Federal Medical Operations Coordination Centers (FMOCCs)
RMOCC Sub-State Level
SMOCC State Level
FMOCC Federal Level
HHS Region A HHS Region B
RegionA
State A
RegionB
State A
RegionC
State A
State D HHS Region B
State E HHS Region B
State A HHS Region A
State B HHS Region A
State C HHS Region A
RegionD
State B
RegionE
State B
RegionF
State C
RegionG
State C Region
H State D
RegionI
State D
RegionJ
State D
RegionK
State E
RegionL
State E Region
M State E
State F HHS Region B
RegionN
State F
RegionO
State F
Patient transfer coordination activity originates with the RMOCC The SMOCC can help transfer patients to a facility in a neighboring sub-state region The FMOCC can transfer patients to a neighboring state or Federal
HHS Region if that is closer 9
MOCCs | General Activity Summary
MOCCs are cells within emergency operations centers (EOCs) at the sub-state regional state and federal levels (FEMAHHS regions) that facilitate patient movement and resource allocation
MOCC PRIORITIES
bull Adding clinical staff to existing EOCs and RRCCsbull Establishing stakeholder agreements that allow for collecting data regarding health system capacity synthesizing the data to
understand the needs of the system and determining areas of the system that may be overwhelmedbull Facilitating movement of patients staff and supplies between healthcare facilities andor states
MOCC ROLE
bull Acting as a single point of contact (POC) for requests from multiple stakeholders such as healthcare facilities RMOCCs and SMOCCsbull Reviewing facilitating and processing patient movement staffing and supply requests and providing medical consultation to
facilitate the decompression of health systems
MOCC DATA ACTIVITIES
bull Collecting analyzing and disseminating information to and from stakeholders to develop comprehensive situational awarenessbull Establishing protocols systems and triggers to inform operational planning stakeholder communications and transfer decision
making
10
~ - ~--~- ----- -
MOCCs | Toolkit
The MOCCs Toolkit contains information on funding a MOCC standard operating procedures for each type of MOCC including integration with ESF-8 roles and responsibilities staffing and transport coordination
FUNDING
bull FEMA Public Assistancebull FEMA Mission Assignmentbull ASPR Hospital Preparedness
Programbull CDC Public Health Emergency
PreparednessCrisis Agreement
STANDARD OPERATING TRANSPORT PROCEDURES COORDINATION
bull RMOCCSMOCC
bull FMOCC
bull Transportation workflows andbull transfer checklists
Each MOCC SOP includes details on bullbullbullbullbull
MOCC Integration with ESF-8Roles and ResponsibilitiesStaffingOperationsPatient MovementMedical Resource Sharing
The MOCCs Toolkit will be located on ASPR TRACIE
11
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Steven Mitchell MD FACEP Medical Director Western Washington Regional COVID Coordination Center Medical Director Emergency Department Harborview Medical Center
12 UnclassifiedFor Public Use
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Western Washington MOCC
bull
bull
bull
First US COVID-19 case Jan 21ndash Snohomish County WA
First US COVID-19 death Feb 29ndash King County WA
First major outbreak late FebMarch1
ndash 167 cases at Long-Term Care Facilitybull 101 residents 50 staff and 16 visitorsbull 43 deaths
1 Epidemiology of Covid-19 in a Long-Term Care Facility in King County Washington N Engl J Med 2020 Mar 27
13
UnclassifiedFor Public Use
THE WALL STREET JOURNAL
One Nursing Home 35 Coronavirus Deaths Inside the Kirkland Disaster
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
King County LTCF Outbreak
~be ~cu Uork ~itnes
Its Pure Panic A Wrenching Wait at Nursing Home Where Coronavirus Took Hold Cut off from their relatives inside a virus-stricken nursing center families are frantically searching for help and basic information
14
UnclassifiedFor Public Use
Characteristics and Outcomes of 21 Critshyically Ill Patients With COVID-19 in Washshyington State Matt Arentz MD1 Eric Yim MD2 Lindy Klaff MD2 et al
Author Affiliations I Article Information
JAMA Published online March 19 2020 doi101001jama20204326
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Single LTCF - Single Hospital
bull Overwhelmed bull No coordination bull Not isolated example
15
UnclassifiedFor Public Use
~) NORTHWEST HEALTHCARE HARBORVIEW MEDICAL CENTER
UW Medicine [f]KingCounty
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Medical Operations Coordinating Cell
bull Disaster Medical Coordination Center
bull Regional COVID Coordination Center (RC3) ndash Harborview Medical CenterKing County ndash Northwest Health Response Network
16
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Regional COVID Coordinating Center ndash Western Washington
17
UnclassifiedFor Public Use
Staffing
Impacts
Resource
Impacts
Ventilators PPE
urveillance of Hospitals
Health
Surveillance of Congregant
Settings
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Two Surveillance Pillars of the RC3
18
UnclassifiedFor Public Use
Health System __-1
Level Loadin
ealth System
Coordination of Resources
ASPR AUIS1ANT bulllCUTtamp~ ~00
UIPAUDgt1111 ~gtIC UfPO~H HUtTHCdl h oUGpound NC1 HpoundhH0Npound~~
I NfORMAT IONGAIEWAf
Two Coordination Pillars of the RC3
19
UnclassifiedFor Public Use
WA HEALTH G) About f) Stevo Mltchell
E-- Home
Q~ _ (WIJ - _uw_ 0
COVIDbulllltl1-t1 ltD _
ltD _
ltD AvilfllHlty - ~c_
44
J -(--
8 j ((MON_
36 j
--0 18 22 0 42 2~
jll 4Jtbull
r 11H -middot- __ ~ -- I 1rA
I --- --J - 353 600 500 1000 806 00 -- -- --
8 J _
101 25
fj)
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH hoUGpoundNC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Emergency Response Platform - Microsoft
bull Constrained Resources ndash Staffing ndash Beds bull Critical Care bull Acute Care
ndash Equipment bull Ventilators bull PPE
ndash COVID-19 patients
20
UnclassifiedFor Public Use
WA HEALTH C) About - Steve
~ Homo
6-hiyenHiiii+MF _ _ a
KING
43 COVID JM1Q
267
55 CD IDlnn1bned
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Emergency Response Platform - Microsoft
bull Next Releasendash Long Term Care Facilitiesbull COVID-19 Impactsndash Positive Patientsndash Positive Health Care
Workers raquo of staff impacted
bull PPE availability
21
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
William Fales MD FACEP FAEMS Medical Director Division of EMS and Trauma Michigan Department of Health and Human Services
22 UnclassifiedFor Public Use
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michiganrsquos Healthcare Preparedness Program bull Michigan Department of Health and Human Services ndash Bureau of EMS Trauma and Preparedness
bull 8 Regional Healthcare Coalitions ndash Hospitals EMS LPH EM LTC Tribal Health ndash Regional Coordinator Assistant Coordinator
Medical Director (25 FTE) ndash Regional Medical Coordination Center bull Multi-Agency Coordination Center bull Statewide use of EMResource by hospitals EMS
23
UnclassifiedFor Public Use
p ror
~ SC ON5
Sault Ste Marie
N
bull
Huron
Madison Milwa uk ee Graed Rapids bull bull e bull ~ 3rnia
L~nsi~ g bull - It bull
bullbullbullbull bull bull bull bull De troi t
bull Glwcago bull bull bull
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Michigan COVID-19 bull bull
bull
First 2 cases ndash March 10 Asymmetric epidemiology ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
24
UnclassifiedFor Public Use
Barrie
Toronto
Hamilton
bull bull
bull
Lake Ontario
bull Ro~besterbull
bull
bull
Brockville bull Kingston
~~w voRK
bull bull bull
bull
bull Pt0NfV VAN1A bull
bull
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H I NfOR MATION GATEWAY
bull
bull bull ~ ba riy
bull bull
Michigan COVID-19 bull First 2 cases ndash March 10
Asymmetric epidemiology bull ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
bull Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
25
UnclassifiedFor Public Use
I I I I I I I I I I I I I
ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City COVID-19 Daily Hospital Admissions
New York City vs Detroit 1800 1600 1400 1200 1000 800 600 400 200 0
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 26
UnclassifiedFor Public Use ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City
1 1 I 11111 111 11 11 1111 1 II II 1 1 1
400
300
200
COVID-19 Daily Hospital Admissions Per 1 Million PopulationNew York City vs Detroit
40-Day Post-Outbreak Mortality bull NY City 646 deaths per million bull Detroit 919 deaths per million
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 27
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Goal bull Save lives and reduce pain and suffering by optimizing
the use of the statersquos healthcare resources ndash Extend conventional standards of care to as many
patients as possible ndash Minimize the need for crisis standards of care bull Especially while conventional capacity exists
28
UnclassifiedFor Public Use
--
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Components bull Relief Hospitals
bull Alternate Care Sites EMS
ndash Home Care Sites
ndash Relief Personnel
29
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals vs Alternate Care Sites bull Relief Hospitals The objective is to extend the
conventional standard of care to as many citizens in need as possible (ie minimize the need to move intocrisis standards of care)
bull Alternate Care Sites (ACS) The objective is to delivercrisis standards of care (as close to the conventional standard of care as possible) in extreme conditions in which the conventional standard of care can not be provided at overloaded hospitals
30
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital ldquoAskrdquo bull Hospitals have been previously asked to be able to
surge an additional 20 above average daily census ndash Increased to 50 ldquosuper surgerdquo
bull Relief Hospitals provide 10 of their expanded capacity to assist severely impacted hospitals ndash While preserving 50 of super-surge capacity bull Many hospitals at very low census
31
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals and Patient Redistribution
bull Intra-Health System Transfer ndash Coordinated by specific health system
bull Intra-Regional Transfer ndash Coordinated by Regional Medical Coordination Center
bull Statewide Transfer ndash Coordinated by Inter-Hospital Coordination Unit bull AKA Medical Operations Coordination Cell (MOCC)
32
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Statewide Inter-Hospital Coordination Unit State EmergencyOperations Center
Planning Finance Operations
Health Branch
Inter-HospitalCoordination Unit
Physician Consultant
EMS Coordination Group
Logistics
MDHHS Health Emergency Operations
Center
Medical Operations
Coordination Cell
33
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs and Patient Redistribution Regional Medical
Coordination Center bull Relief hospitals declare status on
EMResource bull RMCC receives request from
transferring hospital bull RMCC identifies Relief Hospital(s) bull Transferring hospital contacts
Relief Hospital directly bull Relief Hospital accepts patient(s) bull RMCC coordinates EMS PRN
Statewide Inter-Hospital Coordination Unit
Relief hospitals declare status on EMResource
IHCU receives request from RMCC on behalf of transferring hospital
IHCU identifies Relief Hospital(s) Transferring hospital contacts Relief
Hospital directly Relief Hospital accepts patient(s) IHCU coordinates EMS PRN
34
UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Resources
3
bull
bullbullbull
ASPR TRACIE COVID-19 Page
ndash Critical Care Surge Resourcesndash Hospital Triage Screening Resourcesndash Regional Support Resources
ASPR COVID-19 PageCDC COVID-19 PageCoronavirusgov
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Moderator Meghan Treber MS ASPR TRACIE
UnclassifiedFor Public Use 4
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Melissa Harvey RN MSPH Hospital Team Lead Healthcare Resilience Task Force Director Health System Management Office of the Chief Medical Officer US Department of Homeland Security
5 UnclassifiedFor Public Use
6Saving Lives Protecting Americans
Executive Summary
Some hospitals areoverwhelmed with
COVID-19 patients while successful mitigation has
created excess capacity in nearby hospitals creating
an opportunity to transferpatients
MOCCs are a strategy to optimize patientdistribution by
augmenting EOCs withclinical experts that
synthesize and coordinate healthcare capacity
The MOCC strategy can beimplemented nationwide (at sub-state state- and
regional levels) through amodifiable toolkit technical
assistance and federal funding permitting
flexibility for states while optimizing patient
distribution
6
7Saving Lives Protecting Americans
bullbull
--
MOCCs | Problem Statement COVID-19 has resulted in asymmetrical hospital utilization certain regionsrsquo healthcare systems have experienced a surge in patients while others have excess capacity
What are we seeing
Hospitals are the preferred location for seriously ill Facilities with 50+ Beds COVID-19 patients due to existing patient care expertise and resources
Most hot spots are geographically localized overwhelming local healthcare facilities
While some facilities are overwhelmed successfulmitigation in neighboring areas has created excesscapacity in nearby hospitals creating an opportunity to transfer patients
bull bull bull bull
bull middott middot
bull t
bull
D
bull
middot~middotmiddotmiddot
bull le bull l bull bull bull bullt + bull_ I bull bull bull bull bullbull bull bull bull + bull middotmiddot middot middot ~ bullmiddot middotmiddotJ~
-i bullbull bullbullbullbull -ii bull ~ bull ~ bull ~bull bull bull Abull~
bull bullbull i bullbull bullbull middotr bullbullbull bull bullbull bull middotmiddot
i l _
Number of ICU Beds
above 90 control limit of national average below 90 control limit of national average within 90 control limit of national average
Patient transfer coordination through dedicated staffing and data collectionanalysis can improve patient allocation at the sub-state state and federal levels
bull
bullbull
0
7
8Saving Lives Protecting Americans
bull
A MOCC AIMS TO
Move patients to the at the right to improve staff and right time in the patientsupplies provider right way well-being
8
9Saving Lives Protecting Americans
MOCCs | Concept MOCCs can be activated at the Sub-State Regional State and Federal levels to facilitate patient movement and resource allocation during a surge event There are three types of MOCCs included in the concept sub-state Regional Medical Operations Coordination Centers (RMOCCs) State Medical Operations Coordination Centers (SMOCCs) and Federal Medical Operations Coordination Centers (FMOCCs)
RMOCC Sub-State Level
SMOCC State Level
FMOCC Federal Level
HHS Region A HHS Region B
RegionA
State A
RegionB
State A
RegionC
State A
State D HHS Region B
State E HHS Region B
State A HHS Region A
State B HHS Region A
State C HHS Region A
RegionD
State B
RegionE
State B
RegionF
State C
RegionG
State C Region
H State D
RegionI
State D
RegionJ
State D
RegionK
State E
RegionL
State E Region
M State E
State F HHS Region B
RegionN
State F
RegionO
State F
Patient transfer coordination activity originates with the RMOCC The SMOCC can help transfer patients to a facility in a neighboring sub-state region The FMOCC can transfer patients to a neighboring state or Federal
HHS Region if that is closer 9
MOCCs | General Activity Summary
MOCCs are cells within emergency operations centers (EOCs) at the sub-state regional state and federal levels (FEMAHHS regions) that facilitate patient movement and resource allocation
MOCC PRIORITIES
bull Adding clinical staff to existing EOCs and RRCCsbull Establishing stakeholder agreements that allow for collecting data regarding health system capacity synthesizing the data to
understand the needs of the system and determining areas of the system that may be overwhelmedbull Facilitating movement of patients staff and supplies between healthcare facilities andor states
MOCC ROLE
bull Acting as a single point of contact (POC) for requests from multiple stakeholders such as healthcare facilities RMOCCs and SMOCCsbull Reviewing facilitating and processing patient movement staffing and supply requests and providing medical consultation to
facilitate the decompression of health systems
MOCC DATA ACTIVITIES
bull Collecting analyzing and disseminating information to and from stakeholders to develop comprehensive situational awarenessbull Establishing protocols systems and triggers to inform operational planning stakeholder communications and transfer decision
making
10
~ - ~--~- ----- -
MOCCs | Toolkit
The MOCCs Toolkit contains information on funding a MOCC standard operating procedures for each type of MOCC including integration with ESF-8 roles and responsibilities staffing and transport coordination
FUNDING
bull FEMA Public Assistancebull FEMA Mission Assignmentbull ASPR Hospital Preparedness
Programbull CDC Public Health Emergency
PreparednessCrisis Agreement
STANDARD OPERATING TRANSPORT PROCEDURES COORDINATION
bull RMOCCSMOCC
bull FMOCC
bull Transportation workflows andbull transfer checklists
Each MOCC SOP includes details on bullbullbullbullbull
MOCC Integration with ESF-8Roles and ResponsibilitiesStaffingOperationsPatient MovementMedical Resource Sharing
The MOCCs Toolkit will be located on ASPR TRACIE
11
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Steven Mitchell MD FACEP Medical Director Western Washington Regional COVID Coordination Center Medical Director Emergency Department Harborview Medical Center
12 UnclassifiedFor Public Use
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Western Washington MOCC
bull
bull
bull
First US COVID-19 case Jan 21ndash Snohomish County WA
First US COVID-19 death Feb 29ndash King County WA
First major outbreak late FebMarch1
ndash 167 cases at Long-Term Care Facilitybull 101 residents 50 staff and 16 visitorsbull 43 deaths
1 Epidemiology of Covid-19 in a Long-Term Care Facility in King County Washington N Engl J Med 2020 Mar 27
13
UnclassifiedFor Public Use
THE WALL STREET JOURNAL
One Nursing Home 35 Coronavirus Deaths Inside the Kirkland Disaster
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
King County LTCF Outbreak
~be ~cu Uork ~itnes
Its Pure Panic A Wrenching Wait at Nursing Home Where Coronavirus Took Hold Cut off from their relatives inside a virus-stricken nursing center families are frantically searching for help and basic information
14
UnclassifiedFor Public Use
Characteristics and Outcomes of 21 Critshyically Ill Patients With COVID-19 in Washshyington State Matt Arentz MD1 Eric Yim MD2 Lindy Klaff MD2 et al
Author Affiliations I Article Information
JAMA Published online March 19 2020 doi101001jama20204326
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Single LTCF - Single Hospital
bull Overwhelmed bull No coordination bull Not isolated example
15
UnclassifiedFor Public Use
~) NORTHWEST HEALTHCARE HARBORVIEW MEDICAL CENTER
UW Medicine [f]KingCounty
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Medical Operations Coordinating Cell
bull Disaster Medical Coordination Center
bull Regional COVID Coordination Center (RC3) ndash Harborview Medical CenterKing County ndash Northwest Health Response Network
16
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Regional COVID Coordinating Center ndash Western Washington
17
UnclassifiedFor Public Use
Staffing
Impacts
Resource
Impacts
Ventilators PPE
urveillance of Hospitals
Health
Surveillance of Congregant
Settings
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Two Surveillance Pillars of the RC3
18
UnclassifiedFor Public Use
Health System __-1
Level Loadin
ealth System
Coordination of Resources
ASPR AUIS1ANT bulllCUTtamp~ ~00
UIPAUDgt1111 ~gtIC UfPO~H HUtTHCdl h oUGpound NC1 HpoundhH0Npound~~
I NfORMAT IONGAIEWAf
Two Coordination Pillars of the RC3
19
UnclassifiedFor Public Use
WA HEALTH G) About f) Stevo Mltchell
E-- Home
Q~ _ (WIJ - _uw_ 0
COVIDbulllltl1-t1 ltD _
ltD _
ltD AvilfllHlty - ~c_
44
J -(--
8 j ((MON_
36 j
--0 18 22 0 42 2~
jll 4Jtbull
r 11H -middot- __ ~ -- I 1rA
I --- --J - 353 600 500 1000 806 00 -- -- --
8 J _
101 25
fj)
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH hoUGpoundNC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Emergency Response Platform - Microsoft
bull Constrained Resources ndash Staffing ndash Beds bull Critical Care bull Acute Care
ndash Equipment bull Ventilators bull PPE
ndash COVID-19 patients
20
UnclassifiedFor Public Use
WA HEALTH C) About - Steve
~ Homo
6-hiyenHiiii+MF _ _ a
KING
43 COVID JM1Q
267
55 CD IDlnn1bned
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Emergency Response Platform - Microsoft
bull Next Releasendash Long Term Care Facilitiesbull COVID-19 Impactsndash Positive Patientsndash Positive Health Care
Workers raquo of staff impacted
bull PPE availability
21
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
William Fales MD FACEP FAEMS Medical Director Division of EMS and Trauma Michigan Department of Health and Human Services
22 UnclassifiedFor Public Use
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michiganrsquos Healthcare Preparedness Program bull Michigan Department of Health and Human Services ndash Bureau of EMS Trauma and Preparedness
bull 8 Regional Healthcare Coalitions ndash Hospitals EMS LPH EM LTC Tribal Health ndash Regional Coordinator Assistant Coordinator
Medical Director (25 FTE) ndash Regional Medical Coordination Center bull Multi-Agency Coordination Center bull Statewide use of EMResource by hospitals EMS
23
UnclassifiedFor Public Use
p ror
~ SC ON5
Sault Ste Marie
N
bull
Huron
Madison Milwa uk ee Graed Rapids bull bull e bull ~ 3rnia
L~nsi~ g bull - It bull
bullbullbullbull bull bull bull bull De troi t
bull Glwcago bull bull bull
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Michigan COVID-19 bull bull
bull
First 2 cases ndash March 10 Asymmetric epidemiology ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
24
UnclassifiedFor Public Use
Barrie
Toronto
Hamilton
bull bull
bull
Lake Ontario
bull Ro~besterbull
bull
bull
Brockville bull Kingston
~~w voRK
bull bull bull
bull
bull Pt0NfV VAN1A bull
bull
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H I NfOR MATION GATEWAY
bull
bull bull ~ ba riy
bull bull
Michigan COVID-19 bull First 2 cases ndash March 10
Asymmetric epidemiology bull ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
bull Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
25
UnclassifiedFor Public Use
I I I I I I I I I I I I I
ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City COVID-19 Daily Hospital Admissions
New York City vs Detroit 1800 1600 1400 1200 1000 800 600 400 200 0
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 26
UnclassifiedFor Public Use ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City
1 1 I 11111 111 11 11 1111 1 II II 1 1 1
400
300
200
COVID-19 Daily Hospital Admissions Per 1 Million PopulationNew York City vs Detroit
40-Day Post-Outbreak Mortality bull NY City 646 deaths per million bull Detroit 919 deaths per million
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 27
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Goal bull Save lives and reduce pain and suffering by optimizing
the use of the statersquos healthcare resources ndash Extend conventional standards of care to as many
patients as possible ndash Minimize the need for crisis standards of care bull Especially while conventional capacity exists
28
UnclassifiedFor Public Use
--
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Components bull Relief Hospitals
bull Alternate Care Sites EMS
ndash Home Care Sites
ndash Relief Personnel
29
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals vs Alternate Care Sites bull Relief Hospitals The objective is to extend the
conventional standard of care to as many citizens in need as possible (ie minimize the need to move intocrisis standards of care)
bull Alternate Care Sites (ACS) The objective is to delivercrisis standards of care (as close to the conventional standard of care as possible) in extreme conditions in which the conventional standard of care can not be provided at overloaded hospitals
30
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital ldquoAskrdquo bull Hospitals have been previously asked to be able to
surge an additional 20 above average daily census ndash Increased to 50 ldquosuper surgerdquo
bull Relief Hospitals provide 10 of their expanded capacity to assist severely impacted hospitals ndash While preserving 50 of super-surge capacity bull Many hospitals at very low census
31
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals and Patient Redistribution
bull Intra-Health System Transfer ndash Coordinated by specific health system
bull Intra-Regional Transfer ndash Coordinated by Regional Medical Coordination Center
bull Statewide Transfer ndash Coordinated by Inter-Hospital Coordination Unit bull AKA Medical Operations Coordination Cell (MOCC)
32
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Statewide Inter-Hospital Coordination Unit State EmergencyOperations Center
Planning Finance Operations
Health Branch
Inter-HospitalCoordination Unit
Physician Consultant
EMS Coordination Group
Logistics
MDHHS Health Emergency Operations
Center
Medical Operations
Coordination Cell
33
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs and Patient Redistribution Regional Medical
Coordination Center bull Relief hospitals declare status on
EMResource bull RMCC receives request from
transferring hospital bull RMCC identifies Relief Hospital(s) bull Transferring hospital contacts
Relief Hospital directly bull Relief Hospital accepts patient(s) bull RMCC coordinates EMS PRN
Statewide Inter-Hospital Coordination Unit
Relief hospitals declare status on EMResource
IHCU receives request from RMCC on behalf of transferring hospital
IHCU identifies Relief Hospital(s) Transferring hospital contacts Relief
Hospital directly Relief Hospital accepts patient(s) IHCU coordinates EMS PRN
34
UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Moderator Meghan Treber MS ASPR TRACIE
UnclassifiedFor Public Use 4
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Melissa Harvey RN MSPH Hospital Team Lead Healthcare Resilience Task Force Director Health System Management Office of the Chief Medical Officer US Department of Homeland Security
5 UnclassifiedFor Public Use
6Saving Lives Protecting Americans
Executive Summary
Some hospitals areoverwhelmed with
COVID-19 patients while successful mitigation has
created excess capacity in nearby hospitals creating
an opportunity to transferpatients
MOCCs are a strategy to optimize patientdistribution by
augmenting EOCs withclinical experts that
synthesize and coordinate healthcare capacity
The MOCC strategy can beimplemented nationwide (at sub-state state- and
regional levels) through amodifiable toolkit technical
assistance and federal funding permitting
flexibility for states while optimizing patient
distribution
6
7Saving Lives Protecting Americans
bullbull
--
MOCCs | Problem Statement COVID-19 has resulted in asymmetrical hospital utilization certain regionsrsquo healthcare systems have experienced a surge in patients while others have excess capacity
What are we seeing
Hospitals are the preferred location for seriously ill Facilities with 50+ Beds COVID-19 patients due to existing patient care expertise and resources
Most hot spots are geographically localized overwhelming local healthcare facilities
While some facilities are overwhelmed successfulmitigation in neighboring areas has created excesscapacity in nearby hospitals creating an opportunity to transfer patients
bull bull bull bull
bull middott middot
bull t
bull
D
bull
middot~middotmiddotmiddot
bull le bull l bull bull bull bullt + bull_ I bull bull bull bull bullbull bull bull bull + bull middotmiddot middot middot ~ bullmiddot middotmiddotJ~
-i bullbull bullbullbullbull -ii bull ~ bull ~ bull ~bull bull bull Abull~
bull bullbull i bullbull bullbull middotr bullbullbull bull bullbull bull middotmiddot
i l _
Number of ICU Beds
above 90 control limit of national average below 90 control limit of national average within 90 control limit of national average
Patient transfer coordination through dedicated staffing and data collectionanalysis can improve patient allocation at the sub-state state and federal levels
bull
bullbull
0
7
8Saving Lives Protecting Americans
bull
A MOCC AIMS TO
Move patients to the at the right to improve staff and right time in the patientsupplies provider right way well-being
8
9Saving Lives Protecting Americans
MOCCs | Concept MOCCs can be activated at the Sub-State Regional State and Federal levels to facilitate patient movement and resource allocation during a surge event There are three types of MOCCs included in the concept sub-state Regional Medical Operations Coordination Centers (RMOCCs) State Medical Operations Coordination Centers (SMOCCs) and Federal Medical Operations Coordination Centers (FMOCCs)
RMOCC Sub-State Level
SMOCC State Level
FMOCC Federal Level
HHS Region A HHS Region B
RegionA
State A
RegionB
State A
RegionC
State A
State D HHS Region B
State E HHS Region B
State A HHS Region A
State B HHS Region A
State C HHS Region A
RegionD
State B
RegionE
State B
RegionF
State C
RegionG
State C Region
H State D
RegionI
State D
RegionJ
State D
RegionK
State E
RegionL
State E Region
M State E
State F HHS Region B
RegionN
State F
RegionO
State F
Patient transfer coordination activity originates with the RMOCC The SMOCC can help transfer patients to a facility in a neighboring sub-state region The FMOCC can transfer patients to a neighboring state or Federal
HHS Region if that is closer 9
MOCCs | General Activity Summary
MOCCs are cells within emergency operations centers (EOCs) at the sub-state regional state and federal levels (FEMAHHS regions) that facilitate patient movement and resource allocation
MOCC PRIORITIES
bull Adding clinical staff to existing EOCs and RRCCsbull Establishing stakeholder agreements that allow for collecting data regarding health system capacity synthesizing the data to
understand the needs of the system and determining areas of the system that may be overwhelmedbull Facilitating movement of patients staff and supplies between healthcare facilities andor states
MOCC ROLE
bull Acting as a single point of contact (POC) for requests from multiple stakeholders such as healthcare facilities RMOCCs and SMOCCsbull Reviewing facilitating and processing patient movement staffing and supply requests and providing medical consultation to
facilitate the decompression of health systems
MOCC DATA ACTIVITIES
bull Collecting analyzing and disseminating information to and from stakeholders to develop comprehensive situational awarenessbull Establishing protocols systems and triggers to inform operational planning stakeholder communications and transfer decision
making
10
~ - ~--~- ----- -
MOCCs | Toolkit
The MOCCs Toolkit contains information on funding a MOCC standard operating procedures for each type of MOCC including integration with ESF-8 roles and responsibilities staffing and transport coordination
FUNDING
bull FEMA Public Assistancebull FEMA Mission Assignmentbull ASPR Hospital Preparedness
Programbull CDC Public Health Emergency
PreparednessCrisis Agreement
STANDARD OPERATING TRANSPORT PROCEDURES COORDINATION
bull RMOCCSMOCC
bull FMOCC
bull Transportation workflows andbull transfer checklists
Each MOCC SOP includes details on bullbullbullbullbull
MOCC Integration with ESF-8Roles and ResponsibilitiesStaffingOperationsPatient MovementMedical Resource Sharing
The MOCCs Toolkit will be located on ASPR TRACIE
11
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Steven Mitchell MD FACEP Medical Director Western Washington Regional COVID Coordination Center Medical Director Emergency Department Harborview Medical Center
12 UnclassifiedFor Public Use
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Western Washington MOCC
bull
bull
bull
First US COVID-19 case Jan 21ndash Snohomish County WA
First US COVID-19 death Feb 29ndash King County WA
First major outbreak late FebMarch1
ndash 167 cases at Long-Term Care Facilitybull 101 residents 50 staff and 16 visitorsbull 43 deaths
1 Epidemiology of Covid-19 in a Long-Term Care Facility in King County Washington N Engl J Med 2020 Mar 27
13
UnclassifiedFor Public Use
THE WALL STREET JOURNAL
One Nursing Home 35 Coronavirus Deaths Inside the Kirkland Disaster
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
King County LTCF Outbreak
~be ~cu Uork ~itnes
Its Pure Panic A Wrenching Wait at Nursing Home Where Coronavirus Took Hold Cut off from their relatives inside a virus-stricken nursing center families are frantically searching for help and basic information
14
UnclassifiedFor Public Use
Characteristics and Outcomes of 21 Critshyically Ill Patients With COVID-19 in Washshyington State Matt Arentz MD1 Eric Yim MD2 Lindy Klaff MD2 et al
Author Affiliations I Article Information
JAMA Published online March 19 2020 doi101001jama20204326
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Single LTCF - Single Hospital
bull Overwhelmed bull No coordination bull Not isolated example
15
UnclassifiedFor Public Use
~) NORTHWEST HEALTHCARE HARBORVIEW MEDICAL CENTER
UW Medicine [f]KingCounty
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Medical Operations Coordinating Cell
bull Disaster Medical Coordination Center
bull Regional COVID Coordination Center (RC3) ndash Harborview Medical CenterKing County ndash Northwest Health Response Network
16
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Regional COVID Coordinating Center ndash Western Washington
17
UnclassifiedFor Public Use
Staffing
Impacts
Resource
Impacts
Ventilators PPE
urveillance of Hospitals
Health
Surveillance of Congregant
Settings
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Two Surveillance Pillars of the RC3
18
UnclassifiedFor Public Use
Health System __-1
Level Loadin
ealth System
Coordination of Resources
ASPR AUIS1ANT bulllCUTtamp~ ~00
UIPAUDgt1111 ~gtIC UfPO~H HUtTHCdl h oUGpound NC1 HpoundhH0Npound~~
I NfORMAT IONGAIEWAf
Two Coordination Pillars of the RC3
19
UnclassifiedFor Public Use
WA HEALTH G) About f) Stevo Mltchell
E-- Home
Q~ _ (WIJ - _uw_ 0
COVIDbulllltl1-t1 ltD _
ltD _
ltD AvilfllHlty - ~c_
44
J -(--
8 j ((MON_
36 j
--0 18 22 0 42 2~
jll 4Jtbull
r 11H -middot- __ ~ -- I 1rA
I --- --J - 353 600 500 1000 806 00 -- -- --
8 J _
101 25
fj)
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH hoUGpoundNC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Emergency Response Platform - Microsoft
bull Constrained Resources ndash Staffing ndash Beds bull Critical Care bull Acute Care
ndash Equipment bull Ventilators bull PPE
ndash COVID-19 patients
20
UnclassifiedFor Public Use
WA HEALTH C) About - Steve
~ Homo
6-hiyenHiiii+MF _ _ a
KING
43 COVID JM1Q
267
55 CD IDlnn1bned
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Emergency Response Platform - Microsoft
bull Next Releasendash Long Term Care Facilitiesbull COVID-19 Impactsndash Positive Patientsndash Positive Health Care
Workers raquo of staff impacted
bull PPE availability
21
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
William Fales MD FACEP FAEMS Medical Director Division of EMS and Trauma Michigan Department of Health and Human Services
22 UnclassifiedFor Public Use
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michiganrsquos Healthcare Preparedness Program bull Michigan Department of Health and Human Services ndash Bureau of EMS Trauma and Preparedness
bull 8 Regional Healthcare Coalitions ndash Hospitals EMS LPH EM LTC Tribal Health ndash Regional Coordinator Assistant Coordinator
Medical Director (25 FTE) ndash Regional Medical Coordination Center bull Multi-Agency Coordination Center bull Statewide use of EMResource by hospitals EMS
23
UnclassifiedFor Public Use
p ror
~ SC ON5
Sault Ste Marie
N
bull
Huron
Madison Milwa uk ee Graed Rapids bull bull e bull ~ 3rnia
L~nsi~ g bull - It bull
bullbullbullbull bull bull bull bull De troi t
bull Glwcago bull bull bull
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Michigan COVID-19 bull bull
bull
First 2 cases ndash March 10 Asymmetric epidemiology ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
24
UnclassifiedFor Public Use
Barrie
Toronto
Hamilton
bull bull
bull
Lake Ontario
bull Ro~besterbull
bull
bull
Brockville bull Kingston
~~w voRK
bull bull bull
bull
bull Pt0NfV VAN1A bull
bull
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H I NfOR MATION GATEWAY
bull
bull bull ~ ba riy
bull bull
Michigan COVID-19 bull First 2 cases ndash March 10
Asymmetric epidemiology bull ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
bull Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
25
UnclassifiedFor Public Use
I I I I I I I I I I I I I
ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City COVID-19 Daily Hospital Admissions
New York City vs Detroit 1800 1600 1400 1200 1000 800 600 400 200 0
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 26
UnclassifiedFor Public Use ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City
1 1 I 11111 111 11 11 1111 1 II II 1 1 1
400
300
200
COVID-19 Daily Hospital Admissions Per 1 Million PopulationNew York City vs Detroit
40-Day Post-Outbreak Mortality bull NY City 646 deaths per million bull Detroit 919 deaths per million
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 27
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Goal bull Save lives and reduce pain and suffering by optimizing
the use of the statersquos healthcare resources ndash Extend conventional standards of care to as many
patients as possible ndash Minimize the need for crisis standards of care bull Especially while conventional capacity exists
28
UnclassifiedFor Public Use
--
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Components bull Relief Hospitals
bull Alternate Care Sites EMS
ndash Home Care Sites
ndash Relief Personnel
29
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals vs Alternate Care Sites bull Relief Hospitals The objective is to extend the
conventional standard of care to as many citizens in need as possible (ie minimize the need to move intocrisis standards of care)
bull Alternate Care Sites (ACS) The objective is to delivercrisis standards of care (as close to the conventional standard of care as possible) in extreme conditions in which the conventional standard of care can not be provided at overloaded hospitals
30
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital ldquoAskrdquo bull Hospitals have been previously asked to be able to
surge an additional 20 above average daily census ndash Increased to 50 ldquosuper surgerdquo
bull Relief Hospitals provide 10 of their expanded capacity to assist severely impacted hospitals ndash While preserving 50 of super-surge capacity bull Many hospitals at very low census
31
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals and Patient Redistribution
bull Intra-Health System Transfer ndash Coordinated by specific health system
bull Intra-Regional Transfer ndash Coordinated by Regional Medical Coordination Center
bull Statewide Transfer ndash Coordinated by Inter-Hospital Coordination Unit bull AKA Medical Operations Coordination Cell (MOCC)
32
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Statewide Inter-Hospital Coordination Unit State EmergencyOperations Center
Planning Finance Operations
Health Branch
Inter-HospitalCoordination Unit
Physician Consultant
EMS Coordination Group
Logistics
MDHHS Health Emergency Operations
Center
Medical Operations
Coordination Cell
33
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs and Patient Redistribution Regional Medical
Coordination Center bull Relief hospitals declare status on
EMResource bull RMCC receives request from
transferring hospital bull RMCC identifies Relief Hospital(s) bull Transferring hospital contacts
Relief Hospital directly bull Relief Hospital accepts patient(s) bull RMCC coordinates EMS PRN
Statewide Inter-Hospital Coordination Unit
Relief hospitals declare status on EMResource
IHCU receives request from RMCC on behalf of transferring hospital
IHCU identifies Relief Hospital(s) Transferring hospital contacts Relief
Hospital directly Relief Hospital accepts patient(s) IHCU coordinates EMS PRN
34
UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Melissa Harvey RN MSPH Hospital Team Lead Healthcare Resilience Task Force Director Health System Management Office of the Chief Medical Officer US Department of Homeland Security
5 UnclassifiedFor Public Use
6Saving Lives Protecting Americans
Executive Summary
Some hospitals areoverwhelmed with
COVID-19 patients while successful mitigation has
created excess capacity in nearby hospitals creating
an opportunity to transferpatients
MOCCs are a strategy to optimize patientdistribution by
augmenting EOCs withclinical experts that
synthesize and coordinate healthcare capacity
The MOCC strategy can beimplemented nationwide (at sub-state state- and
regional levels) through amodifiable toolkit technical
assistance and federal funding permitting
flexibility for states while optimizing patient
distribution
6
7Saving Lives Protecting Americans
bullbull
--
MOCCs | Problem Statement COVID-19 has resulted in asymmetrical hospital utilization certain regionsrsquo healthcare systems have experienced a surge in patients while others have excess capacity
What are we seeing
Hospitals are the preferred location for seriously ill Facilities with 50+ Beds COVID-19 patients due to existing patient care expertise and resources
Most hot spots are geographically localized overwhelming local healthcare facilities
While some facilities are overwhelmed successfulmitigation in neighboring areas has created excesscapacity in nearby hospitals creating an opportunity to transfer patients
bull bull bull bull
bull middott middot
bull t
bull
D
bull
middot~middotmiddotmiddot
bull le bull l bull bull bull bullt + bull_ I bull bull bull bull bullbull bull bull bull + bull middotmiddot middot middot ~ bullmiddot middotmiddotJ~
-i bullbull bullbullbullbull -ii bull ~ bull ~ bull ~bull bull bull Abull~
bull bullbull i bullbull bullbull middotr bullbullbull bull bullbull bull middotmiddot
i l _
Number of ICU Beds
above 90 control limit of national average below 90 control limit of national average within 90 control limit of national average
Patient transfer coordination through dedicated staffing and data collectionanalysis can improve patient allocation at the sub-state state and federal levels
bull
bullbull
0
7
8Saving Lives Protecting Americans
bull
A MOCC AIMS TO
Move patients to the at the right to improve staff and right time in the patientsupplies provider right way well-being
8
9Saving Lives Protecting Americans
MOCCs | Concept MOCCs can be activated at the Sub-State Regional State and Federal levels to facilitate patient movement and resource allocation during a surge event There are three types of MOCCs included in the concept sub-state Regional Medical Operations Coordination Centers (RMOCCs) State Medical Operations Coordination Centers (SMOCCs) and Federal Medical Operations Coordination Centers (FMOCCs)
RMOCC Sub-State Level
SMOCC State Level
FMOCC Federal Level
HHS Region A HHS Region B
RegionA
State A
RegionB
State A
RegionC
State A
State D HHS Region B
State E HHS Region B
State A HHS Region A
State B HHS Region A
State C HHS Region A
RegionD
State B
RegionE
State B
RegionF
State C
RegionG
State C Region
H State D
RegionI
State D
RegionJ
State D
RegionK
State E
RegionL
State E Region
M State E
State F HHS Region B
RegionN
State F
RegionO
State F
Patient transfer coordination activity originates with the RMOCC The SMOCC can help transfer patients to a facility in a neighboring sub-state region The FMOCC can transfer patients to a neighboring state or Federal
HHS Region if that is closer 9
MOCCs | General Activity Summary
MOCCs are cells within emergency operations centers (EOCs) at the sub-state regional state and federal levels (FEMAHHS regions) that facilitate patient movement and resource allocation
MOCC PRIORITIES
bull Adding clinical staff to existing EOCs and RRCCsbull Establishing stakeholder agreements that allow for collecting data regarding health system capacity synthesizing the data to
understand the needs of the system and determining areas of the system that may be overwhelmedbull Facilitating movement of patients staff and supplies between healthcare facilities andor states
MOCC ROLE
bull Acting as a single point of contact (POC) for requests from multiple stakeholders such as healthcare facilities RMOCCs and SMOCCsbull Reviewing facilitating and processing patient movement staffing and supply requests and providing medical consultation to
facilitate the decompression of health systems
MOCC DATA ACTIVITIES
bull Collecting analyzing and disseminating information to and from stakeholders to develop comprehensive situational awarenessbull Establishing protocols systems and triggers to inform operational planning stakeholder communications and transfer decision
making
10
~ - ~--~- ----- -
MOCCs | Toolkit
The MOCCs Toolkit contains information on funding a MOCC standard operating procedures for each type of MOCC including integration with ESF-8 roles and responsibilities staffing and transport coordination
FUNDING
bull FEMA Public Assistancebull FEMA Mission Assignmentbull ASPR Hospital Preparedness
Programbull CDC Public Health Emergency
PreparednessCrisis Agreement
STANDARD OPERATING TRANSPORT PROCEDURES COORDINATION
bull RMOCCSMOCC
bull FMOCC
bull Transportation workflows andbull transfer checklists
Each MOCC SOP includes details on bullbullbullbullbull
MOCC Integration with ESF-8Roles and ResponsibilitiesStaffingOperationsPatient MovementMedical Resource Sharing
The MOCCs Toolkit will be located on ASPR TRACIE
11
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Steven Mitchell MD FACEP Medical Director Western Washington Regional COVID Coordination Center Medical Director Emergency Department Harborview Medical Center
12 UnclassifiedFor Public Use
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Western Washington MOCC
bull
bull
bull
First US COVID-19 case Jan 21ndash Snohomish County WA
First US COVID-19 death Feb 29ndash King County WA
First major outbreak late FebMarch1
ndash 167 cases at Long-Term Care Facilitybull 101 residents 50 staff and 16 visitorsbull 43 deaths
1 Epidemiology of Covid-19 in a Long-Term Care Facility in King County Washington N Engl J Med 2020 Mar 27
13
UnclassifiedFor Public Use
THE WALL STREET JOURNAL
One Nursing Home 35 Coronavirus Deaths Inside the Kirkland Disaster
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
King County LTCF Outbreak
~be ~cu Uork ~itnes
Its Pure Panic A Wrenching Wait at Nursing Home Where Coronavirus Took Hold Cut off from their relatives inside a virus-stricken nursing center families are frantically searching for help and basic information
14
UnclassifiedFor Public Use
Characteristics and Outcomes of 21 Critshyically Ill Patients With COVID-19 in Washshyington State Matt Arentz MD1 Eric Yim MD2 Lindy Klaff MD2 et al
Author Affiliations I Article Information
JAMA Published online March 19 2020 doi101001jama20204326
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Single LTCF - Single Hospital
bull Overwhelmed bull No coordination bull Not isolated example
15
UnclassifiedFor Public Use
~) NORTHWEST HEALTHCARE HARBORVIEW MEDICAL CENTER
UW Medicine [f]KingCounty
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Medical Operations Coordinating Cell
bull Disaster Medical Coordination Center
bull Regional COVID Coordination Center (RC3) ndash Harborview Medical CenterKing County ndash Northwest Health Response Network
16
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Regional COVID Coordinating Center ndash Western Washington
17
UnclassifiedFor Public Use
Staffing
Impacts
Resource
Impacts
Ventilators PPE
urveillance of Hospitals
Health
Surveillance of Congregant
Settings
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Two Surveillance Pillars of the RC3
18
UnclassifiedFor Public Use
Health System __-1
Level Loadin
ealth System
Coordination of Resources
ASPR AUIS1ANT bulllCUTtamp~ ~00
UIPAUDgt1111 ~gtIC UfPO~H HUtTHCdl h oUGpound NC1 HpoundhH0Npound~~
I NfORMAT IONGAIEWAf
Two Coordination Pillars of the RC3
19
UnclassifiedFor Public Use
WA HEALTH G) About f) Stevo Mltchell
E-- Home
Q~ _ (WIJ - _uw_ 0
COVIDbulllltl1-t1 ltD _
ltD _
ltD AvilfllHlty - ~c_
44
J -(--
8 j ((MON_
36 j
--0 18 22 0 42 2~
jll 4Jtbull
r 11H -middot- __ ~ -- I 1rA
I --- --J - 353 600 500 1000 806 00 -- -- --
8 J _
101 25
fj)
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH hoUGpoundNC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Emergency Response Platform - Microsoft
bull Constrained Resources ndash Staffing ndash Beds bull Critical Care bull Acute Care
ndash Equipment bull Ventilators bull PPE
ndash COVID-19 patients
20
UnclassifiedFor Public Use
WA HEALTH C) About - Steve
~ Homo
6-hiyenHiiii+MF _ _ a
KING
43 COVID JM1Q
267
55 CD IDlnn1bned
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Emergency Response Platform - Microsoft
bull Next Releasendash Long Term Care Facilitiesbull COVID-19 Impactsndash Positive Patientsndash Positive Health Care
Workers raquo of staff impacted
bull PPE availability
21
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
William Fales MD FACEP FAEMS Medical Director Division of EMS and Trauma Michigan Department of Health and Human Services
22 UnclassifiedFor Public Use
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michiganrsquos Healthcare Preparedness Program bull Michigan Department of Health and Human Services ndash Bureau of EMS Trauma and Preparedness
bull 8 Regional Healthcare Coalitions ndash Hospitals EMS LPH EM LTC Tribal Health ndash Regional Coordinator Assistant Coordinator
Medical Director (25 FTE) ndash Regional Medical Coordination Center bull Multi-Agency Coordination Center bull Statewide use of EMResource by hospitals EMS
23
UnclassifiedFor Public Use
p ror
~ SC ON5
Sault Ste Marie
N
bull
Huron
Madison Milwa uk ee Graed Rapids bull bull e bull ~ 3rnia
L~nsi~ g bull - It bull
bullbullbullbull bull bull bull bull De troi t
bull Glwcago bull bull bull
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Michigan COVID-19 bull bull
bull
First 2 cases ndash March 10 Asymmetric epidemiology ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
24
UnclassifiedFor Public Use
Barrie
Toronto
Hamilton
bull bull
bull
Lake Ontario
bull Ro~besterbull
bull
bull
Brockville bull Kingston
~~w voRK
bull bull bull
bull
bull Pt0NfV VAN1A bull
bull
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H I NfOR MATION GATEWAY
bull
bull bull ~ ba riy
bull bull
Michigan COVID-19 bull First 2 cases ndash March 10
Asymmetric epidemiology bull ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
bull Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
25
UnclassifiedFor Public Use
I I I I I I I I I I I I I
ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City COVID-19 Daily Hospital Admissions
New York City vs Detroit 1800 1600 1400 1200 1000 800 600 400 200 0
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 26
UnclassifiedFor Public Use ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City
1 1 I 11111 111 11 11 1111 1 II II 1 1 1
400
300
200
COVID-19 Daily Hospital Admissions Per 1 Million PopulationNew York City vs Detroit
40-Day Post-Outbreak Mortality bull NY City 646 deaths per million bull Detroit 919 deaths per million
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 27
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Goal bull Save lives and reduce pain and suffering by optimizing
the use of the statersquos healthcare resources ndash Extend conventional standards of care to as many
patients as possible ndash Minimize the need for crisis standards of care bull Especially while conventional capacity exists
28
UnclassifiedFor Public Use
--
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Components bull Relief Hospitals
bull Alternate Care Sites EMS
ndash Home Care Sites
ndash Relief Personnel
29
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals vs Alternate Care Sites bull Relief Hospitals The objective is to extend the
conventional standard of care to as many citizens in need as possible (ie minimize the need to move intocrisis standards of care)
bull Alternate Care Sites (ACS) The objective is to delivercrisis standards of care (as close to the conventional standard of care as possible) in extreme conditions in which the conventional standard of care can not be provided at overloaded hospitals
30
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital ldquoAskrdquo bull Hospitals have been previously asked to be able to
surge an additional 20 above average daily census ndash Increased to 50 ldquosuper surgerdquo
bull Relief Hospitals provide 10 of their expanded capacity to assist severely impacted hospitals ndash While preserving 50 of super-surge capacity bull Many hospitals at very low census
31
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals and Patient Redistribution
bull Intra-Health System Transfer ndash Coordinated by specific health system
bull Intra-Regional Transfer ndash Coordinated by Regional Medical Coordination Center
bull Statewide Transfer ndash Coordinated by Inter-Hospital Coordination Unit bull AKA Medical Operations Coordination Cell (MOCC)
32
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Statewide Inter-Hospital Coordination Unit State EmergencyOperations Center
Planning Finance Operations
Health Branch
Inter-HospitalCoordination Unit
Physician Consultant
EMS Coordination Group
Logistics
MDHHS Health Emergency Operations
Center
Medical Operations
Coordination Cell
33
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs and Patient Redistribution Regional Medical
Coordination Center bull Relief hospitals declare status on
EMResource bull RMCC receives request from
transferring hospital bull RMCC identifies Relief Hospital(s) bull Transferring hospital contacts
Relief Hospital directly bull Relief Hospital accepts patient(s) bull RMCC coordinates EMS PRN
Statewide Inter-Hospital Coordination Unit
Relief hospitals declare status on EMResource
IHCU receives request from RMCC on behalf of transferring hospital
IHCU identifies Relief Hospital(s) Transferring hospital contacts Relief
Hospital directly Relief Hospital accepts patient(s) IHCU coordinates EMS PRN
34
UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-
6Saving Lives Protecting Americans
Executive Summary
Some hospitals areoverwhelmed with
COVID-19 patients while successful mitigation has
created excess capacity in nearby hospitals creating
an opportunity to transferpatients
MOCCs are a strategy to optimize patientdistribution by
augmenting EOCs withclinical experts that
synthesize and coordinate healthcare capacity
The MOCC strategy can beimplemented nationwide (at sub-state state- and
regional levels) through amodifiable toolkit technical
assistance and federal funding permitting
flexibility for states while optimizing patient
distribution
6
7Saving Lives Protecting Americans
bullbull
--
MOCCs | Problem Statement COVID-19 has resulted in asymmetrical hospital utilization certain regionsrsquo healthcare systems have experienced a surge in patients while others have excess capacity
What are we seeing
Hospitals are the preferred location for seriously ill Facilities with 50+ Beds COVID-19 patients due to existing patient care expertise and resources
Most hot spots are geographically localized overwhelming local healthcare facilities
While some facilities are overwhelmed successfulmitigation in neighboring areas has created excesscapacity in nearby hospitals creating an opportunity to transfer patients
bull bull bull bull
bull middott middot
bull t
bull
D
bull
middot~middotmiddotmiddot
bull le bull l bull bull bull bullt + bull_ I bull bull bull bull bullbull bull bull bull + bull middotmiddot middot middot ~ bullmiddot middotmiddotJ~
-i bullbull bullbullbullbull -ii bull ~ bull ~ bull ~bull bull bull Abull~
bull bullbull i bullbull bullbull middotr bullbullbull bull bullbull bull middotmiddot
i l _
Number of ICU Beds
above 90 control limit of national average below 90 control limit of national average within 90 control limit of national average
Patient transfer coordination through dedicated staffing and data collectionanalysis can improve patient allocation at the sub-state state and federal levels
bull
bullbull
0
7
8Saving Lives Protecting Americans
bull
A MOCC AIMS TO
Move patients to the at the right to improve staff and right time in the patientsupplies provider right way well-being
8
9Saving Lives Protecting Americans
MOCCs | Concept MOCCs can be activated at the Sub-State Regional State and Federal levels to facilitate patient movement and resource allocation during a surge event There are three types of MOCCs included in the concept sub-state Regional Medical Operations Coordination Centers (RMOCCs) State Medical Operations Coordination Centers (SMOCCs) and Federal Medical Operations Coordination Centers (FMOCCs)
RMOCC Sub-State Level
SMOCC State Level
FMOCC Federal Level
HHS Region A HHS Region B
RegionA
State A
RegionB
State A
RegionC
State A
State D HHS Region B
State E HHS Region B
State A HHS Region A
State B HHS Region A
State C HHS Region A
RegionD
State B
RegionE
State B
RegionF
State C
RegionG
State C Region
H State D
RegionI
State D
RegionJ
State D
RegionK
State E
RegionL
State E Region
M State E
State F HHS Region B
RegionN
State F
RegionO
State F
Patient transfer coordination activity originates with the RMOCC The SMOCC can help transfer patients to a facility in a neighboring sub-state region The FMOCC can transfer patients to a neighboring state or Federal
HHS Region if that is closer 9
MOCCs | General Activity Summary
MOCCs are cells within emergency operations centers (EOCs) at the sub-state regional state and federal levels (FEMAHHS regions) that facilitate patient movement and resource allocation
MOCC PRIORITIES
bull Adding clinical staff to existing EOCs and RRCCsbull Establishing stakeholder agreements that allow for collecting data regarding health system capacity synthesizing the data to
understand the needs of the system and determining areas of the system that may be overwhelmedbull Facilitating movement of patients staff and supplies between healthcare facilities andor states
MOCC ROLE
bull Acting as a single point of contact (POC) for requests from multiple stakeholders such as healthcare facilities RMOCCs and SMOCCsbull Reviewing facilitating and processing patient movement staffing and supply requests and providing medical consultation to
facilitate the decompression of health systems
MOCC DATA ACTIVITIES
bull Collecting analyzing and disseminating information to and from stakeholders to develop comprehensive situational awarenessbull Establishing protocols systems and triggers to inform operational planning stakeholder communications and transfer decision
making
10
~ - ~--~- ----- -
MOCCs | Toolkit
The MOCCs Toolkit contains information on funding a MOCC standard operating procedures for each type of MOCC including integration with ESF-8 roles and responsibilities staffing and transport coordination
FUNDING
bull FEMA Public Assistancebull FEMA Mission Assignmentbull ASPR Hospital Preparedness
Programbull CDC Public Health Emergency
PreparednessCrisis Agreement
STANDARD OPERATING TRANSPORT PROCEDURES COORDINATION
bull RMOCCSMOCC
bull FMOCC
bull Transportation workflows andbull transfer checklists
Each MOCC SOP includes details on bullbullbullbullbull
MOCC Integration with ESF-8Roles and ResponsibilitiesStaffingOperationsPatient MovementMedical Resource Sharing
The MOCCs Toolkit will be located on ASPR TRACIE
11
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Steven Mitchell MD FACEP Medical Director Western Washington Regional COVID Coordination Center Medical Director Emergency Department Harborview Medical Center
12 UnclassifiedFor Public Use
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Western Washington MOCC
bull
bull
bull
First US COVID-19 case Jan 21ndash Snohomish County WA
First US COVID-19 death Feb 29ndash King County WA
First major outbreak late FebMarch1
ndash 167 cases at Long-Term Care Facilitybull 101 residents 50 staff and 16 visitorsbull 43 deaths
1 Epidemiology of Covid-19 in a Long-Term Care Facility in King County Washington N Engl J Med 2020 Mar 27
13
UnclassifiedFor Public Use
THE WALL STREET JOURNAL
One Nursing Home 35 Coronavirus Deaths Inside the Kirkland Disaster
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
King County LTCF Outbreak
~be ~cu Uork ~itnes
Its Pure Panic A Wrenching Wait at Nursing Home Where Coronavirus Took Hold Cut off from their relatives inside a virus-stricken nursing center families are frantically searching for help and basic information
14
UnclassifiedFor Public Use
Characteristics and Outcomes of 21 Critshyically Ill Patients With COVID-19 in Washshyington State Matt Arentz MD1 Eric Yim MD2 Lindy Klaff MD2 et al
Author Affiliations I Article Information
JAMA Published online March 19 2020 doi101001jama20204326
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Single LTCF - Single Hospital
bull Overwhelmed bull No coordination bull Not isolated example
15
UnclassifiedFor Public Use
~) NORTHWEST HEALTHCARE HARBORVIEW MEDICAL CENTER
UW Medicine [f]KingCounty
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Medical Operations Coordinating Cell
bull Disaster Medical Coordination Center
bull Regional COVID Coordination Center (RC3) ndash Harborview Medical CenterKing County ndash Northwest Health Response Network
16
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Regional COVID Coordinating Center ndash Western Washington
17
UnclassifiedFor Public Use
Staffing
Impacts
Resource
Impacts
Ventilators PPE
urveillance of Hospitals
Health
Surveillance of Congregant
Settings
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Two Surveillance Pillars of the RC3
18
UnclassifiedFor Public Use
Health System __-1
Level Loadin
ealth System
Coordination of Resources
ASPR AUIS1ANT bulllCUTtamp~ ~00
UIPAUDgt1111 ~gtIC UfPO~H HUtTHCdl h oUGpound NC1 HpoundhH0Npound~~
I NfORMAT IONGAIEWAf
Two Coordination Pillars of the RC3
19
UnclassifiedFor Public Use
WA HEALTH G) About f) Stevo Mltchell
E-- Home
Q~ _ (WIJ - _uw_ 0
COVIDbulllltl1-t1 ltD _
ltD _
ltD AvilfllHlty - ~c_
44
J -(--
8 j ((MON_
36 j
--0 18 22 0 42 2~
jll 4Jtbull
r 11H -middot- __ ~ -- I 1rA
I --- --J - 353 600 500 1000 806 00 -- -- --
8 J _
101 25
fj)
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH hoUGpoundNC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Emergency Response Platform - Microsoft
bull Constrained Resources ndash Staffing ndash Beds bull Critical Care bull Acute Care
ndash Equipment bull Ventilators bull PPE
ndash COVID-19 patients
20
UnclassifiedFor Public Use
WA HEALTH C) About - Steve
~ Homo
6-hiyenHiiii+MF _ _ a
KING
43 COVID JM1Q
267
55 CD IDlnn1bned
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Emergency Response Platform - Microsoft
bull Next Releasendash Long Term Care Facilitiesbull COVID-19 Impactsndash Positive Patientsndash Positive Health Care
Workers raquo of staff impacted
bull PPE availability
21
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
William Fales MD FACEP FAEMS Medical Director Division of EMS and Trauma Michigan Department of Health and Human Services
22 UnclassifiedFor Public Use
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michiganrsquos Healthcare Preparedness Program bull Michigan Department of Health and Human Services ndash Bureau of EMS Trauma and Preparedness
bull 8 Regional Healthcare Coalitions ndash Hospitals EMS LPH EM LTC Tribal Health ndash Regional Coordinator Assistant Coordinator
Medical Director (25 FTE) ndash Regional Medical Coordination Center bull Multi-Agency Coordination Center bull Statewide use of EMResource by hospitals EMS
23
UnclassifiedFor Public Use
p ror
~ SC ON5
Sault Ste Marie
N
bull
Huron
Madison Milwa uk ee Graed Rapids bull bull e bull ~ 3rnia
L~nsi~ g bull - It bull
bullbullbullbull bull bull bull bull De troi t
bull Glwcago bull bull bull
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Michigan COVID-19 bull bull
bull
First 2 cases ndash March 10 Asymmetric epidemiology ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
24
UnclassifiedFor Public Use
Barrie
Toronto
Hamilton
bull bull
bull
Lake Ontario
bull Ro~besterbull
bull
bull
Brockville bull Kingston
~~w voRK
bull bull bull
bull
bull Pt0NfV VAN1A bull
bull
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H I NfOR MATION GATEWAY
bull
bull bull ~ ba riy
bull bull
Michigan COVID-19 bull First 2 cases ndash March 10
Asymmetric epidemiology bull ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
bull Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
25
UnclassifiedFor Public Use
I I I I I I I I I I I I I
ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City COVID-19 Daily Hospital Admissions
New York City vs Detroit 1800 1600 1400 1200 1000 800 600 400 200 0
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 26
UnclassifiedFor Public Use ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City
1 1 I 11111 111 11 11 1111 1 II II 1 1 1
400
300
200
COVID-19 Daily Hospital Admissions Per 1 Million PopulationNew York City vs Detroit
40-Day Post-Outbreak Mortality bull NY City 646 deaths per million bull Detroit 919 deaths per million
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 27
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Goal bull Save lives and reduce pain and suffering by optimizing
the use of the statersquos healthcare resources ndash Extend conventional standards of care to as many
patients as possible ndash Minimize the need for crisis standards of care bull Especially while conventional capacity exists
28
UnclassifiedFor Public Use
--
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Components bull Relief Hospitals
bull Alternate Care Sites EMS
ndash Home Care Sites
ndash Relief Personnel
29
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals vs Alternate Care Sites bull Relief Hospitals The objective is to extend the
conventional standard of care to as many citizens in need as possible (ie minimize the need to move intocrisis standards of care)
bull Alternate Care Sites (ACS) The objective is to delivercrisis standards of care (as close to the conventional standard of care as possible) in extreme conditions in which the conventional standard of care can not be provided at overloaded hospitals
30
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital ldquoAskrdquo bull Hospitals have been previously asked to be able to
surge an additional 20 above average daily census ndash Increased to 50 ldquosuper surgerdquo
bull Relief Hospitals provide 10 of their expanded capacity to assist severely impacted hospitals ndash While preserving 50 of super-surge capacity bull Many hospitals at very low census
31
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals and Patient Redistribution
bull Intra-Health System Transfer ndash Coordinated by specific health system
bull Intra-Regional Transfer ndash Coordinated by Regional Medical Coordination Center
bull Statewide Transfer ndash Coordinated by Inter-Hospital Coordination Unit bull AKA Medical Operations Coordination Cell (MOCC)
32
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Statewide Inter-Hospital Coordination Unit State EmergencyOperations Center
Planning Finance Operations
Health Branch
Inter-HospitalCoordination Unit
Physician Consultant
EMS Coordination Group
Logistics
MDHHS Health Emergency Operations
Center
Medical Operations
Coordination Cell
33
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs and Patient Redistribution Regional Medical
Coordination Center bull Relief hospitals declare status on
EMResource bull RMCC receives request from
transferring hospital bull RMCC identifies Relief Hospital(s) bull Transferring hospital contacts
Relief Hospital directly bull Relief Hospital accepts patient(s) bull RMCC coordinates EMS PRN
Statewide Inter-Hospital Coordination Unit
Relief hospitals declare status on EMResource
IHCU receives request from RMCC on behalf of transferring hospital
IHCU identifies Relief Hospital(s) Transferring hospital contacts Relief
Hospital directly Relief Hospital accepts patient(s) IHCU coordinates EMS PRN
34
UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

7Saving Lives Protecting Americans
bullbull
--
MOCCs | Problem Statement COVID-19 has resulted in asymmetrical hospital utilization certain regionsrsquo healthcare systems have experienced a surge in patients while others have excess capacity
What are we seeing
Hospitals are the preferred location for seriously ill Facilities with 50+ Beds COVID-19 patients due to existing patient care expertise and resources
Most hot spots are geographically localized overwhelming local healthcare facilities
While some facilities are overwhelmed successfulmitigation in neighboring areas has created excesscapacity in nearby hospitals creating an opportunity to transfer patients
bull bull bull bull
bull middott middot
bull t
bull
D
bull
middot~middotmiddotmiddot
bull le bull l bull bull bull bullt + bull_ I bull bull bull bull bullbull bull bull bull + bull middotmiddot middot middot ~ bullmiddot middotmiddotJ~
-i bullbull bullbullbullbull -ii bull ~ bull ~ bull ~bull bull bull Abull~
bull bullbull i bullbull bullbull middotr bullbullbull bull bullbull bull middotmiddot
i l _
Number of ICU Beds
above 90 control limit of national average below 90 control limit of national average within 90 control limit of national average
Patient transfer coordination through dedicated staffing and data collectionanalysis can improve patient allocation at the sub-state state and federal levels
bull
bullbull
0
7
8Saving Lives Protecting Americans
bull
A MOCC AIMS TO
Move patients to the at the right to improve staff and right time in the patientsupplies provider right way well-being
8
9Saving Lives Protecting Americans
MOCCs | Concept MOCCs can be activated at the Sub-State Regional State and Federal levels to facilitate patient movement and resource allocation during a surge event There are three types of MOCCs included in the concept sub-state Regional Medical Operations Coordination Centers (RMOCCs) State Medical Operations Coordination Centers (SMOCCs) and Federal Medical Operations Coordination Centers (FMOCCs)
RMOCC Sub-State Level
SMOCC State Level
FMOCC Federal Level
HHS Region A HHS Region B
RegionA
State A
RegionB
State A
RegionC
State A
State D HHS Region B
State E HHS Region B
State A HHS Region A
State B HHS Region A
State C HHS Region A
RegionD
State B
RegionE
State B
RegionF
State C
RegionG
State C Region
H State D
RegionI
State D
RegionJ
State D
RegionK
State E
RegionL
State E Region
M State E
State F HHS Region B
RegionN
State F
RegionO
State F
Patient transfer coordination activity originates with the RMOCC The SMOCC can help transfer patients to a facility in a neighboring sub-state region The FMOCC can transfer patients to a neighboring state or Federal
HHS Region if that is closer 9
MOCCs | General Activity Summary
MOCCs are cells within emergency operations centers (EOCs) at the sub-state regional state and federal levels (FEMAHHS regions) that facilitate patient movement and resource allocation
MOCC PRIORITIES
bull Adding clinical staff to existing EOCs and RRCCsbull Establishing stakeholder agreements that allow for collecting data regarding health system capacity synthesizing the data to
understand the needs of the system and determining areas of the system that may be overwhelmedbull Facilitating movement of patients staff and supplies between healthcare facilities andor states
MOCC ROLE
bull Acting as a single point of contact (POC) for requests from multiple stakeholders such as healthcare facilities RMOCCs and SMOCCsbull Reviewing facilitating and processing patient movement staffing and supply requests and providing medical consultation to
facilitate the decompression of health systems
MOCC DATA ACTIVITIES
bull Collecting analyzing and disseminating information to and from stakeholders to develop comprehensive situational awarenessbull Establishing protocols systems and triggers to inform operational planning stakeholder communications and transfer decision
making
10
~ - ~--~- ----- -
MOCCs | Toolkit
The MOCCs Toolkit contains information on funding a MOCC standard operating procedures for each type of MOCC including integration with ESF-8 roles and responsibilities staffing and transport coordination
FUNDING
bull FEMA Public Assistancebull FEMA Mission Assignmentbull ASPR Hospital Preparedness
Programbull CDC Public Health Emergency
PreparednessCrisis Agreement
STANDARD OPERATING TRANSPORT PROCEDURES COORDINATION
bull RMOCCSMOCC
bull FMOCC
bull Transportation workflows andbull transfer checklists
Each MOCC SOP includes details on bullbullbullbullbull
MOCC Integration with ESF-8Roles and ResponsibilitiesStaffingOperationsPatient MovementMedical Resource Sharing
The MOCCs Toolkit will be located on ASPR TRACIE
11
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Steven Mitchell MD FACEP Medical Director Western Washington Regional COVID Coordination Center Medical Director Emergency Department Harborview Medical Center
12 UnclassifiedFor Public Use
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Western Washington MOCC
bull
bull
bull
First US COVID-19 case Jan 21ndash Snohomish County WA
First US COVID-19 death Feb 29ndash King County WA
First major outbreak late FebMarch1
ndash 167 cases at Long-Term Care Facilitybull 101 residents 50 staff and 16 visitorsbull 43 deaths
1 Epidemiology of Covid-19 in a Long-Term Care Facility in King County Washington N Engl J Med 2020 Mar 27
13
UnclassifiedFor Public Use
THE WALL STREET JOURNAL
One Nursing Home 35 Coronavirus Deaths Inside the Kirkland Disaster
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
King County LTCF Outbreak
~be ~cu Uork ~itnes
Its Pure Panic A Wrenching Wait at Nursing Home Where Coronavirus Took Hold Cut off from their relatives inside a virus-stricken nursing center families are frantically searching for help and basic information
14
UnclassifiedFor Public Use
Characteristics and Outcomes of 21 Critshyically Ill Patients With COVID-19 in Washshyington State Matt Arentz MD1 Eric Yim MD2 Lindy Klaff MD2 et al
Author Affiliations I Article Information
JAMA Published online March 19 2020 doi101001jama20204326
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Single LTCF - Single Hospital
bull Overwhelmed bull No coordination bull Not isolated example
15
UnclassifiedFor Public Use
~) NORTHWEST HEALTHCARE HARBORVIEW MEDICAL CENTER
UW Medicine [f]KingCounty
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Medical Operations Coordinating Cell
bull Disaster Medical Coordination Center
bull Regional COVID Coordination Center (RC3) ndash Harborview Medical CenterKing County ndash Northwest Health Response Network
16
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Regional COVID Coordinating Center ndash Western Washington
17
UnclassifiedFor Public Use
Staffing
Impacts
Resource
Impacts
Ventilators PPE
urveillance of Hospitals
Health
Surveillance of Congregant
Settings
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Two Surveillance Pillars of the RC3
18
UnclassifiedFor Public Use
Health System __-1
Level Loadin
ealth System
Coordination of Resources
ASPR AUIS1ANT bulllCUTtamp~ ~00
UIPAUDgt1111 ~gtIC UfPO~H HUtTHCdl h oUGpound NC1 HpoundhH0Npound~~
I NfORMAT IONGAIEWAf
Two Coordination Pillars of the RC3
19
UnclassifiedFor Public Use
WA HEALTH G) About f) Stevo Mltchell
E-- Home
Q~ _ (WIJ - _uw_ 0
COVIDbulllltl1-t1 ltD _
ltD _
ltD AvilfllHlty - ~c_
44
J -(--
8 j ((MON_
36 j
--0 18 22 0 42 2~
jll 4Jtbull
r 11H -middot- __ ~ -- I 1rA
I --- --J - 353 600 500 1000 806 00 -- -- --
8 J _
101 25
fj)
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH hoUGpoundNC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Emergency Response Platform - Microsoft
bull Constrained Resources ndash Staffing ndash Beds bull Critical Care bull Acute Care
ndash Equipment bull Ventilators bull PPE
ndash COVID-19 patients
20
UnclassifiedFor Public Use
WA HEALTH C) About - Steve
~ Homo
6-hiyenHiiii+MF _ _ a
KING
43 COVID JM1Q
267
55 CD IDlnn1bned
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Emergency Response Platform - Microsoft
bull Next Releasendash Long Term Care Facilitiesbull COVID-19 Impactsndash Positive Patientsndash Positive Health Care
Workers raquo of staff impacted
bull PPE availability
21
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
William Fales MD FACEP FAEMS Medical Director Division of EMS and Trauma Michigan Department of Health and Human Services
22 UnclassifiedFor Public Use
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michiganrsquos Healthcare Preparedness Program bull Michigan Department of Health and Human Services ndash Bureau of EMS Trauma and Preparedness
bull 8 Regional Healthcare Coalitions ndash Hospitals EMS LPH EM LTC Tribal Health ndash Regional Coordinator Assistant Coordinator
Medical Director (25 FTE) ndash Regional Medical Coordination Center bull Multi-Agency Coordination Center bull Statewide use of EMResource by hospitals EMS
23
UnclassifiedFor Public Use
p ror
~ SC ON5
Sault Ste Marie
N
bull
Huron
Madison Milwa uk ee Graed Rapids bull bull e bull ~ 3rnia
L~nsi~ g bull - It bull
bullbullbullbull bull bull bull bull De troi t
bull Glwcago bull bull bull
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Michigan COVID-19 bull bull
bull
First 2 cases ndash March 10 Asymmetric epidemiology ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
24
UnclassifiedFor Public Use
Barrie
Toronto
Hamilton
bull bull
bull
Lake Ontario
bull Ro~besterbull
bull
bull
Brockville bull Kingston
~~w voRK
bull bull bull
bull
bull Pt0NfV VAN1A bull
bull
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H I NfOR MATION GATEWAY
bull
bull bull ~ ba riy
bull bull
Michigan COVID-19 bull First 2 cases ndash March 10
Asymmetric epidemiology bull ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
bull Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
25
UnclassifiedFor Public Use
I I I I I I I I I I I I I
ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City COVID-19 Daily Hospital Admissions
New York City vs Detroit 1800 1600 1400 1200 1000 800 600 400 200 0
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 26
UnclassifiedFor Public Use ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City
1 1 I 11111 111 11 11 1111 1 II II 1 1 1
400
300
200
COVID-19 Daily Hospital Admissions Per 1 Million PopulationNew York City vs Detroit
40-Day Post-Outbreak Mortality bull NY City 646 deaths per million bull Detroit 919 deaths per million
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 27
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Goal bull Save lives and reduce pain and suffering by optimizing
the use of the statersquos healthcare resources ndash Extend conventional standards of care to as many
patients as possible ndash Minimize the need for crisis standards of care bull Especially while conventional capacity exists
28
UnclassifiedFor Public Use
--
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Components bull Relief Hospitals
bull Alternate Care Sites EMS
ndash Home Care Sites
ndash Relief Personnel
29
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals vs Alternate Care Sites bull Relief Hospitals The objective is to extend the
conventional standard of care to as many citizens in need as possible (ie minimize the need to move intocrisis standards of care)
bull Alternate Care Sites (ACS) The objective is to delivercrisis standards of care (as close to the conventional standard of care as possible) in extreme conditions in which the conventional standard of care can not be provided at overloaded hospitals
30
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital ldquoAskrdquo bull Hospitals have been previously asked to be able to
surge an additional 20 above average daily census ndash Increased to 50 ldquosuper surgerdquo
bull Relief Hospitals provide 10 of their expanded capacity to assist severely impacted hospitals ndash While preserving 50 of super-surge capacity bull Many hospitals at very low census
31
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals and Patient Redistribution
bull Intra-Health System Transfer ndash Coordinated by specific health system
bull Intra-Regional Transfer ndash Coordinated by Regional Medical Coordination Center
bull Statewide Transfer ndash Coordinated by Inter-Hospital Coordination Unit bull AKA Medical Operations Coordination Cell (MOCC)
32
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Statewide Inter-Hospital Coordination Unit State EmergencyOperations Center
Planning Finance Operations
Health Branch
Inter-HospitalCoordination Unit
Physician Consultant
EMS Coordination Group
Logistics
MDHHS Health Emergency Operations
Center
Medical Operations
Coordination Cell
33
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs and Patient Redistribution Regional Medical
Coordination Center bull Relief hospitals declare status on
EMResource bull RMCC receives request from
transferring hospital bull RMCC identifies Relief Hospital(s) bull Transferring hospital contacts
Relief Hospital directly bull Relief Hospital accepts patient(s) bull RMCC coordinates EMS PRN
Statewide Inter-Hospital Coordination Unit
Relief hospitals declare status on EMResource
IHCU receives request from RMCC on behalf of transferring hospital
IHCU identifies Relief Hospital(s) Transferring hospital contacts Relief
Hospital directly Relief Hospital accepts patient(s) IHCU coordinates EMS PRN
34
UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

8Saving Lives Protecting Americans
bull
A MOCC AIMS TO
Move patients to the at the right to improve staff and right time in the patientsupplies provider right way well-being
8
9Saving Lives Protecting Americans
MOCCs | Concept MOCCs can be activated at the Sub-State Regional State and Federal levels to facilitate patient movement and resource allocation during a surge event There are three types of MOCCs included in the concept sub-state Regional Medical Operations Coordination Centers (RMOCCs) State Medical Operations Coordination Centers (SMOCCs) and Federal Medical Operations Coordination Centers (FMOCCs)
RMOCC Sub-State Level
SMOCC State Level
FMOCC Federal Level
HHS Region A HHS Region B
RegionA
State A
RegionB
State A
RegionC
State A
State D HHS Region B
State E HHS Region B
State A HHS Region A
State B HHS Region A
State C HHS Region A
RegionD
State B
RegionE
State B
RegionF
State C
RegionG
State C Region
H State D
RegionI
State D
RegionJ
State D
RegionK
State E
RegionL
State E Region
M State E
State F HHS Region B
RegionN
State F
RegionO
State F
Patient transfer coordination activity originates with the RMOCC The SMOCC can help transfer patients to a facility in a neighboring sub-state region The FMOCC can transfer patients to a neighboring state or Federal
HHS Region if that is closer 9
MOCCs | General Activity Summary
MOCCs are cells within emergency operations centers (EOCs) at the sub-state regional state and federal levels (FEMAHHS regions) that facilitate patient movement and resource allocation
MOCC PRIORITIES
bull Adding clinical staff to existing EOCs and RRCCsbull Establishing stakeholder agreements that allow for collecting data regarding health system capacity synthesizing the data to
understand the needs of the system and determining areas of the system that may be overwhelmedbull Facilitating movement of patients staff and supplies between healthcare facilities andor states
MOCC ROLE
bull Acting as a single point of contact (POC) for requests from multiple stakeholders such as healthcare facilities RMOCCs and SMOCCsbull Reviewing facilitating and processing patient movement staffing and supply requests and providing medical consultation to
facilitate the decompression of health systems
MOCC DATA ACTIVITIES
bull Collecting analyzing and disseminating information to and from stakeholders to develop comprehensive situational awarenessbull Establishing protocols systems and triggers to inform operational planning stakeholder communications and transfer decision
making
10
~ - ~--~- ----- -
MOCCs | Toolkit
The MOCCs Toolkit contains information on funding a MOCC standard operating procedures for each type of MOCC including integration with ESF-8 roles and responsibilities staffing and transport coordination
FUNDING
bull FEMA Public Assistancebull FEMA Mission Assignmentbull ASPR Hospital Preparedness
Programbull CDC Public Health Emergency
PreparednessCrisis Agreement
STANDARD OPERATING TRANSPORT PROCEDURES COORDINATION
bull RMOCCSMOCC
bull FMOCC
bull Transportation workflows andbull transfer checklists
Each MOCC SOP includes details on bullbullbullbullbull
MOCC Integration with ESF-8Roles and ResponsibilitiesStaffingOperationsPatient MovementMedical Resource Sharing
The MOCCs Toolkit will be located on ASPR TRACIE
11
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Steven Mitchell MD FACEP Medical Director Western Washington Regional COVID Coordination Center Medical Director Emergency Department Harborview Medical Center
12 UnclassifiedFor Public Use
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Western Washington MOCC
bull
bull
bull
First US COVID-19 case Jan 21ndash Snohomish County WA
First US COVID-19 death Feb 29ndash King County WA
First major outbreak late FebMarch1
ndash 167 cases at Long-Term Care Facilitybull 101 residents 50 staff and 16 visitorsbull 43 deaths
1 Epidemiology of Covid-19 in a Long-Term Care Facility in King County Washington N Engl J Med 2020 Mar 27
13
UnclassifiedFor Public Use
THE WALL STREET JOURNAL
One Nursing Home 35 Coronavirus Deaths Inside the Kirkland Disaster
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
King County LTCF Outbreak
~be ~cu Uork ~itnes
Its Pure Panic A Wrenching Wait at Nursing Home Where Coronavirus Took Hold Cut off from their relatives inside a virus-stricken nursing center families are frantically searching for help and basic information
14
UnclassifiedFor Public Use
Characteristics and Outcomes of 21 Critshyically Ill Patients With COVID-19 in Washshyington State Matt Arentz MD1 Eric Yim MD2 Lindy Klaff MD2 et al
Author Affiliations I Article Information
JAMA Published online March 19 2020 doi101001jama20204326
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Single LTCF - Single Hospital
bull Overwhelmed bull No coordination bull Not isolated example
15
UnclassifiedFor Public Use
~) NORTHWEST HEALTHCARE HARBORVIEW MEDICAL CENTER
UW Medicine [f]KingCounty
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Medical Operations Coordinating Cell
bull Disaster Medical Coordination Center
bull Regional COVID Coordination Center (RC3) ndash Harborview Medical CenterKing County ndash Northwest Health Response Network
16
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Regional COVID Coordinating Center ndash Western Washington
17
UnclassifiedFor Public Use
Staffing
Impacts
Resource
Impacts
Ventilators PPE
urveillance of Hospitals
Health
Surveillance of Congregant
Settings
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Two Surveillance Pillars of the RC3
18
UnclassifiedFor Public Use
Health System __-1
Level Loadin
ealth System
Coordination of Resources
ASPR AUIS1ANT bulllCUTtamp~ ~00
UIPAUDgt1111 ~gtIC UfPO~H HUtTHCdl h oUGpound NC1 HpoundhH0Npound~~
I NfORMAT IONGAIEWAf
Two Coordination Pillars of the RC3
19
UnclassifiedFor Public Use
WA HEALTH G) About f) Stevo Mltchell
E-- Home
Q~ _ (WIJ - _uw_ 0
COVIDbulllltl1-t1 ltD _
ltD _
ltD AvilfllHlty - ~c_
44
J -(--
8 j ((MON_
36 j
--0 18 22 0 42 2~
jll 4Jtbull
r 11H -middot- __ ~ -- I 1rA
I --- --J - 353 600 500 1000 806 00 -- -- --
8 J _
101 25
fj)
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH hoUGpoundNC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Emergency Response Platform - Microsoft
bull Constrained Resources ndash Staffing ndash Beds bull Critical Care bull Acute Care
ndash Equipment bull Ventilators bull PPE
ndash COVID-19 patients
20
UnclassifiedFor Public Use
WA HEALTH C) About - Steve
~ Homo
6-hiyenHiiii+MF _ _ a
KING
43 COVID JM1Q
267
55 CD IDlnn1bned
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Emergency Response Platform - Microsoft
bull Next Releasendash Long Term Care Facilitiesbull COVID-19 Impactsndash Positive Patientsndash Positive Health Care
Workers raquo of staff impacted
bull PPE availability
21
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
William Fales MD FACEP FAEMS Medical Director Division of EMS and Trauma Michigan Department of Health and Human Services
22 UnclassifiedFor Public Use
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michiganrsquos Healthcare Preparedness Program bull Michigan Department of Health and Human Services ndash Bureau of EMS Trauma and Preparedness
bull 8 Regional Healthcare Coalitions ndash Hospitals EMS LPH EM LTC Tribal Health ndash Regional Coordinator Assistant Coordinator
Medical Director (25 FTE) ndash Regional Medical Coordination Center bull Multi-Agency Coordination Center bull Statewide use of EMResource by hospitals EMS
23
UnclassifiedFor Public Use
p ror
~ SC ON5
Sault Ste Marie
N
bull
Huron
Madison Milwa uk ee Graed Rapids bull bull e bull ~ 3rnia
L~nsi~ g bull - It bull
bullbullbullbull bull bull bull bull De troi t
bull Glwcago bull bull bull
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Michigan COVID-19 bull bull
bull
First 2 cases ndash March 10 Asymmetric epidemiology ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
24
UnclassifiedFor Public Use
Barrie
Toronto
Hamilton
bull bull
bull
Lake Ontario
bull Ro~besterbull
bull
bull
Brockville bull Kingston
~~w voRK
bull bull bull
bull
bull Pt0NfV VAN1A bull
bull
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H I NfOR MATION GATEWAY
bull
bull bull ~ ba riy
bull bull
Michigan COVID-19 bull First 2 cases ndash March 10
Asymmetric epidemiology bull ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
bull Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
25
UnclassifiedFor Public Use
I I I I I I I I I I I I I
ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City COVID-19 Daily Hospital Admissions
New York City vs Detroit 1800 1600 1400 1200 1000 800 600 400 200 0
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 26
UnclassifiedFor Public Use ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City
1 1 I 11111 111 11 11 1111 1 II II 1 1 1
400
300
200
COVID-19 Daily Hospital Admissions Per 1 Million PopulationNew York City vs Detroit
40-Day Post-Outbreak Mortality bull NY City 646 deaths per million bull Detroit 919 deaths per million
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 27
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Goal bull Save lives and reduce pain and suffering by optimizing
the use of the statersquos healthcare resources ndash Extend conventional standards of care to as many
patients as possible ndash Minimize the need for crisis standards of care bull Especially while conventional capacity exists
28
UnclassifiedFor Public Use
--
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Components bull Relief Hospitals
bull Alternate Care Sites EMS
ndash Home Care Sites
ndash Relief Personnel
29
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals vs Alternate Care Sites bull Relief Hospitals The objective is to extend the
conventional standard of care to as many citizens in need as possible (ie minimize the need to move intocrisis standards of care)
bull Alternate Care Sites (ACS) The objective is to delivercrisis standards of care (as close to the conventional standard of care as possible) in extreme conditions in which the conventional standard of care can not be provided at overloaded hospitals
30
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital ldquoAskrdquo bull Hospitals have been previously asked to be able to
surge an additional 20 above average daily census ndash Increased to 50 ldquosuper surgerdquo
bull Relief Hospitals provide 10 of their expanded capacity to assist severely impacted hospitals ndash While preserving 50 of super-surge capacity bull Many hospitals at very low census
31
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals and Patient Redistribution
bull Intra-Health System Transfer ndash Coordinated by specific health system
bull Intra-Regional Transfer ndash Coordinated by Regional Medical Coordination Center
bull Statewide Transfer ndash Coordinated by Inter-Hospital Coordination Unit bull AKA Medical Operations Coordination Cell (MOCC)
32
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Statewide Inter-Hospital Coordination Unit State EmergencyOperations Center
Planning Finance Operations
Health Branch
Inter-HospitalCoordination Unit
Physician Consultant
EMS Coordination Group
Logistics
MDHHS Health Emergency Operations
Center
Medical Operations
Coordination Cell
33
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs and Patient Redistribution Regional Medical
Coordination Center bull Relief hospitals declare status on
EMResource bull RMCC receives request from
transferring hospital bull RMCC identifies Relief Hospital(s) bull Transferring hospital contacts
Relief Hospital directly bull Relief Hospital accepts patient(s) bull RMCC coordinates EMS PRN
Statewide Inter-Hospital Coordination Unit
Relief hospitals declare status on EMResource
IHCU receives request from RMCC on behalf of transferring hospital
IHCU identifies Relief Hospital(s) Transferring hospital contacts Relief
Hospital directly Relief Hospital accepts patient(s) IHCU coordinates EMS PRN
34
UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

9Saving Lives Protecting Americans
MOCCs | Concept MOCCs can be activated at the Sub-State Regional State and Federal levels to facilitate patient movement and resource allocation during a surge event There are three types of MOCCs included in the concept sub-state Regional Medical Operations Coordination Centers (RMOCCs) State Medical Operations Coordination Centers (SMOCCs) and Federal Medical Operations Coordination Centers (FMOCCs)
RMOCC Sub-State Level
SMOCC State Level
FMOCC Federal Level
HHS Region A HHS Region B
RegionA
State A
RegionB
State A
RegionC
State A
State D HHS Region B
State E HHS Region B
State A HHS Region A
State B HHS Region A
State C HHS Region A
RegionD
State B
RegionE
State B
RegionF
State C
RegionG
State C Region
H State D
RegionI
State D
RegionJ
State D
RegionK
State E
RegionL
State E Region
M State E
State F HHS Region B
RegionN
State F
RegionO
State F
Patient transfer coordination activity originates with the RMOCC The SMOCC can help transfer patients to a facility in a neighboring sub-state region The FMOCC can transfer patients to a neighboring state or Federal
HHS Region if that is closer 9
MOCCs | General Activity Summary
MOCCs are cells within emergency operations centers (EOCs) at the sub-state regional state and federal levels (FEMAHHS regions) that facilitate patient movement and resource allocation
MOCC PRIORITIES
bull Adding clinical staff to existing EOCs and RRCCsbull Establishing stakeholder agreements that allow for collecting data regarding health system capacity synthesizing the data to
understand the needs of the system and determining areas of the system that may be overwhelmedbull Facilitating movement of patients staff and supplies between healthcare facilities andor states
MOCC ROLE
bull Acting as a single point of contact (POC) for requests from multiple stakeholders such as healthcare facilities RMOCCs and SMOCCsbull Reviewing facilitating and processing patient movement staffing and supply requests and providing medical consultation to
facilitate the decompression of health systems
MOCC DATA ACTIVITIES
bull Collecting analyzing and disseminating information to and from stakeholders to develop comprehensive situational awarenessbull Establishing protocols systems and triggers to inform operational planning stakeholder communications and transfer decision
making
10
~ - ~--~- ----- -
MOCCs | Toolkit
The MOCCs Toolkit contains information on funding a MOCC standard operating procedures for each type of MOCC including integration with ESF-8 roles and responsibilities staffing and transport coordination
FUNDING
bull FEMA Public Assistancebull FEMA Mission Assignmentbull ASPR Hospital Preparedness
Programbull CDC Public Health Emergency
PreparednessCrisis Agreement
STANDARD OPERATING TRANSPORT PROCEDURES COORDINATION
bull RMOCCSMOCC
bull FMOCC
bull Transportation workflows andbull transfer checklists
Each MOCC SOP includes details on bullbullbullbullbull
MOCC Integration with ESF-8Roles and ResponsibilitiesStaffingOperationsPatient MovementMedical Resource Sharing
The MOCCs Toolkit will be located on ASPR TRACIE
11
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Steven Mitchell MD FACEP Medical Director Western Washington Regional COVID Coordination Center Medical Director Emergency Department Harborview Medical Center
12 UnclassifiedFor Public Use
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Western Washington MOCC
bull
bull
bull
First US COVID-19 case Jan 21ndash Snohomish County WA
First US COVID-19 death Feb 29ndash King County WA
First major outbreak late FebMarch1
ndash 167 cases at Long-Term Care Facilitybull 101 residents 50 staff and 16 visitorsbull 43 deaths
1 Epidemiology of Covid-19 in a Long-Term Care Facility in King County Washington N Engl J Med 2020 Mar 27
13
UnclassifiedFor Public Use
THE WALL STREET JOURNAL
One Nursing Home 35 Coronavirus Deaths Inside the Kirkland Disaster
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
King County LTCF Outbreak
~be ~cu Uork ~itnes
Its Pure Panic A Wrenching Wait at Nursing Home Where Coronavirus Took Hold Cut off from their relatives inside a virus-stricken nursing center families are frantically searching for help and basic information
14
UnclassifiedFor Public Use
Characteristics and Outcomes of 21 Critshyically Ill Patients With COVID-19 in Washshyington State Matt Arentz MD1 Eric Yim MD2 Lindy Klaff MD2 et al
Author Affiliations I Article Information
JAMA Published online March 19 2020 doi101001jama20204326
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Single LTCF - Single Hospital
bull Overwhelmed bull No coordination bull Not isolated example
15
UnclassifiedFor Public Use
~) NORTHWEST HEALTHCARE HARBORVIEW MEDICAL CENTER
UW Medicine [f]KingCounty
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Medical Operations Coordinating Cell
bull Disaster Medical Coordination Center
bull Regional COVID Coordination Center (RC3) ndash Harborview Medical CenterKing County ndash Northwest Health Response Network
16
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Regional COVID Coordinating Center ndash Western Washington
17
UnclassifiedFor Public Use
Staffing
Impacts
Resource
Impacts
Ventilators PPE
urveillance of Hospitals
Health
Surveillance of Congregant
Settings
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Two Surveillance Pillars of the RC3
18
UnclassifiedFor Public Use
Health System __-1
Level Loadin
ealth System
Coordination of Resources
ASPR AUIS1ANT bulllCUTtamp~ ~00
UIPAUDgt1111 ~gtIC UfPO~H HUtTHCdl h oUGpound NC1 HpoundhH0Npound~~
I NfORMAT IONGAIEWAf
Two Coordination Pillars of the RC3
19
UnclassifiedFor Public Use
WA HEALTH G) About f) Stevo Mltchell
E-- Home
Q~ _ (WIJ - _uw_ 0
COVIDbulllltl1-t1 ltD _
ltD _
ltD AvilfllHlty - ~c_
44
J -(--
8 j ((MON_
36 j
--0 18 22 0 42 2~
jll 4Jtbull
r 11H -middot- __ ~ -- I 1rA
I --- --J - 353 600 500 1000 806 00 -- -- --
8 J _
101 25
fj)
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH hoUGpoundNC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Emergency Response Platform - Microsoft
bull Constrained Resources ndash Staffing ndash Beds bull Critical Care bull Acute Care
ndash Equipment bull Ventilators bull PPE
ndash COVID-19 patients
20
UnclassifiedFor Public Use
WA HEALTH C) About - Steve
~ Homo
6-hiyenHiiii+MF _ _ a
KING
43 COVID JM1Q
267
55 CD IDlnn1bned
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Emergency Response Platform - Microsoft
bull Next Releasendash Long Term Care Facilitiesbull COVID-19 Impactsndash Positive Patientsndash Positive Health Care
Workers raquo of staff impacted
bull PPE availability
21
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
William Fales MD FACEP FAEMS Medical Director Division of EMS and Trauma Michigan Department of Health and Human Services
22 UnclassifiedFor Public Use
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michiganrsquos Healthcare Preparedness Program bull Michigan Department of Health and Human Services ndash Bureau of EMS Trauma and Preparedness
bull 8 Regional Healthcare Coalitions ndash Hospitals EMS LPH EM LTC Tribal Health ndash Regional Coordinator Assistant Coordinator
Medical Director (25 FTE) ndash Regional Medical Coordination Center bull Multi-Agency Coordination Center bull Statewide use of EMResource by hospitals EMS
23
UnclassifiedFor Public Use
p ror
~ SC ON5
Sault Ste Marie
N
bull
Huron
Madison Milwa uk ee Graed Rapids bull bull e bull ~ 3rnia
L~nsi~ g bull - It bull
bullbullbullbull bull bull bull bull De troi t
bull Glwcago bull bull bull
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Michigan COVID-19 bull bull
bull
First 2 cases ndash March 10 Asymmetric epidemiology ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
24
UnclassifiedFor Public Use
Barrie
Toronto
Hamilton
bull bull
bull
Lake Ontario
bull Ro~besterbull
bull
bull
Brockville bull Kingston
~~w voRK
bull bull bull
bull
bull Pt0NfV VAN1A bull
bull
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H I NfOR MATION GATEWAY
bull
bull bull ~ ba riy
bull bull
Michigan COVID-19 bull First 2 cases ndash March 10
Asymmetric epidemiology bull ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
bull Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
25
UnclassifiedFor Public Use
I I I I I I I I I I I I I
ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City COVID-19 Daily Hospital Admissions
New York City vs Detroit 1800 1600 1400 1200 1000 800 600 400 200 0
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 26
UnclassifiedFor Public Use ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City
1 1 I 11111 111 11 11 1111 1 II II 1 1 1
400
300
200
COVID-19 Daily Hospital Admissions Per 1 Million PopulationNew York City vs Detroit
40-Day Post-Outbreak Mortality bull NY City 646 deaths per million bull Detroit 919 deaths per million
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 27
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Goal bull Save lives and reduce pain and suffering by optimizing
the use of the statersquos healthcare resources ndash Extend conventional standards of care to as many
patients as possible ndash Minimize the need for crisis standards of care bull Especially while conventional capacity exists
28
UnclassifiedFor Public Use
--
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Components bull Relief Hospitals
bull Alternate Care Sites EMS
ndash Home Care Sites
ndash Relief Personnel
29
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals vs Alternate Care Sites bull Relief Hospitals The objective is to extend the
conventional standard of care to as many citizens in need as possible (ie minimize the need to move intocrisis standards of care)
bull Alternate Care Sites (ACS) The objective is to delivercrisis standards of care (as close to the conventional standard of care as possible) in extreme conditions in which the conventional standard of care can not be provided at overloaded hospitals
30
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital ldquoAskrdquo bull Hospitals have been previously asked to be able to
surge an additional 20 above average daily census ndash Increased to 50 ldquosuper surgerdquo
bull Relief Hospitals provide 10 of their expanded capacity to assist severely impacted hospitals ndash While preserving 50 of super-surge capacity bull Many hospitals at very low census
31
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals and Patient Redistribution
bull Intra-Health System Transfer ndash Coordinated by specific health system
bull Intra-Regional Transfer ndash Coordinated by Regional Medical Coordination Center
bull Statewide Transfer ndash Coordinated by Inter-Hospital Coordination Unit bull AKA Medical Operations Coordination Cell (MOCC)
32
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Statewide Inter-Hospital Coordination Unit State EmergencyOperations Center
Planning Finance Operations
Health Branch
Inter-HospitalCoordination Unit
Physician Consultant
EMS Coordination Group
Logistics
MDHHS Health Emergency Operations
Center
Medical Operations
Coordination Cell
33
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs and Patient Redistribution Regional Medical
Coordination Center bull Relief hospitals declare status on
EMResource bull RMCC receives request from
transferring hospital bull RMCC identifies Relief Hospital(s) bull Transferring hospital contacts
Relief Hospital directly bull Relief Hospital accepts patient(s) bull RMCC coordinates EMS PRN
Statewide Inter-Hospital Coordination Unit
Relief hospitals declare status on EMResource
IHCU receives request from RMCC on behalf of transferring hospital
IHCU identifies Relief Hospital(s) Transferring hospital contacts Relief
Hospital directly Relief Hospital accepts patient(s) IHCU coordinates EMS PRN
34
UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

MOCCs | General Activity Summary
MOCCs are cells within emergency operations centers (EOCs) at the sub-state regional state and federal levels (FEMAHHS regions) that facilitate patient movement and resource allocation
MOCC PRIORITIES
bull Adding clinical staff to existing EOCs and RRCCsbull Establishing stakeholder agreements that allow for collecting data regarding health system capacity synthesizing the data to
understand the needs of the system and determining areas of the system that may be overwhelmedbull Facilitating movement of patients staff and supplies between healthcare facilities andor states
MOCC ROLE
bull Acting as a single point of contact (POC) for requests from multiple stakeholders such as healthcare facilities RMOCCs and SMOCCsbull Reviewing facilitating and processing patient movement staffing and supply requests and providing medical consultation to
facilitate the decompression of health systems
MOCC DATA ACTIVITIES
bull Collecting analyzing and disseminating information to and from stakeholders to develop comprehensive situational awarenessbull Establishing protocols systems and triggers to inform operational planning stakeholder communications and transfer decision
making
10
~ - ~--~- ----- -
MOCCs | Toolkit
The MOCCs Toolkit contains information on funding a MOCC standard operating procedures for each type of MOCC including integration with ESF-8 roles and responsibilities staffing and transport coordination
FUNDING
bull FEMA Public Assistancebull FEMA Mission Assignmentbull ASPR Hospital Preparedness
Programbull CDC Public Health Emergency
PreparednessCrisis Agreement
STANDARD OPERATING TRANSPORT PROCEDURES COORDINATION
bull RMOCCSMOCC
bull FMOCC
bull Transportation workflows andbull transfer checklists
Each MOCC SOP includes details on bullbullbullbullbull
MOCC Integration with ESF-8Roles and ResponsibilitiesStaffingOperationsPatient MovementMedical Resource Sharing
The MOCCs Toolkit will be located on ASPR TRACIE
11
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Steven Mitchell MD FACEP Medical Director Western Washington Regional COVID Coordination Center Medical Director Emergency Department Harborview Medical Center
12 UnclassifiedFor Public Use
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Western Washington MOCC
bull
bull
bull
First US COVID-19 case Jan 21ndash Snohomish County WA
First US COVID-19 death Feb 29ndash King County WA
First major outbreak late FebMarch1
ndash 167 cases at Long-Term Care Facilitybull 101 residents 50 staff and 16 visitorsbull 43 deaths
1 Epidemiology of Covid-19 in a Long-Term Care Facility in King County Washington N Engl J Med 2020 Mar 27
13
UnclassifiedFor Public Use
THE WALL STREET JOURNAL
One Nursing Home 35 Coronavirus Deaths Inside the Kirkland Disaster
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
King County LTCF Outbreak
~be ~cu Uork ~itnes
Its Pure Panic A Wrenching Wait at Nursing Home Where Coronavirus Took Hold Cut off from their relatives inside a virus-stricken nursing center families are frantically searching for help and basic information
14
UnclassifiedFor Public Use
Characteristics and Outcomes of 21 Critshyically Ill Patients With COVID-19 in Washshyington State Matt Arentz MD1 Eric Yim MD2 Lindy Klaff MD2 et al
Author Affiliations I Article Information
JAMA Published online March 19 2020 doi101001jama20204326
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Single LTCF - Single Hospital
bull Overwhelmed bull No coordination bull Not isolated example
15
UnclassifiedFor Public Use
~) NORTHWEST HEALTHCARE HARBORVIEW MEDICAL CENTER
UW Medicine [f]KingCounty
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Medical Operations Coordinating Cell
bull Disaster Medical Coordination Center
bull Regional COVID Coordination Center (RC3) ndash Harborview Medical CenterKing County ndash Northwest Health Response Network
16
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Regional COVID Coordinating Center ndash Western Washington
17
UnclassifiedFor Public Use
Staffing
Impacts
Resource
Impacts
Ventilators PPE
urveillance of Hospitals
Health
Surveillance of Congregant
Settings
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Two Surveillance Pillars of the RC3
18
UnclassifiedFor Public Use
Health System __-1
Level Loadin
ealth System
Coordination of Resources
ASPR AUIS1ANT bulllCUTtamp~ ~00
UIPAUDgt1111 ~gtIC UfPO~H HUtTHCdl h oUGpound NC1 HpoundhH0Npound~~
I NfORMAT IONGAIEWAf
Two Coordination Pillars of the RC3
19
UnclassifiedFor Public Use
WA HEALTH G) About f) Stevo Mltchell
E-- Home
Q~ _ (WIJ - _uw_ 0
COVIDbulllltl1-t1 ltD _
ltD _
ltD AvilfllHlty - ~c_
44
J -(--
8 j ((MON_
36 j
--0 18 22 0 42 2~
jll 4Jtbull
r 11H -middot- __ ~ -- I 1rA
I --- --J - 353 600 500 1000 806 00 -- -- --
8 J _
101 25
fj)
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH hoUGpoundNC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Emergency Response Platform - Microsoft
bull Constrained Resources ndash Staffing ndash Beds bull Critical Care bull Acute Care
ndash Equipment bull Ventilators bull PPE
ndash COVID-19 patients
20
UnclassifiedFor Public Use
WA HEALTH C) About - Steve
~ Homo
6-hiyenHiiii+MF _ _ a
KING
43 COVID JM1Q
267
55 CD IDlnn1bned
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Emergency Response Platform - Microsoft
bull Next Releasendash Long Term Care Facilitiesbull COVID-19 Impactsndash Positive Patientsndash Positive Health Care
Workers raquo of staff impacted
bull PPE availability
21
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
William Fales MD FACEP FAEMS Medical Director Division of EMS and Trauma Michigan Department of Health and Human Services
22 UnclassifiedFor Public Use
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michiganrsquos Healthcare Preparedness Program bull Michigan Department of Health and Human Services ndash Bureau of EMS Trauma and Preparedness
bull 8 Regional Healthcare Coalitions ndash Hospitals EMS LPH EM LTC Tribal Health ndash Regional Coordinator Assistant Coordinator
Medical Director (25 FTE) ndash Regional Medical Coordination Center bull Multi-Agency Coordination Center bull Statewide use of EMResource by hospitals EMS
23
UnclassifiedFor Public Use
p ror
~ SC ON5
Sault Ste Marie
N
bull
Huron
Madison Milwa uk ee Graed Rapids bull bull e bull ~ 3rnia
L~nsi~ g bull - It bull
bullbullbullbull bull bull bull bull De troi t
bull Glwcago bull bull bull
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Michigan COVID-19 bull bull
bull
First 2 cases ndash March 10 Asymmetric epidemiology ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
24
UnclassifiedFor Public Use
Barrie
Toronto
Hamilton
bull bull
bull
Lake Ontario
bull Ro~besterbull
bull
bull
Brockville bull Kingston
~~w voRK
bull bull bull
bull
bull Pt0NfV VAN1A bull
bull
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H I NfOR MATION GATEWAY
bull
bull bull ~ ba riy
bull bull
Michigan COVID-19 bull First 2 cases ndash March 10
Asymmetric epidemiology bull ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
bull Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
25
UnclassifiedFor Public Use
I I I I I I I I I I I I I
ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City COVID-19 Daily Hospital Admissions
New York City vs Detroit 1800 1600 1400 1200 1000 800 600 400 200 0
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 26
UnclassifiedFor Public Use ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City
1 1 I 11111 111 11 11 1111 1 II II 1 1 1
400
300
200
COVID-19 Daily Hospital Admissions Per 1 Million PopulationNew York City vs Detroit
40-Day Post-Outbreak Mortality bull NY City 646 deaths per million bull Detroit 919 deaths per million
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 27
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Goal bull Save lives and reduce pain and suffering by optimizing
the use of the statersquos healthcare resources ndash Extend conventional standards of care to as many
patients as possible ndash Minimize the need for crisis standards of care bull Especially while conventional capacity exists
28
UnclassifiedFor Public Use
--
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Components bull Relief Hospitals
bull Alternate Care Sites EMS
ndash Home Care Sites
ndash Relief Personnel
29
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals vs Alternate Care Sites bull Relief Hospitals The objective is to extend the
conventional standard of care to as many citizens in need as possible (ie minimize the need to move intocrisis standards of care)
bull Alternate Care Sites (ACS) The objective is to delivercrisis standards of care (as close to the conventional standard of care as possible) in extreme conditions in which the conventional standard of care can not be provided at overloaded hospitals
30
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital ldquoAskrdquo bull Hospitals have been previously asked to be able to
surge an additional 20 above average daily census ndash Increased to 50 ldquosuper surgerdquo
bull Relief Hospitals provide 10 of their expanded capacity to assist severely impacted hospitals ndash While preserving 50 of super-surge capacity bull Many hospitals at very low census
31
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals and Patient Redistribution
bull Intra-Health System Transfer ndash Coordinated by specific health system
bull Intra-Regional Transfer ndash Coordinated by Regional Medical Coordination Center
bull Statewide Transfer ndash Coordinated by Inter-Hospital Coordination Unit bull AKA Medical Operations Coordination Cell (MOCC)
32
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Statewide Inter-Hospital Coordination Unit State EmergencyOperations Center
Planning Finance Operations
Health Branch
Inter-HospitalCoordination Unit
Physician Consultant
EMS Coordination Group
Logistics
MDHHS Health Emergency Operations
Center
Medical Operations
Coordination Cell
33
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs and Patient Redistribution Regional Medical
Coordination Center bull Relief hospitals declare status on
EMResource bull RMCC receives request from
transferring hospital bull RMCC identifies Relief Hospital(s) bull Transferring hospital contacts
Relief Hospital directly bull Relief Hospital accepts patient(s) bull RMCC coordinates EMS PRN
Statewide Inter-Hospital Coordination Unit
Relief hospitals declare status on EMResource
IHCU receives request from RMCC on behalf of transferring hospital
IHCU identifies Relief Hospital(s) Transferring hospital contacts Relief
Hospital directly Relief Hospital accepts patient(s) IHCU coordinates EMS PRN
34
UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

~ - ~--~- ----- -
MOCCs | Toolkit
The MOCCs Toolkit contains information on funding a MOCC standard operating procedures for each type of MOCC including integration with ESF-8 roles and responsibilities staffing and transport coordination
FUNDING
bull FEMA Public Assistancebull FEMA Mission Assignmentbull ASPR Hospital Preparedness
Programbull CDC Public Health Emergency
PreparednessCrisis Agreement
STANDARD OPERATING TRANSPORT PROCEDURES COORDINATION
bull RMOCCSMOCC
bull FMOCC
bull Transportation workflows andbull transfer checklists
Each MOCC SOP includes details on bullbullbullbullbull
MOCC Integration with ESF-8Roles and ResponsibilitiesStaffingOperationsPatient MovementMedical Resource Sharing
The MOCCs Toolkit will be located on ASPR TRACIE
11
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Steven Mitchell MD FACEP Medical Director Western Washington Regional COVID Coordination Center Medical Director Emergency Department Harborview Medical Center
12 UnclassifiedFor Public Use
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Western Washington MOCC
bull
bull
bull
First US COVID-19 case Jan 21ndash Snohomish County WA
First US COVID-19 death Feb 29ndash King County WA
First major outbreak late FebMarch1
ndash 167 cases at Long-Term Care Facilitybull 101 residents 50 staff and 16 visitorsbull 43 deaths
1 Epidemiology of Covid-19 in a Long-Term Care Facility in King County Washington N Engl J Med 2020 Mar 27
13
UnclassifiedFor Public Use
THE WALL STREET JOURNAL
One Nursing Home 35 Coronavirus Deaths Inside the Kirkland Disaster
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
King County LTCF Outbreak
~be ~cu Uork ~itnes
Its Pure Panic A Wrenching Wait at Nursing Home Where Coronavirus Took Hold Cut off from their relatives inside a virus-stricken nursing center families are frantically searching for help and basic information
14
UnclassifiedFor Public Use
Characteristics and Outcomes of 21 Critshyically Ill Patients With COVID-19 in Washshyington State Matt Arentz MD1 Eric Yim MD2 Lindy Klaff MD2 et al
Author Affiliations I Article Information
JAMA Published online March 19 2020 doi101001jama20204326
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Single LTCF - Single Hospital
bull Overwhelmed bull No coordination bull Not isolated example
15
UnclassifiedFor Public Use
~) NORTHWEST HEALTHCARE HARBORVIEW MEDICAL CENTER
UW Medicine [f]KingCounty
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Medical Operations Coordinating Cell
bull Disaster Medical Coordination Center
bull Regional COVID Coordination Center (RC3) ndash Harborview Medical CenterKing County ndash Northwest Health Response Network
16
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Regional COVID Coordinating Center ndash Western Washington
17
UnclassifiedFor Public Use
Staffing
Impacts
Resource
Impacts
Ventilators PPE
urveillance of Hospitals
Health
Surveillance of Congregant
Settings
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Two Surveillance Pillars of the RC3
18
UnclassifiedFor Public Use
Health System __-1
Level Loadin
ealth System
Coordination of Resources
ASPR AUIS1ANT bulllCUTtamp~ ~00
UIPAUDgt1111 ~gtIC UfPO~H HUtTHCdl h oUGpound NC1 HpoundhH0Npound~~
I NfORMAT IONGAIEWAf
Two Coordination Pillars of the RC3
19
UnclassifiedFor Public Use
WA HEALTH G) About f) Stevo Mltchell
E-- Home
Q~ _ (WIJ - _uw_ 0
COVIDbulllltl1-t1 ltD _
ltD _
ltD AvilfllHlty - ~c_
44
J -(--
8 j ((MON_
36 j
--0 18 22 0 42 2~
jll 4Jtbull
r 11H -middot- __ ~ -- I 1rA
I --- --J - 353 600 500 1000 806 00 -- -- --
8 J _
101 25
fj)
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH hoUGpoundNC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Emergency Response Platform - Microsoft
bull Constrained Resources ndash Staffing ndash Beds bull Critical Care bull Acute Care
ndash Equipment bull Ventilators bull PPE
ndash COVID-19 patients
20
UnclassifiedFor Public Use
WA HEALTH C) About - Steve
~ Homo
6-hiyenHiiii+MF _ _ a
KING
43 COVID JM1Q
267
55 CD IDlnn1bned
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Emergency Response Platform - Microsoft
bull Next Releasendash Long Term Care Facilitiesbull COVID-19 Impactsndash Positive Patientsndash Positive Health Care
Workers raquo of staff impacted
bull PPE availability
21
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
William Fales MD FACEP FAEMS Medical Director Division of EMS and Trauma Michigan Department of Health and Human Services
22 UnclassifiedFor Public Use
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michiganrsquos Healthcare Preparedness Program bull Michigan Department of Health and Human Services ndash Bureau of EMS Trauma and Preparedness
bull 8 Regional Healthcare Coalitions ndash Hospitals EMS LPH EM LTC Tribal Health ndash Regional Coordinator Assistant Coordinator
Medical Director (25 FTE) ndash Regional Medical Coordination Center bull Multi-Agency Coordination Center bull Statewide use of EMResource by hospitals EMS
23
UnclassifiedFor Public Use
p ror
~ SC ON5
Sault Ste Marie
N
bull
Huron
Madison Milwa uk ee Graed Rapids bull bull e bull ~ 3rnia
L~nsi~ g bull - It bull
bullbullbullbull bull bull bull bull De troi t
bull Glwcago bull bull bull
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Michigan COVID-19 bull bull
bull
First 2 cases ndash March 10 Asymmetric epidemiology ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
24
UnclassifiedFor Public Use
Barrie
Toronto
Hamilton
bull bull
bull
Lake Ontario
bull Ro~besterbull
bull
bull
Brockville bull Kingston
~~w voRK
bull bull bull
bull
bull Pt0NfV VAN1A bull
bull
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H I NfOR MATION GATEWAY
bull
bull bull ~ ba riy
bull bull
Michigan COVID-19 bull First 2 cases ndash March 10
Asymmetric epidemiology bull ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
bull Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
25
UnclassifiedFor Public Use
I I I I I I I I I I I I I
ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City COVID-19 Daily Hospital Admissions
New York City vs Detroit 1800 1600 1400 1200 1000 800 600 400 200 0
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 26
UnclassifiedFor Public Use ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City
1 1 I 11111 111 11 11 1111 1 II II 1 1 1
400
300
200
COVID-19 Daily Hospital Admissions Per 1 Million PopulationNew York City vs Detroit
40-Day Post-Outbreak Mortality bull NY City 646 deaths per million bull Detroit 919 deaths per million
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 27
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Goal bull Save lives and reduce pain and suffering by optimizing
the use of the statersquos healthcare resources ndash Extend conventional standards of care to as many
patients as possible ndash Minimize the need for crisis standards of care bull Especially while conventional capacity exists
28
UnclassifiedFor Public Use
--
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Components bull Relief Hospitals
bull Alternate Care Sites EMS
ndash Home Care Sites
ndash Relief Personnel
29
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals vs Alternate Care Sites bull Relief Hospitals The objective is to extend the
conventional standard of care to as many citizens in need as possible (ie minimize the need to move intocrisis standards of care)
bull Alternate Care Sites (ACS) The objective is to delivercrisis standards of care (as close to the conventional standard of care as possible) in extreme conditions in which the conventional standard of care can not be provided at overloaded hospitals
30
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital ldquoAskrdquo bull Hospitals have been previously asked to be able to
surge an additional 20 above average daily census ndash Increased to 50 ldquosuper surgerdquo
bull Relief Hospitals provide 10 of their expanded capacity to assist severely impacted hospitals ndash While preserving 50 of super-surge capacity bull Many hospitals at very low census
31
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals and Patient Redistribution
bull Intra-Health System Transfer ndash Coordinated by specific health system
bull Intra-Regional Transfer ndash Coordinated by Regional Medical Coordination Center
bull Statewide Transfer ndash Coordinated by Inter-Hospital Coordination Unit bull AKA Medical Operations Coordination Cell (MOCC)
32
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Statewide Inter-Hospital Coordination Unit State EmergencyOperations Center
Planning Finance Operations
Health Branch
Inter-HospitalCoordination Unit
Physician Consultant
EMS Coordination Group
Logistics
MDHHS Health Emergency Operations
Center
Medical Operations
Coordination Cell
33
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs and Patient Redistribution Regional Medical
Coordination Center bull Relief hospitals declare status on
EMResource bull RMCC receives request from
transferring hospital bull RMCC identifies Relief Hospital(s) bull Transferring hospital contacts
Relief Hospital directly bull Relief Hospital accepts patient(s) bull RMCC coordinates EMS PRN
Statewide Inter-Hospital Coordination Unit
Relief hospitals declare status on EMResource
IHCU receives request from RMCC on behalf of transferring hospital
IHCU identifies Relief Hospital(s) Transferring hospital contacts Relief
Hospital directly Relief Hospital accepts patient(s) IHCU coordinates EMS PRN
34
UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Steven Mitchell MD FACEP Medical Director Western Washington Regional COVID Coordination Center Medical Director Emergency Department Harborview Medical Center
12 UnclassifiedFor Public Use
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Western Washington MOCC
bull
bull
bull
First US COVID-19 case Jan 21ndash Snohomish County WA
First US COVID-19 death Feb 29ndash King County WA
First major outbreak late FebMarch1
ndash 167 cases at Long-Term Care Facilitybull 101 residents 50 staff and 16 visitorsbull 43 deaths
1 Epidemiology of Covid-19 in a Long-Term Care Facility in King County Washington N Engl J Med 2020 Mar 27
13
UnclassifiedFor Public Use
THE WALL STREET JOURNAL
One Nursing Home 35 Coronavirus Deaths Inside the Kirkland Disaster
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
King County LTCF Outbreak
~be ~cu Uork ~itnes
Its Pure Panic A Wrenching Wait at Nursing Home Where Coronavirus Took Hold Cut off from their relatives inside a virus-stricken nursing center families are frantically searching for help and basic information
14
UnclassifiedFor Public Use
Characteristics and Outcomes of 21 Critshyically Ill Patients With COVID-19 in Washshyington State Matt Arentz MD1 Eric Yim MD2 Lindy Klaff MD2 et al
Author Affiliations I Article Information
JAMA Published online March 19 2020 doi101001jama20204326
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Single LTCF - Single Hospital
bull Overwhelmed bull No coordination bull Not isolated example
15
UnclassifiedFor Public Use
~) NORTHWEST HEALTHCARE HARBORVIEW MEDICAL CENTER
UW Medicine [f]KingCounty
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Medical Operations Coordinating Cell
bull Disaster Medical Coordination Center
bull Regional COVID Coordination Center (RC3) ndash Harborview Medical CenterKing County ndash Northwest Health Response Network
16
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Regional COVID Coordinating Center ndash Western Washington
17
UnclassifiedFor Public Use
Staffing
Impacts
Resource
Impacts
Ventilators PPE
urveillance of Hospitals
Health
Surveillance of Congregant
Settings
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Two Surveillance Pillars of the RC3
18
UnclassifiedFor Public Use
Health System __-1
Level Loadin
ealth System
Coordination of Resources
ASPR AUIS1ANT bulllCUTtamp~ ~00
UIPAUDgt1111 ~gtIC UfPO~H HUtTHCdl h oUGpound NC1 HpoundhH0Npound~~
I NfORMAT IONGAIEWAf
Two Coordination Pillars of the RC3
19
UnclassifiedFor Public Use
WA HEALTH G) About f) Stevo Mltchell
E-- Home
Q~ _ (WIJ - _uw_ 0
COVIDbulllltl1-t1 ltD _
ltD _
ltD AvilfllHlty - ~c_
44
J -(--
8 j ((MON_
36 j
--0 18 22 0 42 2~
jll 4Jtbull
r 11H -middot- __ ~ -- I 1rA
I --- --J - 353 600 500 1000 806 00 -- -- --
8 J _
101 25
fj)
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH hoUGpoundNC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Emergency Response Platform - Microsoft
bull Constrained Resources ndash Staffing ndash Beds bull Critical Care bull Acute Care
ndash Equipment bull Ventilators bull PPE
ndash COVID-19 patients
20
UnclassifiedFor Public Use
WA HEALTH C) About - Steve
~ Homo
6-hiyenHiiii+MF _ _ a
KING
43 COVID JM1Q
267
55 CD IDlnn1bned
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Emergency Response Platform - Microsoft
bull Next Releasendash Long Term Care Facilitiesbull COVID-19 Impactsndash Positive Patientsndash Positive Health Care
Workers raquo of staff impacted
bull PPE availability
21
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
William Fales MD FACEP FAEMS Medical Director Division of EMS and Trauma Michigan Department of Health and Human Services
22 UnclassifiedFor Public Use
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michiganrsquos Healthcare Preparedness Program bull Michigan Department of Health and Human Services ndash Bureau of EMS Trauma and Preparedness
bull 8 Regional Healthcare Coalitions ndash Hospitals EMS LPH EM LTC Tribal Health ndash Regional Coordinator Assistant Coordinator
Medical Director (25 FTE) ndash Regional Medical Coordination Center bull Multi-Agency Coordination Center bull Statewide use of EMResource by hospitals EMS
23
UnclassifiedFor Public Use
p ror
~ SC ON5
Sault Ste Marie
N
bull
Huron
Madison Milwa uk ee Graed Rapids bull bull e bull ~ 3rnia
L~nsi~ g bull - It bull
bullbullbullbull bull bull bull bull De troi t
bull Glwcago bull bull bull
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Michigan COVID-19 bull bull
bull
First 2 cases ndash March 10 Asymmetric epidemiology ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
24
UnclassifiedFor Public Use
Barrie
Toronto
Hamilton
bull bull
bull
Lake Ontario
bull Ro~besterbull
bull
bull
Brockville bull Kingston
~~w voRK
bull bull bull
bull
bull Pt0NfV VAN1A bull
bull
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H I NfOR MATION GATEWAY
bull
bull bull ~ ba riy
bull bull
Michigan COVID-19 bull First 2 cases ndash March 10
Asymmetric epidemiology bull ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
bull Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
25
UnclassifiedFor Public Use
I I I I I I I I I I I I I
ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City COVID-19 Daily Hospital Admissions
New York City vs Detroit 1800 1600 1400 1200 1000 800 600 400 200 0
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 26
UnclassifiedFor Public Use ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City
1 1 I 11111 111 11 11 1111 1 II II 1 1 1
400
300
200
COVID-19 Daily Hospital Admissions Per 1 Million PopulationNew York City vs Detroit
40-Day Post-Outbreak Mortality bull NY City 646 deaths per million bull Detroit 919 deaths per million
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 27
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Goal bull Save lives and reduce pain and suffering by optimizing
the use of the statersquos healthcare resources ndash Extend conventional standards of care to as many
patients as possible ndash Minimize the need for crisis standards of care bull Especially while conventional capacity exists
28
UnclassifiedFor Public Use
--
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Components bull Relief Hospitals
bull Alternate Care Sites EMS
ndash Home Care Sites
ndash Relief Personnel
29
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals vs Alternate Care Sites bull Relief Hospitals The objective is to extend the
conventional standard of care to as many citizens in need as possible (ie minimize the need to move intocrisis standards of care)
bull Alternate Care Sites (ACS) The objective is to delivercrisis standards of care (as close to the conventional standard of care as possible) in extreme conditions in which the conventional standard of care can not be provided at overloaded hospitals
30
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital ldquoAskrdquo bull Hospitals have been previously asked to be able to
surge an additional 20 above average daily census ndash Increased to 50 ldquosuper surgerdquo
bull Relief Hospitals provide 10 of their expanded capacity to assist severely impacted hospitals ndash While preserving 50 of super-surge capacity bull Many hospitals at very low census
31
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals and Patient Redistribution
bull Intra-Health System Transfer ndash Coordinated by specific health system
bull Intra-Regional Transfer ndash Coordinated by Regional Medical Coordination Center
bull Statewide Transfer ndash Coordinated by Inter-Hospital Coordination Unit bull AKA Medical Operations Coordination Cell (MOCC)
32
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Statewide Inter-Hospital Coordination Unit State EmergencyOperations Center
Planning Finance Operations
Health Branch
Inter-HospitalCoordination Unit
Physician Consultant
EMS Coordination Group
Logistics
MDHHS Health Emergency Operations
Center
Medical Operations
Coordination Cell
33
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs and Patient Redistribution Regional Medical
Coordination Center bull Relief hospitals declare status on
EMResource bull RMCC receives request from
transferring hospital bull RMCC identifies Relief Hospital(s) bull Transferring hospital contacts
Relief Hospital directly bull Relief Hospital accepts patient(s) bull RMCC coordinates EMS PRN
Statewide Inter-Hospital Coordination Unit
Relief hospitals declare status on EMResource
IHCU receives request from RMCC on behalf of transferring hospital
IHCU identifies Relief Hospital(s) Transferring hospital contacts Relief
Hospital directly Relief Hospital accepts patient(s) IHCU coordinates EMS PRN
34
UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Western Washington MOCC
bull
bull
bull
First US COVID-19 case Jan 21ndash Snohomish County WA
First US COVID-19 death Feb 29ndash King County WA
First major outbreak late FebMarch1
ndash 167 cases at Long-Term Care Facilitybull 101 residents 50 staff and 16 visitorsbull 43 deaths
1 Epidemiology of Covid-19 in a Long-Term Care Facility in King County Washington N Engl J Med 2020 Mar 27
13
UnclassifiedFor Public Use
THE WALL STREET JOURNAL
One Nursing Home 35 Coronavirus Deaths Inside the Kirkland Disaster
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
King County LTCF Outbreak
~be ~cu Uork ~itnes
Its Pure Panic A Wrenching Wait at Nursing Home Where Coronavirus Took Hold Cut off from their relatives inside a virus-stricken nursing center families are frantically searching for help and basic information
14
UnclassifiedFor Public Use
Characteristics and Outcomes of 21 Critshyically Ill Patients With COVID-19 in Washshyington State Matt Arentz MD1 Eric Yim MD2 Lindy Klaff MD2 et al
Author Affiliations I Article Information
JAMA Published online March 19 2020 doi101001jama20204326
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Single LTCF - Single Hospital
bull Overwhelmed bull No coordination bull Not isolated example
15
UnclassifiedFor Public Use
~) NORTHWEST HEALTHCARE HARBORVIEW MEDICAL CENTER
UW Medicine [f]KingCounty
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Medical Operations Coordinating Cell
bull Disaster Medical Coordination Center
bull Regional COVID Coordination Center (RC3) ndash Harborview Medical CenterKing County ndash Northwest Health Response Network
16
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Regional COVID Coordinating Center ndash Western Washington
17
UnclassifiedFor Public Use
Staffing
Impacts
Resource
Impacts
Ventilators PPE
urveillance of Hospitals
Health
Surveillance of Congregant
Settings
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Two Surveillance Pillars of the RC3
18
UnclassifiedFor Public Use
Health System __-1
Level Loadin
ealth System
Coordination of Resources
ASPR AUIS1ANT bulllCUTtamp~ ~00
UIPAUDgt1111 ~gtIC UfPO~H HUtTHCdl h oUGpound NC1 HpoundhH0Npound~~
I NfORMAT IONGAIEWAf
Two Coordination Pillars of the RC3
19
UnclassifiedFor Public Use
WA HEALTH G) About f) Stevo Mltchell
E-- Home
Q~ _ (WIJ - _uw_ 0
COVIDbulllltl1-t1 ltD _
ltD _
ltD AvilfllHlty - ~c_
44
J -(--
8 j ((MON_
36 j
--0 18 22 0 42 2~
jll 4Jtbull
r 11H -middot- __ ~ -- I 1rA
I --- --J - 353 600 500 1000 806 00 -- -- --
8 J _
101 25
fj)
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH hoUGpoundNC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Emergency Response Platform - Microsoft
bull Constrained Resources ndash Staffing ndash Beds bull Critical Care bull Acute Care
ndash Equipment bull Ventilators bull PPE
ndash COVID-19 patients
20
UnclassifiedFor Public Use
WA HEALTH C) About - Steve
~ Homo
6-hiyenHiiii+MF _ _ a
KING
43 COVID JM1Q
267
55 CD IDlnn1bned
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Emergency Response Platform - Microsoft
bull Next Releasendash Long Term Care Facilitiesbull COVID-19 Impactsndash Positive Patientsndash Positive Health Care
Workers raquo of staff impacted
bull PPE availability
21
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
William Fales MD FACEP FAEMS Medical Director Division of EMS and Trauma Michigan Department of Health and Human Services
22 UnclassifiedFor Public Use
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michiganrsquos Healthcare Preparedness Program bull Michigan Department of Health and Human Services ndash Bureau of EMS Trauma and Preparedness
bull 8 Regional Healthcare Coalitions ndash Hospitals EMS LPH EM LTC Tribal Health ndash Regional Coordinator Assistant Coordinator
Medical Director (25 FTE) ndash Regional Medical Coordination Center bull Multi-Agency Coordination Center bull Statewide use of EMResource by hospitals EMS
23
UnclassifiedFor Public Use
p ror
~ SC ON5
Sault Ste Marie
N
bull
Huron
Madison Milwa uk ee Graed Rapids bull bull e bull ~ 3rnia
L~nsi~ g bull - It bull
bullbullbullbull bull bull bull bull De troi t
bull Glwcago bull bull bull
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Michigan COVID-19 bull bull
bull
First 2 cases ndash March 10 Asymmetric epidemiology ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
24
UnclassifiedFor Public Use
Barrie
Toronto
Hamilton
bull bull
bull
Lake Ontario
bull Ro~besterbull
bull
bull
Brockville bull Kingston
~~w voRK
bull bull bull
bull
bull Pt0NfV VAN1A bull
bull
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H I NfOR MATION GATEWAY
bull
bull bull ~ ba riy
bull bull
Michigan COVID-19 bull First 2 cases ndash March 10
Asymmetric epidemiology bull ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
bull Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
25
UnclassifiedFor Public Use
I I I I I I I I I I I I I
ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City COVID-19 Daily Hospital Admissions
New York City vs Detroit 1800 1600 1400 1200 1000 800 600 400 200 0
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 26
UnclassifiedFor Public Use ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City
1 1 I 11111 111 11 11 1111 1 II II 1 1 1
400
300
200
COVID-19 Daily Hospital Admissions Per 1 Million PopulationNew York City vs Detroit
40-Day Post-Outbreak Mortality bull NY City 646 deaths per million bull Detroit 919 deaths per million
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 27
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Goal bull Save lives and reduce pain and suffering by optimizing
the use of the statersquos healthcare resources ndash Extend conventional standards of care to as many
patients as possible ndash Minimize the need for crisis standards of care bull Especially while conventional capacity exists
28
UnclassifiedFor Public Use
--
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Components bull Relief Hospitals
bull Alternate Care Sites EMS
ndash Home Care Sites
ndash Relief Personnel
29
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals vs Alternate Care Sites bull Relief Hospitals The objective is to extend the
conventional standard of care to as many citizens in need as possible (ie minimize the need to move intocrisis standards of care)
bull Alternate Care Sites (ACS) The objective is to delivercrisis standards of care (as close to the conventional standard of care as possible) in extreme conditions in which the conventional standard of care can not be provided at overloaded hospitals
30
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital ldquoAskrdquo bull Hospitals have been previously asked to be able to
surge an additional 20 above average daily census ndash Increased to 50 ldquosuper surgerdquo
bull Relief Hospitals provide 10 of their expanded capacity to assist severely impacted hospitals ndash While preserving 50 of super-surge capacity bull Many hospitals at very low census
31
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals and Patient Redistribution
bull Intra-Health System Transfer ndash Coordinated by specific health system
bull Intra-Regional Transfer ndash Coordinated by Regional Medical Coordination Center
bull Statewide Transfer ndash Coordinated by Inter-Hospital Coordination Unit bull AKA Medical Operations Coordination Cell (MOCC)
32
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Statewide Inter-Hospital Coordination Unit State EmergencyOperations Center
Planning Finance Operations
Health Branch
Inter-HospitalCoordination Unit
Physician Consultant
EMS Coordination Group
Logistics
MDHHS Health Emergency Operations
Center
Medical Operations
Coordination Cell
33
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs and Patient Redistribution Regional Medical
Coordination Center bull Relief hospitals declare status on
EMResource bull RMCC receives request from
transferring hospital bull RMCC identifies Relief Hospital(s) bull Transferring hospital contacts
Relief Hospital directly bull Relief Hospital accepts patient(s) bull RMCC coordinates EMS PRN
Statewide Inter-Hospital Coordination Unit
Relief hospitals declare status on EMResource
IHCU receives request from RMCC on behalf of transferring hospital
IHCU identifies Relief Hospital(s) Transferring hospital contacts Relief
Hospital directly Relief Hospital accepts patient(s) IHCU coordinates EMS PRN
34
UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use
THE WALL STREET JOURNAL
One Nursing Home 35 Coronavirus Deaths Inside the Kirkland Disaster
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
King County LTCF Outbreak
~be ~cu Uork ~itnes
Its Pure Panic A Wrenching Wait at Nursing Home Where Coronavirus Took Hold Cut off from their relatives inside a virus-stricken nursing center families are frantically searching for help and basic information
14
UnclassifiedFor Public Use
Characteristics and Outcomes of 21 Critshyically Ill Patients With COVID-19 in Washshyington State Matt Arentz MD1 Eric Yim MD2 Lindy Klaff MD2 et al
Author Affiliations I Article Information
JAMA Published online March 19 2020 doi101001jama20204326
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Single LTCF - Single Hospital
bull Overwhelmed bull No coordination bull Not isolated example
15
UnclassifiedFor Public Use
~) NORTHWEST HEALTHCARE HARBORVIEW MEDICAL CENTER
UW Medicine [f]KingCounty
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Medical Operations Coordinating Cell
bull Disaster Medical Coordination Center
bull Regional COVID Coordination Center (RC3) ndash Harborview Medical CenterKing County ndash Northwest Health Response Network
16
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Regional COVID Coordinating Center ndash Western Washington
17
UnclassifiedFor Public Use
Staffing
Impacts
Resource
Impacts
Ventilators PPE
urveillance of Hospitals
Health
Surveillance of Congregant
Settings
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Two Surveillance Pillars of the RC3
18
UnclassifiedFor Public Use
Health System __-1
Level Loadin
ealth System
Coordination of Resources
ASPR AUIS1ANT bulllCUTtamp~ ~00
UIPAUDgt1111 ~gtIC UfPO~H HUtTHCdl h oUGpound NC1 HpoundhH0Npound~~
I NfORMAT IONGAIEWAf
Two Coordination Pillars of the RC3
19
UnclassifiedFor Public Use
WA HEALTH G) About f) Stevo Mltchell
E-- Home
Q~ _ (WIJ - _uw_ 0
COVIDbulllltl1-t1 ltD _
ltD _
ltD AvilfllHlty - ~c_
44
J -(--
8 j ((MON_
36 j
--0 18 22 0 42 2~
jll 4Jtbull
r 11H -middot- __ ~ -- I 1rA
I --- --J - 353 600 500 1000 806 00 -- -- --
8 J _
101 25
fj)
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH hoUGpoundNC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Emergency Response Platform - Microsoft
bull Constrained Resources ndash Staffing ndash Beds bull Critical Care bull Acute Care
ndash Equipment bull Ventilators bull PPE
ndash COVID-19 patients
20
UnclassifiedFor Public Use
WA HEALTH C) About - Steve
~ Homo
6-hiyenHiiii+MF _ _ a
KING
43 COVID JM1Q
267
55 CD IDlnn1bned
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Emergency Response Platform - Microsoft
bull Next Releasendash Long Term Care Facilitiesbull COVID-19 Impactsndash Positive Patientsndash Positive Health Care
Workers raquo of staff impacted
bull PPE availability
21
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
William Fales MD FACEP FAEMS Medical Director Division of EMS and Trauma Michigan Department of Health and Human Services
22 UnclassifiedFor Public Use
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michiganrsquos Healthcare Preparedness Program bull Michigan Department of Health and Human Services ndash Bureau of EMS Trauma and Preparedness
bull 8 Regional Healthcare Coalitions ndash Hospitals EMS LPH EM LTC Tribal Health ndash Regional Coordinator Assistant Coordinator
Medical Director (25 FTE) ndash Regional Medical Coordination Center bull Multi-Agency Coordination Center bull Statewide use of EMResource by hospitals EMS
23
UnclassifiedFor Public Use
p ror
~ SC ON5
Sault Ste Marie
N
bull
Huron
Madison Milwa uk ee Graed Rapids bull bull e bull ~ 3rnia
L~nsi~ g bull - It bull
bullbullbullbull bull bull bull bull De troi t
bull Glwcago bull bull bull
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Michigan COVID-19 bull bull
bull
First 2 cases ndash March 10 Asymmetric epidemiology ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
24
UnclassifiedFor Public Use
Barrie
Toronto
Hamilton
bull bull
bull
Lake Ontario
bull Ro~besterbull
bull
bull
Brockville bull Kingston
~~w voRK
bull bull bull
bull
bull Pt0NfV VAN1A bull
bull
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H I NfOR MATION GATEWAY
bull
bull bull ~ ba riy
bull bull
Michigan COVID-19 bull First 2 cases ndash March 10
Asymmetric epidemiology bull ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
bull Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
25
UnclassifiedFor Public Use
I I I I I I I I I I I I I
ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City COVID-19 Daily Hospital Admissions
New York City vs Detroit 1800 1600 1400 1200 1000 800 600 400 200 0
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 26
UnclassifiedFor Public Use ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City
1 1 I 11111 111 11 11 1111 1 II II 1 1 1
400
300
200
COVID-19 Daily Hospital Admissions Per 1 Million PopulationNew York City vs Detroit
40-Day Post-Outbreak Mortality bull NY City 646 deaths per million bull Detroit 919 deaths per million
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 27
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Goal bull Save lives and reduce pain and suffering by optimizing
the use of the statersquos healthcare resources ndash Extend conventional standards of care to as many
patients as possible ndash Minimize the need for crisis standards of care bull Especially while conventional capacity exists
28
UnclassifiedFor Public Use
--
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Components bull Relief Hospitals
bull Alternate Care Sites EMS
ndash Home Care Sites
ndash Relief Personnel
29
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals vs Alternate Care Sites bull Relief Hospitals The objective is to extend the
conventional standard of care to as many citizens in need as possible (ie minimize the need to move intocrisis standards of care)
bull Alternate Care Sites (ACS) The objective is to delivercrisis standards of care (as close to the conventional standard of care as possible) in extreme conditions in which the conventional standard of care can not be provided at overloaded hospitals
30
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital ldquoAskrdquo bull Hospitals have been previously asked to be able to
surge an additional 20 above average daily census ndash Increased to 50 ldquosuper surgerdquo
bull Relief Hospitals provide 10 of their expanded capacity to assist severely impacted hospitals ndash While preserving 50 of super-surge capacity bull Many hospitals at very low census
31
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals and Patient Redistribution
bull Intra-Health System Transfer ndash Coordinated by specific health system
bull Intra-Regional Transfer ndash Coordinated by Regional Medical Coordination Center
bull Statewide Transfer ndash Coordinated by Inter-Hospital Coordination Unit bull AKA Medical Operations Coordination Cell (MOCC)
32
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Statewide Inter-Hospital Coordination Unit State EmergencyOperations Center
Planning Finance Operations
Health Branch
Inter-HospitalCoordination Unit
Physician Consultant
EMS Coordination Group
Logistics
MDHHS Health Emergency Operations
Center
Medical Operations
Coordination Cell
33
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs and Patient Redistribution Regional Medical
Coordination Center bull Relief hospitals declare status on
EMResource bull RMCC receives request from
transferring hospital bull RMCC identifies Relief Hospital(s) bull Transferring hospital contacts
Relief Hospital directly bull Relief Hospital accepts patient(s) bull RMCC coordinates EMS PRN
Statewide Inter-Hospital Coordination Unit
Relief hospitals declare status on EMResource
IHCU receives request from RMCC on behalf of transferring hospital
IHCU identifies Relief Hospital(s) Transferring hospital contacts Relief
Hospital directly Relief Hospital accepts patient(s) IHCU coordinates EMS PRN
34
UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use
Characteristics and Outcomes of 21 Critshyically Ill Patients With COVID-19 in Washshyington State Matt Arentz MD1 Eric Yim MD2 Lindy Klaff MD2 et al
Author Affiliations I Article Information
JAMA Published online March 19 2020 doi101001jama20204326
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Single LTCF - Single Hospital
bull Overwhelmed bull No coordination bull Not isolated example
15
UnclassifiedFor Public Use
~) NORTHWEST HEALTHCARE HARBORVIEW MEDICAL CENTER
UW Medicine [f]KingCounty
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Medical Operations Coordinating Cell
bull Disaster Medical Coordination Center
bull Regional COVID Coordination Center (RC3) ndash Harborview Medical CenterKing County ndash Northwest Health Response Network
16
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Regional COVID Coordinating Center ndash Western Washington
17
UnclassifiedFor Public Use
Staffing
Impacts
Resource
Impacts
Ventilators PPE
urveillance of Hospitals
Health
Surveillance of Congregant
Settings
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Two Surveillance Pillars of the RC3
18
UnclassifiedFor Public Use
Health System __-1
Level Loadin
ealth System
Coordination of Resources
ASPR AUIS1ANT bulllCUTtamp~ ~00
UIPAUDgt1111 ~gtIC UfPO~H HUtTHCdl h oUGpound NC1 HpoundhH0Npound~~
I NfORMAT IONGAIEWAf
Two Coordination Pillars of the RC3
19
UnclassifiedFor Public Use
WA HEALTH G) About f) Stevo Mltchell
E-- Home
Q~ _ (WIJ - _uw_ 0
COVIDbulllltl1-t1 ltD _
ltD _
ltD AvilfllHlty - ~c_
44
J -(--
8 j ((MON_
36 j
--0 18 22 0 42 2~
jll 4Jtbull
r 11H -middot- __ ~ -- I 1rA
I --- --J - 353 600 500 1000 806 00 -- -- --
8 J _
101 25
fj)
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH hoUGpoundNC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Emergency Response Platform - Microsoft
bull Constrained Resources ndash Staffing ndash Beds bull Critical Care bull Acute Care
ndash Equipment bull Ventilators bull PPE
ndash COVID-19 patients
20
UnclassifiedFor Public Use
WA HEALTH C) About - Steve
~ Homo
6-hiyenHiiii+MF _ _ a
KING
43 COVID JM1Q
267
55 CD IDlnn1bned
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Emergency Response Platform - Microsoft
bull Next Releasendash Long Term Care Facilitiesbull COVID-19 Impactsndash Positive Patientsndash Positive Health Care
Workers raquo of staff impacted
bull PPE availability
21
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
William Fales MD FACEP FAEMS Medical Director Division of EMS and Trauma Michigan Department of Health and Human Services
22 UnclassifiedFor Public Use
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michiganrsquos Healthcare Preparedness Program bull Michigan Department of Health and Human Services ndash Bureau of EMS Trauma and Preparedness
bull 8 Regional Healthcare Coalitions ndash Hospitals EMS LPH EM LTC Tribal Health ndash Regional Coordinator Assistant Coordinator
Medical Director (25 FTE) ndash Regional Medical Coordination Center bull Multi-Agency Coordination Center bull Statewide use of EMResource by hospitals EMS
23
UnclassifiedFor Public Use
p ror
~ SC ON5
Sault Ste Marie
N
bull
Huron
Madison Milwa uk ee Graed Rapids bull bull e bull ~ 3rnia
L~nsi~ g bull - It bull
bullbullbullbull bull bull bull bull De troi t
bull Glwcago bull bull bull
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Michigan COVID-19 bull bull
bull
First 2 cases ndash March 10 Asymmetric epidemiology ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
24
UnclassifiedFor Public Use
Barrie
Toronto
Hamilton
bull bull
bull
Lake Ontario
bull Ro~besterbull
bull
bull
Brockville bull Kingston
~~w voRK
bull bull bull
bull
bull Pt0NfV VAN1A bull
bull
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H I NfOR MATION GATEWAY
bull
bull bull ~ ba riy
bull bull
Michigan COVID-19 bull First 2 cases ndash March 10
Asymmetric epidemiology bull ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
bull Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
25
UnclassifiedFor Public Use
I I I I I I I I I I I I I
ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City COVID-19 Daily Hospital Admissions
New York City vs Detroit 1800 1600 1400 1200 1000 800 600 400 200 0
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 26
UnclassifiedFor Public Use ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City
1 1 I 11111 111 11 11 1111 1 II II 1 1 1
400
300
200
COVID-19 Daily Hospital Admissions Per 1 Million PopulationNew York City vs Detroit
40-Day Post-Outbreak Mortality bull NY City 646 deaths per million bull Detroit 919 deaths per million
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 27
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Goal bull Save lives and reduce pain and suffering by optimizing
the use of the statersquos healthcare resources ndash Extend conventional standards of care to as many
patients as possible ndash Minimize the need for crisis standards of care bull Especially while conventional capacity exists
28
UnclassifiedFor Public Use
--
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Components bull Relief Hospitals
bull Alternate Care Sites EMS
ndash Home Care Sites
ndash Relief Personnel
29
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals vs Alternate Care Sites bull Relief Hospitals The objective is to extend the
conventional standard of care to as many citizens in need as possible (ie minimize the need to move intocrisis standards of care)
bull Alternate Care Sites (ACS) The objective is to delivercrisis standards of care (as close to the conventional standard of care as possible) in extreme conditions in which the conventional standard of care can not be provided at overloaded hospitals
30
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital ldquoAskrdquo bull Hospitals have been previously asked to be able to
surge an additional 20 above average daily census ndash Increased to 50 ldquosuper surgerdquo
bull Relief Hospitals provide 10 of their expanded capacity to assist severely impacted hospitals ndash While preserving 50 of super-surge capacity bull Many hospitals at very low census
31
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals and Patient Redistribution
bull Intra-Health System Transfer ndash Coordinated by specific health system
bull Intra-Regional Transfer ndash Coordinated by Regional Medical Coordination Center
bull Statewide Transfer ndash Coordinated by Inter-Hospital Coordination Unit bull AKA Medical Operations Coordination Cell (MOCC)
32
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Statewide Inter-Hospital Coordination Unit State EmergencyOperations Center
Planning Finance Operations
Health Branch
Inter-HospitalCoordination Unit
Physician Consultant
EMS Coordination Group
Logistics
MDHHS Health Emergency Operations
Center
Medical Operations
Coordination Cell
33
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs and Patient Redistribution Regional Medical
Coordination Center bull Relief hospitals declare status on
EMResource bull RMCC receives request from
transferring hospital bull RMCC identifies Relief Hospital(s) bull Transferring hospital contacts
Relief Hospital directly bull Relief Hospital accepts patient(s) bull RMCC coordinates EMS PRN
Statewide Inter-Hospital Coordination Unit
Relief hospitals declare status on EMResource
IHCU receives request from RMCC on behalf of transferring hospital
IHCU identifies Relief Hospital(s) Transferring hospital contacts Relief
Hospital directly Relief Hospital accepts patient(s) IHCU coordinates EMS PRN
34
UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use
~) NORTHWEST HEALTHCARE HARBORVIEW MEDICAL CENTER
UW Medicine [f]KingCounty
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Medical Operations Coordinating Cell
bull Disaster Medical Coordination Center
bull Regional COVID Coordination Center (RC3) ndash Harborview Medical CenterKing County ndash Northwest Health Response Network
16
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Regional COVID Coordinating Center ndash Western Washington
17
UnclassifiedFor Public Use
Staffing
Impacts
Resource
Impacts
Ventilators PPE
urveillance of Hospitals
Health
Surveillance of Congregant
Settings
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Two Surveillance Pillars of the RC3
18
UnclassifiedFor Public Use
Health System __-1
Level Loadin
ealth System
Coordination of Resources
ASPR AUIS1ANT bulllCUTtamp~ ~00
UIPAUDgt1111 ~gtIC UfPO~H HUtTHCdl h oUGpound NC1 HpoundhH0Npound~~
I NfORMAT IONGAIEWAf
Two Coordination Pillars of the RC3
19
UnclassifiedFor Public Use
WA HEALTH G) About f) Stevo Mltchell
E-- Home
Q~ _ (WIJ - _uw_ 0
COVIDbulllltl1-t1 ltD _
ltD _
ltD AvilfllHlty - ~c_
44
J -(--
8 j ((MON_
36 j
--0 18 22 0 42 2~
jll 4Jtbull
r 11H -middot- __ ~ -- I 1rA
I --- --J - 353 600 500 1000 806 00 -- -- --
8 J _
101 25
fj)
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH hoUGpoundNC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Emergency Response Platform - Microsoft
bull Constrained Resources ndash Staffing ndash Beds bull Critical Care bull Acute Care
ndash Equipment bull Ventilators bull PPE
ndash COVID-19 patients
20
UnclassifiedFor Public Use
WA HEALTH C) About - Steve
~ Homo
6-hiyenHiiii+MF _ _ a
KING
43 COVID JM1Q
267
55 CD IDlnn1bned
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Emergency Response Platform - Microsoft
bull Next Releasendash Long Term Care Facilitiesbull COVID-19 Impactsndash Positive Patientsndash Positive Health Care
Workers raquo of staff impacted
bull PPE availability
21
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
William Fales MD FACEP FAEMS Medical Director Division of EMS and Trauma Michigan Department of Health and Human Services
22 UnclassifiedFor Public Use
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michiganrsquos Healthcare Preparedness Program bull Michigan Department of Health and Human Services ndash Bureau of EMS Trauma and Preparedness
bull 8 Regional Healthcare Coalitions ndash Hospitals EMS LPH EM LTC Tribal Health ndash Regional Coordinator Assistant Coordinator
Medical Director (25 FTE) ndash Regional Medical Coordination Center bull Multi-Agency Coordination Center bull Statewide use of EMResource by hospitals EMS
23
UnclassifiedFor Public Use
p ror
~ SC ON5
Sault Ste Marie
N
bull
Huron
Madison Milwa uk ee Graed Rapids bull bull e bull ~ 3rnia
L~nsi~ g bull - It bull
bullbullbullbull bull bull bull bull De troi t
bull Glwcago bull bull bull
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Michigan COVID-19 bull bull
bull
First 2 cases ndash March 10 Asymmetric epidemiology ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
24
UnclassifiedFor Public Use
Barrie
Toronto
Hamilton
bull bull
bull
Lake Ontario
bull Ro~besterbull
bull
bull
Brockville bull Kingston
~~w voRK
bull bull bull
bull
bull Pt0NfV VAN1A bull
bull
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H I NfOR MATION GATEWAY
bull
bull bull ~ ba riy
bull bull
Michigan COVID-19 bull First 2 cases ndash March 10
Asymmetric epidemiology bull ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
bull Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
25
UnclassifiedFor Public Use
I I I I I I I I I I I I I
ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City COVID-19 Daily Hospital Admissions
New York City vs Detroit 1800 1600 1400 1200 1000 800 600 400 200 0
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 26
UnclassifiedFor Public Use ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City
1 1 I 11111 111 11 11 1111 1 II II 1 1 1
400
300
200
COVID-19 Daily Hospital Admissions Per 1 Million PopulationNew York City vs Detroit
40-Day Post-Outbreak Mortality bull NY City 646 deaths per million bull Detroit 919 deaths per million
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 27
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Goal bull Save lives and reduce pain and suffering by optimizing
the use of the statersquos healthcare resources ndash Extend conventional standards of care to as many
patients as possible ndash Minimize the need for crisis standards of care bull Especially while conventional capacity exists
28
UnclassifiedFor Public Use
--
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Components bull Relief Hospitals
bull Alternate Care Sites EMS
ndash Home Care Sites
ndash Relief Personnel
29
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals vs Alternate Care Sites bull Relief Hospitals The objective is to extend the
conventional standard of care to as many citizens in need as possible (ie minimize the need to move intocrisis standards of care)
bull Alternate Care Sites (ACS) The objective is to delivercrisis standards of care (as close to the conventional standard of care as possible) in extreme conditions in which the conventional standard of care can not be provided at overloaded hospitals
30
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital ldquoAskrdquo bull Hospitals have been previously asked to be able to
surge an additional 20 above average daily census ndash Increased to 50 ldquosuper surgerdquo
bull Relief Hospitals provide 10 of their expanded capacity to assist severely impacted hospitals ndash While preserving 50 of super-surge capacity bull Many hospitals at very low census
31
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals and Patient Redistribution
bull Intra-Health System Transfer ndash Coordinated by specific health system
bull Intra-Regional Transfer ndash Coordinated by Regional Medical Coordination Center
bull Statewide Transfer ndash Coordinated by Inter-Hospital Coordination Unit bull AKA Medical Operations Coordination Cell (MOCC)
32
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Statewide Inter-Hospital Coordination Unit State EmergencyOperations Center
Planning Finance Operations
Health Branch
Inter-HospitalCoordination Unit
Physician Consultant
EMS Coordination Group
Logistics
MDHHS Health Emergency Operations
Center
Medical Operations
Coordination Cell
33
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs and Patient Redistribution Regional Medical
Coordination Center bull Relief hospitals declare status on
EMResource bull RMCC receives request from
transferring hospital bull RMCC identifies Relief Hospital(s) bull Transferring hospital contacts
Relief Hospital directly bull Relief Hospital accepts patient(s) bull RMCC coordinates EMS PRN
Statewide Inter-Hospital Coordination Unit
Relief hospitals declare status on EMResource
IHCU receives request from RMCC on behalf of transferring hospital
IHCU identifies Relief Hospital(s) Transferring hospital contacts Relief
Hospital directly Relief Hospital accepts patient(s) IHCU coordinates EMS PRN
34
UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Regional COVID Coordinating Center ndash Western Washington
17
UnclassifiedFor Public Use
Staffing
Impacts
Resource
Impacts
Ventilators PPE
urveillance of Hospitals
Health
Surveillance of Congregant
Settings
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Two Surveillance Pillars of the RC3
18
UnclassifiedFor Public Use
Health System __-1
Level Loadin
ealth System
Coordination of Resources
ASPR AUIS1ANT bulllCUTtamp~ ~00
UIPAUDgt1111 ~gtIC UfPO~H HUtTHCdl h oUGpound NC1 HpoundhH0Npound~~
I NfORMAT IONGAIEWAf
Two Coordination Pillars of the RC3
19
UnclassifiedFor Public Use
WA HEALTH G) About f) Stevo Mltchell
E-- Home
Q~ _ (WIJ - _uw_ 0
COVIDbulllltl1-t1 ltD _
ltD _
ltD AvilfllHlty - ~c_
44
J -(--
8 j ((MON_
36 j
--0 18 22 0 42 2~
jll 4Jtbull
r 11H -middot- __ ~ -- I 1rA
I --- --J - 353 600 500 1000 806 00 -- -- --
8 J _
101 25
fj)
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH hoUGpoundNC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Emergency Response Platform - Microsoft
bull Constrained Resources ndash Staffing ndash Beds bull Critical Care bull Acute Care
ndash Equipment bull Ventilators bull PPE
ndash COVID-19 patients
20
UnclassifiedFor Public Use
WA HEALTH C) About - Steve
~ Homo
6-hiyenHiiii+MF _ _ a
KING
43 COVID JM1Q
267
55 CD IDlnn1bned
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Emergency Response Platform - Microsoft
bull Next Releasendash Long Term Care Facilitiesbull COVID-19 Impactsndash Positive Patientsndash Positive Health Care
Workers raquo of staff impacted
bull PPE availability
21
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
William Fales MD FACEP FAEMS Medical Director Division of EMS and Trauma Michigan Department of Health and Human Services
22 UnclassifiedFor Public Use
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michiganrsquos Healthcare Preparedness Program bull Michigan Department of Health and Human Services ndash Bureau of EMS Trauma and Preparedness
bull 8 Regional Healthcare Coalitions ndash Hospitals EMS LPH EM LTC Tribal Health ndash Regional Coordinator Assistant Coordinator
Medical Director (25 FTE) ndash Regional Medical Coordination Center bull Multi-Agency Coordination Center bull Statewide use of EMResource by hospitals EMS
23
UnclassifiedFor Public Use
p ror
~ SC ON5
Sault Ste Marie
N
bull
Huron
Madison Milwa uk ee Graed Rapids bull bull e bull ~ 3rnia
L~nsi~ g bull - It bull
bullbullbullbull bull bull bull bull De troi t
bull Glwcago bull bull bull
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Michigan COVID-19 bull bull
bull
First 2 cases ndash March 10 Asymmetric epidemiology ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
24
UnclassifiedFor Public Use
Barrie
Toronto
Hamilton
bull bull
bull
Lake Ontario
bull Ro~besterbull
bull
bull
Brockville bull Kingston
~~w voRK
bull bull bull
bull
bull Pt0NfV VAN1A bull
bull
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H I NfOR MATION GATEWAY
bull
bull bull ~ ba riy
bull bull
Michigan COVID-19 bull First 2 cases ndash March 10
Asymmetric epidemiology bull ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
bull Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
25
UnclassifiedFor Public Use
I I I I I I I I I I I I I
ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City COVID-19 Daily Hospital Admissions
New York City vs Detroit 1800 1600 1400 1200 1000 800 600 400 200 0
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 26
UnclassifiedFor Public Use ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City
1 1 I 11111 111 11 11 1111 1 II II 1 1 1
400
300
200
COVID-19 Daily Hospital Admissions Per 1 Million PopulationNew York City vs Detroit
40-Day Post-Outbreak Mortality bull NY City 646 deaths per million bull Detroit 919 deaths per million
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 27
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Goal bull Save lives and reduce pain and suffering by optimizing
the use of the statersquos healthcare resources ndash Extend conventional standards of care to as many
patients as possible ndash Minimize the need for crisis standards of care bull Especially while conventional capacity exists
28
UnclassifiedFor Public Use
--
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Components bull Relief Hospitals
bull Alternate Care Sites EMS
ndash Home Care Sites
ndash Relief Personnel
29
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals vs Alternate Care Sites bull Relief Hospitals The objective is to extend the
conventional standard of care to as many citizens in need as possible (ie minimize the need to move intocrisis standards of care)
bull Alternate Care Sites (ACS) The objective is to delivercrisis standards of care (as close to the conventional standard of care as possible) in extreme conditions in which the conventional standard of care can not be provided at overloaded hospitals
30
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital ldquoAskrdquo bull Hospitals have been previously asked to be able to
surge an additional 20 above average daily census ndash Increased to 50 ldquosuper surgerdquo
bull Relief Hospitals provide 10 of their expanded capacity to assist severely impacted hospitals ndash While preserving 50 of super-surge capacity bull Many hospitals at very low census
31
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals and Patient Redistribution
bull Intra-Health System Transfer ndash Coordinated by specific health system
bull Intra-Regional Transfer ndash Coordinated by Regional Medical Coordination Center
bull Statewide Transfer ndash Coordinated by Inter-Hospital Coordination Unit bull AKA Medical Operations Coordination Cell (MOCC)
32
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Statewide Inter-Hospital Coordination Unit State EmergencyOperations Center
Planning Finance Operations
Health Branch
Inter-HospitalCoordination Unit
Physician Consultant
EMS Coordination Group
Logistics
MDHHS Health Emergency Operations
Center
Medical Operations
Coordination Cell
33
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs and Patient Redistribution Regional Medical
Coordination Center bull Relief hospitals declare status on
EMResource bull RMCC receives request from
transferring hospital bull RMCC identifies Relief Hospital(s) bull Transferring hospital contacts
Relief Hospital directly bull Relief Hospital accepts patient(s) bull RMCC coordinates EMS PRN
Statewide Inter-Hospital Coordination Unit
Relief hospitals declare status on EMResource
IHCU receives request from RMCC on behalf of transferring hospital
IHCU identifies Relief Hospital(s) Transferring hospital contacts Relief
Hospital directly Relief Hospital accepts patient(s) IHCU coordinates EMS PRN
34
UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use
Staffing
Impacts
Resource
Impacts
Ventilators PPE
urveillance of Hospitals
Health
Surveillance of Congregant
Settings
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Two Surveillance Pillars of the RC3
18
UnclassifiedFor Public Use
Health System __-1
Level Loadin
ealth System
Coordination of Resources
ASPR AUIS1ANT bulllCUTtamp~ ~00
UIPAUDgt1111 ~gtIC UfPO~H HUtTHCdl h oUGpound NC1 HpoundhH0Npound~~
I NfORMAT IONGAIEWAf
Two Coordination Pillars of the RC3
19
UnclassifiedFor Public Use
WA HEALTH G) About f) Stevo Mltchell
E-- Home
Q~ _ (WIJ - _uw_ 0
COVIDbulllltl1-t1 ltD _
ltD _
ltD AvilfllHlty - ~c_
44
J -(--
8 j ((MON_
36 j
--0 18 22 0 42 2~
jll 4Jtbull
r 11H -middot- __ ~ -- I 1rA
I --- --J - 353 600 500 1000 806 00 -- -- --
8 J _
101 25
fj)
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH hoUGpoundNC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Emergency Response Platform - Microsoft
bull Constrained Resources ndash Staffing ndash Beds bull Critical Care bull Acute Care
ndash Equipment bull Ventilators bull PPE
ndash COVID-19 patients
20
UnclassifiedFor Public Use
WA HEALTH C) About - Steve
~ Homo
6-hiyenHiiii+MF _ _ a
KING
43 COVID JM1Q
267
55 CD IDlnn1bned
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Emergency Response Platform - Microsoft
bull Next Releasendash Long Term Care Facilitiesbull COVID-19 Impactsndash Positive Patientsndash Positive Health Care
Workers raquo of staff impacted
bull PPE availability
21
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
William Fales MD FACEP FAEMS Medical Director Division of EMS and Trauma Michigan Department of Health and Human Services
22 UnclassifiedFor Public Use
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michiganrsquos Healthcare Preparedness Program bull Michigan Department of Health and Human Services ndash Bureau of EMS Trauma and Preparedness
bull 8 Regional Healthcare Coalitions ndash Hospitals EMS LPH EM LTC Tribal Health ndash Regional Coordinator Assistant Coordinator
Medical Director (25 FTE) ndash Regional Medical Coordination Center bull Multi-Agency Coordination Center bull Statewide use of EMResource by hospitals EMS
23
UnclassifiedFor Public Use
p ror
~ SC ON5
Sault Ste Marie
N
bull
Huron
Madison Milwa uk ee Graed Rapids bull bull e bull ~ 3rnia
L~nsi~ g bull - It bull
bullbullbullbull bull bull bull bull De troi t
bull Glwcago bull bull bull
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Michigan COVID-19 bull bull
bull
First 2 cases ndash March 10 Asymmetric epidemiology ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
24
UnclassifiedFor Public Use
Barrie
Toronto
Hamilton
bull bull
bull
Lake Ontario
bull Ro~besterbull
bull
bull
Brockville bull Kingston
~~w voRK
bull bull bull
bull
bull Pt0NfV VAN1A bull
bull
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H I NfOR MATION GATEWAY
bull
bull bull ~ ba riy
bull bull
Michigan COVID-19 bull First 2 cases ndash March 10
Asymmetric epidemiology bull ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
bull Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
25
UnclassifiedFor Public Use
I I I I I I I I I I I I I
ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City COVID-19 Daily Hospital Admissions
New York City vs Detroit 1800 1600 1400 1200 1000 800 600 400 200 0
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 26
UnclassifiedFor Public Use ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City
1 1 I 11111 111 11 11 1111 1 II II 1 1 1
400
300
200
COVID-19 Daily Hospital Admissions Per 1 Million PopulationNew York City vs Detroit
40-Day Post-Outbreak Mortality bull NY City 646 deaths per million bull Detroit 919 deaths per million
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 27
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Goal bull Save lives and reduce pain and suffering by optimizing
the use of the statersquos healthcare resources ndash Extend conventional standards of care to as many
patients as possible ndash Minimize the need for crisis standards of care bull Especially while conventional capacity exists
28
UnclassifiedFor Public Use
--
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Components bull Relief Hospitals
bull Alternate Care Sites EMS
ndash Home Care Sites
ndash Relief Personnel
29
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals vs Alternate Care Sites bull Relief Hospitals The objective is to extend the
conventional standard of care to as many citizens in need as possible (ie minimize the need to move intocrisis standards of care)
bull Alternate Care Sites (ACS) The objective is to delivercrisis standards of care (as close to the conventional standard of care as possible) in extreme conditions in which the conventional standard of care can not be provided at overloaded hospitals
30
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital ldquoAskrdquo bull Hospitals have been previously asked to be able to
surge an additional 20 above average daily census ndash Increased to 50 ldquosuper surgerdquo
bull Relief Hospitals provide 10 of their expanded capacity to assist severely impacted hospitals ndash While preserving 50 of super-surge capacity bull Many hospitals at very low census
31
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals and Patient Redistribution
bull Intra-Health System Transfer ndash Coordinated by specific health system
bull Intra-Regional Transfer ndash Coordinated by Regional Medical Coordination Center
bull Statewide Transfer ndash Coordinated by Inter-Hospital Coordination Unit bull AKA Medical Operations Coordination Cell (MOCC)
32
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Statewide Inter-Hospital Coordination Unit State EmergencyOperations Center
Planning Finance Operations
Health Branch
Inter-HospitalCoordination Unit
Physician Consultant
EMS Coordination Group
Logistics
MDHHS Health Emergency Operations
Center
Medical Operations
Coordination Cell
33
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs and Patient Redistribution Regional Medical
Coordination Center bull Relief hospitals declare status on
EMResource bull RMCC receives request from
transferring hospital bull RMCC identifies Relief Hospital(s) bull Transferring hospital contacts
Relief Hospital directly bull Relief Hospital accepts patient(s) bull RMCC coordinates EMS PRN
Statewide Inter-Hospital Coordination Unit
Relief hospitals declare status on EMResource
IHCU receives request from RMCC on behalf of transferring hospital
IHCU identifies Relief Hospital(s) Transferring hospital contacts Relief
Hospital directly Relief Hospital accepts patient(s) IHCU coordinates EMS PRN
34
UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use
Health System __-1
Level Loadin
ealth System
Coordination of Resources
ASPR AUIS1ANT bulllCUTtamp~ ~00
UIPAUDgt1111 ~gtIC UfPO~H HUtTHCdl h oUGpound NC1 HpoundhH0Npound~~
I NfORMAT IONGAIEWAf
Two Coordination Pillars of the RC3
19
UnclassifiedFor Public Use
WA HEALTH G) About f) Stevo Mltchell
E-- Home
Q~ _ (WIJ - _uw_ 0
COVIDbulllltl1-t1 ltD _
ltD _
ltD AvilfllHlty - ~c_
44
J -(--
8 j ((MON_
36 j
--0 18 22 0 42 2~
jll 4Jtbull
r 11H -middot- __ ~ -- I 1rA
I --- --J - 353 600 500 1000 806 00 -- -- --
8 J _
101 25
fj)
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH hoUGpoundNC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Emergency Response Platform - Microsoft
bull Constrained Resources ndash Staffing ndash Beds bull Critical Care bull Acute Care
ndash Equipment bull Ventilators bull PPE
ndash COVID-19 patients
20
UnclassifiedFor Public Use
WA HEALTH C) About - Steve
~ Homo
6-hiyenHiiii+MF _ _ a
KING
43 COVID JM1Q
267
55 CD IDlnn1bned
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Emergency Response Platform - Microsoft
bull Next Releasendash Long Term Care Facilitiesbull COVID-19 Impactsndash Positive Patientsndash Positive Health Care
Workers raquo of staff impacted
bull PPE availability
21
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
William Fales MD FACEP FAEMS Medical Director Division of EMS and Trauma Michigan Department of Health and Human Services
22 UnclassifiedFor Public Use
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michiganrsquos Healthcare Preparedness Program bull Michigan Department of Health and Human Services ndash Bureau of EMS Trauma and Preparedness
bull 8 Regional Healthcare Coalitions ndash Hospitals EMS LPH EM LTC Tribal Health ndash Regional Coordinator Assistant Coordinator
Medical Director (25 FTE) ndash Regional Medical Coordination Center bull Multi-Agency Coordination Center bull Statewide use of EMResource by hospitals EMS
23
UnclassifiedFor Public Use
p ror
~ SC ON5
Sault Ste Marie
N
bull
Huron
Madison Milwa uk ee Graed Rapids bull bull e bull ~ 3rnia
L~nsi~ g bull - It bull
bullbullbullbull bull bull bull bull De troi t
bull Glwcago bull bull bull
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Michigan COVID-19 bull bull
bull
First 2 cases ndash March 10 Asymmetric epidemiology ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
24
UnclassifiedFor Public Use
Barrie
Toronto
Hamilton
bull bull
bull
Lake Ontario
bull Ro~besterbull
bull
bull
Brockville bull Kingston
~~w voRK
bull bull bull
bull
bull Pt0NfV VAN1A bull
bull
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H I NfOR MATION GATEWAY
bull
bull bull ~ ba riy
bull bull
Michigan COVID-19 bull First 2 cases ndash March 10
Asymmetric epidemiology bull ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
bull Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
25
UnclassifiedFor Public Use
I I I I I I I I I I I I I
ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City COVID-19 Daily Hospital Admissions
New York City vs Detroit 1800 1600 1400 1200 1000 800 600 400 200 0
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 26
UnclassifiedFor Public Use ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City
1 1 I 11111 111 11 11 1111 1 II II 1 1 1
400
300
200
COVID-19 Daily Hospital Admissions Per 1 Million PopulationNew York City vs Detroit
40-Day Post-Outbreak Mortality bull NY City 646 deaths per million bull Detroit 919 deaths per million
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 27
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Goal bull Save lives and reduce pain and suffering by optimizing
the use of the statersquos healthcare resources ndash Extend conventional standards of care to as many
patients as possible ndash Minimize the need for crisis standards of care bull Especially while conventional capacity exists
28
UnclassifiedFor Public Use
--
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Components bull Relief Hospitals
bull Alternate Care Sites EMS
ndash Home Care Sites
ndash Relief Personnel
29
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals vs Alternate Care Sites bull Relief Hospitals The objective is to extend the
conventional standard of care to as many citizens in need as possible (ie minimize the need to move intocrisis standards of care)
bull Alternate Care Sites (ACS) The objective is to delivercrisis standards of care (as close to the conventional standard of care as possible) in extreme conditions in which the conventional standard of care can not be provided at overloaded hospitals
30
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital ldquoAskrdquo bull Hospitals have been previously asked to be able to
surge an additional 20 above average daily census ndash Increased to 50 ldquosuper surgerdquo
bull Relief Hospitals provide 10 of their expanded capacity to assist severely impacted hospitals ndash While preserving 50 of super-surge capacity bull Many hospitals at very low census
31
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals and Patient Redistribution
bull Intra-Health System Transfer ndash Coordinated by specific health system
bull Intra-Regional Transfer ndash Coordinated by Regional Medical Coordination Center
bull Statewide Transfer ndash Coordinated by Inter-Hospital Coordination Unit bull AKA Medical Operations Coordination Cell (MOCC)
32
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Statewide Inter-Hospital Coordination Unit State EmergencyOperations Center
Planning Finance Operations
Health Branch
Inter-HospitalCoordination Unit
Physician Consultant
EMS Coordination Group
Logistics
MDHHS Health Emergency Operations
Center
Medical Operations
Coordination Cell
33
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs and Patient Redistribution Regional Medical
Coordination Center bull Relief hospitals declare status on
EMResource bull RMCC receives request from
transferring hospital bull RMCC identifies Relief Hospital(s) bull Transferring hospital contacts
Relief Hospital directly bull Relief Hospital accepts patient(s) bull RMCC coordinates EMS PRN
Statewide Inter-Hospital Coordination Unit
Relief hospitals declare status on EMResource
IHCU receives request from RMCC on behalf of transferring hospital
IHCU identifies Relief Hospital(s) Transferring hospital contacts Relief
Hospital directly Relief Hospital accepts patient(s) IHCU coordinates EMS PRN
34
UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use
WA HEALTH G) About f) Stevo Mltchell
E-- Home
Q~ _ (WIJ - _uw_ 0
COVIDbulllltl1-t1 ltD _
ltD _
ltD AvilfllHlty - ~c_
44
J -(--
8 j ((MON_
36 j
--0 18 22 0 42 2~
jll 4Jtbull
r 11H -middot- __ ~ -- I 1rA
I --- --J - 353 600 500 1000 806 00 -- -- --
8 J _
101 25
fj)
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH hoUGpoundNC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Emergency Response Platform - Microsoft
bull Constrained Resources ndash Staffing ndash Beds bull Critical Care bull Acute Care
ndash Equipment bull Ventilators bull PPE
ndash COVID-19 patients
20
UnclassifiedFor Public Use
WA HEALTH C) About - Steve
~ Homo
6-hiyenHiiii+MF _ _ a
KING
43 COVID JM1Q
267
55 CD IDlnn1bned
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Emergency Response Platform - Microsoft
bull Next Releasendash Long Term Care Facilitiesbull COVID-19 Impactsndash Positive Patientsndash Positive Health Care
Workers raquo of staff impacted
bull PPE availability
21
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
William Fales MD FACEP FAEMS Medical Director Division of EMS and Trauma Michigan Department of Health and Human Services
22 UnclassifiedFor Public Use
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michiganrsquos Healthcare Preparedness Program bull Michigan Department of Health and Human Services ndash Bureau of EMS Trauma and Preparedness
bull 8 Regional Healthcare Coalitions ndash Hospitals EMS LPH EM LTC Tribal Health ndash Regional Coordinator Assistant Coordinator
Medical Director (25 FTE) ndash Regional Medical Coordination Center bull Multi-Agency Coordination Center bull Statewide use of EMResource by hospitals EMS
23
UnclassifiedFor Public Use
p ror
~ SC ON5
Sault Ste Marie
N
bull
Huron
Madison Milwa uk ee Graed Rapids bull bull e bull ~ 3rnia
L~nsi~ g bull - It bull
bullbullbullbull bull bull bull bull De troi t
bull Glwcago bull bull bull
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Michigan COVID-19 bull bull
bull
First 2 cases ndash March 10 Asymmetric epidemiology ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
24
UnclassifiedFor Public Use
Barrie
Toronto
Hamilton
bull bull
bull
Lake Ontario
bull Ro~besterbull
bull
bull
Brockville bull Kingston
~~w voRK
bull bull bull
bull
bull Pt0NfV VAN1A bull
bull
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H I NfOR MATION GATEWAY
bull
bull bull ~ ba riy
bull bull
Michigan COVID-19 bull First 2 cases ndash March 10
Asymmetric epidemiology bull ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
bull Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
25
UnclassifiedFor Public Use
I I I I I I I I I I I I I
ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City COVID-19 Daily Hospital Admissions
New York City vs Detroit 1800 1600 1400 1200 1000 800 600 400 200 0
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 26
UnclassifiedFor Public Use ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City
1 1 I 11111 111 11 11 1111 1 II II 1 1 1
400
300
200
COVID-19 Daily Hospital Admissions Per 1 Million PopulationNew York City vs Detroit
40-Day Post-Outbreak Mortality bull NY City 646 deaths per million bull Detroit 919 deaths per million
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 27
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Goal bull Save lives and reduce pain and suffering by optimizing
the use of the statersquos healthcare resources ndash Extend conventional standards of care to as many
patients as possible ndash Minimize the need for crisis standards of care bull Especially while conventional capacity exists
28
UnclassifiedFor Public Use
--
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Components bull Relief Hospitals
bull Alternate Care Sites EMS
ndash Home Care Sites
ndash Relief Personnel
29
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals vs Alternate Care Sites bull Relief Hospitals The objective is to extend the
conventional standard of care to as many citizens in need as possible (ie minimize the need to move intocrisis standards of care)
bull Alternate Care Sites (ACS) The objective is to delivercrisis standards of care (as close to the conventional standard of care as possible) in extreme conditions in which the conventional standard of care can not be provided at overloaded hospitals
30
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital ldquoAskrdquo bull Hospitals have been previously asked to be able to
surge an additional 20 above average daily census ndash Increased to 50 ldquosuper surgerdquo
bull Relief Hospitals provide 10 of their expanded capacity to assist severely impacted hospitals ndash While preserving 50 of super-surge capacity bull Many hospitals at very low census
31
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals and Patient Redistribution
bull Intra-Health System Transfer ndash Coordinated by specific health system
bull Intra-Regional Transfer ndash Coordinated by Regional Medical Coordination Center
bull Statewide Transfer ndash Coordinated by Inter-Hospital Coordination Unit bull AKA Medical Operations Coordination Cell (MOCC)
32
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Statewide Inter-Hospital Coordination Unit State EmergencyOperations Center
Planning Finance Operations
Health Branch
Inter-HospitalCoordination Unit
Physician Consultant
EMS Coordination Group
Logistics
MDHHS Health Emergency Operations
Center
Medical Operations
Coordination Cell
33
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs and Patient Redistribution Regional Medical
Coordination Center bull Relief hospitals declare status on
EMResource bull RMCC receives request from
transferring hospital bull RMCC identifies Relief Hospital(s) bull Transferring hospital contacts
Relief Hospital directly bull Relief Hospital accepts patient(s) bull RMCC coordinates EMS PRN
Statewide Inter-Hospital Coordination Unit
Relief hospitals declare status on EMResource
IHCU receives request from RMCC on behalf of transferring hospital
IHCU identifies Relief Hospital(s) Transferring hospital contacts Relief
Hospital directly Relief Hospital accepts patient(s) IHCU coordinates EMS PRN
34
UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use
WA HEALTH C) About - Steve
~ Homo
6-hiyenHiiii+MF _ _ a
KING
43 COVID JM1Q
267
55 CD IDlnn1bned
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Emergency Response Platform - Microsoft
bull Next Releasendash Long Term Care Facilitiesbull COVID-19 Impactsndash Positive Patientsndash Positive Health Care
Workers raquo of staff impacted
bull PPE availability
21
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
William Fales MD FACEP FAEMS Medical Director Division of EMS and Trauma Michigan Department of Health and Human Services
22 UnclassifiedFor Public Use
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michiganrsquos Healthcare Preparedness Program bull Michigan Department of Health and Human Services ndash Bureau of EMS Trauma and Preparedness
bull 8 Regional Healthcare Coalitions ndash Hospitals EMS LPH EM LTC Tribal Health ndash Regional Coordinator Assistant Coordinator
Medical Director (25 FTE) ndash Regional Medical Coordination Center bull Multi-Agency Coordination Center bull Statewide use of EMResource by hospitals EMS
23
UnclassifiedFor Public Use
p ror
~ SC ON5
Sault Ste Marie
N
bull
Huron
Madison Milwa uk ee Graed Rapids bull bull e bull ~ 3rnia
L~nsi~ g bull - It bull
bullbullbullbull bull bull bull bull De troi t
bull Glwcago bull bull bull
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Michigan COVID-19 bull bull
bull
First 2 cases ndash March 10 Asymmetric epidemiology ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
24
UnclassifiedFor Public Use
Barrie
Toronto
Hamilton
bull bull
bull
Lake Ontario
bull Ro~besterbull
bull
bull
Brockville bull Kingston
~~w voRK
bull bull bull
bull
bull Pt0NfV VAN1A bull
bull
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H I NfOR MATION GATEWAY
bull
bull bull ~ ba riy
bull bull
Michigan COVID-19 bull First 2 cases ndash March 10
Asymmetric epidemiology bull ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
bull Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
25
UnclassifiedFor Public Use
I I I I I I I I I I I I I
ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City COVID-19 Daily Hospital Admissions
New York City vs Detroit 1800 1600 1400 1200 1000 800 600 400 200 0
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 26
UnclassifiedFor Public Use ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City
1 1 I 11111 111 11 11 1111 1 II II 1 1 1
400
300
200
COVID-19 Daily Hospital Admissions Per 1 Million PopulationNew York City vs Detroit
40-Day Post-Outbreak Mortality bull NY City 646 deaths per million bull Detroit 919 deaths per million
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 27
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Goal bull Save lives and reduce pain and suffering by optimizing
the use of the statersquos healthcare resources ndash Extend conventional standards of care to as many
patients as possible ndash Minimize the need for crisis standards of care bull Especially while conventional capacity exists
28
UnclassifiedFor Public Use
--
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Components bull Relief Hospitals
bull Alternate Care Sites EMS
ndash Home Care Sites
ndash Relief Personnel
29
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals vs Alternate Care Sites bull Relief Hospitals The objective is to extend the
conventional standard of care to as many citizens in need as possible (ie minimize the need to move intocrisis standards of care)
bull Alternate Care Sites (ACS) The objective is to delivercrisis standards of care (as close to the conventional standard of care as possible) in extreme conditions in which the conventional standard of care can not be provided at overloaded hospitals
30
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital ldquoAskrdquo bull Hospitals have been previously asked to be able to
surge an additional 20 above average daily census ndash Increased to 50 ldquosuper surgerdquo
bull Relief Hospitals provide 10 of their expanded capacity to assist severely impacted hospitals ndash While preserving 50 of super-surge capacity bull Many hospitals at very low census
31
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals and Patient Redistribution
bull Intra-Health System Transfer ndash Coordinated by specific health system
bull Intra-Regional Transfer ndash Coordinated by Regional Medical Coordination Center
bull Statewide Transfer ndash Coordinated by Inter-Hospital Coordination Unit bull AKA Medical Operations Coordination Cell (MOCC)
32
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Statewide Inter-Hospital Coordination Unit State EmergencyOperations Center
Planning Finance Operations
Health Branch
Inter-HospitalCoordination Unit
Physician Consultant
EMS Coordination Group
Logistics
MDHHS Health Emergency Operations
Center
Medical Operations
Coordination Cell
33
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs and Patient Redistribution Regional Medical
Coordination Center bull Relief hospitals declare status on
EMResource bull RMCC receives request from
transferring hospital bull RMCC identifies Relief Hospital(s) bull Transferring hospital contacts
Relief Hospital directly bull Relief Hospital accepts patient(s) bull RMCC coordinates EMS PRN
Statewide Inter-Hospital Coordination Unit
Relief hospitals declare status on EMResource
IHCU receives request from RMCC on behalf of transferring hospital
IHCU identifies Relief Hospital(s) Transferring hospital contacts Relief
Hospital directly Relief Hospital accepts patient(s) IHCU coordinates EMS PRN
34
UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
William Fales MD FACEP FAEMS Medical Director Division of EMS and Trauma Michigan Department of Health and Human Services
22 UnclassifiedFor Public Use
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michiganrsquos Healthcare Preparedness Program bull Michigan Department of Health and Human Services ndash Bureau of EMS Trauma and Preparedness
bull 8 Regional Healthcare Coalitions ndash Hospitals EMS LPH EM LTC Tribal Health ndash Regional Coordinator Assistant Coordinator
Medical Director (25 FTE) ndash Regional Medical Coordination Center bull Multi-Agency Coordination Center bull Statewide use of EMResource by hospitals EMS
23
UnclassifiedFor Public Use
p ror
~ SC ON5
Sault Ste Marie
N
bull
Huron
Madison Milwa uk ee Graed Rapids bull bull e bull ~ 3rnia
L~nsi~ g bull - It bull
bullbullbullbull bull bull bull bull De troi t
bull Glwcago bull bull bull
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Michigan COVID-19 bull bull
bull
First 2 cases ndash March 10 Asymmetric epidemiology ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
24
UnclassifiedFor Public Use
Barrie
Toronto
Hamilton
bull bull
bull
Lake Ontario
bull Ro~besterbull
bull
bull
Brockville bull Kingston
~~w voRK
bull bull bull
bull
bull Pt0NfV VAN1A bull
bull
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H I NfOR MATION GATEWAY
bull
bull bull ~ ba riy
bull bull
Michigan COVID-19 bull First 2 cases ndash March 10
Asymmetric epidemiology bull ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
bull Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
25
UnclassifiedFor Public Use
I I I I I I I I I I I I I
ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City COVID-19 Daily Hospital Admissions
New York City vs Detroit 1800 1600 1400 1200 1000 800 600 400 200 0
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 26
UnclassifiedFor Public Use ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City
1 1 I 11111 111 11 11 1111 1 II II 1 1 1
400
300
200
COVID-19 Daily Hospital Admissions Per 1 Million PopulationNew York City vs Detroit
40-Day Post-Outbreak Mortality bull NY City 646 deaths per million bull Detroit 919 deaths per million
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 27
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Goal bull Save lives and reduce pain and suffering by optimizing
the use of the statersquos healthcare resources ndash Extend conventional standards of care to as many
patients as possible ndash Minimize the need for crisis standards of care bull Especially while conventional capacity exists
28
UnclassifiedFor Public Use
--
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Components bull Relief Hospitals
bull Alternate Care Sites EMS
ndash Home Care Sites
ndash Relief Personnel
29
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals vs Alternate Care Sites bull Relief Hospitals The objective is to extend the
conventional standard of care to as many citizens in need as possible (ie minimize the need to move intocrisis standards of care)
bull Alternate Care Sites (ACS) The objective is to delivercrisis standards of care (as close to the conventional standard of care as possible) in extreme conditions in which the conventional standard of care can not be provided at overloaded hospitals
30
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital ldquoAskrdquo bull Hospitals have been previously asked to be able to
surge an additional 20 above average daily census ndash Increased to 50 ldquosuper surgerdquo
bull Relief Hospitals provide 10 of their expanded capacity to assist severely impacted hospitals ndash While preserving 50 of super-surge capacity bull Many hospitals at very low census
31
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals and Patient Redistribution
bull Intra-Health System Transfer ndash Coordinated by specific health system
bull Intra-Regional Transfer ndash Coordinated by Regional Medical Coordination Center
bull Statewide Transfer ndash Coordinated by Inter-Hospital Coordination Unit bull AKA Medical Operations Coordination Cell (MOCC)
32
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Statewide Inter-Hospital Coordination Unit State EmergencyOperations Center
Planning Finance Operations
Health Branch
Inter-HospitalCoordination Unit
Physician Consultant
EMS Coordination Group
Logistics
MDHHS Health Emergency Operations
Center
Medical Operations
Coordination Cell
33
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs and Patient Redistribution Regional Medical
Coordination Center bull Relief hospitals declare status on
EMResource bull RMCC receives request from
transferring hospital bull RMCC identifies Relief Hospital(s) bull Transferring hospital contacts
Relief Hospital directly bull Relief Hospital accepts patient(s) bull RMCC coordinates EMS PRN
Statewide Inter-Hospital Coordination Unit
Relief hospitals declare status on EMResource
IHCU receives request from RMCC on behalf of transferring hospital
IHCU identifies Relief Hospital(s) Transferring hospital contacts Relief
Hospital directly Relief Hospital accepts patient(s) IHCU coordinates EMS PRN
34
UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michiganrsquos Healthcare Preparedness Program bull Michigan Department of Health and Human Services ndash Bureau of EMS Trauma and Preparedness
bull 8 Regional Healthcare Coalitions ndash Hospitals EMS LPH EM LTC Tribal Health ndash Regional Coordinator Assistant Coordinator
Medical Director (25 FTE) ndash Regional Medical Coordination Center bull Multi-Agency Coordination Center bull Statewide use of EMResource by hospitals EMS
23
UnclassifiedFor Public Use
p ror
~ SC ON5
Sault Ste Marie
N
bull
Huron
Madison Milwa uk ee Graed Rapids bull bull e bull ~ 3rnia
L~nsi~ g bull - It bull
bullbullbullbull bull bull bull bull De troi t
bull Glwcago bull bull bull
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Michigan COVID-19 bull bull
bull
First 2 cases ndash March 10 Asymmetric epidemiology ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
24
UnclassifiedFor Public Use
Barrie
Toronto
Hamilton
bull bull
bull
Lake Ontario
bull Ro~besterbull
bull
bull
Brockville bull Kingston
~~w voRK
bull bull bull
bull
bull Pt0NfV VAN1A bull
bull
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H I NfOR MATION GATEWAY
bull
bull bull ~ ba riy
bull bull
Michigan COVID-19 bull First 2 cases ndash March 10
Asymmetric epidemiology bull ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
bull Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
25
UnclassifiedFor Public Use
I I I I I I I I I I I I I
ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City COVID-19 Daily Hospital Admissions
New York City vs Detroit 1800 1600 1400 1200 1000 800 600 400 200 0
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 26
UnclassifiedFor Public Use ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City
1 1 I 11111 111 11 11 1111 1 II II 1 1 1
400
300
200
COVID-19 Daily Hospital Admissions Per 1 Million PopulationNew York City vs Detroit
40-Day Post-Outbreak Mortality bull NY City 646 deaths per million bull Detroit 919 deaths per million
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 27
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Goal bull Save lives and reduce pain and suffering by optimizing
the use of the statersquos healthcare resources ndash Extend conventional standards of care to as many
patients as possible ndash Minimize the need for crisis standards of care bull Especially while conventional capacity exists
28
UnclassifiedFor Public Use
--
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Components bull Relief Hospitals
bull Alternate Care Sites EMS
ndash Home Care Sites
ndash Relief Personnel
29
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals vs Alternate Care Sites bull Relief Hospitals The objective is to extend the
conventional standard of care to as many citizens in need as possible (ie minimize the need to move intocrisis standards of care)
bull Alternate Care Sites (ACS) The objective is to delivercrisis standards of care (as close to the conventional standard of care as possible) in extreme conditions in which the conventional standard of care can not be provided at overloaded hospitals
30
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital ldquoAskrdquo bull Hospitals have been previously asked to be able to
surge an additional 20 above average daily census ndash Increased to 50 ldquosuper surgerdquo
bull Relief Hospitals provide 10 of their expanded capacity to assist severely impacted hospitals ndash While preserving 50 of super-surge capacity bull Many hospitals at very low census
31
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals and Patient Redistribution
bull Intra-Health System Transfer ndash Coordinated by specific health system
bull Intra-Regional Transfer ndash Coordinated by Regional Medical Coordination Center
bull Statewide Transfer ndash Coordinated by Inter-Hospital Coordination Unit bull AKA Medical Operations Coordination Cell (MOCC)
32
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Statewide Inter-Hospital Coordination Unit State EmergencyOperations Center
Planning Finance Operations
Health Branch
Inter-HospitalCoordination Unit
Physician Consultant
EMS Coordination Group
Logistics
MDHHS Health Emergency Operations
Center
Medical Operations
Coordination Cell
33
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs and Patient Redistribution Regional Medical
Coordination Center bull Relief hospitals declare status on
EMResource bull RMCC receives request from
transferring hospital bull RMCC identifies Relief Hospital(s) bull Transferring hospital contacts
Relief Hospital directly bull Relief Hospital accepts patient(s) bull RMCC coordinates EMS PRN
Statewide Inter-Hospital Coordination Unit
Relief hospitals declare status on EMResource
IHCU receives request from RMCC on behalf of transferring hospital
IHCU identifies Relief Hospital(s) Transferring hospital contacts Relief
Hospital directly Relief Hospital accepts patient(s) IHCU coordinates EMS PRN
34
UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use
p ror
~ SC ON5
Sault Ste Marie
N
bull
Huron
Madison Milwa uk ee Graed Rapids bull bull e bull ~ 3rnia
L~nsi~ g bull - It bull
bullbullbullbull bull bull bull bull De troi t
bull Glwcago bull bull bull
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfOR MATIO N GATEWAY
Michigan COVID-19 bull bull
bull
First 2 cases ndash March 10 Asymmetric epidemiology ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
24
UnclassifiedFor Public Use
Barrie
Toronto
Hamilton
bull bull
bull
Lake Ontario
bull Ro~besterbull
bull
bull
Brockville bull Kingston
~~w voRK
bull bull bull
bull
bull Pt0NfV VAN1A bull
bull
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H I NfOR MATION GATEWAY
bull
bull bull ~ ba riy
bull bull
Michigan COVID-19 bull First 2 cases ndash March 10
Asymmetric epidemiology bull ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
bull Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
25
UnclassifiedFor Public Use
I I I I I I I I I I I I I
ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City COVID-19 Daily Hospital Admissions
New York City vs Detroit 1800 1600 1400 1200 1000 800 600 400 200 0
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 26
UnclassifiedFor Public Use ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City
1 1 I 11111 111 11 11 1111 1 II II 1 1 1
400
300
200
COVID-19 Daily Hospital Admissions Per 1 Million PopulationNew York City vs Detroit
40-Day Post-Outbreak Mortality bull NY City 646 deaths per million bull Detroit 919 deaths per million
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 27
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Goal bull Save lives and reduce pain and suffering by optimizing
the use of the statersquos healthcare resources ndash Extend conventional standards of care to as many
patients as possible ndash Minimize the need for crisis standards of care bull Especially while conventional capacity exists
28
UnclassifiedFor Public Use
--
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Components bull Relief Hospitals
bull Alternate Care Sites EMS
ndash Home Care Sites
ndash Relief Personnel
29
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals vs Alternate Care Sites bull Relief Hospitals The objective is to extend the
conventional standard of care to as many citizens in need as possible (ie minimize the need to move intocrisis standards of care)
bull Alternate Care Sites (ACS) The objective is to delivercrisis standards of care (as close to the conventional standard of care as possible) in extreme conditions in which the conventional standard of care can not be provided at overloaded hospitals
30
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital ldquoAskrdquo bull Hospitals have been previously asked to be able to
surge an additional 20 above average daily census ndash Increased to 50 ldquosuper surgerdquo
bull Relief Hospitals provide 10 of their expanded capacity to assist severely impacted hospitals ndash While preserving 50 of super-surge capacity bull Many hospitals at very low census
31
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals and Patient Redistribution
bull Intra-Health System Transfer ndash Coordinated by specific health system
bull Intra-Regional Transfer ndash Coordinated by Regional Medical Coordination Center
bull Statewide Transfer ndash Coordinated by Inter-Hospital Coordination Unit bull AKA Medical Operations Coordination Cell (MOCC)
32
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Statewide Inter-Hospital Coordination Unit State EmergencyOperations Center
Planning Finance Operations
Health Branch
Inter-HospitalCoordination Unit
Physician Consultant
EMS Coordination Group
Logistics
MDHHS Health Emergency Operations
Center
Medical Operations
Coordination Cell
33
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs and Patient Redistribution Regional Medical
Coordination Center bull Relief hospitals declare status on
EMResource bull RMCC receives request from
transferring hospital bull RMCC identifies Relief Hospital(s) bull Transferring hospital contacts
Relief Hospital directly bull Relief Hospital accepts patient(s) bull RMCC coordinates EMS PRN
Statewide Inter-Hospital Coordination Unit
Relief hospitals declare status on EMResource
IHCU receives request from RMCC on behalf of transferring hospital
IHCU identifies Relief Hospital(s) Transferring hospital contacts Relief
Hospital directly Relief Hospital accepts patient(s) IHCU coordinates EMS PRN
34
UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use
Barrie
Toronto
Hamilton
bull bull
bull
Lake Ontario
bull Ro~besterbull
bull
bull
Brockville bull Kingston
~~w voRK
bull bull bull
bull
bull Pt0NfV VAN1A bull
bull
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H I NfOR MATION GATEWAY
bull
bull bull ~ ba riy
bull bull
Michigan COVID-19 bull First 2 cases ndash March 10
Asymmetric epidemiology bull ndash SE Michigan ndash Extreme Activity ndash Rest of Michigan ndash Sporadic Activity ndash Comparable to other states
bull Extreme conditions in SE MI ndash Peak hospitalizations gt4400 ndash 12-days with gt1000 on ventilation bull 1223 on ventilation on one day
ndash Peak intubations in 1 day 176 Source John Hopkins Coronavirus Resource Center (Retrieved 4212020)
25
UnclassifiedFor Public Use
I I I I I I I I I I I I I
ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City COVID-19 Daily Hospital Admissions
New York City vs Detroit 1800 1600 1400 1200 1000 800 600 400 200 0
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 26
UnclassifiedFor Public Use ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City
1 1 I 11111 111 11 11 1111 1 II II 1 1 1
400
300
200
COVID-19 Daily Hospital Admissions Per 1 Million PopulationNew York City vs Detroit
40-Day Post-Outbreak Mortality bull NY City 646 deaths per million bull Detroit 919 deaths per million
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 27
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Goal bull Save lives and reduce pain and suffering by optimizing
the use of the statersquos healthcare resources ndash Extend conventional standards of care to as many
patients as possible ndash Minimize the need for crisis standards of care bull Especially while conventional capacity exists
28
UnclassifiedFor Public Use
--
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Components bull Relief Hospitals
bull Alternate Care Sites EMS
ndash Home Care Sites
ndash Relief Personnel
29
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals vs Alternate Care Sites bull Relief Hospitals The objective is to extend the
conventional standard of care to as many citizens in need as possible (ie minimize the need to move intocrisis standards of care)
bull Alternate Care Sites (ACS) The objective is to delivercrisis standards of care (as close to the conventional standard of care as possible) in extreme conditions in which the conventional standard of care can not be provided at overloaded hospitals
30
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital ldquoAskrdquo bull Hospitals have been previously asked to be able to
surge an additional 20 above average daily census ndash Increased to 50 ldquosuper surgerdquo
bull Relief Hospitals provide 10 of their expanded capacity to assist severely impacted hospitals ndash While preserving 50 of super-surge capacity bull Many hospitals at very low census
31
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals and Patient Redistribution
bull Intra-Health System Transfer ndash Coordinated by specific health system
bull Intra-Regional Transfer ndash Coordinated by Regional Medical Coordination Center
bull Statewide Transfer ndash Coordinated by Inter-Hospital Coordination Unit bull AKA Medical Operations Coordination Cell (MOCC)
32
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Statewide Inter-Hospital Coordination Unit State EmergencyOperations Center
Planning Finance Operations
Health Branch
Inter-HospitalCoordination Unit
Physician Consultant
EMS Coordination Group
Logistics
MDHHS Health Emergency Operations
Center
Medical Operations
Coordination Cell
33
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs and Patient Redistribution Regional Medical
Coordination Center bull Relief hospitals declare status on
EMResource bull RMCC receives request from
transferring hospital bull RMCC identifies Relief Hospital(s) bull Transferring hospital contacts
Relief Hospital directly bull Relief Hospital accepts patient(s) bull RMCC coordinates EMS PRN
Statewide Inter-Hospital Coordination Unit
Relief hospitals declare status on EMResource
IHCU receives request from RMCC on behalf of transferring hospital
IHCU identifies Relief Hospital(s) Transferring hospital contacts Relief
Hospital directly Relief Hospital accepts patient(s) IHCU coordinates EMS PRN
34
UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-
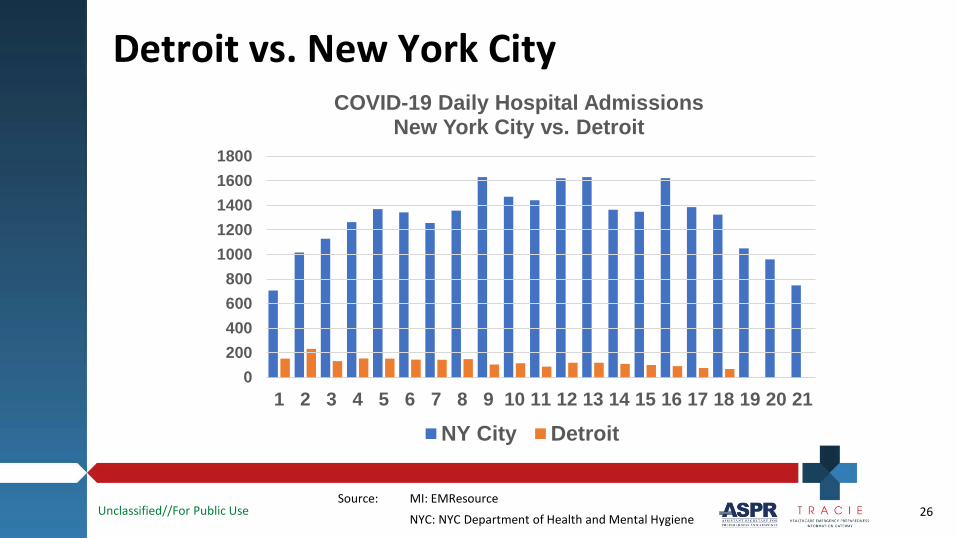
UnclassifiedFor Public Use
I I I I I I I I I I I I I
ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City COVID-19 Daily Hospital Admissions
New York City vs Detroit 1800 1600 1400 1200 1000 800 600 400 200 0
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 26
UnclassifiedFor Public Use ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City
1 1 I 11111 111 11 11 1111 1 II II 1 1 1
400
300
200
COVID-19 Daily Hospital Admissions Per 1 Million PopulationNew York City vs Detroit
40-Day Post-Outbreak Mortality bull NY City 646 deaths per million bull Detroit 919 deaths per million
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 27
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Goal bull Save lives and reduce pain and suffering by optimizing
the use of the statersquos healthcare resources ndash Extend conventional standards of care to as many
patients as possible ndash Minimize the need for crisis standards of care bull Especially while conventional capacity exists
28
UnclassifiedFor Public Use
--
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Components bull Relief Hospitals
bull Alternate Care Sites EMS
ndash Home Care Sites
ndash Relief Personnel
29
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals vs Alternate Care Sites bull Relief Hospitals The objective is to extend the
conventional standard of care to as many citizens in need as possible (ie minimize the need to move intocrisis standards of care)
bull Alternate Care Sites (ACS) The objective is to delivercrisis standards of care (as close to the conventional standard of care as possible) in extreme conditions in which the conventional standard of care can not be provided at overloaded hospitals
30
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital ldquoAskrdquo bull Hospitals have been previously asked to be able to
surge an additional 20 above average daily census ndash Increased to 50 ldquosuper surgerdquo
bull Relief Hospitals provide 10 of their expanded capacity to assist severely impacted hospitals ndash While preserving 50 of super-surge capacity bull Many hospitals at very low census
31
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals and Patient Redistribution
bull Intra-Health System Transfer ndash Coordinated by specific health system
bull Intra-Regional Transfer ndash Coordinated by Regional Medical Coordination Center
bull Statewide Transfer ndash Coordinated by Inter-Hospital Coordination Unit bull AKA Medical Operations Coordination Cell (MOCC)
32
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Statewide Inter-Hospital Coordination Unit State EmergencyOperations Center
Planning Finance Operations
Health Branch
Inter-HospitalCoordination Unit
Physician Consultant
EMS Coordination Group
Logistics
MDHHS Health Emergency Operations
Center
Medical Operations
Coordination Cell
33
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs and Patient Redistribution Regional Medical
Coordination Center bull Relief hospitals declare status on
EMResource bull RMCC receives request from
transferring hospital bull RMCC identifies Relief Hospital(s) bull Transferring hospital contacts
Relief Hospital directly bull Relief Hospital accepts patient(s) bull RMCC coordinates EMS PRN
Statewide Inter-Hospital Coordination Unit
Relief hospitals declare status on EMResource
IHCU receives request from RMCC on behalf of transferring hospital
IHCU identifies Relief Hospital(s) Transferring hospital contacts Relief
Hospital directly Relief Hospital accepts patient(s) IHCU coordinates EMS PRN
34
UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use ASPR TR AC IE ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Detroit vs New York City
1 1 I 11111 111 11 11 1111 1 II II 1 1 1
400
300
200
COVID-19 Daily Hospital Admissions Per 1 Million PopulationNew York City vs Detroit
40-Day Post-Outbreak Mortality bull NY City 646 deaths per million bull Detroit 919 deaths per million
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
NY City Detroit
Source MI EMResource
NYC NYC Department of Health and Mental Hygiene 27
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Goal bull Save lives and reduce pain and suffering by optimizing
the use of the statersquos healthcare resources ndash Extend conventional standards of care to as many
patients as possible ndash Minimize the need for crisis standards of care bull Especially while conventional capacity exists
28
UnclassifiedFor Public Use
--
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Components bull Relief Hospitals
bull Alternate Care Sites EMS
ndash Home Care Sites
ndash Relief Personnel
29
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals vs Alternate Care Sites bull Relief Hospitals The objective is to extend the
conventional standard of care to as many citizens in need as possible (ie minimize the need to move intocrisis standards of care)
bull Alternate Care Sites (ACS) The objective is to delivercrisis standards of care (as close to the conventional standard of care as possible) in extreme conditions in which the conventional standard of care can not be provided at overloaded hospitals
30
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital ldquoAskrdquo bull Hospitals have been previously asked to be able to
surge an additional 20 above average daily census ndash Increased to 50 ldquosuper surgerdquo
bull Relief Hospitals provide 10 of their expanded capacity to assist severely impacted hospitals ndash While preserving 50 of super-surge capacity bull Many hospitals at very low census
31
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals and Patient Redistribution
bull Intra-Health System Transfer ndash Coordinated by specific health system
bull Intra-Regional Transfer ndash Coordinated by Regional Medical Coordination Center
bull Statewide Transfer ndash Coordinated by Inter-Hospital Coordination Unit bull AKA Medical Operations Coordination Cell (MOCC)
32
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Statewide Inter-Hospital Coordination Unit State EmergencyOperations Center
Planning Finance Operations
Health Branch
Inter-HospitalCoordination Unit
Physician Consultant
EMS Coordination Group
Logistics
MDHHS Health Emergency Operations
Center
Medical Operations
Coordination Cell
33
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs and Patient Redistribution Regional Medical
Coordination Center bull Relief hospitals declare status on
EMResource bull RMCC receives request from
transferring hospital bull RMCC identifies Relief Hospital(s) bull Transferring hospital contacts
Relief Hospital directly bull Relief Hospital accepts patient(s) bull RMCC coordinates EMS PRN
Statewide Inter-Hospital Coordination Unit
Relief hospitals declare status on EMResource
IHCU receives request from RMCC on behalf of transferring hospital
IHCU identifies Relief Hospital(s) Transferring hospital contacts Relief
Hospital directly Relief Hospital accepts patient(s) IHCU coordinates EMS PRN
34
UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Goal bull Save lives and reduce pain and suffering by optimizing
the use of the statersquos healthcare resources ndash Extend conventional standards of care to as many
patients as possible ndash Minimize the need for crisis standards of care bull Especially while conventional capacity exists
28
UnclassifiedFor Public Use
--
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Components bull Relief Hospitals
bull Alternate Care Sites EMS
ndash Home Care Sites
ndash Relief Personnel
29
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals vs Alternate Care Sites bull Relief Hospitals The objective is to extend the
conventional standard of care to as many citizens in need as possible (ie minimize the need to move intocrisis standards of care)
bull Alternate Care Sites (ACS) The objective is to delivercrisis standards of care (as close to the conventional standard of care as possible) in extreme conditions in which the conventional standard of care can not be provided at overloaded hospitals
30
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital ldquoAskrdquo bull Hospitals have been previously asked to be able to
surge an additional 20 above average daily census ndash Increased to 50 ldquosuper surgerdquo
bull Relief Hospitals provide 10 of their expanded capacity to assist severely impacted hospitals ndash While preserving 50 of super-surge capacity bull Many hospitals at very low census
31
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals and Patient Redistribution
bull Intra-Health System Transfer ndash Coordinated by specific health system
bull Intra-Regional Transfer ndash Coordinated by Regional Medical Coordination Center
bull Statewide Transfer ndash Coordinated by Inter-Hospital Coordination Unit bull AKA Medical Operations Coordination Cell (MOCC)
32
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Statewide Inter-Hospital Coordination Unit State EmergencyOperations Center
Planning Finance Operations
Health Branch
Inter-HospitalCoordination Unit
Physician Consultant
EMS Coordination Group
Logistics
MDHHS Health Emergency Operations
Center
Medical Operations
Coordination Cell
33
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs and Patient Redistribution Regional Medical
Coordination Center bull Relief hospitals declare status on
EMResource bull RMCC receives request from
transferring hospital bull RMCC identifies Relief Hospital(s) bull Transferring hospital contacts
Relief Hospital directly bull Relief Hospital accepts patient(s) bull RMCC coordinates EMS PRN
Statewide Inter-Hospital Coordination Unit
Relief hospitals declare status on EMResource
IHCU receives request from RMCC on behalf of transferring hospital
IHCU identifies Relief Hospital(s) Transferring hospital contacts Relief
Hospital directly Relief Hospital accepts patient(s) IHCU coordinates EMS PRN
34
UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use
--
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Healthcare Surge Strategy Components bull Relief Hospitals
bull Alternate Care Sites EMS
ndash Home Care Sites
ndash Relief Personnel
29
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals vs Alternate Care Sites bull Relief Hospitals The objective is to extend the
conventional standard of care to as many citizens in need as possible (ie minimize the need to move intocrisis standards of care)
bull Alternate Care Sites (ACS) The objective is to delivercrisis standards of care (as close to the conventional standard of care as possible) in extreme conditions in which the conventional standard of care can not be provided at overloaded hospitals
30
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital ldquoAskrdquo bull Hospitals have been previously asked to be able to
surge an additional 20 above average daily census ndash Increased to 50 ldquosuper surgerdquo
bull Relief Hospitals provide 10 of their expanded capacity to assist severely impacted hospitals ndash While preserving 50 of super-surge capacity bull Many hospitals at very low census
31
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals and Patient Redistribution
bull Intra-Health System Transfer ndash Coordinated by specific health system
bull Intra-Regional Transfer ndash Coordinated by Regional Medical Coordination Center
bull Statewide Transfer ndash Coordinated by Inter-Hospital Coordination Unit bull AKA Medical Operations Coordination Cell (MOCC)
32
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Statewide Inter-Hospital Coordination Unit State EmergencyOperations Center
Planning Finance Operations
Health Branch
Inter-HospitalCoordination Unit
Physician Consultant
EMS Coordination Group
Logistics
MDHHS Health Emergency Operations
Center
Medical Operations
Coordination Cell
33
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs and Patient Redistribution Regional Medical
Coordination Center bull Relief hospitals declare status on
EMResource bull RMCC receives request from
transferring hospital bull RMCC identifies Relief Hospital(s) bull Transferring hospital contacts
Relief Hospital directly bull Relief Hospital accepts patient(s) bull RMCC coordinates EMS PRN
Statewide Inter-Hospital Coordination Unit
Relief hospitals declare status on EMResource
IHCU receives request from RMCC on behalf of transferring hospital
IHCU identifies Relief Hospital(s) Transferring hospital contacts Relief
Hospital directly Relief Hospital accepts patient(s) IHCU coordinates EMS PRN
34
UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals vs Alternate Care Sites bull Relief Hospitals The objective is to extend the
conventional standard of care to as many citizens in need as possible (ie minimize the need to move intocrisis standards of care)
bull Alternate Care Sites (ACS) The objective is to delivercrisis standards of care (as close to the conventional standard of care as possible) in extreme conditions in which the conventional standard of care can not be provided at overloaded hospitals
30
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital ldquoAskrdquo bull Hospitals have been previously asked to be able to
surge an additional 20 above average daily census ndash Increased to 50 ldquosuper surgerdquo
bull Relief Hospitals provide 10 of their expanded capacity to assist severely impacted hospitals ndash While preserving 50 of super-surge capacity bull Many hospitals at very low census
31
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals and Patient Redistribution
bull Intra-Health System Transfer ndash Coordinated by specific health system
bull Intra-Regional Transfer ndash Coordinated by Regional Medical Coordination Center
bull Statewide Transfer ndash Coordinated by Inter-Hospital Coordination Unit bull AKA Medical Operations Coordination Cell (MOCC)
32
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Statewide Inter-Hospital Coordination Unit State EmergencyOperations Center
Planning Finance Operations
Health Branch
Inter-HospitalCoordination Unit
Physician Consultant
EMS Coordination Group
Logistics
MDHHS Health Emergency Operations
Center
Medical Operations
Coordination Cell
33
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs and Patient Redistribution Regional Medical
Coordination Center bull Relief hospitals declare status on
EMResource bull RMCC receives request from
transferring hospital bull RMCC identifies Relief Hospital(s) bull Transferring hospital contacts
Relief Hospital directly bull Relief Hospital accepts patient(s) bull RMCC coordinates EMS PRN
Statewide Inter-Hospital Coordination Unit
Relief hospitals declare status on EMResource
IHCU receives request from RMCC on behalf of transferring hospital
IHCU identifies Relief Hospital(s) Transferring hospital contacts Relief
Hospital directly Relief Hospital accepts patient(s) IHCU coordinates EMS PRN
34
UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital ldquoAskrdquo bull Hospitals have been previously asked to be able to
surge an additional 20 above average daily census ndash Increased to 50 ldquosuper surgerdquo
bull Relief Hospitals provide 10 of their expanded capacity to assist severely impacted hospitals ndash While preserving 50 of super-surge capacity bull Many hospitals at very low census
31
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals and Patient Redistribution
bull Intra-Health System Transfer ndash Coordinated by specific health system
bull Intra-Regional Transfer ndash Coordinated by Regional Medical Coordination Center
bull Statewide Transfer ndash Coordinated by Inter-Hospital Coordination Unit bull AKA Medical Operations Coordination Cell (MOCC)
32
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Statewide Inter-Hospital Coordination Unit State EmergencyOperations Center
Planning Finance Operations
Health Branch
Inter-HospitalCoordination Unit
Physician Consultant
EMS Coordination Group
Logistics
MDHHS Health Emergency Operations
Center
Medical Operations
Coordination Cell
33
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs and Patient Redistribution Regional Medical
Coordination Center bull Relief hospitals declare status on
EMResource bull RMCC receives request from
transferring hospital bull RMCC identifies Relief Hospital(s) bull Transferring hospital contacts
Relief Hospital directly bull Relief Hospital accepts patient(s) bull RMCC coordinates EMS PRN
Statewide Inter-Hospital Coordination Unit
Relief hospitals declare status on EMResource
IHCU receives request from RMCC on behalf of transferring hospital
IHCU identifies Relief Hospital(s) Transferring hospital contacts Relief
Hospital directly Relief Hospital accepts patient(s) IHCU coordinates EMS PRN
34
UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospitals and Patient Redistribution
bull Intra-Health System Transfer ndash Coordinated by specific health system
bull Intra-Regional Transfer ndash Coordinated by Regional Medical Coordination Center
bull Statewide Transfer ndash Coordinated by Inter-Hospital Coordination Unit bull AKA Medical Operations Coordination Cell (MOCC)
32
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Statewide Inter-Hospital Coordination Unit State EmergencyOperations Center
Planning Finance Operations
Health Branch
Inter-HospitalCoordination Unit
Physician Consultant
EMS Coordination Group
Logistics
MDHHS Health Emergency Operations
Center
Medical Operations
Coordination Cell
33
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs and Patient Redistribution Regional Medical
Coordination Center bull Relief hospitals declare status on
EMResource bull RMCC receives request from
transferring hospital bull RMCC identifies Relief Hospital(s) bull Transferring hospital contacts
Relief Hospital directly bull Relief Hospital accepts patient(s) bull RMCC coordinates EMS PRN
Statewide Inter-Hospital Coordination Unit
Relief hospitals declare status on EMResource
IHCU receives request from RMCC on behalf of transferring hospital
IHCU identifies Relief Hospital(s) Transferring hospital contacts Relief
Hospital directly Relief Hospital accepts patient(s) IHCU coordinates EMS PRN
34
UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Statewide Inter-Hospital Coordination Unit State EmergencyOperations Center
Planning Finance Operations
Health Branch
Inter-HospitalCoordination Unit
Physician Consultant
EMS Coordination Group
Logistics
MDHHS Health Emergency Operations
Center
Medical Operations
Coordination Cell
33
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs and Patient Redistribution Regional Medical
Coordination Center bull Relief hospitals declare status on
EMResource bull RMCC receives request from
transferring hospital bull RMCC identifies Relief Hospital(s) bull Transferring hospital contacts
Relief Hospital directly bull Relief Hospital accepts patient(s) bull RMCC coordinates EMS PRN
Statewide Inter-Hospital Coordination Unit
Relief hospitals declare status on EMResource
IHCU receives request from RMCC on behalf of transferring hospital
IHCU identifies Relief Hospital(s) Transferring hospital contacts Relief
Hospital directly Relief Hospital accepts patient(s) IHCU coordinates EMS PRN
34
UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs and Patient Redistribution Regional Medical
Coordination Center bull Relief hospitals declare status on
EMResource bull RMCC receives request from
transferring hospital bull RMCC identifies Relief Hospital(s) bull Transferring hospital contacts
Relief Hospital directly bull Relief Hospital accepts patient(s) bull RMCC coordinates EMS PRN
Statewide Inter-Hospital Coordination Unit
Relief hospitals declare status on EMResource
IHCU receives request from RMCC on behalf of transferring hospital
IHCU identifies Relief Hospital(s) Transferring hospital contacts Relief
Hospital directly Relief Hospital accepts patient(s) IHCU coordinates EMS PRN
34
UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use
Critical 2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed - Care Bed - Critical Critical Take Take Non-COVID-19 non- Care Bed- Care Bed - COVID-19 COVID-19
COVID-19 COVID-19 non- Patients Patients COVID-19
No Yes
22 0 0 o - 4 4 16 24
1 1 5 5
h Ctr 40 8 8 10
1 0 5 5
68 13 34 51
2 Critical 3 Non- 4 Non- Willing to Willing to Comment Care Bed Critical Critical Take Take Non-bull non- Care Bed Care Bed COVID-19 COVID-19 COVID-19 - - non- Patients Patients
COVID-19 COVID-19
nton 0 0 0 0 No No
0 0 24 3 No No Already exceeding critical No No Already exceeding critical
0 0 0 0 ----Already exceeding critical
0 Already exceeding critical
ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
EMResource Relief Hospital Participation
35
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCC-Facilitated vs Direct Contact Transfers MOCC Facilitated
bull Hospital has need to transfer bull Regional State MOCC
contacted bull EMResource reviewed by MOCC
to identify Relief Hospitals bull MOCC connects transferring
hospital to Relief Hospital bull Relief Hospital accepts
patient(s) bull MOCC coordinates EMS PRN
Direct Contact Hospital has need to transfer Regional State MOCC
bypassed EMResource reviewed by hospital
to identify Relief Hospitals Transferring hospital contacts
Relief Hospital directly Relief Hospital accepts
patient(s) MOCC coordinates EMS PRN
36
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Patient Redistribution ndash 5 Key Elements
bull bull bull bull bull
Transferring Hospitals Coordinating entity (MOCCs) Situational awareness platform (EMResource) EMS Relief Hospitals
37
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Relief Hospital Recruitment Challenges
Why were so many hospitals in minimally impacted regions resistant to accept patients bull Fea
bull Fear of introducing bringing COVID-19 into their hospital
r of impending ldquostormrdquo ndash ldquoItrsquos just a matter of time till wersquore Detroitrdquo
Need for Epidemiologic Intelligence
38
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-
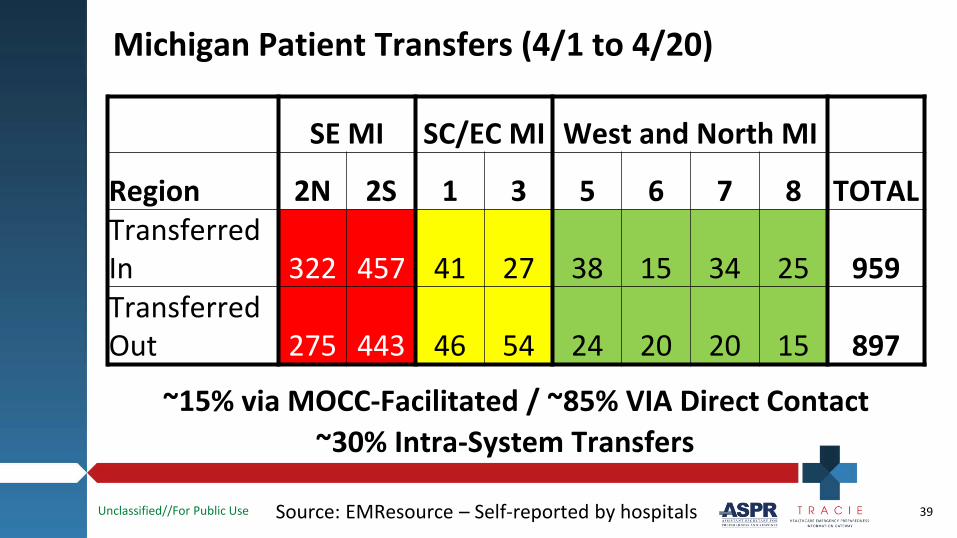
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Michigan Patient Transfers (41 to 420)
SE MI SCEC MI West and North MI
Region 2N 2S 1 3 5 6 7 8 TOTAL Transferred In 322 457 41 27 38 15 34 25 959 Transferred Out 275 443 46 54 24 20 20 15 897
~15 via MOCC-Facilitated ~85 VIA Direct Contact ~30 Intra-System Transfers
Source EMResource ndash Self-reported by hospitals 39
UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use
Bureau of EMS Trauma amp Preparedness
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
MOCCs in Michigan
bull Role Facilitation not control bull Staffing at State MOCC ndash Experienced paramedics EMS control center bull Remote component to SEOC
bull Physician role ndash Consultative problem solving medical leadership
bull Use of statewide hospital status application essential ndash Allows hospitals to connect directly
40
UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use
DHHS Michigan Department or Health amp Human Services
-ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Summary bull Relief Hospital concept works bull Statewide MOCC successful in coordinating transfers bull EMResource serves as an invaluable tool for
identifying Relief Hospitals bull Decentralized approach where hospitals in need
contact hospitals with capacity requires minimal central coordination
bull Recruitment of Relief Hospitals can be challenging
41
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
Ronald Stewart MD Chair Department of Surgery UT Health San Antonio Long School of Medicine Eric Epley Executive Director CEO Southwest Texas Regional Advisory Council for Trauma (STRAC)
UnclassifiedFor Public Use 42
~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

~ University - Health System
Regional Disaster Response in Texas Implementation of the
RMOC Concept Ronald M Stewart Eric Epley Brian Eastridge Dudley Wait Joe Palifini Dave Miramontes Craig Cooley Donald
Jenkins and the Southwest Texas Regional Advisory Council Team and
Texas Emergency Medical Task Force Region Leaders
ASPR Tracie Webinar April 24 2020
UnclassifiedFor Public Use 43
SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

SouchweGt Tebullas Region1il Aduisory Council
Introduction
UnclassifiedFor Public Use
bull
bull
Trauma system development
bull Routine multiple small-scale disasters
bull Structured cooperation and communication Trauma system infrastructure for
bull bull
Disaster Stroke STEMI Mental Health Perinatal
bull Trauma System Complete Evolution to EmergencyHealth Care SystemmdashWill use Trauma System andEmergency Health Care System interchangeably
bull Health Care Coalition
bull Right Patient Right Place Right Time 44
THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

THE TEXAS TRAUMA SYSTEM
UnclassifiedFor Public Use
22 TRAUMA SERVICE AREAS
REGIONAL ADVISORY COUNCILS
TRAUMA CENTER DESIGNATIONS
STANDARDS OF CARE
HOSPITAL PREPAREDNESS GRANTS
CONSISTENCY THROUGHOUT URBAN SUBURBAN RURAL AND
FRONTIER
45
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-
Southwest Teus Regional Ad11lsory Council
l The Committee -~
on Trauma 1 middot
EHC System Complex Problem Solving
bull Maximally inclusive with respect to stakeholders bull Dialogue and consensus centered upon bull Whatrsquos the right thing to do for the patient or population being served
bull Timely bull Structured cooperation bull Communication ndash Robust and redundant bull Actionable data
bull Bias for action bull Performance improvement processes
UnclassifiedFor Public Use 46
911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

911 Commission
1) FAILURE OF IMAGINATION
2) FAILURE OF POLICY (A FAILURE TO HAVE THE RIGHT INFRASTRUCTURE IN PLACE)
3) FAILURE OF CAPABILITY (A FAILURE TO HAVE THE RIGHT RESOURCES)
4) FAILURE OF MANAGEMENT (THE FAILURE TO COORDINATE THE AVAILABLE RESOURCES AND INFRASTRUCTURE)
Challenge of Large-Scale Disaster Preparation and Management
UnclassifiedFor Public Use 47
Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

Southwest Tecas Regional Advisory Council
Our Experience
A functioning regional trauma (EHC) system provides the framework for an effective response to large-scale disasters
Education and drills are not enough
Linked regional medical operations centers ( or MOCCs) critical to effective disaster response from all causes
UnclassifiedFor Public Use 48
a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

a
Southwest Texas Regional Advisory Council
Managing Wide-Scale Disasters
UnclassifiedFor Public Use 49
Acute Health Care System
bull Critical for emergency response and treatment of acute illness or injury
bull Mostly private and public mix bull Services to individuals bull Distributed and complex
network of providers bull Decisions made clinically
within minutes to hours
Public Health System
bull Largely responsible for most significant health improvements
bull Safety and wellbeing of populations
bull Multidisciplinary science bull Mainly public with centralized
communication bull Decisions with deliberation
and testing usually takes days
EmergencyManagement System
Local State
Federal Emergency Management Response
These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

These Three Systems Must Function Seamlessly and Flawlessly Together
Acute Health Care System
Public Health
Emergency Management
UnclassifiedFor Public Use 50
Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

Communications Problems Common to failures Disasters
Unworkable and Must have a credible and untested plans workable solution to each of these problemsmdashif we are to improve disaster response Lack of coordinated
response UnclassifiedFor Public Use 51
MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

MEDCOM
bull Trauma Transfers-500mo bull Air Medical Management bull Trauma Team Paging bull MCI load-balancing bull Navigation of mental health
patients via Law Enforcement directly topsychiatric facilities
UnclassifiedFor Public Use 52
D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

D D
D D
How to Integrate Disaster Acute Care and Public Health Systems
bull Trauma MEDCOM Communications Center
bull Regional Medical Operations Center
bull Integrated with Local Emergency Operations Center(EOC)
bull Linked to State Emergency Operations Center
UnclassifiedFor Public Use
bull Linked to Federal Emergency Management System53
Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

Southwest Texas Regional Aduisory Council Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use
Upregulated MEDCOMmdashdramatically enhanced data and comm Functional for 17 years in San Antonio bull Essential elements
bull Formal agreements insuring collaborationbull Representatives of all major stakeholders in one room-physical or virtualbull Formal communication link to the Emergency Operations Centers (EOC)bull Fault tolerant communications systemsbull Software systems ndashWebEOC software
bull bull bull
Monitor and coordinate all critical hospital capacity Monitor all critical public health data Monitor and coordinate all critical EMS agencies
bull Direct tie to the EOC and SOCbull EMTF functionmdashAbility to physically expand and adapt Emergency Medical Task
Forces amp Mobile Medical Units54
Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

Regional Medical Operations Center (RMOC) Regional Medical Operations Center (RMOC)
UnclassifiedFor Public Use 55
Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

Feasible Plan Must work in
real world conditions
UnclassifiedFor Public Use 56
Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

Southwest Te11as Regional Adv isory Council
RMOC Abilities and Advantages
bull Situational AwarenessmdashRegional Consciousness bull Virtual expansion of bed capacity
bull Distribute to all regional facilitiesmdashnot just a few ndashMany Hands Make Light Work bull Proven many times over 15 yearsmdashdistribution of 1000s of patients over a few days
bull Enables health care regional response teams bull Multi-agency rescue teamsmdashswift water rescue etc bull Mobile medical unitsmdashtemporary hospital replacements or augments
bull Load balancing during a surge of patients bull Network with other regions ndash8 RMOC equivalents in Texas bull Integration of Public Health Acute Care and Disaster Management Systems
UnclassifiedFor Public Use 57
Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

Vancouver
Seattle
Idaho Oregon
Nevada
San Francisco
California
lls Angeles
Montana No11 Dakota
Minnesota
South Dakcta
Wyoming
Wisconsin
Iowa Ne~raska
Toronto c ~New Y0rk Boston Detroit middot
ChicatJo middotimiddot New r ark
Denver Oli io
St Louis Kansas
K~ ntucilty Vitgin 1c1
tfort Ca r0 l1na
New Mexico Arlltansas
Atla11ta Oaas
Georgiamp
Texas
Houston
Monterrey C - Gulf of
Miami
RMOC Response and Function to COVID-19
UnclassifiedFor Public Use 58
INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

INTERNAL REPORT - PHI DATA This report contains Protected Health Information and is not intended for public distribution
Date COVID+ Patients COVD+ in ICU
04212020 82
04202020 81 -
04192020 81
Normal
Part ici pating HCS COVID Data as of 0815 Zl-Apr-20
VentBed Data as of 0910 21-Apr-20
41
41
41
COVID+ on Ventilator
24
25
24
BTRAC
All Healthcare Systems
Available Vents I Total Vents Available Vents
554 713 7896
514 710 7296 - ~ -
555 704 7996
Healthcare System Stress Score
I
Available Staffed Total Staffed Available Staffed Beds Beds Beds
1752 4 730 3796
1792 4 700 3896 - - - - - 7 1635 4707 3596
Severe
UnclassifiedFor Public Use 59
INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

INTERNAL REPORT - PHI DAT A This report contains Protected Health Information and is not intended for public distribution
San Antonio Healthcare Systems COVI D-19 Patient Count
Positive Patients on 4212020
Positive Patients Trend 312212020 - 412112020
322 327 411 4 6 4 11 4 16
Systems Reporting Daily Morning Data
Health Sys I Heal th Sys2 HS3 HS4 HSS HS6
PUI Patients on 4212020
82 50
PUI Patients Trend 312012020 - 42112020
80
60
40 38
20
o __ _________________ _
4 21 322 3 27 4 I 4 6 41 I 4 1 6 42 1
H Tuesday April Z1 2020 STll=IAC _c
TOT AL Patients on 4212020
132
TOTAL Patients Trend 312212020 - 412112020
150 151
100
50
o __ __________________ _
3122 327 4 1 4 16 4 1 1 4 16 42 1
UnclassifiedFor Public Use 60
HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

HOSPITALS Due DAILY 0900 hrs Hospital PPE IDR Materials Status Medical Dashboard (Bed and Ventilator Status) httpserisstracorgeoc7
EMS Due WEEKLY Friday 1200 hrs httpswwwsurveymonkeycomrEMSPPE2
ALL OTHER Coalition and ARHC Members Due WEEKLY Friday 1200 hrs https www surveymonkeycomrRMOCPPEOuery
1900 041220
Number of Regional Hospitals Reporting PPE Shortfall amp Days Remaining Until Depletion 5 - 7 Da s 8 - 11 Da s 12 - 14 Da s 15+ Da s
0 8 14 5 Data derived from facilities Hospital PPE IDR Materials Status - Facilities listed have indicated a disruption in their supply chain for any of the following PPE N95s Surgical Masks Gowns Gloves Face Shields Goggles
UnclassifiedFor Public Use 61
1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

1015
Weekly COVID-19 Update Epidemiology Program
39 191 97 Tota l Cases Reported Tota l Deaths Re po rted Ever Hospita lized Adm itted to ICU
VI
45
40
35
~ 30 ro u 0 25
1 20
sect 15 z
10
5
0
23
Cases of COVID-19 by Date of Illness Onset (n=880)1 and Cumulative by Date Reported Bexar County 4182020
Female( )Ma le 51 49
210 217 224 32 39 316 323 330 46 413
- Number of Cases - cumulative Cases
1 aased on cor1pleted d31 ai 3s or 4181020 a t 800 PM dditiomd crases 3re 1111der feview
1200
t moo V
QI VI ro u
800 0
~ QI 0
- 600 E 0
u
Nl z ii - 400 ~ _
ro S
- 200 E u
-0
CITY OF SAN ANTONIO METROPOLITAN HEALTH DISTRICT
so 276 Mechanica l Venti lat ion Recovered
Percentage of Cases by Raceethnicity
American IndianAlaska Native
Asian
Black
White
Hispanic
Other
Cases by Age Group
~~ I 39 4n1 i 300 sect 200 z
100 3 0 +------------------~~~~-~~ ----r-~ ~ ~ -
17
0-17 18-40 41-64 65+
Age Grou p in Yea rs
Median ace - 46 years (age range 0-100 years)
UnclassifiedFor Public Use 62
RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

RMOCs Mobile Drive Through COVID-19 Testing over 268000 Square Miles
UnclassifiedFor Public Use 63
= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

= sect111ntomo tprrssmiddotXrws uesce ~
NEW5
Texas San Antonio officials launch investigations of nursing home overrun by coronavirus
LaurenCan1ba Apri112Q20 UpdacedApfd-12020212pm fWBinGi P 0
COVJCgt-19 ~ uitefldid lifo iil5 w~ kriew it inTeitas tradeLmithequtiOllsyouw1nt
nswered illd the issues YMI think we
sAQllid be lnvmlgadllg lndodamp- )Our
email iind an pounditpessbullNllWS journ11Nt will
follow up
Hot Spot Evaluation and Coordination
UnclassifiedFor Public Use 64
RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

RMOC Function in COVID-19 Response
bull Situational awareness bull Integration of public health acute health care and disaster
management functions bull Actionable data from consolidating public health and acute health
care data sources bull Controlling and coordinating hot-spots bull Drive through testing management across the entire State bull Ability to Load balance across multiple health systems and
organizations UnclassifiedFor Public Use 65
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Quiroz RN Nurse Manager Los Angeles County Emergency Medical Services
UnclassifiedFor Public Use 66
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
bull 247 Medical amp Health Coordinator for the County and Region I
bull Coordinate Patient Transfers and Transportation bull Coordinate medical and heath resource management bull 911 Providers Hospitals LTC Clinics Dialysis Surgical
67
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATION GATEWAY
Los Angeles County and Region I
68
ifornia Reg1ions
Coastal OES Region n
Southem oes Regiion I
Inl and OES Region IV
Soutiheim Santa Barbara OES Reg Ion VI
I
Kerrn
Los Angeles
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Normal Operations vs Emergency and Disaster Response
Normal Operationsbull DHS Hospital and Clini
System bull EMTALA Transfers bull Air Medical bull Hyperbaric Chamber bull MCI Patient
Destinations bull TransferTransport
c
Emergency Disaster bull Hospital evacuations bull Resource Request bull Alternate Care Sites ndash Mercy ndash LASH ndash IsolationQuarantine
bull TransferTransport bull Prehospital Care Policy
69
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Keys to Success
bull 247 Base of Operationsbull Communicationsndash Telephony Radio Internet ReddiNet
bull DOC Room to expand operation during disasterbull Information System to document and analyze all lines
of businessbull Trained and talented staffbull Planning and exercise
70
UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use
TRACIE HEALTHCARE EMERGENCY PREPAREDNESS
INFORMATION GATEWAY
ASPR ASSISTANT SECRETARY ~-OR
PREPAREDNES S AND RESPONSE
John Hick MD Hennepin Healthcare MN
UnclassifiedFor Public Use 71
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Minnesota SHCC bull Statewide Healthcare Coordination Centerbull Located at State EOC as well as virtual ndash roughly
40 people directly engaged including regionalleads
bull Joint MDH HSEM MHA 8 regional MN coalitionconstruct
bull Main areas of planning responsendash ndash ndash ndash ndash
Referrals and transfers Alternate care sites Long term care ndash reactive and proactive PPE policy and acquisition Ventilator medical supply acquisition
72
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Referrals and Transfers bull Single phone number for LTC issues including hospital discharge and
COVID + patient support (eg assisted living transfer to COVID +designated SNF)
bull Co-located with SEOC public hotline but different staffing numbers bull Single (separate) phone number for ICU referrals ndash Mainly for greater MN but also inter-metro ndash Awareness of resources on MnTrac and real-time health system
information ndash Also provides direct connection to critical care consultation ndash May also be used to make triage decisions if referral needed and
no resources available (care-in-place recommendations) ndash May also be used to distribute load
73
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Staffing bull
bull
bull
bull
Call-taker ndash Medical background preferred ndash ndash
Gatekeeper for referral to SME May connect caller with resources and then referrals handled per usual
Shift Supervisor ndash ndash
Clinical background and experience with bed placement (eg house nursing supervisor) Manages information resource availability with facilities and more complicatedsituations
Clinician on-call ndash ndash
Critical care Contacts with each major health system critical care for ECMO and other resourceallocation situations
Unit supervisor ndash Works with SHCC manager on overall operations processes protocols
74
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Triggers
bull
bull
LTC ndash ndash ndash
Difficulty obtaining hospital discharges for LTC patients Achieved and hotline operational (Note ndash hotline also coordinates connections to infection preventioncontrol MDH Health Regulation Division palliative care consultations and can trigger strike team evaluation staffing support transfer support)
ICU ndash ndash ndash
lt 10 ICU beds available statewide Request from MHA or a coalition due to difficulty coordinating destinations Further triggers for engagement of clinician at request or when no ICU bedsavailable for reasonable match
75
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Other uses considerations
bull Matching to EMS transport services bull Patient ICU transfer considerations ndash Need for higher level of care ndash first priority ndash ECMO ventilators etc
bull Patients presenting to facility that lacks appropriate resources atbaseline
ndash
ndash
Load balancing ndash second priority bull Convalescent patients bull
bull
Intubated and stable patients (regional ndash if significant capacity under-utilized) Riskbenefit considerations
Resource movement ndash eg ventilators (vs anesthesia machines) or staff (virtual or in-person)
76
UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Question amp Answer
77
UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-

UnclassifiedFor Public Use -ASPR ANT bulllCatrtbull~ ~obull HUtTHCtH h oUGpound NC1 HpoundhHONpound~~ UIPAUDgt1111 ~NC UfPO~H INfORMATIO N GATEWAY
Contact Us
asprtraciehhsgov 1-844-5-TRACIE askasprtraciehhsgov
78
- Developing a Healthcare Coalition Pediatric Surge Annex
- ASPR TRACIE Three Domains
- Resources
- Overview of AAP and Pediatric Centers of Excellence
- Overview of AAP and Pediatric Centers of Excellence
- Executive Summary
- MOCCs Problem Statement
- A MOCC Aims to
- MOCCs Concept
- MOCCs | General Activity Summary
- MOCCs Toolkit
- Deanna Dahl-Grove MD FAAP Associate Professor Pediatric Emergency Medicine Rainbow Babies and Childrenrsquos Hospital Member AAP CoDPR Executive Committee13
- Western Washington MOCC
- King County LTCF Outbreak
- Single LTCF - Single Hospital
- Medical Operations Coordinating Cell
- Regional COVID Coordinating Center ndash Western Washington
- Two Surveillance Pillars of the RC3
- Two Coordination Pillars of the RC3
- Emergency Response Platform - Microsoft
- Emergency Response Platform - Microsoft
- Christopher Newton MD13Associate Professor of Surgery Division of Pediatric Surgery Director of Trauma Care UCSF Benioff Childrenrsquos Hospital Oakland13
- Michiganrsquos Healthcare Preparedness Program
- Michigan COVID-19
- Michigan COVID-19
- Detroit vs New York City
- Detroit vs New York City
- Michigan Healthcare Surge Strategy Goal
- Michigan Healthcare Surge Strategy Components
- Relief Hospitals vs Alternate Care Sites
- Relief Hospital ldquoAskrdquo
- Relief Hospitals and Patient Redistribution
- Statewide Inter-Hospital Coordination Unit
- MOCCs and Patient Redistribution
- EMResource Relief Hospital Participation
- MOCC-Facilitated vs Direct Contact Transfers
- Patient Redistribution ndash 5 Key Elements
- Relief Hospital Recruitment Challenges
- Michigan Patient Transfers (41 to 420)
- MOCCs in Michigan
- Summary
- Sarita Chung MD FAAP13Director of Disaster Preparedness Division of Emergency Medicine Childrenrsquos Hospital Boston Member American Academy of Pediatrics (AAP) Council on Disaster Preparedness and Recovery13
- Regional Disaster Response in Texas Implementation of the RMOC Concept
- Introduction
- The Texas Trauma System
- EHC System Complex Problem Solving
- 911 Commission
- Our Experience
- Managing Wide-Scale Disasters
- Acute Health Care SystemPublic Health Emergency Management
- Problems Common to DisastersMust have a credible and workable solution to each of these problemsmdashif we are to improve disaster response
- MEDCOM
- How to Integrate Disaster Acute Care and Public Health Systems
- Regional Medical Operations Center(RMOC)
- Regional Medical Operations Center
- Feasible Plan Must work in real world conditions
- RMOC Abilities and Advantages
- RMOC Response and Function to COVID-19
- STRAC Report
- STRAC Report
- STRAC Report
- Weekly COVID-19 Update
- RMOCsMobile Drive Through COVID-19 Testing over 268000 Square Miles
- Hot Spot Evaluation and Coordination
- RMOC Function in COVID-19 Response
- Moderator Roundtable
- Los Angeles (LA) County Medical Operations Coordination Cell (MOCC)
- Los Angeles County and Region I
- Normal Operations vs Emergency and DisasterResponse
- Keys to Success
- Moderator Roundtable
- Minnesota SHCC
- Referrals and Transfers
- Staffing
- Triggers
- Other uses considerations
- Question amp Answer
- Contact Us
-