espen congress lisbon 2015 nutritional management in stoma care · 2015-10-31 · n=143 ~74 y...
TRANSCRIPT

ESPEN Congress Lisbon 2015
Perioperative nutritional management in cystectomy patientsP. Coti (CH)
NUTRITIONAL MANAGEMENT IN STOMA CARE

Perioperative nutritional management in cystectomy patients
Pauline Coti Bertrand
Clinical Nutrition Team
Endocrinology, Metabolism and Diabetology

Introduction • Radical cystectomy
– major surgery– high nutritional risk
• Postoperative morbidity– High … 64% at 90 days and LOS: 17.4 days– Reduced by enhanced recovery after surgery
(ERAS) protocols … nutritional care

Cystectomy … Major surgery
• Bladder resection• Urinary diversion with or without continence• Bilateral pelvic lymph node dissection in cancer• Neobladder with intestinal segment
• Operation time : 4 to 10 hours

Nutritional risk• Major surgery
– Surgical technique– Metabolic stress
• Patients– Main disease– Age

ERAS protocols• Keys principles
– Preoperative counseling to teach in regard to surgery, plan of care and hospital orientation
– Standardised analgesic and anestheticregimens (epidural and non opioid analgesia)
– Early mobilisation – Optimisation of nutrition

Optimisation of nutrition• Is preoperative mechanical bowel preparation useful ?
– To rid the large bowel of solid fecal contents and to lowerbacterial load
• Is preoperative immuno-nutrition indicated ?– To reduce postoperative morbidity
• Is preoperative fasting from midnight useful ?– To prevent aspiration and regurgitation
• Is postoperative parenteral nutrition indicated ?– To prevent vomiting and bowel anastomotic leaks

IS PREOPERATIVE MECHANICALBOWEL PREPARATION USEFUL ?

Preoperative mechanical bowelpreparationRoutine use to reduce the incidence of postoperative infectious complications
• Cause of metabolic and electrolyte imbalance, dehydration, abdominal pain/bloating and fatigue
• Solid faeces liquefaction which may increase the risk of intraoperativespillage of contaminant
• Absence of benefit– No difference in anastomotic leakage, septic complications, fascial dehiscence and
mortalityRCT of 1431 patients at 13 colorectal centres. Contant CM et al. Lancet 2007
• Increased risk of postoperative complications– Anastomotic leaks– Wound infections– Intra-abdominal abcesses
Metanalysis of 10 RCT and nearly 2000 patients. Bucher P et al. Arch Surg 2004

IS PREOPERATIVEIMMUNONUTRITION INDICATED?

Is preoperative immunonutritionindicated ?
• Immunosuppression is induced by– Malnutrition– Surgical stress
• Preoperative malnutrition is associated with highermortality and morbidity
• Malnutrition is present before surgery in 16-22% patients and surgical stress makes it worse by inducing a decrease of muscle mass and function

Gregg JR et al. J Urol 2011;185(1):90-6.
Nutritional deficiency is a strong predictor of 90-day mortality and poor overall survival
538 patients undergoing radical cystectomy for urothelial carcinoma19% with nutritional deficiency
Nutritional deficiency is defined• Albuminemia < 3,5 mg/dl• BMI < 18.5 kg/m2• Preoperative weight loss > 5%
HR 2.91; 95% CI 1.36, 6.23; p < 0.01
At 3 years 67,6% versus 44,5%; p < 0.01
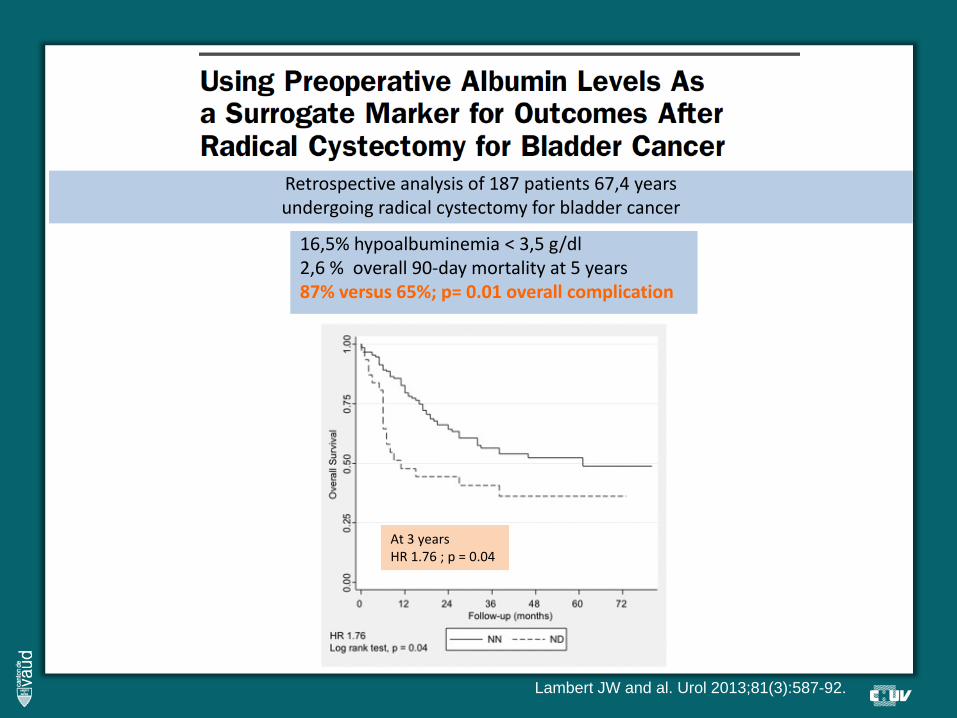
Retrospective analysis of 187 patients 67,4 yearsundergoing radical cystectomy for bladder cancer
16,5% hypoalbuminemia < 3,5 g/dl2,6 % overall 90‐day mortality at 5 years87% versus 65%; p= 0.01 overall complication
At 3 yearsHR 1.76 ; p = 0.04
Lambert JW and al. Urol 2013;81(3):587-92.
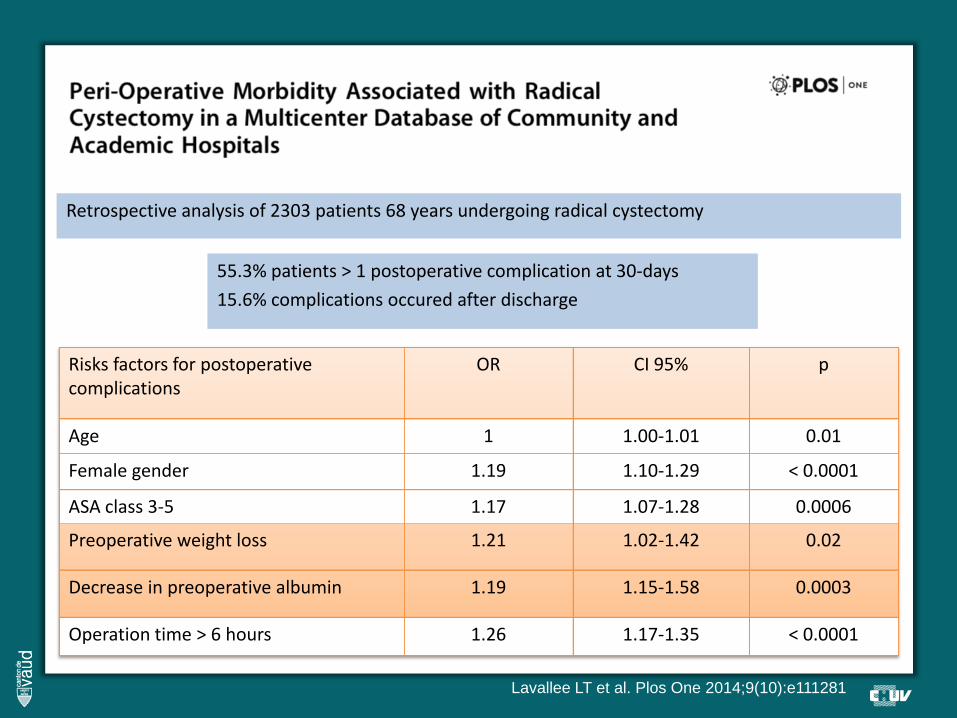
Retrospective analysis of 2303 patients 68 years undergoing radical cystectomy
Lavallee LT et al. Plos One 2014;9(10):e111281
55.3% patients > 1 postoperative complication at 30‐days15.6% complications occured after discharge
Risks factors for postoperativecomplications
OR CI 95% p
Age 1 1.00‐1.01 0.01
Female gender 1.19 1.10‐1.29 < 0.0001
ASA class 3‐5 1.17 1.07‐1.28 0.0006
Preoperative weight loss 1.21 1.02‐1.42 0.02
Decrease in preoperative albumin 1.19 1.15‐1.58 0.0003
Operation time > 6 hours 1.26 1.17‐1.35 < 0.0001

Mathur S and al. BJU Int 2008;101(8):973-7
11 patients 66 years radical cystectomy oral nutritionisotope measures and indirect calorimetry before surgery , after 2 weeks and 6 months
11% higher than predicted
Postoperative catabolic
muscle mass loss is not
regained by 6 months

Preoperative Standard Oral Nutrition Supplements vs Immunonutrition
Results of a Systematic Review and Meta-Analysis
Hegazi RA and al. J Am Coll Surg 2014;219(5):1078-87
Wound infection
Infectious complications
Non infectious complications
LOS
895 patients undergoing abdominal surgery in 9 RCTs of preoperative IN vs no ONS

60 patients undergoing radical cystectomy 7 days of preoperative IN vs no ONS
Bertrand J and al. World J Urol 2014;32(1):233-7

IS PREOPERATIVE FASTINGFROM MIDNIGHT USEFUL ?

Is preoperative fasting frommidnight indicated ?
• Surgical stress is associated withhyperglycemia and protein catabolism– increased cortisol– insulin resistance
• Insulin resistance is associated with– poor wound healing– infectious complications– prolonged length of stay

Is preoperative fasting frommidnight indicated ?
• Insulin resistance depends on– surgery extent– pain relief– hyperglycemia control– fasting time
• Solids up to 6 hours before surgery• Clear fluids up to 2 hours• … risk of aspiration and regurgitation ?

Preoperative fasting timeGastric emptying of water and other inert, non‐caloric fluids follows an extremely fastexponential curve with a mean half‐time of 10 min
Gastric emptying of solid food startsapproximately 1 h after a meal. Within 2 h, approximately 50% of the solid food ingestedis passed to the duodenum. The gastricemptying of solids is independent of the amount of food ingested but dependent on the caloric density of the meal.
Soreide E. Doctoral thesis Anaesthesia and gastric content. New methods and trends. 1995

Preoperative fasting time
27 RCTs 1976 patientsAbdominal (18), orthopaedic (4), cardiac (4), thyroid surgery (1)
At least 45 g carbohydrates within 4 hours before surgeryversus placebo or overnight fasting
No difference in the risk of postoperative complicationsNo report of aspiration pneumonitis
Increased insulin sensitivityShortened time to passage of flatus by 0.39 days
Shortened LOS by 0.30 days
Smith MD et al. Cochrane Database Syst Rev 2014;8:CD009161
Fluids evaluated included water, coffee, fruit juice, clearfluids and other drinks (isotonic or carbohydrate drink)

IS POSTOPERATIVEPARENTERAL NUTRITION INDICATED ?

Is postoperative parenteral nutrition indicated ?
• Metabolic complications• Nausea / Vomiting• Postoperative ileus

Metabolic complicationsDepend on bowel segment and length used
• Bowel dysfunction and fat malabsorption … diarrhea … hypokaliemia, hyponatremia, dehydration
• Acid-base abnormalities … metabolic acidosis in 10% patients with an ileal segment
• Bone demineralisation• Vitamin B12 deficiency … after 3-5 years• Hyperammonemia in hepatic disease… infection

Nausea - VomitingThe use of routine naso-gastric tube decompression shouldbe avoided after surgery and any tube placed duringsurgery should be removed prior to extubation
Inman BA et al. Urol 2003;170(5):1888-91
Retrospective analysis of 430 patients undergoing cystectomyEarly removal of nasogastric tube
Shortened time to first bowel sounds and first flatusShortened LOS
Decreased the incidence of fever, atelectasis and pneumonia

Postoperative ileus• Incidence of 1.6-23.5% • Increased length of stay
• Multiple causes– Bowel resection– Perception of pain … general and epidural anesthesia (at
thoracic level T9-T11)– Fluid overload … intraoperative management
– Mechanical bowel preparation– Fasting before surgery– Use of nasogastric tube

And chewing gum• Increases cephalo-vagal stimulation
– Increased gastric motility– Reduced inhibitory inputs from the sympathetic
nervous system
• Benefit in improving recovery of GI function
Short V et al. Cochrane Database Syst Rev 2015;2:CD006506
Meta‐analysis of 81 studies 9072 patients
Shortened time to first flatus 10.4 hoursShortened LOS of 0.7 days

Pham KN et al. WMJ 2014;113(1):20-3
Retrospective analysis of 174 patients undergoing radical cystectomy

32 % 11 %
Roth B et al. Eur Urol 2013;63(3):475-82

Non randomised prospective study of 94 patients undergoing cystectomy
Declercq P et al. Int J Clin Pharm 2015;37:379-86
Parenteral nutrition Oral nutrition


n=28 ~74.2 (55-82) y radical cystectomy with intestinal urinary reconstruction
Return of peristalsis 2 days (range 2-5)Reinstitution of regular diet 4 days (range 3-8)Postoperative ileus beyond POD 4 17,7% of the patients Complications 26,1% of the patients Mortality 3.7 %
Maffezzini M et al. J Urol 2006;176(3):948-9

Maffezzini M et al. Surg Oncol 2008;17(1):41-8
n=143 ~74 y radical cystectomy with intestinal urinary reconstruction
Return of peristalsis 2 days (range 1-6)Reinstitution of regular diet 4 days (range 3-9)Postoperative ileus beyond POD 4 17,7% of the patients Complications 26,1% of the patients Mortality 3.7 %
Thank you for your attention