erythrocyte catalase activity in more frequent microcytic
TRANSCRIPT

Research ArticleErythrocyte Catalase Activity in More FrequentMicrocytic Hypochromic Anemia Beta-ThalassemiaTrait and Iron Deficiency Anemia
Sandra Stella Lazarte1 Mariacutea Eugenia Moacutenaco12 Cecilia Laura Jimenez1
Miryam Emilse Ledesma Achem1 Magdalena Mariacutea Teraacuten1 and Blanca Alicia Isseacute1
1 Instituto de Bioquımica Aplicada Facultad de Bioquımica Quımica y Farmacia Universidad Nacional de Tucuman (UNT)Balcarce 747 San Miguel de Tucuman 4000 Tucuman Argentina2Instituto de Biologıa Facultad de Bioquımica Quımica y Farmacia Universidad Nacional de Tucuman Chacabuco 461San Miguel de Tucuman 4000 Tucuman Argentina
Correspondence should be addressed to Sandra Stella Lazarte slazartefbqfunteduar
Received 18 June 2015 Revised 10 September 2015 Accepted 16 September 2015
Academic Editor Elvira Grandone
Copyright copy 2015 Sandra Stella Lazarte et al This is an open access article distributed under the Creative Commons AttributionLicense which permits unrestricted use distribution and reproduction in any medium provided the original work is properlycited
Most common microcytic hypochromic anemias are iron deficiency anemia (IDA) and 120573-thalassemia trait (BTT) in whichoxidative stress (OxS) has an essential role Catalase causes detoxification of H2O2 in cells and it is an indispensable antioxidantenzyme The study was designed to measure erythrocyte catalase activity (ECAT) in patients with IDA (10) or BTT (21) to relateit with thalassemia mutation type (1205730 or 120573+) and to compare it with normal subjects (67) Ninety-eight individuals were analyzedsince September 2013 to June 2014 in Tucuman Argentina Total blood count hemoglobin electrophoresis at alkaline pH HbA2catalase and iron status were performed 120573-thalassemicmutations were determined by real-time PCR Normal range for ECATwas700ndash1300MUL ECATwas increased in 14 (321) of BTT subjects and decreased in 40 (410) of those with IDA No significantdifference (p = 0245) was shown between normal and BTT groups while between IDA and normal groups the difference wasproved to be significant (p = 0000) In 1205730 and 120573+ groups no significant difference (p = 0359) was observed An altered ECAT wasdetected in IDA and BTT These results will help to clarify how the catalase activity works in these anemia types
1 Introduction
Normal erythrocytes are protected against potentially dan-gerous combination of oxygen and iron (hemichromes andheme associated iron) for extremely efficient endogenousmechanisms such as superoxide dismutase (SOD) catalaseglutathione peroxidase (GPx) reduced glutathione and vita-min E Microcytosis is the physiological consequence ofreduced hemoglobin content in the red blood cell (RBC) dueto a synthesis defect of globin chains or heme [1] Experi-mental data in mice showed that the mitotic events duringdifferentiation are associated with a substantial reduction inthe mean corpuscular volume (MCV) [2] In addition tomorphological biochemical and metabolic changes smallcell erythrocytes are characterized by shorter survival being
the oxidative damage to RBCmembrane one of the underly-ing mechanisms responsible [3]
Microcytosis is defined by MCV lower than 80 fL andhypochromia through mean corpuscular hemoglobin lowerthan 27 pg Hypochromicmicrocytic anemiamay result froman iron deficiency (iron deficiency anemia) a defect in theglobin genes (hemoglobinopathies or thalassemia) a defectin heme synthesis (sideroblastic anemia) or a defect iniron availability and acquisition by erythroblast (anemia ofchronic disease)
According to World Health Organization (WHO) theprimary cause of anemia is iron deficiency especially inpregnant women and children [4] Regarding hemoglo-binopathies at present about 5 of world populationis carrier of a potentially pathological hemoglobin gene
Hindawi Publishing CorporationAdvances in HematologyVolume 2015 Article ID 343571 7 pageshttpdxdoiorg1011552015343571
2 Advances in Hematology
Beta- (120573-) thalassemia is the most common hemoglobinopa-thy in theMediterranean basin theMiddle East andAsia [5]Accordingly in Argentina 120573-thalassemia is the most com-mon inherited anemia [6ndash8] Therefore the most frequenthypochromic microcytic anemias are iron deficiency anemiaand 120573-thalassemia
There are two molecular forms of 120573-thalassemia 120573+thalassemia in which a small amount of 120573-globin chainsare detectable and 1205730 thalassemia in which they are unde-tectable Till this day there are over 200 gene mutationscapable of producing thalassemia phenotypes [9] Clinically120573-thalassemia is classified as minor (asymptomatic) or major(severe anemia) depending on the mutation responsible forthis alteration is present in heterozygous or homozygousstate There is also a moderate clinical features syndromeknown as thalassemia intermedia (homozygous or doubleheterozygous) In 120573-thalassemia as a result of 120573-chainsdecrease a relative alpha- (120572-) chains excess occurs [10]Free 120572-chains are unable to form viable tetramers andprecipitate in RBC precursors in bone marrow forminginclusion bodies called hemichromes They are responsiblefor the large intramedullary destruction of erythroblastsand therefore for ineffective erythropoiesis in 120573-thalassemia[11] Hemichromes also precipitate in membrane of matureRBC and cause changes in its structure which induce lipidperoxidation and exposure of anionic phospholipids whichtogether leads to premature clearance by the spleen [12]In both erythroid precursors and mature RBCs free ironresulting from heme denaturation produces damage to lipidsmembrane cellular proteins or DNA Free iron is toxicbecause it triggers Fenton reaction in which free radicals areformed increasing cellular oxidative stress (OxS) due to reac-tive oxygen species (ROS) production such as superoxidehydrogen peroxide (H2O2) and hydroxyl radicals [13]
Several studies have evaluated the oxidant and antiox-idant status in thalassemia major and intermedia [14 15]and in severe 120573-thalassemia it is difficult to evaluate the roleplayed by the antioxidant enzymes because of the relevantproportion of normal red cells due to multiple transfusionsFurthermore little is known about the oxidative status in 120573-thalassemia trait (BTT) subjects and its relationwith different120573-thalassemia mutations Such assessment is important dueto the large genotypic and phenotypic heterogeneity ofdifferent populations
The antioxidant system has been proposed as a biomarkerof OxS throughmeasuring detoxifying enzymes such as cata-lase [16] The enzyme was first discovered by Louis JacquesThenard in 1818 It is an intracellular enzyme constituted byfour polypeptide chains with four heme-porphyrin groupsThe human catalase gene (CAT NCBI Gene ID 847) is local-ized on the short arm of chromosome 11 (11p13) NM 0017523and NP 0017431 Catalase is responsible for detoxification ofH2O2 in cells [15] Decreased activity of catalase may leadto increased H2O2 concentration and damage of oxidationsensitive tissues that may contribute to the manifestation ofvarious diseases such as diabetes mellitus and anemia [17]
Iron deficiency affects activity of many iron-dependentenzymes (like catalase) and in iron deficiency anemia (IDA)
RBCs are more susceptible to oxidation RBCs from IDAsubjects lyse more readily than normal cells on in vitroexposure to H2O2 [18] suggesting some defect in the pro-tection mechanism of iron-deficient RBCs against oxidantdamage Increased hemoglobin autoxidation and subsequentgeneration of ROS can account for the shorter RBC lifespanand other pathological changes associated with IDA [19]Theliterature offers contradictory and limited data on oxidativestress and antioxidant defense in patients with IDA andincreased [20] and decreased catalase activity [21] have beenreported
The present study was designed to measure catalaseactivity in individuals suffering from some of the mostcommon microcytic hypochromic anemia that is IDA orBTT and to compare it with normal subjects It was alsoproposed to relate the type of 120573-thalassemia mutation withthe catalase activity
2 Materials and Methods
Design A descriptive cross-sectional study was conducted
Subjects The sample consisted of 31 patients who attendedInstituto de Bioquımica Aplicada (Tucuman Argentina) forthe diagnosis of hereditary anemia during the period ofSeptember 2013 up to June 2014 Sixty-seven normal individ-uals whose participation was voluntary were also includedBlood was drawn and placed in two different tubes onecontaining K2-EDTA anticoagulant and the other withoutanticoagulant with the purpose of obtaining serum
Inclusion Criteria Patients diagnosed with 120573-thalassemiaminor or iron deficiency anemia and normal subjects thatneeded to be older than 1 year old were included
Exclusion Criteria People under vitamin intake people whosmoke with diabetes coronary heart disease rheumatoidarthritis dyslipidemia hypertension malignancy chronicliver disease and renal dysfunction and patients under irontherapy during 21 days prior to analysis or who have receivedtransfusions in the last three months were excluded
Hematological Studies Total blood count was performed inhematology analyzer Sysmex KX-21N (Kobe Japan) Thediagnosis of the 120573-thalassemia trait was performed by cellu-lose acetate hemoglobin (Hb) electrophoresis at alkaline pHand HbA2 quantification by microcolumn chromatography(BioSystems Barcelona Spain) IDA diagnosis was madeby determining serum iron total iron binding capacity(TIBC) and transferrin saturation (SAT) through colorimet-ricmethod (Wiener Lab Rosario Argentina) SAT lower than16 was considered diagnostic of IDA
Erythrocyte Catalase Activity (ECAT) The enzyme was ana-lyzed in K2-EDTA anticoagulated whole blood using Gothtechnique [22] Absorbance (119860) of the yellow complexof molybdate and hydrogen peroxide was measured at405 nm against blank 3 Sample contained 10mL substrate(65 120583molmL H2O2 in 60mmolL sodium-potassium buffer
Advances in Hematology 3
pH 74) and 30 120583L hemolysate and after 60 seconds the enzy-matic reaction was stopped by adding 10mL of 324mmolLammonium molybdate Blank 1 contained 10mL substrate10mL molybdate and 30 120583L hemolysate blank 2 contained10mL substrate 10mLmolybdate and 30120583L buffer blank 3contained 10mL buffer 10mL molybdate and 30 120583L bufferOne unit of catalase decomposes 1 120583mol of H2O2 in 1 minuteunder these conditions and it is related to 1 L of whole bloodCatalase activity was expressed in Mega UnitsL (MUL) andwas calculated with the following formula
Erythrocyte catalase activity [MUL]
=[119860 (blank 1) minus 119860 (sample)] times 426 times 100119860 (blank 2) minus 119860 (blank 3)
(1)
Molecular Analysis Characterization of 120573-thalassemic muta-tions was realized by real-time PCR Genomic DNA isola-tion was performed with High Pure PCR Template Prepa-ration Kit (Roche Diagnostics) PCR dissociation curvesand subsequent analysis were executed on the LightCycler20 (Roche) equipment simultaneously measuring signalsfrom two different fluorophores Primers were designed toamplify a 587 bp region of 120573-globin gene Forward Primer51015840-gctgtcatc act acctca tag-31015840 Reverse Primer 51015840-gct gcaagt-caccactca g-31015840 Two combinations of hybridization probeslabeled with different fluorophores were used [23]
Statistical Analysis Results were analyzed using SPSS 210statistical program The results were reported as Media plusmnStandard Deviation For comparison Student 119905-Test andANOVA were used A significance level of p lt 005 wasadopted The influence of iron serum on catalase valuesindependent of the group (normal IDA or BTT) wasevaluated by simple regression analysis
3 Results
Ninety-eight individuals were studied of which 67 were nor-mal (N group) 21 with 120573-thalassemia trait (BTT group) and10 with iron deficiency anemia (IDA group) Table 1 showsthe results for catalase activity hematological parameters andiron status in all BTT and IDA patients Subjects were dividedaccording to age children (le12 years) adolescents (13ndash18years) adults (19ndash59 years) and older adults (ge60 years)ANOVA detected no significant differences (119901 = 0187) inECAT between the stated groups
Five individuals who were more than 60 years old werenormal (567 75) 2 120573-thalassemia carriers (221 95)and 2 IDA (210 20) Only one of these subjects whichbelonged to the normal group showed increased catalaseactivity (139MUL) Apparently age has no influence in theECAT of this population
In order to establish the normal range of catalase activity5th and 95th percentiles of N group results were determinedA range from 700 to 1300MUL was obtained
Increased catalase activity in 14 (321) of BTT subjectswas observed No significant differences (119901 = 0245) wereobserved when N and BTT groups were compared
Cata
lase
(MU
L)
N BTT IDA
500
1000
1500
Figure 1 Erythrocyte catalase activity in 120573-thalassemia minor irondeficiency anemia and normal subjects 119901 lt 005 between IDAand N groups N normal IDA iron deficiency anemia BTT 120573-thalassemia trait
Four IDA individuals (40) showed decreased catalaseactivity No significant differences between men and womenwere detected in all groups When N and IDA groups werecompared significant difference (119901 = 0000) was observedsince the IDA subjects had lower values than N group(Figure 1)
Table 2 shows the results in N BTT and IDA groupsaccording to sex Female IDA subjects have significant differ-ences (119901 lt 005) with normal group in all parameters exceptTIBC Catalase in male IDA patients did not demonstratesignificant differences (119901 gt 005) when compared withnormal and BTT groups
The 120573-thalassemia mutations detected in order of fre-quency were codon 39 (CrarrT) (5 subjects) IVS-I-110 (GrarrA) (5 subjects) IVS-I-1 (GrarrA) (4 subjects) and IVS-I-6 (TrarrC) (2 subjects) and in 5 cases the mutation couldnot be assigned The small number of patients for eachgroup prevented the comparative study between themThere-fore differences between 1205730 (9 subjects ECAT = 1046 plusmn316MUL) and 120573+ (7 subjects ECAT = 918 plusmn 174MUL)groups were studied which were not significant (119901 = 0359)
There was no influence of iron levels on catalase values(1199032 = 0153) in these samples
4 Discussion
Oxidative stress is defined as the interruption of balancebetween oxidants and reductants within the body due tothe excess production of peroxides and free radicals Duringthe course of metabolism superoxide anion is convertedto H2O2 by ubiquitous enzyme SOD Normally H2O2 isconverted to innocuous compounds by the action of catalaseand peroxidase But if free iron is available it reacts withH2O2 to form hydroxyl radicals which are extremely reac-tive species leading to depolymerisation of polysaccharideDNA strand breakage inactivation of functional proteinsand other events [24] Therefore this imbalance will cause
4 Advances in Hematology
Table 1 Laboratory data of 120573-thalassemia trait and iron deficiency anemia patients
Groups Age[years]
HTO[LL]
HB[gL]
ECAT[MUL]
Fe[120583gdL]
TIBC[120583gdL]
SAT[]
IDA groupFemale (6)P1 3 026 64 1162 13 262 5P2 14 034 103 543 25 444 6P3 76 037 118 610 33 293 11P4 44 035 101 598 29 313 9P5 43 038 117 813 43 358 12P6 15 017 38 370 31 397 8
Male (4)P1 1 033 97 904 15 352 4P2 1 031 89 834 18 323 6P3 11 031 79 717 25 216 12P4 63 040 115 770 32 403 8
BTT groupFemale (15)P1 12 035 106 953 78 297 26P2 10 033 100 873 75 380 20P3 57 037 107 1139 34 233 15P4 48 039 121 888 80 247 32P5 33 037 108 879 90 285 31P6 33 036 103 835 63 203 31P7 34 034 104 836 50 180 28P8 38 038 115 1062 176 341 52P9 63 038 110 730 81 238 34P10 56 036 106 798 100 220 45P11 11 035 105 752 103 322 32P12 32 037 111 1279 80 228 35P13 22 035 104 865 104 332 31P14 28 037 114 1622 71 258 28P15 26 034 101 1401 83 283 29
Male (6)P1 45 039 115 1354 259 266 97P2 1 032 93 744 29 347 8P3 12 038 112 934 66 244 27P4 65 047 142 1073 144 318 45P5 21 040 121 1133 127 208 61P6 16 041 126 1000 58 247 23
HTO hematocrit HB hemoglobin ECAT erythrocyte catalase activity Fe serum iron TIBC total iron binding capacity SAT transferrin saturation IDAiron deficiency anemia BTT 120573-thalassemia trait P patient
damage to cellular components and tissues in the bodyleading to OxS and catalase has a role in it
Kosa et al [25] revealed a significant decrease in cata-lase activity of 43 120573-thalassemia carriers and attributed itto catalase protein damage by increased free radicals andH2O2 Another study reported increased levels of antioxi-dant enzymes like SOD catalase and GPx in RBCs of 120573-thalassemia minor individuals and near normal values of
these enzymes in RBCs of 120573-thalassemia major patients[26] They concluded that 120573-thalassemia minor RBCs reactto increased OxS rising activities of antioxidant enzymeswhile in 120573-thalassemia major normal antioxidant enzymelevels are due to the presence of normal RBCs from multipleblood transfusions However Boudrahem-Addour et al [27]observed a significant increase (119901 lt 005) of catalase activityin 120573-thalassemia major and intermedia The present results
Advances in Hematology 5
Table 2 Hematological parameters iron status and catalase according to pathology and sex (Media plusmn Standard Deviation)
PathologySex
Age[years]
HTO[LL]
HB[gL]
ECAT[MUL]
Fe[120583gdL]
TIBC[120583gdL]
SAT[]
IDA groupFemale (6) 20 plusmn 19 031 plusmn 008lowastDagger 90 plusmn 32lowastDagger 683 plusmn 274lowastDagger 29 plusmn 10lowastDagger 344 plusmn 68Dagger 8 plusmn 3lowastDagger
Male (4) 19 plusmn 30 034 plusmn 004lowast 95 plusmn 15lowast 806 plusmn 81 22 plusmn 8lowast 324 plusmn 79 7 plusmn 3lowast
BTT groupFemale (15) 34 plusmn 17 036 plusmn 002dagger 108 plusmn 6dagger 994 plusmn 259 84 plusmn 32 270 plusmn 56 31 plusmn 9Male (6) 27 plusmn 6 039 plusmn 005dagger 118 plusmn 16dagger 1040 plusmn 204 114 plusmn 83 272 plusmn 52 44 plusmn 32
N groupFemale (39) 36 plusmn 13 041 plusmn 002 137 plusmn 10 968 plusmn 175 81 plusmn 18 301 plusmn 54 28 plusmn 11Male (28) 37 plusmn 15 044 plusmn 002 147 plusmn 9 931 plusmn 154 94 plusmn 28 282 plusmn 38 34 plusmn 11
lowast119901 lt 005 between IDA and N groups by sex dagger119901 lt 005 between BTT and N groups by sex Dagger119901 lt 005 between IDA and BTT womenIDA iron deficiency anemia BTT 120573-thalassemia trait N normal HTO hematocrit HB hemoglobin ECAT erythrocyte catalase activity Fe iron TIBC totaliron binding capacity SAT transferrin saturation
in concordance with Gerli et al [26] showed that some BTTsubjects had increased catalase activity
Several authors reported increased antioxidant capacityin BTT individuals but they do notmeasured catalase activity[28 29] Instead they used a novel automated measurementmethod and Trolox equivalent antioxidant capacity
In the catalase activity comparison between 1205730 and 120573+thalassemia traits the results were not significant Also Kosaet al [25] did not find significant differences and concludedthat catalase activity was not related to specific 120573-thalassemiamutations Furthermore Labib et al [30] reported no differ-ences in total antioxidant capacity of 1205730 and 120573+ thalassemiatraits
The normal range of erythrocyte catalase activity wasslightly lower than the one reported by another authors [31]which was 803 to 1463MUL Difference may be due to theracial characteristics of the population methodological dif-ferences and because they used 25th and 975th percentiles toestablish normal range Men and women have no significantdifferences in what catalase activity concerns Instead Vitaiand Goth [31] found slightly higher values in male subjects
In this study like Ondei et al [29] there was no rela-tionship between ECAT and iron serum In 120573-thalassemiamajor and intermedia iron excess can lead to organ damageespecially in liver and heart and to endocrine dysfunction[32] Recent studies have shown the importance of othermarkers such as non-transferrin bound iron (NTBI) andlabile plasma iron (LPI) to detect iron excess in thalassemiapatients due to the direct correlation of these markers withthe formation of free radicals [33]
Decreasing serum iron concentration causes insufficientHb synthesis with subsequent reduction of erythrocytes pro-liferation Iron deficiency also affects the production of otheriron-containing proteins such as cytochrome myoglobincatalase and peroxidase Therefore a decreased catalaseactivity could be anticipated in iron deficiency and has beencorroborated in this study in agreement with other works[21 34 35] However Madhikarmi andMurthy [20] detectedan unexplained increase of catalase activity in IDA andTekin et al [36] reported no differences in SOD and catalase
activities between IDA patients and controls Bay et al [37]compared antioxidant capacity between IDA and normalsubjects and detected no significant differences
Increased OxS have been reported in patients with IDA[3 21 35] which occurs primarily in RBC membrane ROSmembrane surface contributes to deformability alteration[38] and phosphatidylserine exposure which have been usedto explain the reduction of RBCs life in IDA [39] Alsoin BTT an altered oxidative state was reported by someinvestigators [28 30] Therefore OxS is present in the mostcommon hypochromic microcytic anemia IDA and BTTbeing one of the determining factors of altered catalaseactivity Hypochromic microcytic RBCs of BTT and IDAindividuals have been studied in the past decades and OxScontribution in reducing the RBCs useful life has beendocumented Previous studies on the catalase activity ofhypochromic microcytic anemia such as IDA and BTT havereported disagreeing results [20 21 25 26 34 35] In thepresent work catalase activity was decreased in IDA andincreased in some BTT subjects with no significant differ-ences between beta-thalassemia mutationsThese results willhelp to clarify how the catalase activity works in these anemiatypesThe lownumber of samples is a limitation of this reportProbably the incorporation of a larger number of participantswill allow revealing hidden differences in current work
Consent
All patients signed an informed consent previously approvedby the Comite de Bioetica de la Facultad de Medicina UNT
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
This work was supported by grants from the Consejo deInvestigaciones de la Universidad Nacional de Tucuman
6 Advances in Hematology
(CIUNT 26D520) The authors thank Biochemist SpecialistGuillermo Fabian Vechetti and Laboratorio Tucuman for theuse of its molecular biology equipment
References
[1] A Lolascon L De Falco and C Beaumont ldquoMolecular basis ofinheritedmicrocytic anemia due to defects in iron acquisitionorheme synthesisrdquo Haematologica vol 94 no 3 pp 395ndash4082009
[2] A Coopersmith andM Ingram ldquoRed cell volumes and erythro-poiesis II Age density volume relationships of macrocytesrdquoAmerican Journal of Physiology vol 216 no 3 pp 473ndash4821969
[3] J L V Corrons A Miguel-Garcia M A Pujades et alldquoIncreased susceptibility ofmicrocytic red blood cells to in vitrooxidative stressrdquo European Journal of Haematology vol 55 no5 pp 327ndash331 1995
[4] WHO Global Database on Anaemia Worldwide Prevalenceof Anaemia 1993ndash2005 2008 httpwhqlibdocwhointpublications20089789241596657 engpdf
[5] OMS ldquoTalasemia y otras hemoglobinopatıas Informe dela Secretarıardquo mayo de 2006 httpappswhointgbarchivepdf filesEB118B118 5-sppdf
[6] M S Abreu and J A Penalver ldquoS hemoglobinopathies inArgentinardquoMedicina (Buenos Aires) vol 52 no 4 pp 341ndash3461992
[7] S Lazarte B Isse and G Aguero ldquoHemoglobinophaties andthalassemia syndromes in Tucuman preliminary studyrdquoBiocellvol 25 no 1 2001
[8] A Larregina E Reimer N Suldrup S Luis J Zavatti andN NPolini ldquoDiagnostico diferencial de anemias microcıticasrdquo ActaBioquimica Clinica Latinoamericana vol 38 no 4 pp 465ndash4692004
[9] S LThein ldquoThemolecular basis of 120573-thalassemiardquo Cold SpringHarbor Perspectives inMedicine vol 3 no 5 Article ID a0117002013
[10] B E Clark and S L Thein ldquoMolecular diagnosis ofhaemoglobin disordersrdquo Clinical and Laboratory Haematologyvol 26 no 3 pp 159ndash176 2004
[11] S L Thein ldquoPathophysiology of beta thalassemiamdasha guide tomolecular therapiesrdquoHematologyAmerican Society of Hematol-ogy Education Program pp 31ndash37 2005
[12] M D Cappellini D Tavazzi L Duca et al ldquoMetabolic indica-tors of oxidative stress correlate with haemichrome attachmentto membrane band 3 aggregation and erythrophagocytosis in120573-thalassaemia intermediardquoBritish Journal of Haematology vol104 no 3 pp 504ndash512 1999
[13] R Evstatiev and C Gasche ldquoIron sensing and signallingrdquo Gutvol 61 no 6 pp 933ndash952 2012
[14] C Kattamis C Lazaropoulou P Delaporta F Apostolakou AKattamis and I Papassotiriou ldquoDisturbances of biomarkers ofiron and oxidant-antioxidant homeostasis in patients with beta-thalassemia intermediardquo Pediatric Endocrinology Reviews vol8 pp 256ndash262 2011
[15] Q Shazia Z H Mohammad T Rahman and H U ShekharldquoCorrelation of oxidative stress with serum trace elementlevels and antioxidant enzyme status in beta thalassemia majorpatients a review of the literaturerdquoAnemia vol 2012 Article ID270923 7 pages 2012
[16] E Fibach and E Rachmilewitz ldquoThe role of oxidative stress inhemolytic anemiardquoCurrentMolecularMedicine vol 8 no 7 pp609ndash619 2008
[17] T Nagy E Paszti M Kaplar H P Bhattoa and L Goth ldquoFur-ther acatalasemia mutations in human patients from Hungarywith diabetes and microcytic anemiardquo Mutation ResearchmdashFundamental and Molecular Mechanisms of Mutagenesis vol772 pp 10ndash14 2015
[18] L G Macdougall ldquoRed cell metabolism in iron deficiencyanemia III The relationship between glutathione peroxidasecatalase serum vitamin E and susceptibility of iron-deficientred cells to oxidative hemolysisrdquo The Journal of Pediatrics vol80 no 5 pp 775ndash782 1972
[19] ENagababu S Gulyani C J Earley R G CutlerM PMattsonand JM Rifkind ldquoIron-deficiency anaemia enhances red bloodcell oxidative stressrdquo Free Radical Research vol 42 no 9 pp824ndash829 2008
[20] N L Madhikarmi and K R S Murthy ldquoAntioxidant enzymesand oxidative stress in the erythrocytes of iron deficiency ane-mic patients supplemented with vitaminsrdquo Iranian BiomedicalJournal vol 18 no 2 pp 82ndash87 2014
[21] E Kurtoglu A Ugur A K Baltaci and L Undar ldquoEffect of ironsupplementation on oxidative stress and antioxidant status iniron-deficiency anemiardquo Biological Trace Element Research vol96 no 1ndash3 pp 117ndash123 2003
[22] L Goth ldquoTwo cases of acatalasemia in Hungaryrdquo ClinicaChimica Acta vol 207 no 1-2 pp 155ndash158 1992
[23] S S Lazarte M E Monaco A C Haro C L Jimenez ME Ledesma Achem and B A Isse ldquoMolecular characteriza-tion and phenotypical study of 120573-thalassemia in TucumanArgentinardquo Hemoglobin vol 38 no 6 pp 394ndash401 2014
[24] F Simsek G Ozturk S Kemahli D Erbas and A HasanogluldquoOxidant and antioxidant status in beta thalassemia majorpatientsrdquo Ankara Universitesi Tıp Fakultesi Mecmuası vol 58pp 34ndash38 2005
[25] Z Kosa T Nagy E Nagy F Fazakas and L Goth ldquoDecreasedblood catalase activity is not related to specific beta-thalassemiamutations in Hungaryrdquo International Journal of LaboratoryHematology vol 34 no 2 pp 172ndash178 2012
[26] G C Gerli L Beretta M Bianchi A Pellegatta and AAgostoni ldquoErythrocyte superoxide dismutase catalase andglutathione peroxidase activities in 120573-thalassemia (major andminor)rdquo Scandinavian Journal of Haematology vol 25 no 1 pp87ndash92 1980
[27] N Boudrahem-Addour M Izem-Meziane K Bouguerra etal ldquoOxidative status and plasma lipid profile in 120573-thalassemiapatientsrdquo Hemoglobin vol 39 no 1 pp 36ndash41 2015
[28] S Selek M Aslan M Horoz M Gur and O Erel ldquoOxidativestatus and serum PON1 activity in beta-thalassemia minorrdquoClinical Biochemistry vol 40 no 5-6 pp 287ndash291 2007
[29] L D S Ondei I D F Estevao M I P Rocha et al ldquoOxidativestress and antioxidant status in beta-thalassemia heterozygotesrdquoRevista Brasileira de Hematologia e Hemoterapia vol 35 no 6pp 409ndash413 2013
[30] H A Labib R L Etewa O A Gaber M Atfy T M Mostafaand I Barsoum ldquoParaoxonase-1 and oxidative status in com-mon Mediterranean 120573-thalassaemia mutations trait and theirrelations to atherosclerosisrdquo Journal of Clinical Pathology vol64 no 5 pp 437ndash442 2011
[31] M Vitai and L Goth ldquoReference ranges of normal blood cata-lase activity and levels in familial hypocatalasemia in HungaryrdquoClinica Chimica Acta vol 261 no 1 pp 35ndash42 1997
Advances in Hematology 7
[32] S Gardenghi R W Grady and S Rivella ldquoAnemia ineffectiveerythropoiesis and hepcidin interacting factors in abnormaliron metabolism leading to iron overload in 120573-thalassemiardquoHematologyOncology Clinics of North America vol 24 no 6pp 1089ndash1107 2010
[33] P BrissotM Ropert C Le Lan andO Loreal ldquoNon-transferrinbound iron a key role in iron overload and iron toxicityrdquoBiochimica et Biophysica ActamdashGeneral Subjects vol 1820 no3 pp 403ndash410 2012
[34] F Amirkhizi F Siassi S Minaie M Djalali A Rahimi andM Chamari ldquoAssessment of lipid peroxidation and activitiesof erythrocyte cytoprotective enzymes in women with irondeficiency anemiardquo Journal of Research in Medical Sciences vol13 no 5 pp 248ndash254 2008
[35] J-H Yoo H-Y Maeng Y-K Sun et al ldquoOxidative status iniron-deficiency anemiardquo Journal of Clinical Laboratory Analysisvol 23 no 5 pp 319ndash323 2009
[36] D Tekin S Yavuzer M Tekin N Akar and S Cin ldquoPossibleeffects of antioxidant status on increased platelet aggregation inchildhood iron-deficiency anemiardquoPediatrics International vol43 no 1 pp 74ndash77 2001
[37] A Bay M Dogan K Bulan S Kaba N Demir and A FOner ldquoA study on the effects of pica and iron-deficiency anemiaon oxidative stress antioxidant capacity and trace elementsrdquoHuman and Experimental Toxicology vol 32 no 9 pp 895ndash9032013
[38] A Vaya M Simo M Santaolaria J Todolı and J Aznar ldquoRedblood cell deformability in iron deficiency anaemiardquo ClinicalHemorheology and Microcirculation vol 33 no 1 pp 75ndash802005
[39] D S Kempe P A Lang C Duranton et al ldquoEnhancedprogrammed cell death of iron-deficient erythrocytesrdquo TheFASEB Journal vol 20 no 2 pp 368ndash370 2006
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 Advances in Hematology
Beta- (120573-) thalassemia is the most common hemoglobinopa-thy in theMediterranean basin theMiddle East andAsia [5]Accordingly in Argentina 120573-thalassemia is the most com-mon inherited anemia [6ndash8] Therefore the most frequenthypochromic microcytic anemias are iron deficiency anemiaand 120573-thalassemia
There are two molecular forms of 120573-thalassemia 120573+thalassemia in which a small amount of 120573-globin chainsare detectable and 1205730 thalassemia in which they are unde-tectable Till this day there are over 200 gene mutationscapable of producing thalassemia phenotypes [9] Clinically120573-thalassemia is classified as minor (asymptomatic) or major(severe anemia) depending on the mutation responsible forthis alteration is present in heterozygous or homozygousstate There is also a moderate clinical features syndromeknown as thalassemia intermedia (homozygous or doubleheterozygous) In 120573-thalassemia as a result of 120573-chainsdecrease a relative alpha- (120572-) chains excess occurs [10]Free 120572-chains are unable to form viable tetramers andprecipitate in RBC precursors in bone marrow forminginclusion bodies called hemichromes They are responsiblefor the large intramedullary destruction of erythroblastsand therefore for ineffective erythropoiesis in 120573-thalassemia[11] Hemichromes also precipitate in membrane of matureRBC and cause changes in its structure which induce lipidperoxidation and exposure of anionic phospholipids whichtogether leads to premature clearance by the spleen [12]In both erythroid precursors and mature RBCs free ironresulting from heme denaturation produces damage to lipidsmembrane cellular proteins or DNA Free iron is toxicbecause it triggers Fenton reaction in which free radicals areformed increasing cellular oxidative stress (OxS) due to reac-tive oxygen species (ROS) production such as superoxidehydrogen peroxide (H2O2) and hydroxyl radicals [13]
Several studies have evaluated the oxidant and antiox-idant status in thalassemia major and intermedia [14 15]and in severe 120573-thalassemia it is difficult to evaluate the roleplayed by the antioxidant enzymes because of the relevantproportion of normal red cells due to multiple transfusionsFurthermore little is known about the oxidative status in 120573-thalassemia trait (BTT) subjects and its relationwith different120573-thalassemia mutations Such assessment is important dueto the large genotypic and phenotypic heterogeneity ofdifferent populations
The antioxidant system has been proposed as a biomarkerof OxS throughmeasuring detoxifying enzymes such as cata-lase [16] The enzyme was first discovered by Louis JacquesThenard in 1818 It is an intracellular enzyme constituted byfour polypeptide chains with four heme-porphyrin groupsThe human catalase gene (CAT NCBI Gene ID 847) is local-ized on the short arm of chromosome 11 (11p13) NM 0017523and NP 0017431 Catalase is responsible for detoxification ofH2O2 in cells [15] Decreased activity of catalase may leadto increased H2O2 concentration and damage of oxidationsensitive tissues that may contribute to the manifestation ofvarious diseases such as diabetes mellitus and anemia [17]
Iron deficiency affects activity of many iron-dependentenzymes (like catalase) and in iron deficiency anemia (IDA)
RBCs are more susceptible to oxidation RBCs from IDAsubjects lyse more readily than normal cells on in vitroexposure to H2O2 [18] suggesting some defect in the pro-tection mechanism of iron-deficient RBCs against oxidantdamage Increased hemoglobin autoxidation and subsequentgeneration of ROS can account for the shorter RBC lifespanand other pathological changes associated with IDA [19]Theliterature offers contradictory and limited data on oxidativestress and antioxidant defense in patients with IDA andincreased [20] and decreased catalase activity [21] have beenreported
The present study was designed to measure catalaseactivity in individuals suffering from some of the mostcommon microcytic hypochromic anemia that is IDA orBTT and to compare it with normal subjects It was alsoproposed to relate the type of 120573-thalassemia mutation withthe catalase activity
2 Materials and Methods
Design A descriptive cross-sectional study was conducted
Subjects The sample consisted of 31 patients who attendedInstituto de Bioquımica Aplicada (Tucuman Argentina) forthe diagnosis of hereditary anemia during the period ofSeptember 2013 up to June 2014 Sixty-seven normal individ-uals whose participation was voluntary were also includedBlood was drawn and placed in two different tubes onecontaining K2-EDTA anticoagulant and the other withoutanticoagulant with the purpose of obtaining serum
Inclusion Criteria Patients diagnosed with 120573-thalassemiaminor or iron deficiency anemia and normal subjects thatneeded to be older than 1 year old were included
Exclusion Criteria People under vitamin intake people whosmoke with diabetes coronary heart disease rheumatoidarthritis dyslipidemia hypertension malignancy chronicliver disease and renal dysfunction and patients under irontherapy during 21 days prior to analysis or who have receivedtransfusions in the last three months were excluded
Hematological Studies Total blood count was performed inhematology analyzer Sysmex KX-21N (Kobe Japan) Thediagnosis of the 120573-thalassemia trait was performed by cellu-lose acetate hemoglobin (Hb) electrophoresis at alkaline pHand HbA2 quantification by microcolumn chromatography(BioSystems Barcelona Spain) IDA diagnosis was madeby determining serum iron total iron binding capacity(TIBC) and transferrin saturation (SAT) through colorimet-ricmethod (Wiener Lab Rosario Argentina) SAT lower than16 was considered diagnostic of IDA
Erythrocyte Catalase Activity (ECAT) The enzyme was ana-lyzed in K2-EDTA anticoagulated whole blood using Gothtechnique [22] Absorbance (119860) of the yellow complexof molybdate and hydrogen peroxide was measured at405 nm against blank 3 Sample contained 10mL substrate(65 120583molmL H2O2 in 60mmolL sodium-potassium buffer
Advances in Hematology 3
pH 74) and 30 120583L hemolysate and after 60 seconds the enzy-matic reaction was stopped by adding 10mL of 324mmolLammonium molybdate Blank 1 contained 10mL substrate10mL molybdate and 30 120583L hemolysate blank 2 contained10mL substrate 10mLmolybdate and 30120583L buffer blank 3contained 10mL buffer 10mL molybdate and 30 120583L bufferOne unit of catalase decomposes 1 120583mol of H2O2 in 1 minuteunder these conditions and it is related to 1 L of whole bloodCatalase activity was expressed in Mega UnitsL (MUL) andwas calculated with the following formula
Erythrocyte catalase activity [MUL]
=[119860 (blank 1) minus 119860 (sample)] times 426 times 100119860 (blank 2) minus 119860 (blank 3)
(1)
Molecular Analysis Characterization of 120573-thalassemic muta-tions was realized by real-time PCR Genomic DNA isola-tion was performed with High Pure PCR Template Prepa-ration Kit (Roche Diagnostics) PCR dissociation curvesand subsequent analysis were executed on the LightCycler20 (Roche) equipment simultaneously measuring signalsfrom two different fluorophores Primers were designed toamplify a 587 bp region of 120573-globin gene Forward Primer51015840-gctgtcatc act acctca tag-31015840 Reverse Primer 51015840-gct gcaagt-caccactca g-31015840 Two combinations of hybridization probeslabeled with different fluorophores were used [23]
Statistical Analysis Results were analyzed using SPSS 210statistical program The results were reported as Media plusmnStandard Deviation For comparison Student 119905-Test andANOVA were used A significance level of p lt 005 wasadopted The influence of iron serum on catalase valuesindependent of the group (normal IDA or BTT) wasevaluated by simple regression analysis
3 Results
Ninety-eight individuals were studied of which 67 were nor-mal (N group) 21 with 120573-thalassemia trait (BTT group) and10 with iron deficiency anemia (IDA group) Table 1 showsthe results for catalase activity hematological parameters andiron status in all BTT and IDA patients Subjects were dividedaccording to age children (le12 years) adolescents (13ndash18years) adults (19ndash59 years) and older adults (ge60 years)ANOVA detected no significant differences (119901 = 0187) inECAT between the stated groups
Five individuals who were more than 60 years old werenormal (567 75) 2 120573-thalassemia carriers (221 95)and 2 IDA (210 20) Only one of these subjects whichbelonged to the normal group showed increased catalaseactivity (139MUL) Apparently age has no influence in theECAT of this population
In order to establish the normal range of catalase activity5th and 95th percentiles of N group results were determinedA range from 700 to 1300MUL was obtained
Increased catalase activity in 14 (321) of BTT subjectswas observed No significant differences (119901 = 0245) wereobserved when N and BTT groups were compared
Cata
lase
(MU
L)
N BTT IDA
500
1000
1500
Figure 1 Erythrocyte catalase activity in 120573-thalassemia minor irondeficiency anemia and normal subjects 119901 lt 005 between IDAand N groups N normal IDA iron deficiency anemia BTT 120573-thalassemia trait
Four IDA individuals (40) showed decreased catalaseactivity No significant differences between men and womenwere detected in all groups When N and IDA groups werecompared significant difference (119901 = 0000) was observedsince the IDA subjects had lower values than N group(Figure 1)
Table 2 shows the results in N BTT and IDA groupsaccording to sex Female IDA subjects have significant differ-ences (119901 lt 005) with normal group in all parameters exceptTIBC Catalase in male IDA patients did not demonstratesignificant differences (119901 gt 005) when compared withnormal and BTT groups
The 120573-thalassemia mutations detected in order of fre-quency were codon 39 (CrarrT) (5 subjects) IVS-I-110 (GrarrA) (5 subjects) IVS-I-1 (GrarrA) (4 subjects) and IVS-I-6 (TrarrC) (2 subjects) and in 5 cases the mutation couldnot be assigned The small number of patients for eachgroup prevented the comparative study between themThere-fore differences between 1205730 (9 subjects ECAT = 1046 plusmn316MUL) and 120573+ (7 subjects ECAT = 918 plusmn 174MUL)groups were studied which were not significant (119901 = 0359)
There was no influence of iron levels on catalase values(1199032 = 0153) in these samples
4 Discussion
Oxidative stress is defined as the interruption of balancebetween oxidants and reductants within the body due tothe excess production of peroxides and free radicals Duringthe course of metabolism superoxide anion is convertedto H2O2 by ubiquitous enzyme SOD Normally H2O2 isconverted to innocuous compounds by the action of catalaseand peroxidase But if free iron is available it reacts withH2O2 to form hydroxyl radicals which are extremely reac-tive species leading to depolymerisation of polysaccharideDNA strand breakage inactivation of functional proteinsand other events [24] Therefore this imbalance will cause
4 Advances in Hematology
Table 1 Laboratory data of 120573-thalassemia trait and iron deficiency anemia patients
Groups Age[years]
HTO[LL]
HB[gL]
ECAT[MUL]
Fe[120583gdL]
TIBC[120583gdL]
SAT[]
IDA groupFemale (6)P1 3 026 64 1162 13 262 5P2 14 034 103 543 25 444 6P3 76 037 118 610 33 293 11P4 44 035 101 598 29 313 9P5 43 038 117 813 43 358 12P6 15 017 38 370 31 397 8
Male (4)P1 1 033 97 904 15 352 4P2 1 031 89 834 18 323 6P3 11 031 79 717 25 216 12P4 63 040 115 770 32 403 8
BTT groupFemale (15)P1 12 035 106 953 78 297 26P2 10 033 100 873 75 380 20P3 57 037 107 1139 34 233 15P4 48 039 121 888 80 247 32P5 33 037 108 879 90 285 31P6 33 036 103 835 63 203 31P7 34 034 104 836 50 180 28P8 38 038 115 1062 176 341 52P9 63 038 110 730 81 238 34P10 56 036 106 798 100 220 45P11 11 035 105 752 103 322 32P12 32 037 111 1279 80 228 35P13 22 035 104 865 104 332 31P14 28 037 114 1622 71 258 28P15 26 034 101 1401 83 283 29
Male (6)P1 45 039 115 1354 259 266 97P2 1 032 93 744 29 347 8P3 12 038 112 934 66 244 27P4 65 047 142 1073 144 318 45P5 21 040 121 1133 127 208 61P6 16 041 126 1000 58 247 23
HTO hematocrit HB hemoglobin ECAT erythrocyte catalase activity Fe serum iron TIBC total iron binding capacity SAT transferrin saturation IDAiron deficiency anemia BTT 120573-thalassemia trait P patient
damage to cellular components and tissues in the bodyleading to OxS and catalase has a role in it
Kosa et al [25] revealed a significant decrease in cata-lase activity of 43 120573-thalassemia carriers and attributed itto catalase protein damage by increased free radicals andH2O2 Another study reported increased levels of antioxi-dant enzymes like SOD catalase and GPx in RBCs of 120573-thalassemia minor individuals and near normal values of
these enzymes in RBCs of 120573-thalassemia major patients[26] They concluded that 120573-thalassemia minor RBCs reactto increased OxS rising activities of antioxidant enzymeswhile in 120573-thalassemia major normal antioxidant enzymelevels are due to the presence of normal RBCs from multipleblood transfusions However Boudrahem-Addour et al [27]observed a significant increase (119901 lt 005) of catalase activityin 120573-thalassemia major and intermedia The present results
Advances in Hematology 5
Table 2 Hematological parameters iron status and catalase according to pathology and sex (Media plusmn Standard Deviation)
PathologySex
Age[years]
HTO[LL]
HB[gL]
ECAT[MUL]
Fe[120583gdL]
TIBC[120583gdL]
SAT[]
IDA groupFemale (6) 20 plusmn 19 031 plusmn 008lowastDagger 90 plusmn 32lowastDagger 683 plusmn 274lowastDagger 29 plusmn 10lowastDagger 344 plusmn 68Dagger 8 plusmn 3lowastDagger
Male (4) 19 plusmn 30 034 plusmn 004lowast 95 plusmn 15lowast 806 plusmn 81 22 plusmn 8lowast 324 plusmn 79 7 plusmn 3lowast
BTT groupFemale (15) 34 plusmn 17 036 plusmn 002dagger 108 plusmn 6dagger 994 plusmn 259 84 plusmn 32 270 plusmn 56 31 plusmn 9Male (6) 27 plusmn 6 039 plusmn 005dagger 118 plusmn 16dagger 1040 plusmn 204 114 plusmn 83 272 plusmn 52 44 plusmn 32
N groupFemale (39) 36 plusmn 13 041 plusmn 002 137 plusmn 10 968 plusmn 175 81 plusmn 18 301 plusmn 54 28 plusmn 11Male (28) 37 plusmn 15 044 plusmn 002 147 plusmn 9 931 plusmn 154 94 plusmn 28 282 plusmn 38 34 plusmn 11
lowast119901 lt 005 between IDA and N groups by sex dagger119901 lt 005 between BTT and N groups by sex Dagger119901 lt 005 between IDA and BTT womenIDA iron deficiency anemia BTT 120573-thalassemia trait N normal HTO hematocrit HB hemoglobin ECAT erythrocyte catalase activity Fe iron TIBC totaliron binding capacity SAT transferrin saturation
in concordance with Gerli et al [26] showed that some BTTsubjects had increased catalase activity
Several authors reported increased antioxidant capacityin BTT individuals but they do notmeasured catalase activity[28 29] Instead they used a novel automated measurementmethod and Trolox equivalent antioxidant capacity
In the catalase activity comparison between 1205730 and 120573+thalassemia traits the results were not significant Also Kosaet al [25] did not find significant differences and concludedthat catalase activity was not related to specific 120573-thalassemiamutations Furthermore Labib et al [30] reported no differ-ences in total antioxidant capacity of 1205730 and 120573+ thalassemiatraits
The normal range of erythrocyte catalase activity wasslightly lower than the one reported by another authors [31]which was 803 to 1463MUL Difference may be due to theracial characteristics of the population methodological dif-ferences and because they used 25th and 975th percentiles toestablish normal range Men and women have no significantdifferences in what catalase activity concerns Instead Vitaiand Goth [31] found slightly higher values in male subjects
In this study like Ondei et al [29] there was no rela-tionship between ECAT and iron serum In 120573-thalassemiamajor and intermedia iron excess can lead to organ damageespecially in liver and heart and to endocrine dysfunction[32] Recent studies have shown the importance of othermarkers such as non-transferrin bound iron (NTBI) andlabile plasma iron (LPI) to detect iron excess in thalassemiapatients due to the direct correlation of these markers withthe formation of free radicals [33]
Decreasing serum iron concentration causes insufficientHb synthesis with subsequent reduction of erythrocytes pro-liferation Iron deficiency also affects the production of otheriron-containing proteins such as cytochrome myoglobincatalase and peroxidase Therefore a decreased catalaseactivity could be anticipated in iron deficiency and has beencorroborated in this study in agreement with other works[21 34 35] However Madhikarmi andMurthy [20] detectedan unexplained increase of catalase activity in IDA andTekin et al [36] reported no differences in SOD and catalase
activities between IDA patients and controls Bay et al [37]compared antioxidant capacity between IDA and normalsubjects and detected no significant differences
Increased OxS have been reported in patients with IDA[3 21 35] which occurs primarily in RBC membrane ROSmembrane surface contributes to deformability alteration[38] and phosphatidylserine exposure which have been usedto explain the reduction of RBCs life in IDA [39] Alsoin BTT an altered oxidative state was reported by someinvestigators [28 30] Therefore OxS is present in the mostcommon hypochromic microcytic anemia IDA and BTTbeing one of the determining factors of altered catalaseactivity Hypochromic microcytic RBCs of BTT and IDAindividuals have been studied in the past decades and OxScontribution in reducing the RBCs useful life has beendocumented Previous studies on the catalase activity ofhypochromic microcytic anemia such as IDA and BTT havereported disagreeing results [20 21 25 26 34 35] In thepresent work catalase activity was decreased in IDA andincreased in some BTT subjects with no significant differ-ences between beta-thalassemia mutationsThese results willhelp to clarify how the catalase activity works in these anemiatypesThe lownumber of samples is a limitation of this reportProbably the incorporation of a larger number of participantswill allow revealing hidden differences in current work
Consent
All patients signed an informed consent previously approvedby the Comite de Bioetica de la Facultad de Medicina UNT
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
This work was supported by grants from the Consejo deInvestigaciones de la Universidad Nacional de Tucuman
6 Advances in Hematology
(CIUNT 26D520) The authors thank Biochemist SpecialistGuillermo Fabian Vechetti and Laboratorio Tucuman for theuse of its molecular biology equipment
References
[1] A Lolascon L De Falco and C Beaumont ldquoMolecular basis ofinheritedmicrocytic anemia due to defects in iron acquisitionorheme synthesisrdquo Haematologica vol 94 no 3 pp 395ndash4082009
[2] A Coopersmith andM Ingram ldquoRed cell volumes and erythro-poiesis II Age density volume relationships of macrocytesrdquoAmerican Journal of Physiology vol 216 no 3 pp 473ndash4821969
[3] J L V Corrons A Miguel-Garcia M A Pujades et alldquoIncreased susceptibility ofmicrocytic red blood cells to in vitrooxidative stressrdquo European Journal of Haematology vol 55 no5 pp 327ndash331 1995
[4] WHO Global Database on Anaemia Worldwide Prevalenceof Anaemia 1993ndash2005 2008 httpwhqlibdocwhointpublications20089789241596657 engpdf
[5] OMS ldquoTalasemia y otras hemoglobinopatıas Informe dela Secretarıardquo mayo de 2006 httpappswhointgbarchivepdf filesEB118B118 5-sppdf
[6] M S Abreu and J A Penalver ldquoS hemoglobinopathies inArgentinardquoMedicina (Buenos Aires) vol 52 no 4 pp 341ndash3461992
[7] S Lazarte B Isse and G Aguero ldquoHemoglobinophaties andthalassemia syndromes in Tucuman preliminary studyrdquoBiocellvol 25 no 1 2001
[8] A Larregina E Reimer N Suldrup S Luis J Zavatti andN NPolini ldquoDiagnostico diferencial de anemias microcıticasrdquo ActaBioquimica Clinica Latinoamericana vol 38 no 4 pp 465ndash4692004
[9] S LThein ldquoThemolecular basis of 120573-thalassemiardquo Cold SpringHarbor Perspectives inMedicine vol 3 no 5 Article ID a0117002013
[10] B E Clark and S L Thein ldquoMolecular diagnosis ofhaemoglobin disordersrdquo Clinical and Laboratory Haematologyvol 26 no 3 pp 159ndash176 2004
[11] S L Thein ldquoPathophysiology of beta thalassemiamdasha guide tomolecular therapiesrdquoHematologyAmerican Society of Hematol-ogy Education Program pp 31ndash37 2005
[12] M D Cappellini D Tavazzi L Duca et al ldquoMetabolic indica-tors of oxidative stress correlate with haemichrome attachmentto membrane band 3 aggregation and erythrophagocytosis in120573-thalassaemia intermediardquoBritish Journal of Haematology vol104 no 3 pp 504ndash512 1999
[13] R Evstatiev and C Gasche ldquoIron sensing and signallingrdquo Gutvol 61 no 6 pp 933ndash952 2012
[14] C Kattamis C Lazaropoulou P Delaporta F Apostolakou AKattamis and I Papassotiriou ldquoDisturbances of biomarkers ofiron and oxidant-antioxidant homeostasis in patients with beta-thalassemia intermediardquo Pediatric Endocrinology Reviews vol8 pp 256ndash262 2011
[15] Q Shazia Z H Mohammad T Rahman and H U ShekharldquoCorrelation of oxidative stress with serum trace elementlevels and antioxidant enzyme status in beta thalassemia majorpatients a review of the literaturerdquoAnemia vol 2012 Article ID270923 7 pages 2012
[16] E Fibach and E Rachmilewitz ldquoThe role of oxidative stress inhemolytic anemiardquoCurrentMolecularMedicine vol 8 no 7 pp609ndash619 2008
[17] T Nagy E Paszti M Kaplar H P Bhattoa and L Goth ldquoFur-ther acatalasemia mutations in human patients from Hungarywith diabetes and microcytic anemiardquo Mutation ResearchmdashFundamental and Molecular Mechanisms of Mutagenesis vol772 pp 10ndash14 2015
[18] L G Macdougall ldquoRed cell metabolism in iron deficiencyanemia III The relationship between glutathione peroxidasecatalase serum vitamin E and susceptibility of iron-deficientred cells to oxidative hemolysisrdquo The Journal of Pediatrics vol80 no 5 pp 775ndash782 1972
[19] ENagababu S Gulyani C J Earley R G CutlerM PMattsonand JM Rifkind ldquoIron-deficiency anaemia enhances red bloodcell oxidative stressrdquo Free Radical Research vol 42 no 9 pp824ndash829 2008
[20] N L Madhikarmi and K R S Murthy ldquoAntioxidant enzymesand oxidative stress in the erythrocytes of iron deficiency ane-mic patients supplemented with vitaminsrdquo Iranian BiomedicalJournal vol 18 no 2 pp 82ndash87 2014
[21] E Kurtoglu A Ugur A K Baltaci and L Undar ldquoEffect of ironsupplementation on oxidative stress and antioxidant status iniron-deficiency anemiardquo Biological Trace Element Research vol96 no 1ndash3 pp 117ndash123 2003
[22] L Goth ldquoTwo cases of acatalasemia in Hungaryrdquo ClinicaChimica Acta vol 207 no 1-2 pp 155ndash158 1992
[23] S S Lazarte M E Monaco A C Haro C L Jimenez ME Ledesma Achem and B A Isse ldquoMolecular characteriza-tion and phenotypical study of 120573-thalassemia in TucumanArgentinardquo Hemoglobin vol 38 no 6 pp 394ndash401 2014
[24] F Simsek G Ozturk S Kemahli D Erbas and A HasanogluldquoOxidant and antioxidant status in beta thalassemia majorpatientsrdquo Ankara Universitesi Tıp Fakultesi Mecmuası vol 58pp 34ndash38 2005
[25] Z Kosa T Nagy E Nagy F Fazakas and L Goth ldquoDecreasedblood catalase activity is not related to specific beta-thalassemiamutations in Hungaryrdquo International Journal of LaboratoryHematology vol 34 no 2 pp 172ndash178 2012
[26] G C Gerli L Beretta M Bianchi A Pellegatta and AAgostoni ldquoErythrocyte superoxide dismutase catalase andglutathione peroxidase activities in 120573-thalassemia (major andminor)rdquo Scandinavian Journal of Haematology vol 25 no 1 pp87ndash92 1980
[27] N Boudrahem-Addour M Izem-Meziane K Bouguerra etal ldquoOxidative status and plasma lipid profile in 120573-thalassemiapatientsrdquo Hemoglobin vol 39 no 1 pp 36ndash41 2015
[28] S Selek M Aslan M Horoz M Gur and O Erel ldquoOxidativestatus and serum PON1 activity in beta-thalassemia minorrdquoClinical Biochemistry vol 40 no 5-6 pp 287ndash291 2007
[29] L D S Ondei I D F Estevao M I P Rocha et al ldquoOxidativestress and antioxidant status in beta-thalassemia heterozygotesrdquoRevista Brasileira de Hematologia e Hemoterapia vol 35 no 6pp 409ndash413 2013
[30] H A Labib R L Etewa O A Gaber M Atfy T M Mostafaand I Barsoum ldquoParaoxonase-1 and oxidative status in com-mon Mediterranean 120573-thalassaemia mutations trait and theirrelations to atherosclerosisrdquo Journal of Clinical Pathology vol64 no 5 pp 437ndash442 2011
[31] M Vitai and L Goth ldquoReference ranges of normal blood cata-lase activity and levels in familial hypocatalasemia in HungaryrdquoClinica Chimica Acta vol 261 no 1 pp 35ndash42 1997
Advances in Hematology 7
[32] S Gardenghi R W Grady and S Rivella ldquoAnemia ineffectiveerythropoiesis and hepcidin interacting factors in abnormaliron metabolism leading to iron overload in 120573-thalassemiardquoHematologyOncology Clinics of North America vol 24 no 6pp 1089ndash1107 2010
[33] P BrissotM Ropert C Le Lan andO Loreal ldquoNon-transferrinbound iron a key role in iron overload and iron toxicityrdquoBiochimica et Biophysica ActamdashGeneral Subjects vol 1820 no3 pp 403ndash410 2012
[34] F Amirkhizi F Siassi S Minaie M Djalali A Rahimi andM Chamari ldquoAssessment of lipid peroxidation and activitiesof erythrocyte cytoprotective enzymes in women with irondeficiency anemiardquo Journal of Research in Medical Sciences vol13 no 5 pp 248ndash254 2008
[35] J-H Yoo H-Y Maeng Y-K Sun et al ldquoOxidative status iniron-deficiency anemiardquo Journal of Clinical Laboratory Analysisvol 23 no 5 pp 319ndash323 2009
[36] D Tekin S Yavuzer M Tekin N Akar and S Cin ldquoPossibleeffects of antioxidant status on increased platelet aggregation inchildhood iron-deficiency anemiardquoPediatrics International vol43 no 1 pp 74ndash77 2001
[37] A Bay M Dogan K Bulan S Kaba N Demir and A FOner ldquoA study on the effects of pica and iron-deficiency anemiaon oxidative stress antioxidant capacity and trace elementsrdquoHuman and Experimental Toxicology vol 32 no 9 pp 895ndash9032013
[38] A Vaya M Simo M Santaolaria J Todolı and J Aznar ldquoRedblood cell deformability in iron deficiency anaemiardquo ClinicalHemorheology and Microcirculation vol 33 no 1 pp 75ndash802005
[39] D S Kempe P A Lang C Duranton et al ldquoEnhancedprogrammed cell death of iron-deficient erythrocytesrdquo TheFASEB Journal vol 20 no 2 pp 368ndash370 2006
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Advances in Hematology 3
pH 74) and 30 120583L hemolysate and after 60 seconds the enzy-matic reaction was stopped by adding 10mL of 324mmolLammonium molybdate Blank 1 contained 10mL substrate10mL molybdate and 30 120583L hemolysate blank 2 contained10mL substrate 10mLmolybdate and 30120583L buffer blank 3contained 10mL buffer 10mL molybdate and 30 120583L bufferOne unit of catalase decomposes 1 120583mol of H2O2 in 1 minuteunder these conditions and it is related to 1 L of whole bloodCatalase activity was expressed in Mega UnitsL (MUL) andwas calculated with the following formula
Erythrocyte catalase activity [MUL]
=[119860 (blank 1) minus 119860 (sample)] times 426 times 100119860 (blank 2) minus 119860 (blank 3)
(1)
Molecular Analysis Characterization of 120573-thalassemic muta-tions was realized by real-time PCR Genomic DNA isola-tion was performed with High Pure PCR Template Prepa-ration Kit (Roche Diagnostics) PCR dissociation curvesand subsequent analysis were executed on the LightCycler20 (Roche) equipment simultaneously measuring signalsfrom two different fluorophores Primers were designed toamplify a 587 bp region of 120573-globin gene Forward Primer51015840-gctgtcatc act acctca tag-31015840 Reverse Primer 51015840-gct gcaagt-caccactca g-31015840 Two combinations of hybridization probeslabeled with different fluorophores were used [23]
Statistical Analysis Results were analyzed using SPSS 210statistical program The results were reported as Media plusmnStandard Deviation For comparison Student 119905-Test andANOVA were used A significance level of p lt 005 wasadopted The influence of iron serum on catalase valuesindependent of the group (normal IDA or BTT) wasevaluated by simple regression analysis
3 Results
Ninety-eight individuals were studied of which 67 were nor-mal (N group) 21 with 120573-thalassemia trait (BTT group) and10 with iron deficiency anemia (IDA group) Table 1 showsthe results for catalase activity hematological parameters andiron status in all BTT and IDA patients Subjects were dividedaccording to age children (le12 years) adolescents (13ndash18years) adults (19ndash59 years) and older adults (ge60 years)ANOVA detected no significant differences (119901 = 0187) inECAT between the stated groups
Five individuals who were more than 60 years old werenormal (567 75) 2 120573-thalassemia carriers (221 95)and 2 IDA (210 20) Only one of these subjects whichbelonged to the normal group showed increased catalaseactivity (139MUL) Apparently age has no influence in theECAT of this population
In order to establish the normal range of catalase activity5th and 95th percentiles of N group results were determinedA range from 700 to 1300MUL was obtained
Increased catalase activity in 14 (321) of BTT subjectswas observed No significant differences (119901 = 0245) wereobserved when N and BTT groups were compared
Cata
lase
(MU
L)
N BTT IDA
500
1000
1500
Figure 1 Erythrocyte catalase activity in 120573-thalassemia minor irondeficiency anemia and normal subjects 119901 lt 005 between IDAand N groups N normal IDA iron deficiency anemia BTT 120573-thalassemia trait
Four IDA individuals (40) showed decreased catalaseactivity No significant differences between men and womenwere detected in all groups When N and IDA groups werecompared significant difference (119901 = 0000) was observedsince the IDA subjects had lower values than N group(Figure 1)
Table 2 shows the results in N BTT and IDA groupsaccording to sex Female IDA subjects have significant differ-ences (119901 lt 005) with normal group in all parameters exceptTIBC Catalase in male IDA patients did not demonstratesignificant differences (119901 gt 005) when compared withnormal and BTT groups
The 120573-thalassemia mutations detected in order of fre-quency were codon 39 (CrarrT) (5 subjects) IVS-I-110 (GrarrA) (5 subjects) IVS-I-1 (GrarrA) (4 subjects) and IVS-I-6 (TrarrC) (2 subjects) and in 5 cases the mutation couldnot be assigned The small number of patients for eachgroup prevented the comparative study between themThere-fore differences between 1205730 (9 subjects ECAT = 1046 plusmn316MUL) and 120573+ (7 subjects ECAT = 918 plusmn 174MUL)groups were studied which were not significant (119901 = 0359)
There was no influence of iron levels on catalase values(1199032 = 0153) in these samples
4 Discussion
Oxidative stress is defined as the interruption of balancebetween oxidants and reductants within the body due tothe excess production of peroxides and free radicals Duringthe course of metabolism superoxide anion is convertedto H2O2 by ubiquitous enzyme SOD Normally H2O2 isconverted to innocuous compounds by the action of catalaseand peroxidase But if free iron is available it reacts withH2O2 to form hydroxyl radicals which are extremely reac-tive species leading to depolymerisation of polysaccharideDNA strand breakage inactivation of functional proteinsand other events [24] Therefore this imbalance will cause
4 Advances in Hematology
Table 1 Laboratory data of 120573-thalassemia trait and iron deficiency anemia patients
Groups Age[years]
HTO[LL]
HB[gL]
ECAT[MUL]
Fe[120583gdL]
TIBC[120583gdL]
SAT[]
IDA groupFemale (6)P1 3 026 64 1162 13 262 5P2 14 034 103 543 25 444 6P3 76 037 118 610 33 293 11P4 44 035 101 598 29 313 9P5 43 038 117 813 43 358 12P6 15 017 38 370 31 397 8
Male (4)P1 1 033 97 904 15 352 4P2 1 031 89 834 18 323 6P3 11 031 79 717 25 216 12P4 63 040 115 770 32 403 8
BTT groupFemale (15)P1 12 035 106 953 78 297 26P2 10 033 100 873 75 380 20P3 57 037 107 1139 34 233 15P4 48 039 121 888 80 247 32P5 33 037 108 879 90 285 31P6 33 036 103 835 63 203 31P7 34 034 104 836 50 180 28P8 38 038 115 1062 176 341 52P9 63 038 110 730 81 238 34P10 56 036 106 798 100 220 45P11 11 035 105 752 103 322 32P12 32 037 111 1279 80 228 35P13 22 035 104 865 104 332 31P14 28 037 114 1622 71 258 28P15 26 034 101 1401 83 283 29
Male (6)P1 45 039 115 1354 259 266 97P2 1 032 93 744 29 347 8P3 12 038 112 934 66 244 27P4 65 047 142 1073 144 318 45P5 21 040 121 1133 127 208 61P6 16 041 126 1000 58 247 23
HTO hematocrit HB hemoglobin ECAT erythrocyte catalase activity Fe serum iron TIBC total iron binding capacity SAT transferrin saturation IDAiron deficiency anemia BTT 120573-thalassemia trait P patient
damage to cellular components and tissues in the bodyleading to OxS and catalase has a role in it
Kosa et al [25] revealed a significant decrease in cata-lase activity of 43 120573-thalassemia carriers and attributed itto catalase protein damage by increased free radicals andH2O2 Another study reported increased levels of antioxi-dant enzymes like SOD catalase and GPx in RBCs of 120573-thalassemia minor individuals and near normal values of
these enzymes in RBCs of 120573-thalassemia major patients[26] They concluded that 120573-thalassemia minor RBCs reactto increased OxS rising activities of antioxidant enzymeswhile in 120573-thalassemia major normal antioxidant enzymelevels are due to the presence of normal RBCs from multipleblood transfusions However Boudrahem-Addour et al [27]observed a significant increase (119901 lt 005) of catalase activityin 120573-thalassemia major and intermedia The present results
Advances in Hematology 5
Table 2 Hematological parameters iron status and catalase according to pathology and sex (Media plusmn Standard Deviation)
PathologySex
Age[years]
HTO[LL]
HB[gL]
ECAT[MUL]
Fe[120583gdL]
TIBC[120583gdL]
SAT[]
IDA groupFemale (6) 20 plusmn 19 031 plusmn 008lowastDagger 90 plusmn 32lowastDagger 683 plusmn 274lowastDagger 29 plusmn 10lowastDagger 344 plusmn 68Dagger 8 plusmn 3lowastDagger
Male (4) 19 plusmn 30 034 plusmn 004lowast 95 plusmn 15lowast 806 plusmn 81 22 plusmn 8lowast 324 plusmn 79 7 plusmn 3lowast
BTT groupFemale (15) 34 plusmn 17 036 plusmn 002dagger 108 plusmn 6dagger 994 plusmn 259 84 plusmn 32 270 plusmn 56 31 plusmn 9Male (6) 27 plusmn 6 039 plusmn 005dagger 118 plusmn 16dagger 1040 plusmn 204 114 plusmn 83 272 plusmn 52 44 plusmn 32
N groupFemale (39) 36 plusmn 13 041 plusmn 002 137 plusmn 10 968 plusmn 175 81 plusmn 18 301 plusmn 54 28 plusmn 11Male (28) 37 plusmn 15 044 plusmn 002 147 plusmn 9 931 plusmn 154 94 plusmn 28 282 plusmn 38 34 plusmn 11
lowast119901 lt 005 between IDA and N groups by sex dagger119901 lt 005 between BTT and N groups by sex Dagger119901 lt 005 between IDA and BTT womenIDA iron deficiency anemia BTT 120573-thalassemia trait N normal HTO hematocrit HB hemoglobin ECAT erythrocyte catalase activity Fe iron TIBC totaliron binding capacity SAT transferrin saturation
in concordance with Gerli et al [26] showed that some BTTsubjects had increased catalase activity
Several authors reported increased antioxidant capacityin BTT individuals but they do notmeasured catalase activity[28 29] Instead they used a novel automated measurementmethod and Trolox equivalent antioxidant capacity
In the catalase activity comparison between 1205730 and 120573+thalassemia traits the results were not significant Also Kosaet al [25] did not find significant differences and concludedthat catalase activity was not related to specific 120573-thalassemiamutations Furthermore Labib et al [30] reported no differ-ences in total antioxidant capacity of 1205730 and 120573+ thalassemiatraits
The normal range of erythrocyte catalase activity wasslightly lower than the one reported by another authors [31]which was 803 to 1463MUL Difference may be due to theracial characteristics of the population methodological dif-ferences and because they used 25th and 975th percentiles toestablish normal range Men and women have no significantdifferences in what catalase activity concerns Instead Vitaiand Goth [31] found slightly higher values in male subjects
In this study like Ondei et al [29] there was no rela-tionship between ECAT and iron serum In 120573-thalassemiamajor and intermedia iron excess can lead to organ damageespecially in liver and heart and to endocrine dysfunction[32] Recent studies have shown the importance of othermarkers such as non-transferrin bound iron (NTBI) andlabile plasma iron (LPI) to detect iron excess in thalassemiapatients due to the direct correlation of these markers withthe formation of free radicals [33]
Decreasing serum iron concentration causes insufficientHb synthesis with subsequent reduction of erythrocytes pro-liferation Iron deficiency also affects the production of otheriron-containing proteins such as cytochrome myoglobincatalase and peroxidase Therefore a decreased catalaseactivity could be anticipated in iron deficiency and has beencorroborated in this study in agreement with other works[21 34 35] However Madhikarmi andMurthy [20] detectedan unexplained increase of catalase activity in IDA andTekin et al [36] reported no differences in SOD and catalase
activities between IDA patients and controls Bay et al [37]compared antioxidant capacity between IDA and normalsubjects and detected no significant differences
Increased OxS have been reported in patients with IDA[3 21 35] which occurs primarily in RBC membrane ROSmembrane surface contributes to deformability alteration[38] and phosphatidylserine exposure which have been usedto explain the reduction of RBCs life in IDA [39] Alsoin BTT an altered oxidative state was reported by someinvestigators [28 30] Therefore OxS is present in the mostcommon hypochromic microcytic anemia IDA and BTTbeing one of the determining factors of altered catalaseactivity Hypochromic microcytic RBCs of BTT and IDAindividuals have been studied in the past decades and OxScontribution in reducing the RBCs useful life has beendocumented Previous studies on the catalase activity ofhypochromic microcytic anemia such as IDA and BTT havereported disagreeing results [20 21 25 26 34 35] In thepresent work catalase activity was decreased in IDA andincreased in some BTT subjects with no significant differ-ences between beta-thalassemia mutationsThese results willhelp to clarify how the catalase activity works in these anemiatypesThe lownumber of samples is a limitation of this reportProbably the incorporation of a larger number of participantswill allow revealing hidden differences in current work
Consent
All patients signed an informed consent previously approvedby the Comite de Bioetica de la Facultad de Medicina UNT
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
This work was supported by grants from the Consejo deInvestigaciones de la Universidad Nacional de Tucuman
6 Advances in Hematology
(CIUNT 26D520) The authors thank Biochemist SpecialistGuillermo Fabian Vechetti and Laboratorio Tucuman for theuse of its molecular biology equipment
References
[1] A Lolascon L De Falco and C Beaumont ldquoMolecular basis ofinheritedmicrocytic anemia due to defects in iron acquisitionorheme synthesisrdquo Haematologica vol 94 no 3 pp 395ndash4082009
[2] A Coopersmith andM Ingram ldquoRed cell volumes and erythro-poiesis II Age density volume relationships of macrocytesrdquoAmerican Journal of Physiology vol 216 no 3 pp 473ndash4821969
[3] J L V Corrons A Miguel-Garcia M A Pujades et alldquoIncreased susceptibility ofmicrocytic red blood cells to in vitrooxidative stressrdquo European Journal of Haematology vol 55 no5 pp 327ndash331 1995
[4] WHO Global Database on Anaemia Worldwide Prevalenceof Anaemia 1993ndash2005 2008 httpwhqlibdocwhointpublications20089789241596657 engpdf
[5] OMS ldquoTalasemia y otras hemoglobinopatıas Informe dela Secretarıardquo mayo de 2006 httpappswhointgbarchivepdf filesEB118B118 5-sppdf
[6] M S Abreu and J A Penalver ldquoS hemoglobinopathies inArgentinardquoMedicina (Buenos Aires) vol 52 no 4 pp 341ndash3461992
[7] S Lazarte B Isse and G Aguero ldquoHemoglobinophaties andthalassemia syndromes in Tucuman preliminary studyrdquoBiocellvol 25 no 1 2001
[8] A Larregina E Reimer N Suldrup S Luis J Zavatti andN NPolini ldquoDiagnostico diferencial de anemias microcıticasrdquo ActaBioquimica Clinica Latinoamericana vol 38 no 4 pp 465ndash4692004
[9] S LThein ldquoThemolecular basis of 120573-thalassemiardquo Cold SpringHarbor Perspectives inMedicine vol 3 no 5 Article ID a0117002013
[10] B E Clark and S L Thein ldquoMolecular diagnosis ofhaemoglobin disordersrdquo Clinical and Laboratory Haematologyvol 26 no 3 pp 159ndash176 2004
[11] S L Thein ldquoPathophysiology of beta thalassemiamdasha guide tomolecular therapiesrdquoHematologyAmerican Society of Hematol-ogy Education Program pp 31ndash37 2005
[12] M D Cappellini D Tavazzi L Duca et al ldquoMetabolic indica-tors of oxidative stress correlate with haemichrome attachmentto membrane band 3 aggregation and erythrophagocytosis in120573-thalassaemia intermediardquoBritish Journal of Haematology vol104 no 3 pp 504ndash512 1999
[13] R Evstatiev and C Gasche ldquoIron sensing and signallingrdquo Gutvol 61 no 6 pp 933ndash952 2012
[14] C Kattamis C Lazaropoulou P Delaporta F Apostolakou AKattamis and I Papassotiriou ldquoDisturbances of biomarkers ofiron and oxidant-antioxidant homeostasis in patients with beta-thalassemia intermediardquo Pediatric Endocrinology Reviews vol8 pp 256ndash262 2011
[15] Q Shazia Z H Mohammad T Rahman and H U ShekharldquoCorrelation of oxidative stress with serum trace elementlevels and antioxidant enzyme status in beta thalassemia majorpatients a review of the literaturerdquoAnemia vol 2012 Article ID270923 7 pages 2012
[16] E Fibach and E Rachmilewitz ldquoThe role of oxidative stress inhemolytic anemiardquoCurrentMolecularMedicine vol 8 no 7 pp609ndash619 2008
[17] T Nagy E Paszti M Kaplar H P Bhattoa and L Goth ldquoFur-ther acatalasemia mutations in human patients from Hungarywith diabetes and microcytic anemiardquo Mutation ResearchmdashFundamental and Molecular Mechanisms of Mutagenesis vol772 pp 10ndash14 2015
[18] L G Macdougall ldquoRed cell metabolism in iron deficiencyanemia III The relationship between glutathione peroxidasecatalase serum vitamin E and susceptibility of iron-deficientred cells to oxidative hemolysisrdquo The Journal of Pediatrics vol80 no 5 pp 775ndash782 1972
[19] ENagababu S Gulyani C J Earley R G CutlerM PMattsonand JM Rifkind ldquoIron-deficiency anaemia enhances red bloodcell oxidative stressrdquo Free Radical Research vol 42 no 9 pp824ndash829 2008
[20] N L Madhikarmi and K R S Murthy ldquoAntioxidant enzymesand oxidative stress in the erythrocytes of iron deficiency ane-mic patients supplemented with vitaminsrdquo Iranian BiomedicalJournal vol 18 no 2 pp 82ndash87 2014
[21] E Kurtoglu A Ugur A K Baltaci and L Undar ldquoEffect of ironsupplementation on oxidative stress and antioxidant status iniron-deficiency anemiardquo Biological Trace Element Research vol96 no 1ndash3 pp 117ndash123 2003
[22] L Goth ldquoTwo cases of acatalasemia in Hungaryrdquo ClinicaChimica Acta vol 207 no 1-2 pp 155ndash158 1992
[23] S S Lazarte M E Monaco A C Haro C L Jimenez ME Ledesma Achem and B A Isse ldquoMolecular characteriza-tion and phenotypical study of 120573-thalassemia in TucumanArgentinardquo Hemoglobin vol 38 no 6 pp 394ndash401 2014
[24] F Simsek G Ozturk S Kemahli D Erbas and A HasanogluldquoOxidant and antioxidant status in beta thalassemia majorpatientsrdquo Ankara Universitesi Tıp Fakultesi Mecmuası vol 58pp 34ndash38 2005
[25] Z Kosa T Nagy E Nagy F Fazakas and L Goth ldquoDecreasedblood catalase activity is not related to specific beta-thalassemiamutations in Hungaryrdquo International Journal of LaboratoryHematology vol 34 no 2 pp 172ndash178 2012
[26] G C Gerli L Beretta M Bianchi A Pellegatta and AAgostoni ldquoErythrocyte superoxide dismutase catalase andglutathione peroxidase activities in 120573-thalassemia (major andminor)rdquo Scandinavian Journal of Haematology vol 25 no 1 pp87ndash92 1980
[27] N Boudrahem-Addour M Izem-Meziane K Bouguerra etal ldquoOxidative status and plasma lipid profile in 120573-thalassemiapatientsrdquo Hemoglobin vol 39 no 1 pp 36ndash41 2015
[28] S Selek M Aslan M Horoz M Gur and O Erel ldquoOxidativestatus and serum PON1 activity in beta-thalassemia minorrdquoClinical Biochemistry vol 40 no 5-6 pp 287ndash291 2007
[29] L D S Ondei I D F Estevao M I P Rocha et al ldquoOxidativestress and antioxidant status in beta-thalassemia heterozygotesrdquoRevista Brasileira de Hematologia e Hemoterapia vol 35 no 6pp 409ndash413 2013
[30] H A Labib R L Etewa O A Gaber M Atfy T M Mostafaand I Barsoum ldquoParaoxonase-1 and oxidative status in com-mon Mediterranean 120573-thalassaemia mutations trait and theirrelations to atherosclerosisrdquo Journal of Clinical Pathology vol64 no 5 pp 437ndash442 2011
[31] M Vitai and L Goth ldquoReference ranges of normal blood cata-lase activity and levels in familial hypocatalasemia in HungaryrdquoClinica Chimica Acta vol 261 no 1 pp 35ndash42 1997
Advances in Hematology 7
[32] S Gardenghi R W Grady and S Rivella ldquoAnemia ineffectiveerythropoiesis and hepcidin interacting factors in abnormaliron metabolism leading to iron overload in 120573-thalassemiardquoHematologyOncology Clinics of North America vol 24 no 6pp 1089ndash1107 2010
[33] P BrissotM Ropert C Le Lan andO Loreal ldquoNon-transferrinbound iron a key role in iron overload and iron toxicityrdquoBiochimica et Biophysica ActamdashGeneral Subjects vol 1820 no3 pp 403ndash410 2012
[34] F Amirkhizi F Siassi S Minaie M Djalali A Rahimi andM Chamari ldquoAssessment of lipid peroxidation and activitiesof erythrocyte cytoprotective enzymes in women with irondeficiency anemiardquo Journal of Research in Medical Sciences vol13 no 5 pp 248ndash254 2008
[35] J-H Yoo H-Y Maeng Y-K Sun et al ldquoOxidative status iniron-deficiency anemiardquo Journal of Clinical Laboratory Analysisvol 23 no 5 pp 319ndash323 2009
[36] D Tekin S Yavuzer M Tekin N Akar and S Cin ldquoPossibleeffects of antioxidant status on increased platelet aggregation inchildhood iron-deficiency anemiardquoPediatrics International vol43 no 1 pp 74ndash77 2001
[37] A Bay M Dogan K Bulan S Kaba N Demir and A FOner ldquoA study on the effects of pica and iron-deficiency anemiaon oxidative stress antioxidant capacity and trace elementsrdquoHuman and Experimental Toxicology vol 32 no 9 pp 895ndash9032013
[38] A Vaya M Simo M Santaolaria J Todolı and J Aznar ldquoRedblood cell deformability in iron deficiency anaemiardquo ClinicalHemorheology and Microcirculation vol 33 no 1 pp 75ndash802005
[39] D S Kempe P A Lang C Duranton et al ldquoEnhancedprogrammed cell death of iron-deficient erythrocytesrdquo TheFASEB Journal vol 20 no 2 pp 368ndash370 2006
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
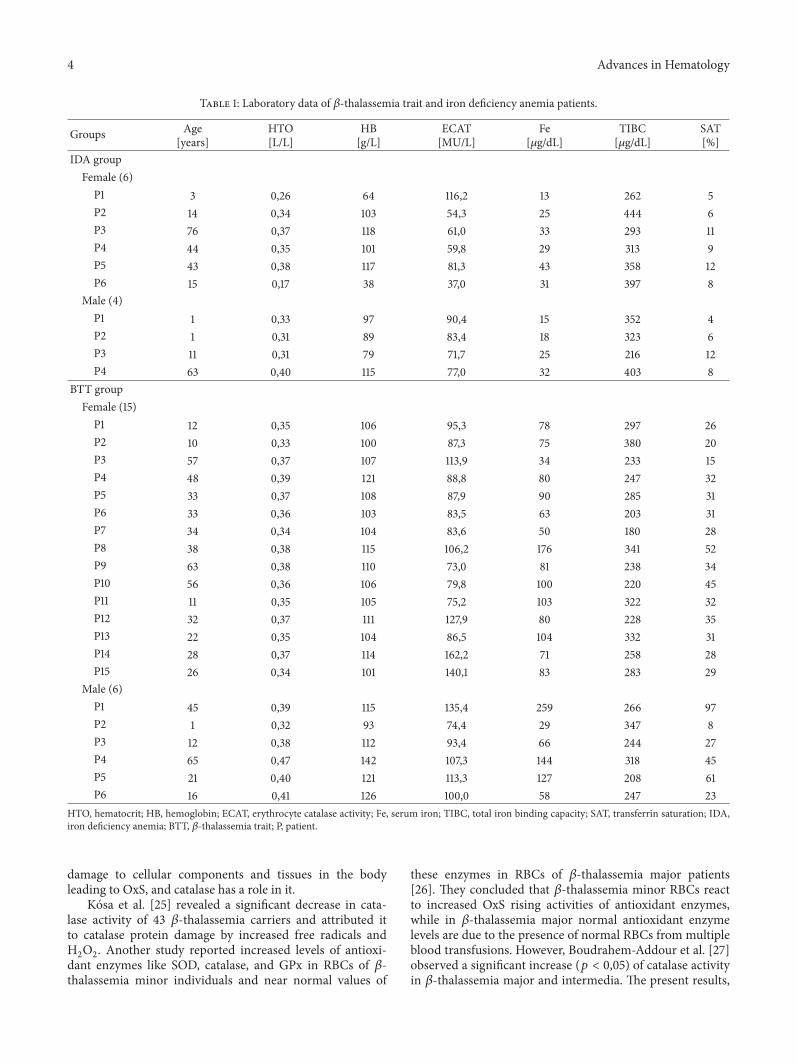
4 Advances in Hematology
Table 1 Laboratory data of 120573-thalassemia trait and iron deficiency anemia patients
Groups Age[years]
HTO[LL]
HB[gL]
ECAT[MUL]
Fe[120583gdL]
TIBC[120583gdL]
SAT[]
IDA groupFemale (6)P1 3 026 64 1162 13 262 5P2 14 034 103 543 25 444 6P3 76 037 118 610 33 293 11P4 44 035 101 598 29 313 9P5 43 038 117 813 43 358 12P6 15 017 38 370 31 397 8
Male (4)P1 1 033 97 904 15 352 4P2 1 031 89 834 18 323 6P3 11 031 79 717 25 216 12P4 63 040 115 770 32 403 8
BTT groupFemale (15)P1 12 035 106 953 78 297 26P2 10 033 100 873 75 380 20P3 57 037 107 1139 34 233 15P4 48 039 121 888 80 247 32P5 33 037 108 879 90 285 31P6 33 036 103 835 63 203 31P7 34 034 104 836 50 180 28P8 38 038 115 1062 176 341 52P9 63 038 110 730 81 238 34P10 56 036 106 798 100 220 45P11 11 035 105 752 103 322 32P12 32 037 111 1279 80 228 35P13 22 035 104 865 104 332 31P14 28 037 114 1622 71 258 28P15 26 034 101 1401 83 283 29
Male (6)P1 45 039 115 1354 259 266 97P2 1 032 93 744 29 347 8P3 12 038 112 934 66 244 27P4 65 047 142 1073 144 318 45P5 21 040 121 1133 127 208 61P6 16 041 126 1000 58 247 23
HTO hematocrit HB hemoglobin ECAT erythrocyte catalase activity Fe serum iron TIBC total iron binding capacity SAT transferrin saturation IDAiron deficiency anemia BTT 120573-thalassemia trait P patient
damage to cellular components and tissues in the bodyleading to OxS and catalase has a role in it
Kosa et al [25] revealed a significant decrease in cata-lase activity of 43 120573-thalassemia carriers and attributed itto catalase protein damage by increased free radicals andH2O2 Another study reported increased levels of antioxi-dant enzymes like SOD catalase and GPx in RBCs of 120573-thalassemia minor individuals and near normal values of
these enzymes in RBCs of 120573-thalassemia major patients[26] They concluded that 120573-thalassemia minor RBCs reactto increased OxS rising activities of antioxidant enzymeswhile in 120573-thalassemia major normal antioxidant enzymelevels are due to the presence of normal RBCs from multipleblood transfusions However Boudrahem-Addour et al [27]observed a significant increase (119901 lt 005) of catalase activityin 120573-thalassemia major and intermedia The present results
Advances in Hematology 5
Table 2 Hematological parameters iron status and catalase according to pathology and sex (Media plusmn Standard Deviation)
PathologySex
Age[years]
HTO[LL]
HB[gL]
ECAT[MUL]
Fe[120583gdL]
TIBC[120583gdL]
SAT[]
IDA groupFemale (6) 20 plusmn 19 031 plusmn 008lowastDagger 90 plusmn 32lowastDagger 683 plusmn 274lowastDagger 29 plusmn 10lowastDagger 344 plusmn 68Dagger 8 plusmn 3lowastDagger
Male (4) 19 plusmn 30 034 plusmn 004lowast 95 plusmn 15lowast 806 plusmn 81 22 plusmn 8lowast 324 plusmn 79 7 plusmn 3lowast
BTT groupFemale (15) 34 plusmn 17 036 plusmn 002dagger 108 plusmn 6dagger 994 plusmn 259 84 plusmn 32 270 plusmn 56 31 plusmn 9Male (6) 27 plusmn 6 039 plusmn 005dagger 118 plusmn 16dagger 1040 plusmn 204 114 plusmn 83 272 plusmn 52 44 plusmn 32
N groupFemale (39) 36 plusmn 13 041 plusmn 002 137 plusmn 10 968 plusmn 175 81 plusmn 18 301 plusmn 54 28 plusmn 11Male (28) 37 plusmn 15 044 plusmn 002 147 plusmn 9 931 plusmn 154 94 plusmn 28 282 plusmn 38 34 plusmn 11
lowast119901 lt 005 between IDA and N groups by sex dagger119901 lt 005 between BTT and N groups by sex Dagger119901 lt 005 between IDA and BTT womenIDA iron deficiency anemia BTT 120573-thalassemia trait N normal HTO hematocrit HB hemoglobin ECAT erythrocyte catalase activity Fe iron TIBC totaliron binding capacity SAT transferrin saturation
in concordance with Gerli et al [26] showed that some BTTsubjects had increased catalase activity
Several authors reported increased antioxidant capacityin BTT individuals but they do notmeasured catalase activity[28 29] Instead they used a novel automated measurementmethod and Trolox equivalent antioxidant capacity
In the catalase activity comparison between 1205730 and 120573+thalassemia traits the results were not significant Also Kosaet al [25] did not find significant differences and concludedthat catalase activity was not related to specific 120573-thalassemiamutations Furthermore Labib et al [30] reported no differ-ences in total antioxidant capacity of 1205730 and 120573+ thalassemiatraits
The normal range of erythrocyte catalase activity wasslightly lower than the one reported by another authors [31]which was 803 to 1463MUL Difference may be due to theracial characteristics of the population methodological dif-ferences and because they used 25th and 975th percentiles toestablish normal range Men and women have no significantdifferences in what catalase activity concerns Instead Vitaiand Goth [31] found slightly higher values in male subjects
In this study like Ondei et al [29] there was no rela-tionship between ECAT and iron serum In 120573-thalassemiamajor and intermedia iron excess can lead to organ damageespecially in liver and heart and to endocrine dysfunction[32] Recent studies have shown the importance of othermarkers such as non-transferrin bound iron (NTBI) andlabile plasma iron (LPI) to detect iron excess in thalassemiapatients due to the direct correlation of these markers withthe formation of free radicals [33]
Decreasing serum iron concentration causes insufficientHb synthesis with subsequent reduction of erythrocytes pro-liferation Iron deficiency also affects the production of otheriron-containing proteins such as cytochrome myoglobincatalase and peroxidase Therefore a decreased catalaseactivity could be anticipated in iron deficiency and has beencorroborated in this study in agreement with other works[21 34 35] However Madhikarmi andMurthy [20] detectedan unexplained increase of catalase activity in IDA andTekin et al [36] reported no differences in SOD and catalase
activities between IDA patients and controls Bay et al [37]compared antioxidant capacity between IDA and normalsubjects and detected no significant differences
Increased OxS have been reported in patients with IDA[3 21 35] which occurs primarily in RBC membrane ROSmembrane surface contributes to deformability alteration[38] and phosphatidylserine exposure which have been usedto explain the reduction of RBCs life in IDA [39] Alsoin BTT an altered oxidative state was reported by someinvestigators [28 30] Therefore OxS is present in the mostcommon hypochromic microcytic anemia IDA and BTTbeing one of the determining factors of altered catalaseactivity Hypochromic microcytic RBCs of BTT and IDAindividuals have been studied in the past decades and OxScontribution in reducing the RBCs useful life has beendocumented Previous studies on the catalase activity ofhypochromic microcytic anemia such as IDA and BTT havereported disagreeing results [20 21 25 26 34 35] In thepresent work catalase activity was decreased in IDA andincreased in some BTT subjects with no significant differ-ences between beta-thalassemia mutationsThese results willhelp to clarify how the catalase activity works in these anemiatypesThe lownumber of samples is a limitation of this reportProbably the incorporation of a larger number of participantswill allow revealing hidden differences in current work
Consent
All patients signed an informed consent previously approvedby the Comite de Bioetica de la Facultad de Medicina UNT
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
This work was supported by grants from the Consejo deInvestigaciones de la Universidad Nacional de Tucuman
6 Advances in Hematology
(CIUNT 26D520) The authors thank Biochemist SpecialistGuillermo Fabian Vechetti and Laboratorio Tucuman for theuse of its molecular biology equipment
References
[1] A Lolascon L De Falco and C Beaumont ldquoMolecular basis ofinheritedmicrocytic anemia due to defects in iron acquisitionorheme synthesisrdquo Haematologica vol 94 no 3 pp 395ndash4082009
[2] A Coopersmith andM Ingram ldquoRed cell volumes and erythro-poiesis II Age density volume relationships of macrocytesrdquoAmerican Journal of Physiology vol 216 no 3 pp 473ndash4821969
[3] J L V Corrons A Miguel-Garcia M A Pujades et alldquoIncreased susceptibility ofmicrocytic red blood cells to in vitrooxidative stressrdquo European Journal of Haematology vol 55 no5 pp 327ndash331 1995
[4] WHO Global Database on Anaemia Worldwide Prevalenceof Anaemia 1993ndash2005 2008 httpwhqlibdocwhointpublications20089789241596657 engpdf
[5] OMS ldquoTalasemia y otras hemoglobinopatıas Informe dela Secretarıardquo mayo de 2006 httpappswhointgbarchivepdf filesEB118B118 5-sppdf
[6] M S Abreu and J A Penalver ldquoS hemoglobinopathies inArgentinardquoMedicina (Buenos Aires) vol 52 no 4 pp 341ndash3461992
[7] S Lazarte B Isse and G Aguero ldquoHemoglobinophaties andthalassemia syndromes in Tucuman preliminary studyrdquoBiocellvol 25 no 1 2001
[8] A Larregina E Reimer N Suldrup S Luis J Zavatti andN NPolini ldquoDiagnostico diferencial de anemias microcıticasrdquo ActaBioquimica Clinica Latinoamericana vol 38 no 4 pp 465ndash4692004
[9] S LThein ldquoThemolecular basis of 120573-thalassemiardquo Cold SpringHarbor Perspectives inMedicine vol 3 no 5 Article ID a0117002013
[10] B E Clark and S L Thein ldquoMolecular diagnosis ofhaemoglobin disordersrdquo Clinical and Laboratory Haematologyvol 26 no 3 pp 159ndash176 2004
[11] S L Thein ldquoPathophysiology of beta thalassemiamdasha guide tomolecular therapiesrdquoHematologyAmerican Society of Hematol-ogy Education Program pp 31ndash37 2005
[12] M D Cappellini D Tavazzi L Duca et al ldquoMetabolic indica-tors of oxidative stress correlate with haemichrome attachmentto membrane band 3 aggregation and erythrophagocytosis in120573-thalassaemia intermediardquoBritish Journal of Haematology vol104 no 3 pp 504ndash512 1999
[13] R Evstatiev and C Gasche ldquoIron sensing and signallingrdquo Gutvol 61 no 6 pp 933ndash952 2012
[14] C Kattamis C Lazaropoulou P Delaporta F Apostolakou AKattamis and I Papassotiriou ldquoDisturbances of biomarkers ofiron and oxidant-antioxidant homeostasis in patients with beta-thalassemia intermediardquo Pediatric Endocrinology Reviews vol8 pp 256ndash262 2011
[15] Q Shazia Z H Mohammad T Rahman and H U ShekharldquoCorrelation of oxidative stress with serum trace elementlevels and antioxidant enzyme status in beta thalassemia majorpatients a review of the literaturerdquoAnemia vol 2012 Article ID270923 7 pages 2012
[16] E Fibach and E Rachmilewitz ldquoThe role of oxidative stress inhemolytic anemiardquoCurrentMolecularMedicine vol 8 no 7 pp609ndash619 2008
[17] T Nagy E Paszti M Kaplar H P Bhattoa and L Goth ldquoFur-ther acatalasemia mutations in human patients from Hungarywith diabetes and microcytic anemiardquo Mutation ResearchmdashFundamental and Molecular Mechanisms of Mutagenesis vol772 pp 10ndash14 2015
[18] L G Macdougall ldquoRed cell metabolism in iron deficiencyanemia III The relationship between glutathione peroxidasecatalase serum vitamin E and susceptibility of iron-deficientred cells to oxidative hemolysisrdquo The Journal of Pediatrics vol80 no 5 pp 775ndash782 1972
[19] ENagababu S Gulyani C J Earley R G CutlerM PMattsonand JM Rifkind ldquoIron-deficiency anaemia enhances red bloodcell oxidative stressrdquo Free Radical Research vol 42 no 9 pp824ndash829 2008
[20] N L Madhikarmi and K R S Murthy ldquoAntioxidant enzymesand oxidative stress in the erythrocytes of iron deficiency ane-mic patients supplemented with vitaminsrdquo Iranian BiomedicalJournal vol 18 no 2 pp 82ndash87 2014
[21] E Kurtoglu A Ugur A K Baltaci and L Undar ldquoEffect of ironsupplementation on oxidative stress and antioxidant status iniron-deficiency anemiardquo Biological Trace Element Research vol96 no 1ndash3 pp 117ndash123 2003
[22] L Goth ldquoTwo cases of acatalasemia in Hungaryrdquo ClinicaChimica Acta vol 207 no 1-2 pp 155ndash158 1992
[23] S S Lazarte M E Monaco A C Haro C L Jimenez ME Ledesma Achem and B A Isse ldquoMolecular characteriza-tion and phenotypical study of 120573-thalassemia in TucumanArgentinardquo Hemoglobin vol 38 no 6 pp 394ndash401 2014
[24] F Simsek G Ozturk S Kemahli D Erbas and A HasanogluldquoOxidant and antioxidant status in beta thalassemia majorpatientsrdquo Ankara Universitesi Tıp Fakultesi Mecmuası vol 58pp 34ndash38 2005
[25] Z Kosa T Nagy E Nagy F Fazakas and L Goth ldquoDecreasedblood catalase activity is not related to specific beta-thalassemiamutations in Hungaryrdquo International Journal of LaboratoryHematology vol 34 no 2 pp 172ndash178 2012
[26] G C Gerli L Beretta M Bianchi A Pellegatta and AAgostoni ldquoErythrocyte superoxide dismutase catalase andglutathione peroxidase activities in 120573-thalassemia (major andminor)rdquo Scandinavian Journal of Haematology vol 25 no 1 pp87ndash92 1980
[27] N Boudrahem-Addour M Izem-Meziane K Bouguerra etal ldquoOxidative status and plasma lipid profile in 120573-thalassemiapatientsrdquo Hemoglobin vol 39 no 1 pp 36ndash41 2015
[28] S Selek M Aslan M Horoz M Gur and O Erel ldquoOxidativestatus and serum PON1 activity in beta-thalassemia minorrdquoClinical Biochemistry vol 40 no 5-6 pp 287ndash291 2007
[29] L D S Ondei I D F Estevao M I P Rocha et al ldquoOxidativestress and antioxidant status in beta-thalassemia heterozygotesrdquoRevista Brasileira de Hematologia e Hemoterapia vol 35 no 6pp 409ndash413 2013
[30] H A Labib R L Etewa O A Gaber M Atfy T M Mostafaand I Barsoum ldquoParaoxonase-1 and oxidative status in com-mon Mediterranean 120573-thalassaemia mutations trait and theirrelations to atherosclerosisrdquo Journal of Clinical Pathology vol64 no 5 pp 437ndash442 2011
[31] M Vitai and L Goth ldquoReference ranges of normal blood cata-lase activity and levels in familial hypocatalasemia in HungaryrdquoClinica Chimica Acta vol 261 no 1 pp 35ndash42 1997
Advances in Hematology 7
[32] S Gardenghi R W Grady and S Rivella ldquoAnemia ineffectiveerythropoiesis and hepcidin interacting factors in abnormaliron metabolism leading to iron overload in 120573-thalassemiardquoHematologyOncology Clinics of North America vol 24 no 6pp 1089ndash1107 2010
[33] P BrissotM Ropert C Le Lan andO Loreal ldquoNon-transferrinbound iron a key role in iron overload and iron toxicityrdquoBiochimica et Biophysica ActamdashGeneral Subjects vol 1820 no3 pp 403ndash410 2012
[34] F Amirkhizi F Siassi S Minaie M Djalali A Rahimi andM Chamari ldquoAssessment of lipid peroxidation and activitiesof erythrocyte cytoprotective enzymes in women with irondeficiency anemiardquo Journal of Research in Medical Sciences vol13 no 5 pp 248ndash254 2008
[35] J-H Yoo H-Y Maeng Y-K Sun et al ldquoOxidative status iniron-deficiency anemiardquo Journal of Clinical Laboratory Analysisvol 23 no 5 pp 319ndash323 2009
[36] D Tekin S Yavuzer M Tekin N Akar and S Cin ldquoPossibleeffects of antioxidant status on increased platelet aggregation inchildhood iron-deficiency anemiardquoPediatrics International vol43 no 1 pp 74ndash77 2001
[37] A Bay M Dogan K Bulan S Kaba N Demir and A FOner ldquoA study on the effects of pica and iron-deficiency anemiaon oxidative stress antioxidant capacity and trace elementsrdquoHuman and Experimental Toxicology vol 32 no 9 pp 895ndash9032013
[38] A Vaya M Simo M Santaolaria J Todolı and J Aznar ldquoRedblood cell deformability in iron deficiency anaemiardquo ClinicalHemorheology and Microcirculation vol 33 no 1 pp 75ndash802005
[39] D S Kempe P A Lang C Duranton et al ldquoEnhancedprogrammed cell death of iron-deficient erythrocytesrdquo TheFASEB Journal vol 20 no 2 pp 368ndash370 2006
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Advances in Hematology 5
Table 2 Hematological parameters iron status and catalase according to pathology and sex (Media plusmn Standard Deviation)
PathologySex
Age[years]
HTO[LL]
HB[gL]
ECAT[MUL]
Fe[120583gdL]
TIBC[120583gdL]
SAT[]
IDA groupFemale (6) 20 plusmn 19 031 plusmn 008lowastDagger 90 plusmn 32lowastDagger 683 plusmn 274lowastDagger 29 plusmn 10lowastDagger 344 plusmn 68Dagger 8 plusmn 3lowastDagger
Male (4) 19 plusmn 30 034 plusmn 004lowast 95 plusmn 15lowast 806 plusmn 81 22 plusmn 8lowast 324 plusmn 79 7 plusmn 3lowast
BTT groupFemale (15) 34 plusmn 17 036 plusmn 002dagger 108 plusmn 6dagger 994 plusmn 259 84 plusmn 32 270 plusmn 56 31 plusmn 9Male (6) 27 plusmn 6 039 plusmn 005dagger 118 plusmn 16dagger 1040 plusmn 204 114 plusmn 83 272 plusmn 52 44 plusmn 32
N groupFemale (39) 36 plusmn 13 041 plusmn 002 137 plusmn 10 968 plusmn 175 81 plusmn 18 301 plusmn 54 28 plusmn 11Male (28) 37 plusmn 15 044 plusmn 002 147 plusmn 9 931 plusmn 154 94 plusmn 28 282 plusmn 38 34 plusmn 11
lowast119901 lt 005 between IDA and N groups by sex dagger119901 lt 005 between BTT and N groups by sex Dagger119901 lt 005 between IDA and BTT womenIDA iron deficiency anemia BTT 120573-thalassemia trait N normal HTO hematocrit HB hemoglobin ECAT erythrocyte catalase activity Fe iron TIBC totaliron binding capacity SAT transferrin saturation
in concordance with Gerli et al [26] showed that some BTTsubjects had increased catalase activity
Several authors reported increased antioxidant capacityin BTT individuals but they do notmeasured catalase activity[28 29] Instead they used a novel automated measurementmethod and Trolox equivalent antioxidant capacity
In the catalase activity comparison between 1205730 and 120573+thalassemia traits the results were not significant Also Kosaet al [25] did not find significant differences and concludedthat catalase activity was not related to specific 120573-thalassemiamutations Furthermore Labib et al [30] reported no differ-ences in total antioxidant capacity of 1205730 and 120573+ thalassemiatraits
The normal range of erythrocyte catalase activity wasslightly lower than the one reported by another authors [31]which was 803 to 1463MUL Difference may be due to theracial characteristics of the population methodological dif-ferences and because they used 25th and 975th percentiles toestablish normal range Men and women have no significantdifferences in what catalase activity concerns Instead Vitaiand Goth [31] found slightly higher values in male subjects
In this study like Ondei et al [29] there was no rela-tionship between ECAT and iron serum In 120573-thalassemiamajor and intermedia iron excess can lead to organ damageespecially in liver and heart and to endocrine dysfunction[32] Recent studies have shown the importance of othermarkers such as non-transferrin bound iron (NTBI) andlabile plasma iron (LPI) to detect iron excess in thalassemiapatients due to the direct correlation of these markers withthe formation of free radicals [33]
Decreasing serum iron concentration causes insufficientHb synthesis with subsequent reduction of erythrocytes pro-liferation Iron deficiency also affects the production of otheriron-containing proteins such as cytochrome myoglobincatalase and peroxidase Therefore a decreased catalaseactivity could be anticipated in iron deficiency and has beencorroborated in this study in agreement with other works[21 34 35] However Madhikarmi andMurthy [20] detectedan unexplained increase of catalase activity in IDA andTekin et al [36] reported no differences in SOD and catalase
activities between IDA patients and controls Bay et al [37]compared antioxidant capacity between IDA and normalsubjects and detected no significant differences
Increased OxS have been reported in patients with IDA[3 21 35] which occurs primarily in RBC membrane ROSmembrane surface contributes to deformability alteration[38] and phosphatidylserine exposure which have been usedto explain the reduction of RBCs life in IDA [39] Alsoin BTT an altered oxidative state was reported by someinvestigators [28 30] Therefore OxS is present in the mostcommon hypochromic microcytic anemia IDA and BTTbeing one of the determining factors of altered catalaseactivity Hypochromic microcytic RBCs of BTT and IDAindividuals have been studied in the past decades and OxScontribution in reducing the RBCs useful life has beendocumented Previous studies on the catalase activity ofhypochromic microcytic anemia such as IDA and BTT havereported disagreeing results [20 21 25 26 34 35] In thepresent work catalase activity was decreased in IDA andincreased in some BTT subjects with no significant differ-ences between beta-thalassemia mutationsThese results willhelp to clarify how the catalase activity works in these anemiatypesThe lownumber of samples is a limitation of this reportProbably the incorporation of a larger number of participantswill allow revealing hidden differences in current work
Consent
All patients signed an informed consent previously approvedby the Comite de Bioetica de la Facultad de Medicina UNT
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
This work was supported by grants from the Consejo deInvestigaciones de la Universidad Nacional de Tucuman
6 Advances in Hematology
(CIUNT 26D520) The authors thank Biochemist SpecialistGuillermo Fabian Vechetti and Laboratorio Tucuman for theuse of its molecular biology equipment
References
[1] A Lolascon L De Falco and C Beaumont ldquoMolecular basis ofinheritedmicrocytic anemia due to defects in iron acquisitionorheme synthesisrdquo Haematologica vol 94 no 3 pp 395ndash4082009
[2] A Coopersmith andM Ingram ldquoRed cell volumes and erythro-poiesis II Age density volume relationships of macrocytesrdquoAmerican Journal of Physiology vol 216 no 3 pp 473ndash4821969
[3] J L V Corrons A Miguel-Garcia M A Pujades et alldquoIncreased susceptibility ofmicrocytic red blood cells to in vitrooxidative stressrdquo European Journal of Haematology vol 55 no5 pp 327ndash331 1995
[4] WHO Global Database on Anaemia Worldwide Prevalenceof Anaemia 1993ndash2005 2008 httpwhqlibdocwhointpublications20089789241596657 engpdf
[5] OMS ldquoTalasemia y otras hemoglobinopatıas Informe dela Secretarıardquo mayo de 2006 httpappswhointgbarchivepdf filesEB118B118 5-sppdf
[6] M S Abreu and J A Penalver ldquoS hemoglobinopathies inArgentinardquoMedicina (Buenos Aires) vol 52 no 4 pp 341ndash3461992
[7] S Lazarte B Isse and G Aguero ldquoHemoglobinophaties andthalassemia syndromes in Tucuman preliminary studyrdquoBiocellvol 25 no 1 2001
[8] A Larregina E Reimer N Suldrup S Luis J Zavatti andN NPolini ldquoDiagnostico diferencial de anemias microcıticasrdquo ActaBioquimica Clinica Latinoamericana vol 38 no 4 pp 465ndash4692004
[9] S LThein ldquoThemolecular basis of 120573-thalassemiardquo Cold SpringHarbor Perspectives inMedicine vol 3 no 5 Article ID a0117002013
[10] B E Clark and S L Thein ldquoMolecular diagnosis ofhaemoglobin disordersrdquo Clinical and Laboratory Haematologyvol 26 no 3 pp 159ndash176 2004
[11] S L Thein ldquoPathophysiology of beta thalassemiamdasha guide tomolecular therapiesrdquoHematologyAmerican Society of Hematol-ogy Education Program pp 31ndash37 2005
[12] M D Cappellini D Tavazzi L Duca et al ldquoMetabolic indica-tors of oxidative stress correlate with haemichrome attachmentto membrane band 3 aggregation and erythrophagocytosis in120573-thalassaemia intermediardquoBritish Journal of Haematology vol104 no 3 pp 504ndash512 1999
[13] R Evstatiev and C Gasche ldquoIron sensing and signallingrdquo Gutvol 61 no 6 pp 933ndash952 2012
[14] C Kattamis C Lazaropoulou P Delaporta F Apostolakou AKattamis and I Papassotiriou ldquoDisturbances of biomarkers ofiron and oxidant-antioxidant homeostasis in patients with beta-thalassemia intermediardquo Pediatric Endocrinology Reviews vol8 pp 256ndash262 2011
[15] Q Shazia Z H Mohammad T Rahman and H U ShekharldquoCorrelation of oxidative stress with serum trace elementlevels and antioxidant enzyme status in beta thalassemia majorpatients a review of the literaturerdquoAnemia vol 2012 Article ID270923 7 pages 2012
[16] E Fibach and E Rachmilewitz ldquoThe role of oxidative stress inhemolytic anemiardquoCurrentMolecularMedicine vol 8 no 7 pp609ndash619 2008
[17] T Nagy E Paszti M Kaplar H P Bhattoa and L Goth ldquoFur-ther acatalasemia mutations in human patients from Hungarywith diabetes and microcytic anemiardquo Mutation ResearchmdashFundamental and Molecular Mechanisms of Mutagenesis vol772 pp 10ndash14 2015
[18] L G Macdougall ldquoRed cell metabolism in iron deficiencyanemia III The relationship between glutathione peroxidasecatalase serum vitamin E and susceptibility of iron-deficientred cells to oxidative hemolysisrdquo The Journal of Pediatrics vol80 no 5 pp 775ndash782 1972
[19] ENagababu S Gulyani C J Earley R G CutlerM PMattsonand JM Rifkind ldquoIron-deficiency anaemia enhances red bloodcell oxidative stressrdquo Free Radical Research vol 42 no 9 pp824ndash829 2008
[20] N L Madhikarmi and K R S Murthy ldquoAntioxidant enzymesand oxidative stress in the erythrocytes of iron deficiency ane-mic patients supplemented with vitaminsrdquo Iranian BiomedicalJournal vol 18 no 2 pp 82ndash87 2014
[21] E Kurtoglu A Ugur A K Baltaci and L Undar ldquoEffect of ironsupplementation on oxidative stress and antioxidant status iniron-deficiency anemiardquo Biological Trace Element Research vol96 no 1ndash3 pp 117ndash123 2003
[22] L Goth ldquoTwo cases of acatalasemia in Hungaryrdquo ClinicaChimica Acta vol 207 no 1-2 pp 155ndash158 1992
[23] S S Lazarte M E Monaco A C Haro C L Jimenez ME Ledesma Achem and B A Isse ldquoMolecular characteriza-tion and phenotypical study of 120573-thalassemia in TucumanArgentinardquo Hemoglobin vol 38 no 6 pp 394ndash401 2014
[24] F Simsek G Ozturk S Kemahli D Erbas and A HasanogluldquoOxidant and antioxidant status in beta thalassemia majorpatientsrdquo Ankara Universitesi Tıp Fakultesi Mecmuası vol 58pp 34ndash38 2005
[25] Z Kosa T Nagy E Nagy F Fazakas and L Goth ldquoDecreasedblood catalase activity is not related to specific beta-thalassemiamutations in Hungaryrdquo International Journal of LaboratoryHematology vol 34 no 2 pp 172ndash178 2012
[26] G C Gerli L Beretta M Bianchi A Pellegatta and AAgostoni ldquoErythrocyte superoxide dismutase catalase andglutathione peroxidase activities in 120573-thalassemia (major andminor)rdquo Scandinavian Journal of Haematology vol 25 no 1 pp87ndash92 1980
[27] N Boudrahem-Addour M Izem-Meziane K Bouguerra etal ldquoOxidative status and plasma lipid profile in 120573-thalassemiapatientsrdquo Hemoglobin vol 39 no 1 pp 36ndash41 2015
[28] S Selek M Aslan M Horoz M Gur and O Erel ldquoOxidativestatus and serum PON1 activity in beta-thalassemia minorrdquoClinical Biochemistry vol 40 no 5-6 pp 287ndash291 2007
[29] L D S Ondei I D F Estevao M I P Rocha et al ldquoOxidativestress and antioxidant status in beta-thalassemia heterozygotesrdquoRevista Brasileira de Hematologia e Hemoterapia vol 35 no 6pp 409ndash413 2013
[30] H A Labib R L Etewa O A Gaber M Atfy T M Mostafaand I Barsoum ldquoParaoxonase-1 and oxidative status in com-mon Mediterranean 120573-thalassaemia mutations trait and theirrelations to atherosclerosisrdquo Journal of Clinical Pathology vol64 no 5 pp 437ndash442 2011
[31] M Vitai and L Goth ldquoReference ranges of normal blood cata-lase activity and levels in familial hypocatalasemia in HungaryrdquoClinica Chimica Acta vol 261 no 1 pp 35ndash42 1997
Advances in Hematology 7
[32] S Gardenghi R W Grady and S Rivella ldquoAnemia ineffectiveerythropoiesis and hepcidin interacting factors in abnormaliron metabolism leading to iron overload in 120573-thalassemiardquoHematologyOncology Clinics of North America vol 24 no 6pp 1089ndash1107 2010
[33] P BrissotM Ropert C Le Lan andO Loreal ldquoNon-transferrinbound iron a key role in iron overload and iron toxicityrdquoBiochimica et Biophysica ActamdashGeneral Subjects vol 1820 no3 pp 403ndash410 2012
[34] F Amirkhizi F Siassi S Minaie M Djalali A Rahimi andM Chamari ldquoAssessment of lipid peroxidation and activitiesof erythrocyte cytoprotective enzymes in women with irondeficiency anemiardquo Journal of Research in Medical Sciences vol13 no 5 pp 248ndash254 2008
[35] J-H Yoo H-Y Maeng Y-K Sun et al ldquoOxidative status iniron-deficiency anemiardquo Journal of Clinical Laboratory Analysisvol 23 no 5 pp 319ndash323 2009
[36] D Tekin S Yavuzer M Tekin N Akar and S Cin ldquoPossibleeffects of antioxidant status on increased platelet aggregation inchildhood iron-deficiency anemiardquoPediatrics International vol43 no 1 pp 74ndash77 2001
[37] A Bay M Dogan K Bulan S Kaba N Demir and A FOner ldquoA study on the effects of pica and iron-deficiency anemiaon oxidative stress antioxidant capacity and trace elementsrdquoHuman and Experimental Toxicology vol 32 no 9 pp 895ndash9032013
[38] A Vaya M Simo M Santaolaria J Todolı and J Aznar ldquoRedblood cell deformability in iron deficiency anaemiardquo ClinicalHemorheology and Microcirculation vol 33 no 1 pp 75ndash802005
[39] D S Kempe P A Lang C Duranton et al ldquoEnhancedprogrammed cell death of iron-deficient erythrocytesrdquo TheFASEB Journal vol 20 no 2 pp 368ndash370 2006
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

6 Advances in Hematology
(CIUNT 26D520) The authors thank Biochemist SpecialistGuillermo Fabian Vechetti and Laboratorio Tucuman for theuse of its molecular biology equipment
References
[1] A Lolascon L De Falco and C Beaumont ldquoMolecular basis ofinheritedmicrocytic anemia due to defects in iron acquisitionorheme synthesisrdquo Haematologica vol 94 no 3 pp 395ndash4082009
[2] A Coopersmith andM Ingram ldquoRed cell volumes and erythro-poiesis II Age density volume relationships of macrocytesrdquoAmerican Journal of Physiology vol 216 no 3 pp 473ndash4821969
[3] J L V Corrons A Miguel-Garcia M A Pujades et alldquoIncreased susceptibility ofmicrocytic red blood cells to in vitrooxidative stressrdquo European Journal of Haematology vol 55 no5 pp 327ndash331 1995
[4] WHO Global Database on Anaemia Worldwide Prevalenceof Anaemia 1993ndash2005 2008 httpwhqlibdocwhointpublications20089789241596657 engpdf
[5] OMS ldquoTalasemia y otras hemoglobinopatıas Informe dela Secretarıardquo mayo de 2006 httpappswhointgbarchivepdf filesEB118B118 5-sppdf
[6] M S Abreu and J A Penalver ldquoS hemoglobinopathies inArgentinardquoMedicina (Buenos Aires) vol 52 no 4 pp 341ndash3461992
[7] S Lazarte B Isse and G Aguero ldquoHemoglobinophaties andthalassemia syndromes in Tucuman preliminary studyrdquoBiocellvol 25 no 1 2001
[8] A Larregina E Reimer N Suldrup S Luis J Zavatti andN NPolini ldquoDiagnostico diferencial de anemias microcıticasrdquo ActaBioquimica Clinica Latinoamericana vol 38 no 4 pp 465ndash4692004
[9] S LThein ldquoThemolecular basis of 120573-thalassemiardquo Cold SpringHarbor Perspectives inMedicine vol 3 no 5 Article ID a0117002013
[10] B E Clark and S L Thein ldquoMolecular diagnosis ofhaemoglobin disordersrdquo Clinical and Laboratory Haematologyvol 26 no 3 pp 159ndash176 2004
[11] S L Thein ldquoPathophysiology of beta thalassemiamdasha guide tomolecular therapiesrdquoHematologyAmerican Society of Hematol-ogy Education Program pp 31ndash37 2005
[12] M D Cappellini D Tavazzi L Duca et al ldquoMetabolic indica-tors of oxidative stress correlate with haemichrome attachmentto membrane band 3 aggregation and erythrophagocytosis in120573-thalassaemia intermediardquoBritish Journal of Haematology vol104 no 3 pp 504ndash512 1999
[13] R Evstatiev and C Gasche ldquoIron sensing and signallingrdquo Gutvol 61 no 6 pp 933ndash952 2012
[14] C Kattamis C Lazaropoulou P Delaporta F Apostolakou AKattamis and I Papassotiriou ldquoDisturbances of biomarkers ofiron and oxidant-antioxidant homeostasis in patients with beta-thalassemia intermediardquo Pediatric Endocrinology Reviews vol8 pp 256ndash262 2011
[15] Q Shazia Z H Mohammad T Rahman and H U ShekharldquoCorrelation of oxidative stress with serum trace elementlevels and antioxidant enzyme status in beta thalassemia majorpatients a review of the literaturerdquoAnemia vol 2012 Article ID270923 7 pages 2012
[16] E Fibach and E Rachmilewitz ldquoThe role of oxidative stress inhemolytic anemiardquoCurrentMolecularMedicine vol 8 no 7 pp609ndash619 2008
[17] T Nagy E Paszti M Kaplar H P Bhattoa and L Goth ldquoFur-ther acatalasemia mutations in human patients from Hungarywith diabetes and microcytic anemiardquo Mutation ResearchmdashFundamental and Molecular Mechanisms of Mutagenesis vol772 pp 10ndash14 2015
[18] L G Macdougall ldquoRed cell metabolism in iron deficiencyanemia III The relationship between glutathione peroxidasecatalase serum vitamin E and susceptibility of iron-deficientred cells to oxidative hemolysisrdquo The Journal of Pediatrics vol80 no 5 pp 775ndash782 1972
[19] ENagababu S Gulyani C J Earley R G CutlerM PMattsonand JM Rifkind ldquoIron-deficiency anaemia enhances red bloodcell oxidative stressrdquo Free Radical Research vol 42 no 9 pp824ndash829 2008
[20] N L Madhikarmi and K R S Murthy ldquoAntioxidant enzymesand oxidative stress in the erythrocytes of iron deficiency ane-mic patients supplemented with vitaminsrdquo Iranian BiomedicalJournal vol 18 no 2 pp 82ndash87 2014
[21] E Kurtoglu A Ugur A K Baltaci and L Undar ldquoEffect of ironsupplementation on oxidative stress and antioxidant status iniron-deficiency anemiardquo Biological Trace Element Research vol96 no 1ndash3 pp 117ndash123 2003
[22] L Goth ldquoTwo cases of acatalasemia in Hungaryrdquo ClinicaChimica Acta vol 207 no 1-2 pp 155ndash158 1992
[23] S S Lazarte M E Monaco A C Haro C L Jimenez ME Ledesma Achem and B A Isse ldquoMolecular characteriza-tion and phenotypical study of 120573-thalassemia in TucumanArgentinardquo Hemoglobin vol 38 no 6 pp 394ndash401 2014
[24] F Simsek G Ozturk S Kemahli D Erbas and A HasanogluldquoOxidant and antioxidant status in beta thalassemia majorpatientsrdquo Ankara Universitesi Tıp Fakultesi Mecmuası vol 58pp 34ndash38 2005
[25] Z Kosa T Nagy E Nagy F Fazakas and L Goth ldquoDecreasedblood catalase activity is not related to specific beta-thalassemiamutations in Hungaryrdquo International Journal of LaboratoryHematology vol 34 no 2 pp 172ndash178 2012
[26] G C Gerli L Beretta M Bianchi A Pellegatta and AAgostoni ldquoErythrocyte superoxide dismutase catalase andglutathione peroxidase activities in 120573-thalassemia (major andminor)rdquo Scandinavian Journal of Haematology vol 25 no 1 pp87ndash92 1980
[27] N Boudrahem-Addour M Izem-Meziane K Bouguerra etal ldquoOxidative status and plasma lipid profile in 120573-thalassemiapatientsrdquo Hemoglobin vol 39 no 1 pp 36ndash41 2015
[28] S Selek M Aslan M Horoz M Gur and O Erel ldquoOxidativestatus and serum PON1 activity in beta-thalassemia minorrdquoClinical Biochemistry vol 40 no 5-6 pp 287ndash291 2007
[29] L D S Ondei I D F Estevao M I P Rocha et al ldquoOxidativestress and antioxidant status in beta-thalassemia heterozygotesrdquoRevista Brasileira de Hematologia e Hemoterapia vol 35 no 6pp 409ndash413 2013
[30] H A Labib R L Etewa O A Gaber M Atfy T M Mostafaand I Barsoum ldquoParaoxonase-1 and oxidative status in com-mon Mediterranean 120573-thalassaemia mutations trait and theirrelations to atherosclerosisrdquo Journal of Clinical Pathology vol64 no 5 pp 437ndash442 2011
[31] M Vitai and L Goth ldquoReference ranges of normal blood cata-lase activity and levels in familial hypocatalasemia in HungaryrdquoClinica Chimica Acta vol 261 no 1 pp 35ndash42 1997
Advances in Hematology 7
[32] S Gardenghi R W Grady and S Rivella ldquoAnemia ineffectiveerythropoiesis and hepcidin interacting factors in abnormaliron metabolism leading to iron overload in 120573-thalassemiardquoHematologyOncology Clinics of North America vol 24 no 6pp 1089ndash1107 2010
[33] P BrissotM Ropert C Le Lan andO Loreal ldquoNon-transferrinbound iron a key role in iron overload and iron toxicityrdquoBiochimica et Biophysica ActamdashGeneral Subjects vol 1820 no3 pp 403ndash410 2012
[34] F Amirkhizi F Siassi S Minaie M Djalali A Rahimi andM Chamari ldquoAssessment of lipid peroxidation and activitiesof erythrocyte cytoprotective enzymes in women with irondeficiency anemiardquo Journal of Research in Medical Sciences vol13 no 5 pp 248ndash254 2008
[35] J-H Yoo H-Y Maeng Y-K Sun et al ldquoOxidative status iniron-deficiency anemiardquo Journal of Clinical Laboratory Analysisvol 23 no 5 pp 319ndash323 2009
[36] D Tekin S Yavuzer M Tekin N Akar and S Cin ldquoPossibleeffects of antioxidant status on increased platelet aggregation inchildhood iron-deficiency anemiardquoPediatrics International vol43 no 1 pp 74ndash77 2001
[37] A Bay M Dogan K Bulan S Kaba N Demir and A FOner ldquoA study on the effects of pica and iron-deficiency anemiaon oxidative stress antioxidant capacity and trace elementsrdquoHuman and Experimental Toxicology vol 32 no 9 pp 895ndash9032013
[38] A Vaya M Simo M Santaolaria J Todolı and J Aznar ldquoRedblood cell deformability in iron deficiency anaemiardquo ClinicalHemorheology and Microcirculation vol 33 no 1 pp 75ndash802005
[39] D S Kempe P A Lang C Duranton et al ldquoEnhancedprogrammed cell death of iron-deficient erythrocytesrdquo TheFASEB Journal vol 20 no 2 pp 368ndash370 2006
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Advances in Hematology 7
[32] S Gardenghi R W Grady and S Rivella ldquoAnemia ineffectiveerythropoiesis and hepcidin interacting factors in abnormaliron metabolism leading to iron overload in 120573-thalassemiardquoHematologyOncology Clinics of North America vol 24 no 6pp 1089ndash1107 2010
[33] P BrissotM Ropert C Le Lan andO Loreal ldquoNon-transferrinbound iron a key role in iron overload and iron toxicityrdquoBiochimica et Biophysica ActamdashGeneral Subjects vol 1820 no3 pp 403ndash410 2012
[34] F Amirkhizi F Siassi S Minaie M Djalali A Rahimi andM Chamari ldquoAssessment of lipid peroxidation and activitiesof erythrocyte cytoprotective enzymes in women with irondeficiency anemiardquo Journal of Research in Medical Sciences vol13 no 5 pp 248ndash254 2008
[35] J-H Yoo H-Y Maeng Y-K Sun et al ldquoOxidative status iniron-deficiency anemiardquo Journal of Clinical Laboratory Analysisvol 23 no 5 pp 319ndash323 2009
[36] D Tekin S Yavuzer M Tekin N Akar and S Cin ldquoPossibleeffects of antioxidant status on increased platelet aggregation inchildhood iron-deficiency anemiardquoPediatrics International vol43 no 1 pp 74ndash77 2001
[37] A Bay M Dogan K Bulan S Kaba N Demir and A FOner ldquoA study on the effects of pica and iron-deficiency anemiaon oxidative stress antioxidant capacity and trace elementsrdquoHuman and Experimental Toxicology vol 32 no 9 pp 895ndash9032013
[38] A Vaya M Simo M Santaolaria J Todolı and J Aznar ldquoRedblood cell deformability in iron deficiency anaemiardquo ClinicalHemorheology and Microcirculation vol 33 no 1 pp 75ndash802005
[39] D S Kempe P A Lang C Duranton et al ldquoEnhancedprogrammed cell death of iron-deficient erythrocytesrdquo TheFASEB Journal vol 20 no 2 pp 368ndash370 2006
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom