erasmus mundus master course in emergency and critical ... pokhrel bhattarai.pdf · (acls) among...
TRANSCRIPT
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
(EMECC NURSING)
“AWARENESS ON ADVANCED CARDIAC LIFE SUPPORT AMONG NURSES”
AUTHOR
SUNITA POKHREL BHATTARAI
FEBRUARY, 2017
Master´s Thesis
ii
Erasmus Mundus Master Course in Emergency and Critical Care Nursing

iii
Erasmus Mundus Master Course in Emergency and Critical Care Nursing

iv
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
(EMECC NURSING)
“AWARENESS ON ADVANCED CARDIAC LIFE SUPPORT AMONG NURSES”
Master’s Thesis
Name of Author
Sunita Pokhrel Bhattarai

v
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
LIST OF ACRONYMS AND ABBREVIATIONS
ACLS Advanced cardiac life support
AHA American Heart Association
ALS Advance Life Support
BLS Basic Life Support
CCU Coronary Care Units
CMS Center for Medical Simulation
CPA Cardiopulmonary arrest
CPR Cardiopulmonary Resusciation
ECC Emergency Cardiac Care
ECG Electrocardiography
ED Emergency Departments
ER Emergency
ICU Intensive Care Unit
INE Instituto Nacional de Estatística
MICU Medical Intensive Care Unit
SICU Surgical Intensive Care Unit
SPSS Statistical Package for Social Science

vi
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
TABLE OF CONTENTS
1. INTRODUCTION ................................................................................................................... 1
1.1 RATIONAL OF THE STUDY ................................................................................................. 3
1.2 OBJECTIVES ........................................................................................................................... 4
2.LITERATURE REVIEW ............................................................................................................ 5
3. METHODOLOGY ................................................................................................................... 11
3.1 Research Design .................................................................................................................. 11
3.2 Paradigm and Research Type .............................................................................................. 11
3.3 Delineation of Space (context) and Time ............................................................................ 11
3.4 Study Population ................................................................................................................. 12
3.5 Sampling.............................................................................................................................. 12
3.6 Inclusion Criteria ................................................................................................................. 12
3.7 Exclusion Criteria ................................................................................................................ 12
3.8 Data collection..................................................................................................................... 12
3.9 Process of Data Collection .................................................................................................. 13
3.10 Reliability and Validity of the Questionnaire ................................................................... 14
3.11 Data Analysis Process ....................................................................................................... 14
3.12 Variables............................................................................................................................ 15

vii
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
3.13 Operational Definitions ..................................................................................................... 16
3.14 Ethical Consideration ........................................................................................................ 17
3.15 Limitation .......................................................................................................................... 17
4.RESULTS .................................................................................................................................. 19
5. DISCUSSION ........................................................................................................................... 30
6. CONCLUSION ......................................................................................................................... 32
7. RECOMMENDATION ............................................................................................................ 33
REFERENCES
ANNEX I
ANNEX II
ANNEX III

viii
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
TABLES
Table 1: Study Participant’s Basic Characteristics ....................................................................... 19
Table 2: Working Area of the Participants’. ................................................................................. 21
Table 3: Respondents’ Clinical Competence ................................................................................ 21
Table 4: ACLS Training ............................................................................................................... 22
Table 5: Time of ACLS Training Taken ....................................................................................... 22
Table 6: Performed ACLS ............................................................................................................ 22
Table 7: Patient's outcome after ACLS ......................................................................................... 23
Table 8: Outcome of Awareness Based Questions ....................................................................... 23
Table 9Awareness among the Student Nurse and the Professional Nurse ................................... 24
Table 10 Cross Tabulation based on Clinical competence and Outcome ..................................... 25
Table 11: Country and Awareness Outcomes Cross Tabulation .................................................. 25
Table 12: Cross Tabulation based on Education and Outcome of Awareness based Questions .. 25
Table 13: Cross Tabulation of Economic Status and Outcome of Awareness ............................. 26
Table 14Work Experience and Outcome Cross Tabulation ......................................................... 27
Table 15 ACLS Training and Outcome Cross Tabulation............................................................ 27
Table 16 Clinical Competence and Outcome of Awareness Cross Tabulation ............................ 28
Table 17 Outcome of Awareness and Patient's Condition Cross Tabulation .............................. 28
ix
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
FIGURES
Figure 1 Conceptual Framework of the study............................................................................... 10
Figure 2 Distribution of the Study Participants. ........................................................................... 11
Figure 3 Process of data collection ............................................................................................... 14

x
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
ACKNOWLEDGEMENT
This study has been conducted to identify the awareness of Advanced Cardiac Life Support among
the nurses in Nepal and Portugal.
First, I would like to thank my thesis supervisor Professor, José Amendoeira for his great co-
operation, continuous support, valuable comments, feedback and advice on this study enhancing
the successful completion of the study. I want to acknowledge Dr. Cátia Luís nursing school of
Santarem for helping me in translation of my survey tool.
I express my deep gratitude to campus chief Muna Rana for giving me permission for data
collection, Instructor Srijana Chaudhary, Indira Chaurasiya, sister Pramila Shrestha and nursing
ward in-charges at Shahid Gangalal National Heart Center for helping me during the entire period
of data collection. Thankful to Binita Tamrakar for helping me in the process of ethical approval
process at Intuitional review board at Shahid Gangalal National Heart Center.
This study was made possible by continuous cooperation of my daughter Aahana, my husband and
my parents.
Last but not the least, I would like to extend my thanks to all the people who helped directly or
indirectly during this entire study.
xi
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
ABSTRACT
Objective of this study is to identify the awareness regarding Advanced Cardiac Life Support
(ACLS) among student and the professional nurses. Health care professional are expected to have
awareness on Advanced Cardiac Life Support guidelines to revive unresponsive patient This study
is conceptualized based on the Patricia Benner’s nursing theory Novice to Expert theory. A cross-
sectional study was conducted to identify the awareness regarding Advanced Cardiac Life Support
(ACLS) among nurses using online survey. Questions and Answers were validated in accordance
with American Heart Association’s ACLS pre-assessment test and results were analyzed. The
response rate for this online survey is 33.5%. Among the 66 participants 4.5% were male and
94.5% were female. Mean age of the participants was 29.42(SD± 7.9). Participants from Nepal
were 74.2% and 24.8% from Portugal. Mean score of awareness based questions among the
respondents were 12.92 (SD±7.812). Only 10.06% of them passed the American Heart
Association’s standard 84% of the awareness based questions test and greater than 50% score was
achieved by 34.84%. There are no statistically significant findings in terms of age, sex, work
experience and working area in this study. Statistically significant correlation was not seen (p=0.9)
between the training of ACLS of the participants and the awareness. This study shows no statistical
significant between the educational background (p=0.06), ACLS performed (p=0.2) and ACLS
training taken 3 months ago, (p=0.9), 6 months ago (p=0.9), 1 year ago(p=0.9), 2 years ago,(p=0.7)
and more than 2 years(p=0.9) and awareness. ACLS provided by ACLS- trained or non-trained
participants, the survival rate was two-fold higher when the participant assisting the patient was
ACLS trained. There was no significant association found between different clinical competence

xii
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
(p= 0.00), demographic variables and patient outcomes with the awareness of ACLS. This study
highlights the level of awareness of ACLS among the student nurses and Professional nurses is
poor. Student nurses were less aware than the professional nurses. Poor awareness makes more
challenging for the nurses working in critical care settings. This study findings concludes that
nurses were less aware of ACLS. Therefore, this study recommends to incorporate ACLS courses
into the nursing curriculum and Certification Program should be initiated for the nurses working
in critical care settings as refreshing training should be organized in the hospital.
KEY WORDS: Advanced Cardiac Life Support, Nurses, Awareness.
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
1. INTRODUCTION`
The American Heart Association (AHA) frames and periodically updates Cardiopulmonary
Resuscitation (CPR) and Emergency Cardiac Care (ECC) guidelines on how to provide basic and
advanced cardiac life support (BLS/ACLS) to resuscitate valuable lives(AHA,2015). Initially,
emergency medical services have invested substantial resources to establish advanced life support
(ALS) programs (Isenberg DL, 2005). This helps for high- performance team dynamics and
communication, system of care, recognition and intervention of cardiopulmonary arrest,
immediate post-cardiac arrest, acute dysrhythmia, stroke, and acute coronary syndromes
(ACS)(American Heart Association, 2015). Nurses are expected to have current
knowledge/awareness of BLS/ACLS guidelines to revive unresponsive and cardiac arrest
patients(Nambiar, 2016). Unlike in Western countries, there are no strict licensing protocols in
Nepal and other developing countries that mandate physicians, nurses and paramedics to be trained
in current BLS/ACLS guideline.
Nepal is a country with 26,494,504 of population and youth male and female literacy rate is 89.9%
and 77.5% respectively. Total health expenditure per capita 68$. The health workforce doctors and
nurses along with midwives are 0.17 and 0.51 per thousand population respectively (MoHP,2014).
According to the Instituto Nacional de Estatística (INE) Portugal has 10,562,178 population in
2011 (Wikipedia , 2016) with adult literacy rate 95.43%.Portugal has one of the lowest nurse to
population and to physician ratios in develop countries, and one of the highest physician to
population ratios (James Buchan, 2013).
2
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
Nursing professionals are usually the first to witness a cardiac arrest at the hospital (H. Gombotz,
2006).It is important that nurses must be able to respond correctly in the event of a cardiac arrest
in hospital (Bruce SA, 2009). Most of the nursing educational institutes have resuscitations training
within their curricula to meet these expectations and to ensure that students are competent at
commencing life support in case of cardiac arrest and it is very important component in nursing
education because nurses are involved in every level of resuscitation from early identification to
post-care and rehabilitation (Hagyard-Wiebe, 2007). Therefore, knowledge regarding the location
of emergency equipment as well as checking and stocking for resuscitation is required, they should
have the education and ability to perform the tasks (Practice Resource Network., 2008).
Knowledge breeds knowledge and the clinical skills and knowledge needed to care for patients
continue to change dramatically (Hall, 2015). It is the individual nurse’s professional
responsibility to ensure he or she is updated with current guidelines and it is also the employer’s
responsibility to assist the nurse in maintaining the competence by providing opportunities to
practice mock scenarios for maintaining the psychomotor skills and critically thinking abilities
required to manage a cardiac arrest effectively (Hagyard-Wiebe T. , 2007). Several studies show
that medical and nursing staff lack knowledge and skills in acute care(Jasmeet Soar, 2015)
Therefore, with this background we can see that many studies have been conducted to evaluate the
knowledge and skill before and after ACLS training by using the self –administer questionnaire
and observing the practical skill by using check list. But studies for identifying the awareness
hasn’t been conducted before in Nepal. The aim of this study is to identify the awareness of ACLS

3
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
among nurses working in critical care settings in hospital and academic institutions in Nepal and
Portugal.
1.1 RATIONAL OF THE STUDY
Nursing care is an integral part of health service delivery in hospitals, care homes as well as
community. Over the time nursing profession has been professionalized as being a part of business.
The need of well qualified nurses in developed countries became a catalytic factor for booming
nurse producing industry in a developing country like Nepal (Subedi, 2014).Hence, public
expectations from healthcare professionals in emergency care are also high both in Nepal and
Portugal.
This study focuses on the awareness on core components of advanced cardiac life support among
the nurses such as ECG interpretation, pharmacology and application. It is very important to
integrate in nursing curriculum as well as training to the professional nurses. Therefore, this study
will help to identify the level of awareness among the student nurses and professional nurses and
helps to make attention to the concern bodies in the academic institutions and hospital authorities.

4
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
1.2 OBJECTIVES
ACLS guidelines have evolved over the past several decades. AHA developed the most recent
ACLS guidelines in 2010 using the comprehensive review of resuscitation literature performed by
the International Liaison Committee on Resuscitation (ILCOR), and these were updated in 2015.
Guidelines are reviewed continually but are formally released every five years (Pozner, 2016).
It is not possible to enroll all health care staff in the hospital for such a training as it is time
consuming and the cost of such training programs is high. Training and certification would easily
cost more money and it is a significant cost for staff to afford it (Saravana Kumar, 2014).
General Objective:
The aim of the study is to assess the nurses’ existing awareness on Advance Cardiac Life Support
among student nurses and professional nurses.
Specific Objectives:
1. To identify the existing awareness among student nurses and professional nurses.
2. To assess the factors that affects the awareness for ACLS.
5
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
2.LITERATURE REVIEW
Advance cardiac life support (ACLS) is a systematic approach of resuscitation efforts, and the aim
of the resuscitation is to sustain the neurological functioning and the same quality of life that
previously experienced by the patient. Advanced cardiac life support (ACLS) was designed to
achieve this aim and survival from cardiac arrest depends largely on prompt initiation of
cardiopulmonary resuscitation. Day by day cardiac arrest is becoming the major healthcare issue,
and according to recent publications approximately half of the in-hospital cardiac arrests happen
in intensive care units (Efendijev, 2014). Cardiac arrest is considerably increased in recent decades
and low rates of cardiopulmonary resuscitation (CPR) is performed which results only 1.6%
cardiac arrest patient survived in hospital (Davidson Ocen, 2015).
An organized team response and trained nursing staff in the emergency room critical patient area
are the main factors to determine cardiopulmonary resuscitation (CPR) success rates(A Villamor,
2014).Although nurses must be able to respond quickly and effectively to cardiac arrest, numerous
studies demonstrated poor performances (Sissel I Eikeland Husebø, 2012). Similarly, nurses'
knowledge and skill retention of resuscitation is reported to be poor (Hamilton, 2013).
Nursing professionals are usually the first to witness a cardiac arrest at the hospital (H. Gombotz,
2006).It is important that nurses must be able to respond correctly in the event of a cardiac arrest
in hospital (Bruce SA, 2009). Most of the nursing educational institutes have resuscitations training
within their curricula to meet these expectations and to ensure that students are competent at
commencing life support in case of cardiac arrest and it is very important component in nursing
education because nurses are involved in every level of resuscitation from early identification to

6
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
post-care and rehabilitation (Hagyard-Wiebe, 2007). Therefore, knowledge regarding the location
of emergency equipment as well as checking and stocking for resuscitation is required, they should
have the education and ability to perform the tasks (Practice Resource Network., 2008).
Knowledge breeds knowledge and the clinical skills and knowledge needed to care for patients
continue to change dramatically (Hall, 2015). Although we have come a long way in
multidisciplinary resuscitation education, there remains a gap in the standardization of ACLS
training as a requirement for nurses’ employment both nationally and internationally. Training in
these principles to improve the quality of ACLS performed by healthcare clinicians is feasible and
recommended (Pozner, 2016). It is estimated that ACLS training costs approximately one billion
dollars annually. It is the individual nurse’s professional responsibility also the employer’s
responsibility to assist the nurse in maintaining this competence by providing opportunities to
practice mock scenarios for maintaining the psychomotor skills and critical thinking abilities
required to manage a cardiac arrest effectively. to ensure he or she is updated with current
guidelines (Hagyard-Wiebe T. , 2007).
Cardiac arrest is a major public health issue, with more than 500, 000 deaths of children and adults
per year in the United States (Stiell IG, 2012). In Europe, major European institutions report
cardiovascular diseases are the first cause of death in adults, with cardiac arrest and sudden death
(Freddy K. Lippert, 2010). Those diseases are increases day by day in developing countries. This
should be treated in very short period. As we know that among all the health professional nurses
are the one who stay 24 hour with patient and discover the cardio pulmonary attest and provide
care. Therefore, the advanced cardiac life support (ACLS) is an essential competency which all

7
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
nurses should acquire ( B. Prasanatikom, 2010). ACLS requires the ability to manage the patient’s
airway, initiate intravenous access, read and interpret electrocardiograms, and deliver emergency
pharmacology that aims to treat or reverse the cause of the arrest. Even though nurses are expected
to perform ACLS many literatures suggested that has nurses’ poor knowledge of ACLS and lack
of confidence to work. One study on in-hospital resuscitation: association between ACLS training
and survival to discharge has shown the presence of at least one professional trained in ALS
increase the survival of cardiac arrest victim(Lima S. G., 2009). Dane et al reported increase of the
survival in around four times when the nursing professional was trained in ALS (Dane, 2000).
Primarily mushrooming of nursing colleges is a big challenge to improve the quality of nursing
care in Nepal. Almost 6, 000 certificate level of nurses and Bsc. Nurses were produced. It is very
important to know how competent they are to work with direct patient in the hospital. To develop
the competency in ACLS center for Medical Simulation (CMS) has been established since 2014.
Apart from this hospital hasn’t conducted any formal trainings to nurses in Nepal. So, it is
important to know the existing awareness of ACLS among nurses. This area is chosen because
critical care settings are normally well equipped with experienced professional services, including
intensive care units (ICUs) and emergency care services. And the awareness on ACLS is also
important for critical care settings Nurses and student nurses to develop work competency.
Therefore, with this background we can see that studies have been conducted to evaluate the
knowledge and skill before and after ACLS training by using the self –administer questionnaire
and observing the practical skill by using check list (Hamilton, 2013). But studies for identifying
the awareness in general hasn’t been conducted before. The aim of this study is to identify the

8
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
awareness of ACLS among nurses working in critical care settings in hospital and academic
institutions in Nepal and Portugal.
Awareness is the knowledge and understanding of a situation. To be aware for something
knowledge is very important component. Working in a critical care settings requires constant
updates in knowledge (EAPCI, 2016).This framework has been developed. This study is based on
framework developed by Cardiovascular Council of Nurses and Allied Professions (CCNAP)
(Felicity Astin, 2015) and study in Spain based on nurse education and professional profile and
seeks to measure nurse expertise and hospital context to characterize their potential impact in
patient health outcome (Faura T, 2014).
The nurse theorist, Patricia Benner, provides us with a useful model that describes a continuum of
nursing experience made up of five levels ranging from novice to expert (Benner P, 1982). This
study used this model to identify the level of awareness of ACLS among nurses (student and
professional).
Benner’s Model Novice to Expert Theory
Benner’s (1984) model of Novice to Expert shows the importance of experience in developing
expert nurses. According to (Benner,1984) knowledge developing in nursing expands practical
knowledge through theory and clinical experience. The Dreyfus model applied to nursing practice
is described in five stages : Novice, Advanced Beginner, Competent, Proficient , and Expert
(Benner,1984). Nursing students are novices and they have limited understanding of the
applicaation of textbook terms in the cliniccal settings (Benner,1984). Advanced beginners are
9
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
nurses that demonstrates acceptable performances through experience of actual situation in which
knowledge is applied to nursing (Benner,1984). Competent nurses have experiences related
situations in nursing practice and have utilized strategies to achieve efficiency and organization
(Benner,1984). The Proficient nurses views experiences holistically and develps meaning through
long-term goals (Benner,1984) . The Proficient nurse has learned what to expect in certain situation
and understand how to adjust actions in response to events (Benner,1984). The Expert nurse
understands each situations and focuses on the specific problem without having to eliminate others
options first (Benner,1984).
This study consider novice level to the student who is in final year in Nursing program and had
experience in critical care setting, advanced beginner less than one year ,competent 2-3 years ,
Proficient 3-5 years and Expert more than 5 years of clinical experience in critical care setting.
The four paradigms
Nursing: Nursing is an academic discipline and practice profession which consists of two
components academic and practice which helps to qualify to provide evidenced-based care to
patient to achieve the optimal level of patient’s wellness.
Person: Person is a nurse providing nursing care to critically ill or unresponsive patient.
Health: Health is the state of critically ill patient or unresponsive patient’s outcome after the
nurses’ effort associated with clinical competence, awareness, and environment that affects the
awareness .
Environment: It is a context,settings or situation that affects the awareness of care giver and helath
status of care recipient.

10
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
Figure 1 Conceptual Framework of the study
Levels of work experiences
in critical areas
Level 1: Novice (beginning of
the study in critical care or
emergency)
Level 2: Advanced Beginner
(experience less than 1 year)
Level3: Competent
(experience between 2-3
years)
Level 4: Proficient (experience
between 3-5 years)
Level 5: Expert (experience
more than 5 years)
Nursing: Care based
on Nurses’
awareness of
Advanced Cardiac
Life Support in the
aspect of Rhythm
identification,
Pharmacology and
practical Implication
Environment
(Situation)
i. Economic
condition
ii. Education
iii. Training of
ACLS
iv. Time gap for
training
v. Experience of
working with
unresponsive
patient
vi. Frequency of
working with
unresponsive
patient
Health: Patient Outcomes
Person(Nurse): Age Sex,
11
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
This chapter dealt with the review of published and unpublished literature related to the research
study. This enabled the investigator to have deep insight into the problem under study and helped
to develop tool, methodology and in completing the research study.
3. METHODOLOGY
3.1 Research Design
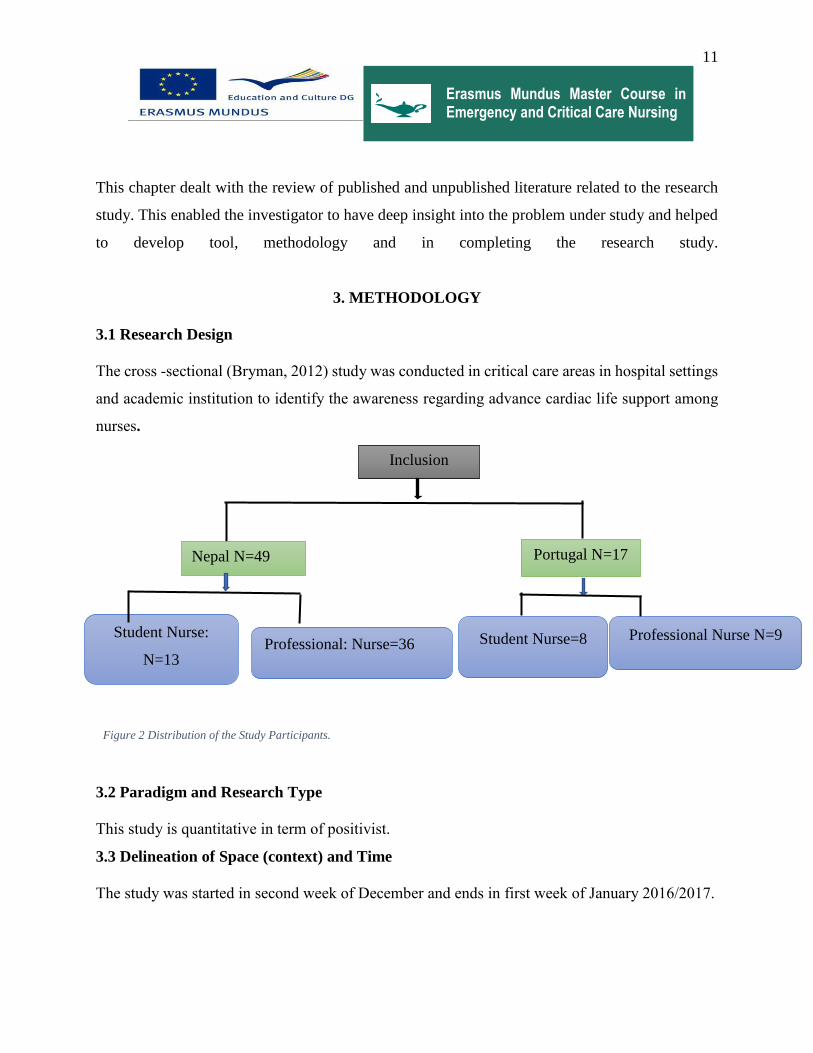
The cross -sectional (Bryman, 2012) study was conducted in critical care areas in hospital settings
and academic institution to identify the awareness regarding advance cardiac life support among
nurses.
Figure 2 Distribution of the Study Participants.
3.2 Paradigm and Research Type
This study is quantitative in term of positivist.
3.3 Delineation of Space (context) and Time
The study was started in second week of December and ends in first week of January 2016/2017.
Inclusion
Portugal N=17 Nepal N=49
Student Nurse:
N=13 Professional: Nurse=36 Student Nurse=8 Professional Nurse N=9

12
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
3.4 Study Population
This study was conducted in intensive care units (ICUs), Coronary Care Units(CCU), Medical
|Intensive care unit(MICU), Surgical Intensive Care Unit(SICU) and Emergency Departments at
Shahid Gangalal National Heart Centre in Kathmandu and Hospital of Santarém in Portugal and
for academic institution Birgunj Nursing Campus in Birgunj and Escola Superior de Saúde de
Santarém to identify the awareness regarding advance cardiac life support among nurses.
3.5 Sampling
Non-probability (convenient) sampling method was used in this study.
3.6 Inclusion Criteria
The inclusion criteria for this research study:
Student Nurses who are studying in final year for Nursing.
Working registered nurses in critical care setting.
Nurses who are willing to participate
Nurses who are available at the time of data collection
3.7 Exclusion Criteria
Nurses who are not willing to participate in the study were excluded.
Nurses who were on leave for various purposes e.g. sick leave, maternity leave, study leave
etc. during data collection period were not included in the study.
Nurses in managerial level e.g. nursing in charge, nursing supervisor.
3.8 Data collection
For data collection, online survey was used to collect information from the respondents including
multiple choice format. This online survey method is used because it is user-friendly, saves time
and it also reduces the likelihood of errors in the processing of data(Bryman, 2012). Online

13
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
surveying practice varies greatly. For example, in Australia, the University of South Australia uses
a system supporting solely online administration of surveys, while Murdoch University and Curtin
University among others are moving the same way (Nulty, 2008).
3.9 Process of Data Collection
After the ethical approval was accepted from the Nepal Health Research Council and Institutional
Review Board from Hospital Nursing supervisor was informed and explained about the data
collection process, nursing supervisor informed all the nursing unit in-charge and informed about
the study and online survey process and unit in- charge provided the survey link to all the interested
participants. For the Nursing college permission was taken from the chief of the college and survey
link was provided to selected students in Nepal.
In Portugal, after my research title was approved by the school of nursing in Santarem my
supervisor facilitated me to make the network with the students and hospital in an organized way
and helped me for data collection by providing the online survey link to the participants. In
addition, he also helped by sending messages for reminding them to fill the survey tool.

14
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
Figure 3 Process of data collection
3.10 Reliability and Validity of the Questionnaire
Internal reliability was measured by calculating the correlation between the variables(Bryman,
2012). Measurement scale were consistent (Bryman, 2012)to evaluate the awareness among
nurses’ tools were adopted from the American Heart Association for self -assessment test. To
establish the validity in the study, study tools were asked to judge with experience and expert in
the related field. In addition, content validity was tested and reviewed by expert and process of
assessment was explained to the expert. Study tool was translated in the Portuguese by the
authorized person and again the retroversion by another expert from Portuguese to English after
translation. The content validity of the questionnaire was examined by compiling the content of
the instrument with available literature review on the topic.
3.11 Data Analysis Process
Data collection was followed by data analysis and interpretation of collected data. Collected data
was analysed and interpreted in accordance with study objectives.
Hospitals
Academic Institution
Nursing Supervisor
Ward In-charge
Participants
Campus Chief
Faculty Head

15
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
Data editing was done to make the uniformity of the data. Sampling errors were identified and
incomplete respondent were removed.
Data Coding was done into numerical values or assigning numbers to the various categories of a
variable was used in data analysis.
Data classification / distribution: Percentage distribution was calculated for the followings:
Demographic and Variables Part one: Age, Sex, Education, Economic condition, Work
Experience, Training on ACLS, Time of Training, Experience of working with unresponsive
patient, Frequency of working with the unresponsive patient.
Awareness related Variables: Aware and Aware
Statistical data distribution: Mean average was calculated to the appropriate variables.
4. Tabulation of the data: The finding of the study was displayed by inserting the frequency
tables and contingency tables.
Data was analysed by using the Statistical Package for Social Sciences (SPSS) Version 24.0
program. Descriptive statistics such as frequencies: percentiles, descriptive: mean, range and
standard deviation and cross tabulation: cross tabulation of different variables and correlations was
analyzed.
Relationships between demographic variables and awareness outcome was analyzed by using the
logistic regression and chi-square .
3.12 Variables
Dependent Variables: ACLS awareness
Independent Variables: Training of ACLS, Time gap for training, Experience of working with
cardiac arrest, Frequency of working with cardiac arrest.

16
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
Demographic variables: Age, Gender, Education, Economic condition
Classification of the different types of variable that are generated during this study
Continuous Variables: Age, work experience, time of training or frequency of training
Ordinal Variables: Education, Clinical competence,
Nominal Variables/ Dichotomous variables: Gender, Training on ACLS, Economic
condition
3.13 Operational Definitions
Age: it is the age of the respondent
Gender: gender of respondent
Education: Education in nursing field i.e. certificate nurse, diploma nurse, bachelor nurse, master
and any other specialization
Economic condition: affordable or unaffordable for the ACLS training
Work Experience: total duration of work experience in nursing field
Training on ACLS: formal training with certificate for ACLS
Time of Training: time of training taken total in month
Frequency of taking or gap for training: how often training was taken 2 yearly as recommended
by AHA.
Aware: Respondent one who scored ≤84% of awareness based questions.
Unware: Respondent one who scored < 84% of awareness based questions.
Clinical Competence
Level I: Final year of Clinical Education with critical care setting experiences

17
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
Level II: less than 1 year of work experience in critical care setting
Level III: on the job for 2 to 3 years and able to develop actions in terms of long goal or
plans
Level IV:3-5 years’ experiences
Level V: Expert more than 5 years of work experience
3.14 Ethical Consideration
Before conducting the study the title was approved by the supervisor and Instructional Review
Board of Institute of Polytechnic Santarem, Portugal, Nepal Health Research Council and
institutional review board from the hospitals, colleges in Portugal and Nepal. The study technique
was considered ethically safe or neutral and free from harm such as physical harm; harm to
participants’ development; loss of self-esteem; stress. The development of the study was mindful
of manner of wordings to be emotionally neutral. The study didn’t include identifying personal
information; therefore, confidentiality was maintained. Informed consent was attached to the
questionnaire so that participants can make decision whether they like to participate or not.
Online Survey link was send to all the participants attached one who agreed to participate in the
study. A covering letter was attached to link page, explaining the details of the study. Participation
were voluntary. The right to decline or to withdraw from the study at any stage was explained. All
data were kept locked up, accessible only to the researcher.
3.15 Limitation
Since this is an online questionnaire based study, awareness cannot be assessed in detailed. The
study tools used only the theoretical part so skill cannot be studied. Time frame for data collection

18
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
is short because it took long time for ethical approval from hospital and research council. Lack of
internet services for participants cannot participate in the study. This study included only the nurses
who are working in the critical care setting and final year nursing students from the academic
institution. This study adopted the non-probability sampling method therefore, there might be bias
and small sample size so that this study findings cannot be generalized to other population.

19
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
4.RESULTS
The objective of this study is to assess the nurses’ existing awareness on Advance Cardiac Life
Support among student and professional nurses. Study tool for this study contains two parts, part
one for socio-demographic information and part two for awareness based questions. There were
30 questions total based on awareness fractioned in three sections, section 1 namely Rhythm
Identification (10 questions), section 2 pharmacology (10 questions), and section 3 practical
application (10 questions). The rhythm identification section tested the ability to identify the most
common normal and abnormal ECGs, which include ventricular fibrillation, ventricular
tachycardia, etc. The pharmacology section tested when and how to use medications correctly in
those complicated ACLS scenarios, and the practical application section asked participants to
identify rhythms and choose correct interventions or drugs. Each question has equal worth
therefore, each question contains one mark. There were total 96 respondents until the deadline of
data collection. Out of total 96 respondents 32 of them were excluded because of the missing data.
The response rate for online survey was 33.5%. The basic characteristics of the study participants
were summarized in the Tables 1.
Table 1: Study Participant’s Basic Characteristics
Gender n=66
Frequency Percent
Male 3 4.5
Female 63 95.5
Country
Frequency Percent

20
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
Nepal 49 74.2
Portugal 17 25.8
Education
Frequency Percent
Ongoing Certificate Level of
Nursing
1 1.5
Completed Certificate Level of
Nursing
10 15.2
Ongoing Bachelor Level of Nursing 12 18.2
Completed Bachelor Level of
Nursing
32 48.5
Master’s Degree in Nursing 8 12.1
Specialized course taken (please
specify the area)
3 4.5
Economic Status
Frequency Percent
Affordable to ACLS 44 66.7
Unaffordable to ACLS 22 33.3
Total 66 100.0
The minimum age of the participants was 19 years and maximum aged 53 years. Mean age was
29.42(SD± 7.9).
Among all the respondents 4.5% of them were male and 95.5% of them were female. Three- fourth
of the respondents were from Nepal and remaining one-fourth were from Portugal.
Majority of the respondents 48.5% had completed Bachelor level of Nursing followed by, ongoing
Bachelor level of nursing, completed certificate level of nursing, master’s degree in Nursing with
18.2%, 15.2% and 12.1% respectively. Only 1.5 % of the respondents were studying certificate
level of nursing and 4.5% of them had had some specialized courses.

21
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
Respondents were asked about the economic status to identify whether they were affordable or
unaffordable for ACLS training two-third (66.7%) of them were identified that they were
affordable and one- third (33.3%) were unfordable.
Work experience were calculated from the respondent it varies from less than 1 year to 30 years
(SD±7.5).
Table 2: Working Area of the Participants’.
Working Area
Frequency Percent
Cath lab 4 6.0
MICU 5 7.6
Student 7 10.6
Cardiology 10 15.2
CCU 10 15.2
SICU 10 15.2
ER 21 31.8
Total 66 100.0
Working area of the participants were summarized in Table 2. Majority of the respondents 31.8%
were working at Emergency Department (ER), respondents from surgical intensive care unit
(SICU), Coronary care unit (CCU), and Cardiology were 15.2% in each, 10.6% were students,
Medical intensive care units (MICU) and Cardiac Catherization lab 7.6 and 6% respectively.
Table 3: Respondents’ Clinical Competence
Clinical Competence
Frequency Percent
Level I 6 9.1
22
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
Level II 23 34.8
Level III - -
Level IV 22 33.3
Level V 15 22.7
Total 66 100.0
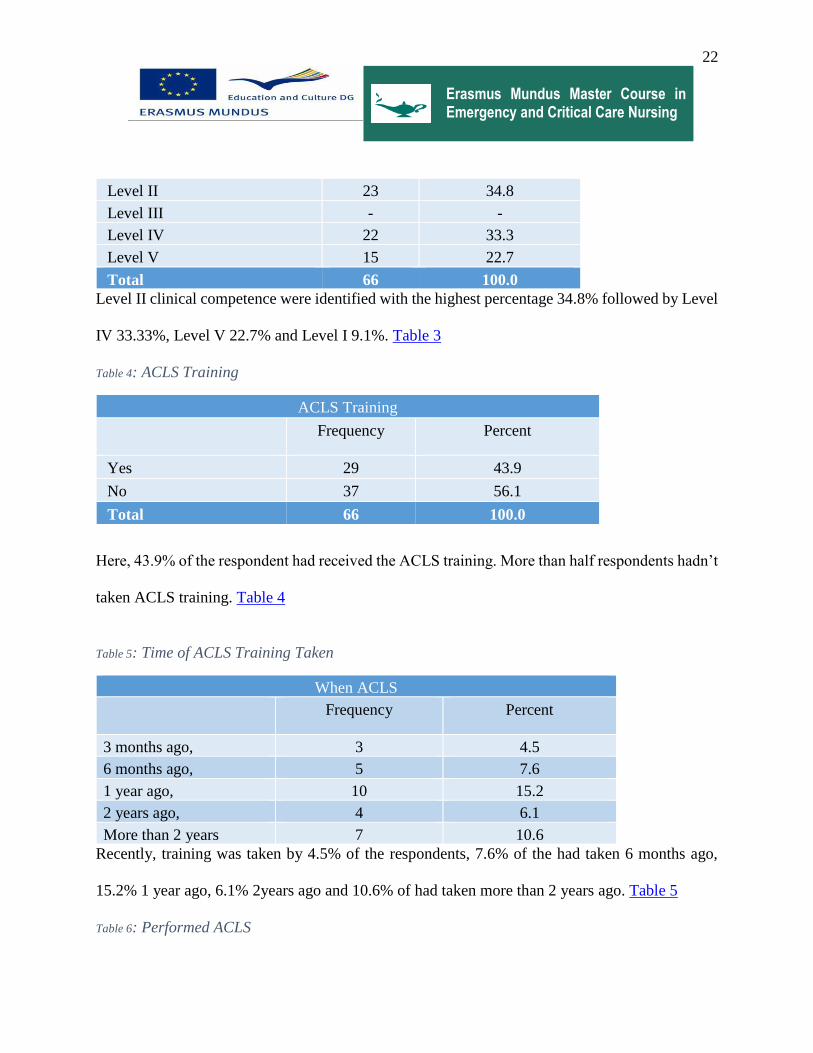
Level II clinical competence were identified with the highest percentage 34.8% followed by Level
IV 33.33%, Level V 22.7% and Level I 9.1%. Table 3
Table 4: ACLS Training
ACLS Training
Frequency Percent
Yes 29 43.9
No 37 56.1
Total 66 100.0
Here, 43.9% of the respondent had received the ACLS training. More than half respondents hadn’t
taken ACLS training. Table 4
Table 5: Time of ACLS Training Taken
When ACLS
Frequency Percent
3 months ago, 3 4.5
6 months ago, 5 7.6
1 year ago, 10 15.2
2 years ago, 4 6.1
More than 2 years 7 10.6
Recently, training was taken by 4.5% of the respondents, 7.6% of the had taken 6 months ago,
15.2% 1 year ago, 6.1% 2years ago and 10.6% of had taken more than 2 years ago. Table 5
Table 6: Performed ACLS

23
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
Performed ACLS to Unresponsive Patient
Frequency Percent
Yes 44 66.7
No 22 33.3
Total 66 100.0
Two-third of the respondents had performed ACLS and one-third hadn’t performed ACLS to
unresponsive patients. When questioned was asked if they had performed how often was it
performed respondent’s highest frequency was performed for 10-15 times per months but most of
them performed for 3-4 times per month. Table 6
Table 7: Patient's outcome after ACLS
Patient’s Condition
Frequency Percent
Survived 37 56.1
Expired 9 13.6
Respondents’ were asked about the patient’s condition after performing the ACLS to unresponsive
patients 56.1% of them responded that patients survived and 13.6% responded they were expired.
Table 7
Awareness Based Results
Mean score of awareness based questions among the respondents were 12.92 (SD±7.812). There
were all together 30 awareness based questions. AHA guidelines for successful course completion
and pass the written test of ACLS the test score should be 84% or higher. Only 10.06% of them
passed the AHA standard scoring 84% of the awareness based questions test.
Table 8: Outcome of Awareness Based Questions
Outcome of Awareness

24
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
Frequency Percent
Aware 7 10.6
Unaware 59 89.4
Total 66 100.0
Nearly, 90% of the respondents were unaware only, 10.6% were of ACLS. Table 8
Table 9Awareness among the Student Nurse and the Professional Nurse
Awareness Outcome* Student Professional Nurse Crosstabulation
Status Total
Student
Nurse
Professional
Nurse
Outcome Aware Count 2 5 7
% within Student
Professional Nurse
9.5% 11.1% 10.6%
Unaware Count 19 40 59
% within Student
Professional Nurse
90.5% 88.9% 89.4%
Total Count 21 45 66
% within Student
and Professional
Nurse
100.0% 100.0% 100.0%
Awareness Outcome with student and professional nurse crosstabulation shows that student nurses
were less aware compared to professional nurses. Among the student nurses, more than 90% were
unware of ACLS whereas 88.9% of the professional nurses shows unware. Altogether 10.6% were
aware and 89.4% were unware of ACLS. To establish how confident we can be that there is a
relationship between the two variables awareness outcome with student nurse and professional
nurse by calculating the chi-square (χ2) test in which associated level of significance is p <0.8.
This means this relation between the variables is less significant in this study. Table 9

25
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
Table 10 Cross Tabulation based on Clinical competence and Outcome
Awareness Outcome Total
Aware Unaware
Clinical Competence Level I 0(0) 6(9.09) 6
Level II 2(3.03) 21(31.18) 23
Level IV 4(6.06) 18(27.27) 22
Level V: 1(1.51) 14(21.21) 15
Total 7(10.60) 59(89.40) 66
*Paracentesis contains Percentage.
This cross tabulation in Table10 shows level IV has the highest level of awareness on ACLS and
Level I respondents were totally unware, in Level II respondents 3.03% of aware which is followed
by level V with 1.51%. Pearson Chi-square shows week relationship with p<0.4 and coefficient
value is 0.1.
Table 11: Country and Awareness Outcomes Cross Tabulation
Country * Awareness Outcome Crosstabulation
Awareness Outcomes Total
Aware Unaware
Country Nepal 6(9.09) 43(65.15) 49(74.24)
Portugal 1(1.51) 16(24.24) 17(25.75)
Total 7(10.60) 59(89.40) 66(100.0) *Paracentesis contains Percentage
Nearly 75% of the respondents were participated from Nepal among them 9.09% and 1.51 % were
aware of ACLS respectively from Nepal and Portugal. Table 11
Table 12: Cross Tabulation based on Education and Outcome of Awareness based Questions
Education * Outcome of Awareness based Questions Crosstabulation

26
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
Awareness based questions
outcome
Total
Aware> 84% Unaware
84%
Education Ongoing Certificate Level of
Nursing
0 1 1
Completed Certificate Level of
Nursing
0 10 10
Ongoing Bachelor Level of Nursing 1 11 12
Completed Bachelor Level of
Nursing
5 27 32
Masters in Nursing 1 7 8
Specialized course taken (please
specify the area)
0 3 3
Total 7 59 66
The cross tabulation in Table 12 reveals education and outcomes of awareness shows that
respondents studying certificate level of nursing and one who had completed certificate level of
nursing were unware about ACLS and increases by education highest number of respondents had
completed Bachelor in Nursing and had highest number of awareness in this group. Relationship
between level of competence and awareness outcome was evaluated Pearson’s R value -0.5 and
P<0.6 which reveals the weak relationship between them.
Table 13: Cross Tabulation of Economic Status and Outcome of Awareness
Economic * Awareness Crosstabulation
Awareness Total
Aware Unware
Economic Affordable to ACLS 4(6.06) 40(60.60) 44(66.67)

27
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
Unaffordable to ACLS 3(4.54) 19(28.78) 22(33.33)
Total 7(10.60) 59(89.40) 66(100) *Paracentesis contains Percentage
Among the respondents who were affordable to ACLS 6.06% were aware and 4.54% were aware
for unaffordable. Table 13
Table 14Work Experience and Outcome Cross Tabulation
Work Experience * Outcome Crosstabulation
Outcome Total
Aware Unaware
Work
Experience
Less than 1 year 0(0) 7(10.60) 7(10.60)
1-3 1(1.51) 19(28.78) 20(30.30)
4-10 4(6.06) 22(33.33) 26(39.39)
Above 10 Years 2(3.03) 11(16.67) 13(19.69)
Total 7(10.60) 59(89.40) 66(100) *Paracentesis contains Percentage
Table 14 presents respondents with 4-10 years of work experience were more aware compared to
less experienced. Work experience less than 1 year all unware. It has weak relationship between
work experience and outcome of awareness where p<0.2 and coefficient value is 0.5.
Table 15 ACLS Training and Outcome Cross Tabulation
ACLS Training * Outcome Crosstabulation
Outcome Total
Aware Unaware
ACLS Training Yes 2(3.03) 27(40.90) 29(43.93)
No 5(7.57) 32(48.48) 37(56.06)
Total 7(10.60) 59(89.40) 66(100) *Paracentesis contains Percentage

28
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
The respondents with ACLS training 3.03% were aware and without training 7.57% were aware
of ACLS.ACLS training taken and awareness outcome for ACLS was calculated relation between
them shows p<0.2 and coefficient value is 0.5 which is week relationship in this study. Table 15
Logistic regression was calculated to show the relationship between gap of ACLS training has
been received and outcome of awareness of ACLS. It shows poor relationship between participants
received training before 3months, 6 month, 1 year, 2 years and more than 2 years and awareness
outcome with p<0.9, p<0.9, p<0.9, p<0.7, p<0.9 respectively.
Table 16 Clinical Competence and Outcome of Awareness Cross Tabulation
Outcome of Awareness * Clinical Competence Crosstabulation
Clinical Competence Total
Level I Level II Level IV Level V:
Aware 0 2(3.03) 4(6.06) 1(1.51) 7(10.60)
Unaware 6(9.09) 21(31.81) 18(27.27) 14(21.21) 59(89.40)
Total 6(9.09) 23(34.84) 22(33.33) 15(22.72) 66(100)
Table 16 shows the relationship between level of clinical competence and outcome of awareness.
None of them were aware from level one. In level II 3.03% were aware in Level IV and level V
6.06% and 1.51% respectively reveals awareness of ACLS. Contingency coefficient shows
insignificant relationship between clinical competence and awareness p<0.4.
Clinical Competence of all the levels with health outcome of the patient was calculated
contingency coefficient value was o.62 and p<0.00. This finding shows no relation between them.
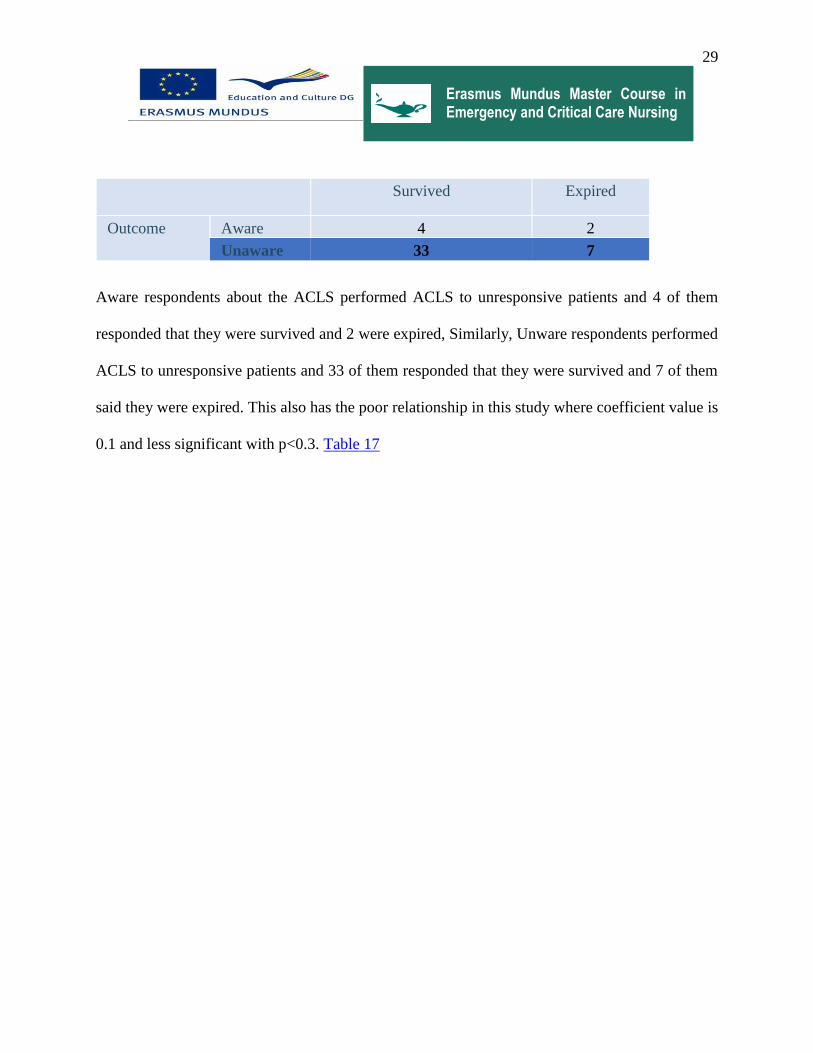
Table 17 Outcome of Awareness and Patient's Condition Cross Tabulation
Outcome * Patient’s Condition Crosstabulation
Patient’s Condition
29
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
Survived Expired
Outcome Aware 4 2
Unaware 33 7
Aware respondents about the ACLS performed ACLS to unresponsive patients and 4 of them
responded that they were survived and 2 were expired, Similarly, Unware respondents performed
ACLS to unresponsive patients and 33 of them responded that they were survived and 7 of them
said they were expired. This also has the poor relationship in this study where coefficient value is
0.1 and less significant with p<0.3. Table 17
30
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
5. DISCUSSION
The primary outcome measure in this study was awareness of ACLS among the nurses working in
critical care areas in Nepal and Portugal. This study found low level of awareness in ACLS, with
mean score12.92{43.06%} (SD±7.812). Though, different measures of ACLS were used in similar
studies, the mean score of respondents in the current study was marginally higher compared to
41.6% in North- Kerala(Nambiar, 2016). A greater than 50% score was achieved by 34.84% of
the participants of the study which was less compared to 48.2% in North- Kerala (Nambiar, 2016).
It should be noted that 10.60% of participants in this surpassed the >80% standard set by AHA.
AHA guidelines require that students should achieve 84% or higher for successful course
completion and pass the written test of ACLS(AHA, 2016). This study shows better score
compared to 4.3% in North-Kerala(Nambiar, 2016) and study results shown by Sinha Akritia and
others where 1% respondent responded >80% and similar study results were shown by Shanta
Chandrasekaran et al where none of the participants scored above 85% while 85% of participants
scored less than 50%(Chandrasekaran S, 2010) . One study in China also shows that none of the
scored above 80% only the score ranges averagely 20.12 ± 4.13 out of 40 questions were correct,
ranging from 6 to 31 and which contributed to the total average accuracy rate of 50.31% (Xi,
2015). This study was conceptualized by adopting the P. Benner’s Novice to Expert theory. This
awareness of ACLS for nurses is influenced by various factors such as age and sex, environment,
and level of competence.
This study results shows that are no statistically significant findings in terms of Nurses’ age, sex,
work experience, ACLS training, gap of training, clinical competence and working area with

31
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
awareness of ACLS among nurses. This study has adopted Patricia Benner’s Novice to expert
theory to categories the level of clinical competence. There was no significant association found
between different clinical competence Level I, Level II, Level III, Level IV and Level V (p= 0.00),
demographic variables, patient outcomes, and with the awareness of ACLS. Nambiar showed
mean scores decreased with age. (Nambiar, 2016) Logistic regression shows insignificant relation
between age and sex with awareness p<0.2 and p<0.9 respectively. The study conducted in South-
Africa(Ehlers, 2014) had similar findings, although a study conducted in Belgium demonstrated
that accumulated work experience was associated with improved awareness and skills
(Verplancke, 2008) whereas, this study has poor relationship between work experience and
outcome of awareness where p<0.2 and coefficient value is 0.5
This study shows 43.93% of the participants had undergone formal training for ACLS. HN Harsha
Kumar et al have also shown poor level of training among the under graduate medical students(HN
Harsha Kumar, 2013).Low levels of training have been reported from Pakistan and the UK (Zaheer
H, 2009). Only 3.6% was shown in New Delhi (Akritia, 2014).
Statistically significant correlation was not seen (p=0.9) between the training of ACLS of the
participants and the awareness. Sinha Akriti showed significant correlation between formal
training and awareness (Akritia, 2014) and Other studies have also concluded that the knowledge
of trained personnel was better than those of untrained ones(Abbas A, 2011). This result may be
because of most of the other studies compared knowledge and awareness gain by a pre-training
and an immediate post-training questionnaire this study studies the existing awareness. Though it

32
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
not significant statistically, the mean score was low for trained participants compared to untrained
participants.
Study in Brazil demonstrates that the professional level of educational background influence the
rate of right answer(Lima, 2009).This study shows no statistical significant between the
educational background (p=0.06) ,ACLS performed (p=0.2) and ACLS training taken 3 months
ago (p=0.9), 6 months ago(p=0.9), 1 year ago(p=0.9), 2 years ago(p=0.7) and more than 2
years(p=0.9) and awareness.
Contingency coefficient shows insignificant relationship between clinical competence and
awareness p<0.4 and clinical competence of all the levels with health outcome of the patient was
calculated contingency coefficient value was o.62 and p<0.00. This finding shows no relation
between them. ACLS provided by ACLS- trained or non-trained participants, the survival rate
was two-fold higher when the participant assisting the patient was ACLS trained, and this variable
was considered as independent predictor in the logistic regression analysis. Similar study in
Georgia, United States reveled that survival rate was four-fold higher when the nurses assisting
the patient was ACLS trained(Dane FC, 2000).
6. CONCLUSION
This study highlights the level of awareness regarding the ACLS among the student nurses and
Professional nurses is poor. The study participants were from two different countries Nepal and
Portugal. Both male and female nurses were the study participants. Educational status of the
participants was ongoing certificate level, completed certificate level, ongoing bachelor level,
completed bachelor level, ongoing masters level of nursing and nurses with specialized course and

33
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
training were involved in the study. Clinical competence of the nurses were categories based on P.
Benner Novice to Expert Theory. Only 10.06% of the respondents were aware of ACLS. This
study shows insignificant relationship with the nurses age and sex and awareness of ACLS on
nurses. Similarly, it is also shows insignificant relationship with nurse’s economic condition,
education, training, work experience, and frequency of working with unresponsive patients. There
is no association between environment and patient health outcome. This study shows level of
clinical competencies Novice to Expert have insignificant relationship with health outcomes and
awareness of ACLS among nurses. This issue needs to be addressed promptly. To ensure better
and safer health-care, it is essential for all graduating nurses as well as professional nurses to be
well versed with ACLS. These findings show insignificant results this might be due to small sample
size for the study.
7. RECOMMENDATION
Nursing in acute-care settings has grown so complex that it is no longer possible to standardize,
routinize, and delegate much of what the nurse does. Poor awareness makes more challenging for
the nurses working in critical care settings. Therefore, graduating nurses should be well trained
before starting the job and professional nurses should be updated with the new updates of ACLS.
This study purpose recommendation to:
Clinical:
1. ACLS training should be provided to the nurses working in the critical care settings.
2. It is recommended that the courses should be not only included but also regular refreshing
courses are necessary with hands on experience.
Education

34
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
1.ACLS courses should be incorporated into the nursing curriculum.
Research
1. A large -scale study can be carried out to generalized the findings.
2. Further study is recommended by observing skill together with the awareness.
Management
1. Certification Program should be initiated from related higher authorities.
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
REFERENCES
A Villamor, A. Y. (2014). Emergency room advanced life support after cardiac arrest: outcomes
and survival, nursing care and team response. Criticla Care , 485 .
Aari, R. R.-C.-K. (2004). Biological and physiological knowledge and skills of graduating Finnish
nursing students to practice in intensive care. Nurse Education Today, 24(4), 293-300 8p.
Abbas A, B. S. (2011). Knowledge of first aid and basic life support amongst medical students:a
comparison between trained and untrained students. . JPMA, 80-82.
Abella BS, S. N. (2005). Cheat compression rates during cardiopulmonary Resusciation are
suboptimal: a prospective study during in-hospital cardiac Circulation. Circulation,
111(4):428.
Akritia, S. (2014). Basic Life Support and Advanced Cardiac Life Support. Journal of Young
Medical Researchers, 2-9.
Auble TE, M. J. (1995). Effect of out-of- hospital defibrillation by basic life support provider on
cardiac arrest moratlity: a meta-analysis. Ann Emerg Med, 25: 642-658.
B. Prasanatikom. (2010). Knowledge & skill retention after the advanced cardiac life support
workshop—A study in nursing in nursing practitioners at the Udonthani, Thailand.
European Resussciatation Council, 93.
Benner, P. (2012). Novice to Expert. 402-407.
Berden HJ, B. J. (1994). Resuscitation skills of lay public after recent training. Ann Emerg Med.,
1003–1008.
ii
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
Bruce SA, S. Y. (2009). A COLLABORATIVE EXERCISE: Between Graduate and
Undergraduate Nursing Students Using a COMPUTER-ASSISTED SIMULATOR in a
Mock Cardiac Arrest. Nurs Educ Perspect, 30 (1): 22-27.
Centre, R. (2015, 11 28). CAR NET. Retrieved from KNOWLEDGE ASSESSMENT
(EVALUATION) THEORY.
Chandrasekaran S, K. S. (2010). Awareness of BLS and ALS among Nurses. Indian J Anaesthesia,
121-126.
Christina Passaliemail, I. D. (2011). Evaluation of nurses’ and doctors’ knowledge of basic &
advanced life support resuscitation guidelines. Nurse Education in Practice, 365–369.
Dane FC, R.-L. K. (2000). In-hospital resuscitation: association between ACLS training and
survival to discharge. Resuscitation, 83-7.
Davidson Ocen, S. K. (2015). Prevalence, outcomes and factors associated with adult in hospital
cardiac arrests in a low-income country tertiary hospital: a prospective observational study.
BMC Emergency Medicine, 1-6.
Denise F. Polit, C. T. (2004). Nursing Research principles and Methods. USA: Lippincott
Williams & Wilkins.
Efendijev, I. R. (2014). Temporal trends in cardiac arrest incidence and outcome in Finnish
intensive care units from 2003 to 2013. Intensive Care Medicine, 1853-1861 9p.
Ehlers, V. &. (2014). ‘Cardiopulmonary resuscitation knowledge and skills of registered nurses in
Botswana. Curationis, 1259-1266.
iii
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
Field JM, H. M. (2010 Nov 2;122(18 Suppl 3)). Part 1: executive summary: 2010 American Heart
Association Guidelines for Cardiopulmonary Resuscitation and Emergency
Cardiovascular Care. Circulation, S640-56.
Francis C. Dane, K. S.-L. (2000). In-hospital resuscitation: association between ACLS training
and survival to discharge. Resuscitation., 47: 83-7.
Freddy K. Lippert, V. R. (2010). European Resuscitation Council Guidelines for Resuscitation
2010 Section 10. The ethics of resuscitation and end-of-life decisions. Journal of European
Resusciatation Council, 1445 - 1451.
H. Gombotz, W. B. (2006). In-hospital cardiac resuscitation outside the ICU by nursing staff
equipped with automated external defibrillators - the first 500 cases. Resuscitation, 70 (3):
416-22. .
Hagyard-Wiebe, T. (2007). Should critical care nurses be ACLS-trained? Dynamics, 18(4), 28-31
4p.
Hagyard-Wiebe, T. (2007). Should critical care nurses be ACLS-trained? Dynamics, 18(4), 28-31
4p.
Hall, A. (2015). Defining nursing knowledge. Nursing Times, 34. Retrieved from Nursing Times.
Hamilton, R. (2013). Nurses' knowledge and skill retention following cardiopulmonary
resuscitation training: a review of the literature. Journal of Advanced Nursing,, 51 (3)
(2005), pp. 288–297.
iv
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
HN Harsha Kumar, P. S. (2013). A cross-sectional study on awareness and perception about basic
life support/cardio-pulmonary resuscitation coastal South India. Int J Med Pub Health,
146-150.
Isenberg DL, B. R. (2005). Does advanced life support provide benefits to patients?: A literature
review. Prehosp Disaster Med., 265-70.
James Buchan, M. T. (2013). Nurses in advanced roles: a review of acceptability in Portugal. Rev.
Latino-Am. Enfermagem, 38-46.
Jasmeet Soar, J. P. (2015). European Resuscitation Council Guidelines for Resuscitation 2015
Section 3. Adult advanced life support. Resuscitation, 100–147.
Lima, S. G. (2009). Permanent Education in BLS and ACLS: impact on the knowledge of nursing
professionals. Arquivos Brasileiros de Cardiologia, 630-636.
MA, M. (2001). Eficácia do treinamento em suporte avançado de vida nos resultados das manobras
de ressuscitação cardiopulmonar. São Paulo, 130p.
MINISTRY FOR FOREIGN AFFAIRS OF FINLAND. (2014). Country Strategy for Development
Cooperation with Nepal 2013 -2016. Kathmandu: MINISTRY FOR FOREIGN AFFAIRS
OF FINLAND.
Ministry of Health and Population Nepal, Partnership for Maternal, Newborn & Child Health,
WHO, World Bank and Alliance for Health Policy and Systems Research. (2014). Success Factors
for Women’s and Children’s Health : Nepal. Geneva: World Health Organisation.

v
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
Model A. c. (2011, September 16). Nursing Theories. Retrieved from From Novice to Expert
Patricia E. Benner:
http://currentnursing.com/nursing_theory/Patricia_Benner_From_Novice_to_Expert.html
Nambiar, M. N. (2016). Is current training in basic and advanced cardiac life support (BLS &
ACLS) effective? World Journal of Emergency Medicine, 263–269.
Practice Resource Network. (2008). Should ACLS training be mandatory for critical care and
progressive care nurses? AACN News 25, no. 3: 3-3 1p. Retrieved from AACN News 25.
Sissel I Eikeland Husebø, C. A. (2012). A comparative study of defibrillation and cardiopulmonary
resuscitation performance during simulated cardiac arrest in nursing student teams.
Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine, 20:23.
Stiell IG, B. S. (2012). What is the role of chest compression depth during out-of-hospital cardiac
arrest resuscitation? . Critical Care Medicine, 40:1192–1198.
Subedi, D. R. (2014). Growth of nursing education sector and its effects on professionalization of
nurses in Nepal. IOSR-JNHS, 34-39.
Verplancke, T. P. (2008). ‘Determinants of the quality of basic life support by hospital nurses’,.
Resuscitation, 75-80.
Wikipedia . (2016, December 16). Demographics of Portugal. Retrieved from
https://en.wikipedia.org/wiki/Demographics_of_Portugal
Zaheer H, H. Z. (2009). Awareness about BLS (CPR) among medical students: status and
requirements. J Pak Med Assoc., 57-59.
vi
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
ANNEX I
vii
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
ANNEX II
Circle an appropriate answer given in the right column.
PART ONE
Demographic Information
1. Age
2. Gender: 1. Male
2. Female
3. Education 1. Ongoing Certificate Level of Nursing
2. Completed Certificate Level of Nursing
3. Ongoing Bachelor Level of Nursing
4. Completed Bachelor Level of Nursing
5. Specialized course taken (please specify the
area)
4. Economic Condition 1. Affordable for ACLS Training
2. Unaffordable for ACLS Training
5. Work Area (only for working Nurses)
6. Work Experience (only for working
Nurses):
In Months
7. Level of clinical competence Level I :1st year of clinical education (nursing
student)
Level II: newly joined job gaining prior experience in
actual situations

viii
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
Level III: on the job for 2 to 3 years and able to
develop actions in terms of long-range goals or plans
Level IV: 3-5 years’ experiences
Level V: expert
8. Had you taken the formal ACLS
Training
1. Yes
2. No
9. If yes , when did you take
1. 3 months ago
2. 6 months ago
3. 1 year ago
4. 2 years ago
5. More than 2 years
10. Had you ever performed ACLS
interventions patient with cardiac
arrest?
1. Yes
2. No
11. If yes, how often?
12. If performed after the intervention
condition of patient
Patient
1. Survived
2. Died

ix
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
PART TWO
Awareness Based Questions
There are three sections: Rhythm Identification, Pharmacology and Application. Take the Rhythm
Identification and Pharmacology and test awareness of their application based on ACLS core
material and algorithms.
Rhythm Identification: This will test the ability to identify the rhythms in the core ALS algorithms
and cases.
1. Please identify the rhythm by selecting the best single answer.
a. Agonal rhythm/asystole
b. Atrial fibrillation
c. Atrial flutter
d. Coarse Ventricular fibrillation
e. Fine ventricular fibrillation
f. Monomorphic ventricular tachycardia
g. Normal sinus rhythm
h. Polymorphic ventricular tachycardia
i. Pulseless electrical activity
j. Reentry supraventricular tachycardia
k. Second-degree AV block ( Mobitz I Wenckebach)
l. Second-degree AV block ( Mobitz II block)
m. Sinus bradycardia
n. Sinus tachycardia
o. Third-degree AV block
2. Please identify the rhythm by selecting the best single answer.

x
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
a. Agonal rhythm/asystole
b. Atrial fibrillation
c. Atrial flutter
d. Coarse Ventricular fibrillation
e. Fine ventricular fibrillation
f. Monomorphic ventricular tachycardia
g. Normal sinus rhythm
h. Polymorphic ventricular tachycardia
i. Pulseless electrical activity
j. Reentry supraventricular tachycardia
k. Second-degree AV block (Mobitz I Wenckebach)
l. Second-degree AV block (Mobitz II block)
m. Sinus bradycardia
n. Sinus tachycardia
o. Third-degree AV block
3. Please identify the rhythm by selecting the best answer.
a. Agonal rhythm/asystole
b. Atrial fibrillation
c. Atrial flutter
d. Coarse Ventricular fibrillation
e. Fine ventricular fibrillation
f. Monomorphic ventricular tachycardia
g. Normal sinus rhythm
h. Polymorphic ventricular tachycardia
i. Pulseless electrical activity
j. Reentry supraventricular tachycardia
k. Second-degree AV block (Mobitz I Wenckebach)
l. Second-degree AV block (Mobitz II block)
m. Sinus bradycardia
n. Sinus tachycardia
o. Third-degree AV block
4. Please identify the rhythm by selecting the best single answer.

xi
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
a. Agonal rhythm/asystole
b. Atrial fibrillation
c. Atrial flutter
d. Coarse Ventricular fibrillation
e. Fine ventricular fibrillation
f. Monomorphic ventricular tachycardia
g. Normal sinus rhythm
h. Polymorphic ventricular tachycardia
i. Pulseless electrical activity
j. Reentry supraventricular tachycardia
k. Second-degree AV block ( Mobitz I Wenckebach)
l. Second-degree AV block ( Mobitz II block)
m. Sinus bradycardia
n. Sinus tachycardia
o. Third-degree AV block
5. There is no pulse with this rhythm. Please identify the rhythms by selecting the best single
answer.
a. Agonal rhythm/asystole
b. Atrial fibrillation
c. Atrial flutter
d. Coarse Ventricular fibrillation
e. Fine ventricular fibrillation
f. Monomorphic ventricular tachycardia
g. Normal sinus rhythm
h. Polymorphic ventricular tachycardia

xii
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
i. Pulseless electrical activity
j. Reentry supraventricular tachycardia
k. Second-degree AV block ( Mobitz I Wenckebach)
l. Second-degree AV block ( Mobitz II block)
m. Sinus bradycardia
n. Sinus tachycardia
o. Third-degree AV block
6. Please identify the rhythms by selecting the best single answer.
a. Agonal rhythm/asystole
b. Atrial fibrillation
c. Atrial flutter
d. Coarse Ventricular fibrillation
e. Fine ventricular fibrillation
f. Monomorphic ventricular tachycardia
g. Normal sinus rhythm
h. Polymorphic ventricular tachycardia
i. Pulseless electrical activity
j. Reentry supraventricular tachycardia
k. Second-degree AV block (Mobitz I Wenckebach)
l. Second-degree AV block (Mobitz II block)
m. Sinus bradycardia
n. Sinus tachycardia
o. Third-degree AV block
7. Please identify the rhythm by selecting the best single answer.
a. Agonal rhythm/asystole
b. Atrial fibrillation

xiii
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
c. Atrial flutter
d. Coarse Ventricular fibrillation
e. Fine ventricular fibrillation
f. Monomorphic ventricular tachycardia
g. Normal sinus rhythm
h. Polymorphic ventricular tachycardia
i. Pulseless electrical activity
j. Reentry supraventricular tachycardia
k. Second-degree AV block (Mobitz I Wenckebach)
l. Second-degree AV block (Mobitz II block)
m. Sinus bradycardia
n. Sinus tachycardia
o. Third-degree AV block
8. Please identify the rhythm by selecting the best single answer.
a. Agonal rhythm/asystole
b. Atrial fibrillation
c. Atrial flutter
d. Coarse Ventricular fibrillation
e. Fine ventricular fibrillation
f. Monomorphic ventricular tachycardia
g. Normal sinus rhythm
h. Polymorphic ventricular tachycardia
i. Pulseless electrical activity
j. Reentry supraventricular tachycardia
k. Second-degree AV block ( Mobitz I Wenckebach)
l. Second-degree AV block ( Mobitz II block)
m. Sinus bradycardia
n. Sinus tachycardia
o. Third-degree AV block
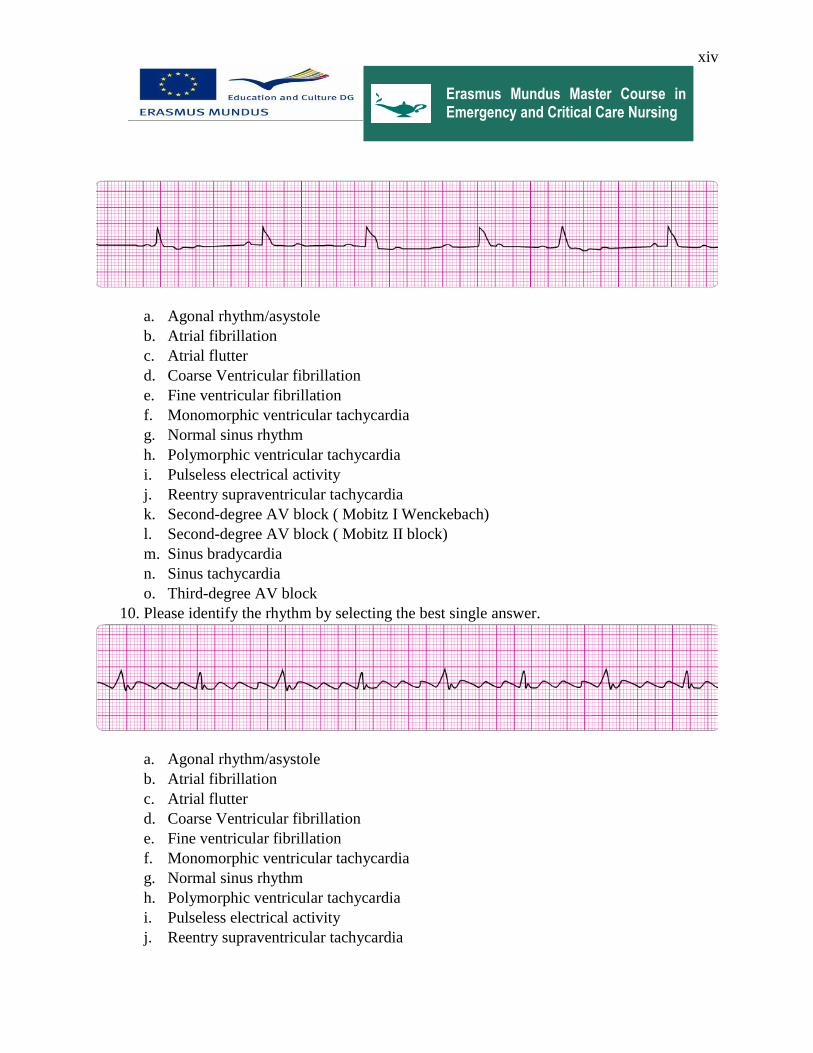
9. Please identify the rhythm by selecting the best single answer.
xiv
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
a. Agonal rhythm/asystole
b. Atrial fibrillation
c. Atrial flutter
d. Coarse Ventricular fibrillation
e. Fine ventricular fibrillation
f. Monomorphic ventricular tachycardia
g. Normal sinus rhythm
h. Polymorphic ventricular tachycardia
i. Pulseless electrical activity
j. Reentry supraventricular tachycardia
k. Second-degree AV block ( Mobitz I Wenckebach)
l. Second-degree AV block ( Mobitz II block)
m. Sinus bradycardia
n. Sinus tachycardia
o. Third-degree AV block
10. Please identify the rhythm by selecting the best single answer.
a. Agonal rhythm/asystole
b. Atrial fibrillation
c. Atrial flutter
d. Coarse Ventricular fibrillation
e. Fine ventricular fibrillation
f. Monomorphic ventricular tachycardia
g. Normal sinus rhythm
h. Polymorphic ventricular tachycardia
i. Pulseless electrical activity
j. Reentry supraventricular tachycardia

xv
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
k. Second-degree AV block ( Mobitz I Wenckebach)
l. Second-degree AV block (Mobitz II block)
m. Sinus bradycardia
n. Sinus tachycardia
o. Third-degree AV block
Pharmacology: This section will help to identify your knowledge of ACLS core drugs used.
1. A 57- year-old woman has palpitations, chest discomfort, and tachycardia. The
monitor shows a regular wide- complex QRS at a rate of 180/min. She becomes
diaphoretic, and her blood pressure is 80/60 mm Hg. The next action is to
a. Give amiodarone 300 mg IV push
b. Establish IV access
c. Obtain a 12-lead ECG
d. Perform immediate electrical cardioversion
2. A patient has a rapid irregular wide-complex tachycardia. The ventricular rate is
138/min. He is asymptomatic, with a blood pressure of 100/70 mm Hg. He has a
history of angina. Which of the following actions is recommended?
a. Immediate synchronized cardioversion
b. Giving lidocaine 1 to 1.5 mg IV bolus
c. Seeking expert consultation
d. Giving adenosine 6 mg IV bolus
3. Bradycardia require treatment when
a. The blood pressure is less than 100 mm Hg systolic with or without symptoms.
b. The patient’s 12-lead ECG shows an MI
c. Chest pain or shortness of breath is present
d. The heart rate is less than 60/min with or without symptoms
4. A patient with ST-segment elevation MI has ongoing chest discomfort. Fibrinolytic
therapy has been ordered. Heparin 4000 units IV bolus was administered. Aspirin
was not taken by the patient because he had a history of gastritis treated 5 years
ago. You next action is to
a. Give aspirin 160 to 325 mg chewed immediately.
b. Give 75 mg enteric-coated aspirin orally.
c. Give 325 mg enteric-coated aspiration rectally.
d. Substitute clopidogrel 300 mg loading dose.
5. A patient is in cardiac arrest. Ventricular fibrillation has been refractory to an initial
shock. What is the recommended route for drug administration during CPR?
a. Femoral

xvi
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
b. Endotracheal
c. External Jugular vein
d. Central line
e. IV or IO
6. You arrive on the scene with the code team. High – quality CPR is in progress. An
AED has previously advised “no shock indicated”. A rhythm check now finds
asystole. After resuming high- quality compressions, your next action is to
a. Place an esophageal- tracheal tube or laryngeal mask airway
b. Gain IV or IO access
c. Attempt endotracheal intubation with minimal interruptions in CPR
d. Call for a pulse check
7. A patient with a possible acute coronary syndrome has ongoing chest discomfort
unresponsive to 3 sublingual nitroglycerin tablets. There are no contraindication,
and 4 mg of morphine sulfate was administered. Shortly afterward, blood pressure
falls to 88/60 mm Hg, and the patient has increased chest discomfort. You should
a. Give an additional 2 mg of morphine sulfate
b. Give normal saline 250 ml to 500 ml fluid bolus
c. Start dopamine at 2mcg/kg per minute and titrate to a systolic blood pressure
reading of 100 mm Hg
d. Give sublingual nitroglycerin 0.4 mg.
8. A patient is in cardiac arrest. Ventricular fibrillation has been refractory to a second
shock. Of the following, which drug and dose should be administered first by the
IV/IO route?
a. Atropine 1 mg
b. Epinephrine 1 mg
c. Sodium bicarbonate 50 mEq
d. Vasopressin 20 units
9. A patient with sinus bradycardia and a heart rate of 42/min has diaphoresis and a
blood pressure of 80/60 mm Hg. What is the initial dose of atropine?
a. 0.5mg
b. 3mg
c. 1mg
d. 0.1md
10. A patient is in pulseless ventricular tachycardia. Two shocks and 1 dose of
epinephrine have been given. Which is the next drug/dose to anticipate to
administer?
a. Amiodarone 150 mg
b. Epinephrine 3mg
c. Amiodarone 300mg

xvii
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
d. Lidocaine 0.5 mg/kg
e. Vasopressin 40 units
Practical Application
This section will be able to identify a rhythm and then select a treatment or intervention on the
basis of your identification of the rhythm and your knowledge of ACLS drug and treatment
algorithms.
It will help to identify the rhythm and select a treatment or intervention on the basis of your
identification of rhythm and your knowledge of ACLS drugs and treatment algorithms.
1. A patient becomes unresponsive. You are uncertain if a pulse is present with the given
below rhythm. What is your next action?
a. Begin CPR, starting with high-quality chest compressions.
b. Consider causes of pulseless electrical activity.
c. Order transcutaneous pacing.
d. Start an IV and give epinephrine 1 mg IV
e. Start an IV and give atropine 1 mg.
2. You are monitoring a patient. He suddenly has the below rhythm. You ask about symptoms,
and he reports that he has mild palpitations, but otherwise he is clinically stable with
unchanged vital sign. What is your next actions?
a. Give sedation and perform synchronized cardioversion.
b. Give an immediate unsynchronized shock
c. Administer adenosine 6 mg; seek expert consultation.

xviii
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
d. Give an immediate synchronized shock
e. Administer magnesium sulfate 1 to 2 g IV diluted in 10 ml D5W over 5 to 20 minutes.
3. A patient in the emergency department develops recurrent chest discomfort ( 8/10)
suspicious for ischemia. His monitored rhythms becomes irregular as seen above . Oxygen
is being administered by nasal cannula at 4L/min, and an IV line is in place. Blood pressure
is 160/96 mm Hg. There are no allergies or contraindications to any medication. You would
first order
a. IV nitroglycerin initiated at 10 mcg/min and titrated to patient response
b. Amiodarone 150 mg IV
c. Sublingual nitroglycerine 0.4 mg
d. Lidocaine 1 mg/kg IV infusion 2 mg/min
e. Morphine sulfate 2 to 4 mg IV
4. A patient was in refractory ventricular fibrillation. The third shock has just been
administered. Your team looks to you for instructions. You immediate next order are
a. Give atropine 1 mg IV.
b. Give amiodarone 300 mg IV.
c. Resume high-quality chest compressions.
d. Check the carotid pulse.
e. Perform endotracheal intubation.
5. The patient has been resuscitated from cardiac arrest. During the resuscitation, amiodarone
300 mg was administered. The patient developed severe chest discomfort with diaphoresis,
He is now unresponsive. What is the next indicated action?

xix
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
a. Perform immediate synchronized cardioversion.
b. Give lidocaine 1 to 1.5 mg/kg IV.
c. Repeat amiodarone 150 mg IV.
d. Give an immediate unsynchronized high-energy shock (defibrillation dose).
e. Repeat amiodarone 300mg IV.
6. You are monitoring the patient and note the above rhythm on the cardiac monitor. She has
dizziness, and her blood pressure is 80/40 mm Hg. She has an IV in place. What is your
next action?
a. Administer sedation and begin immediate transcutaneous pacing at 80/min
b. Give atropine 0.5 mg IV.
c. Start dopamine at 2 to 10 mcg/kg per minute and titrate to patient response.
d. Give atropine 1 mg IV
e. Start transcutaneous pacing
7. The patient suddenly becomes unconscious and has a weak carotid pulse. Cardiac
monitoring, supplementary oxygen, and IV have been initiated. The code cart with all the
drugs and a transcutaneous pacer are immediately available. Next you would
a. Give atropine 0.5 mg IV.
b. Initiate epinephrine at 2 to 10 mcg/kg per minute
c. Initiate dopamine at 10 20 mcg/kg per minute and to patient response
d. Begin transcutaneous pacing

xx
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
e. Initiate dopamine at 2 to 10 mcg/kg minute and titrate to patient response.
8. A 35 years –old woman presents to the emergency department with the chief complaint of
palpitation. She has no chest discomfort, shortness of breath. Or light-headedness. Which
of the following is indicated first?
a. Perform vagal maneuvers.
b. Give adenosine 3 mg IV bolus.
c. Give adenosine 12 mg IV slow push (over 1 to 2 minutes).
d. Give metoprolol 5 mg IV and repeat if necessary.
9. You are monitoring a patient with chest discomfort who suddenly becomes unresponsive.
You observe the following rhythms on the monitor. A defibrillator is present. What is your
first action?
a. Establish an IV and give vasopressin 40 units.
b. Establish an IV and give epinephrine 1 mg.
c. Intubate the patient and give epinephrine 2 to 4 mg via the endotracheal tube.
d. Give a single shock.
e. Begin CPR with chest compression for 2 minutes or about 5 cycles of compressions and
ventilations.
10. You arrive on the scene to find a 56 years old diabetic woman with dizziness. She is pale
and diaphoretic. Her blood pressure is 80/60 mm Hg. The cardiac monitor documents the
rhythm above. She is receiving oxygen at 4 L/min by nasal cannula, and an IV has been
established. Your next order is
xxi
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
a. Atropine 1 mg IV
b. Sublingual nitroglycerine 0.4 mg
c. Dopamine at 2 to 10 mcg/kg per minute
d. Morphine sulfate 4 mg IV
e. Atropine 0.5 mg IV.
Thank You for Participation!!
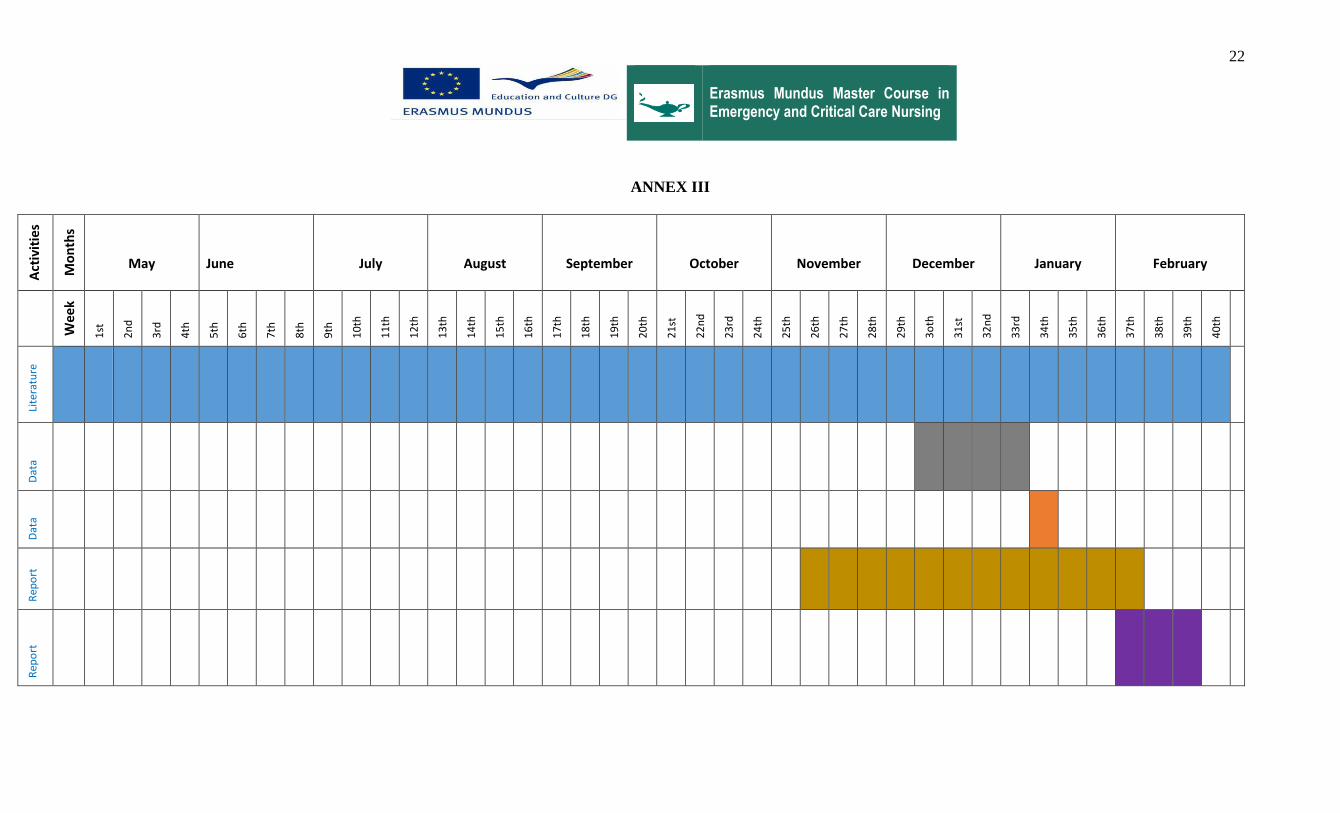
22
Erasmus Mundus Master Course in Emergency and Critical Care Nursing
ANNEX III
Act
ivit
ies
Mo
nth
s
May June July August September October November December January February
Wee
k
s 1
st
2n
d
3rd
4th
5th
6th
7th
8th
9th
10
th
11
th
12
th
13
th
14
th
15
th
16
th
17
th
18
th
19
th
20
th
21
st
22
nd
23
rd
24
th
25
th
26
th
27
th
28
th
29
th
3o
th
31
st
32
nd
33
rd
34
th
35
th
36
th
37
th
38
th
39
th
40
th
Lit
erat
ure
Rev
iew
Dat
a
Co
llect
ion
Dat
a
An
alys
is
Rep
ort
Wri
tin
g
Rep
ort
Pre
sen
tati
o
n