epma: what works?
TRANSCRIPT


EPMA: WHAT
WORKS? Peter J Murphy
Consultant In Paediatric Anaesthesia
Clinical Lead EPMA UHBristol

CONTENT OF PRESENTATION
Secondary Care Prescribing
Why EPMA (current views)?
Medication errors
Prescribing Process (how and where EPMA works)
Evidence Base for EPMA
Why EPMA (the vision)?

WHY EPMA? (A). SAFETY

WHY EPMA (B).COST
Medication errors cost
the NHS up to £2.5bn a
year

“Primum non nocere”
Safety/Quality Agenda/commissioning (Never Events..including new expanded list)
Patient expectations/medico-legal
Staff expectations (Staff supportive of EPMA)
Potential shortfall in Nursing Numbers (especially senior nurses)
Less experienced junior doctors (WTD)
Secondary Care is becoming much more complex
Financial/resource issues (National and Local)
Population/demographic changes (aging population)


MEDICATION ERRORS

MEDICATION ERRORS IN CLINICAL
PRACTICE
High Incidence of low risk prescription errors (Chart not signed/ prescription illegible/ time of administration not ticked/ drug not available)….”low hanging fruit” which most ePrescribing Systems largely eliminate
Moderate Risk Issues (Missed drugs, significant drug interactions, incorrect doses in renal/hepatic failure etc,)
Low incidence of High Risk errors (administration errors/incorrect prescription and drug still given/wrong route administration/wrong patient/wrong drug/”picking” errors)

High risk
Critical Care
Maternity
Operating
Theatres
Accident and
Emergency
Care of the
Elderly
Mental Health
Paediatrics Oncology
Renal/Hepatology/Transplantation Neonates
High Risk Areas for Medication Errors

EPMA SYSTEM HAS TO BE SEEN TO WORK IN
TERMS OF TOTAL MEDICINES MANAGEMENT
PROCESS IN ORDER TO BE EFFECTIVE
Implementing EPMA should include;
EPMA Systems (esp in high risk areas)
Interface for TTO’s supporting patient discharge
Knowledge Support
Clinical Decision Support
Advanced Decision Support
Intra-operability with Other Clinical Systems (esp order comms/Pathology)
Support for Drug Administration
Networks and Hardware
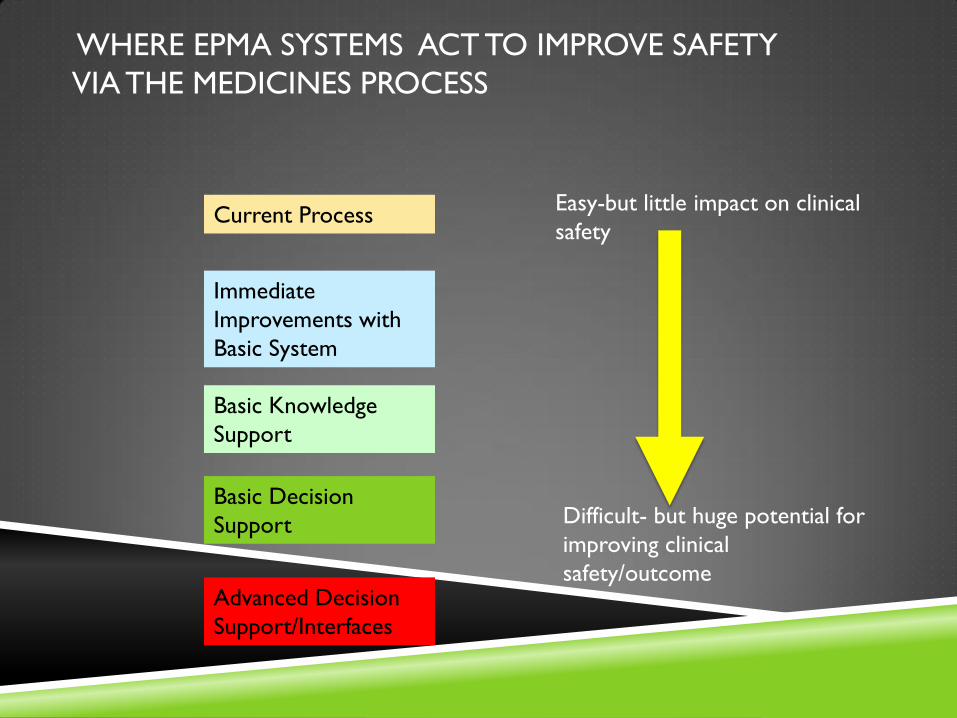
WHERE EPMA SYSTEMS ACT TO IMPROVE SAFETY
VIA THE MEDICINES PROCESS
Current Process
Basic Knowledge
Support
Basic Decision
Support
Advanced Decision
Support/Interfaces
Easy-but little impact on clinical
safety
Difficult- but huge potential for
improving clinical
safety/outcome
Immediate
Improvements with
Basic System

Prescriber
Local Prescribing
Guidelines “on line”
Allows Formulary
Control and Cost Savings
Ensures
Legible/Complete/
Sensible
Prescription plus
Electronic
Signature and
Audit Trail
Prescription
Pharmacist
Intermediate decision
support
i.e. Drug Interactions
First Data Bank
software and updates
Knowledge
support (i.e.
BNF for
Children)
Availability of
locally produced
“Order Sentences
and Order Sets”
Basic Decision
Support
(Allergy Check)
Checks
Intra-operability with other Clinical Systems (Order
Comms) eg Renal Failure/ Meds needing Blood Levels
Calculations, weight
based prescribing and
dosage limits
Support for complex IV’s,
Medical Gases etc.
Integrating
Prescribing With
Care Bundles
Paper Chart
Intra-Operability
with other EPMA
systems (ICU,
Oncology)

Prescription
Checks
Pharmacist
Nurse Drug
Pharmacy
Supplies
Alerts Pharmacy
(Stock Control)
Knowledge Support/Local
Guidelines for preparing
drugs
Picking
Support
(PYXIS) and
Staff
Identification
Barcodes to ensure
correct drug has
been picked
Standardisation for
EPMA allows
standard infusions to
be produced in
pharmacy

EPMA System
highlights
missed/delayed doses
all drugs administered
have to be signed for
Drug Nurse/Doctor
2nd
Checker
Drug
administered to
Patient
“On Line” knowledge
Support for
administering
drugs/preparing
infusions/calculations
Bar-coded wrist
bands ensure
correct patient
Intelligent Infusion Devices
recognise bar-coded
infusions and calculate rate
of infusion/ confirm route of
admin etc.


PRESCRIBING INDICATORS STUDY EDELPHI
(COLLABORATION UHB AND UNIVERSITY OF
EDINBURGH/HARVARD)
Digoxin prescribed at a dose of >125 micrograms daily for a patient with heart failure who is in sinus rhythm (Increased risk of digoxin toxicity)
Thiazide diuretic prescribed for a patient with a history of gout (Increased risk of exacerbating symptoms in pre-existing gout)
Thiazide diuretics prescribed for a patient with eGFR <30mL/min/1.73m2 (Increased risk of side effects)
Amiodarone prescribed for a patient with abnormal thyroid function tests (TFTs) (Increased risk of thyroid disorders)
Beta-adrenoceptor blocking drug prescribed for a patient with serum potassium >5mmol/L (Increased risk of hyperkalaemia)
Non-selective beta-adrenoceptor blocking drug prescribed for a patient with asthma (Increased risk of bronchospasm and acute deterioration)
Aliskiren prescribed concomitantly with ACE inhibitors or angiotensin-II receptor antagonists (Increased risk of serious adverse cardiovascular and renal outcomes)
Aliskiren prescribed for a patient with an eGFR< 30ml/min/1.73m2 (Risk of hyperkalaemia)
Super advanced
decision support



IN SUMMARY
Most UK EPMA systems are very very basic. They significantly reduce medication errors (low hanging fruit) but do not exclude serious errors particularly around drug administration. They are not suitable for many high risk areas (paediatrics). Most systems will not interface with Order Comms/Pathology or indeed other EPMA systems. Therefore these systems are unlikely to show significant improvements in clinical outcomes.
They do give the Trust better control of the Hospital Formulary, and better drug audit capabilities and allow for improvements in drug error investigations.
Deployment of EPMA systems is expensive, and it is hard to see where and when cost savings envisaged by the tech fund are going to arise
SHOW ME THE EVIDENCE THAT
EPMA IMPROVES OUTCOMES
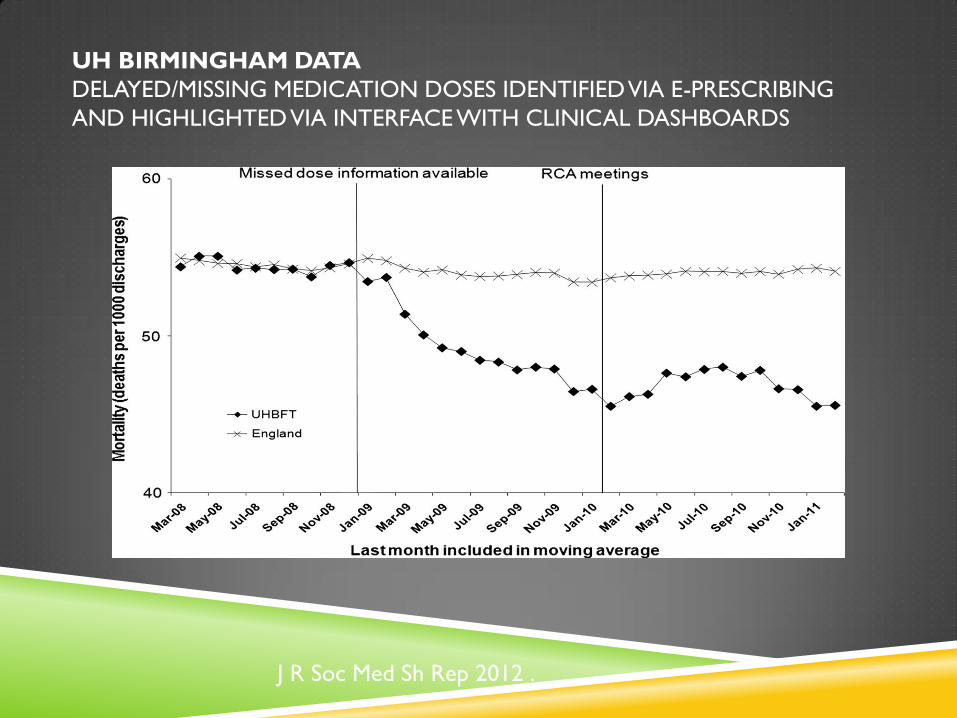
UH BIRMINGHAM DATA
DELAYED/MISSING MEDICATION DOSES IDENTIFIED VIA E-PRESCRIBING
AND HIGHLIGHTED VIA INTERFACE WITH CLINICAL DASHBOARDS
J R Soc Med Sh Rep 2012 .
WHY AM I STILL ENTHUSIASTIC?
EPMA represents the best (only) long term hope of reducing
medication errors in hospitals (aging population/junior staff etc).
We need to get basic EPMA systems in and working before gradually
building advanced EPMA Systems (advanced decision support, links to
other clinical systems and devices) which will significantly reduce errors
and improve clinical outcomes

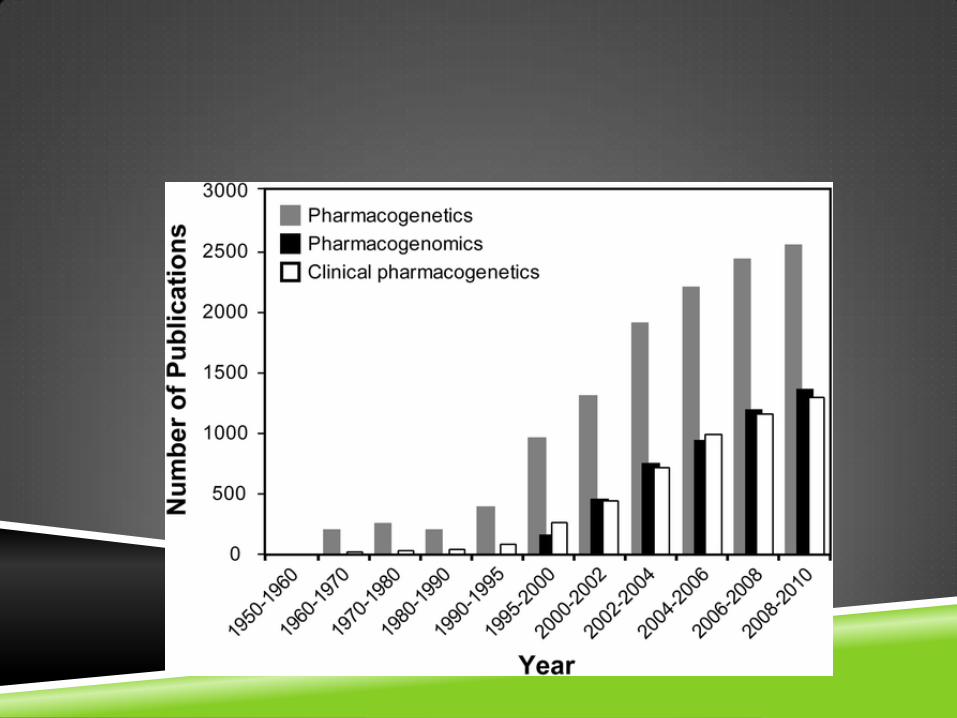
PERSONALISED HEALTH
Pharmacogenetic research holds out the prospect of personalised
medical care in the future….in terms of medication this can only be
achieved with EPMA

PERSONALIZED (PRECISION) MEDICINE
Pharmacogenetics/Pharmacogenomics
the study of inherited genetic differences in drug metabolic pathways which
can affect individual responses to drugs, both in terms of therapeutic effect
as well as adverse effects

Pharmacogenetics and Asthma
Pharmacogenetics and Pain Therapy
Presonalising Treatment Strategies on Oncology Haematology
Personalised Immonosuppression
Pharmacogenetics of Cardiovascular and Diabetic Drugs
Personalised therapy for Metabolic Disorders
Genomics & Pharmacogenomics
September 21-23, 2015 San Antonio, USA

RECENT US NIH GRANTS
St Judes Children’s Research Hospital (July8th 2015) $12Milion
Precision Medicine for the treatment of Leukaemia
eMERGE program (1st Sept 2015) $48million
Linking the EHR to an individuals genome to enable personalised care
Vanderbilt University Phenome Scanning of EHR (1st Sept 2015) $12.8 Million
"Our goal is to understand the fundamental mechanisms putting patients at risk for severe adverse drug reactions and, more broadly, to predict how individual patients will respond to drug therapy,”

AREAS DEVELOPING
PERSONALISED/PRECISION THERAPY
Rheumatology
Oncology
Pain Medicine
HIV Therapy
Metabolic Disease/Diabetes
Treatment of Cardiovascular Disease


CODEINE
Widely used in Paediatric Practice
Codeine is metabolised in the liver by the enzyme CYP2D6 to its active ingredient Morphine
The CYP2D6 isoenzyme is polymorphic, with individuals classified according to one of four levels of activity: poor metabolisers, intermediate metabolisers, extensive metabolisers and ultrarapid metabolisers (URM). Individuals (1.7% Population) with duplication or multiduplication of the CYP2D6 gene are URM’s.
URM’s are more common among some ethnic groups. 29% of North African and Ethiopian populations are URM’s.

Codeine now banned in most
Paediatric Hospitals
Caution in Breast Feeding Mothers

EPMA WILL ENABLE
a scientific approach for individuals affected by adverse drug reactions
individuals to be given the drugs which will work best for them
Individuals to avoid drugs which will have side effects
clinicians to use the best drugs for particular types of disease in
particular individuals
