episode-based reimbursement and supply chain: … · with benchmark data, guidelines, ......
TRANSCRIPT

Episode-Based Reimbursement and Supply Chain: Keys to Success
Winifred S. Hayes, PhD, RN, ANP, CEO & Founder, Hayes, Inc.
Karla Barber, RN, BSN, CVAHP, System Director of Clinical Value Analysis, Centura Health
FACULTY DISCLOSURE
The faculty reported the following financial relationships or relationships to products or devices they or their spouse/life partner have with commercial interests related to the content of this CE activity:
Winifred S. Hayes, PhD, RN, ANP – Ownership Interest: Hayes, Inc.
Karla Barber, RN, BSN, CVAHP – Nothing to disclose

Learning Objectives
• Explore the current role of supply chain and value analysis in episode-based payment models
• Illustrate the utilization of evidence in combination with benchmark data, guidelines, and consensus data in standardizing the health technologies used within bundles
• Explore the implications of bundled payments within the context of population health
• Review a case study

US Healthcare and the Rationale for Value-Based Purchasing
• Population health indicators
• Cost of care
• Cost drivers
• Quality drivers
• Current initiatives to:
–Reduce costs
– Improve population health
– Improve the patient experience References: #14, #12, #11, and #10
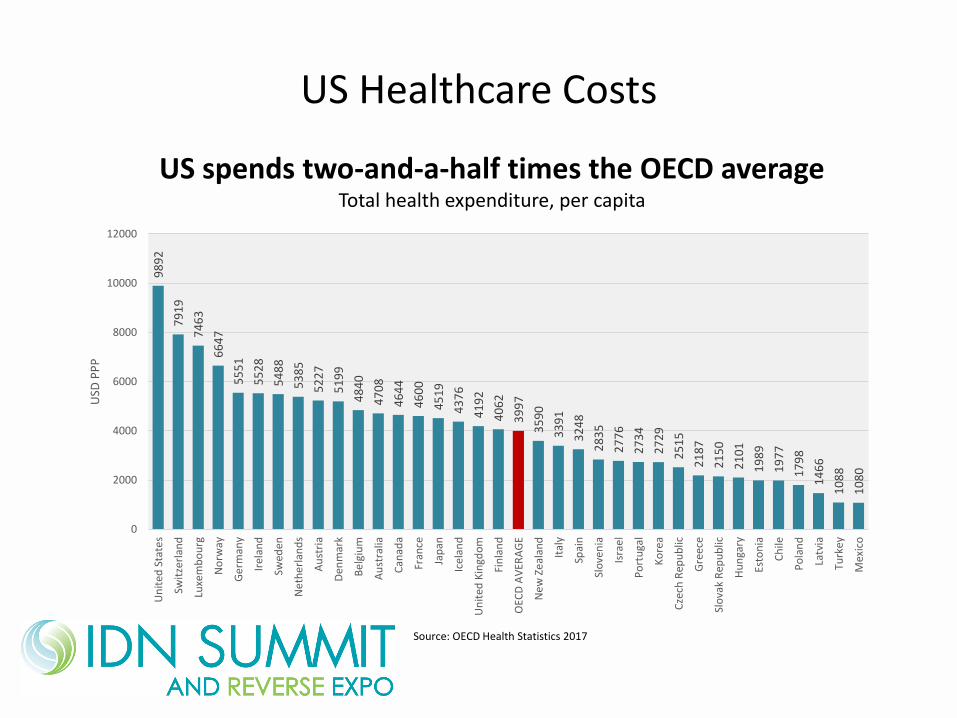
US Healthcare Costs
98
92
79
19
74
63
66
47
55
51
55
28
54
88
53
85
52
27
51
99
48
40
47
08
46
44
46
00
45
19
43
76
41
92
40
62
39
97
35
90
33
91
32
48
28
35
27
76
27
34
27
29
25
15
21
87
21
50
21
01
19
89
19
77
17
98
14
66
10
88
10
80
0
2000
4000
6000
8000
10000
12000
Un
ited
Sta
tes
Swit
zerl
and
Luxe
mb
ou
rg
No
rway
Ge
rman
y
Irel
and
Swed
en
Ne
the
rlan
ds
Au
stri
a
Den
mar
k
Bel
giu
m
Au
stra
lia
Can
ada
Fran
ce
Jap
an
Icel
and
Un
ited
Kin
gdo
m
Fin
lan
d
OEC
D A
VER
AG
E
Ne
w Z
eal
and
Ital
y
Spai
n
Slo
ven
ia
Isra
el
Po
rtu
gal
Ko
rea
Cze
ch R
epu
blic
Gre
ece
Slo
vak
Rep
ub
lic
Hu
nga
ry
Esto
nia
Ch
ile
Po
lan
d
Latv
ia
Turk
ey
Mex
ico
USD
PP
P
Source: OECD Health Statistics 2017
US spends two-and-a-half times the OECD averageTotal health expenditure, per capita
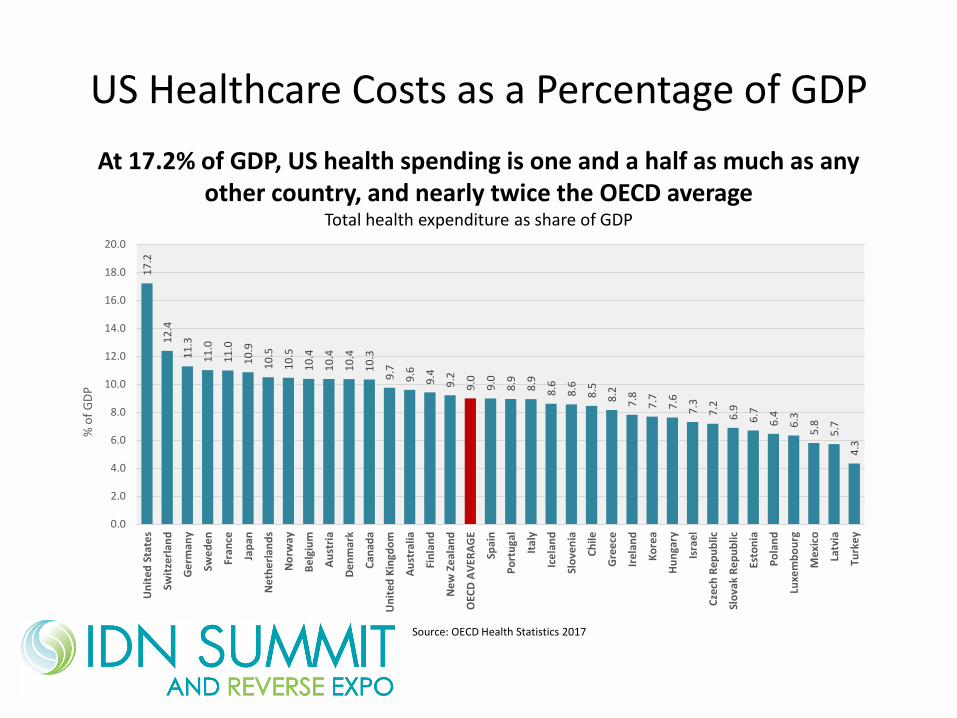
US Healthcare Costs as a Percentage of GDP1
7.2
12
.4
11
.3
11
.0
11
.0
10
.9
10
.5
10
.5
10
.4
10
.4
10
.4
10
.3
9.7
9.6
9.4
9.2
9.0
9.0
8.9
8.9
8.6
8.6
8.5
8.2
7.8
7.7
7.6
7.3
7.2
6.9
6.7
6.4
6.3
5.8
5.7
4.3
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
16.0
18.0
20.0
Un
ited
Sta
tes
Swit
zerl
and
Ge
rman
y
Swe
de
n
Fran
ce
Jap
an
Ne
the
rlan
ds
No
rway
Be
lgiu
m
Au
stri
a
De
nm
ark
Can
ada
Un
ited
Kin
gdo
m
Au
stra
lia
Fin
lan
d
Ne
w Z
eal
and
OEC
D A
VER
AG
E
Spai
n
Po
rtu
gal
Ital
y
Ice
lan
d
Slo
ven
ia
Ch
ile
Gre
ece
Irel
and
Ko
rea
Hu
nga
ry
Isra
el
Cze
ch R
ep
ub
lic
Slo
vak
Re
pu
blic
Esto
nia
Po
lan
d
Luxe
mb
ou
rg
Mex
ico
Latv
ia
Turk
ey
% o
f G
DP
Source: OECD Health Statistics 2017
At 17.2% of GDP, US health spending is one and a half as much as any other country, and nearly twice the OECD average
Total health expenditure as share of GDP

US Health Spending By Category of Care
Reference: #14

US vs Other Countries: Health Procedure Prices
Reference: #14

US vs Other OECD Countries Volume of Healthcare Procedures
Reference: #14
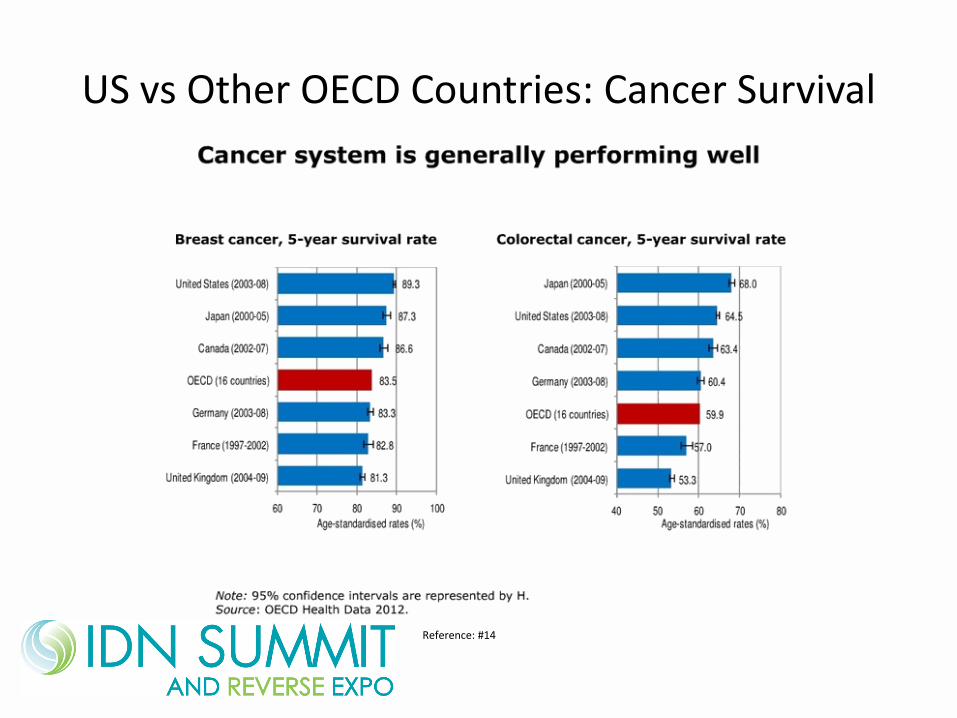
US vs Other OECD Countries: Cancer Survival
Reference: #14
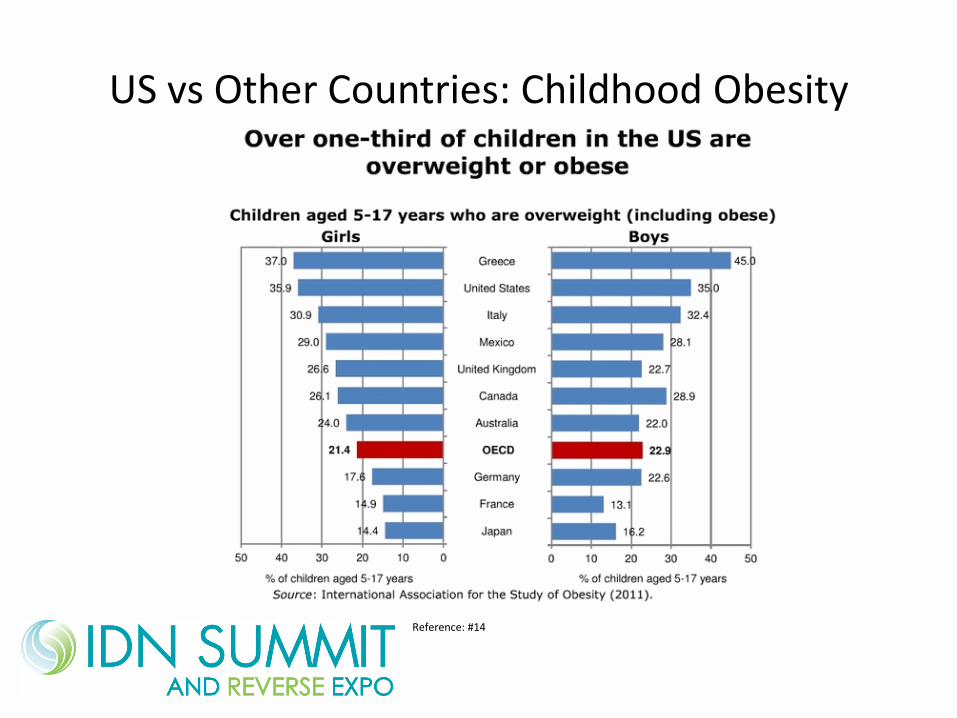
US vs Other Countries: Childhood Obesity
Reference: #14
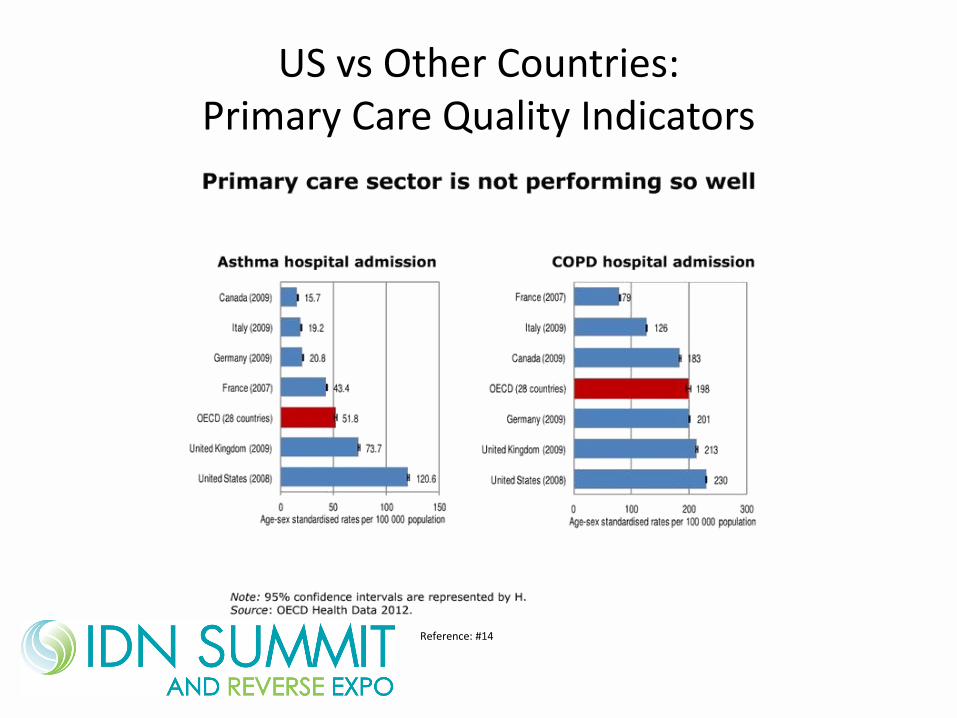
US vs Other Countries:Primary Care Quality Indicators
Reference: #14
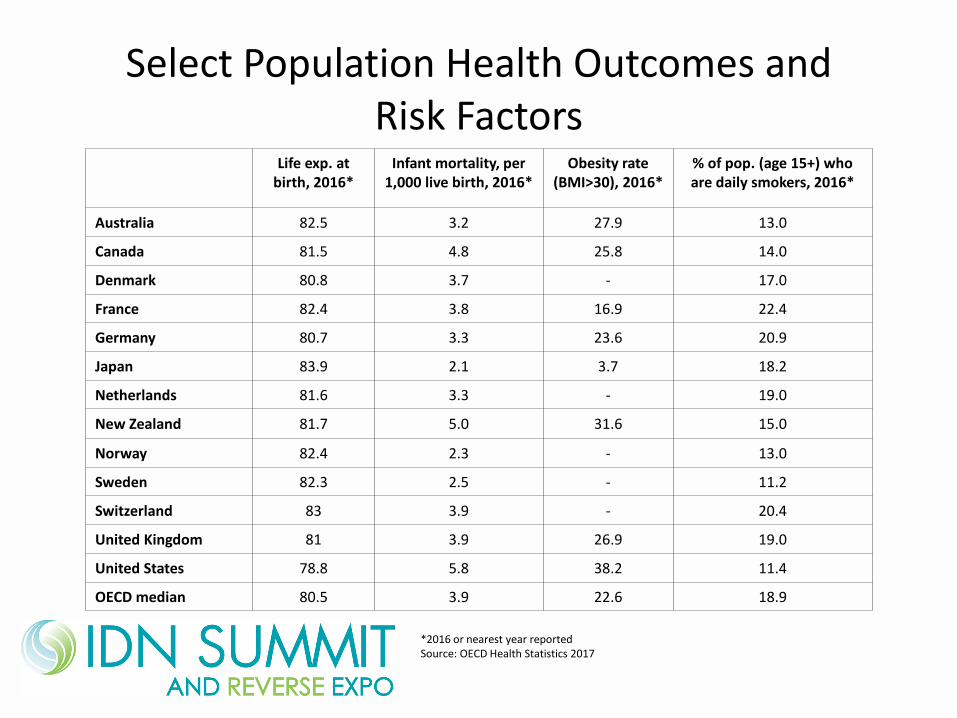
Select Population Health Outcomes and Risk Factors
Life exp. atbirth, 2016*
Infant mortality, per 1,000 live birth, 2016*
Obesity rate (BMI>30), 2016*
% of pop. (age 15+) who are daily smokers, 2016*
Australia 82.5 3.2 27.9 13.0
Canada 81.5 4.8 25.8 14.0
Denmark 80.8 3.7 - 17.0
France 82.4 3.8 16.9 22.4
Germany 80.7 3.3 23.6 20.9
Japan 83.9 2.1 3.7 18.2
Netherlands 81.6 3.3 - 19.0
New Zealand 81.7 5.0 31.6 15.0
Norway 82.4 2.3 - 13.0
Sweden 82.3 2.5 - 11.2
Switzerland 83 3.9 - 20.4
United Kingdom 81 3.9 26.9 19.0
United States 78.8 5.8 38.2 11.4
OECD median 80.5 3.9 22.6 18.9
*2016 or nearest year reportedSource: OECD Health Statistics 2017

Healthcare Cost Drivers
• New medical technologies
• Excess and medically unnecessary use of healthcare products
• Financial incentives that reward overutilization
• Clinical variation and inefficiencies
• Opinion and preference-based healthcare decisions
• Medical errors and poor transitions of care
Reference: #2

Aligning Reimbursement with Value: Value-Based Purchasing (VBP)
• VBP models are “operationally defined as financial incentives that aim to improve clinical quality and outcomes for patients, while simultaneously containing (or better yet) reducing healthcare costs.”
Reference: #6
How can providers achieve successful VBP initiatives?
• Create efficient infrastructures with seamless transitions of care within an integrated care network
• Escape the “hamster wheel”-volume-driven patient care and payment models to generate revenue
• Adopt payment models that promote and reward clinical practices that improve health
In other words: deliver evidence-based, cost-effective healthcare
Reference: #6
Value-Based Payment Models
• Shared savings within ACOs
• Primary care capitation
• Reference pricing
• Global payments
• Pay for performance (P4P)
• Bundled payments
Reference: #6
Bundled Payments
• “A method in which payments to healthcare providers are related to the predetermined expected costs of a grouping, or ‘bundle’ of related healthcare services within a defined episode of care.”
• Purpose is to decrease healthcare spending while improving or maintaining the quality of care.
• Bundled payments may provide reimbursement for both surgical procedures and medical conditions.
Reference: #10
Impact of Bundled Payments on Quality and Cost
• Early findings include:
–Reductions in healthcare spending and utilization
– Inconsistent and generally small effects on quality measures
– Strength of evidence: Weak or insufficient
Reference: #10

Impact of Bundled Payments: Recent Findings
• Surgical vs medical bundles yield higher and more consistent savings
• Shorter episodes of care are easier to manage
• Standardizing health technologies and managing utilization contribute to cost reduction
• Managing post acute care (PAC) essential
Reference: #8
Potential Unintended Consequences
• Possible overdiagnosis
• May create incentive to underuse tests and treatments
• Impact upon the decision to hospitalize or to perform surgery
• Providers may be rewarded for increasing patients’ awareness of symptoms and overprescribing tests
• Hospital-centric
Reference: #9
Your Challenges in Defining Bundles
• Defining the bundle episode/time frame
• Determining the appropriate mix of services/ technologies
• Defining the appropriate costs
• Using a normative approach (pros and cons)
• Utilizing the best available evidence
Reference: #9
CMS Bundled Payment: Recent Announcements
CMS has reduced the number of mandatory geographic areas participating in the :
–Comprehensive Care for Joint Replacement (CJR) from 67 to 34
– the 33 remaining areas will participate on a voluntary basis as will all low volume and rural hospitals
CMS has proposed to cancel all Episode Payment models and Cardiac Rehabilitation (CR) incentive model
This gives CMS greater flexibility to design and test new models
https://www.cms.gov/Newsroom/MediaReleaseDatabase/Press-releases/2017-Press-releases-items/2017-08-15.html
Your Role in Bundled Payments
• Reducing clinical variation through: –Product standardization
–Utilization protocols
• Improving clinical outcomes through: –Development and application of comparative effectiveness
research reviews
– Informing new technology acquisition, formulary inclusion, and utilization protocols
• Supporting development of evidence-based: –Clinical policies
–Medical necessity determinations and guidelines
Expert Commentary: Altarum’s Francois de Brantes
• CMS’ withdrawal of hospital-centric mandated bundled payment program does not mean a CMS retreat from value-based payment.
• The current models were deeply flawed
• The Payment Model Technical Advisory Committee proposed earlier this year, new proposed APMs that are varied BPs
• States have adopted various BP models
• Employers are set on payment reform and expanding their use of BP programs (ex. CarrumHealth)
• National, regional and local plans are engaged in comprehensive BP programs
HealthExecSnapshot, August 24, 2017

Shift the ‘locus of control’ of bundled payments from a hospital-centric model to…..
• Close to the patient’s needs,
• Community based and
• Under physician control
How do ‘bundled payment programs’ apply to you?
• Review your job description. Negotiate changes.
• Ask to be assigned to clinical committees supporting the creation of bundled payments. Provide clinical colleagues with the needed clinical evidence analyses.
• Anticipate standardization decisions and utilization protocols necessary in bundles.
• Incorporate the evaluation of applicable health technologies in your workflow, using the best available evidence.
• Interface with your counterparts in the community with regard to the health technologies that are part of the bundle.
Prioritize Your Work Efforts
• Look for high-cost products appearing in multiple bundles
• Bundles mandated by CMS’s CJR model or negotiated within commercial contracts
• Health technology categories with wide variation in costs and high rates of utilization
• Other approaches

Case Study: Centura Health
Up to $900,000 annual savings
“Practice change is really where sustainability is. Providing physicians with the evidence from Hayes to make good decisions is where the real value comes from.”
Karla Barber, RN, BSN, CVAHPSystem Director of Clinical Value Analysis
Case Study: Centura Health
• Challenge:
–Centura Health had significant variation in the utilization patterns of antibiotic-impregnated bone cement in total joint replacements.
– Some physicians were using it on every patient, regardless of whether or not it was a new joint replacement or a revision
– There was also variation in the type of antibiotic used along with the dosage, as well as disagreement as to whether to use a premixed cement or to compound on site
Case Study: Centura Health
• Solution:
–Collaboration between Hayes and multiple stakeholders at Centura Health resulted in a standard of practice in the use of antibiotics in bone cement that took into account:
•When to use an antibiotic and for which patients
•Proper dosing
•Use of premix vs. compounding
Case Study: Centura Health
• Hayes’ Advantage
–Prior to their subscription to the Hayes evidence solution, Centura partnered with a competing health technology assessment provider.
– The competing HTA provider was unable to provide customized reports or product comparisons and did not include regulatory information or summary checklists.
–Hayes was able to meet all of Centura’s needs and provide a valuable outcome.


REFERENCES
1. Case study: Delivery and payment reform in congestive heart failure at two large academic centers. Meaghan George, Sara Bencic, Sarah Bleiberg, Nawara Alawa, Darshak Sanghavi. Healthcare Vol. 2 (2014) 107-112.
2. Evaluating the State of Quality-Improvement Science through Evidencre Synthesis: Insights from the Closing the Quality Gap Series. Kathryn M. McDonald, MM; Ellen M. Schultz, MS; Christine Chang, MD, MPH. The Permanente Journal/Fall 2013/Vol. 17 No. 4 (see Quotes and Tables).
3. Relationship between the Charlson Comorbidity Index and cost of treating hip fractures: Implications for bundled payment. Daniel J. Johnson, Sarah E. Greenberg, Vasanth Sathiyakumar, Rachel Thakore, Jesse M. Ehrenfeld, William T. Obremskey, Manish K. Sethi. JOrthopaed Traumatol (2015) 16:209-213.
4. Bundled Payment and Care of Acute Stroke – What Does it Take to Make it Work? David Bruce Matchar, MD, Hai V. Nguyen, PhD, YuanTian, MSc. Stroke (2015) 46:1414-1421 (see Table on P 8/1418-1419).
5. Large Variations in Medicare Payments for Surgery Highlight Savings Potential From Bundled Payment Programs. David C. Miller, Cathryn Gust, Justin B. Dimick, Nancy Birkmeyer, Jonathan Skinner, John D. Birkmeyer. Health Affairs Vol. 30, No. 11 (2011):2107-2115.
6. Implementing Value-Based Payment Reform: A Conceptual Framework and Case Examples. Douglas A. Conrad, Matthew Vaughn, David Grembowski, Miriam Marcus-Smith. Medical Care Research and Review (2016) Vol. 73 (4) 437-457.
7. Episode-Based Payment: Evaluating the Impact on Chronic Conditions. Thomas J. O’Byrne, Nilay D. Shah, Douglas Wood, Robert E. Nesse, Patrick J. F. Killinger, William J. Litchy, Robert J. Stroebel, Amy E. Wagie, James M. Naessens. Medicare and Medicaid Research Review (2013) Vol. 3 (3).
8. Cost of Joint Replacement Using Bundled Payment Models. Amol S. Navathe, MD, PhD; Andrea B. Troxel, ScD; Joshua M. Liao, MD, Nan , MS; Jingsan Zhu, MS; Wenjun Zbhong, PhD; Ezekiel J. Emanuel, MD, PhD. JAMA Intern Med. Doi:10.1001/jamainternmed.2016.8263.
9. Paying More Wisely: Effects of Payment Reforms on Evidence-based Clinical Decision Making. Timothy K. Lake, Eugene C. Rich, Christal Stone Valenzano, Myles M. Maxfield. Journal of Comparative Effectiveness Research. 2.3 (May 2013): p 249.

REFERENCES
10. Bundled Payment: Effects on Health Care Spending and Quality – Closing the Quality Gap: Revisiting the State of the Science. Evidence Report/Technology Assessment (No. 208), AHRQ.
11. CMS Bundled Payments for Care Improvement Initiative Models 2-4: Year 2 Evaluation & Monitoring Annual Report. The Lewin Group (Laura Dummit, Grecia Marrufo, Jaclyn Marshall, Ellen Tan, Aylin Bradley, Cornelia Hall, Younyoung Lee, Jon Kelly, Megan Hyland, Rebecca Cherry, Court Melin, Brandon Maughan, Ayah Fannoun, Ashley Johnson, Gina Zurbey, Susan Joy, Sarah Tucker, Sebastian Negrusa, Madison Davidson, Nina Alesci, Ian Glenn, Dan Gregory, Laura Smith, David Zhang, Alex Lampert, Nick Morgan, Greyson Gordon, Jessica Steier, Dean Farley, Qian Gu, Ian Breunig, Matt Trombley, Andrea Hassol, Christine LaRocca, Lindsay Kirsch. (August 2016): Centers for Medicare and Medicaid Services, Contract No. HHSM-500-2011 Task Order HHSM-500-T0007.
12. Bundled Payments for Care Improvement (BPCI) Initiative: General Information. Centers for Medicare & Medicaid Services.
13. Alternative Payment Models. Katherine Baicker, PhD; Michael E. Chernew, PhD. JAMA Internal Medicine. Published online January 3,2017.
14. U.S. Health Care from a Global Perspective – Spending, Use of Services, Prices, and Health in 13 Countries. David Squires, ChloeAnderson. The Commonwealth Fund, October 2015.
15. Value-Based Purchasing: The Evidence. Gloria B. Eldridge, PhD, MSc; Holly Korda, PhD, MA. Am J Manag Care 2011; 17(8):e310-e313).
16. Bundled Payment Initiatives for Medicare and Non-Medicare Total Joint Arthroplasty Patients at a Community Hospital: Bundles in the Real World. James P. Doran, BS; Stephen J. Zabinski, MD. The Journal of Arthroplasty 30 (2015) 353-355.
17. ProvenCare: quality improvement model for designing highly reliable care in cardiac surgery. SA Berry, MC Doll, KE McKinley, AS Casale, A Bothe Jr. Qual Self Health Care 2009:18:360-368.
