environmental factors of importance in myasthenia...
TRANSCRIPT

ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2018
Digital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1439
Environmental Factors ofImportance in Myasthenia Gravis
Emphasis on Physical Activity
ELISABET WESTERBERG
ISSN 1651-6206ISBN 978-91-513-0262-1urn:nbn:se:uu:diva-344667

Dissertation presented at Uppsala University to be publicly examined in Gunnesalen,Psykiatrins hus, Akademiska sjukhuset, ingång 10, Uppsala, Friday, 27 April 2018 at 09:00for the degree of Doctor of Philosophy (Faculty of Medicine). The examination will beconducted in English. Faculty examiner: Professor Chantal Tallaksen (Oslo universitet).
AbstractWesterberg, E. 2018. Environmental Factors of Importance in Myasthenia Gravis. Emphasison Physical Activity. Digital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1439. 75 pp. Uppsala: Acta Universitatis Upsaliensis.ISBN 978-91-513-0262-1.
Myasthenia Gravis (MG) is an autoimmune disease caused by antibodies directed againstproteins at the neuromuscular junction (NMJ). The disturbed neuromuscular transmissioninduces fatigable weakness in skeletal muscles. The severity of MG ranges from purely ocularsymptoms to extensive weakness with, at worst, respiratory failure and need of intensive care.Due to different pathogenic antibodies, as well as varying phenotypes there is a classificationinto MG subgroups.
As lifestyle disorders are common conditions they occur also in MG patients. It is unknownwhether there are any lifestyle factors associated with MG or MG subgroups. However,medication side effects and disability due to disease could contribute to higher risks for lifestylerelated diseases. General treatment guidelines are not suitable to MG patients, since variousmedications are known to affect the disease negatively and as the tolerance and effects ofphysical activity in MG is unknown.
In this thesis the occurrence of lifestyle related environmental factors in MG patients wereinvestigated. MG epidemiology, subgroup differences and the presence of lifestyle related risksin MG patients were evaluated in Jönköping county in Southern Sweden. The findings werecompared to a similar evaluation in a region of Estonia. We found that MG patients in the late-onset disease subgroup had a more disadvantageous pattern of life-style related risk factors, witha higher rate of obesity, smoking and physical inactivity and a lower rate of fish consumptionin comparison to matched population controls. Furthermore, we found that despite comparableclinical muscle fatigue status, Estonian MG patients subjectively scored fatigue and diseaseseverity higher than Swedish MG patients. More Estonian patients were physically inactive.The tolerance and effects of physical exercise was further evaluated in two intervention studies,where MG patients with stable disease performed a 12-week-training-program according togeneral exercise recommendations to healthy adults. We found that physical exercise was welltolerated by the MG patients and that they had a beneficial skeletal muscle response to physicalexercise.
Keywords: Myasthenia Gravis, MG subgroups, Environmental factors, Lifestyle, Physicalactivity, Exercise
Elisabet Westerberg, Department of Neuroscience, Clinical Neurophysiology, Akademiskasjukhuset, Uppsala University, SE-75185 Uppsala, Sweden.
© Elisabet Westerberg 2018
ISSN 1651-6206ISBN 978-91-513-0262-1urn:nbn:se:uu:diva-344667 (http://urn.kb.se/resolve?urn=urn:nbn:se:uu:diva-344667)

”To tell the probability, the whole probabilityand nothing but the probability.”
Tage Danielsson


List of Papers
This thesis is based on the following papers, which are referred to in the text by their Roman numerals.
I Sabre L*, Westerberg E*, Liik M, Punga AR. (2017) Diversity
in mental fatigue and social profile of patients with myasthenia gravis in two different Northern European countries. Brain Be-havior, Mar 1;7(4):e00653. doi: 10.1002/brb3.653. eCollection 2017 Apr.
II Westerberg E, Landtblom AM, Punga AR. Lifestyle factors and gender-related differences in clinical subgroups of Myasthenia Gravis in southern Sweden. Submitted manuscript.
III Westerberg E, Molin CJ, Lindblad I, Emtner M, Punga AR. (2017) Physical exercise in myasthenia gravis is safe and im-proves neuromuscular parameters and physical performance-based measures: A pilot study. Muscle & Nerve. Aug;56(2):207-214. doi: 10.1002/mus.25493. Epub 2017 Apr 2.
IV Westerberg E, Molin CJ, Spörndly Nees S, Widenfalk J, Punga AR. The impact of physical exercise on functional muscle measures in Myasthenia Gravis patients - a single subject design study. Submitted manuscript. * Equal contribution.
Reprints were made with permission from the respective publishers.


Contents
Introduction ................................................................................................... 13 Brief history.............................................................................................. 13 Epidemiology ........................................................................................... 14 Pathophysiology ....................................................................................... 14
Neuromuscular dysfunction ................................................................. 15 Autoimmunity ...................................................................................... 16 Genetics and epigenetics in MG .......................................................... 18
Clinical presentation ................................................................................. 19 Muscle weakness and fatigability ........................................................ 19 Myasthenic and cholinergic crises ....................................................... 19 Disease severity ................................................................................... 20 Other features of MG ........................................................................... 20 MG impact on everyday life ................................................................ 21
Diagnosis .................................................................................................. 21 Clinical evaluation ............................................................................... 21 Bedside tests ........................................................................................ 22 Electrophysiological tests .................................................................... 22 Antibody serology ............................................................................... 23 Thymus radiology ................................................................................ 23
Classification, MG subgroups .................................................................. 24 MG subgroups ..................................................................................... 24
Management ............................................................................................. 28 Environmental factors .............................................................................. 28
Lifestyle factors and MG ..................................................................... 29 Physical activity and MG ..................................................................... 29
Aims .............................................................................................................. 31 Specific aims ............................................................................................ 31
Study I .................................................................................................. 31 Study II ................................................................................................ 31 Study III ............................................................................................... 31 Study IV ............................................................................................... 31

Methods ........................................................................................................ 32 Study design ............................................................................................. 32 Ethics ........................................................................................................ 32 Subjects .................................................................................................... 32
Study I-III ............................................................................................ 33 Study IV ............................................................................................... 33
Data collection .......................................................................................... 33 Medical records. .................................................................................. 34 Questionnaires ..................................................................................... 34 Clinical neurological examination. ...................................................... 35 Electrophysiological assessments ........................................................ 35 Physical performance-based measures ................................................ 36 Physical activity patterns ..................................................................... 36 Anthropometric measures .................................................................... 36 Blood samples and analysis ................................................................. 36 Circulating microRNAs ....................................................................... 37
Physical exercise regimen ........................................................................ 37 Statistical methods .................................................................................... 37
Study I and II. ...................................................................................... 37 Study III and IV. .................................................................................. 38
Results ........................................................................................................... 39 Study I ...................................................................................................... 39
Differences and similarities between MG patients in Tartu and Jönköping regions. ............................................................................... 39
Study II ..................................................................................................... 41 Lifestyle factors and gender-related differences of MG subgroups in southern Sweden. ............................................................................. 41 The MG cohort .................................................................................... 41 Comparisons to the control group ........................................................ 46
Study III ................................................................................................... 48 The safety of physical exercise in MG. ............................................... 48
Study IV ................................................................................................... 51 Muscular effects of physical exercise in MG patients. ........................ 51
Discussion ..................................................................................................... 54 Epidemiological considerations ............................................................... 54 Comparison between different geographical regions ............................... 55
Prevalence, distribution of subgroups and gender ............................... 55 Symptoms, perceived health, clinical status and treatment ................. 55
Comparisons between different subgroups .............................................. 56 Distribution of subgroups, age and gender .......................................... 56 Time to diagnosis, clinical picture and status ...................................... 56 Treatment ............................................................................................. 57

Comparisons to matched population controls .......................................... 57 Occurrence and management of high-prevalence disorders in patients with a low-prevalence disease ................................................ 57 Lifestyle factors ................................................................................... 58 Impact on everyday life ....................................................................... 59
MG and physical activity ......................................................................... 59 Drawbacks with exercise studies ......................................................... 59 How to measure effects of exercise ..................................................... 60 Safety and effects of exercise in MG patients ..................................... 61
Conclusions ................................................................................................... 63
Sammanfattning på svenska – Summary in Swedish .................................... 64
Acknowledgements ....................................................................................... 66
References ..................................................................................................... 68


Abbreviations
ACh Acetylcholine AChEI Acetylcholine esterase inhibitors AChR Acetylcholine receptor AChR+ Acetylcholine receptor antibody seropositive AChR- Acetylcholine receptor antibody seronegative AD Autoimmune disease AOR Adjusted odds ratio BMI Body mass index CMAP Compound motor action potential ESES Exercise self-efficacy scale EOMG Early onset myasthenia gravis FSS Fatigue severity scale HHD Hand-held dynamometer HLA Human leucocyte antigen IM Immunosuppressive therapy other than corticoster-
oids (specified as a, azathioprine; c, ciklosporin; r,rituximab)
IVIG Intravenous immunoglobulins LOMG Late onset myasthenia gravis LRP4 Lipoprotein receptor-related protein 4 LRP4+ Lipoprotein receptor-related protein 4 antibody sero-
positive MG Myasthenia gravis MGC Myasthenia gravis composite scale MGFA Myasthenia Gravis Foundation of America MGFA-PIS MGFA Post-Intervention Status MGQoL-15 Myasthenia gravis quality of life – 15 item scale MHC Major histocompatibility complex miRNA MicroRNA mRNA Messenger RNA MuSK Muscle specific tyrosine kinase MuSK+ Muscle specific tyrosine kinase antibody seropositiveNMJ Neuromuscular junction NT No therapy OMG Ocular myasthenia gravis PEF Peak expiratory flow

PR Prednisone and other corticosteroids QMG Quantitative myasthenia gravis test RA Rheumatoid arthritis RIA Radioimmunoassay RNS Repetitive nerve stimulation SFEMG Single fiber electromyography SLE Systemic lupus erythematosus SPT Status post thymectomy TUG Timed up and go 6MWT Six-minute walk test 12MWT Twelve-minute walk test 30SCST Thirty-second chair stand test

13
Introduction
Myasthenia Gravis (MG) is an autoimmune disease (AD) caused by antibod-ies directed against proteins at the neuromuscular junction (NMJ). The dis-turbed neuromuscular transmission induces fatigable weakness in skeletal muscles. With emerging knowledge on MG subgroup differences, the need for tailored medical as well as non-medical management is growing.
The focus of this thesis was to characterize lifestyle factors of importance in MG and to assess the safety and potential benefits of physical exercise in MG patients. Additionally, similarities and differences between MG sub-groups were evaluated.
Brief history The first detailed account of MG is dated to 1672 when Thomas Willis de-scribed the disease “spurious palsy” [1]. In the late 19th century the disease was more thoroughly depicted by Erb and Goldflam, who emphasized the dis-tinctions from other paralyses, and for some years the disease was called Erb’s or Erb–Goldflam disease. In 1895 the German neurologist Friedrich Jolly pro-posed the name “Myasthenia Gravis pseudoparalytica” [1], which is a mixture of Greek and Latin (gr. myasthenia=muscle weakness, lat. Gravis=severe, gr. pseudo=false and gr. & lat. paralysis=paralysis). Jolly also showed the my-asthenic decrease in muscle contraction in response to repetitive stimulation of the innervating nerve. During the 1920s the understanding of synaptic trans-mission started to grow; the chemical nature of neurotransmission was identi-fied and acetylcholine (ACh) was found to be the neuromuscular transmitter substance [2]. In 1934 Mary Walker successfully treated MG patients with physostigmine, an acetylcholinesterase inhibitor (AChEI) and likewise the an-tidote to curare, as she had noticed the clinical similarities between MG and curare poisoning [3]. During the following decades an autoimmune mecha-nism was suggested, due to observed benefits from thymectomy, the discovery of thymus abnormalities and the observed high occurrence of other ADs in MG patients. A hypothesis of autoantibodies directed against an endplate pro-tein at the NMJ was formulated by the Scottish neurologist John A. Simpson in 1960 [4], but it was Jim Patrick and Jon Lindstrom who in the 1970s finally consolidated the autoimmune hypothesis by immunizing rabbits with acetyl-choline receptor (AChR) and demonstrating a consequent raise in antibodies

14
directed against AChR [5]. The pathogenic role of the AChR antibodies was further confirmed by the improvement of MG patients upon depletion of the antibodies by plasma exchange [6]. Assays to assess AChR antibodies in the clinical management of MG patients were developed and their sensitivity has continuously improved. In previously AChR antibody seronegative patients, pathogenic antibodies directed to muscle specific tyrosine kinase (MuSK) [7] and lipoprotein receptor-related protein 4 (LRP4) [8] have been found in par-allel with increased understanding of the immune mechanisms of the disease. Still, the underlying cause of MG remains unknown [9].
Epidemiology The annual global incidence of MG is estimated to be 4–12 per million and the prevalence rate ranges from 15 to 250 per million [10-17]. As older epide-miological MG studies tend to report lower prevalence rates than more recent surveys, the wide prevalence range is probably explained by modified re-search methodology over time, as well as novel disease knowledge, improved treatment regimens and an increased number of elderly people in the popula-tion. Nevertheless, true regional differences probably do exist, especially with regard to MG subgroups, due to genetic, environmental and socioeconomic differences [12].
Due to clinical and immunological heterogeneity, MG is often divided into subgroups. Therefore, within MG epidemiology it is necessary to specify whether the information concerns all patients with a clinical diagnosis of MG or if a certain subgroup is considered [10]. Estimated worldwide prevalence of the subgroups is shown in figure 3 (page 27).
The prevalence of MG is higher in females, which is often seen in autoim-mune conditions. Gender differences vary between MG subgroups and the fe-male predominance is particularly high in early onset MG (EOMG), where the female to male ratio commonly is set at 3:1 [11], although ratios as high as 9:1 have occasionally been reported [18]. The gender ratio in late onset MG (LOMG) shows a slight male predominance [11].
Pathophysiology MG is caused by antibodies against components of the muscle membrane at the NMJ. The origin of the autoimmune dysfunction remains unknown. To understand MG pathophysiology the mechanisms of autoimmunity and neu-romuscular dysfunction, as well as their mutual interactions, need to be further elucidated.

15
Neuromuscular dysfunction When autoantibodies bind to components of the NMJ, the resulting block of neuromuscular transmission, i.e. neuromuscular dysfunction, gives rise to the characteristic muscle weakness of MG. This occurs through a series of reac-tions mainly located at the muscle membrane. A schematic picture of the NMJ is shown in figure 1.
Figure 1. Simplified, schematic illustration of the NMJ, with the most common MG antigens (AChR, MuSK, LRP4, agrin) indicated.
Normal neuromuscular transmission The principal task of the NMJ is to transfer motor neuron action potentials to the skeletal muscle fiber [19].
Each skeletal muscle fiber is innervated by only one single α-motor neuron. This single motor neuron branches within the muscle to nerve terminals that synapse on different muscle fibers. When an action potential is generated by the motor neuron its connected muscle fibers contract simultaneously. The single motor neuron and its associated muscle fibers together constitute the smallest unit of force that can be activated to produce movement; the motor unit [20].
ACh has an important function in mediating the signal between the nerve terminal and its muscle fiber. Upon depolarization of the nerve terminal, ACh is released and binds to AChRs at the muscle membrane. In response to the receptor binding, the AChR channel opens and positively charged ions flow into the muscle cell. Consequently, endplate potentials are generated, which causes muscle contraction.

16
To ensure normal neuromuscular transmission, the release of ACh into the synapse is much higher than needed to produce a muscle contraction. Further-more, the AChRs are clustered at the synaptic cleft and the area of the muscle membrane is increased by arrangement into synaptic folds. There are many proteins, e.g. muscle specific tyrosine kinase (MuSK), low-density lipoprotein receptor-related protein 4 (LRP4) and agrin, known to be crucial for the AChR clustering and the maintenance of the NMJ architecture [21-25].
Impaired neuromuscular transmission Impaired neuromuscular transmission is the hallmark of MG, giving rise to the typical symptoms of fatigable muscle weakness. Neuromuscular dysfunc-tion is caused by autoantibodies directed against antigens at the NMJ. The antigens differ between MG subgroups, as do their specific effects on proteins at the NMJ. In most cases there is a reduction of AChRs at the NMJ and a destruction of the postsynaptic membrane architecture. Direct AChR blocking mechanisms have occasionally been described [26].
Autoimmunity As in other ADs the origin of the autoimmune dysfunction in MG is unknown. Several features are similar among ADs, suggesting common pathogenic mechanisms. There are numerous autoimmune hypotheses addressing predis-posing factors (e.g. genetics, epigenetics, hormones, vitamin D status, micro-biota), triggering components (e.g. infections, drugs) and their interactions with the immune system [18]. It is reasonable to assume that autoimmunity could not be explained by one of these hypotheses exclusively [27] and an improved understanding of their mutual relationships are of probable im-portance to better understand the development of ADs.
Autoimmunity is characterized by an inappropriate immune response di-rected against structures of one’s own body. There are two major forms of immune response; a B-cell derived autoantibody-mediated mechanism and a T-cell derived mechanism mediated by autoreactive T-lymphocytes [28]. The autoimmune response of MG is typically autoantibody-mediated [29], alt-hough (probably subsidiary) pathological T-cell-reactions have been de-scribed [30]. Antibody-producing B-cells organize into germinal centers, which in the physiological situation are localized in secondary lymphoid or-gans such as lymph nodes, tonsils and spleen. In most ADs the B-cell expan-sion takes place in structures resembling secondary lymphoid organs, within the target organ, which is also the site of inflammation. This is different in MG, where the specific target of the autoantibodies, i.e. the NMJ, is not the site of the immune infiltration. Instead, the immune infiltration occurs in the thymus, the organ where development of immunological self-tolerance nor-mally takes place.

17
Autoantibodies in MG There are different autoantibodies of known importance in the disease mech-anisms of MG. With a few exceptions, most individual cases have only one type of pathogenic antibody. However, some patients do not have any detect-able antibodies. Furthermore, some patients have additional antibodies of as-sumed non-pathogenic nature. The autoantibodies target postsynaptic antigens at the NMJ.
Antibodies against the acetylcholine receptor The predominant disease-causing antibodies, found in about 85% of patients, are directed at the AChR, located on the muscle membrane at the NMJ. The AChR antibodies are mainly of IgG1 and IgG3 subclasses [31], which through complement-mediated destruction cause a reduced number of AChRs and a derangement of the muscular synaptic folds. As the pathogenicity differs be-tween antibodies directed at different AChR subunits, antibody concentrations do not necessarily correlate with symptom severity between patients [32-36]. Fluctuations in AChR antibody concentration in an individual patient could however sometimes correlate with disease severity [33]. It has been shown though, that the loss of functional AChRs are of greater importance to disease severity [36].
Antibodies against muscle specific tyrosine kinase Antibodies against MuSK [37] are present in 1-5% of all MG patients, mainly in AChR antibody seronegative (AChR-) patients. MuSK antibodies are di-rectly pathogenic antibodies of the IgG4 subclass [33, 36, 38]. Their main ac-tion is to cause disassembly of the NMJ by reducing the postsynaptic density of AChRs [39, 40]. There is an intraindividual correlation between the disease severity and the antibody titer [41-43].
Antibodies against low density lipoprotein receptor related protein 4 LRP4 is a protein, which, through interaction with agrin, activates MuSK [8, 44]. Antibodies to LRP4 are detected in 1–3% of all MG patients [11]. They are complement binding IgG1 subclass antibodies [42].
Other antibodies In addition to the above described, directly pathogenic antibodies, other anti-bodies have been found in some MG patients, both seropositive and seroneg-ative to AChR, MuSK and LRP4. These antibodies are often directed against cytoplasmic muscle proteins such as titin, ryanodine receptor and actin [45]. The importance of these antibodies remains largely unclear. They could some-times, serve as markers of a thymoma [32, 33, 46], as they are detected in 75–85% of patients with thymomatous MG [32, 46].

18
Antibodies to agrin can be detected in few MG patients with or without antibodies against AChR, MuSK or LRP4 [47]. They seem to be disease spe-cific. Agrin is important to the formation, maintenance and regeneration of the NMJ [24].
Thymic dysfunction The physiological function of the thymus is to regulate T-cell differentiation and establish central tolerance by elimination of autoreactive T cells [28, 40]. The thymus has an important role in MG pathogenesis [48, 49], although the detailed mechanisms remain unclear. Consequently, thymectomy is beneficial to some subgroups of MG patients [50], in particular EOMG that is associated with thymic medullary follicular hyperplasia. Further, MG can be caused by a thymoma, but in contrast not all thymoma patients develop MG. The type of thymic dysfunction differs between MG subgroups [49]. Follicular thymic hy-perplasia consists of lymph node-like infiltrates including T cell areas and ger-minal centers (B-cell areas) [51]. Thymic cells are known to produce AChR antibodies both in hyperplastic and some atrophic thymuses [52]. For patients with thymoma the pathogenesis is thought to be closer related to the produc-tion of T lymphocytes [49].
Genetics and epigenetics in MG Genetics The development of autoimmunity generally requires a genetic predisposition in addition to being exposed to a triggering environmental factor. The major histocompatibility complex (MHC) region represents the most important ge-netic risk factor for most ADs [18, 53] and many MG subgroups are associated with specific human leucocyte antigen (HLA) haplotypes.
Epigenetics Epigenetic mechanisms including microRNA, DNA methylation, and histone acetylation are thought to influence the development of ADs. MicroRNAs (miRNAs) are 20-22 nucleotide long non-coding RNA molecules involved in post-transcriptional regulation of certain messenger RNAs (mRNAs). Through this mechanism miRNAs can regulate major cellular processes such as apoptosis, cell differentiation and immune functions [18] and thereby pro-mote or suppress autoreactivity in ADs. In the sera of AChR antibody sero-positive (AChR+) MG patients miR-150-5p and miR-21-5p have been found to be specifically dysregulated [18, 54].

19
Clinical presentation The cardinal symptoms of MG are skeletal muscle weakness and abnormal muscle fatigue, both caused by disturbed neuromuscular transmission. Despite having this mandatory muscle fatigue in common, the disease can present very differently between patients.
Muscle weakness and fatigability The distribution and severity of muscle weakness differ among patients and the clinical course is highly variable. The weakness can be generalized or lo-calized and the disease severity can range from minimal symptoms to exten-sive weakness with occurrence of several exacerbations over time and, at worst, respiratory failure. Extraocular muscles are very often involved; with diplopia and ptosis as typical symptoms of MG. Intriguingly, extraocular symptoms are often asymmetrical [11]. Some patients have isolated ocular symptoms and never develop symptoms in other muscles. Limb weakness is fairly common, usually more proximal than distal and almost always symmet-rical. In some patients, bulbar dysfunction including difficulties in chewing and swallowing are the main symptoms.
Typically, the muscle weakness progresses over the day, due to fatigability in response to repeated muscle use. It also increases in response to exercise, with different time to recovery in different patients, probably depending on both current disease activity and individual differences. The degree of weak-ness also fluctuates over longer time periods, often without identifiable rea-sons.
Myasthenic and cholinergic crises A potentially life-threatening complication of MG is respiratory failure. This may be secondary to an exacerbation of the disease itself (myasthenic crisis) or, to treatment with excessive doses of cholinesterase inhibitors (cholinergic crisis).
Myasthenic crisis is a result of disease exacerbation, the cause of which often remains unknown but sometimes can be caused by insufficient MG med-ication, an infection or adverse effects to other medications. The primary goal of MG management is to achieve an asymptomatic state, but certain attention also must be focused on reducing the risks of developing a myasthenic crisis. According to studies from the 1990’s approximately 15 to 20% of MG patients will experience at least one episode of myasthenic crisis. Since then, the risk seems to have been reduced, although current figures are lacking [55-57]. Late-onset MG, as well as the presence of an additional AD, is associated with a higher risk of myasthenic crisis [58].

20
Cholinergic crisis is a result of overmedication of AChEIs. The overuse of AChEIs though, is often a result of insufficient immune suppression, where persisting neuromuscular dysfunction leads to increased doses of the sympto-matic therapy.
It is often hard to distinguish between myasthenic and cholinergic crisis clinically, since respiratory failure is the dominant symptom and the classical cholinergic symptoms (such as miosis, diarrhea, urinary incontinence, brady-cardia, emesis and excessive salivation) might be less profuse or not even pre-sent. The primary management is, regardless of the cause, to secure airways and sustain adequate breathing. Since the respiratory status can worsen quickly and unpredictably, a patient at risk should be continuously monitored, preferably at the intensive care unit [11, 55-57].
Disease severity Severity of MG could refer to current status as well as worst status ever. To assess current disease severity and objective clinical changes over time the clinical scales of muscular fatigue, preferably myasthenia gravis composite scale (MGC) or quantitative myasthenia gravis test (QMG) are used. Since disease severity can vary markedly between patients within the same subgroup it is sometimes – mainly for research purposes – desirable to further organize the patients in accordance with “the worst disease activity ever”, as a plausible indication of degree of severity. This could be done using the Myasthenia Gravis Foundation of America (MGFA) classification system [59, 60], rang-ing from Class I (no symptoms or isolated ocular symptoms) to Class V (in-tubation, with or without mechanical ventilation). This is a classification sys-tem with quite a high examiner subjectivity component, but which is still widely used and has no existing alternatives.
Other features of MG About 15% of MG patients have polyautoimmunity [61-63]. Especially pa-tients in the EOMG and the ocular subgroups are likely to have a second AD, typically thyroid disease or rheumatoid arthritis [12, 64]. Patients with thy-moma-associated MG are at higher risk to develop hematological autoimmune disorders [12].
The muscle weakness could contribute to an increased risk of respiratory infections and osteoporosis [12].
Mental fatigue, sleep disturbance and cognitive impairment have been re-ported to occur in MG patients more often than expected [65-69]. Possible ACh related effects on the central nervous system are currently a topic of re-search interest [70, 71].
21
MG impact on everyday life The impact of the disease on everyday life varies markedly between individ-uals. These differences can to some extent be attributed to disease severity [72, 73], but there are also differences between patients with a clinically sim-ilar degree of disease. Of course, coping mechanisms and personality can play important roles, but it could be speculated that different subgroup inherencies, including autoantibodies, can contribute to varying atypical or unrecognized symptoms, such as the cognitive impairment described in the previous para-graph.
Diagnosis The diagnosis of MG is based on typical clinical symptoms and the presence of autoantibodies, most commonly directed against the AChR. To evaluate neuromuscular transmission, electrophysiological tests with repetitive nerve stimulation (RNS) and single fiber electromyography (SFEMG) are required. Sometimes a beneficial clinical response to AChEI can further support the diagnosis. Importantly, with typical clinical symptoms, a negative laboratory test does not rule out the diagnosis.
Clinical evaluation In order to facilitate the clinical examination, both for diagnosis and follow-up, scaling instruments are used to evaluate current muscle fatigue. The most commonly applied scales are MGC [74] and QMG [75]. MGC consists of ten items of both anamnestic and examination information. QMG consists of thir-teen items assessing myasthenic features. MGC differs from QMG in that it is a hybrid of physician-reported and patient-reported test items [74], i.e., it takes anamnestic information into account, whereas QMG is strictly based on eval-uation findings. The combination of clinical evaluation and selected anamnes-tic details is especially appropriate as an MG outcome measure since the fluc-tuations in weakness limit the reliability of measuring disease status based on a “snapshot” examination. Furthermore, especially bulbar symptoms are often difficult to assess and might be more evident to the patient [74]. The MGC has been scientifically evaluated and validated and is recommended as “the quan-titative measure for determining improvement and worsening for patients with generalized disease” by the task force of the Medical Scientific Advisory Board (MSAB) of the MGFA 2012 [59].

22
Bedside tests As bedside tests are both less specific and less sensitive than the combinations of clinical evaluation, antibodies and electrophysiology, they are of less value in the common diagnostic procedure and only occasionally used.
Edrophonium test Edrophonium is a short-acting inhibitor of acetylcholinesterase. It prolongs the duration of action of ACh in the NMJ and thereby enhances neuromuscular transmission. The drug is given intravenously, and most MG patients respond with improved muscle strength within a few minutes. The test has shown to be most objective and reliable when improvement is observed in extraocular muscles, especially when ptosis improves [56, 76].
Ice pack test The ice pack test is a non-pharmacological test with no adverse effects. It is performed by placing an ice pack over the closed eye for 2–5 minutes and assessing for improvement in ptosis [56, 77]. The test is of limited diagnostic value as it can only assess improvement of ptosis, but has historically been of some use, for example when the edrophonium test was contraindicated.
Electrophysiological tests
Repetitive Nerve Stimulation Repeated low-frequency electrical stimulation (at a frequency of 3 Hz) of a motor nerve with normal neuromuscular function results in repeated com-pound motor action potentials (CMAPs) with preserved amplitude (and area) from its innervated muscle. This indicates a constant number of activated mus-cle fibers, due to a constant number of responding AChRs. When there is a postsynaptic disturbance of neuromuscular transmission there is a “run down”, also known as decrement, of the amplitude in the CMAP response to the repeated electrical stimulations; simulating exercise fatigue. This is the result of the reduced number of normally functioning AChRs, with a corre-sponding proportion of endplate potentials being reduced to sub threshold level and thereby insufficient to cause a depolarization of the muscle fiber. The most pronounced decrement on RNS is typically measured between the 1st and the 4th CMAP, which are used for assessing neuromuscular transmis-sion failure in MG.
Single fiber electromyography SFEMG [78] is a sensitive method to detect even subclinical defects in neu-romuscular transmission. Recording is typically done during slight muscle contraction, which can be achieved voluntarily or by electrical stimulation. A

23
needle electrode with a very small uptake area is used to record the action potentials (APs) from two muscle fibers innervated by the same axon. One AP is used as a time reference and the variability in the time difference between the two APs is measured. In MG, there is typically increased variability (jitter) between two APs and if this is large enough, blocking of muscle fibers occurs.
Antibody serology Pathogenic antibodies are highly specific for MG [76], and their presence combined with muscle weakness principally confirms the diagnosis.
AChR antibodies The “first-line screening test” for AChR antibodies is performed on a radio-immunoprecipitation assay (RIA) based on a mixture of solubilized embry-onic and adult AChRs. AChR antibodies are highly specific for MG in symp-tomatic individuals [33, 35, 36].
About 70% of all MG patients have detectable antibodies to AChRs, as measured by this method; antibodies are detected in approximately 85% of patients with generalized MG and about 50% of patients with ocular MG [32, 56, 76, 79, 80]. Another 5–10% of all patients can be found to have AChR antibodies if more sensitive, cell-based assays are used [33, 81, 82]. These latter tests, however, are not commercially available.
MuSK antibodies RIA is the most common technique for MuSK antibody detection, although cell-based assays are more sensitive [19, 33, 83]. In AChR- patients with gen-eralized MG about 40% have antibodies to MuSK detected with immunopre-cipitation, whereas 65% are MuSK+ when using cell-based assays. Patients with ocular MG rarely have MuSK antibodies.
LRP4 antibodies As of yet there is no available commercial test for LRP4 antibodies. Analysis is recommended in patients who are AChR-/MuSK- and found in 7–33% of these patients [8, 33, 84].
Thymus radiology Computerized tomography (CT) of the chest should be performed in all pa-tients with AChR+ MG, to explore the possible presence of a thymoma. Usu-ally, all patients are screened out of practical reasons and this inclusive ap-proach could be justified, as AChR+ MG constitutes the majority of patients and the scientific knowledge regarding thymus pathology in other subgroups is sparse. Some also advocate repeated CT scans if a patient with AChR+ MG was not thymectomized [85].

24
Classification, MG subgroups Despite having muscle fatigue in common there are many differences between MG patients. These differences are most evident between patients with differ-ent autoantibodies, but hitherto unexplained variants also occur within sub-groups with similar, or even identical, antibodies. Some examples of differing features are the distribution of weakness, the severity of disease, the propen-sity to exacerbations, the response to different therapies and the co-occurrence of other diseases. A limited range of differences could be expected within a certain disease, but the extent of disparities in MG patients is wide enough to suspect different underlying disease mechanisms, and thereby even different disease entities. To deal with these differences, there have been many attempts to subgroup MG patients. The crucial aim, regardless of subgrouping, is to identify markers of importance to predict disease severity and response to treatment.
MG subgroups There is a fairly well established classification into MG subgroups [12], alt-hough this classification is not uniformly applied. The classification, which is depicted in figure 2, is mainly based on the presence of specific antibodies, age at onset, distribution of weakness and thymus pathology. This approach is not without problems, as the mutual relation between the different subgroup-ing factors does not have an evident hierarchy and a patient could fit into more than one subgroup or change subgroup over time. Still, this is currently the most optimal strategy available. Unfortunately, there is no subgrouping within the ICD-10 system, which complicates registry studies on MG subgroups. As more detailed biochemical knowledge approaches we are becoming more aware of in-depth differences between the patients and the current subgroup-ing will probably eventually have to be adjusted. Figure 3 shows estimates of global prevalence of MG subgroups.

25
Figure 2. Flow chart of classification into MG subgroups.
Early onset MG with AChR antibodies (EOMG) Typically, generalized MG with AChR antibodies shows a bimodal pattern of age at onset, with one peak at around 30 years (early onset MG; EOMG), and a second peak at around 70 years (late onset MG; LOMG). The cut-off be-tween EOMG and LOMG is often arbitrarily set to disease onset before or after the age of 50 years although the age limit varies between studies [12, 32, 85-87].
There is a strong female predominance of about 3:1 in the EOMG subgroup [10, 15]. Thymus pathology often shows thymic hyperplasia [10, 11, 29, 88] and patients respond well to thymectomy [50]. EOMG is strongly associated with the human leukocyte antigen (HLA)-B*08/DRB1*03 and concomitant ADs are overrepresented in the EOMG patients [61, 89] as well as in their first-degree relatives [61]. The distribution of muscle weakness varies be-tween EOMG patients, as does disease severity and there is no described dom-inant phenotype. Juvenile MG (onset before 15 years of age) is considered a subtype of EOMG and its highest prevalence occurs in east Asia [12].
Late onset MG with AChR antibodies (LOMG) In the LOMG subgroup the sex ratio is described to be close to 1, or sometimes with a slight male preponderance [86]. The thymus is usually atrophic [11, 12, 29, 88]. Thymic hyperplasia occurs only rarely and there is no evidence of improvement following thymectomy in this group. Weak associations with HLA-DR2, HLA-B7, and HLA-DRB1*15:01 have been described [90].

26
The distribution of muscle weakness varies between LOMG patients, as does disease severity and there is no described dominating phenotype. LOMG in combination with a second AD increases the risk of an exacerbation [58].
MuSK+ MG MuSK antibody seropositive (MuSK+) MG typically has predominantly facial and bulbar symptoms with neck weakness, speech and swallowing difficulties and sometimes even breathing problems [91-95]. Ocular weakness is thought to be less common than in AChR+ MG, being described in about one third of the MuSK+ patients [92]. Recent data shows that this might be underestimated [96]. Limb weakness is also less frequent [92]. The weakness tends to be more severe than for other subgroups and diurnal fluctuations are not so marked. Muscle atrophy is a frequent feature [85, 95] and typically clinical response to AChEI is not very good [97-100]. The prevalence of MuSK+ MG varies geographically. In Europe there is a higher prevalence in the southern regions and in North America the prevalence is higher in African-Americans [10, 36, 91, 95, 101]. This variation is thought to have genetic rather than environmen-tal background and there is an association with HLA-DQ5 [102, 103]. There is a female predominance and thymus pathology is usually normal [91, 93, 101] which explains why thymectomy shows no beneficial evidence [101].
LRP4+ MG LRP4+ MG was defined only quite recently and is relatively rare, the preva-lence being estimated to 1-5% of all patients with MG. In patients seronega-tive to AChR and MuSK antibodies (AChR-/MuSK-) the frequency of LRP4 antibodies has been described in a wide range from 2 to 50% [12, 84, 104, 105]. Clinically, the muscle weakness is predominantly mild. In about 20% of patients the symptoms are limited to ocular weakness for more than 2 years [84, 104, 105]. Apart from that, the phenotype is not yet thoroughly described [104].
Seronegative MG with generalized symptoms Approximately 10% of MG patients do not have detectable antibodies in standard assays [11]. This can be due to yet unrecognized pathogenic antibod-ies against other postsynaptic membrane antigens than the AChR, MuSK or LRP4. Or, the levels of the antibodies may be below the detection limit. In a clinical setting there are also patients who have antibodies to AChR, MuSK, or LRP4 antigen targets that are only identified by cell-based methods (i.e. not detectable in routine assays) [81, 106, 107] and who are “incorrectly” placed into the seronegative group if not further analyzed. These patients seem to have a similar disease presentation as patients with detectable antibodies against the same antigen [12]. Otherwise the seronegative MG group is clini-cally heterogeneous, with no dominating phenotype depicted.

27
Ocular MG with or without AChR antibodies In 15% of patients the muscle weakness is restricted to the extraocular mus-cles. Diplopia and ptosis are common initial symptoms in MG, but in most patients they are soon accompanied by generalized weakness [12]. About half of the patients with ocular MG (OMG) have AChR antibodies, which are as-sociated with a higher risk to generalize and motivate subdivision of OMG according to antibody presence. If the symptoms remain purely ocular for more than two years – regardless of antibody status – the risk of generalization decreases; a majority of those patients will remain in the OMG subgroup [108, 109]. No age or gender predominance has been shown in OMG [85].
Thymoma-associated MG About 10% of all patients with MG have a thymoma. Thymomas can occur at any age, although the prevalence increases with age. As stated above, practi-cally all patients with a diagnosed MG should undergo imaging of the medi-astinum to evaluate the presence of a potential thymoma. Nearly all patients with thymoma-associated MG have AChR antibodies [12], and quite often also antibodies to muscle antigens such as titin and ryanodine receptor [46]. Thymoma-associated MG is almost always generalized. It should be noted that only about 30% of patients with a thymoma have MG [12, 49].
Figure 3. Estimates of global prevalence of MG subgroups. Modified from Gilhus, N.E., Myasthenia Gravis. N Engl J Med, 2016.

28
Management Treatment protocols for MG are not based purely on results from well con-trolled studies or guidelines based on such studies, because well controlled studies are sparse. Neither do the treatment protocols take into account the variation in therapeutic response among the diagnostic subgroups [12]. As MG is a rare and heterogeneous disease, clinical trials are not easy to do. Cur-rent treatment strategies for MG and MG subgroups are thereby mainly based on experience and traditions.
There is no curative treatment for MG, although most patients respond very well to disease modifying and symptomatic treatment, but the exceptional de-teriorations in disease cannot always be predicted or prevented. The therapeu-tic aim should be to obtain no symptoms, i.e. remission or so called minimal manifestation status [60], as well as to minimize the risks of exacerbations. Most AChR+ patients have positive effects from AChEIs. AChEIs are purely symptomatic and higher doses are often accompanied by intolerable musca-rinic side effects such as abdominal cramps, diarrhea, increased salivation and sweating.
All disease modifying therapies are of immunosuppressive nature. Most commonly corticosteroids are used, but if too high doses are required for maintenance therapy other immunosuppressive drugs are preferred. Azathio-prine, cyclosporine, mycophenolate mofetil and rituximab are suggested in most guidelines [110], but so far MG is not a formal indication for any of them, mainly due to the difficulties of performing clinical trials in rare dis-eases. Thymectomy is another immunosuppressive intervention, which for a long time has been part of the treatment regimen for patients under 60 years of age and positive to AChR antibodies, as well as for patients with thymomas. The beneficial clinical response of thymectomy was recently confirmed in the first ever large-scale prospective multicenter study [50].
Environmental factors Many diseases are thought to be of multifactorial origin. The causative factors could be divided into two major groups – genetic and environmental. Envi-ronmental factors often represent everything that is not considered genetic. The traditional definition of environmental factors that focuses primarily on toxic substances in the surroundings is outdated. The newer approaches define environmental factors more broadly, by encompassing a range of physical and social features in the environment [111].
Environmental factors have impact on a large range of health outcomes [111], i.e., they are not only important for disease causation. For example, they may also affect the disease course, disease experience and response to treat-ment.

29
Among the environmental factors, lifestyle factors have earned a special interest over the last decades because of their strong association to non-com-municable diseases as well as their potentially modifiable nature.
Lifestyle factors and MG Lifestyle factors can be described as “the modifiable habits and ways of life that can greatly influence overall health and well-being”. Commonly ad-dressed lifestyle factors are dietary habits, smoking, physical activity/seden-tary behavior and psychological stress. Many lifestyle factors have proven im-plications on cardiovascular risk factors such as hypertension, being over-weight, hypercholesterolemia and diabetes [112-116].
It is not known whether there are any lifestyle factors affecting the occur-rence or course of MG. One study found smoking more prevalent amongst MG patients, and male LOMG patients had shorter education and more often worked in crafts [117]. These associations were, as of yet, neither confirmed nor disproved in other studies.
However, MG and MG treatment most likely affect lifestyle and cardiovas-cular risk factors. The muscular fatigue could prevent patients from physical activity. A sedentary lifestyle, in combination with corticosteroid treatment, increases the risks of hypertension, being overweight, diabetes and osteopo-rosis.
The treatment of concomitant disease represents a major challenge in pa-tients with MG [11]. Various medications are known to affect MG negatively, e.g., statins, which can increase muscle weakness in some patients [118-120]. For many drugs however, the assumed association with MG deterioration is based on occasional case reports and an association “by chance” is very likely. The possible risk of deterioration though, often makes both patients and care-givers reluctant to use appropriate medications for concomitant diseases.
Physical activity and MG The benefits of physical exercise in healthy individuals are well known [121, 122] and physical inactivity is ranked as one of the top five risk factors for overall mortality globally [123]. These general health benefits could be as-sumed to be valid also for MG patients.
Although muscle fatigue is the cardinal symptom of MG, the tolerance and effects of physical activity in MG are only sparsely studied. There are a few case reports [124-126], some studies on respiratory muscle training [127-130] and one study from 1993 comparing strength training unilaterally to the un-trained contralateral side [131]. One study reported adverse effects on dy-namic spirometry parameters in response to training [127], but only in patients receiving AChEIs. Patients who were not on AChEI had no adverse effects.

30
Very recently a Danish study showed good tolerability to eight weeks of mod-erate to high intensity aerobic or resistance training for MG patients with mild disease [132]. Functional and structural muscular response to exercise in MG patients has not been thoroughly studied.
Despite a well-described neuromuscular disease mechanism, it has been difficult to theoretically predict whether and how physical exercise would af-fect MG disease activity and muscle fatigue in the long run. Besides, the fa-tigue could limit the patients’ ability to perform physical exercise. Tradition-ally, the advice on physical exercise to patients with MG has been very re-strictive or even discouraging [133], mainly out of lack of knowledge.
Importantly, physical exercise is well tolerated and has disease-related pos-itive effects in several chronic diseases. For example, high-intensity resistance training improves fatigue and quality of life in multiple sclerosis [134, 135] and exercise of different kinds reduces systemic inflammation and disease ac-tivity and increases muscle strength in many autoimmune rheumatic diseases [136]. Further, exercise training improves oxidative capacity and skeletal muscle function in chronic obstructive pulmonary disease [137]. Physical ex-ercise has therefore become a cornerstone in the treatment regimens of many diseases and well-established exercise recommendations are increasingly re-quested also for other disorders.

31
Aims
The overall aim of this thesis was to epidemiologically describe MG and MG subgroups in an assumed representative region of Sweden regarding back-ground factors, disease specific factors and factors of possible importance to lifestyle diseases and common health. A second aim was to investigate the habits, tolerability and effects of physical exercise in MG patients.
Specific aims Study I To evaluate clinical and social similarities and differences in MG patients in comparable regions in Estonia and Sweden.
Study II To evaluate disease-specific items in MG subgroups and to illustrate possible differences important for individually tailored care. To compare socio-economic issues, frequency of co-morbidity and patterns of environmental and lifestyle factors between MG patients of different sub-groups and non-MG-diseased population controls.
Study III To evaluate the safety for MG patients to perform physical exercise in accord-ance with general exercise recommendations without deterioration in disease activity.
Study IV To evaluate functional skeletal muscle response to physical exercise in MG patients conducting a 12-week supervised physical exercise program.

32
Methods
Study design Study I a cross-sectional questionnaire-based study on possible clinical
and social similarities and differences in MG patients in Esto-nia and Sweden.
Study II an observational trans-sectional questionnaire-based cohort and case-control study of patients with MG and randomly cho-sen population controls.
Study III a prospective interventional study on the safety of physical ex-ercise in MG patients, where each patient served as his/her own control.
Study IV a prospective interventional study on the skeletal muscle re-sponse to physical exercise in MG patients conducting a 12-week supervised training program. Each patient served as his/her own control.
Ethics The studies were approved by the Regional Ethical Review Board in Linkö-ping, Sweden (study I-III, Dnr 2014/459-31), the Research Ethics Committee of the University of Tartu, Estonia (study I, 245/T-12) and the Regional Ethi-cal Review Board in Uppsala, Sweden (study IV, Dnr 2016/144). All subjects gave written informed consent to participate in the studies.
Subjects All patients included in the studies had a diagnosis of MG according to the MGFA criteria [60] as confirmed by their medical records. According to MGFA MG diagnosis is set if ≥2 of the following criteria are fulfilled: (1) objective clinical fatigue based on neurologist consultation; (2) disturbed neu-romuscular transmission on RNS or SFEMG; and (3) presence of serum anti-bodies against AChRs or MuSK.
Population controls (Study II) were randomly chosen from the Swedish population registry, excluding diagnosed MG patients.

33
Study I-III The Jönköping cohort, studies I-III Patients. All patients with ICD-10 codes G70.0 or G70.9, who were followed at the neurological departments at the hospitals in Jönköping, Eksjö, or Vär-namo during the years 2010–2014, were identified. Of these a total of 70 pa-tients (34 women, mean age 66±16 years) with confirmed MG diagnosis and still living in the region were identified from the medical records, out of which 40 patients (20 women, mean age 64.3±16.2 years) agreed to take part in the questionnaire study, 34 came to a clinical disease evaluation and 13 patients (4 women; 66±13 years) were included in the training study (study III). Controls. In study II, 400 randomly chosen age and gender matched popula-tion controls, excluding MG, were asked to answer the questionnaire. A total of 188 controls (86 women, mean age 63.7±15.3 years) agreed to participate in the questionnaire part of the study. Age and gender did not differ between responders and non-responders (117 women, 96 men, p=0.072, mean age 64.5±16.3 years, p=0.595).
The Tartu cohort, study I The Estonian patient cohort in study I was identified at Tartu University Hos-pital through ICD-10 codes G70.0 or G70.9 over the years 2005 to 2014. A total of 92 alive patients with a confirmed MG diagnosis were identified and 53 (39 women, mean age 59.4 ± 16.9 years) agreed to take part in the study.
Study IV All patients with ICD-10 code G70.0, who were followed at the outpatient Neurology clinic of Uppsala University Hospital in Sweden during the years 2001-2015 were identified. Of these a total of 73 patients with confirmed MG diagnosis and still living in the region were identified from the medical records and 54 patients (29 women, mean age 56±18 years) were found eligible ac-cording to the inclusion criteria (age over 18 years, living <100 kilometers from Uppsala, no current pregnancy or unstable heart disease). Finally, 14 pa-tients (8 women, mean age 57±17) were included in the study.
Data collection Data were largely collected by questionnaires. Information on patients’ cur-rent disease status was also evaluated through clinical and electrophysiologi-cal examinations. Physical fitness and muscle status were assessed by physical performance-based and electrophysiological measures. Anthropometrics and blood sample analyses were accomplished in the exercise studies. A limited amount of patient data was collected from medical records.

34
Medical records. Medical records were studied to confirm MG diagnosis, to extract information on worst MGFA class ever and to check for antibody status, if thymectomy was done and if so, thymus histology.
Questionnaires
Environmental MG questionnaire A self-administered questionnaire, developed, validated and previously ap-plied to MG patients in Norway [117, 138] was translated to Swedish and Estonian and slightly adapted to local circumstances. The questionnaire in-cludes eight main topics: background, education and work, type of income, MG disease-specific issues (only in the patient questionnaire), other diseases, lifestyle, physical activity and hormonal aspects. Of these, certain focus was put on selected parameters, considered to be of particular interest regarding the study objectives.
Quality of life questionnaire The Myasthenia Gravis Quality of Life-15, MGQoL-15, is a 15-item quality-of-life instrument developed and shown to be sensitive for MG [139]. The final score ranges from 0 (good quality of life) to 60 (poor quality of life). MGQoL-15 was sent both to the MG patients and to the population controls.
Fatigue questionnaire Fatigue Severity Scale (FSS) is a questionnaire with nine questions estimating the fatigue severity in different situations during the past week. Grading ranges from 1 (strong disagreement) to 7 (strong agreement) where the final score is the mean value of the nine items, and a score ≥4 is interpreted as fatigue [140].
Questionnaire on physical activity habits The activity level and habits of physical activity was evaluated by a question-naire, developed by the Swedish National Board of Health and Welfare. The questionnaire was recently validated [141] and found to be reasonably accu-rate as compared to the more expensive and time-consuming accelerometer measuring, which nowadays is regarded as standard. The questionnaire con-tains two questions; one on strenuous exercise habits and one on habits of physical activity not regarded as exercise.

35
Physical activity self-assessment The Exercise Self Efficacy Scale (ESES) is a questionnaire consisting of 10 questions (maximum 4 points per question, higher scores indicating higher confidence) regarding self-confidence in performance of physical tasks [142].
Clinical neurological examination. The scaling instruments MGC [74] and QMG [75], described in more detail in the introduction, were used to assess current disease status.
Electrophysiological assessments Compound motor action potential, CMAP Motor nerve stimulation and recordings of CMAP were achieved in the biceps brachii and rectus femoris muscles with Synergy EMG (Viasys Healthcare™) or Key Point Classic (Alpine Biomed; Skovlunde, Denmark). A supramaximal CMAP was obtained, and the amplitude was measured from baseline to neg-ative peak. CMAP amplitudes in proximal muscles have been described higher in individuals who regularly perform high resistance muscle training than in those who do not [143], and can be assumed to measure muscular changes in response to training. Therefore, the CMAP amplitude was used as an outcome measure in the studies on physical exercise (III and IV).
Repetitive nerve stimulation, RNS RNS was performed in the biceps brachii and rectus femoris muscles, as a neurophysiological complement to the clinical evaluation, to assess neuro-muscular transmission failure. RNS at 3 Hz was performed with the recording and stimulating electrode in the same positions as for CMAP. Ten stimuli were delivered, and the decrement was calculated between the first and the fourth CMAP amplitudes. An abnormal decrement was defined as ≥10%.
Isometric muscle force Isometric muscle force was recorded with a hand-held dynamometer (HHD, model 01165; Lafayette Instrument Company, Lafayette®, Ind., USA). Peak force was measured in kg during a 5-second period, repeated three times and the maximum force noted.
Neuromuscular ultrasound As it has been reported that some muscles seem to be thicker in trained indi-viduals than in untrained [144] on neuromuscular ultrasound and since this is a well-tolerated examination method it was chosen to evaluate structural mus-cle changes due to physical exercise in study IV. The thicknesses of the biceps, the rectus femoris and the vastus intermedius muscles were measured with a

36
stationary ultrasound device (LOGIQ S8; GE 17 Healthcare) using a ML6-15 MHz linear array transducer, patients laying supine with extended legs during examination. Measurements were taken at the muscle belly center. To obtain a correct muscle thickness, the transducer was held against the skin with min-imal pressure, with a visible layer of ultrasound gel between the transducer and the skin on the ultrasound image, i.e. the transducer had no direct contact with the skin. The largest measured diameter was recorded. Three consecutive images and measurements were performed, and the mean was calculated.
Physical performance-based measures Timed Up and Go (TUG) [145], Six Minute Walk Test (6MWT), Twelve Mi-nute Walk Test (12MWT) [146], 30-Second Chair Stand Test (30SCST) [147], handgrip strength test (Jamar) and toe-rise endurance test were used to assess physical performance in the studies on physical exercise (III and IV). The tests are considered well established and not further described here.
Physical activity patterns Physical activity patterns were estimated using an accelerometer (DynaPort MoveMonitor, McRoberts, The Hague, The Netherlands) continuously (ex-cept when having a shower/bath) for 7 consecutive days. Especially mean number of steps/24 hours, mean sedentary time/24 hours and mean sedentary time during awake hours were assessed.
Anthropometric measures Height (m) and body weight (kg) were measured, and body mass index (BMI) was calculated. Fat-free mass, skeletal muscle mass and bone mass were as-sessed with the dual-energy x-ray absorptiometry method using the Bioelec-trical Impedance Analysis (Tanita Body Composition Analyzer SC-240 MA, Tanita, Japan).
Blood samples and analysis In patients where antibody status was missing, analysis of AChR antibodies was done and in AChR- patients analysis of antibodies against MuSK was undertaken. Antibody analyses were performed with radioimmunoassay at the department of Immunology, Karolinska Institute, Stockholm, Sweden.
In study III and IV blood samples were collected from each patient before and after the training period and in study III samples were also collected from each patient within 1 hour before and after a single training session (at approx-imately 10 weeks). Serum calcium, phosphate, myoglobin, creatine kinase,

37
CKMB, CRP, IL-6, lactate, myoglobin, creatinine, glucose, HbA1c, choles-terol, HDL, LDL, triglycerides, apolipoprotein A1, apolipoprotein B, parathy-roid hormone, 25-hydroxyvitamin D and antibodies against the AChR were carried out (in somewhat different combinations in the two studies) at the hos-pital laboratories at Ryhov county hospital and Akademiska university hospi-tal respectively.
In study III IL-6 was analyzed with enzyme-linked immunosorbent assay (ELISA) using Human IL-6 SET (hIL-6-EIA-5, MabTag, Germany), follow-ing the manufacturer’s instructions. All samples were assayed in duplicate at an absorbance of 450 nm, and the detection level was 6.1 pg/ml. Intervariabil-ity between IL-6 duplicate readings was 0.002 (median of differences).
Circulating microRNAs RNA isolation and cDNA synthesis were performed (study III) with all RT-qPCR reactions carried out on 384-well Pick-&-Mix microRNA PCR panel plates (Exiqon). The ∆CT value of hemolysis markers [∆CT (hemolysis) = CT (miR-23a-3p) − CT(miR-451a)], was used to detect hemolysis. Quantification of relative miRNA expression of miR-150-5p and miR-21-5p, that are specif-ically elevated in AChRab seropositive MG, was performed with the compar-ative CT method using the formula 2^−∆∆CT, where ∆∆CT=[(CT gene of in-terest−CT reference gene) sample A − (CT gene of interest − CT reference gene) sample B] by using miR-93-5p as the reference gene.
Physical exercise regimen The physical exercise regimen used in both study III and study IV was based on the general exercise recommendations for healthy adults [122] and individ-ually tailored. It was carried through twice a week for twelve weeks. Each exercise session lasted 90 minutes and was supervised by a physiotherapist or a research assistant. Every session consisted of aerobic training on stationary bicycles, muscle resistance exercises mainly targeting proximal limb muscles and trunk, and balance training.
Statistical methods Study I and II. Student t test was used for parametric data and Mann–Whitney U test was used for nonparametric data, when analyzing continuous variables in the com-parisons between MG cohorts and MG subgroups. Fisher’s exact test was used

38
to evaluate differences in categorical data if the sample was small and ex-pected values were less than 5, otherwise Chi-square test was used.
In the case-control analysis conditional logistic regression was used to es-timate the adjusted odds ratios (AORs) and confidence intervals of possible associations between MG or MG subgroups and the different variables meas-ured for. Stratification was used to adjust for the different number of controls.
Statistical analysis was performed with Graph Pad Prism and SPSS soft-ware. A P-value < 0.05 was considered significant.
Study III and IV. Parametric data from electrophysiological and laboratory parameters were presented as mean ± SD and non-parametric clinical scores were presented as median ± IQR. Wilcoxon signed-rank test was used to compare nonparametric data before and after the training in each patient. The statistical analysis was performed with the Graph Pad Prism software. A P-value < 0.05 was consid-ered significant.

39
Results
Study I Differences and similarities between MG patients in Tartu and Jönköping regions. Demographics and subgroups MG prevalence rate in Tartu area was 235 per million and in Jönköping county 203 per million. Participation rates were 39% in Tartu and 57% in Jönköping. Age at participation did not differ (Tartu: 60.9±18.3 years, Jönköping: 64.3±16.2 years, p=0.39). Overall female to male ratio was 2:1 in Tartu and 1:1 in Jönköping. Gender ratios in the subgroups were more marked in Jönkö-ping, with a female to male ratio of 8.5:1 in EOMG and 1:5.3 in LOMG. In Tartu the female to male ratio was 4:1 in EOMG and 1.3:1 in LOMG.
Age at disease onset was similar in the regions (Tartu: 52.8 ± 18.8 years, Jönköping: 49.5 ± 22.1 years, p=0.22).
85% of the Swedish patients and 72% of the Estonian patients were AChR+, none were MuSK+. As shown in table 1 factors of importance to subgrouping were similar in the two regions.
Table 1. Distribution of age at onset, phenotype-based subdivision and antibody sta-tus among MG patients in Estonia and Sweden.
TARTU JÖNKÖPING p-value
Age at onset, N (%) Juvenile MG 0 2 (5.3) 0.49 EOMG 15 (42.9) 16 (44.4) >0.99 LOMG 20 (57.1) 20 (55.6) 0.88 Phenotype, N (%) Generalized 29 (80.6) 31 (79.5) >0.99 Pure bulbar 3 (8.3) 2 (5.1) 0.67 Pure ocular 4 (11.1) 6 (15) 0.74 Antibody serology, N (%) AChR+ 23 (71.9) 34 (85) 0.06 MuSK+ 0 0 AChR-/MuSK- 9 (28.1) 6 (15) 0.42 Missing antibodies 4 (11.1) <0.05* Thymoma MG, N (%) 2 (5.5) 4 (10) 0.77

40
Clinical evaluation and symptoms At clinical evaluation the QMG score did not differ between the two regions (5.0±3.7 in Estonia and 5.4±4.4 in Sweden, p=0.68). Still, significantly more Estonian patients reported current chewing difficulties (32.4%; 11 patients vs. 10.3%; 4 patients, p = 0.02) and arm weakness (61.8%; 21 patients vs. 38.5%; 15 patients, p < 0.05). The proportion of patients reporting no myasthenic symptoms during the last three months was significantly higher in Sweden (23.1%; 9 patients vs. 8.6%; 3 patients, p = 0.09). On a 10-point-scale, Esto-nian patients scored their current subjective disease severity higher (5.6 ± 2.8) compared to the Swedish patients (3.4±2.3, p=0.0005) and they had higher FSS scores (5.0 ± 1.7 vs 3.5 ± 1.6; p = 0.001).
Treatment Treatment regimens differed in that Estonian patients tended to have higher daily doses of AChEI (367 ± 199 mg vs. 231 ± 161 mg, p = 0.007), fewer were on corticosteroids (22.9% vs. 38.5%, p = 0.15) and more were on azathioprine (p = 0.04) as compared to Swedish patients. Thymectomy had been performed to similar frequencies.
Physical activity The Swedish patients reported to be more active, both regarding more strenu-ous and somewhat lighter types of physical activity. As an example of this 71.9% of Estonian patients did not perform physical exercise training at all compared to 25.8% of Swedish patients (p=0.004).
Concomitant diseases There was a higher number of patients with autoimmune thyroiditis among the Estonian patients (28.6% vs. 8.8%, p=0.04).

41
Study II Lifestyle factors and gender-related differences of MG subgroups in southern Sweden.
The MG cohort
Subgroups 34 patients were AChR+, none were MuSK+ and 6 were AChR-/MuSK-. De-tailed subgrouping is shown in figure 4. When patients, for practical reasons, were divided into only three subgroups the proportions were adjusted as fol-lows: EOMG 42.5%, LOMG 45% and thymoma 12.5%. Subgroup character-istics are shown in table 2.
Figure 4. Distribution of MG subgroups in Jönköping county 2015.
Gender and age There was a marked gender difference between the EOMG (female: male, 15:2) and LOMG (female:male, 3:15) subgroups (p<0.0001). Within the EOMG subgroup mean age at disease onset was 24±9 years and within the LOMG subgroup it was 72±8 years. Age at disease onset was significantly lower for women (32.9±20.8 years) than for men (61.8±14.1 years, p<0.0001). Age at disease onset, time from initial symptoms to diagnosis and age and disease duration at participation are shown in table 2. Time to diagnosis was significantly longer in EOMG than in LOMG patients (4.5±7.5 vs 0.9±1.7 years, p=0.0386).

42
Figure 5. Distribution of age at disease onset for women (n=20) and men (n=19).
The distribution of age at disease onset is illustrated in figure 5. The marked skewed distribution of gender and age within the subgroups implicated strati-fication limitations. Because of this, further comparisons between subgroups were not applicable in parameters where age and gender could be suspected to have a large influence.
43
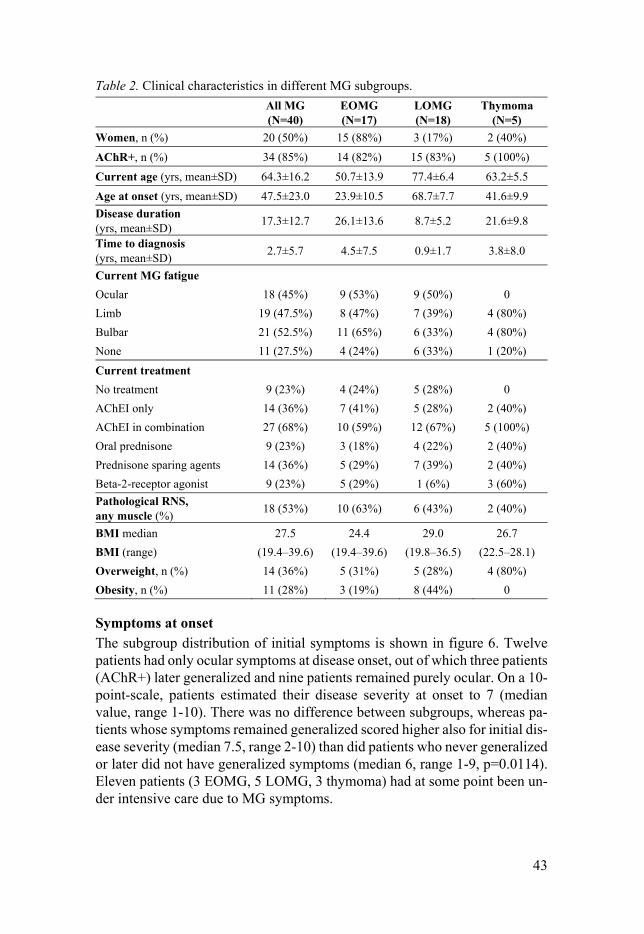
Table 2. Clinical characteristics in different MG subgroups.
All MG (N=40)
EOMG (N=17)
LOMG (N=18)
Thymoma (N=5)
Women, n (%) 20 (50%) 15 (88%) 3 (17%) 2 (40%)
AChR+, n (%) 34 (85%) 14 (82%) 15 (83%) 5 (100%)
Current age (yrs, mean±SD) 64.3±16.2 50.7±13.9 77.4±6.4 63.2±5.5
Age at onset (yrs, mean±SD) 47.5±23.0 23.9±10.5 68.7±7.7 41.6±9.9
Disease duration (yrs, mean±SD)
17.3±12.7 26.1±13.6 8.7±5.2 21.6±9.8
Time to diagnosis (yrs, mean±SD)
2.7±5.7 4.5±7.5 0.9±1.7 3.8±8.0
Current MG fatigue
Ocular 18 (45%) 9 (53%) 9 (50%) 0
Limb 19 (47.5%) 8 (47%) 7 (39%) 4 (80%)
Bulbar 21 (52.5%) 11 (65%) 6 (33%) 4 (80%)
None 11 (27.5%) 4 (24%) 6 (33%) 1 (20%)
Current treatment
No treatment 9 (23%) 4 (24%) 5 (28%) 0
AChEI only 14 (36%) 7 (41%) 5 (28%) 2 (40%)
AChEI in combination 27 (68%) 10 (59%) 12 (67%) 5 (100%)
Oral prednisone 9 (23%) 3 (18%) 4 (22%) 2 (40%)
Prednisone sparing agents 14 (36%) 5 (29%) 7 (39%) 2 (40%)
Beta-2-receptor agonist 9 (23%) 5 (29%) 1 (6%) 3 (60%)
Pathological RNS, any muscle (%)
18 (53%) 10 (63%) 6 (43%) 2 (40%)
BMI median 27.5 24.4 29.0 26.7
BMI (range) (19.4–39.6) (19.4–39.6) (19.8–36.5) (22.5–28.1)
Overweight, n (%) 14 (36%) 5 (31%) 5 (28%) 4 (80%)
Obesity, n (%) 11 (28%) 3 (19%) 8 (44%) 0
Symptoms at onset The subgroup distribution of initial symptoms is shown in figure 6. Twelve patients had only ocular symptoms at disease onset, out of which three patients (AChR+) later generalized and nine patients remained purely ocular. On a 10-point-scale, patients estimated their disease severity at onset to 7 (median value, range 1-10). There was no difference between subgroups, whereas pa-tients whose symptoms remained generalized scored higher also for initial dis-ease severity (median 7.5, range 2-10) than did patients who never generalized or later did not have generalized symptoms (median 6, range 1-9, p=0.0114). Eleven patients (3 EOMG, 5 LOMG, 3 thymoma) had at some point been un-der intensive care due to MG symptoms.

44
Current symptoms The subgroup distribution of current symptoms is shown in figure 7. Eleven patients reported no MG symptoms at all during the last 3 months, four of whom previously had only ocular symptoms. On the 10-point scale patients estimated their current disease severity as 3 (median value, range 1-9), with no difference between subgroups. Patients with current generalized symptoms scored higher (median 4, range 1-9) than patients with purely ocular symptoms (median 2, range 1-4, p=0.0187).
Figure 6. Distribution of initial symptoms in MG subgroups.
Figure 7. Distribution of current symptoms in MG subgroups.

45
Clinical evaluation Median MGC for all patients was 5 (range 0-17). EOMG patients had signif-icantly higher MGC (median 7, range 1-17) than did LOMG patients (median 3, range 0-15; p=0.0448). Median MGC for thymoma patients was 9 (range 5-13), which did not significantly differ from EOMG (p=0.566) or LOMG (p=0.137). Median peak expiratory flow (PEF) value for all MG patients was 350 (range 190-630), with no difference between EOMG and LOMG.
Treatment As could be expected, all patients had been treated with AChEI at some point during their disease. Other medications prescribed at some time were predni-sone (38%), azathioprine (36%) and cyclosporine (8%). Current treatment is shown in table 2. There was no significant difference in current treatment be-tween the different subgroups.
Nineteen patients were thymectomized, with significantly higher ratios in the EOMG (12 patients, p=0.0005) and thymoma (5 patients, p=0.0006) than in the LOMG (2 patients) subgroups.
Factors influencing or influenced by disease Psychological stress (44%), physical stress (36%) and infections (36%) were the three most frequently reported factors perceived to influence disease ac-tivity. EOMG patients, and to some extent patients in the thymoma subgroup, were more prone to report external factor impacts on disease activity.
MG as a disease was reported to influence the choice of profession in 4 (10%) patients. Another three (7.5%) patients had had to change their occupa-tion and 7 (17.5%) had had to discontinue working due to MG symptoms.
MG-QoL-15 and FSS EOMG patients scored similarly to LOMG patients on the MGQoL-15 ques-tionnaire (median 9.5 versus median 7; p=0.563). Patients with current gener-alized MG scored higher on MGQoL-15 (median 15.5, range 0-42) than pa-tients with no current generalized symptoms (median 1.5, range 0-11; p<0.0001).
Sixty-seven percent of the EOMG patients, 62% of the LOMG patients and all of the thymoma patients answering the FSS questionnaire scored ≥4, i.e., reached the fatigue limit. Patients with current generalized symptoms were significantly more likely to suffer from fatigue (OR 7.0, p=0.0450). When an-alyzing the lowest scoring quartile (≤1.9; n=7) and the highest scoring quartile (>4.9, n=7) EOMG patients had a significantly higher risk of worse FSS (OR 23.8, p=0.0069).

46
Comparisons to the control group As the cases and controls were matched, there were no differences in age and gender between the MG and control groups. AORs for the approached varia-bles in the comparison between the whole MG group and the matched controls are shown in table 3.
Background Fifteen percent of the MG patients and 9% of the controls were born outside of Sweden. The majority of both patients and controls spent their childhood in Sweden. Current civil status was similar between the groups and there was no difference in having children or not.
Twenty-eight percent of the MG patients (39% of EOMG, 18% of LOMG and 20% of thymoma patients) had completed post-secondary school as com-pared to 39% of the controls. Ordinary school was the highest educational level for 49% of the MG patients (28% of EOMG, 71% of LOMG and 40% of thymoma patients) and for 39% of the controls. There was no significant difference in highest educational level.
There was no significant difference in occupation between MG patients and controls. For the LOMG group there was a tendency toward higher represen-tation in occupations of mainly manual labor work, as compared to matched controls (OR 2.82, 95% CI 0.87-9.12, p=0.083). Nine of the MG patients (6 EOMG and 3 thymoma) and eleven of the controls had received sickness ben-efits during the last year. There were significantly higher AORs for being on sickness leave (OR 8.0, 95% CI 1.3-47.1, p=0.021; Table 2), as well as receiv-ing sickness benefits (OR 10.1, 95% CI 1.9-52.8, p=0.006) in the EOMG group.
Concomitant diseases MG patients reported mental health problems more often than the population controls, (OR 2.9, 95% CI 1.1-7.4, p=0.024). This was most pronounced in the LOMG group (OR 5.9, 95% CI 2.0-17.1, p=0.001). There were no differ-ences in any other lifestyle related disease. MG patients were receiving anti-depressants more often than controls (OR 7.91, p=0.008).
More first-degree relatives of MG patients than of controls were reported to have thyroid disease (OR 5.7, 95% CI 1.9-17.0, p=0.002).
Lifestyle factors There were no significant differences in smoking habits, although there was a tendency towards a higher degree of smoking in the LOMG group than in controls (OR 4.1, 95% CI 0.8-20.7, p=0.086). There was no difference in smoking habits between EOMG patients and the control group. In the LOMG group there was an AOR of 13.7 (95% CI 1.7-112.9, p=0.015) toward obesity

47
(BMI≥30). There were no differences regarding being overweight (BMI 25-29.9 kg/m2).
MG patients, especially LOMG patients, were eating fish significantly less frequently compared to controls (table 3, LOMG vs control: OR 4.10, 95% CI 1.37-12.32, p=0.012). There were no significant differences in coffee or tea drinking, vitamin D supplementation, sun reactions and sun exposure habits or vaccination patterns.
Table 3. Adjusted risks of work absence, life-style diseases, life-style habits and physical inactivity in MG patients compared to matched non-MG controls.
All MG n (%)
Non-MG n (%) AOR; 95% CI
Work related features Sickness leave 4 (10%) 7 (4%) 6.00 (1.33-27.0)* Sickness benefit 9 (23%) 11 (6%) 9.18 (2.38-35.3)* Lifestyle diseases Mental health problems 8 (24%) 19 (11%) 2.92 (1.15-7.44)* Antidepressant treatment 4 (10%) 4 (2%) 7.91 (1.70-36.83)* Diabetes type I 1 (3%) 5 (3%) 0.85 (0.08-8.65) Diabetes type II 1 (3%) 18 (10%) 0.27 (0.03-2.16) Hypertension 8 (24%) 65 (36%) 0.47 (0.,19-1.19) Hypercholesterolemia 5 (15%) 33 (18%) 0.60 (0.18-2.00) Overweight 1 (3%) 18 (10%) 0.25 (0.03-1.99) Obesity 25 (64%) 104 (57%) 1.23 (0.58-2.58) Lifestyle habits Current smoking 6 (15%) 14 (7%) 2.14 (0.78-5.88) Eating fish less than once a week 20 (53%) 68 (37%) 2.28 (1.06-4.90)* Physical inactivity No strenuous physical exercise 22 (69%) 57 (44%) 2.36 (1.01-5.50)* No strength training 23 (85%) 63 (62%) 3.67 (1.12-12.02)* No aerobic exercise 19 (70%) 53 (51%) 2.10 (0.83-5.30)
* p<0.05.
Physical inactivity MG patients were less likely to do focused physical activity than controls, especially with regard to more strenuous activity and strength training.
Quality of Life MG patients scored higher on MGQoL-15 (median 8, range 0-42) than did
the controls (median 1, range 0-43), p<0.0001.

48
Study III The safety of physical exercise in MG. Subjects Of the thirteen MG patients included, ten (4 women; 65±14 years) completed the training program. None of the three patients terminating the training pro-gram prematurely did so because of deterioration in disease. Participation rate ranged from 71 to 95% over the 12-week-training-period. Clinical character-istics of the patients are presented in table 4.
Table 4. Patient characteristics, study III.
MGC score
No. Gen-der, age
Disease dura-tion (yr)
MG sub-
group
Anti-body sta-
tus
MGFA class B
efor
e
6 w
eeks
Aft
er
Medication
1 M, 59 23 EOMG AChR+ II b 2 0 0 CH, PR, IM(c), SPT
2 W, 57 34 EOMG AChR+ II a 7 7 5 CH, PR, IM(c,r), SPT*
3 M, 73 4 LOMG AChR+ I 4 5 4 NT 4 M, 75 8 LOMG AChR+ I 0 0 0 IM(a) 5 W, 73 40 EOMG AChR- I 6 4 4 CH, IVIG 6 W, 66 27 EOMG AChR- II b 4 11 8 CH, PR 7 M, 86 10 LOMG AChR+ II b 1 4 3 IM(a) 8 W, 34 5 EOMG AChR+ II a 5 7 4 CH, IM(r), SPT 9 M, 56 29 EOMG AChR+ II a 9 0 2 PR, IM(r), SPT 10 M, 69 11 LOMG AChR+ I 5 2 0 CH, PR M, man; W, woman; EOMG, early onset MG; LOMG, late onset MG; AChR+, acetylcholine receptor antibody seropositive; AChR-, acetylcholine receptor antibody seronegative; NT, no therapy; SPT, status post thymectomy; CH, cholinesterase inhibitors; PR, corticosteroids; IM, immunosuppressive therapy other than corticosteroids (specified as a, azathioprine; c, cyclo-sporine; r, rituximab); IVIG, intravenous immunoglobulins.*Patient #2 was also treated for RA.
Baseline At baseline the number of steps per day ranged from 2839 to 16743 (median: 7873 steps/day, mean±SD: 8025±4069 steps/day) and median sedentary time was 18 hours/day, ranging from 16 to 21 hours/day. Six patients reported al-most no active strenuous training, whereas four patients devoted 30-60 minutes to strenuous training during a typical week. ESES scores ranged from 25 to 38 (median 29.5). Median BMI was 27.6 (range 21.3-36.0).

49
Tolerance to exercise Physical exercise was well tolerated, as measured by unchanged MGC score, median was before start 4.5 (range 0-9) and after fulfilled program 3.5 (range 0-8) (p=0.25).
Physical performance measures
Figure 8. Muscle resistance weights and CMAP amplitudes increased significantly for the biceps brachii and the rectus femoris muscles after the training period, as compared to baseline.
Figure 9. 6MWT and 30SCST improved significantly after the training intervention.
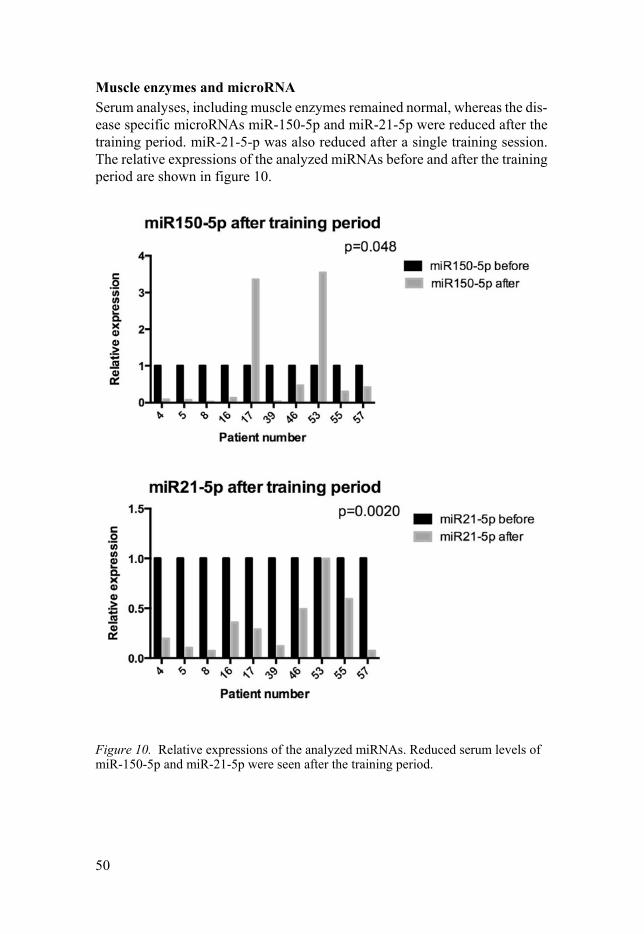
50
Muscle enzymes and microRNA Serum analyses, including muscle enzymes remained normal, whereas the dis-ease specific microRNAs miR-150-5p and miR-21-5p were reduced after the training period. miR-21-5-p was also reduced after a single training session. The relative expressions of the analyzed miRNAs before and after the training period are shown in figure 10.
Figure 10. Relative expressions of the analyzed miRNAs. Reduced serum levels of miR-150-5p and miR-21-5p were seen after the training period.

51
Study IV Muscular effects of physical exercise in MG patients. Subjects Eleven patients (6 women; 60±18 years) completed the training program. Three patients discontinued the study, two due to lack of time and one due to work related health problems. None of them showed any signs of clinical de-terioration (according to MGC and QMG) or described other uneasiness with regards to the training regimen. Participation rate ranged from 75 to 96% over the 12-week-training-period. Clinical characteristics of the patients are pre-sented in table 5.
Table 5. Patient characteristics, study IV.
MGC QMG CH dose mg/24 h
# Gen-der, age
MG dur (yrs)
Worst MGFA class
MGFA -PIS
Bef
ore
Aft
er
Bef
ore
Aft
er
Medications
Bef
ore
Aft
er
1 M60 10 I MM-3 3 0 3 1 CH, PR, Aza 180 0 2 F70 11 III b MM-3 4 2 2 1 Aza, SPT 0 0 3 M83 17 I MM-0 5 5 0 0 NT 0 0 4 F28 6 II b MM-1 0 0 0 0 PR, SPT 0 0 5 F30 14 IV a I 1 0 3 1 CH, PR, Aza 480 120 6 M75 33 III a I 5 2 3 2 PR, SPT 0 0 7 F70 4 III a I 7 2 6 1 CH, PR 240 240 8 F65 35 II b MM-3 3 4 1 2 CH, SPT 180 180
9 M72 3 III b MM-2 2 3 0 3 CH, PR, Aza, SPT 60 60
10 F57 14 III a I 9 7 6 1 CH, PR, SPT 60 0 11 M54 31 II a MM 3 2 3 3 SPT 0 0 MGFA Class, Myasthenia Gravis Foundation of America clinical classification; MGFA-PIS, Myasthenia Gravis Foundation of America Post-intervention Status before the exercise regi-men, MM. minimal manifestations; MM-0, no treatment for ≥1 year; MM-1, immunosuppres-sion; MM-2, only low dose CH for ≥1 year; MM-3, I, improved; CH and immunosuppression for ≥1 year; MGC, MG composite scale; QMG, Quantitative MG score; NT, no therapy; SPT, Status post thymectomy; CH, cholinesterase inhibitors; PR, corticosteroids; Aza, azathioprine; IVIG, intravenous immunoglobulins.
Baseline Before start of the training period, the median number of steps per day was 8801 (IQR 6746-9723) and the median sedentary time was 18.8 hours/24 hours (IQR 16.7-19.4). When rated only for waking hours, the median seden-tary time was 10.0 hours/day (IQR 9.0-10.9). Self-reported time devoted to strenuous exercise during a typical week ranged from 0 to >120 minutes a week (median: <30 minutes a week) and self-reported time devoted to physi-cal-activity-not-regarded-as-exercise during a typical week ranged from <30 minutes a week to >300 minutes a week (median: 150-300 minutes a week).

52
When compared to suggested risk levels of insufficient physical activity 1 pa-tient were at risk considering number of steps/day (<7000), and 4 patients were at risk considering self-reported physical activity (<150 minutes of mod-erate activity per week).
Tolerance to exercise Physical exercise was well tolerated by the MG patients, as measured by a slight decrease of -1 in MGC (range -5 to +1, p=0.0430) after the training period and no change in QMG. Individual MGC and QMG scores are shown in table 5.
Muscle function and muscle thickness As shown in figure 11, the CMAP amplitude increased significantly after the training period in the quadriceps muscle (4.5 ± 2.6 vs 5.3 ± 2.8 mV; p=0.016), but not in the biceps brachii muscle (5.5 ± 2.1 vs 4.6 ± 1.3mV; p=0.63).
Neuromuscular ultrasound showed significant increase in muscle thickness for both the rectus femoris (19.6 ± 5.6 vs 23.0 ± 3.9 mm; p=0.0098) and the vastus intermedius (18.0 ± 5.8 vs 22.0 ± 6.2 mm p=0.034) muscles. There was no significant change in the biceps brachii muscle (33.3 ± 6.5 versus 32.1 ± 6.2 mm; p=0.11).
Isometric muscle force (HHD) increased significantly in the quadriceps muscle (25.2 ± 4.4 versus 30.2 ± 3.8 kg; p=0.014), but not in the biceps brachii muscle (21.0 ± 6.0 versus 21.9 ± 5.6 kg; p=0.58).
Physical performance 30SCST improved significantly (median change +2, p=0.0039). TUG, 12MWT and Jamar remained unchanged (p>0.05 for all).
Serum analyses and anthropometrics Apolipoprotein A1 increased significantly (from 1.7 ± 0.3 to 1.9 ± 0.4 g/L, p=0.039). Plasma 25-hydroxyvitamin D decreased significantly (70.2 ± 11.0 versus 62.1 ± 12.5 nmol/L; p=0.032). There was a tendency for lowered long-time glucose (HbA1C) from 37.8 ± 6.5 to 36.2 ± 6.7 mmol/mol (p=0.078). No other significant changes were found in the serum analyses.
Blood pressure, pulse at rest, body weight, BMI and body composition var-iables (fat free mass, skeletal muscle mass, body mass) did not change signif-icantly.
Quality of life, fatigue and ESES MGQoL-15, showed a tendency towards higher scores and thus improved
quality of life, although this change was not significant (5 [4-11] versus 8 [6-11]; p>0.05). There were no significant changes in fatigue score with FSS (3.1 [2.3-3.6] versus 2.8 [1.6-4.4]; p>0.05) or ESES (33 [28-38] versus 30 [20-36; p>0.05).

53
Figure 11. Change in muscle parameters and clinical muscle fatigue after the train-ing period in Study IV.

54
Discussion
In this thesis MG epidemiology was evaluated in two regions, one in Sweden and one in Estonia. The results were related to what has been reviewed world-wide. In the Swedish cohort a certain focus was also directed at the distribution of MG subgroups and subgroup differences regarding disease characteristics, as well as co-occurrence of chronic non-communicable diseases and lifestyle related risk factors. Further, the safety and effects of physical activity in MG patients were investigated.
Epidemiological considerations In rare, heterogeneous disorders like MG, there is a need to combine or com-pare epidemiological findings from different regions and the need for stand-ardized epidemiological approaches is evident. It is also necessary to conduct epidemiological studies regionally to raise awareness of possible local differ-ences and knowledge on how to best implement results from studies in other regions. In study I and II we used a questionnaire which was previously vali-dated and applied to MG patients in Norway [138]. Except for drawbacks gen-erally related to questionnaires, such as traditional recall and participation bi-ases, there are some other considerations with regard to these studies. Alt-hough the questionnaire was considered suitable for both Swedish and Esto-nian patients (after smaller adjustments), there could be cultural differences in responses to questionnaires, for example regarding when subjects choose not to leave an answer at all. These differences might have affected our results, for instance due to different amounts of, and reasons for, missing data in the two regions. It could be argued that questionnaires should be separately vali-dated in every new cultural region where they are used, but such an approach is not always practical, and it is not at all obvious where and how to draw the borders of such regions. Another drawback of the studies is the lack of an internet-based response alternative, which could have increased the number of participants, perhaps especially in the younger age groups. As for the sub-grouping, the fairly low number of participants is a disadvantage since the subgroups of interest became very small. This in turn caused limitations in comparison both between the subgroups and to the matched controls. Still, our results must be regarded important regionally, as they describe a majority of

55
MG patients in the addressed areas. They could also serve as interesting ob-servations: small contributions to the large puzzle of MG epidemiology and as an encouragement for further research in larger populations.
Comparison between different geographical regions Prevalence, distribution of subgroups and gender The overall prevalence of MG was similar in Tartu and Jönköping and fell within the wide range of MG prevalence described worldwide [10, 11]. Our chosen data collection unfortunately didn’t allow incidence calculation.
Subgroup distribution, when limited to EOMG, LOMG and thymoma, did not differ between the two regions.
The gender distribution in the EOMG and LOMG subgroups differed largely between Tartu and Jönköping. In the Tartu cohort the gender distribu-tion in the subgroups was similar to worldwide figures, although there was a slight female predominance also in the LOMG group. In the Jönköping cohort there was a more marked gender difference both in the EOMG and the LOMG subgroups. The female to male ratio of 15:2 in the EOMG group was higher than expected according to existing literature [10-12]. Even more salient was the male predominance of 15:3 in the LOMG subgroup. If this would not be the true distribution, one could assume that it might be due to underdiagnosis of LOMG among women in this region.
Symptoms, perceived health, clinical status and treatment Although the distribution of symptoms and disease severity were similar at onset, current symptoms differed in that Estonian patients reported more upper limb weakness, more chewing difficulties and a higher self-estimated disease severity. In accordance, more Swedish patients were asymptomatic during the last three months. The perceived health satisfaction was significantly lower and fatigue severity scores were higher among the Estonian patients, although objective MG status was comparable to the Swedish patients. The rate of im-munosuppressive treatment was similar, whereas Estonian patients were on higher doses of AChEI. Also, a higher percentage of the Estonian patients were physically inactive. There are different possible, although unproven ex-planations for these differences. There could be a difference in how disease is perceived in general between the two countries, possibly linked to the higher prevalence of depression in Estonia [148] or to a more insecure healthcare and benefit system [149-151]. Self-rated health has been the poorest in the former Soviet Union and a strong correlation with economic status exists [152, 153]. It is intriguing that Estonian patients were on higher doses of AChEI, as too high doses paradoxically can increase symptomatic fatigue, which in turn can

56
be misinterpreted as myasthenic weakness and lead to even higher doses of AChEI. Still, one must remember that similar clinical status does not neces-sarily mean similar disease activity, as the treatment might differ. Anyhow, similar status in combination with more poorly perceived symptoms and higher doses of AChEI being the only treatment difference implies a possible need for additional immunosuppressive treatment.
Comparisons between different subgroups Knowledge about differences and similarities between MG subgroups is of importance to make clinicians aware of disease-associated features that need to be focused on to individualize and optimize the care of MG patients. It is inevitable though, that studies on these differences often have to deal with the low subgroup prevalence and that the participation numbers often are insuffi-cient to draw any convincing conclusions. For the same reasons it is not pos-sible to stratify the groups and direct comparisons between subgroups are largely prohibited by the marked age and gender differences. With emerging biochemical knowledge, it could be argued that the subgroups are completely different diseases, where direct comparisons are illogical except for pheno-types, which – like in all differential diagnostics – are valuable clinical clues to inform the choice of further investigations.
Distribution of subgroups, age and gender Detailed subgroup distribution in Jönköping county differed from what is de-scribed worldwide, which could be due to the small number of participants, but probably also has genetic and environmental explanations which would be useful to identify. This was not, however, within the scope of the current stud-ies.
The age differences are not of phenotypic interest, as age is used as part of the subgrouping strategy. Gender differences between the EOMG and LOMG subgroups were striking, as described above. This must be kept in mind when discussing further differences between the groups.
Time to diagnosis, clinical picture and status Time to diagnosis was longer in EOMG patients and, to our knowledge this has not been described previously. In this study we were unable to identify the reason for this; both patient’s and doctor’s delay could contribute. It could be speculated that younger people tolerate disease symptoms longer before seek-ing medical care, but another plausible cause is that fatigue symptoms among women are more often misinterpreted.

57
EOMG patients had higher MGC scores at the clinical evaluation than did LOMG patients. This was unexpected, since EOMG patients as a group are usually depicted as having a slower disease course after the first 2-3 years, and the EOMG disease duration in our study was much longer (26±13 years). Un-like QMG, MGC also takes into account reported bulbar symptoms, which was the most frequent current symptom reported by 65% of the EOMG pa-tients (as compared to 32% of the LOMG patients) in the questionnaire. MGC, that is validated and now recommended for both clinical and research pur-poses [59, 74], was developed later than QMG, and many earlier studies are based on QMG. Therefore, previous studies might not have recognized the bulbar symptoms due to the lack of reliable objective clinical test maneuvers for these muscles.
As could be expected, patients with current generalized symptoms rated their disease severity higher and they scored lower on MGQoL and FSS, than did patients with purely ocular symptoms. This justifies the treatment goal aimed at minimizing symptoms, i.e., not to settle for “only” a substantial im-provement.
Treatment As already stated, immunosuppressive and symptomatic treatment should be tailored individually according to antibody subtype, age (EOMG versus LOMG), symptoms, etc. The strategies for this are as of yet not clearly out-lined [87, 110] and our findings that there were no differences in treatment between subgroups, underline the need for further subgroup characterization as well as the need to spread knowledge to individualize and optimize MG treatment in the clinical setting.
Comparisons to matched population controls Comparisons to age and gender matched population controls are often done to identify disease causative factors. When evaluating the co-occurrence and management of highly prevalent diseases in patients with an underlying low-prevalence disease like MG this approach could also be of use, as depicted below.
Occurrence and management of high-prevalence disorders in patients with a low-prevalence disease High-prevalence diseases, such as many chronic non-communicable diseases, are often related to lifestyle and thereby offer an important opportunity for

58
primary prevention. Secondary prevention of many of these diseases is also quite well established.
Individuals who suffer from low-prevalence diseases are not exempted from having lifestyle related diseases. In the case of covariant risk factors, medication side effects and disability the occurrence could possibly be even higher than in the overall population. Pending improved scientific knowledge, it is reasonable to assume that individuals with low-prevalence diseases are at least at the same risk as others to develop lifestyle diseases.
Considering the risk in MG to trigger a life-threatening deterioration, it is reasonable to be cautious with medications and other measures of unknown effect on the underlying disease. Notwithstanding, to withhold a well-docu-mented preventive measure could also be regarded as unequal care. Further, the demand on the individual physician to foresee which is the most favorable management is unreasonable when scientific data are lacking. The trend has traditionally been to prefer the restrictive path, i.e., what “not to do” has been thought to be less harmful. With improving knowledge of pronounced bene-ficial effects of primary preventive measures this is no longer considered a sufficient approach.
The occurrence and possible risk profiles of chronic non-communicable diseases in MG, as well as the safety of implementing preventive measures to lifestyle disorders in MG patients was addressed in this thesis. Again, as the number of participants in each subgroup is low, no thorough conclusions can be made. Still, pilot data on higher risk individuals for some life style disorders warrant follow up in larger scale studies both for further validation and to gain evidence on how to deal with these issues in clinical practice.
Lifestyle factors Obesity, low fish consumption, smoking, lower educational level, manual la-bor occupations and low rates of physical activity were all seen to some extent in the LOMG subgroup. Similar findings regarding education and occupation were reported in a previous Norwegian study [117] and regardless of the rea-son for the higher presence of these risk factors, it is of importance to evaluate and approach them in the clinical setting. Concerning the low fish consump-tion, it is also of importance to consider assessment of vitamin D status in MG patients in a clinical setting, since vitamin D levels have been shown to be of importance to clinical MG status [154]. Intake of supplementary vitamin D did not differ between patients and controls and we did not analyze serum levels of vitamin D, which is why a possible correlation with fish consumption is only speculative.
The reported rate of physical activity was lower in the MG group than in the controls. MG and physical activity will be further discussed below.

59
Impact on everyday life In comparison to matched controls, MG patients scored higher on MGQoL-15. It must be noted though, that MG-QoL is disease-specific, i.e. designed for MG symptoms and does not address quality of life in a holistic perspective. Therefore, the conclusion only concerns MG related symptoms, as other qual-ity of life (QoL) scales were not used. Albeit, some other measures of putative impact on QoL differed between the patients and the controls. MG patients reported higher frequency of mental health problems and were more often re-ceiving antidepressants. During the last year EOMG patients had been on sick-ness leave as well as received sickness benefits to a higher extent than had the matched controls.
MG and physical activity Although muscle fatigue is the cardinal symptom of MG, the tolerance and effects of physical activity in MG are hitherto only sparsely studied [65, 131, 132]. Based on current knowledge of MG pathophysiology and the unknown mechanisms of factors eliciting disease deterioration, it is difficult to theoret-ically predict how physical exercise will affect disease activity and muscle fatigue. As a result, there are no consensus guidelines on physical exercise in MG [155] and traditionally many patients have even been dissuaded from ex-ercising. In study II the MG patients accordingly reported a lower rate of phys-ical activity than did the matched population controls. With the well-known health benefits of physical exercise, this is not a justifiable strategy.
Drawbacks with exercise studies The aim of Study III was to evaluate the safety of physical exercise in MG patients. This seems like a straightforward objective; however, there are few guidelines on how to best design such a study. These issues include study du-ration, number of training occasions and minimum participation rates. Exer-cise studies are time consuming and costly, both for the researchers and for the patients, which often results in quite small participant numbers. The low number of participants in our studies also limited the possibility of further subgroup analysis. Therefore, we cannot rule out differences in training re-sponse with respect to MG subgroup, gender or disease duration. The inter-vention period of most training studies is about three months, a time probably set by practical issues such as the time-consuming nature of the studies. Longer interventions could lead to a higher number of drop outs. Further, the longer the follow-up time the higher the risk for more confounding factors. There have been different attempts to use control groups in training studies, but it is a delicate challenge to design a comparable “placebo group” in an

60
exercise context. We hence chose to use the patients as their own controls, mainly because of a lack of possibilities to set up a reasonably matched control group based on the low incidence and heterogeneity of MG.
There is a large number and variety of types of training exercises; still the training regimen must be chosen carefully to allow for scientific evaluation. We chose to apply the training regimen recommended for healthy adults [122], for many reasons. This regimen is supported by national and international ex-pert boards and designed to provide the many advantages of the proven health benefits of physical exercise. It is also possible to individually tailor based on previous physical activity level. Further, it is easy to implement in everyday life if proven beneficial. This choice of exercise program, as would any other, still leaves behind questions regarding optimal type of training regimen for MG patients. As this was not our primary focus it will have to be an aim of further studies.
How to measure effects of exercise Possible measures of exercise effects span a wide range of different categories. Endpoints could be related to effects on physical fitness, to structural or bio-chemical changes of skeletal muscles, to effects on general physical and men-tal health, to quality of life or to the influence of exercise on an underlying disease. The choice of outcome measures should be determined by the study objective. However, as only few of these measures are thoroughly validated it is not always clear-cut how to interpret their results in varying settings.
In study III the objective was to evaluate the safety of physical exercise in MG patients, as measured mainly by stable (or improved) MGC. This is a recommended clinical outcome measure in MG studies [59], and thereby un-controversial.
In study IV the objective was to assess if MG patients have similar func-tional and structural muscle effects of physical exercise, as do healthy adults. Functional muscle measures have been widely used in various studies and are fairly well established. Neurophysiological or gross structural measures of ex-ercise effects on skeletal muscle are not extensively evaluated [143, 156-160] and when it comes to neuromuscular diseases, they are basically not studied at all. Accordingly, there are no optimally validated measures of muscle struc-ture in response to exercise and further studies are needed to improve the full understanding of muscle measurements.
Due to a lack of fully validated variables CMAP was chosen, as CMAP amplitudes are higher in the biceps and quadriceps muscles of well-trained healthy adults compared with healthy individuals not performing resistance training [143, 156]. Additionally, CMAP correlates with isometric muscle strength [143]. Although it could be speculated that individuals with constitu-tionally lower CMAP amplitudes are more inactive, this explanation is not very likely. The noted increase in CMAP amplitudes in trained muscles in the

61
MG patients in study III would also indicate that physical exercise increases CMAP amplitudes.
Neuromuscular ultrasound was chosen as another variable to study, as the muscle diameter and cross-sectional area have been suggested to increase in response to training [157, 158]. Another possible muscle imaging method is magnetic resonance tomography (MR) which has been used to measure mus-cle thickness in training studies [158]. Results of neuromuscular ultrasound correlate with results of MR [161] and as ultrasound is a more convenient method for the patients we chose this method. A muscle biopsy would have provided additional data of possible importance to the study objective, but we considered the patient discomfort and risks of two biopsies in the same muscle to be too high to be justified.
Safety and effects of exercise in MG patients The most important finding of the training studies in this thesis was that MG patients with mild disease activity could adhere to the general recommenda-tions for physical activity for healthy adults, without risk of disease deteriora-tion. In both studies the exercise program was well tolerated, and none of the patients discontinued the training because of increased MG fatigue, based on the MGC score and neuromuscular decrement. Neither did they describe any other uneasiness regarding the training regimen.
In both studies we found physical improvements, although these were somewhat diverse. In study III CMAP amplitudes and resistance weights of proximal muscles, especially the biceps muscles, had increased at the end of the training period. In study IV there was improvement of functional muscle measures, including isometric muscle force, muscle thickness, clinical fatigue and CMAP in proximal leg muscles, as well as improvement of the 30SCST. Functional measures of proximal arm muscles did not display a similar im-provement in study IV.
The improvement of functional outcome measures is in line with the im-provement of clinical muscle function seen in single previous studies of MG and exercise [131, 132]. It is also in agreement with the muscle response seen in healthy well-trained individuals [143]. The absence of improvement in arm muscles in study IV, could be regarded as somewhat puzzling, although a sim-ilar arm-leg difference was reported in one previous study [131]. In study III and yet another study [132] there was at least some arm muscle improvement in response to training. There was no obvious difference in clinical or neuro-physiological fatigability in arm versus leg muscle before the intervention. A larger amount of leg muscle training in the exercise regimen, due to the aero-bic cycling, could be an explanation for the difference in study IV, but this would not explain the difference/non-difference in the other studies. As the quadriceps muscle is naturally more active in everyday life, we could specu-late that a higher degree of arm inactivity at baseline would require a longer

62
duration of training intervention to reach similar effects. A gender-related CMAP arm-leg difference has been described, where trained healthy women have higher CMAP amplitudes in quadriceps and trained healthy men have higher CMAP amplitudes in the biceps brachii [143] compared to untrained individuals of the same sex. As there was a slight female preponderance in study IV, as well as in a previous study with similar results [131], this could possibly contribute to the arm-leg difference in response to training.
In both training studies (III and IV) we evaluated the changes in common cardiovascular risk factors, such as weight, blood pressure, serum cholesterol and blood glucose. There were no changes before and after the intervention, although the short study duration of three months probably is too short to ex-pect such changes. There is no obvious reason though, to believe that MG patients wouldn’t have the same health benefits from physical exercise as proven for healthy adults.
In study III, a decrease in the disease specific microRNAs miR-150-5p and miR-21-5p were seen after the training period. Levels of miR-150-5p have been described to decrease in correlation with MG disease improvement after thymectomy [54]. The exercise-related decrease in miR-150-5p could be sug-gestive of a possible reduction in inflammatory activity similar to what has been seen after long-term exercise in healthy adults, as well as in individuals with other diseases [162, 163].
Regarding the low number of participants in these training studies, it can be questioned if the result of exercise tolerability in MG patients is well doc-umented enough to be put into treatment guidelines. The health risks of sed-entary behavior due to MG fatigue should be taken seriously, as should possi-ble unfavorable health effects of medications and disease-associated condi-tions [11]. This underlines the need for improved and tailored training recom-mendations for MG patients. The findings of exercise tolerability and improved functional muscle measures in this thesis, although based on few patients, suggest that the applied exercise program, according to the general recommendations for healthy adults [122], can be recommended to patients who want to remain or become physically active, despite having MG. As long as there is no contradictory evidence any other approach would be untenable.

63
Conclusions
Despite comparable clinical muscle fatigue status, Estonian MG patients sub-jectively score both fatigue and disease severity higher than do Swedish MG patients. Estonian MG patients also receive higher doses of AChEI and tend to be less physically active. There is a difference in gender distribution be-tween MG patients in the Tartu region and Jönköping county, especially re-garding LOMG. These differences underline the importance to take regional epidemiology and socioeconomical factors into account when interpreting and implementing results from research studies. The prevalence of MG in Jönköping county (203 per million) fall within the wide range of prevalence estimates for MG worldwide (150-250 per million). Still, the subgroup distribution in Jönköping county differs from the suggested worldwide subgroup distribution, mainly due to a higher proportion of EOMG and a lower proportion of LOMG. The reason for this remains unclear, but an underdiagnosis of LOMG among female patients cannot be ruled out. MGC could be better than QMG in recognizing bulbar symptoms. LOMG patients tend to have a disadvantageous pattern of life-style related risk factors as compared to matched population controls, which preferably should be addressed in the clinical follow-up of these patients. MG patients with mild to moderate disease activity can perform physical ex-ercise, as recommended by the general guidelines for healthy adults, without disease deterioration. MG patients develop beneficial skeletal muscle responses to physical exercise.

64
Sammanfattning på svenska – Summary in Swedish
Myasthenia Gravis (MG) är en autoimmun neuromuskulär sjukdom som or-sakar fluktuerande muskelsvaghet och som drabbar ca 25/100 000 individer i Sverige. Sjukdomen orsakas av antikroppar riktade mot strukturer i den neuromuskulära synapsen. Dessa ger upphov till en störd signalöverföring mellan nerv och muskel, med abnorm muskeluttröttbarhet och muskelsvaghet i tvärstrimmig skelettmuskulatur som följd. Utbredning och grad av muskel-svaghet varierar mellan olika patienter. De allra flesta har ögonsymtom, med dubbelseende och ptos (hängande ögonlock). Många har även tal- och svälj-svårigheter, nacksvaghet och/eller svaghet i extremiteterna. Diagnosen MG ställs genom klinisk neurologisk undersökning, neurofysiologisk analys av störd nerv-muskelsignalering och blodprovsanalys av antikroppar mot acetyl-kolin-receptorn (AChR) och muskelspecifikt tyrosinkinas (MuSK). Det finns ingen botande behandling vid MG, men de flesta har god effekt av immunmo-dulerande läkemedel i kombination med symtomlindrande medicinering. Pa-tienter med AChR-antikroppar och som insjuknat före 50 års ålder har därtill ofta nytta av thymektomi.
Eftersom livsstilssjukdomar är vanligt förekommande, drabbas även MG patienter av dessa sjukdomstillstånd. MG-symtom och -behandling utgör dessutom en tänkbar riskökning avseende livsstilssjukdomar. Samtidigt är all-männa riktlinjer för prevention av livsstilssjukdomar inte säkert tillämpbara vid MG, eftersom läkemedel såsom statiner kan ge försämring i sjukdomen. Trots att MG drabbar muskelfunktionen har det också länge varit okänt om personer med sjukdomen kan vara fysiskt aktiva, utan risk för försämring.
Inom ramen för denna avhandling undersöktes förekomsten av livsstilsre-laterade miljöfaktorer vid MG. I en enkät- och blodprovsstudie i Region Jön-köping beräknades förekomsten av MG, och MG-subgrupper jämfördes avse-ende sjukdomskarakteristika och livsstilsrelaterade riskfaktorer. Resultaten jämfördes också med resultat från en liknande enkätundersökning i Tartu, Est-land. I jämförelse med matchade kontrollpersoner var patienter med sjuk-domsdebut efter 50 års ålder i större utsträckning överviktiga, de rökte mer, tränade mindre och åt mer sällan fisk. Estländska patienter hade en högre sub-jektiv sjukdomsskattning, trots att muskeluttröttbarheten vid klinisk undersök-ning inte skiljde sig åt jämfört med svenska patienter. Estländska patienter tränade mindre ofta.

65
Effekter av fysisk träning vid MG undersöktes i två studier där patienter fick träna i enlighet med generella riktlinjer för friska vuxna. Trots viss (för-väntad) direktupplevd trötthet kunde MG-patienter genomföra träningspro-grammet utan försämring i sjukdomen. Muskelparametrar och funktionspro-ver förbättrades tydligt.

66
Acknowledgements
The work on this thesis was carried out at the Department of Neuroscience, Uppsala University, the Neurology Department at Ryhov hospital in Jönkö-ping and the Department of Clinical Neurophysiology at Uppsala University Hospital. It was supported by grants from Neuroförbundet (NEURO Sweden), FUTURUM, Palle Ferbs Memorial Foundation and Selanders Memorial Foundation. I am grateful to all of you, who in different ways took part in this research. This thesis would not have been possible without your efforts. Thank you! Especially I want to thank: All patients and control individuals who voluntarily sacrificed their time, blood and sweat as subjects in the studies.
Anna Rostedt Punga, my supervisor, colleague and friend, who with endless enthusiasm and accuracy guided me through the process of this research. My co-supervisor, Ann-Marie Landtblom. My co-authors Liis Sabre, Maarika Liik, Carl-Johan Molin, Ida Lindblad, Margareta Emtner, Sören Spörndly Nees and Johan Widenfalk.
Maria Landén and Samuel Ånfors, physiotherapists, who supervised the exer-cise regimen in study III. Margaretha Rostedt, research assistant who supervised the exercise regimen in study IV. Margaretha Eklöf Grindlund, biomedical technician who performed the elec-trophysiological measurements in study IV. Martha Lewandowska for invaluable language assistance. The biomedical technicians at Clinical Neurophysiology Lab at Ryhov hospi-tal in Jönköping.

67
Co-workers in the Research group at Clinical Neurophysiology, Department of Neuroscience.
Colleagues and co-workers at the Department of Clinical Neurophysiology at Uppsala University Hospital.
Colleagues and co-workers at the Neurology Department at Ryhov hospital in Jönköping. I am also grateful to my wonderful family for never-ending support, love and patience. My mother, Christina, for always being there. My sisters and brother. Saga, Sakarias, Sabina, Siri and Sofia. Per-Anton, for everything.

68
References
1. Hughes, T., The early history of myasthenia gravis. Neuromuscul Disord, 2005. 15(12): p. 878-86.
2. Dale, H.H., W. Feldberg, and M. Vogt, Release of acetylcholine at voluntary motor nerve endings. J Physiol, 1936. 86(4): p. 353-80.
3. Walker, M.B., Case showing the Effect of Prostigmin on Myasthenia Gravis. Proc R Soc Med, 1935. 28(6): p. 759-61.
4. John, A.S., Myasthenia Gravis: A New Hypothesis. Scottish Medical Journal, 1960. 5(10): p. 419-436.
5. Patrick, J. and J. Lindstrom, Autoimmune response to acetylcholine receptor. Science, 1973. 180(4088): p. 871-2.
6. Pinching, A.J. and D.K. Peters, Remission of myasthenia gravis following plasma-exchange. Lancet, 1976. 2(8000): p. 1373-6.
7. Hoch, W., et al., Auto-antibodies to the receptor tyrosine kinase MuSK in pa-tients with myasthenia gravis without acetylcholine receptor antibodies. Nat Med, 2001. 7(3): p. 365-8.
8. Pevzner, A., et al., Anti-LRP4 autoantibodies in AChR- and MuSK-antibody-negative myasthenia gravis. J Neurol, 2012. 259(3): p. 427-35.
9. Vincent, A., Unravelling the pathogenesis of myasthenia gravis. Nat Rev Im-munol, 2002. 2(10): p. 797-804.
10. Carr, A.S., et al., A systematic review of population based epidemiological studies in Myasthenia Gravis. BMC Neurol, 2010. 10: p. 46.
11. Gilhus, N.E., Myasthenia Gravis. N Engl J Med, 2016. 375(26): p. 2570-2581. 12. Gilhus, N.E. and J.J. Verschuuren, Myasthenia gravis: subgroup classification
and therapeutic strategies. Lancet Neurol, 2015. 14(10): p. 1023-36. 13. Phillips, L.H., The epidemiology of myasthenia gravis. Semin Neurol, 2004.
24(1): p. 17-20. 14. Pakzad, Z., T. Aziz, and J. Oger, Increasing incidence of myasthenia gravis
among elderly in British Columbia, Canada. Neurology, 2011. 76(17): p. 1526-8.
15. Heldal, A.T., et al., Seropositive myasthenia gravis: a nationwide epidemio-logic study. Neurology, 2009. 73(2): p. 150-1.
16. Andersen, J.B., et al., Myasthenia gravis requiring pyridostigmine treatment in a national population cohort. Eur J Neurol, 2010. 17(12): p. 1445-50.
17. McGrogan, A., S. Sneddon, and C.S. de Vries, The incidence of myasthenia gravis: a systematic literature review. Neuroepidemiology, 2010. 34(3): p. 171-83.
18. Berrih-Aknin, S., Myasthenia Gravis: paradox versus paradigm in autoim-munity. J Autoimmun, 2014. 52: p. 1-28.
19. Plomp, J.J., M.G.M. Huijbers, and J. Verschuuren, Neuromuscular synapse electrophysiology in myasthenia gravis animal models. Ann N Y Acad Sci, 2018. 1412(1): p. 146-153.

69
20. Dale Purves, G.A., David Fitzpatrick, William Hall, Anthony-Samuel Laman-tia, Leonard White Neuroscience. 5th Edition. 2012.
21. Otsuka, K., et al., Collagen Q and anti-MuSK autoantibody competitively sup-press agrin/LRP4/MuSK signaling. Sci Rep, 2015. 5: p. 13928.
22. Messeant, J., et al., MuSK frizzled-like domain is critical for mammalian neu-romuscular junction formation and maintenance. J Neurosci, 2015. 35(12): p. 4926-41.
23. Kaminski, H.J., J.I. Suarez, and R.L. Ruff, Neuromuscular junction physiology in myasthenia gravis. Isoforms of the acetylcholine receptor in extraocular muscle and the contribution of sodium channels to the safety factor, 1997. 48(Suppl 5): p. 8S-17S.
24. Burden, S.J., M.G. Huijbers, and L. Remedio, Fundamental Molecules and Mechanisms for Forming and Maintaining Neuromuscular Synapses. Int J Mol Sci, 2018. 19(2).
25. Punga, A.R. and M.A. Ruegg, Signaling and aging at the neuromuscular syn-apse: lessons learnt from neuromuscular diseases. Curr Opin Pharmacol, 2012. 12(3): p. 340-6.
26. Eymard, B., et al., Anti-acetylcholine receptor antibodies in neonatal myasthe-nia gravis: heterogeneity and pathogenic significance. J Autoimmun, 1991. 4(2): p. 185-95.
27. Brooks, W.H., A Review of Autoimmune Disease Hypotheses with Introduction of the "Nucleolus" Hypothesis. Clin Rev Allergy Immunol, 2017. 52(3): p. 333-350.
28. AK, A., L. AH, and P. S, Cellular and Molecular Immunology. 8th ed. 2014. 29. Vincent, A., J. Palace, and D. Hilton-Jones, Myasthenia gravis. Lancet, 2001.
357(9274): p. 2122-8. 30. Cao, Y., et al., Autoreactive T Cells from Patients with Myasthenia Gravis Are
Characterized by Elevated IL-17, IFN-gamma, and GM-CSF and Diminished IL-10 Production. J Immunol, 2016. 196(5): p. 2075-84.
31. Phillips, W.D. and A. Vincent, Pathogenesis of myasthenia gravis: update on disease types, models, and mechanisms. F1000Res, 2016. 5.
32. Meriggioli, M.N. and D.B. Sanders, Autoimmune myasthenia gravis: emerging clinical and biological heterogeneity. Lancet Neurol, 2009. 8(5): p. 475-90.
33. Meriggioli, M.N. and D.B. Sanders, Muscle autoantibodies in myasthenia gravis: beyond diagnosis? Expert Rev Clin Immunol, 2012. 8(5): p. 427-38.
34. Gilhus, N.E., Myasthenia and the neuromuscular junction. Curr Opin Neurol, 2012. 25(5): p. 523-9.
35. Querol, L. and I. Illa, Myasthenia gravis and the neuromuscular junction. Curr Opin Neurol, 2013. 26(5): p. 459-65.
36. Verschuuren, J.J., et al., Pathophysiology of myasthenia gravis with antibodies to the acetylcholine receptor, muscle-specific kinase and low-density lipopro-tein receptor-related protein 4. Autoimmun Rev, 2013. 12(9): p. 918-23.
37. Koneczny, I., J. Cossins, and A. Vincent, The role of muscle-specific tyrosine kinase (MuSK) and mystery of MuSK myasthenia gravis. J Anat, 2014. 224(1): p. 29-35.
38. Huijbers, M.G., et al., IgG4-mediated autoimmune diseases: a niche of anti-body-mediated disorders. Ann N Y Acad Sci, 2018. 1413(1): p. 92-103.
39. Le Panse, R. and S. Berrih-Aknin, Autoimmune myasthenia gravis: autoanti-body mechanisms and new developments on immune regulation. Curr Opin Neurol, 2013. 26(5): p. 569-76.

70
40. Berrih-Aknin, S. and R. Le Panse, Myasthenia gravis: a comprehensive review of immune dysregulation and etiological mechanisms. J Autoimmun, 2014. 52: p. 90-100.
41. Bartoccioni, E., et al., Anti-MuSK antibodies: correlation with myasthenia gravis severity. Neurology, 2006. 67(3): p. 505-7.
42. Huijbers, M.G., et al., Pathogenic immune mechanisms at the neuromuscular synapse: the role of specific antibody-binding epitopes in myasthenia gravis. J Intern Med, 2014. 275(1): p. 12-26.
43. McConville, J., et al., Detection and characterization of MuSK antibodies in seronegative myasthenia gravis. Ann Neurol, 2004. 55(4): p. 580-4.
44. Zhang, B., et al., LRP4 serves as a coreceptor of agrin. Neuron, 2008. 60(2): p. 285-97.
45. Oger, J. and H. Frykman, An update on laboratory diagnosis in myasthenia gravis. Clin Chim Acta, 2015. 444: p. 126-31.
46. Romi, F., Thymoma in myasthenia gravis: from diagnosis to treatment. Auto-immune Dis, 2011. 2011: p. 474512.
47. Zhang, B., et al., Autoantibodies to agrin in myasthenia gravis patients. PLoS One, 2014. 9(3): p. e91816.
48. Hohlfeld, R. and H. Wekerle, Reflections on the "intrathymic pathogenesis" of myasthenia gravis. J Neuroimmunol, 2008. 201-202: p. 21-7.
49. Marx, A., et al., The different roles of the thymus in the pathogenesis of the various myasthenia gravis subtypes. Autoimmun Rev, 2013. 12(9): p. 875-84.
50. Wolfe, G.I., H.J. Kaminski, and G.R. Cutter, Randomized Trial of Thymectomy in Myasthenia Gravis. N Engl J Med, 2016. 375(20): p. 2006-2007.
51. Berrih-Aknin, S., et al., Ectopic germinal centers, BAFF and anti-B-cell ther-apy in myasthenia gravis. Autoimmun Rev, 2013. 12(9): p. 885-93.
52. Ishii, W., et al., Comparison of the histological and immunohistochemical fea-tures of the thymus in young- and elderly-onset myasthenia gravis without thy-moma. J Clin Neurosci, 2007. 14(2): p. 110-5.
53. Rioux, J.D., et al., Mapping of multiple susceptibility variants within the MHC region for 7 immune-mediated diseases. Proc Natl Acad Sci U S A, 2009. 106(44): p. 18680-5.
54. Punga, T., et al., Circulating miRNAs in myasthenia gravis: miR-150-5p as a new potential biomarker. Ann Clin Transl Neurol, 2014. 1(1): p. 49-58.
55. Godoy, D.A., et al., The myasthenic patient in crisis: an update of the manage-ment in Neurointensive Care Unit. Arq Neuropsiquiatr, 2013. 71(9a): p. 627-39.
56. Nicolle, M.W., Myasthenia Gravis and Lambert-Eaton Myasthenic Syndrome. Continuum (Minneap Minn), 2016. 22(6, Muscle and Neuromuscular Junction Disorders): p. 1978-2005.
57. Thomas, C.E., et al., Myasthenic crisis: clinical features, mortality, complica-tions, and risk factors for prolonged intubation. Neurology, 1997. 48(5): p. 1253-60.
58. de Meel, R.H., et al., Prognostic factors for exacerbations and emergency treatments in myasthenia gravis. J Neuroimmunol, 2015. 282: p. 123-5.
59. Benatar, M., et al., Recommendations for myasthenia gravis clinical trials. Muscle Nerve, 2012. 45(6): p. 909-17.
60. Jaretzki, A., 3rd, et al., Myasthenia gravis: recommendations for clinical re-search standards. Task Force of the Medical Scientific Advisory Board of the Myasthenia Gravis Foundation of America. Neurology, 2000. 55(1): p. 16-23.
61. Fang, F., et al., The autoimmune spectrum of myasthenia gravis: a Swedish population-based study. J Intern Med, 2015. 277(5): p. 594-604.
71
62. Evoli, A., et al., Poly-autoimmunity in patients with myasthenia gravis: A sin-gle-center experience. Autoimmunity, 2015. 48(6): p. 412-7.
63. Gilhus, N.E., et al., Myasthenia gravis and risks for comorbidity. Eur J Neurol, 2015. 22(1): p. 17-23.
64. Nacu, A., et al., Complicating autoimmune diseases in myasthenia gravis: a review. Autoimmunity, 2015. 48(6): p. 362-8.
65. Elsais, A., et al., Fatigue in myasthenia gravis: is it more than muscular weak-ness? BMC Neurol, 2013. 13: p. 132.
66. Kaltsatou, A., et al., Cognitive impairment as a central cholinergic deficit in patients with Myasthenia Gravis. BBA Clin, 2015. 3: p. 299-303.
67. Mao, Z., et al., Association between myasthenia gravis and cognitive function: A systematic review and meta-analysis. Ann Indian Acad Neurol, 2015. 18(2): p. 131-7.
68. Paul, R.H., et al., Fatigue and its impact on patients with myasthenia gravis. Muscle Nerve, 2000. 23(9): p. 1402-6.
69. Sieminski, M., M. Bilinska, and W.M. Nyka, Increased frequency of restless legs syndrome in myasthenia gravis. Eur Neurol, 2012. 68(3): p. 166-70.
70. Marra, C., et al., Determinants of cognitive impairment in elderly myasthenia gravis patients. Muscle Nerve, 2009. 40(6): p. 952-9.
71. Paul, R.H., et al., Cognitive dysfunction in individuals with myasthenia gravis. J Neurol Sci, 2000. 179(S 1-2): p. 59-64.
72. Hoffmann, S., et al., Fatigue in myasthenia gravis: risk factors and impact on quality of life. Brain Behav, 2016. 6(10): p. e00538.
73. Kumar, R., et al., MG-QoL-15 scores in treated myasthenia gravis: Experience from a university hospital in India. Neurol India, 2016. 64(3): p. 405-10.
74. Burns, T.M., M. Conaway, and D.B. Sanders, The MG Composite: A valid and reliable outcome measure for myasthenia gravis. Neurology, 2010. 74(18): p. 1434-40.
75. Bedlack, R.S., et al., Quantitative myasthenia gravis score: assessment of re-sponsiveness and longitudinal validity. Neurology, 2005. 64(11): p. 1968-70.
76. Benatar, M., A systematic review of diagnostic studies in myasthenia gravis. Neuromuscul Disord, 2006. 16(7): p. 459-67.
77. Larner, A.J., The place of the ice pack test in the diagnosis of myasthenia gravis. Int J Clin Pract, 2004. 58(9): p. 887-8.
78. Stalberg, E., J. Ekstedt, and A. Broman, Neuromuscular transmission in myas-thenia gravis studied with single fibre electromyography. J Neurol Neurosurg Psychiatry, 1974. 37(5): p. 540-7.
79. Lindstrom, J.M., et al., Antibody to acetylcholine receptor in myasthenia gravis. Prevalence, clinical correlates, and diagnostic value. Neurology, 1976. 26(11): p. 1054-9.
80. Vincent, A. and J. Newsom-Davis, Acetylcholine receptor antibody as a diag-nostic test for myasthenia gravis: results in 153 validated cases and 2967 di-agnostic assays. J Neurol Neurosurg Psychiatry, 1985. 48(12): p. 1246-52.
81. Leite, M.I., et al., IgG1 antibodies to acetylcholine receptors in 'seronegative' myasthenia gravis. Brain, 2008. 131(Pt 7): p. 1940-52.
82. Tsonis, A.I., et al., MuSK autoantibodies in myasthenia gravis detected by cell based assay--A multinational study. J Neuroimmunol, 2015. 284: p. 10-7.
83. Chang, T., et al., Clinical and serological study of myasthenia gravis using both radioimmunoprecipitation and cell-based assays in a South Asian popu-lation. J Neurol Sci, 2014. 343(1-2): p. 82-7.

72
84. Zisimopoulou, P., et al., A comprehensive analysis of the epidemiology and clinical characteristics of anti-LRP4 in myasthenia gravis. J Autoimmun, 2014. 52: p. 139-45.
85. Berrih-Aknin, S., M. Frenkian-Cuvelier, and B. Eymard, Diagnostic and clin-ical classification of autoimmune myasthenia gravis. J Autoimmun, 2014. 48-49: p. 143-8.
86. Alkhawajah, N.M. and J. Oger, Late-onset myasthenia gravis: a review when incidence in older adults keeps increasing. Muscle Nerve, 2013. 48(5): p. 705-10.
87. Skeie, G.O., et al., Guidelines for treatment of autoimmune neuromuscular transmission disorders. Eur J Neurol, 2010. 17(7): p. 893-902.
88. Sieb, J.P., Myasthenia gravis: an update for the clinician. Clin Exp Immunol, 2014. 175(3): p. 408-18.
89. Klein, R., et al., Autoimmune associations and autoantibody screening show focused recognition in patient subgroups with generalized myasthenia gravis. Hum Immunol, 2013. 74(9): p. 1184-93.
90. Maniaol, A.H., et al., Late onset myasthenia gravis is associated with HLA DRB1*15:01 in the Norwegian population. PLoS One, 2012. 7(5): p. e36603.
91. Evoli, A. and L. Padua, Diagnosis and therapy of myasthenia gravis with an-tibodies to muscle-specific kinase. Autoimmun Rev, 2013. 12(9): p. 931-5.
92. Guptill, J.T., D.B. Sanders, and A. Evoli, Anti-MuSK antibody myasthenia gravis: clinical findings and response to treatment in two large cohorts. Mus-cle Nerve, 2011. 44(1): p. 36-40.
93. Hurst, R.L. and C.L. Gooch, Muscle-Specific Receptor Tyrosine Kinase (MuSK) Myasthenia Gravis. Curr Neurol Neurosci Rep, 2016. 16(7): p. 61.
94. Reddel, S.W., M. Morsch, and W.D. Phillips, Clinical and scientific aspects of muscle-specific tyrosine kinase-related myasthenia gravis. Curr Opin Neurol, 2014. 27(5): p. 558-65.
95. Evoli, A., et al., Myasthenia gravis with antibodies to MuSK: an update. Ann N Y Acad Sci, 2018. 1412(1): p. 82-89.
96. Evoli, A., et al., Pattern of ocular involvement in myasthenia gravis with MuSK antibodies. J Neurol Neurosurg Psychiatry, 2017. 88(9): p. 761-763.
97. Evoli, A., et al., Response to therapy in myasthenia gravis with anti-MuSK antibodies. Ann N Y Acad Sci, 2008. 1132: p. 76-83.
98. Hatanaka, Y., et al., Nonresponsiveness to anticholinesterase agents in pa-tients with MuSK-antibody-positive MG. Neurology, 2005. 65(9): p. 1508-9.
99. Lavrnic, D., et al., The features of myasthenia gravis with autoantibodies to MuSK. J Neurol Neurosurg Psychiatry, 2005. 76(8): p. 1099-102.
100. Shin, H.Y., et al., Clinical and Electrophysiologic Responses to Acetylcholin-esterase Inhibitors in MuSK-Antibody-Positive Myasthenia Gravis: Evidence for Cholinergic Neuromuscular Hyperactivity. J Clin Neurol, 2014. 10(2): p. 119-24.
101. Morren, J. and Y. Li, Myasthenia Gravis with Muscle-Specific Tyrosine Kinase (MuSK) Antibodies- A Narrative Review. Muscle Nerve, 2018.
102. Alahgholi-Hajibehzad, M., et al., Association of HLA-DRB1 *14, -DRB1 *16 and -DQB1 *05 with MuSK-myasthenia gravis in patients from Turkey. Hum Immunol, 2013. 74(12): p. 1633-5.
103. Bartoccioni, E., et al., HLA class II allele analysis in MuSK-positive myasthe-nia gravis suggests a role for DQ5. Neurology, 2009. 72(2): p. 195-7.
104. Higuchi, O., et al., Autoantibodies to low-density lipoprotein receptor-related protein 4 in myasthenia gravis. Ann Neurol, 2011. 69(2): p. 418-22.

73
105. Zhang, B., et al., Autoantibodies to lipoprotein-related protein 4 in patients with double-seronegative myasthenia gravis. Arch Neurol, 2012. 69(4): p. 445-51.
106. Cossins, J., et al., The search for new antigenic targets in myasthenia gravis. Ann N Y Acad Sci, 2012. 1275: p. 123-8.
107. Vincent, A., et al., Myasthenia gravis seronegative for acetylcholine receptor antibodies. Ann N Y Acad Sci, 2008. 1132: p. 84-92.
108. Oosterhuis, H.J., The natural course of myasthenia gravis: a long term follow up study. J Neurol Neurosurg Psychiatry, 1989. 52(10): p. 1121-7.
109. Evoli, A., et al., Ocular myasthenia: diagnostic and therapeutic problems. Acta Neurol Scand, 1988. 77(1): p. 31-5.
110. Kerty, E., et al., EFNS/ENS Guidelines for the treatment of ocular myasthenia. Eur J Neurol, 2014. 21(5): p. 687-93.
111. U.S. Health in International Perspective: Shorter Lives, Poorer Health. Mil Med, 2016. 181(9): p. 945-6.
112. Kjeldsen, S.E., Hypertension and cardiovascular risk: General aspects. Phar-macol Res, 2018. 129: p. 95-99.
113. Herrod, P.J.J., et al., Exercise and other nonpharmacological strategies to re-duce blood pressure in older adults: a systematic review and meta-analysis. J Am Soc Hypertens, 2018.
114. Hunter, G.R., et al., Why intensity is not a bad word: Optimizing health status at any age. Clin Nutr, 2018. 37(1): p. 56-60.
115. Foright, R.M., et al., Is regular exercise an effective strategy for weight loss maintenance? Physiol Behav, 2018. 188: p. 86-93.
116. Akter, S., A. Goto, and T. Mizoue, Smoking and the risk of type 2 diabetes in Japan: A systematic review and meta-analysis. J Epidemiol, 2017. 27(12): p. 553-561.
117. Maniaol, A.H., et al., Smoking and socio-economic status may affect myasthe-nia gravis. Eur J Neurol, 2013. 20(3): p. 453-60.
118. Cartwright, M.S., et al., Statin-associated exacerbation of myasthenia gravis. Neurology, 2004. 63(11): p. 2188.
119. Oh, S.J., et al., Statins may aggravate myasthenia gravis. Muscle Nerve, 2008. 38(3): p. 1101-7.
120. Purvin, V., et al., Statin-associated myasthenia gravis: report of 4 cases and review of the literature. Medicine (Baltimore), 2006. 85(2): p. 82-5.
121. Biswas, A., et al., Sedentary time and its association with risk for disease in-cidence, mortality, and hospitalization in adults: a systematic review and meta-analysis. Ann Intern Med, 2015. 162(2): p. 123-32.
122. Garber, C.E., et al., American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespir-atory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc, 2011. 43(7): p. 1334-59.
123. World Health Organization. Global Health Risks: Mortality and Burden of Disease Attributable to Selected Major Risks. 2009, WHO: Geneva.
124. Lucia, A., et al., Double trouble (McArdle's disease and myasthenia gravis): how can exercise help? Muscle Nerve, 2007. 35(1): p. 125-8.
125. Scheer, B.V., E. Valero-Burgos, and R. Costa, Myasthenia gravis and endur-ance exercise. Am J Phys Med Rehabil, 2012. 91(8): p. 725-7.
126. Stout, J.R., et al., Effects of resistance exercise and creatine supplementation on myasthenia gravis: a case study. Med Sci Sports Exerc, 2001. 33(6): p. 869-72.

74
127. Elsais, A., B. Johansen, and E. Kerty, Airway limitation and exercise intoler-ance in well-regulated myasthenia gravis patients. Acta Neurol Scand Suppl, 2010(190): p. 12-7.
128. Fregonezi, G.A., et al., Effects of 8-week, interval-based inspiratory muscle training and breathing retraining in patients with generalized myasthenia gravis. Chest, 2005. 128(3): p. 1524-30.
129. Rassler, B., et al., The effect of respiratory muscle endurance training in pa-tients with myasthenia gravis. Neuromuscul Disord, 2007. 17(5): p. 385-91.
130. Weiner, P., et al., Respiratory muscle training in patients with moderate to severe myasthenia gravis. Can J Neurol Sci, 1998. 25(3): p. 236-41.
131. Lohi, E.L., C. Lindberg, and O. Andersen, Physical training effects in myas-thenia gravis. Arch Phys Med Rehabil, 1993. 74(11): p. 1178-80.
132. Rahbek, M.A., et al., Exercise in myasthenia gravis: A feasibility study of aer-obic and resistance training. Muscle Nerve, 2017.
133. Anziska, Y. and A. Sternberg, Exercise in neuromuscular disease. Muscle Nerve, 2013. 48(1): p. 3-20.
134. Giesser, B.S., Exercise in the management of persons with multiple sclerosis. Ther Adv Neurol Disord, 2015. 8(3): p. 123-30.
135. Kierkegaard, M., et al., High-intensity resistance training in multiple sclerosis - An exploratory study of effects on immune markers in blood and cerebrospi-nal fluid, and on mood, fatigue, health-related quality of life, muscle strength, walking and cognition. J Neurol Sci, 2016. 362: p. 251-7.
136. Perandini, L.A., et al., Exercise as a therapeutic tool to counteract inflamma-tion and clinical symptoms in autoimmune rheumatic diseases. Autoimmun Rev, 2012. 12(2): p. 218-24.
137. Spruit, M.A., et al., An official American Thoracic Society/European Respira-tory Society statement: key concepts and advances in pulmonary rehabilita-tion. Am J Respir Crit Care Med, 2013. 188(8): p. e13-64.
138. Maniaol, A.H., C. Brunborg, and C.M. Tallaksen, Development and validation of a self-administered questionnaire for myasthenia gravis patients. Neuroep-idemiology, 2010. 34(4): p. 253-61.
139. Burns, T.M., et al., Less is more, or almost as much: a 15-item quality-of-life instrument for myasthenia gravis. Muscle Nerve, 2008. 38(2): p. 957-63.
140. Valko, P.O., et al., Validation of the fatigue severity scale in a Swiss cohort. Sleep, 2008. 31(11): p. 1601-7.
141. Olsson, S.J., et al., Categorical answer modes provide superior validity to open answers when asking for level of physical activity: A cross-sectional study. Scand J Public Health, 2016. 44(1): p. 70-6.
142. Kroll, T., et al., The SCI Exercise Self-Efficacy Scale (ESES): development and psychometric properties. Int J Behav Nutr Phys Act, 2007. 4: p. 34.
143. Molin, C.J. and A.R. Punga, Compound Motor Action Potential: Electrophys-iological Marker for Muscle Training. J Clin Neurophysiol, 2016. 33(4): p. 340-5.
144. Molin, C.J., J. Widenfalk, and A.R. Punga, High-resistance strength training does not affect nerve cross sectional area – An ultrasound study. Clinical Neu-rophysiology Practice, 2017. 2: p. 163-169.
145. Podsiadlo, D. and S. Richardson, The timed "Up & Go": a test of basic func-tional mobility for frail elderly persons. J Am Geriatr Soc, 1991. 39(2): p. 142-8.
146. McGavin, C.R., S.P. Gupta, and G.J. McHardy, Twelve-minute walking test for assessing disability in chronic bronchitis. Br Med J, 1976. 1(6013): p. 822-3.

75
147. Jones, C.J., R.E. Rikli, and W.C. Beam, A 30-s chair-stand test as a measure of lower body strength in community-residing older adults. Res Q Exerc Sport, 1999. 70(2): p. 113-9.
148. Aluoja, A., et al., Symptoms of depression in the Estonian population: preva-lence, sociodemographic correlates and social adjustment. J Affect Disord, 2004. 78(1): p. 27-35.
149. Olsen, K.M. and S.A. Dahl, Health differences between European countries. Soc Sci Med, 2007. 64(8): p. 1665-78.
150. Rekand, T., et al., Long term outcome after poliomyelitis in different health and social conditions. J Epidemiol Community Health, 2003. 57(5): p. 368-72.
151. Sabre, L., et al., Traumatic spinal cord injury in two European countries: why the differences? Eur J Neurol, 2013. 20(2): p. 293-9.
152. Carlson, P., Self-perceived health in East and West Europe: another European health divide. Soc Sci Med, 1998. 46(10): p. 1355-66.
153. Carlson, P., The European health divide: a matter of financial or social capi-tal? Soc Sci Med, 2004. 59(9): p. 1985-92.
154. Askmark, H., et al., Vitamin D deficiency in patients with myasthenia gravis and improvement of fatigue after supplementation of vitamin D3: a pilot study. Eur J Neurol, 2012. 19(12): p. 1554-60.
155. Cass, S., Myasthenia gravis and sports participation. Curr Sports Med Rep, 2013. 12(1): p. 18-21.
156. Duez, L., et al., Electrophysiological characteristics of motor units and muscle fibers in trained and untrained young male subjects. Muscle Nerve, 2010. 42(2): p. 177-83.
157. Estes, R.R., et al., The Effect of High Intensity Interval Run Training on Cross-sectional Area of the Vastus Lateralis in Untrained College Students. Int J Ex-erc Sci, 2017. 10(1): p. 137-145.
158. Franchi, M.V., et al., Muscle thickness correlates to muscle cross sectional area in the assessment of strength training induced hypertrophy. Scand J Med Sci Sports, 2017.
159. Massey, G., P. Evangelidis, and J. Folland, Influence of contractile force on the architecture and morphology of the quadriceps femoris. Exp Physiol, 2015. 100(11): p. 1342-51.
160. Folland, J.P. and A.G. Williams, The adaptations to strength training : mor-phological and neurological contributions to increased strength. Sports Med, 2007. 37(2): p. 145-68.
161. Walton, J.M., N. Roberts, and G.H. Whitehouse, Measurement of the quadri-ceps femoris muscle using magnetic resonance and ultrasound imaging. Br J Sports Med, 1997. 31(1): p. 59-64.
162. Forti, L.N., et al., Effects of resistance training at different loads on inflamma-tory markers in young adults. Eur J Appl Physiol, 2017. 117(3): p. 511-519.
163. van der Vlist, J. and T.W. Janssen, The potential anti-inflammatory effect of exercise in chronic obstructive pulmonary disease. Respiration, 2010. 79(2): p. 160-74.

Acta Universitatis UpsaliensisDigital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1439
Editor: The Dean of the Faculty of Medicine
A doctoral dissertation from the Faculty of Medicine, UppsalaUniversity, is usually a summary of a number of papers. A fewcopies of the complete dissertation are kept at major Swedishresearch libraries, while the summary alone is distributedinternationally through the series Digital ComprehensiveSummaries of Uppsala Dissertations from the Faculty ofMedicine. (Prior to January, 2005, the series was publishedunder the title “Comprehensive Summaries of UppsalaDissertations from the Faculty of Medicine”.)
Distribution: publications.uu.seurn:nbn:se:uu:diva-344667
ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2018