enhancing clinical and translational research at unmc lynell klassen, jennifer larsen, elizabeth...
Post on 20-Dec-2015
215 views
TRANSCRIPT
Enhancing Clinical and Translational Research at
UNMCLynell Klassen, Jennifer Larsen,
Elizabeth Seaquist
What is Clinical Research?

What Clinical Research is NOT…
• Research done by an MD
• Publication of clinical observations
• Post-marketing observational trials
NIH definition of Clinical Research (PHS 398)
• Patient-oriented research. Research conducted with human subjects (or of human origin - tissues, specimens and cognitive phenomena) for which an investigator (or colleague) directly interacts with human subjects: (a) mechanisms of human disease, (b) therapeutic interventions, (c) clinical trials, or (d) development of new technologies.
• Epidemiologic and behavioral studies.
• Outcomes and health services research.
What is Translational Research?
• There are two types• Type 1: Preclinical= bench to bedside
–Pre-clinical modeling–Clinically based hypothesis
• Type 2: Post-clinical= trial to community (best practices)
UNMC Clinical Research: Today
• State-of-the art clinical facilities and specialized regional centers for a variety of diseases with a Children’s Hospital for pediatric specialty care
• CRC to support investigator-initiated research with space, research nurses, lab, research support
• Clinical Trials Office for Pharma-driven trials
Current Clinical Research enterprise
• Additional research spaces: Cruzan Center for Dental Research in Lincoln, Clinical research space at OVAMC; but not Children’s Hospital
• Electronic medical record and nationally known medical informatics expertise
• Biostatistics/trial design previously in Prev Soc Med moved to the COPH; additional qualitative analysis expertise at UNL
• Nationally known expertise in human studies regulation and bioethics

Current Clinical Research enterprise
• Growing bioinformatics and biotechnology expertise
• GMP facility for cellular therapies under construction
• Expertise in distance learning, web-based data entry, and long distance research collaborations
• Strong community partnerships with rural communities, minority groups in and outside NE
• Clinical research training in evolution: Stats-Epi track in MPH, interdisciplinary Clinical Research track within MSIA, and Health Services PhD
Building clinical and translational research
Elizabeth Seaquist MD
Professor of Medicine
Program Director, General Clinical Research Center
Co-PI, CTSA
University of Minnesota

BENCH BEDSIDE COMMUNITY
A Transforming Approach: A Transforming Approach: NIH Institutional Clinical and Translational Science NIH Institutional Clinical and Translational Science
Awards (CTSA)Awards (CTSA)
Implementing biomedical discoveries made in the last 10 years demands an evolution of clinical science
New prevention strategies and treatments must be developed, tested, and brought into medical practice more rapidly
CTSA awards will lower barriers between disciplines, and encourage creative, innovative approaches to solve complex medical problems
These clinical and translational science awards will catalyze change -- breaking silos, breaking barriers, and breaking conventions
How is this transformation achieved?
Through the NIH Roadmap for Medical Research, create an integrated environment for the clinical and translational researcher that can provide:– an academic home for clinical research (a Center,
Department, or Institute [C/D/I]) – support for protocol preparation, regulatory
compliance and data management– support for participant recruitment, human subject
safety monitoring– education leading to advanced degrees in clinical
research– specialized cores and services for translational
research
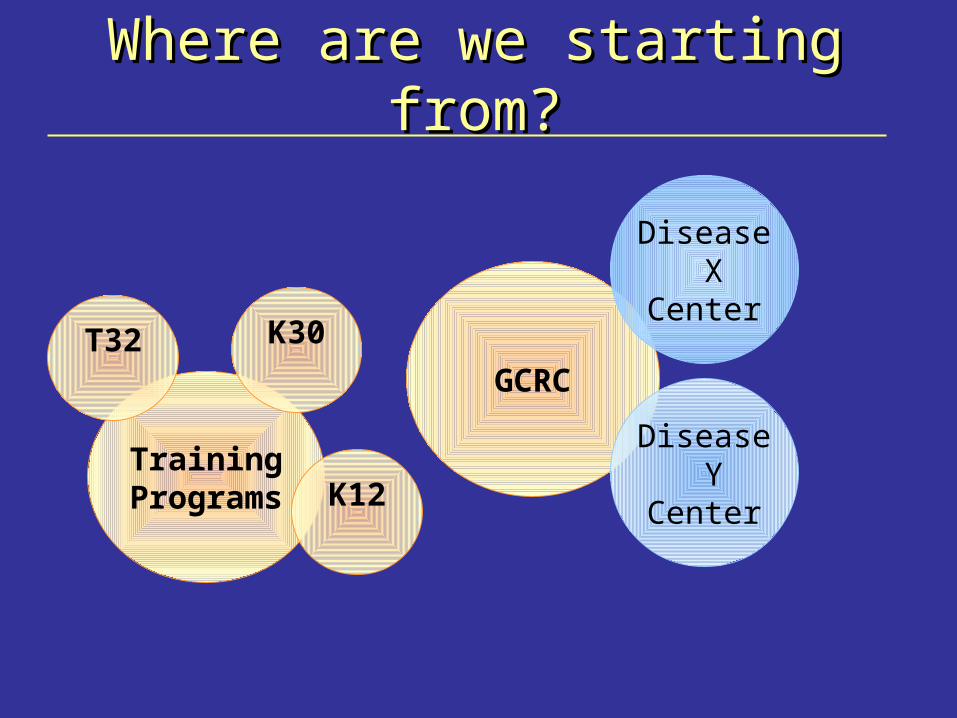
Where are we starting from?Where are we starting from?
TrainingPrograms K12
GCRC
Disease X
Center
Disease Y
Center
K30T32
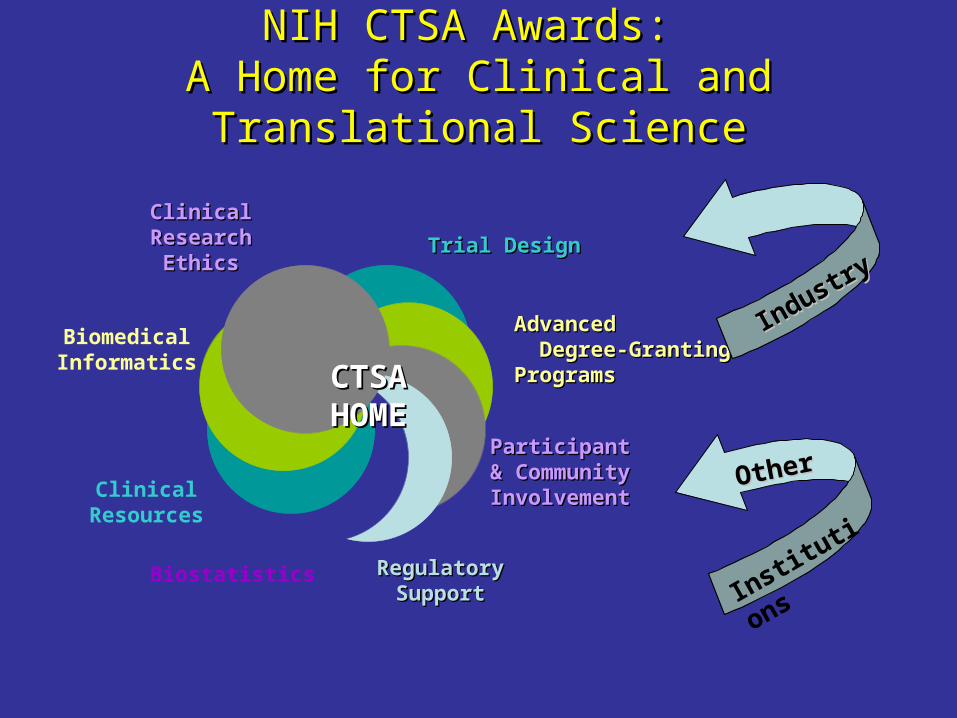
NIH CTSA Awards: NIH CTSA Awards: A Home for Clinical and Translational ScienceA Home for Clinical and Translational Science
Trial DesignTrial Design
AdvancedAdvanced Degree-GrantingDegree-Granting
ProgramsPrograms
ParticipantParticipant& Community& CommunityInvolvementInvolvement
RegulatoryRegulatorySupportSupport
Biostatistics
ClinicalResources
BiomedicalInformatics
ClinicalClinicalResearchResearch
EthicsEthics
CTSACTSAHOMEHOME
Industry
Industry
OtherOther
Institutio
ns
NIH Clinical & Translational Science Awards (CTSA)NIH Clinical & Translational Science Awards (CTSA)
By 2010 (2012?), all GCRCs and Roadmap training programs (T32/K30/K12) will disappear or be incorporated into a CTSA
Approximately 60 CTSAs will be funded in total CTSA award will lower barriers between disciplines, and
encourage creative, innovative approaches to solve complex medical problems
CTSA award will provide new opportunities for institutions to be truly innovative in proposals to transform their programs and resources to foster clinical and translational science.
Long term goal is to speed discoveries to improved patient care
CTSA Specific Objectives (RFA 3/07)CTSA Specific Objectives (RFA 3/07) Provide opportunities and resources for original research on novel methods and approaches to translational and clinical science Provide translational technologies and knowledge base for spectrum of clinical and translational science , including all types and sizes of studies and disciplines Integrate translational and clinical science by fostering collaboration between departments and schools within institution and between institutions and industry Provide a point a contact for partnerships with industry, foundations, and community physicians Provide research education, training and career development leading to a MS or PhD for the next generation of clinical and translational researchers Conduct self-evaluation activities and participate in a national evaluation of the CTSA program
CTSA components
1. Development of Novel Clinical and Translational Methodologies
2. Pilot and Collaborative Translational and Clinical Studies
3. Biomedical Informatics4. Design, Biostatistics, & Clinical Research Ethics5. Regulatory Knowledge and Support6. Participant and Clinical Interactions7. Community Engagement 8. Translational Technologies and Resources9. Research Education, Training, and Career Development
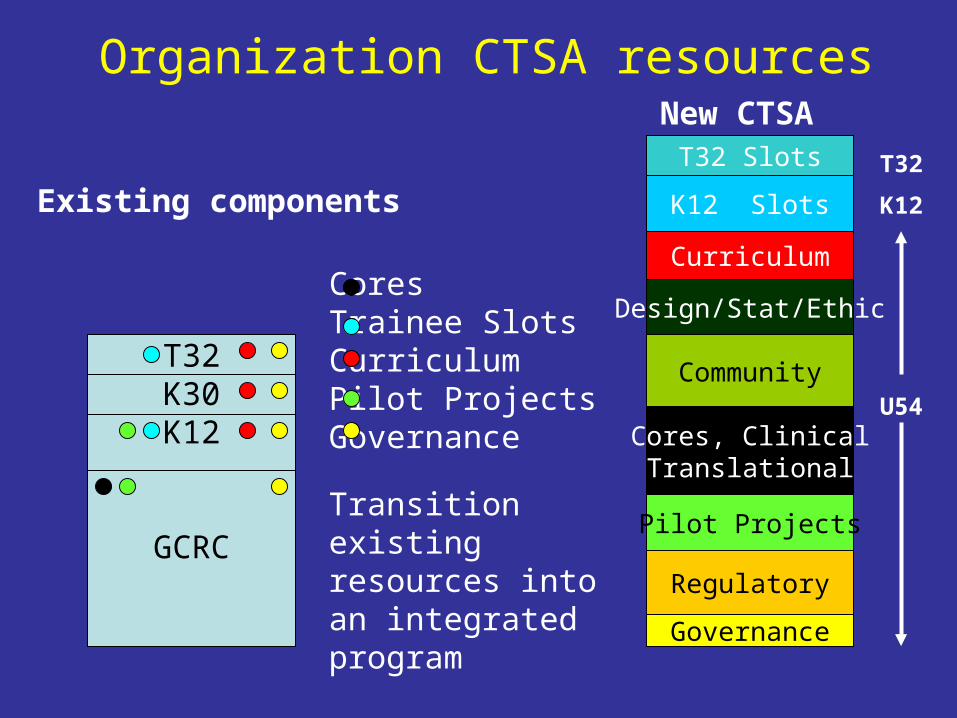
Organization CTSA resources
T32K30K12
GCRC
Cores Trainee SlotsCurriculumPilot ProjectsGovernance
Existing components
New CTSA
Governance
Pilot Projects
Curriculum
T32 Slots
Cores, ClinicalTranslational
Design/Stat/Ethic
Community
Regulatory
Transition existing resources into an integrated program
T32
K12
U54
K12 Slots

Budgetary constraints I.
• Only 1 application may be submitted from each degree granting institution
• Total cost = Combined budgets of existing GCRC/T32/K30/K12 awards + $6 million
• Institutions like UNMC without GCRC/T32/K30/K12 can request up to $6 million
• IDC = institutional rate U54 portion, 8% of K12/T32 portion
Budgetary constraints II.
If more than $4 million total costs above existing GCRC/T32/K30/K12 is requested, applicants must – discuss how they will develop and support
translational research and career development in pediatrics
– discuss the opportunities that will carry their clinical and translational science endeavors into community settings
– describe the institutional commitments that match the increased scale of the program

Round one of applications
34 ApplicationsAwards given to 12 centers
Columbia University Health SciencesDuke UniversityMayo Clinic College of MedicineOregon Health & Science UniversityRockefeller UniversityUniversity of California, DavisUniversity of California, San FranciscoUniversity of PennsylvaniaUniversity of PittsburghUniversity of RochesterUniversity of Texas Health Science Center at HoustonYale University

Round 2 of applications
• 27 are believed to have applied
• Up to 8 will be awarded ($38 million available)
• Review is in May
• Start date is September 2007
Elements of successful applications
• Strong institutional support
($ ~ equal to grant request + new space, has gone >$100 million over grant period)
• Clear vision• Well integrated• Multidisciplinary• Innovative
How has the University of Minnesota responded to the RFA?
• Fall 2003: AHC Clinical Research Task Force starts• 11/04 Task Force Report released• 9/05 AHC Office of Clinical Research opened with Jas Ahluwalia as
Executive Director• First CTSA RFA released 10/05• 10/05-3/06 - Grant planned, written, submitted • Application incorporated 36 yr old GCRC with its specialized cores
and research support services + newly funded Roadmap K12 + institutional support for industry protocols
• $66 million in total costs requested• Institutional commitment: 30,000 sq ft in renovated bldg for CTSA,
renovation of existing 10,000 sq ft GCRC, + ~$50 million over 10 yrs
How has the University of Minnesota responded to the RFA?
• Summer 06: Application not funded (249)• Strengths:
– Institutional commitment– Training section– Bioethics– Creation of physical home
• Weaknesses:– organization complexity– lack of details about implementation/integration– all MDs in leadership– unrealistic about potential problems– poor bioinformatics

How has the University of Minnesota responded to the RFA?
• October 06: Second RFA released• 10/06-12/06: Draft prepared and rejected -
decided to defer to 10/07• 3/07: Third RFA released• Plan to re-submit October 2007

CTSA ReviewEach application is assigned 8 reviewers and each reviewer is assigned one of following areas1. Significance, Approach, Innovation, Environment, and
Implementation2. Staffing, Governance, Institutional Commitment,
Evaluation Plans3. Biomedical Informatics4. Clinical Research Design and Biostatistics,Community
Engagement, Regulatory Knowledge and Support5. Translational Technologies and Resources, Pilot
Studies6. Training7,8. Overall (Integration, Impact, Anticipates problems)
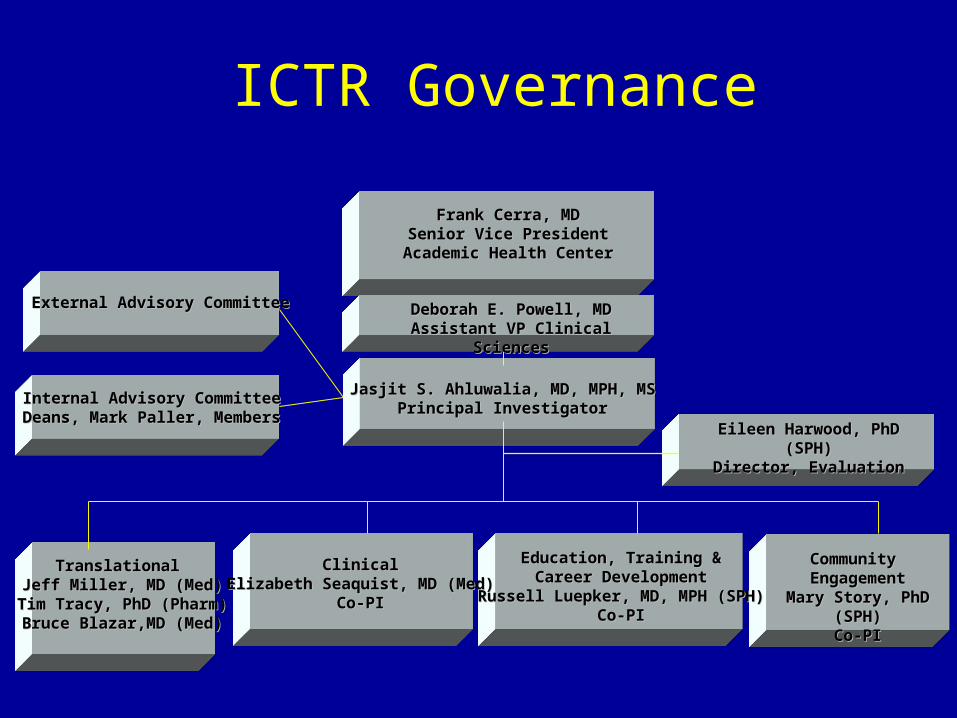
Jasjit S. Ahluwalia, MD, MPH, MSJasjit S. Ahluwalia, MD, MPH, MSPrincipal InvestigatorPrincipal Investigator
Translational Translational Jeff Miller, MD (Med)Jeff Miller, MD (Med)
Tim Tracy, PhD (Pharm)Tim Tracy, PhD (Pharm)Bruce Blazar,MD (Med)Bruce Blazar,MD (Med)
ClinicalClinicalElizabeth Seaquist, MD (Med)Elizabeth Seaquist, MD (Med)
Co-PICo-PI
Community Community EngagementEngagement
Mary Story, PhD (SPH)Mary Story, PhD (SPH)Co-PICo-PI
Education, Training &Education, Training &Career DevelopmentCareer Development
Russell Luepker, MD, MPH (SPH)Russell Luepker, MD, MPH (SPH)Co-PICo-PI
External Advisory CommitteeExternal Advisory Committee
Frank Cerra, MDFrank Cerra, MDSenior Vice PresidentSenior Vice President
Academic Health CenterAcademic Health Center
Internal Advisory CommitteeInternal Advisory CommitteeDeans, Mark Paller, MembersDeans, Mark Paller, Members
Eileen Harwood, PhD (SPH)Eileen Harwood, PhD (SPH)Director, EvaluationDirector, Evaluation
Deborah E. Powell, MDDeborah E. Powell, MDAssistant VP Clinical SciencesAssistant VP Clinical Sciences
ICTR Governance
CTSA Challenges• Balance - Finding balance between describing what you do well
and what needs to change is difficult (i.e., Why should NIH give us grant if we already do everything well? vs. If we describe everything that needs changing, it seems negative.)
• Perspective – All investigators believe what they do is most innovative and deserves highest priority. CTSA includes implicit judgment (e.g., In what order does one list functions? How does the budget get allocated?)
• Budget - $6 million additional per year is not enough (especially since only $4 million is direct costs) to do all that is asked for in the RFA
• Change – It is difficult to acknowledge that what we have been doing is not optimal (Clinical Research TF helped) and figuring out how to change it is even more so. Most people will agree to change in the abstract – the devil is in details.

CTSA Lessons Learned
• Be flexible – good ideas can come after initial decisions have been made
• Listen to the skeptics – they will make your grant stronger• Provide a structure for sections early on and don’t let
authors argue that the structure “doesn’t fit for my section”• Make a timeline that allows time for internal and external
review and stick to it• It’s never too early to begin gathering biosketches• The best sections were drafted early and went through
many reviews• The best sections incorporated ideas from many
individuals• Identify reviewers that are not intimately involved with the
grant to provide feedback on ideas and to proof read
State of clinical and translational research 2013
• Clinical and translational research will be supported by a robust network of centers supported by CTSA program
• Funded centers will collaborate with each other and with unfunded institutions in their region to speed discovery into practice
• Clinical and translational research will become the preferred career path for talented health professionals

What don’t we have?• Current clinical research space inadequate-temporary,
small, and at Children’s-- nonexistent• Clinical research training programs still being
developed-clinical research mentor pool still small• Clinical research processes are not transparent-no one
place, no one person knows everything• Processes not efficient: time to contract and time to final
IRB approval (benchmark<4-6 weeks), biotechnology licensing, separate IRB approval and credentialing of research personnel at Children’s time consuming

What don’t we have?• New collaborations slowed by many factors:
faculty #, type, or difficult to find• No facility to manufacture drugs• Mixed messages on value of interdisciplinary
clinical research: no space assigned for funded clinical research, only PI given ‘credit’ for research performed by investigator teams
• Accountability less than clear: who is “in charge” of clinical research?
What don’t we have?• Serving the larger community
– Health data in our hospital, county, or state not easily accessible to evaluate or study health concerns or outcomes
– CTSA RFA: need to show how we can move basic research all the way to community implementation and take community concerns back to the laboratory- What will it take to do this?
Securing an NIH CTSA• A physical and administrative “home” for Clinical research
across UNMC• Mentored interdisciplinary clinical research training• New ways of organizing our research enterprise to speed
up translation from bench <=> bedside <=> community: better access to available data, new and innovative ways to gather new data, teams to address health issues, minority and rural community engagement
• This work can only be accomplished by a team of individuals who have been given institutional authority and committed to UNMC’s success
A lot is at stake
• The final 60 CTSAs will be the driving force behind NIH-funded clinical research for the next 40 years
• The CTSA is now the model of how clinical research should be done => UNMC needs to transform its research enterprise just to “keep in the game”