enhanced recovery after surgery programme - wales.nhs.uk care pathway_ugi... · this integrated...
TRANSCRIPT

Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
1
Enhanced Recovery after Surgery Programme
Subtotal / Partial Gastrectomy Integrated Care Pathway
Age:
Consultant:
Pre Operative Assessment Outcome:
Suitable for Day of surgery admission (DOSA)? Y N
Day before Surgery Admission (DBSA) Y N Admit .........days pre-op.
Critical care bed required post-op?
Booked Yes □ No □
Y N Level 2 or 3
Is the patient allergic to latex? Y N If Yes theatre informed:
Date:
Time:
Is the patient’s BMI > 40? Y N If Yes theatre informed:
Date:
Time:
Does the patient need to be first on list? Y N
Is the patient suitable for carbohydrate loading Y N
Assessing Nurse: Signature: Date:
Date of Admission:
Operation:
Date of surgery:
Predicted date of discharge
(PDD):
Actual date of
discharge:
Length of stay
Removed from pathway
Date: Reason
Addressograph
Unit no.: DoB:
Name:
Address:
Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
2
1. This Integrated Care Pathway (ICP) is a multidisciplinary document and replaces all other documentation to
form the patient’s sole record of care. It is intended as a guide to good practice and is evidence based. (NB
point
2. The ICP is not a rigid document and clinicians are free to use their own professional judgement as appropriate,
recording as a variance any alterations to the practice outlined, or any deviation from the expected plan of
treatment.
3. When using the pathway, sign yourself on below stating your discipline. Always use black ink
4. All sections should be fully completed. Please follow all instructions.
5. It is essential that all entries are signed and dated as indicated. Sign only for care that YOU have carried out or
outcomes that have been met.
6. When completing the pathway insert:
� Your initials if the outcome / plan has been met
� A X if it has not been met
� A 0 If the outcome / plan is not applicable to that patient
7. Any variation from the expected plan/ outcome of care: anything that happens that is not expected outcome /
plan is recorded as a VARIANCE.
8. In recording variances, please give as much information as possible
9. All variances must be recorded on the variance / multi-disciplinary notes sheet. Document the variance code
for the relevant action / outcome alongside the written detail of the variance
10. The Cardiff and Vale UHB generic risk assessment book must be used alongside this ICP to ensure that
patients undergo appropriate risk assessment during their stay
11. It may also be appropriate to use a nursing care plan as an adjunct to the pathway. Please make a record
below of the care plans in place and ensure each one is evaluated TDS in the multidisciplinary notes.
All patients Generic risk assessment book
Diabetic patients Diabetes core care plan
Relevant acute pain team care
plans
Epidural care plan
PCA care plan
Intrathecal morphine care plan
Patients with Jejunostomy tube Jejunostomy feeding care plan
12. If an outcome of care is not applicable to that patient write (N/A)

Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
3
13. If the pathway is no longer suitable for a patient, discontinue the pathway, document why as a variance and
fill in the date in the table on page 1.
SIGNATURE PRINT NAME INITIALS JOB TITLE Bleep
/Extension

Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
4
SOCIAL ASSESSMENT
Patient lives with:
Are they fit and well? Yes � No
Are they coping at home at present? Yes � No �
Are there stairs / steps in the home? Yes � No �
Does the patient care for anyone? Yes � No �
If Yes who?
Does the patient have a carer? Yes � No �
If Yes who?
Would patient or family like to see a Social
Worker Yes � No � If yes, reason:
Is OT assessment required Yes � No �
Does the patient have complex discharge needs?
Yes � No �
Are patient and family happy with social
circumstances and to organise own support
on discharge?
Yes � No �
Are there any adaptations / rails in the home?
Yes � No �
Date: Nurse signature:
Patient details Patient Known as:
Home telephone: Mobile telephone:
Email address Marital status:
Occupation Religion
1st Language Translator required Yes � No �
First contact Second contact
Name: Name:
Relationship to patient: Relationship to patient:
Address:
Address:
Home telephone: Home telephone:
Work telephone: Work telephone:
Mobile telephone: Mobile telephone:
To be contacted:
In an emergency: Yes � No �
At night: Yes � No �
To be contacted:
In an emergency: Yes � No �
At night: Yes � No �
GP details
Telephone number:
Practice address:
If social work referral required / discharge is complex complete Unified Assessment forms
Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
5
Presenting Symptoms: (include dysphagia, vomiting, weight loss, anaemia, mass, appetite loss, pain, GI
bleed)
Pre-op chemotherapy? yes ☐☐☐☐ no ☐☐☐☐ regime regime regime regime ☐☐☐☐ date completeddate completeddate completeddate completed ☐☐☐☐
Pre-op chemoradiotherapy? yes ☐☐☐☐ no ☐☐☐☐ date completeddate completeddate completeddate completed ☐☐☐☐
Previous
anaesthetic problems:
Family history of anaesthetic problems:
Previous motion sickness or post-operative nausea/vomiting: yes ☐☐☐☐ no ☐☐☐☐
Pre-operative clerking
Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
6
Cardiovascular Y N Expand here:
MI □ □
Angina / Chest pain □ □
Hypertension □ □
AF / Arrhythmia □ □
Heart failure □ □
Stroke / TIA □ □
Previous cardiac surgery □ □
Coronary artery stents □ □
Pacemaker □ □
DVT / PE □ □
Palpitations / faints / syncope □ □
Rheumatic fever □ □
Peripheral vascular disease □ □
Respiratory
Asthma □ □
COPD / bronchitis / emphysema □ □
TB □ □
Sleep apnoea / snoring □ □
Cough □ □ Productive □ Haemoptysis □
Endocrine
Diabetes □ □ diet □ tablets □ insulin □
Thyroid disease □ □
Haematological
Excessive bleeding / bruising □ □
Anaemia / blood disorders □ □
Sickle cell disease □ □
GI/GU
Liver disease / jaundice / hepatitis □ □
Heartburn / acid reflux □ □
Hiatus hernia □ □
Stomach / duodenal ulcer □ □
Past medical history

Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
7
Kidney / bladder problems □ □
CNS
Epilepsy / fits □ □
Neurological disorder □ □
Anxiety / Depression □ □
Psychiatric Illness □ □
Other
Arthritis/joint problems □ □
LMP …………….. Could you be pregnant? Yes No
Inoculation risk □ □
Other □ □ Maximum walking distance on flat …………… (yards / metres)
□ bed bound □ wheelchair bed to chair □ 5m end of room
□ 25m end of ward □ 100m length of football pitch □ 400m
□ 2km 30min walk □ >2km normal pace, no exercise limitation ��
Walking limited by □ joint pain □ breathing □ chest pain □ leg pain
□ balance □ fatigue □ other
Do you get SOB walking up a flight of 12 stairs? Y N Do you get chest pain walking up a flight of 12 stairs? Y N Orthopnoea Y N (State no. of pillows ……..) PND Y N Peripheral Oedema Y N
Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
8
Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
9
Abdomen
WEIGHT LOSS:
Weight pre illness:
Weight loss in KG:
Time frame of weight
loss:
Hand Signs:
Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
10
Neurological
Investigations ordered (*=essential)
□ FBC* Hb: Plat: WCC: MCV:
□ U&E* Na: K: Ur: Creat:
□ G+S*
□ LFT*
□ Coagulation screen
□ Blood Glucose
□ HbA1c
□ TFT
□ Sickle cell
□ Arterial blood gases
□ MSU
□ MRSA swabs
□ ECG
□ CXR
□ Echocardiogram
□ Pulmonary function tests
□ CPX
□ Other
* NB: Please document FBC, U+E results and any other abnormal results above
Possum-O
Calculate Possum-O on-line - http://www.riskprediction.org.uk/op-index.php
Score = ………………….
Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
11
Signature ………………… Date ……………..
Commence Drug chart
Prescribe the following, unless contraindicated for this patient
Complete thromboprophylaxis risk assessment Yes ☐
Enoxaparin (Clexane) Yes ☐ N/A ☐
� dose as per thromboprophylaxis risk assessment
� Commence at 1800 if admitted day before surgery (Do not give on morning of surgery)
Thromboembolism
Anti-embolism stockings (AES) Yes ☐ N/A ☐
Bowel Preparation
Refer to consultant instruction
Is bowel prep indicated and required Yes ☐ No ☐
Picolax prescribed if indicated in management plan Yes ☐ No ☐
Picolax Prescribed if indicated at management plan Yes ☐ N/A ☐
Aspirin/Clopidogrel - stop 7days before surgery (discuss with anaesthetist)
Yes ☐ N/A ☐
Continue patients other usual medications (See anaesthetic guidelines on
‘Management of Perioperative Medicines’) Yes ☐ N/A ☐
Warfarin – discuss management with POAC anaesthetist Yes ☐ N/A ☐
Analgesia Paracetamol 1g qds (IV/oral) from post-op day 0 Yes ☐
Anti-emetics Cyclizine 50mg tds IV/oral Yes ☐ Ondansetron 4mg tds IV/oral Yes ☐
Antibiotics Co-Amoxiclav 1.2mgs IV on induction Yes ☐
Metronidazole 500mg IV on induction Yes ☐
Oxygen Oxygen therapy continually post-operation Yes ☐
Nutrition Carbohydrate loading: Refer to ward protocol Yes ☐ N/A ☐ document to be given 2-3 hours before surgery on drug chart � NB: Do not give within 4 hours of operation if previous gastric surgery or
severe reflux
Contra indications to NSAIDs Caution to NSAID use
Renal impairment Pregnancy / breast feeding

Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
12
History of peptic ulceration Asthma
Hypersensitivity to NSAIDs CCF
Asthma hypersensitivity to aspirin Concurrent anti-coagulant therapy
Coagulopathy Hepatic impairment
Preoperative nursing assessment
Baseline assessment to be added in here
Doctors name: Signature: Date:

Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
13
Baseline assessment to be added in here
Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
14
Risk assessments completed and documented in generic risk assessment book
Initials
Waterlow Pressure ulcer risk assessment tool
Malnutrition risk assessment (WAASP) Weight……....Kgs (actual not estimated)
Pat-e-bac risk assessment
Falls and bedrails Risk assessment
Thromboprophylaxis risk assessment (doctor to complete)
Unified Assessment: Not to be completed for simple discharges
Patient education record:
Relative/carer present: Yes ☐ No ☐ Relationship to patient:
Teaching provided. Date: Yes N/A Initials
Understanding of Enhanced Recovery Programme & patient’s role
Fasting instructions
Pain control
Bowel preparation
Mobilisation post-op
Carbohydrate loading
Pre and post operative dietary advice
Nutritional supplements
Thromboprophylaxis therapy
Deep breathing, leg exercises and preventing pressure ulcers
Smoking cessation advice
Written information provided:
Enhanced recovery programme
Surgery
Anaesthesia/analgesia
Discharge plans discussed
Family/social support plans for discharge discussed
Patient contract signed
Patient Diary given
Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
15
Referrals
Y
Reason for
referral
Name/contact
referred to
Anaesthetist for notes review
Upper GI CNS
Dietician
Physiotherapist
Occupational Therapist
Acute pain team
Social services
Smoking cessation
Other
MRSA screen:
Full MRSA screen required if patient is being admitted from a nursing home or another hospital,
or if they are known to have had MRSA in the past:
MRSA screen sent: Yes ☐ No ☐ Not applicable ☐
Name of pre-assessment nurse:
Signature: Date

Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
16
Physiotherapy – Preoperative Check List
Yes No Reason
Pain relief, in relation to Physiotherapy
Attachments, in relation Physiotherapy
Suitable clothing and footwear
Getting in and out of bed
Early mobilisation
Generic exercises
Breathing exercises taught and practiced
Supported cough
Return to normal activities
Driving
Booklet provided
Scholes Score: High Low
At risk of PPC?
Chest assessment : complete for all patients with a high Scholes score, chronic chest disease or cough
HABAM Score: Balance Transfers Mobility
At risk of mobility problems?
Taking into account complete assessment findings - is the Patient for routine post- operative Physiotherapy review?
Sign: Date: Print:
Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
17
Nutrition and Dietetic - Preoperative Checklist
Yes No Reason
WAASP completed
MUST completed
SGA completed
Advised on carbohydrate loading
Food fortification advice
Advised on need for nutritional supplements x 3 day and explain different types available
Post operative dietary advice - early oral diet
Weight history and anthropometric assessment
Record of dietary intake
Diet sheet provided
Snacks and high protein options discussed
Any special dietary requirements?
Catering informed of special dietary requirement (as appropriate)
Nutritional requirements calculated Energy…………kcal Protein……….g
Malnutrition Risk Screening - WAASP
W A A S P Overall Risk of
Malnutrition
Malnutrition Universal Screening Tool - MUST
Step 1 Step 2 Step 3 Overall risk of Malnutrition
Sign: Date: Print:

Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
18
Anaesthetic /CPX Clinic Revised Cardiac Risk Index Score: Score 1 point for each variable:
High-risk surgery (includes any intraperitoneal, intrathoracic, or suprainguinal vascular procedures)
History of ischemic heart disease (history of MI or a positive exercise test, current complaint of chest pain considered to be secondary to myocardial ischemia, use
of nitrate therapy, or ECG with pathological Q waves; do not count prior coronary revascularization procedure unless one of the
other criteria for ischemic heart disease is present).
History of heart failure
History of cerebrovascular disease
Diabetes mellitus requiring treatment with insulin
Preoperative serum creatinine >177 µmol/L
TOTAL
CPX test Y N
ASA status 1 2 3 4 5
Peri-operative medicines instructions:
Continue all medicines on day of surgery ☐ or Continue all meds except list below ☐
Drug chart amended re: above instructions Yes ☐ No ☐
Anaesthetist name & signature: Date:

Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
19

Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
20
Variances/ Multidisciplinary Notes
Please record all variances or multidisciplinary notes below
Date, Time and
Variance code
Details, reason and action taken
Signature and
bleep number

Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
21
Pre-operative Admission Day. Date:……………
Doctor: pm night Variance Code
Record changes in health status since POA in multidisciplinary notes PDr1
Record changes in medicines since POA in multidisciplinary notes PDr2
Check consent form has been signed and white copy has been given to patient PDr3
X-rays and ECG available PDr4
Investigations completed and results available PDr5
FBC/U&E/LFT performed within 14 days? Yes ☐ No ☐
If no then repeat on admission Yes ☐ N/A ☐
PDr6
If patient on warfarin INR check Yes ☐ Anaesthetist informed if INR > 1.4 Yes ☐ PDr7
G+S sample sent (2nd G+S sample for electronic blood issue) PDr8
Prescription chart written PDr9
Bowel preparation: Discussed with consultant / Registrar and prescribed if required – please make a record on variance sheet if required
PBp
On admission:
Patient fully aware of planned surgery PT1
Patient orientated to ward [NB: access to nutritional supplements] PT2
Repeat observations. (T, P, R, BP, SpO2 + weight) POb
Enoxaparin given at 1800 hours PM1
If prescribed patient measured for Anti-embolic stockings and stockings provided PAes
Identity band in place, patient details confirmed PN1
Referrals: Referred to pain control nurse PNr1
Inform physiotherapist of admission PNr2
Inform dietician of admission PNr3
Referred to Social worker, OT and Discharge liaison if required
Please document these referrals on variance sheet PNr4
Nutrition
Normal diet and fluids – stop diet 6 hours pre theatre: Time diet to stop:
(Unless undergoing bowel preparation) ………… PNU1
Bowel preparation: Administered as prescribed PM3
Record weight (kg) Insert weight………..(KG) PNW
Recalculate Malnutrition risk assessment and record changes (WAASP) PNA
Ensure Plus x2 supplement drinks are given 1 ☐ 2 ☐ PNS
If on the morning theatre list - Carbohydrate loading give 4 x 200ml ‘pre-op’
drinks evening before surgery 1 ☐ 2 ☐ 3 ☐ 4 ☐ NIGHT STAFF:NIGHT STAFF:NIGHT STAFF:NIGHT STAFF: please refer to operation day 0 re: administration of ‘Pre-Op’ drinks x 2 between 05.00 and 06.00. NB: Do not give within 4 hours of operation
if previous gastric surgery or severe reflux
PClam
Insert initials if achieved, a x if
not achieved and 0 if not
applicable

Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
22
If on the afternoon theatre list: Commence carbohydrate loading as soon as patient awake on day of surgery.
PClpm
Patient Education
Importance of mobility post op and deep breathing and limb exercises PEm
Surgery / treatment plan PST
Importance of post op nutrition and early enteral feeding PN2
Patient’s and relatives’ roles in recovery process PEr
Discharge arrangements PDis
Operation Day (day 0) Date:...................
Preoperative: Estimated time of surgery:
Yes Signature
Doctor :
Confirm G+S sample sent (2nd G+S sample for electronic blood issue)
No food for 6 hours prior to surgery
If morning list - Carbohydrate loading x2 ‘Pre-op’ drinks and clear fluids (up to 2 hr before start of theatre list) NB: Do not give within 4 hours of operation if previous gastric surgery or severe reflux
If afternoon list – ‘Pre-op’ drinks x6 to commence as soon as awake. Up to 2hrs before start of theatre list then nil by mouth for 2hrs. NB: Do not give within 4 hours of operation if previous gastric surgery or severe reflux
Theatre check list completed
Wearing AES (Anti-embolism stockings)
Patient’s usual medications given as prescribed
(omit ACE inhibitors or Angiotensin II Receptor blockers
on day of surgery)
Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
23
Operation Notes Date: Consultant: Surgeon 1: Surgeon 2: Surgeon 3: Surgeon 4: Anaesthetist: Scrub Nurse: Anaesthetic time started: Time into theatre: Operation time started: Time finished: Site of cancer: Operation title: Cancer treatment intent:
Blood loss:
HDU/ICU admission (please circle): Planned Unplanned
Directions for ward staff re acceptable hourly urine estimation, diet and fluids over next 24 hours:
Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
24
Yes No Long-acting sedative premed avoided Seen in preop Anaesthetic Clinic CPX test performed DOSA Long-acting sedative pre-med avoided Carbohydrate loading taken 2-3hours preop Spinal Intrathecal Diamorphine Intrathecal Diamorphine with 0.5% heavy Bupivacaine TAP block Epidural Intraop Dexamethasone given as antiemetic Intraop Ondansetron given as antiemetic Bair Hugger Temp probe Warmed iv fluids Temp on leaving theatre Antibiotics prior to skin excision Cardiac output monitor used Volume (mls)
Total intraop crystalloid volume given Total intraop colloid volume given
Anaesthetic data (to be completed in theatre by anaesthetist

Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
25
Post op: Day 0 (Day of operation) Date:....................
Plan: Pain well controlled, IV fluids, oxygen, catheter insitu, oral fluids and mobilise
PM Night Variance
Code
Observations and EWS score completed ½ hrly for 2 hrs, 1 hrly for 2 hrs and then
2 hrly. Actions taken as per EWS chart: document actions on variance sheet 0Ob
Deep breathing promoted, patient able to deep breath and cough. 0Db
Sputum clear 0Sp
Oxygen in place as prescribed and oxygen saturations maintained above 94%-
97%
0O2
Fluid balance chart completed hourly 0Fb
Administer IV fluids (1.5L Hartmanns over 24 hrs = 62.5 mls/hr) Follow
GIFTASUP recommendations
0ivi
Hourly catheter measurements (maintain 0.3 ml/kg/hour averaged over 4 hours)
Expected 1hourly output =…………….ml/hr Expected 4 hourly rate: …………..
0Uc
Oral fluids tolerated
(Ensure Consultant has documented on operation notes that patient able to drink)
0Of
Ensure Plus TDS and Ensure Two Cal 50ml QDS 0Su
Patient checked for signs of paralytic ileus – ie: nausea / vomiting, increased pain,
pulse >100 and/or abdominal distension – nil present
0Pi
Pain assessed with each set of observations at rest and deep breathing and pain well controlled (0-1) ( If pain not well controlled actions taken as per protocol and relevant care plans (PCA / epidural) and documented on variance sheet)
0Pa
Epidural site: checked 8 hourly, no redness, oozing or swelling present ( If redness / oozing / swelling refer to per protocol and epidural care plan and document on variance sheet)
0Ep
If epidural insitu: straight leg raises checked 4 hourly – patient able to raise leg (If patient unable to SLR refer to protocol and epidural care plan and document on variance sheet)
0Slr
NG tube insitu on free drainage only – no fresh blood noted
Do NOT aspirate or repass a tube without consultant direction 0Ng
Nausea assessments with each set of observations – nausea well controlled
0Na
VIP score completed for all venflons insitu 0Vip
Wound observed when observations recorded - no bleeding / signs of infection
0W
Insert initials if achieved,
a x if not achieved and
0 if not applicable

Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
26
PM Night Variance
Code
Abdominal drains checked, drainage measured and recorded before 12MN, blood
and haemoserous fluid draining volume is less than 200 mls
Number of drains insitu: …………………….
0Ad
6 hours after return to ward patient sat out of bed (only if this is before 7pm).
Sit in chair for 30 mins: Time of return to ward:…………………..
Time sat out in chair: ………………… to ………………
0Si
Patient assisted to reposition 2 hourly by day / ………….. hourly by night 0Rep
Pressure areas checked all blanching with no discolouration / broken areas 0Pr
AES in situ (Legs, feet and heels checked all blanching and no discolouration / broken areas present) 0Aes
Waterlow, Pat-e-bac, falls and WAASP risk assessments recalculated post op 0Ra
Doctor: Review drug chart, change medications to IV whilst NBM 0Dr3
Variances/ Multidisciplinary Notes
Please record all variances or multidisciplinary notes below
Date, Time and
Variance code
Details, reason and action taken
Signature and
bleep number
Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
27
Variances/ Multidisciplinary Notes
Please record all variances or multidisciplinary notes below
Date, Time and
Variance code
Details, reason and action taken
Signature and
bleep number

Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
28
Plan: Oral fluids, good pain control, sitting out in chair for 6 hours and 3 x 60m walks
am pm night Variance Code
Observations and EWS score recorded 2 hourly. Actions taken as per EWS chart: document actions required on variance sheet
1Ob
Deep breathing promoted, patient able to deep breathe and cough. 1Db
Sputum clear 1Sp
Oxygen in place as prescribed and oxygen saturations maintained above 94%- 97%
1O2
Fluid balance chart completed hourly 1Fb
Flatus passed 1Fl
Bowels opened 1Bo
Administer IV fluids (1.5L Hartmanns over 24 hrs = 62.5 mls/hr) Follow GIFTASUP recommendations
1ivi
VIP score completed for all venflons in situ – Score 0 1Vip
Catheter insitu - Monitor urine output 1 hourly (maintain minimum of 0.3 ml/kg/hour averaged over 4 hours)
1Uc
Ensure Plus TDS and Ensure Two Cal 50ml QDS 1Su
Taking oral fluids well - aim for 2000ml oral fluid over 24hours 1Of
Weight recorded ………Kgs 1Wt
Build up to normal diet as tolerated maintain food chart (encourage patient to record this)
1Nd
Patient checked for paralytic ileus - i.e. nausea/vomiting, increased pain, pulse> 100 and/or abdominal distension, nil present
1Pi
Pain assessed 2 hourly at rest and deep breathing and pain well controlled (0-1)
( If pain not well controlled actions taken as per protocol and relevant care plans (PCA / epidural) and documented on variance sheet)
1Pa
Epidural site: checked 8 hourly, no redness, oozing or swelling present
( If redness / oozing / swelling refer to per protocol and epidural care plan and document on variance sheet)
1Ep
If epidural insitu: straight leg raises checked 4 hourly – patient able to raise leg (If patient unable to SLR refer to protocol and epidural care plan and document on variance sheet)
1Slr
NG tube insitu and reviewed by consultant, haemoserous fluid / bile
draining. Less than 200 mls drained over 4 hour period
(seek surgical review if > 200mls drained over 4 hours)
1Ng
Nausea assessed 2 hourly and actions taken as per protocol 1Na
Hygiene needs met including catheter care 1Hy
Wound observed no bleeding / signs of infection noted 1W
Abdominal drains monitored and reviewed by Registrar / Consultant 1Ad
Out of bed x 2 times in total and record length of time sat out
1 ☐ ……………… 2 ☐ ……………… 1Sc
Post-op: Day 1. Date:............................
Insert initials if achieved,
a x if not achieved and
0 if not applicable
Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
29
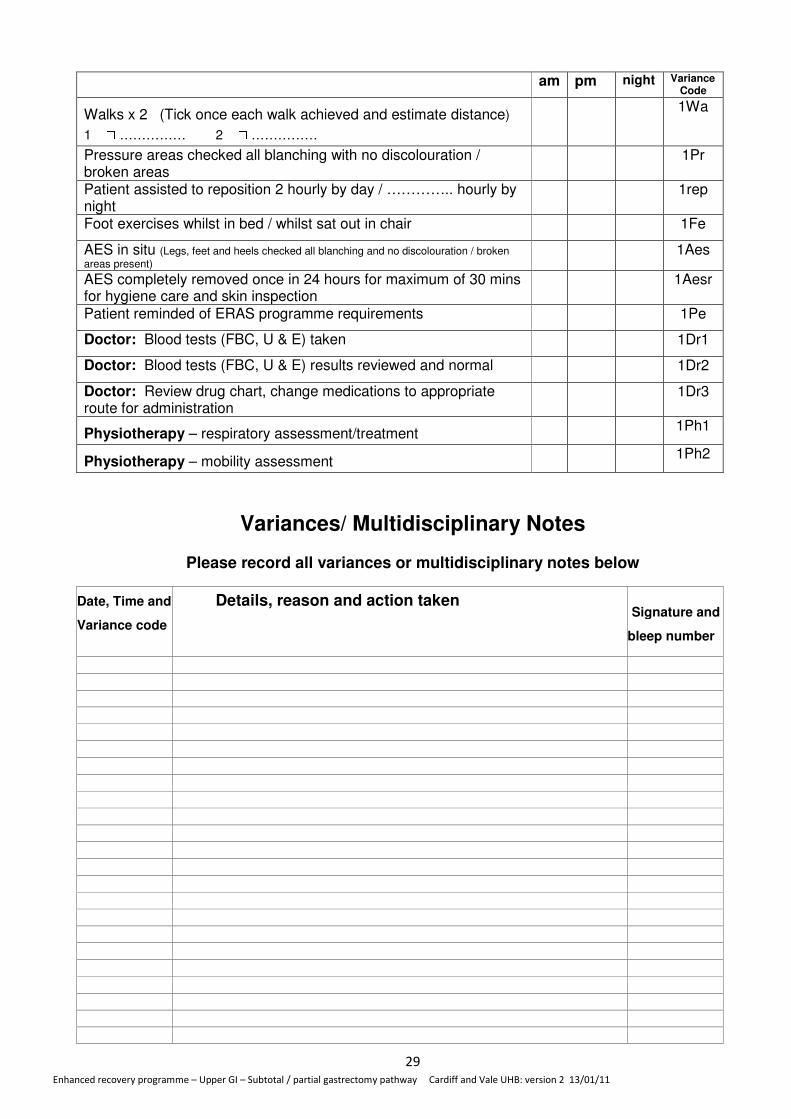
am pm night Variance
Code
Walks x 2 (Tick once each walk achieved and estimate distance)
1 ☐ …………… 2 ☐ ……………
1Wa
Pressure areas checked all blanching with no discolouration / broken areas
1Pr
Patient assisted to reposition 2 hourly by day / ………….. hourly by night
1rep
Foot exercises whilst in bed / whilst sat out in chair 1Fe
AES in situ (Legs, feet and heels checked all blanching and no discolouration / broken
areas present) 1Aes
AES completely removed once in 24 hours for maximum of 30 mins for hygiene care and skin inspection
1Aesr
Patient reminded of ERAS programme requirements 1Pe
Doctor: Blood tests (FBC, U & E) taken 1Dr1
Doctor: Blood tests (FBC, U & E) results reviewed and normal 1Dr2
Doctor: Review drug chart, change medications to appropriate route for administration
1Dr3
Physiotherapy – respiratory assessment/treatment 1Ph1
Physiotherapy – mobility assessment 1Ph2
Variances/ Multidisciplinary Notes
Please record all variances or multidisciplinary notes below
Date, Time and
Variance code
Details, reason and action taken
Signature and
bleep number

Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
30
Variances/ Multidisciplinary Notes
Please record all variances or multidisciplinary notes below
Date, Time and
Variance code
Details, reason and action taken
Signature and
bleep number

Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
31
Postoperative Morbidity Survey (POMS) Day 1 post-op
* If no scores above then please state reason why patient still in hospital:
Morbidity type Criteria Tick if
present*
Pulmonary Has the patient developed a new requirement for oxygen or respiratory support.
Infectious Currently on antibiotics and/or has had a temperature of
>38°C in the last 24hr.
Renal Presence of oliguria <500 ml/24 hr; Increased serum creatinine (>30% from preoperative level); Urinary catheter in situ.
Gastrointestinal Unable to tolerate an oral diet for any reason including nausea, vomiting, and abdominal distension.
Use of antiemetic.
Cardiovascular Diagnostic tests or therapy within the last 24 hr for any of the following:
• new myocardial infarction or ischemia,
• hypotension (requiring fluid therapy >200 mL/hr or pharmacological therapy),
• atrial or ventricular arrhythmias,
• cardiogenic pulmonary oedema,
• thrombotic event (requiring anticoagulation).
Neurological New focal neurological deficit, confusion, delirium, or coma.
Haematological Requirement for any of the following within the last 24 hr: packed erythrocytes, platelets, fresh-frozen plasma, or cryoprecipitate.
Wound Wound dehiscence requiring surgical exploration or drainage of pus from the operation wound with or without isolation of organisms.
Pain New postoperative pain significant enough to require IV or IM opioids or regional analgesia.
Date: Doctor’s signature: Bleep no:

Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
32
Plan: Oral fluids and diet, good pain control, sitting out in chair
for 8hours and 4 x 60m walks, NG tube removed
AM PM Night Variance
code
Observations and EWS chart score recorded 2hourly whilst PCA and
epidural insitu, Actions taken as per EWS recommendations: document
all actions on variance sheet
2Ob
Deep breathing promoted, patient able to deep breath and cough. 2Db
Sputum clear 2Sp
Oxygen in place as prescribed and oxygen saturations maintained
above 94%- 97%
2O2
Fluid balance chart completed 1 hourly 2Fb
VIP score completed for all venflons in situ – Score 0 2Vip
Stop IV fluids (keep cannula) 2ivi
Ensure Plus TDS and Ensure Two Cal 50ml QDS
2Su
Oral fluids tolerated well (aim for 2000ml oral fluid over 24hours)
2Of
Build up to normal diet as tolerated maintain food chart (encourage patient to record this)
2Nd
NG tube reviewed by consultant, NG removed 2Ng
Flatus passed 2Fl
Faeces passed. 2Bo
Patient checked for paralytic ileus - i.e. nausea/vomiting, increased
pain, pulse> 100 and/or abdominal distension, nil present
2Pi
Weight recorded ………Kgs 2Wt
If weight gain>3kgs request surgical review 2Wtg
Pain assessed 2 hourly at rest and deep breathing and pain well controlled (0-1) ( If pain not well controlled actions taken as per protocol and relevant care plans (PCA / epidural) and documented on variance sheet)
2Pa
Epidural site: checked 8 hourly, no redness, oozing or swelling present ( If redness / oozing / swelling refer to per protocol and epidural care plan and document on variance sheet)
2Ep
If epidural insitu: straight leg raises checked 4 hourly – patient able to raise leg (If patient unable to SLR refer to protocol and epidural care plan and document on variance sheet)
2Slr
Nausea assessed 2 hourly and anti-emetics given as per protocol if
required – nausea well controlled
2N10
Insert initials if achieved, a x if
unachieved and 0 if not
applicable
Post op day 2 Date:
Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
33
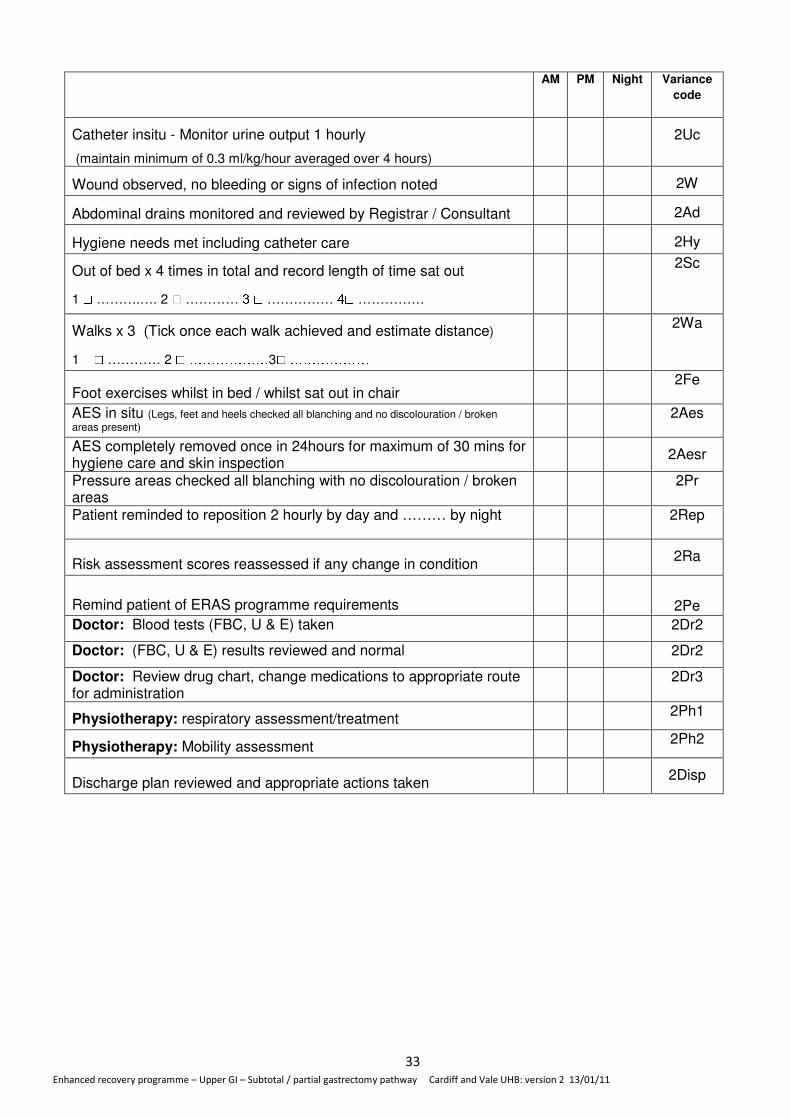
AM PM Night Variance
code
Catheter insitu - Monitor urine output 1 hourly
(maintain minimum of 0.3 ml/kg/hour averaged over 4 hours)
2Uc
Wound observed, no bleeding or signs of infection noted 2W
Abdominal drains monitored and reviewed by Registrar / Consultant 2Ad
Hygiene needs met including catheter care 2Hy
Out of bed x 4 times in total and record length of time sat out
1 ☐ ……….…. 2 ☐ ………… 3 ☐ …………… 4☐ ……………
2Sc
Walks x 3 (Tick once each walk achieved and estimate distance)
1 ☐ ………… 2 ☐ ………………3☐ ……………… 2Wa
Foot exercises whilst in bed / whilst sat out in chair 2Fe
AES in situ (Legs, feet and heels checked all blanching and no discolouration / broken
areas present) 2Aes
AES completely removed once in 24hours for maximum of 30 mins for hygiene care and skin inspection 2Aesr
Pressure areas checked all blanching with no discolouration / broken areas
2Pr
Patient reminded to reposition 2 hourly by day and ……… by night 2Rep
Risk assessment scores reassessed if any change in condition 2Ra
Remind patient of ERAS programme requirements 2Pe
Doctor: Blood tests (FBC, U & E) taken 2Dr2
Doctor: (FBC, U & E) results reviewed and normal 2Dr2
Doctor: Review drug chart, change medications to appropriate route for administration
2Dr3
Physiotherapy: respiratory assessment/treatment 2Ph1
Physiotherapy: Mobility assessment 2Ph2
Discharge plan reviewed and appropriate actions taken 2Disp

Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
34
Variances/ Multidisciplinary Notes
Please record all variances or multidisciplinary notes below
Date, Time and
Variance code
Details, reason and action taken
Signature and
bleep number

Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
35
Postoperative Morbidity Survey (POMS) Day 2 post-op
Morbidity type Criteria Tick if
present*
Pulmonary Has the patient developed a new requirement for oxygen or respiratory support.
Infectious Currently on antibiotics and/or has had a temperature of
>38°C in the last 24hr.
Renal Presence of oliguria <500 ml/24 hr; Increased serum creatinine (>30% from preoperative level); Urinary catheter in situ.
Gastrointestinal Unable to tolerate an oral diet for any reason including nausea, vomiting, and abdominal distension.
Use of antiemetic.
Cardiovascular Diagnostic tests or therapy within the last 24 hr for any of the following:
• new myocardial infarction or ischemia,
• hypotension (requiring fluid therapy >200 mL/hr or pharmacological therapy),
• atrial or ventricular arrhythmias,
• cardiogenic pulmonary oedema,
• thrombotic event (requiring anticoagulation).
Neurological New focal neurological deficit, confusion, delirium, or coma.
Haematological Requirement for any of the following within the last 24 hr: packed erythrocytes, platelets, fresh-frozen plasma, or cryoprecipitate.
Wound Wound dehiscence requiring surgical exploration or drainage of pus from the operation wound with or without isolation of organisms.
Pain New postoperative pain significant enough to require IV or IM opioids or regional analgesia.
* If no scores above then please state reason why patient still in hospital:
Date: Doctor’s signature: Bleep no:

Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
36
Plan: Eating and drinking, NG tube removed, stop IV fluids, mobile
and pain well controlled
AM PM Night Variance
code
Observations and EWSC completed 2hourly whilst PCA and epidural
insitu, 4 hourly once discontinued. Actions taken as per EWSC
document all actions on variance sheet
3Ob
Deep breathing promoted, patient able to deep breath and cough. 3Db
Sputum clear 3Sp
Stop oxygen (if mobile and oxygen saturations > 94%-97% on room
air)
3O2
Fluid balance chart completed 1 hourly 3Fb
VIP score completed for all venflons in situ – Score 0 3vip
Stop IV fluids (keep a cannula in place if required for analgesia) 3ivi
Ensure Plus TDS and Ensure Two Cal 50ml QDS
3Su
Oral fluids tolerated well (aim for 2000ml oral fluid over 24hours)
3Of
Build up to normal diet as tolerated maintain food chart (encourage patient to record this)
3Nd
Nausea assessed 2 hourly and anti-emetics given as per protocol if
required – nausea well controlled no NG tube required
3Na
Flatus passed 3Fl
Faeces passed. 3Bo
Patient checked for paralytic ileus - i.e. nausea/vomiting, increased
pain, pulse> 100 and/or abdominal distension, nil present
3Pi
Catheter insitu - Monitor urine output 1 hourly
(maintain minimum of 0.3 ml/kg/hour averaged over 4 hours)
3Uc
Weight recorded ………Kgs 3Wt
If weight gain>3kgs request surgical review 3Wtg
Consider discontinuing epidural /PCA and commencing IV / oral analgesia. (Document if epidural / PCA discontinued on variance sheet)
3Epr
Pain assessed 2 hourly at rest and deep breathing and pain well controlled (0-1) ( If pain not well controlled actions taken as per protocol and relevant care plans (PCA / epidural) and documented on variance sheet)
3Pa
Epidural site: checked 8 hourly, no redness, oozing or swelling present
( If redness / oozing / swelling refer to per protocol and epidural care plan and document on variance sheet)
3Ep
Straight leg raises checked 4 hourly – patient able to raise leg
(If patient unable to SLR refer to protocol and epidural care plan and document on variance sheet)
3Slr
Post op day 3 Date: Insert initials if achieved, a x if
unachieved and O if not
applicable
Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
37
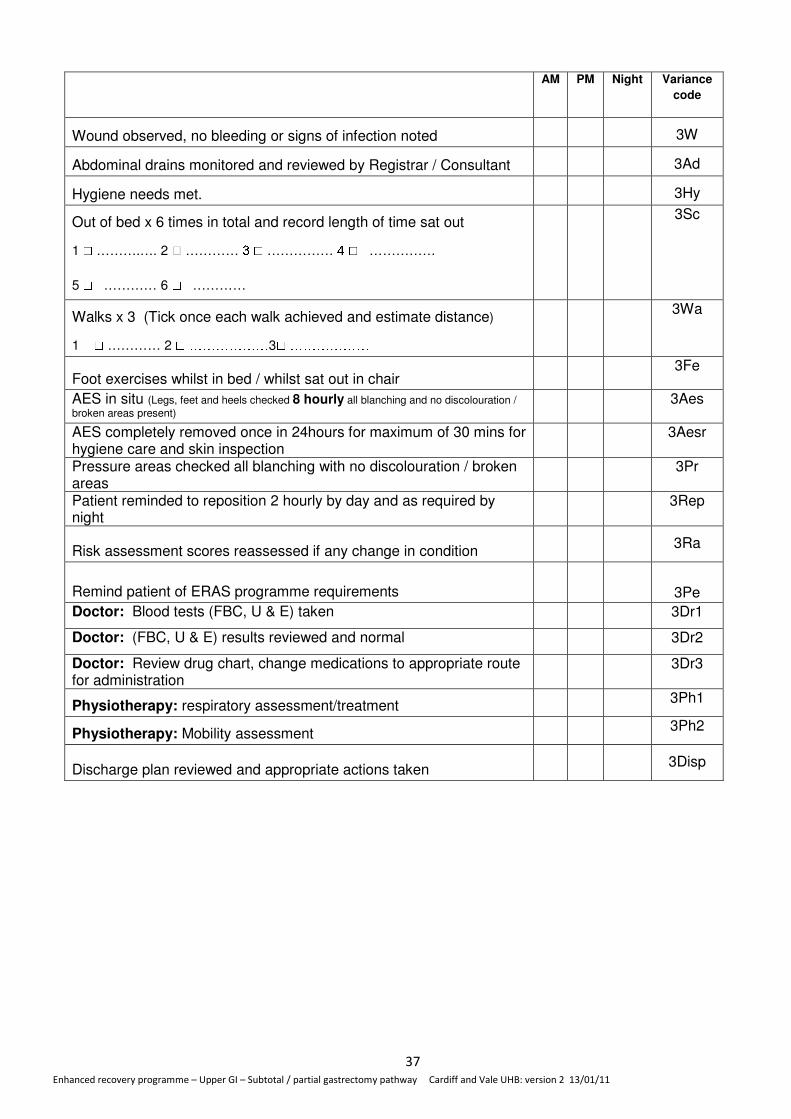
AM PM Night Variance
code
Wound observed, no bleeding or signs of infection noted 3W
Abdominal drains monitored and reviewed by Registrar / Consultant 3Ad
Hygiene needs met. 3Hy
Out of bed x 6 times in total and record length of time sat out
1 ☐ ……….…. 2 ☐ ………… 3 ☐ …………… 4 ☐ ……………
5 ☐ ………… 6 ☐ …………
3Sc
Walks x 3 (Tick once each walk achieved and estimate distance)
1 ☐ ………… 2 ☐ ………………3☐ ……………… 3Wa
Foot exercises whilst in bed / whilst sat out in chair 3Fe
AES in situ (Legs, feet and heels checked 8 hourly all blanching and no discolouration /
broken areas present) 3Aes
AES completely removed once in 24hours for maximum of 30 mins for hygiene care and skin inspection
3Aesr
Pressure areas checked all blanching with no discolouration / broken areas
3Pr
Patient reminded to reposition 2 hourly by day and as required by night
3Rep
Risk assessment scores reassessed if any change in condition 3Ra
Remind patient of ERAS programme requirements 3Pe
Doctor: Blood tests (FBC, U & E) taken 3Dr1
Doctor: (FBC, U & E) results reviewed and normal 3Dr2
Doctor: Review drug chart, change medications to appropriate route for administration
3Dr3
Physiotherapy: respiratory assessment/treatment 3Ph1
Physiotherapy: Mobility assessment 3Ph2
Discharge plan reviewed and appropriate actions taken 3Disp
Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
38
Variances/ Multidisciplinary Notes
Please record all variances or multidisciplinary notes below
Date, Time and
Variance code
Details, reason and action taken
Signature and
bleep number
Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
39
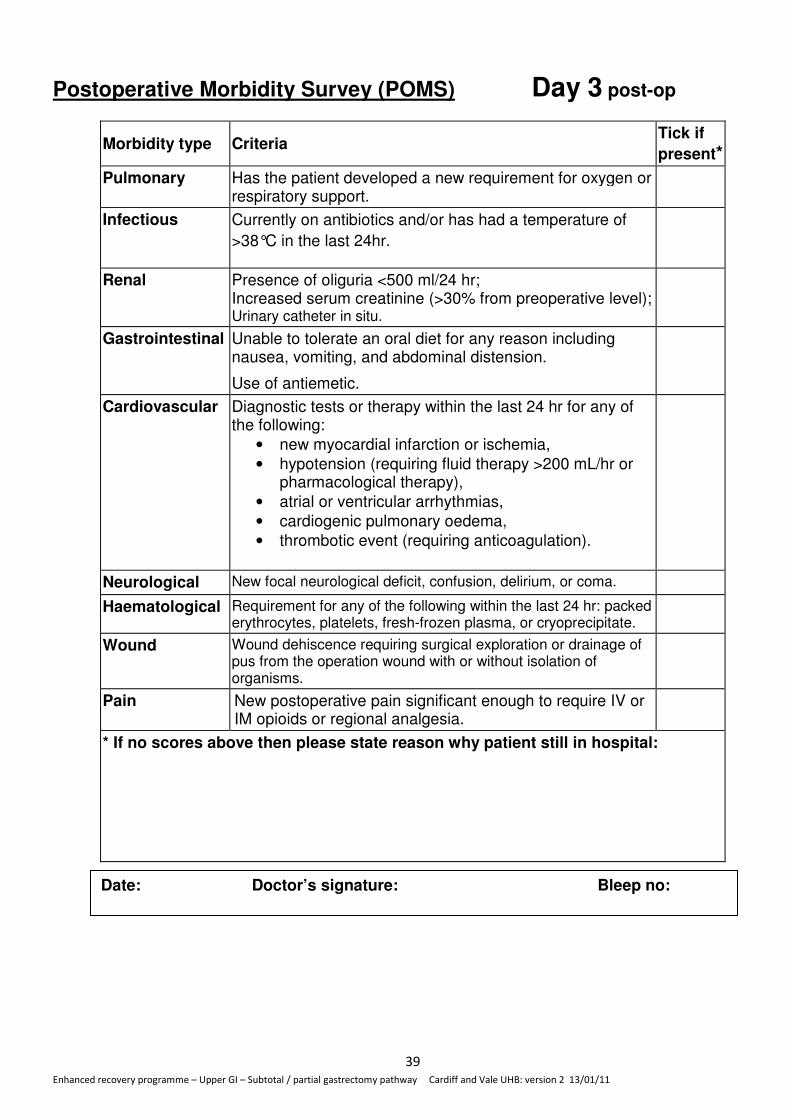
Postoperative Morbidity Survey (POMS) Day 3 post-op
Morbidity type Criteria Tick if
present*
Pulmonary Has the patient developed a new requirement for oxygen or respiratory support.
Infectious Currently on antibiotics and/or has had a temperature of
>38°C in the last 24hr.
Renal Presence of oliguria <500 ml/24 hr; Increased serum creatinine (>30% from preoperative level); Urinary catheter in situ.
Gastrointestinal Unable to tolerate an oral diet for any reason including nausea, vomiting, and abdominal distension.
Use of antiemetic.
Cardiovascular Diagnostic tests or therapy within the last 24 hr for any of the following:
• new myocardial infarction or ischemia,
• hypotension (requiring fluid therapy >200 mL/hr or pharmacological therapy),
• atrial or ventricular arrhythmias,
• cardiogenic pulmonary oedema,
• thrombotic event (requiring anticoagulation).
Neurological New focal neurological deficit, confusion, delirium, or coma.
Haematological Requirement for any of the following within the last 24 hr: packed erythrocytes, platelets, fresh-frozen plasma, or cryoprecipitate.
Wound Wound dehiscence requiring surgical exploration or drainage of pus from the operation wound with or without isolation of organisms.
Pain New postoperative pain significant enough to require IV or IM opioids or regional analgesia.
* If no scores above then please state reason why patient still in hospital:
Date: Doctor’s signature: Bleep no:

Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
40
Plan: Eating and drinking, pain well controlled, discontinue
epidural/PCA and remove urinary catheter
AM PM Night Variance
code
Observations and EWS chart completed 6 hourly. Actions taken as
per EWS recommendations: document all actions on variance sheet
4Ob
Deep breathing promoted, patient able to deep breath and cough. 4Db
Sputum clear 4Sp
oxygen saturations > 94%-97% on room air 4O2
Fluid balance chart completed 2 hourly 4Fb
VIP score completed for all venflons in situ – Score 0 4vip
Stop IV fluids (keep a cannula in place if required for analgesia) 4ivi
Ensure Plus TDS and Ensure Two Cal 50ml QDS
4Su
Oral fluids tolerated well (aim for 2000ml oral fluid over 24hours)
4Of
Build up to normal diet as tolerated maintain food chart (encourage patient to record this)
4Nd
Flatus passed 4Fl
Faeces passed. 4Bo
Patient checked for paralytic ileus - i.e. nausea/vomiting, increased
pain, pulse> 100 and/or abdominal distension, nil present
4Pi
Weight recorded ………Kgs 4Wt
If weight gain>3kgs request surgical review 4Wtg
PCA / epidural discontinued Epr
Pain assessed 6 hourly and well controlled using prescribed
analgesia
4Pa
Nausea assessed 6 hourly and anti-emetics given as per protocol if
required – nausea well controlled no NG tube required
4Na
Catheter removed if epidural removed – urine output monitored on fluid balance chart
4Uc
Epidural site satisfactory – no oozing, redness or swelling 4Ep
Straight leg raises checked 6 hourly for 24 hours post removal of epidural – patient able to raise leg (If patient unable to SLR refer to protocol and epidural care plan and document on variance sheet)
4Slr
Wound observed, no bleeding or signs of infection noted 4W
Abdominal drains monitored and reviewed by Registrar / Consultant
4Ad
Insert initials if achieved, a x if
unachieved and O if not
applicable
Post op day 4 Date:
Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
41
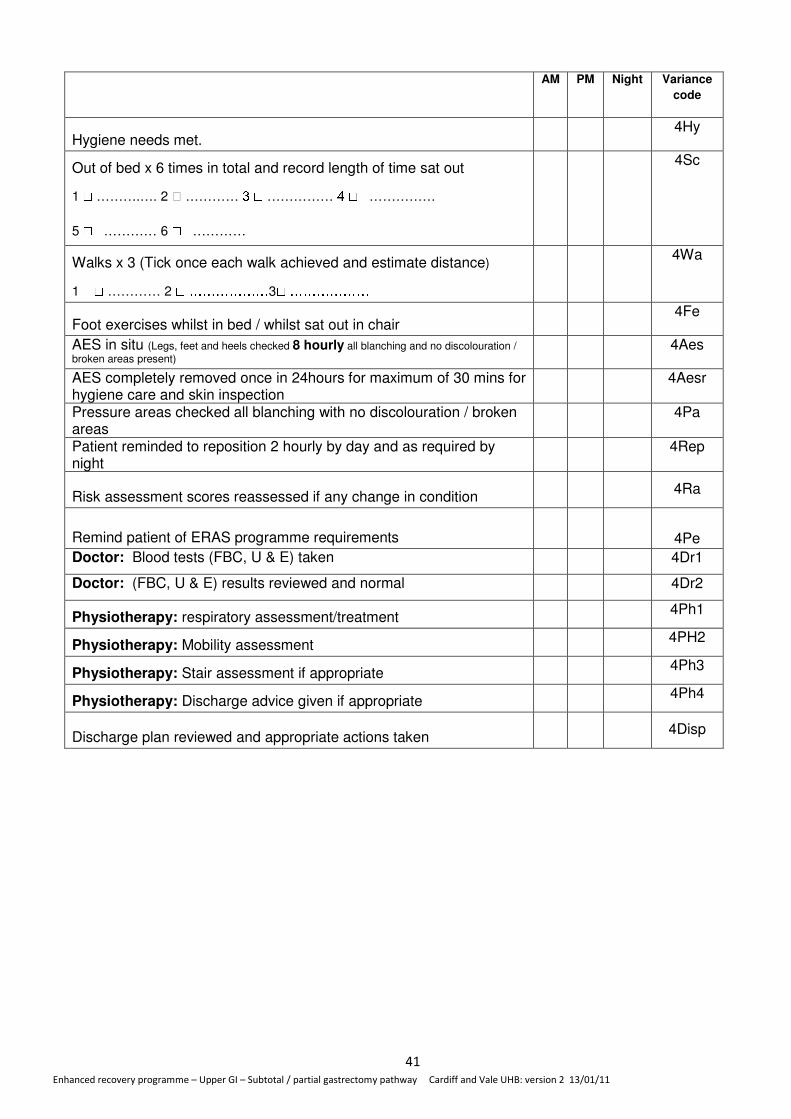
AM PM Night Variance
code
Hygiene needs met. 4Hy
Out of bed x 6 times in total and record length of time sat out
1 ☐ ……….…. 2 ☐ ………… 3 ☐ …………… 4 ☐ ……………
5 ☐ ………… 6 ☐ …………
4Sc
Walks x 3 (Tick once each walk achieved and estimate distance)
1 ☐ ………… 2 ☐ ………………3☐ ……………… 4Wa
Foot exercises whilst in bed / whilst sat out in chair 4Fe
AES in situ (Legs, feet and heels checked 8 hourly all blanching and no discolouration /
broken areas present) 4Aes
AES completely removed once in 24hours for maximum of 30 mins for hygiene care and skin inspection
4Aesr
Pressure areas checked all blanching with no discolouration / broken areas
4Pa
Patient reminded to reposition 2 hourly by day and as required by night
4Rep
Risk assessment scores reassessed if any change in condition 4Ra
Remind patient of ERAS programme requirements 4Pe
Doctor: Blood tests (FBC, U & E) taken 4Dr1
Doctor: (FBC, U & E) results reviewed and normal 4Dr2
Physiotherapy: respiratory assessment/treatment 4Ph1
Physiotherapy: Mobility assessment 4PH2
Physiotherapy: Stair assessment if appropriate 4Ph3
Physiotherapy: Discharge advice given if appropriate 4Ph4
Discharge plan reviewed and appropriate actions taken 4Disp
Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
42
Variances/ Multidisciplinary Notes
Please record all variances or multidisciplinary notes below
Date, Time and
Variance code
Details, reason and action taken
Signature and
bleep number
Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
43
Postoperative Morbidity Survey (POMS) Day 4 postop
Morbidity type Criteria Tick if
present*
Pulmonary Has the patient developed a new requirement for oxygen or respiratory support.
Infectious Currently on antibiotics and/or has had a temperature of
>38°C in the last 24hr.
Renal Presence of oliguria <500 ml/24 hr; Increased serum creatinine (>30% from preoperative level); Urinary catheter in situ.
Gastrointestinal Unable to tolerate an oral diet for any reason including nausea, vomiting, and abdominal distension.
Use of antiemetic.
Cardiovascular Diagnostic tests or therapy within the last 24 hr for any of the following:
• new myocardial infarction or ischemia,
• hypotension (requiring fluid therapy >200 mL/hr or pharmacological therapy),
• atrial or ventricular arrhythmias,
• cardiogenic pulmonary oedema,
• thrombotic event (requiring anticoagulation).
Neurological New focal neurological deficit, confusion, delirium, or coma.
Haematological Requirement for any of the following within the last 24 hr: packed erythrocytes, platelets, fresh-frozen plasma, or cryoprecipitate.
Wound Wound dehiscence requiring surgical exploration or drainage of pus from the operation wound with or without isolation of organisms.
Pain New postoperative pain significant enough to require IV or IM opioids or regional analgesia.
* If no scores above then please state reason why patient still in hospital:
Date: Doctor’s signature: Bleep no:

Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
44
Plan: Eating and drinking discharge, mobile, independent of hygiene needs, confirm discharge arrangements
AM PM Night Variance
code
Observations and EWSC completed 8 hourly. Actions taken as per
EWSC: document all actions on variance sheet
5Ob
Deep breathing promoted, patient able to deep breath and cough. 5Db
Sputum clear 5Sp
oxygen saturations > 94%-97% on room air 5O2
All venflons removed 5vip
Ensure Plus TDS and Ensure Two Cal 50ml QDS
5Su
Oral fluids tolerated well (aim for 2000ml oral fluid over 24hours)
5Of
Normal diet as tolerated maintain food chart (encourage patient to record this)
5Nd
Faeces passed. 5Bo
Patient checked for paralytic ileus - i.e. nausea/vomiting, increased
pain, pulse> 100 and/or abdominal distension, nil present
5Pi
Weight recorded ………Kgs 5Wt
If weight gain>3kgs request surgical review 5Wtg
Pain assessed 8 hourly and well controlled using prescribed
analgesia
5Pa
Nausea assessed 8 hourly and anti-emetics given as per protocol if
required – nausea well controlled no NG tube required
5Na
Passing urine without difficulties 5Uo
Epidural site satisfactory – no oozing, redness or swelling 5Ep
Wound observed, no bleeding or signs of infection noted 5W
Drain sites checked 5Ad
Independent of hygiene needs 5Hy
Out of bed x 8 times in total and record length of time sat out
1 ☐ ……….…. 2 ☐ ………… 3 ☐ …………… 4 ☐ ……………
5 ☐ ………… 6 ☐ …………7 ☐ ……………8 ☐ ……………
5Sc
Walks x 4 (Tick once each walk achieved and estimate distance)
1 ☐ ………… 2 ☐ ………………3☐ ……………… 4☐ ………………
5Wa
Foot exercises whilst in bed / whilst sat out in chair 5Fe
AES in situ (Legs, feet and heels checked 8 hourly all blanching and no discolouration /
broken areas present) 5Aes
AES completely removed once in 24hours for maximum of 30 mins for hygiene care and skin inspection
5Aesr
Post op day 5 Date:
Insert initials if achieved, a x if unachieved and O if not applicable

Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
45
Pressure areas checked all blanching with no discolouration / broken areas
5Pr
AM PM Night Variance
code
Patient reminded to reposition 2 hourly by day and as required by
night
5Rep
Risk assessment scores reassessed if any change in condition 5Ra
Remind patient of ERAS programme requirements 5Pe
Doctor: Blood tests (FBC, U & E) taken 5Dr1
Doctor: (FBC, U & E) results reviewed and normal 5Dr2
Physiotherapy: respiratory assessment/treatment 5Ph1
Physiotherapy: Mobility assessment 5Ph2
Physiotherapy: Stair assessment if appropriate 5Ph3
Physiotherapy: Discharge advice given if appropriate 5Ph4
Confirm discharge plan with patient and relatives 5Disp
Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
46
Variances/ Multidisciplinary Notes
Please record all variances or multidisciplinary notes below
Date, Time and
Variance code
Details, reason and action taken
Signature and
bleep number
Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
47
Postoperative Morbidity Survey (POMS) Day 5 postop
Morbidity type Criteria Tick if
present*
Pulmonary Has the patient developed a new requirement for oxygen or respiratory support.
Infectious Currently on antibiotics and/or has had a temperature of
>38°C in the last 24hr.
Renal Presence of oliguria <500 ml/24 hr; Increased serum creatinine (>30% from preoperative level); Urinary catheter in situ.
Gastrointestinal Unable to tolerate an oral diet for any reason including nausea, vomiting, and abdominal distension.
Use of antiemetic.
Cardiovascular Diagnostic tests or therapy within the last 24 hr for any of the following:
• new myocardial infarction or ischemia,
• hypotension (requiring fluid therapy >200 mL/hr or pharmacological therapy),
• atrial or ventricular arrhythmias,
• cardiogenic pulmonary oedema,
• thrombotic event (requiring anticoagulation).
Neurological New focal neurological deficit, confusion, delirium, or coma.
Haematological Requirement for any of the following within the last 24 hr: packed erythrocytes, platelets, fresh-frozen plasma, or cryoprecipitate.
Wound Wound dehiscence requiring surgical exploration or drainage of pus from the operation wound with or without isolation of organisms.
Pain New postoperative pain significant enough to require IV or IM opioids or regional analgesia.
* If no scores above then please state reason why patient still in hospital:
Date: Doctor’s signature: Bleep no:
Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
48
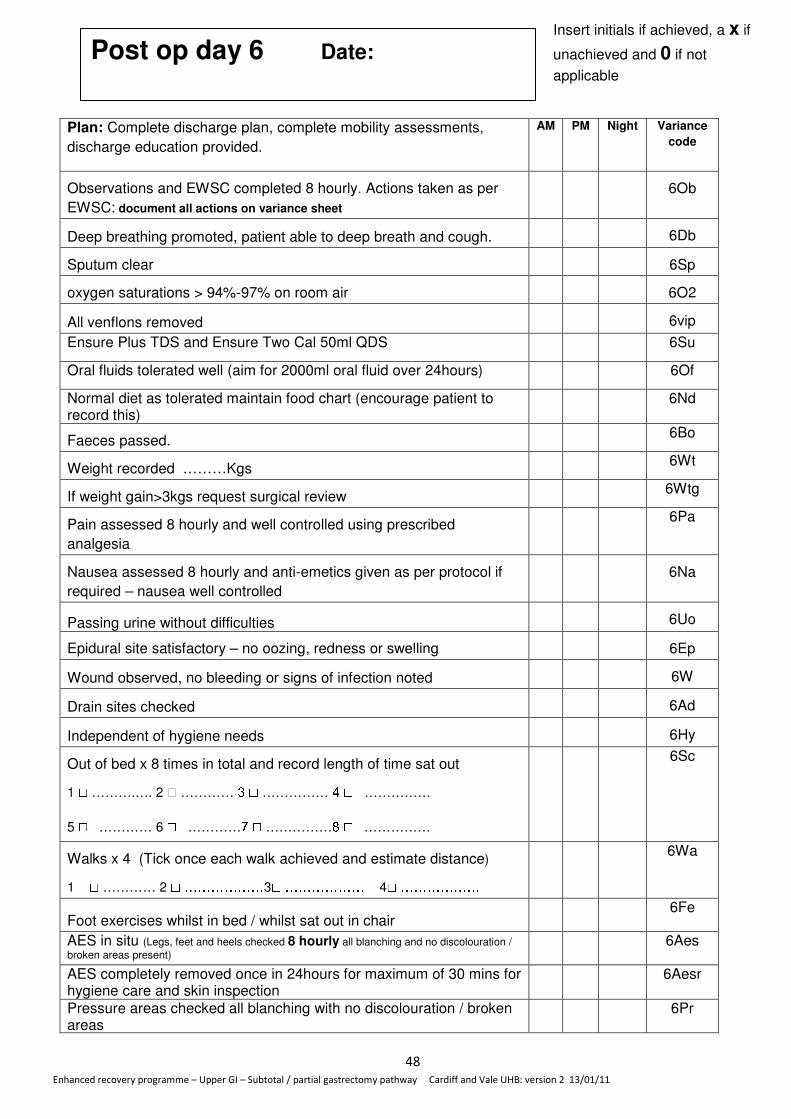
Plan: Complete discharge plan, complete mobility assessments,
discharge education provided.
AM PM Night Variance
code
Observations and EWSC completed 8 hourly. Actions taken as per
EWSC: document all actions on variance sheet
6Ob
Deep breathing promoted, patient able to deep breath and cough. 6Db
Sputum clear 6Sp
oxygen saturations > 94%-97% on room air 6O2
All venflons removed 6vip
Ensure Plus TDS and Ensure Two Cal 50ml QDS
6Su
Oral fluids tolerated well (aim for 2000ml oral fluid over 24hours)
6Of
Normal diet as tolerated maintain food chart (encourage patient to record this)
6Nd
Faeces passed. 6Bo
Weight recorded ………Kgs 6Wt
If weight gain>3kgs request surgical review 6Wtg
Pain assessed 8 hourly and well controlled using prescribed
analgesia
6Pa
Nausea assessed 8 hourly and anti-emetics given as per protocol if
required – nausea well controlled
6Na
Passing urine without difficulties 6Uo
Epidural site satisfactory – no oozing, redness or swelling 6Ep
Wound observed, no bleeding or signs of infection noted 6W
Drain sites checked 6Ad
Independent of hygiene needs 6Hy
Out of bed x 8 times in total and record length of time sat out
1 ☐ ……….…. 2 ☐ ………… 3 ☐ …………… 4 ☐ ……………
5 ☐ ………… 6 ☐ …………7 ☐ ……………8 ☐ ……………
6Sc
Walks x 4 (Tick once each walk achieved and estimate distance)
1 ☐ ………… 2 ☐ ………………3☐ ……………… 4☐ ………………
6Wa
Foot exercises whilst in bed / whilst sat out in chair 6Fe
AES in situ (Legs, feet and heels checked 8 hourly all blanching and no discolouration /
broken areas present) 6Aes
AES completely removed once in 24hours for maximum of 30 mins for hygiene care and skin inspection
6Aesr
Pressure areas checked all blanching with no discolouration / broken areas
6Pr
Post op day 6 Date:
Insert initials if achieved, a x if
unachieved and 0 if not
applicable
Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
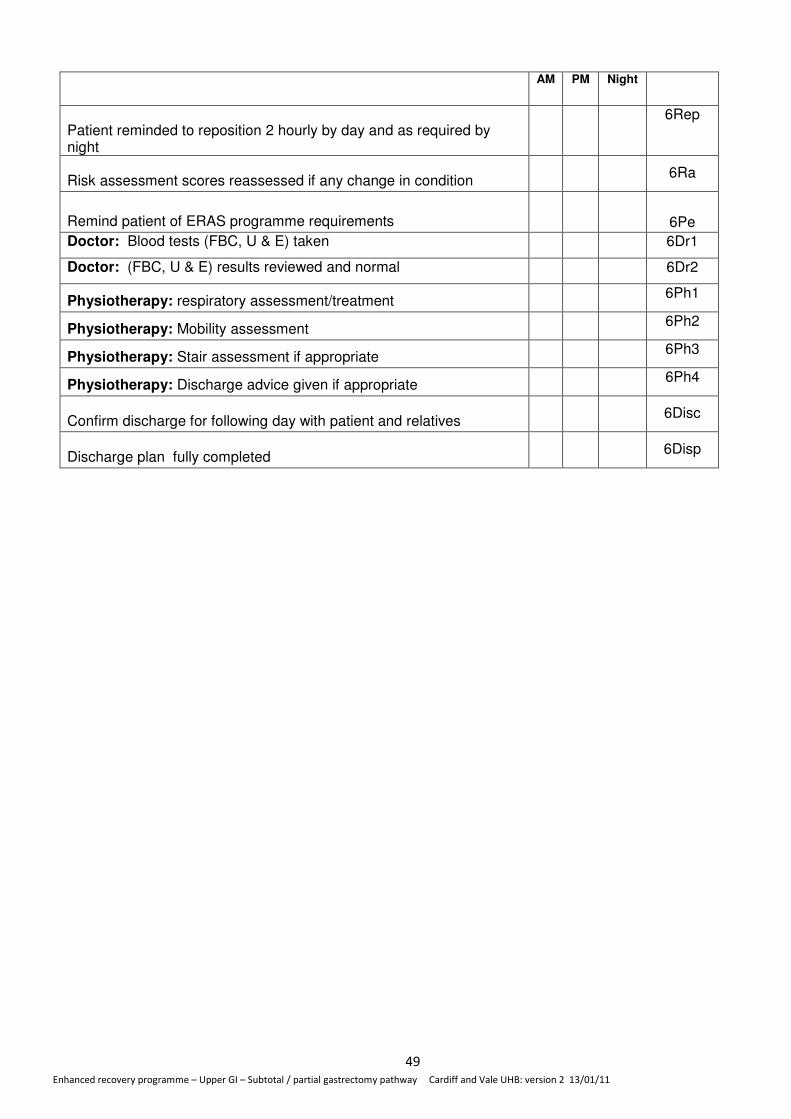
49
AM PM Night
Patient reminded to reposition 2 hourly by day and as required by night
6Rep
Risk assessment scores reassessed if any change in condition 6Ra
Remind patient of ERAS programme requirements 6Pe
Doctor: Blood tests (FBC, U & E) taken 6Dr1
Doctor: (FBC, U & E) results reviewed and normal 6Dr2
Physiotherapy: respiratory assessment/treatment 6Ph1
Physiotherapy: Mobility assessment 6Ph2
Physiotherapy: Stair assessment if appropriate 6Ph3
Physiotherapy: Discharge advice given if appropriate 6Ph4
Confirm discharge for following day with patient and relatives 6Disc
Discharge plan fully completed 6Disp

Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
50
Variances/ Multidisciplinary Notes
Please record all variances or multidisciplinary notes below
Date, Time and
Variance code
Details, reason and action taken
Signature and
bleep number
Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
51
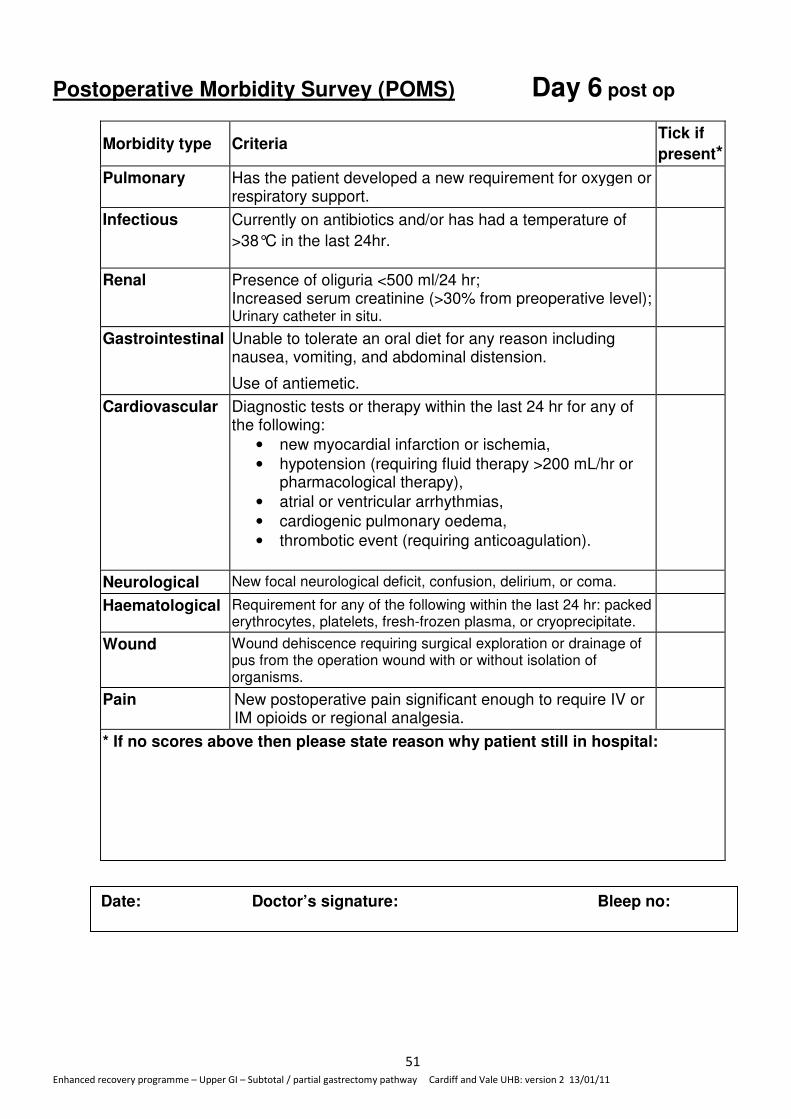
Postoperative Morbidity Survey (POMS) Day 6 post op
Morbidity type Criteria Tick if
present*
Pulmonary Has the patient developed a new requirement for oxygen or respiratory support.
Infectious Currently on antibiotics and/or has had a temperature of
>38°C in the last 24hr.
Renal Presence of oliguria <500 ml/24 hr; Increased serum creatinine (>30% from preoperative level); Urinary catheter in situ.
Gastrointestinal Unable to tolerate an oral diet for any reason including nausea, vomiting, and abdominal distension.
Use of antiemetic.
Cardiovascular Diagnostic tests or therapy within the last 24 hr for any of the following:
• new myocardial infarction or ischemia,
• hypotension (requiring fluid therapy >200 mL/hr or pharmacological therapy),
• atrial or ventricular arrhythmias,
• cardiogenic pulmonary oedema,
• thrombotic event (requiring anticoagulation).
Neurological New focal neurological deficit, confusion, delirium, or coma.
Haematological Requirement for any of the following within the last 24 hr: packed erythrocytes, platelets, fresh-frozen plasma, or cryoprecipitate.
Wound Wound dehiscence requiring surgical exploration or drainage of pus from the operation wound with or without isolation of organisms.
Pain New postoperative pain significant enough to require IV or IM opioids or regional analgesia.
* If no scores above then please state reason why patient still in hospital:
Date: Doctor’s signature: Bleep no:

Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
52
Plan: Discharge home AM PM Night Variance
code
Observations and EWSC completed 8 hourly. Actions taken as per
EWSC: document all actions on variance sheet
7Ob
Deep breathing promoted, patient able to deep breath and cough. 7Db
Sputum clear 7Sp
All venflons removed 7vip
Ensure Plus TDS and Ensure Two Cal 50ml QDS
7Su
Oral fluids tolerated well (aim for 2000ml oral fluid over 24hours)
7Of
Normal diet as tolerated maintain food chart (encourage patient to record this)
7Nd
Bowels open 7Bo
Weight recorded ………Kgs 7Wt
If weight gain>3kgs request surgical review 7Wtg
Pain assessed 8 hourly and well controlled using prescribed
analgesia
7Pa
Nausea assessed 8 hourly and anti-emetics given as per protocol if
required – nausea well controlled
7Na
Passing urine without difficulties 7Uo
Epidural site satisfactory – no oozing, redness or swelling 7Ep
Wound observed, no bleeding or signs of infection noted 7W
Drain sites checked 7Ad
Independent of hygiene needs 7Hy
Out of bed x 8 times in total and record length of time sat out
1 ☐ ……….…. 2 ☐ ………… 3 ☐ …………… 4 ☐ ……………
5 ☐ ………… 6 ☐ …………7 ☐ ……………8 ☐ ……………
7Sc
Walks x 4 (Tick once each walk achieved and estimate distance)
1 ☐ ………… 2 ☐ ………………3☐ ……………… 4☐ ………………
7Wa
Foot exercises whilst in bed / whilst sat out in chair 7Fe
AES in situ (Legs, feet and heels checked 8 hourly all blanching and no discolouration /
broken areas present) 7Aes
AES completely removed once in 24hours for maximum of 30 mins for hygiene care and skin inspection
7Aesr
Pressure areas checked all blanching with no discolouration / broken areas
7Pa
Patient reminded to reposition 2 hourly by day and as required by night
7Rep
Post op day 7 Date:
Insert initials if achieved, a x if
unachieved and 0 if not
applicable

Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
53
AM PM Night Variance
code
Risk assessment scores reassessed if any change in condition 7Ra
Remind patient of ERAS programme requirements 7Pe
Doctor: Blood tests (FBC, U & E) taken 7DR1
Doctor: (FBC, U & E) results reviewed and normal 7Dr2
Physiotherapy: respiratory assessment/treatment 7Ph1
Physiotherapy: Mobility assessment 7Ph2
Physiotherapy: Stair assessment if appropriate 7Ph3
Physiotherapy: Discharge advice given if appropriate 7Ph4
Discharged home 7Dis

Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
54
Variances/ Multidisciplinary Notes
Please record all variances or multidisciplinary notes below
Date, Time and
Variance code
Details, reason and action taken
Signature and
bleep number

Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
55
Postoperative Morbidity Survey (POMS) Day 7 postop
Morbidity type Criteria Tick if present*
Pulmonary Has the patient developed a new requirement for oxygen or respiratory support.
Infectious Currently on antibiotics and/or has had a temperature of >38°C
in the last 24hr.
Renal Presence of oliguria <500 mL/24 hr; Increased serum creatinine (>30% from preoperative level); Urinary catheter in situ.
Gastrointestinal Unable to tolerate an oral diet for any reason including nausea, vomiting, and abdominal distension.
Use of antiemetic.
Cardiovascular Diagnostic tests or therapy within the last 24 hr for any of the following:
• new myocardial infarction or ischemia,
• hypotension (requiring fluid therapy >200 mL/hr or pharmacological therapy),
• atrial or ventricular arrhythmias,
• cardiogenic pulmonary oedema,
• thrombotic event (requiring anticoagulation).
Neurological New focal neurological deficit, confusion, delirium, or coma.
Haematological Requirement for any of the following within the last 24 hr: packed erythrocytes, platelets, fresh-frozen plasma, or cryoprecipitate.
Wound Wound dehiscence requiring surgical exploration or drainage of pus from the operation wound with or without isolation of organisms.
Pain New postoperative pain significant enough to require IV or IM opioids or regional analgesia.
* If no scores above then please state reason why patient still in hospital:
Date: Doctor’s signature: Bleep number:
Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
56
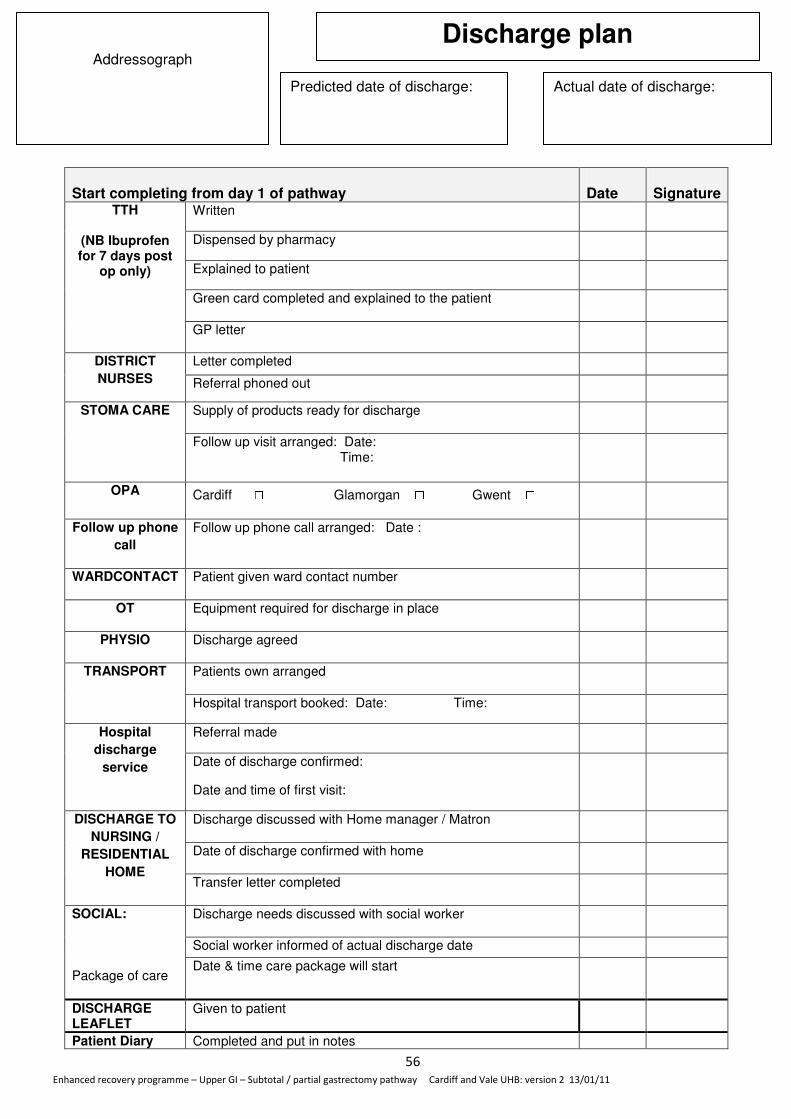
Start completing from day 1 of pathway
Date
Signature
Written
Dispensed by pharmacy
Explained to patient
Green card completed and explained to the patient
TTH
(NB Ibuprofen for 7 days post
op only)
GP letter
Letter completed
DISTRICT
NURSES Referral phoned out
Supply of products ready for discharge STOMA CARE
Follow up visit arranged: Date: Time:
OPA Cardiff ☐ Glamorgan ☐ Gwent ☐
Follow up phone
call
Follow up phone call arranged: Date :
WARDCONTACT Patient given ward contact number
OT Equipment required for discharge in place
PHYSIO Discharge agreed
Patients own arranged TRANSPORT
Hospital transport booked: Date: Time:
Referral made Hospital
discharge
service Date of discharge confirmed:
Date and time of first visit:
Discharge discussed with Home manager / Matron
Date of discharge confirmed with home
DISCHARGE TO
NURSING /
RESIDENTIAL
HOME Transfer letter completed
Discharge needs discussed with social worker
Social worker informed of actual discharge date
SOCIAL:
Package of care Date & time care package will start
DISCHARGE LEAFLET
Given to patient
Patient Diary Completed and put in notes
Addressograph
Discharge plan
Predicted date of discharge: Actual date of discharge:
Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
57
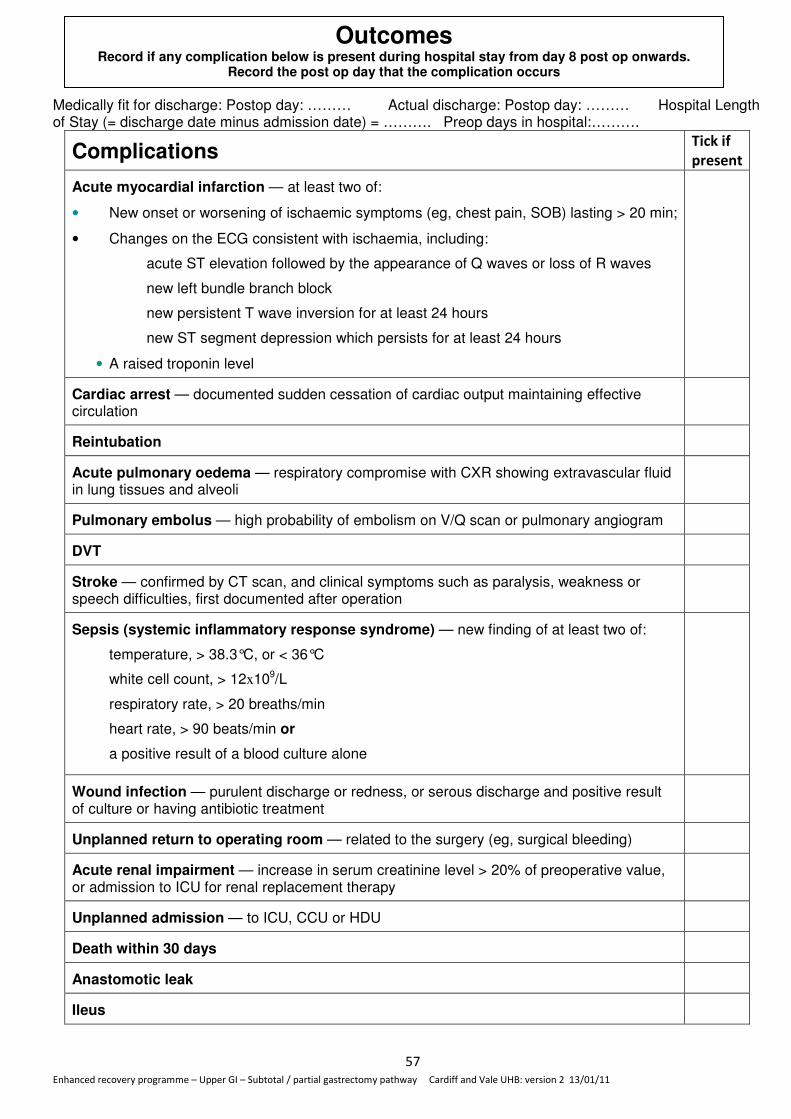
Medically fit for discharge: Postop day: ……… Actual discharge: Postop day: ……… Hospital Length of Stay (= discharge date minus admission date) = ………. Preop days in hospital:……….
Complications Tick if
present
Acute myocardial infarction — at least two of:
• New onset or worsening of ischaemic symptoms (eg, chest pain, SOB) lasting > 20 min;
• Changes on the ECG consistent with ischaemia, including:
acute ST elevation followed by the appearance of Q waves or loss of R waves
new left bundle branch block
new persistent T wave inversion for at least 24 hours
new ST segment depression which persists for at least 24 hours
• A raised troponin level
Cardiac arrest — documented sudden cessation of cardiac output maintaining effective circulation
Reintubation
Acute pulmonary oedema — respiratory compromise with CXR showing extravascular fluid in lung tissues and alveoli
Pulmonary embolus — high probability of embolism on V/Q scan or pulmonary angiogram
DVT
Stroke — confirmed by CT scan, and clinical symptoms such as paralysis, weakness or speech difficulties, first documented after operation
Sepsis (systemic inflammatory response syndrome) — new finding of at least two of:
temperature, > 38.3°C, or < 36°C
white cell count, > 12x109/L
respiratory rate, > 20 breaths/min
heart rate, > 90 beats/min or
a positive result of a blood culture alone
Wound infection — purulent discharge or redness, or serous discharge and positive result of culture or having antibiotic treatment
Unplanned return to operating room — related to the surgery (eg, surgical bleeding)
Acute renal impairment — increase in serum creatinine level > 20% of preoperative value, or admission to ICU for renal replacement therapy
Unplanned admission — to ICU, CCU or HDU
Death within 30 days
Anastomotic leak
Ileus
Outcomes Record if any complication below is present during hospital stay from day 8 post op onwards.
Record the post op day that the complication occurs

Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
58
Possum-O
Calculate Possum-O on-line - http://www.riskprediction.org.uk/op-index.php
Score = ………………….
Signature ………………… Date ……………..
Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
59
Analgesia Appendix
Pain assessment
Pain must be assessed at rest, on movement and deep breathing using the terms none, mild, moderate or
severe (0-3). Pain should be assessed at least two hourly although in the initial postoperative period or if there
is a pain related problem more frequently.
Analgesia
Epidural analgesia with 2micrograms fentanyl/0.1% bupivacaine
Or
5micrograms fentanyl/0.1% bupivacaine
Or
0.1% bupivacaine only
With
Regular intravenous paracetamol
Intravenous PCA with regular paracetamol + NSAID (if not contraindicated)
Once epidural or PCA have been discontinued:
Intravenous step down analgesia day 4-7
Continue regular intravenous paracetamol
Regular intravenous tramadol 50-100mgs
S/C morphine hourly as required (algorithm)
Oral step down analgesia day 9 >
Continue regular intravenous paracetamol
Regular oral tramadol 50-100mgs
Oramorph hourly as required (algorithm)
Anti emetics
1st line Cyclizine 50 mgs as required 8 hourly intravenously
2nd line Ondansetron 4mgs as required 8 hourly intravenously
3rd line Prochloperazine 3-6 mgs twice daily as required via buccal mucosa

Enhanced recovery programme – Upper GI – Subtotal / partial gastrectomy pathway Cardiff and Vale UHB: version 2 13/01/11
60
Postoperative fluid management: • Hartmann’s 1.5L over 24 hrs (=62.5 mls/hr)
• Oral intake 800mls on day of surgery.
• IVI down on post op day 1
• Oral intake 2000mls from day 1 (includes 3 nutritional supplement drinks)
• Aim for mean BP ≥60mmHg.
• If poor urine output or hypotension requiring iv fluids, use 250ml boluses of colloid.
• Patients with epidural analgesia may require more postoperative fluids than other
anaesthetic/analgesic techniques due to the vasodilatory effects of the epidural
• Acceptance of a lower average urine output (0.3 mls/kg/hr averaged over 4
hours)in the first 24-48hrs post-operatively helps to avoid fluid overload with no
adverse effect on the patient – as long as other parameters are normal and patient is
euvolaemic with no renal impairment. In the absence of complications, oliguria
occurring soon after operation is usually a normal physiological response to surgery.
• Oliguria soon after surgery does not necessarily reflect hypovolaemia and should be
evaluated in the context of the patient’s volume status. The key question is whether or
not the oliguric patient has significant intravascular hypovolaemia which needs
treatment. Clinical signs reflecting intravascular volume include capillary refill, jugular
(central) venous pressure, and the trend in pulse and blood pressure. Urine output
should be interpreted in the light of these clinical signs, bearing in mind the normal
short term physiological effects of surgery on urine output.