endocrinology in primary care -...
TRANSCRIPT

Endocrinology in Primary Care
HN Buch

Endocrinology in Primary Care
Death by Powerpoint
HN Buch

Agenda
Endocrine Condition Primary v Secondary Care
Focus of Discussion Initial management Follow up
Hypothyroidism Largely primary care
Primary care Pitfalls in management
Hyperthyroidism Secondary care Secondary care Pre-referral management
Hyperparathyroidism Most need referral Many in primary care
Follow up strategy
Hyperprolactinaemia If “true” all need referral
Some in primary care
Check list prior to referral

Hypothyroidism is Easy
• Aetiology is either autoimmune or iatrogenic: Surgery,
RAI and it does not affect the treatment
• Easy to diagnose
– High prevalence: 2% in women, 0.1% of men
– Well recognised clinical features
– Easy-to-interpret, cheap test - high TSH and low FT4/FT3
– No need for imaging

• Easy to manage
– Cheap treatment
– Single agent (T3, armour thyroid etc have no advantage)
– No significant interactions
– Treatment can be easily monitored with TSH
– Most patients respond well to treatment; those that do not,
do not respond to much else!!
Hypothyroidism is Easy

• Start 50-100mcg; 25mcg in cardiac patients or elderly
• Weight based regimes offer no advantage
• Adjust at intervals not shorter than 6-8 weeks
• Aim to maintain TSH in the lower half of reference range
• If >200mcg is required consider
– Suboptimal compliance
– Malabsorption
Hypothyroidism is Easy

Hypothyroidism is Easy

Not Always Easy!
• Diagnostic pitfalls

Case 1
• 34/F, recurrent hyperthyroidism
• Received radioiodine therapy (RAI)
Pre RAI 2/12 post
FT4 (10-22)
55
FT3 (3.5-6.5)
19
TSH (0.5-4.0)
<0.01 <0.01
Persistent Hyperthyroidism
Pre RAI 4/12 post
FT4 (10-22)
55 6
FT3 (3.5-6.5)
19 2.9
TSH (0.5-4.0)
<0.01 <0.01
Post-RAI Hypothyroidism

Case 1
During transition from hyperthyroidism to hypothyroidism
only TSH is not enough to diagnose hypothyroidism

Case 2
• 61/male, presented with lethargy, tiredness, weakness /12
after CABG
• UE/LFT/Bone/FBC normal/vitamin D 19
• TSH 1.1 (0.5-4.0)
• Started on vitamin D but no improvement
• 3/12 later represented with reduced right eye vision
• Ophthalmology: optic nerve dysfunction with VF impairment
• MRI: larger pituitary tumour

Case 2
Initial 2/12 later
FT4 7.2
FT3 3.6
TSH 1.0 1.0
Peak Synacthen cortisol: 298
Testosterone (4.5 -28) 3.1
MRI: Normal but smaller pituitary
gland
Diagnosis: Hypopituitarism possibly secondary to
hemodynamic instability during CABG

Case 2
TSH is not enough to diagnose secondary hypothyroidism

• 56/M, presented with
lethargy and TSH was 7.6
• Started on thyroxine 50
• 3/12: bumping in to
people
• MRI showed a large
pituitary tumour on MRI
Case 3

Case 3
Full TFT:
• TSH: 7.6
• T4: 31 (10-22)
• T3: 7.2 (3.5-6.8)
Diagnosis:
• TSH producing Pituitary macroadenoma

Case 3
High TSH is not always due to hypothyroidism
Other causes Drugs TSHoma Adrenal insufficiency

Cases 1, 2 and 3
All patients with hypothyroidism do not have high TSH and all patients with high TSH do not have
hypothyroidism

Cases 1, 2 and 3
Although TSH alone is sufficient for the diagnosis and treatment monitoring of primary hypothyroidism most cases , full TFT should be requested in patients
• Who are in transition from hyperthyroidism
• With clinical suspicion of pituitary pathology

Not Always Easy!
• Management challenges
• 22, male, university student
• 2/12 history of lethargy, dizziness and 2 kg weight loss
• TSH: 80mU/L (0.5-4.0); FT4: 8.2pmol/L (12-22)
• TPO 1:1000
• Diagnosis: Autoimmune hypothyroidism
• Thyroxine 75mcg, increased to 125mcg over 3/12
Case 3

3 months later
Clinically and biochemically well replaced
• TSH 1.7mU/L, FT4 16pmol/L
However “not feeling well”
• Further 2kg weight loss
• More dizzy
Haemoglobin 12.4 LFT Normal
S Creatinine 0.78 Calcium 9.8
S Na 143 CXR Normal
S K 5.4 ECG Normal

Diagnostic Test was Performed
Short synacthen test (ACTH 250mcg IV)
Time (min) Cortisol
0 92
30 176
60 198
ACTH-128 (8-60)
Autoimmune Polyglandular Syndrome 2
Diagnosis
Addison’s disease +
Primary Hypothyroidism
APS 1 APS 2
Inheritance AR, no HLA Polygenic
DR3/DR4
Age Infancy/childhood Adult
Gender M=F F>M
Major
conditions
Addison’s
Hypoparathy MC
candidiasis
(~90% each)
Addison’s
(100%)
Thyroid (70%)
T1DM (50%)

Management
• Hydrocortisone PO
– 10mg immediately on rising, 5mg at midday, 5mg at
5pm
• Fludrocortisone 100mcg
• Thyroxine 100mcg
Excellent clinical response
Absence of clinical response despite achieving biochemical
target should prompt a search for additional pathology
especially autoimmune

• 38, businessman
• Bronchial asthma on inhalers
• Anaemia on iron supplements for 12 months
• Lethargy, weight gain
• TSH: 38mU/L, FT4: 10.1pmol/L, TPO positive
• Thyroxine commenced
Case 4

THYROXINE DOSE TSH (mU/L) fT4 (pmol/L)
Diagnosis 38 10.1
100mcg 32.7 12.5
5 months later
100 250 18.4 15.1
TTG antibodies and D2 biopsy: Coeliac disease
Gluten free diet instituted
250 <0.01 25
150 2.1 18.2
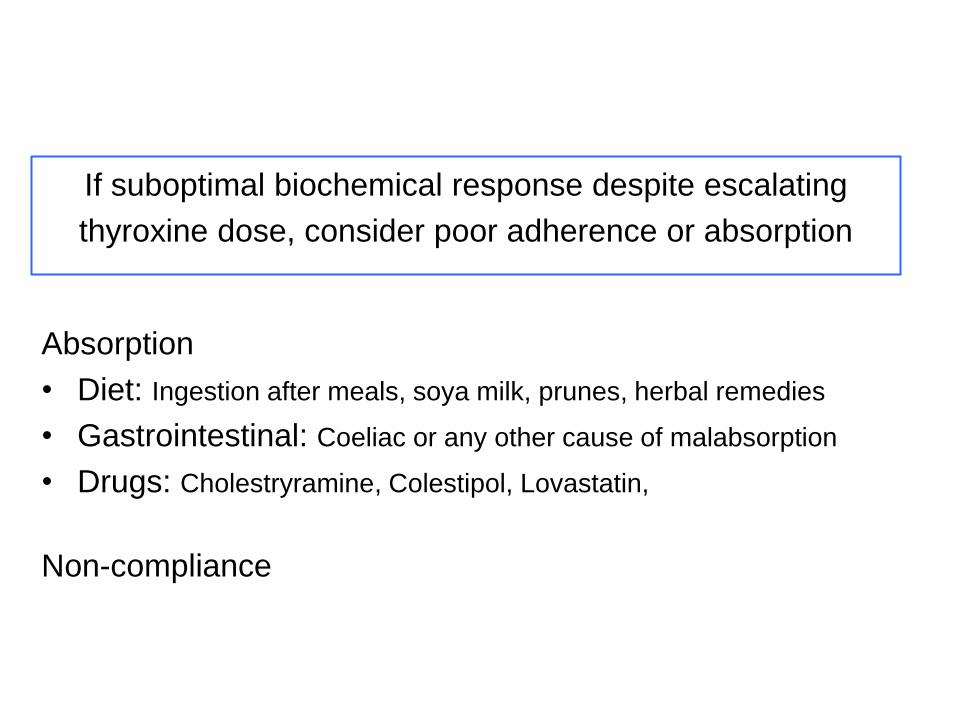
Absorption
• Diet: Ingestion after meals, soya milk, prunes, herbal remedies
• Gastrointestinal: Coeliac or any other cause of malabsorption
• Drugs: Cholestryramine, Colestipol, Lovastatin,
Non-compliance
If suboptimal biochemical response despite escalating
thyroxine dose, consider poor adherence or absorption

Case 5
• 27/F, hair loss, dry skin, mild weight gain (6/12)
• T4 15.2 , TSH 8.1
• More information ? – Any drugs
– Radioiodine
– TPO 1:126
• Options – Treat with thyroxine
– No treatment, monitor TFT
Dx 4/12 12/12 24/12
TSH (0.5-4.0)
8.1 7.8 9.0 6.9
FT4 (10-22)
15.2 15.6 16.9 17.1
FT3 (3.5-6.5)
4.3
No treatment given

Case 5
Diagnosis: Subclinical hypothyroidism
– A biochemical diagnosis (TSH, normal T4/T3),
– 2-4%
– Possible causes
• Impending thyroid failure; 2% p.a. progress to hypothyroidism
• Drugs e.g. amiodarone
• “Normal”

TSH distribution curve
TSH 0.5-4.0 mU/L
Euthyroid people

Treat or Not to Treat
• No convincing evidence of beneficial effect on
– Symptoms
– CV outcomes despite association with risk factors
• Treat, if the lifetime risk of overt hypothyroidism is high
– TSH >10 (10 -15% per annum)
– TPO or associated AI conditions (5 -10% p.a.)
– Post RAI >80% risk over 10 years
– Pregnant or pregnancy is planned
Consensus guidelines, 2005, ATA & AES

Case 6
24/F, recently married, presents with weight gain (Endo clinic)
• T4: 10.5 (12-22), TSH 12.1 (0.5-4.0), TPO +
Commenced on T4 50mcg 75mcg
• T4: 17.3 (12-22), TSH 1.4 (0.5-4.0) – discharged to PC 6/12 TFT
6/12 later: 7/40 pregnant
• T4: 11.3 (12-22), TSH 7.4 (0.5-4.0),
Thyroxine increased: 75mcg 125mcg
• 12/40 - T4: 17 (12-22), TSH 3.1 (0.5-4.0),

Case 6
Why was her management sub-optimal during the initial
hospital consultation?
Patient should have been advised to thyroxine dose by
25-50mcg as soon as pregnancy was confirmed
Why?

Foetus is entirely dependent on
maternal T4 until mid-gestation
Placenta is relatively
impermeable to thyroxine
hCG induced in
maternal T4
in demand of
maternal T4
Fails in patients with
atrophic thyroid
Subtle neurodevelopment
deficiencies in baby

Pregnancy and Hypothyroidism
Maternal Foetal Optimum Management
Sub-fertility
Pre-eclampsia,
preterm birth,
higher CS rate
(overt HT)
Neurodevelopmental disorders with lower
IQ
Maintain TSH <2.5 during the period leading up to pregnancy When pregnancy is confirmed increase thyroxine by 30-50% proactively Close follow up; optimise thyroid status 4-8 weekly intervals

Conclusions
• Please manage hypothyroidism in PC but consider
referral if:
– TFT are discordant
– Central (secondary) hypothyroidism is suspected
– Suboptimal clinical/biochemical response to T4
– Patient is considering pregnancy or is pregnant
– Associated multiple autoimmune conditions
– Uncertainty in some of the patients with subclinical
hypothyroidism

Do Not Ignore Hypothyroidism
Researchers determined that the 6/12 Republican presidents over the past 50 years had an average IQ of 115.5, with President Nixon having the highest at 155. President Bush (Jr) had the lowest at 91.
Why?

All 3 in this photo had thyroid dysfunction

Hyperthyroidism
• Well recognised clinical symptoms and signs
• High T4/T3 and suppressed TSH
Please refer all patients
• No need for US or RN scan prior to referral
• Please initiate treatment in patients with significant clinical or biochemical hyperthyroidism

Pre-referral Treatment Initiation
• Carbimazole (CMZ) 40mg od
• Warn about agranulocytosis
• Beta-blockers as appropriate; the only treatment in patients with mild rise T4 and no symptoms
• If rashes – Propylthiouracil 200mg BD
• If agranulocytosis or hepatitis – not for PTU; urgent referral

Caveats
• Request urgent review
– Pregnant
– Significant thyroid eye disease
– Active CV/psychiatric disorder
– Agranulocytosis or hepatitis to CMZ
• Do not start treatment if
– No symptoms + mild rise of T3/T4
– Discordant biochemical picture
– Tender goitre with fever and raised ESR
– Post RAI
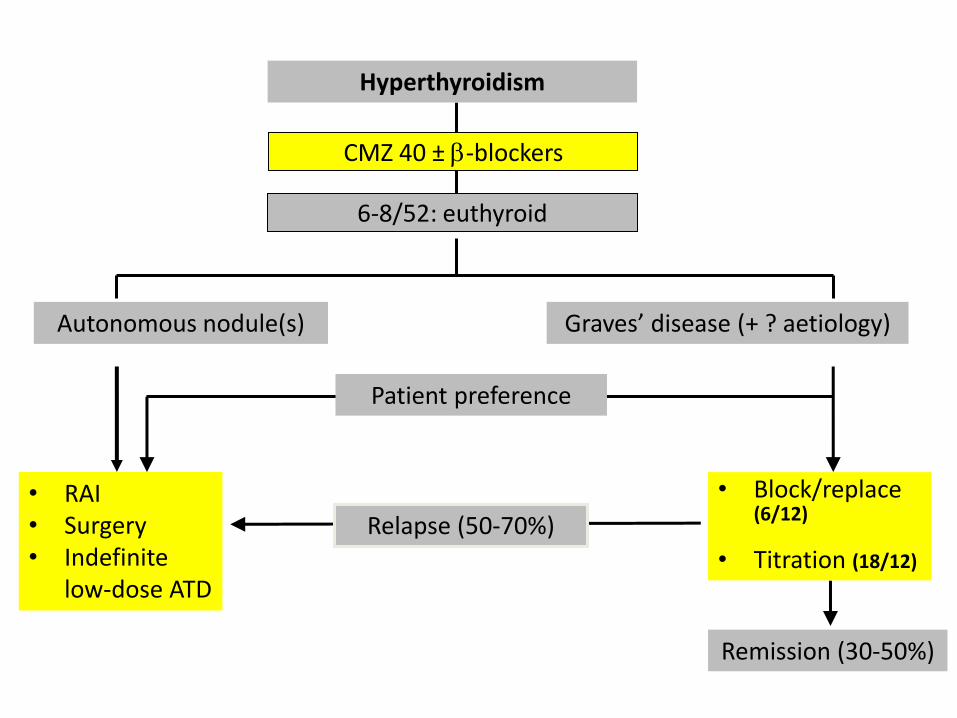
• Block/replace (6/12)
• Titration (18/12)
Remission (30-50%)
• RAI • Surgery • Indefinite
low-dose ATD
Relapse (50-70%)
Hyperthyroidism
CMZ 40 ± -blockers
Patient preference
Graves’ disease (+ ? aetiology) Autonomous nodule(s)
6-8/52: euthyroid

Aetiology
5 min uptake= 0%
5 min uptake= 6%

Case 7
• 79/F
• Routine testing: T4 17.1, TSH 0.005
• What next?
• FT3 – 6.7 (3.5-5.7)
• Diagnosis: T3 toxicosis; management is identical to hyperthyroidism with high T4

Case 7
• 79/F
• Routine testing: T4 17.1, TSH 0.005
• What next?
• FT3 – 5.1 (3.5-5.7)
• Diagnosis: Sub-clinical hyperthyroidism
• Increases risk of AF and osteoporosis but no treatment as no convincing intervention data
• 6-12 monthly TFT

FT4, TSH
Hyperthyroidism
Both normal High FT4 & suppressed TSH
FT3
Normal FT4 & suppressed TSH
No further tests
Normal Subclinical hyperthyroidism
High T3 Thyrotoxicosis
Thyrotoxicosis

Primary Hyperparathyroidism
Diagnosis
• High calcium
• High PTH
Much less common possibilities: • Tertiary hyperparathyroidism (End-stage renal failure, long-standing
severe vitamin D deficiency)
• Genetic conditions: hypocalciuric hypercalcaemia

Primary Hyperparathyroidism (PHPT)
Should all patients be referred?
Yes
Should all patients be followed up in specialist care?
No

Confirm diagnosis: repeat calcium, PTH
• Age • H/O fractures, fracture risk (DEXA, FRAX) • H/O renal stones, KUB imaging • eGFR • Vitamin D status
Needs surgery Endocrine follow-up
May need surgery Endocrine follow
up ~2 years
Does not need surgery Discharge for annual
primary care follow up
PHPT: Endocrine Clinic
Indications for surgery
What needs monitoring?

Indications for Surgery
• Age <50
• Calcium>2.85
• Fragility fracture or vertebral fracture
• BMD <-2.5
• Renal calculi
• Decline in eGFR to <60
• (High urinary calcium)

Primary Care Follow Up
Surgery is not likely to be required in foreseeable future
• Annual calcium
• Ensuring adequate vitamin D replacement
• Re-referral – If serum calcium rises to >2.80
– New onset symptoms, osteoporosis, fractures and renal stones/dysfunction

Hyperprolactinaemia
Cause Prolactin level
Macroprolactinoma 5000-100,000 mU/L
Microprolactinoma
Up to 2500 mU/L Other large non-functioning pituitary tumours with compression on the pituitary stalk
Drugs
Miscellaneous: stress, PCO

Hyperprolactinaemia
Exclude macroprolactin
• Repeat PRL • Exclude
hypothyroidism • Drug history
Not MRI
If persistently high PRL and euthyroid refer Urgency dictated by visual symptoms

Macroprolactinaemia
• Not to be confused with macroprolactinoma
• Biologically inactive large molecules of PRL and IG
• Routinely measured in all patients with high prolactin
• High total PRL with normal monomeric PRL– no action needed

Agenda
Endocrine Condition Primary v Secondary Care
Focus of Discussion Initial management Follow up
Hypothyroidism Largely primary care
Primary care Pitfalls in management
Hyperthyroidism Secondary care Secondary care Pre-referral management
Hyperparathyroidism Most need referral Many in primary care
Follow up strategy
Hyperprolactinaemia If “true” all need referral
Some in primary care
Check list prior to referral

Conclusions
Endocrine Condition Primary v Secondary Care
Conclusions Initial management Follow up
Hypothyroidism Largely primary care
Primary care Limitations of TSH
Hyperthyroidism Secondary care Secondary care Carbimazole 40
Hyperparathyroidism Most need referral Many in primary care
Surgery v observation
Hyperprolactinaemia If “true” all need referral
Some in primary care
Exclude macroprolactin

La Fin

Agenda
Endocrine Condition Primary v Secondary Care Focus of Discussion
Hypothyroidism Managed in primary care; only a few need referral
Pitfalls in management
Hyperthyroidism All need referral Pre-referral management
Hyperparathyroidism Most need referral but many can be followed up in primary care
Follow up strategy
Prolactinomas If “true hyperprolactinaemia” need referral; some can be followed up in primary care
Check list prior to referral
Take Home Message
• Consider thyroiditis in patients with
– Spontaneously fluctuating thyroid status
– Significant thyroid dysfunction with disproportionately less
symptoms
– Tender inflamed thyroid
• Appropriate setting
– Post partum
– Sub-acute thyroiditis
– Post-RAI

Subclinical hypothyroidism
• 27/F
• Aches and pains
• Weight gain 4 kg in 1 year
• No relevant PH, FH
• OCP
• FT4 15.6, TSH 6.8
• 3 months later: FT4 16.1, TSH 6.6
Subclinical hypothyroidism
• Treat or not to treat

Subclinical hypothyroidism
Causes
• Recent onset thyroid failure
• Drug induced: amiodarone, antiepileptics
• Hypocortisolism
• Heterophile antibodies
• “Normal”

Subclinical hypothyroidism
Treat if
• TSH>10
• TPO antibodies strongly positive
• Post RAI
• Pregnant or planning pregnancy
Not for symptoms in absence of above

Hyperprolactinaemia
• Exclude macroprolactin
• Repeat prolactin with other relevant investigation
– Baseline biochemistry: UE, LFT
– Repeat prolactin, testosterone/oestradiol, FSH, LH, TFT
– Not for MRI
• If persistent hyperprolactinaemia with euthyroidism refer with urgency dictated by recent onset visual symptoms

Pre-referral Check-list
• Confirm persistently high levels
• Exclude hypothyroidism
• Exclude drug related causes and withdraw if possible
• Exclude macroprolactin

Isotope scan
• Technetium, simple, harmless
• Contraindicated during pregnancy
Indications to request:
• Hyperthyroid patient when low uptake state is suspected
Graves’ disease Solitary nodule Thyroiditis/factitious
Ocassionally

Grave’s Disease
• Incidence 2-3 per 1000 per year (Sex ratio 5:1)
• Prevalence 1.9% female, 0.16% male
• 90% of patients have a diffuse painless goitre
• Autoimmune driven conditiona
Spontaneous remission in around 50% of patients after 12-18 months on ATD
Other manifestations of Graves disease?

11/10/06

11/10/06 68
Multi-nodular goitre
• Common cause of hyperthyroidism in the elderly
• No spontaneous remission

ATD B/R 6/12 or
Titration 18/12
Remission (40-50%)
RAI Surgery Indefinite ATD
Relapse (50-60%)
Hyperthyroidism
CMZ 40 OD + -blockers
Patient preference
Graves’ disease
(+ ? aetiology)
Autonomous nodule(s)
4-6/52: euthyroid

Case 5
• 24 year, housewife
• Delivered a baby boy 5 months ago
• Presented to GP with 2 week history of tiredness, some
weight loss, mood changes although better for last 4
days
• Suspected to be hyperthyroid
• FT4: <5 pmol/L (9-19) , TSH: >100mU/L (0.5-4.5)

Case 5
Endocrine clinic: 2/52
• No clinical signs of thyroid dysfunction
• No goitre
• TPO antibodies: negative
• FT4: 6.2 pmol/L (9-19), TSH: >100mU/L (0.5-4.5)
• No treatment

FT4
(9-19pmol/L)
TSH
(0.5-4.5mU/L)
At presentation <5 >100
2/52 6.2 62
6/52 8.2 36
3/12 9.4 20
4/12 11.2 3.9
Case 5
Diagnosis
Post-partum thyroiditis
Presenting with hypothyroidism
Case 5

Post partum thyroiditis
• Incidence: 5-10% pregnancies
• Histopathology: Inflammation with an autoimmune basis
• Clinical presentation at 3-12 months post-partum
• Permanent hypothyroidism: 20-30% (50% after 10 years)
• Recurrence during subsequent pregnancies 70%
Hyperthyroid Hypothyroid Euthyroid
4-8 weeks 2-3 months -
Inflammation Dysfunction Recovery
No hyperthyroid phase 25%
No hypothyroid phase 25%

Management
• Observational policy
• Symptomatic treatment (-blockers) during hyperthyroid phase (Anti-thyroid drugs are not effective)
• Thyroxine may be given (for ~4-6/12) to those with prolonged and symptomatic hypothyroidism

Interpretation of Difficult TFT
T4 (9-19)
T3 (3.5-5.7)
TSH (0.5-4.0)
Interpretation Action
8.2 3.6 0.19 Not Primary HT, could be Secondary HT Sick euthyroid/Drugs
Do not treat, please refer
22 5.0 0.64 Not hyperthyroid, could be Assay related Drugs Normal
Do not treat, no need to refer in most cases
24 7 3.6 Not Primary TT, most likely TSHoma or TH resistance
Please refer
16 6.3 1.2 Not hyperthyroid, could be Assay related
Do no treat, please discuss/repeat
7.0 6.8 0.01 T3 toxic Ignore T4 and manage as hyperthyroid
7.0 3.3 7 Consider secondary hypothyroidism
Please refer