endocrine. common pediatric endocrine disorders type i diabetes congenital hypothyroidism acquired...
TRANSCRIPT
Endocrine
Common Pediatric Endocrine Disorders
• Type I Diabetes• Congenital Hypothyroidism• Acquired Hypothyroidism (Hashimoto’s
Disease)• Hyperthyroidism (Graves disease)• Growth Hormone Deficiency
The Endocrine System
• Glands• Hormones• Endocrine Disorders are either
• Hypofunction• Primary• Secondary
• Hyperfunction• Primary• Secondary

Pediatric Differences in the Endocrine System
• The endocrine system is less developed at birth than any other body system
• Hormonal control of many body functions is lacking until 12-18 months of age
• Infants might manifest imbalances in concentration of fluids, electrolytes, amino acids, glucose, and trace substances
Type 1 Diabetes
Type 1 Diabetes
• Most common endocrine disorder in children
• Pancreas becomes unable to produce and secrete insulin
• Peak age: 5-7, or at puberty• Abrupt onset• Genetic link
Type 1 Diabetes
• Beta cells- type of cell found in the Islets of Langerhans within the pancreas that make and release insulin
• Insulin is a hormone required to move the glucose into cells throughout the body• If no insulin can be produced, the glucose
stays in the blood instead, where it can cause serious damage to all the organ systems of the body
Etiology
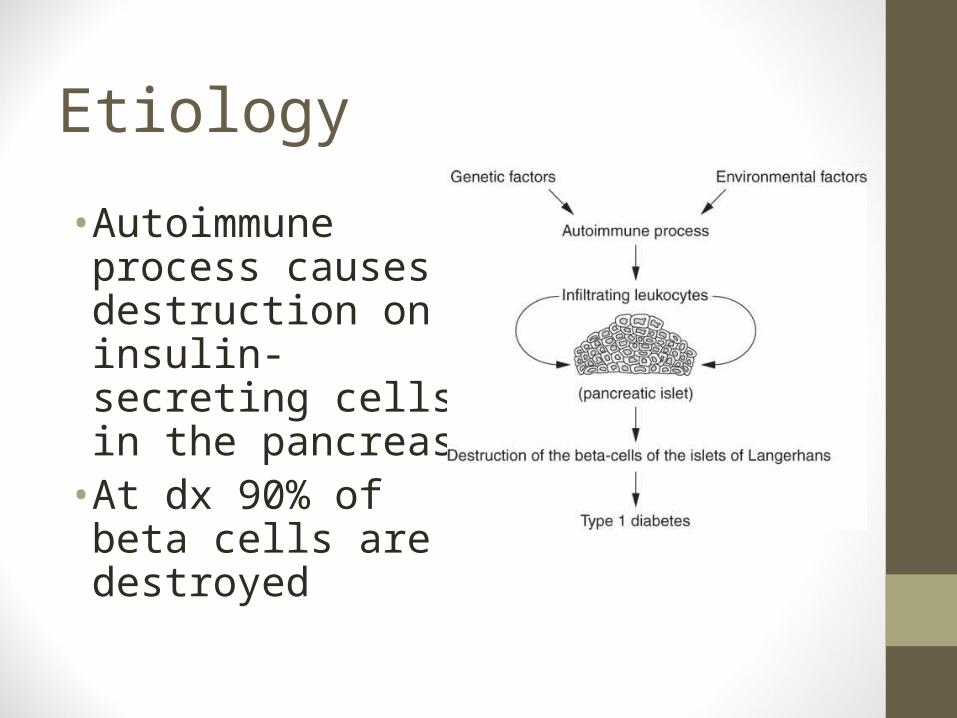
• Autoimmune process causes destruction on insulin-secreting cells in the pancreas
• At dx 90% of beta cells are destroyed
Type 1 Diabetes
No cure, but JDRF is funding studies that perfect pancreas transplantation and regeneration the body’s own beta cells without islet transplantation
Serum Glucose Levels
• Normal fasting glucose 70-110mg/dl
• Glycosated Hemoglobin (Hgb A1C) < 6.0%
Initial Clinical Manifestations
PolyuriaPolydipsia PolyphagiaFatigue Blurred visionHeadacheShortened attention spanMood changes
Diabetic Ketoacidosis(DKA)
• Medical Emergency• As glucose levels rise, child will progress
into DKA if not treated• Blood glucose levels > 300
• Cellular starvation leads to ketone production• Nausea, vomiting, abdominal pain• Acetone (fruity) breath odor• Dehydration• Kussmaul respirations
• Coma if untreated
When to Monitor for DKA
• Abdominal pain• Nausea and vomiting that persists for over
6 hours• More than five diarrheal stools in 1 day• A 1- or 2-day history of polyuria and
polydipsia• Has illness (e.g., viral or other) and is
unable to eat
Type 1 Diabetes Treatment
• Multidiscipline• Promote normal growth and development• Optimal glucose control• Minimal complications• Adjustment to disease• Treatment consists of
• Insulin replacement• Diet• Blood glucose monitoring• Exercise
Diet Therapy
• Consistent intake & timing of food to correspond to insulin prescribed
• Well-balanced, enough caloric intake to support growth and development
• Three meals, snacks spaced throughout the day
• No diet, sugar-free foods• Don’t omit meals
Exercise• Encouraged, never restricted• Lowers blood glucose levels, by
aiding the body’s use of food• Decreases insulin requirements• Proper snack before
• Add an extra 15- to 30-g carbohydrate snack for each 45-60 minutes of exercise
Blood Glucose Monitoring
Finger stick glucose monitoring several times a day
Urine testing for glucose and ketones Teach good record keeping Self-management at age appropriate level
2-6 choose food, clean finger for stick 4-6 dip own urine 6-8 Blood glucose management 8-10 insulin injections, keep diary 10-14 nutritional decisions 12-18 full management
InsulinPrecise dose cannot be predicted
Amount is based upon average capillary or serum blood glucose levels
Will change based of growth
Can be administered twice daily

Types of InsulinSynthetic Human Insulin
• Rapid acting• Lispro (Humalog)• Aspart (Novolog)
• Fast acting• Regular ®
• Intermediate• NPH (N)
• Mixed (70/30)• Long Acting
• Glargine (Lantus)• Ultra Lente
Typical Management
• The peak of the insulin should occur Post-Prandial (after meal) to avoid hypoglycemia
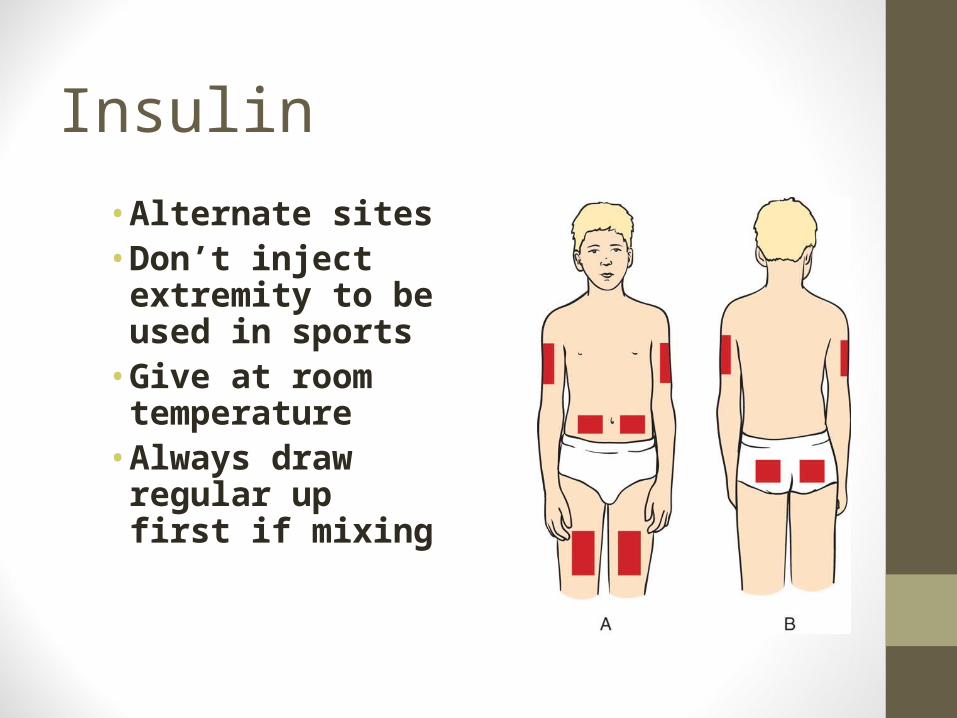
Insulin
• Alternate sites • Don’t inject
extremity to be used in sports
• Give at room temperature
• Always draw regular up first if mixing

Pumps
• Delivers fixed amounts of short-acting insulin continuously
• Worn on a belt, the tubing & catheter are changed Q48 hours and taped in place
• Should not be removed for > 1-2 hours
• Subject to minimal malfunction
• Must be self-motivated

Pumps• Advantages
• Less scar tissue• No daily injections• Less to carry• Private• Sense of control
• Disadvantages• Must wear continuously• Need to carry extra battery• Good BGM• If insurance dose not cover
$$$$$• Still need emergency
needles, insulin, and remember how to inject
Illness alters diabetic management
• Dosage requirements may increase, decrease, or remain unchanged depending on the severity of the illness & the child’s appetite
• Rapid-acting insulin only is used to manage hyperglycemia associated with illness
• Monitor fluids, may require extra oral fluids while ill
“Sick Day” Guidelines
• Seek medical attention for fever or other signs of infection.
• Monitor the blood glucose levels more often than routine (1 to 4 hours).
• Test urine ketones when the blood glucose level is greater than 200 mg/dL.
• Do not skip doses of insulin.
• Large fluid intake (drinks with carbohydrates) is essential if the child cannot eat as usual.
• If the child cannot consume adequate amounts of fluids, seek medical attention.
Hyperglycemia BG > 110Gradual onsetLethargic, fatigueConfusedWeakness
PolyuriaPolydypsiaPolyphagia
Glucose 250 mg/dl Large ketones in blood & urine Blurred vision Ketoacidosis Coma
Hypoglycemia BG < 70Commonly occurs before meals
when the insulin effect is peaking
Burst of physical activity without additional food
Delayed, omitted, or incompletely consumed meals or snacks
Too much insulin-wrong dose

Hypoglycemia BG < 70Rapid onset•Irritable, nervousness•Difficulty concentrating•Shaky feeling, tremors, hunger•Diplopia•Pallor•Weakness•Headache, dizziness•Sweating•Unconsciousness and convulsions

Treatment of Hypoglycemia
Give simple concentrated sugarGlucose gel or SL tablets Hard candySugar cubesLow-fat milk or OJ
Followed by a complex CHO & ProteinSlice of bread or cracker with peanut butterGlucagon SQ for severe hypoglycemia (may cause
vomiting, prevent aspiration)
Nursing Considerations Begins with survival education
Educate child & family regarding Nature of disease, hypo/hyperglycemia Meal planning (3 spaced meals, 3 snacks) Wearing ID bracelet Effective duration, onset & peak action of insulin Injection procedure, rotate sites Glucose monitoring, urine testing, record keeping Exercise regime
Nursing Considerations• Provide emotional support
• Encourage growth and development
• Identify home care needs
Disorders of the Thyroid
• Congenital Hypothyroidism
• Acquired Hypothyroidism
• Hyperthyroidism
Congenital Hypothyroidism
CONGENITAL HYPOTHYROIDISM
• Disorder at birth
• Body is producing insufficient thyroid hormone to meet metabolic needs caused by absent or underdeveloped thyroid gland
• If not treated can lead to severe cognitive impairment
• Detected in Newborn Screen
CONGENITAL HYPOTHYROIDISM
• Caused by defect in the embryonic period in thyroid glad production
• Also caused by inborn error of thyroid hormone synthesis (an inherited autosomal recessive trait)
• Can be secondary to pituitary dysfunction
• Thyroid gland is unable to produce T3 and T4

Clinical Manifestations • Mottled skin• Large fontanel• Large tongue• Hypotonia/slow
reflexes• Distended abdomen• Low T4 < 6• High TSH > 40
CONGENITAL HYPOTHYROIDISM
•An infant with a low T4 <6 and a TSH value exceeding 40 is considered to have primary hypothyroidism until proven otherwise
Treatment• Treated with lifelong thyroid replacement
therapy• Synthroid 10-15 mcg/kg/day
• Taken 30-60 minutes before meals for optimal absorption
• Crush pill and mix with formula or breast milk

Parental Education
• Monitor Growth and Development and Thermoregulation
• Labs every 2 weeks then every 3 months look for upper range of normal
• Stress medication compliance
• Teach parents to monitor for medication induced hyperthyroidism
Signs of Medication induced Hyperthyroidism
•Nervousness/anxiety•Diarrhea•Heat intolerance•Weight loss• Increased HR
Outcome
• Prevention of cognitive impairment– newborn screening on all babies
• Early treatment has had significant impact on morbidity
• Most children progress to within normal ranges on developmental assessment
• Poor prognosis in more severe cases
Acquired Hypothyroidism (Hashimoto’s disease)
Acquired Hypothyroidism
• Autoimune disorder• Antibodies and developed against
thyroid gland• Gland becomes inflamed, infiltrated by
antibodies and destroyed• Thyroid produces inadequate levels of
thyroid hormone > age 2• T4 decreases, TSH rises
Types of Acquired Hypothyroidism
• Primary (Hashimoto’s thyroiditis)• Most common• Autoimmune• Childhood, adolescents, females>males
• Secondary• Associated with other conditions that affect the
thyroid• Pituitary and hypothalmic dysfunction
• Tertiary • Radiation, surgery, trauma
Clinical Manifestations
• Goiter• Dry, thick skin• Coarse hair• Fatigue• Cold intolerance• Delayed puberty and
menses
• Decelerated growth
• Edema around eyes, face and hands
• Constipation• Sleepiness • Mental decline-not
permanent cognitive impairment

Acquired Hypothyroidism Treatment
• Thyroid hormone replacement-Synthroid• Starting dose 10 -15 mcg/kg/day
• Taken 30-60 minutes before meals for optimal absorption
• Teach child to swallow pill or crush • Repeat thyroid function test one month should see
normalization of TSH• Requires lifetime follow up• Dose and adjustments based on clinical evaluation & TSH• Prognosis is good if kept euthyroid (normal)

Acquired Hyperthyroidism (Grave’s Disease)
Acquired Hyperthyroidism• A hyperfunction of the thyroid gland• Produces excessive circulating thyroid
hormone (T3 and T4)• Four times more common in girls• Occurs between the ages of
12 – 14 yrs. (puberty)• Manifestations develop gradually with an
interval between onset & diagnosis of 6 to 12 months
• Genetics involved• Follows a viral illness or period of stress
Clinical Manifestations
• Emotional liability• Physical restlessness at rest• Decreased school performance• Excessive appetite without weight gain• Fatigue• Hair fine, unable to curl• Diarrhea• Poor attention span• Insomnia• Increased perspiration/heat intolerance
Clinical Manifestations
• Increased HR • Palpitations• Widened pulse pressure• Exothalmos• Wide-eyed expression with lid lag• Fine tremors• Systolic murmurs
Thyroid Storm
• Acute Onset• Severe irritability & restlessness• Vomiting and diarrhea• Hyperthermia• Hypertension• Severe tachycardia• Prostration• May progress to death
Treatment
• To suppress thyroxine• PTU - propythioracil • MTZ – methimazole
• Subtotal thyroidectomy
• Ablation with radioiodine
Nursing Care• Needs quiet un-stimulating environment
conducive to rest• Maintain a regular routine to minimizing
stress of coping with unexpected demands
• Physical activity is restricted• Tire easily, experience muscle
weakness and are unable to relax to recoup their strength
Nursing Care
• Increased need for calories to meet their metabolic rate
• Offer 5-6 moderate meals throughout the day, and vitamin supplements
• Stress good hygiene because of excessive sweating
• If taking PTU or MTZ observe for side effects of medications• Neutropenia and Hepatotoxicity
Nursing Care
• If surgery is planned administer iodine a few weeks before the procedure• Mixed in a strong-tasting fruit juice given
through a straw• Fear of having throat cut is real• Post-op position neck slightly flexed and
observe for bleeding• Supplemental thyroid hormone then for life
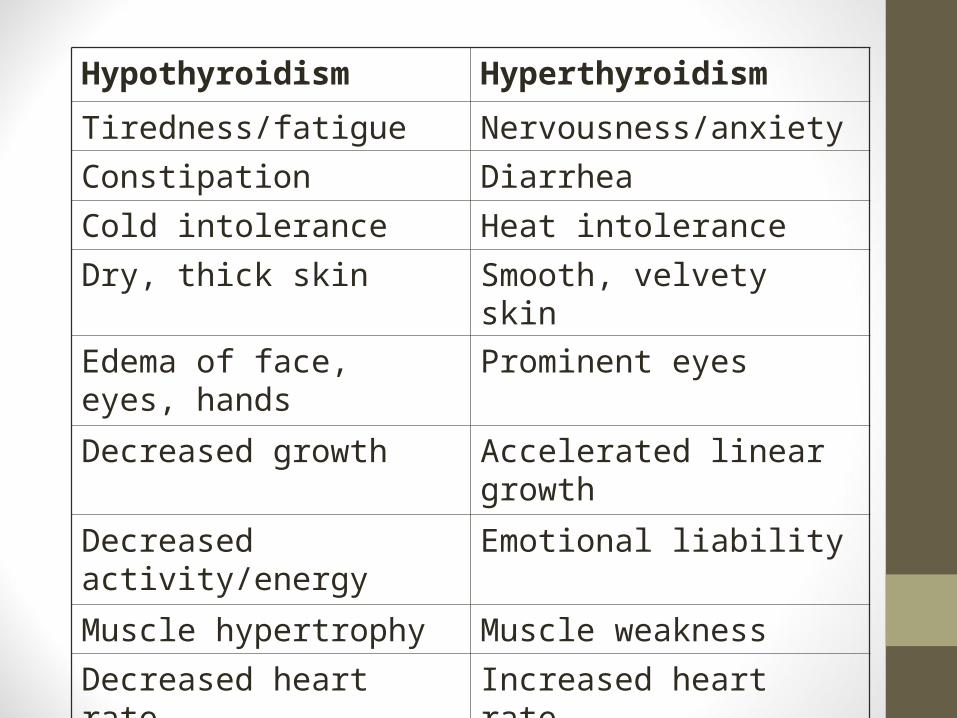
Hypothyroidism Hyperthyroidism
Tiredness/fatigue Nervousness/anxiety
Constipation Diarrhea
Cold intolerance Heat intolerance
Dry, thick skin Smooth, velvety skin
Edema of face, eyes, hands
Prominent eyes
Decreased growth Accelerated linear growth
Decreased activity/energy Emotional liability
Muscle hypertrophy Muscle weakness
Decreased heart rate Increased heart rate
Growth Hormone Deficiency
Growth Hormone Deficiency
• Failure of the pituitary to produce growth hormone
• Affected boys=girls• Boys tend to be evaluated more• 75% cause is idiopathic• Can be a result of injury and destruction of
anterior pituitary gland from• Brain tumor• Infection• radiation
Symptoms
• Normal size and weight at birth• Within first few years child will fall below
the 3rd percentile on growth chart• Late onset of puberty• Delayed dentition• High-pitched voice• Child-like face with large forehead

Criteria for Suspecting Growth Hormone (GH) Deficiency
• Consistently poor growth (<5 cm/yr)• Growth rate more than two standard
deviations below the mean for age• Downward deviation from the previous
growth curve
Assessment and Diagnosis• Evaluate family history• Prenatal/birth history R/O pituitary tumor• Growth charts
• Diagnosis• X ray, MRI to study bone age• Pituitary function tests
Management
• IM recombinant human growth hormone 2-3 times per week
• Given at bedtime when GH usually peaks• GH is a powder that needs to be mixed
with diluent• Parents/child need teaching• Rapid growth is often painful, pain
management is needed
Nursing Considerations
• Speak to child in age appropriate manner (be careful not to address as a younger child)
• Be discrete when providing step stools, etc• Provide with anticipatory guidance for
adolescence• Dress in clothing that reflects age not size• Choose sports that height is not a requirement
Practice Questions!
A 10-year old with type 1 diabetes tells the school nurse that he has some early signs of hypoglycemia. The nurse recommends that the child:
1. Take an extra injection of regular insulin2. Drink a glass of orange juice3. Skip the next dose of insulin4. Start exercising
An adolescent with Type I diabetes has had several episodes demonstrating lack of diabetic control. The nurse teaches the client by stating: “The best way to maintain control of your disease is to:
1. Check your urine glucose three times a week2. Check the HgA1C every 3 months and every 6 months
when stable3. Check your BG four times a day and HgA1C every 3
months4. Check glucose daily as long as you feel well

A 10-year-old girl with type 1 diabetes comes to the office of the school nurse after recess. She was just out of school for an extended illness and reports that she returned to her usual insulin dosing schedule today. The nurse notices she is nervous with hand tremors, pale, sweaty, and complaining of feeling drowsy. The nurse suspects:
1. Exercise-induced hypoglycemia2. Hyperglycemia caused by increased intake at lunch3. Ketoacidosis caused by infection4. The child is avoiding returning to class
After being diagnosed with Hyperthyroidism, a teenager begins taking PTU for treatment of the disease. What symptom would indicate to the nurse that the dose may be too high?
1. Weight loss2. Polyphagia3. Lethargy4. Difficulty with school work
A child with type 1 diabetes 7:00 am blood glucose is 189. The previous evening at 5:30 pm the child injected rapid insulin and NPH, ate dinner and had a 10 pm snack. The nurse concludes (select all that apply)
1. Rapid insulin dose may be to low2. NPH insulin dose may be to low3. NPH insulin dose may be to high4. The child ate too little dinner5. The child ate too much snack
• The nurse is teaching a parent of a child with type 1 diabetes about the different types of insulin. The nurse assumes the parent understands rapid insulin peak times if the parent states that when injecting at 6:45 am, be sure the child does not miss:1. 7:00 AM Breakfast2. 12:30 PM Lunch3. 6:30 PM Dinner4. 10:00 AM Snack