enamel hypoplasia as a
TRANSCRIPT

Enamel Hypoplasia as aPrerequisite to Rampant Caries
Yihong Li, DDS, MPH, DrPH
Timothy Bromage, PhD
Page W. Caufield, DDS, PhD

Yihong Li in the field
EHP_Beijing, 1996

Enamel hypoplasia (EHP)• Developmental Enamel Defects (DED)
– Various forms of enamel defects seen• Linear
• Pitted
• Opaque (most commonly called hypoplasia)
• Decreased and flawed mineralization, surfaceirregularities
– Colonization/retentive sites for cariogenic bacteria
– Less resistant to acid attack
• Position and extent of defect corresponds timeof insult

Hypoplasia vs White Spot Lesion?
Early – Moderate – Advanced - New definitions?

Conditions preceding EHP
• Malnutrition
• Low birthweight
• Prematurity
• Maternal illness
• Smoking
• Drug abuse
• Liver disease
• Other systemic diseases

Contributing factors tosubsequent caries
• High sugar intake
• Mutans streptococci
– Early colonization of EHP
– MS dominate biota
– Source?
• Poor oral hygiene
• Incisor crowding
• Difficulty with early detection by HCW

SEM scan S-ECC incisor


Prevention of ECC begins with intervention in the pre-natal and perinatal
periods.11 Women should be advised to optimize nutrition during the thirdtrimester and the infant’s first year, when enamel is undergoing maturation.Enamel hypoplasia is common in children with low birthweight or systemicillness in the neonatal period.12,13 There is considerable presumptiveevidence that malnutrition/undernutrition during the perinatal period causeshypoplasia.14 A consistent association exists between clinical hypoplasia andECC.12,15 Cariogenic bacteria (specifically mutans streptococci) may betransmitted to the child; decreasing the mother’s/primarycaregiver’s/sibling(s)’ mutans streptococci …………….
ECC = S-ECC?
Evidence supporting perinatalevents predate EHP
• 37 published studies in literature
• 3 studies
– Li et al., 1994
– Needleman et al., 1994
– Seow, et al.,
EHP_Beijing, 1996

•Macroscopic examination of 455 primary incisors from childrenhaving perinatal histories
•Enamel defects reported in 77% of children from"underdeveloped" countries. This study – 18.5% prevalence
•Antecedents to hypoplasia:
•Delayed pre-natal care past first trimester (p <0.007)
•Premature labor (p<0.004)
•Prematurity (p<0.001)
•Special care nursery (p<0.005)
•Greater prepregnancy weight of mothers (p<0.001)
•Measles infection (p<0.0008)
•Smoking (p<0.008)
1994

•Case-control study of 617 Australian children age <4 yo
•S-ECC group receiving restorative treatment under generalanesthesia
•EHP significantly higher among Aboriginal population
•Correlation to low household income, mother education,employment status (p<0.001)
•Significant risk indicators:
•Enamel hypoplasia (OR 4.2)
•Presence of S. mutans (OR 4.8)
•Sweeten drinks/diet (OR 4.0)
•Mother's anxiety (OR 5.1)
Caries Research 2009

• 25 percent of this racial group lives at the poverty level.
• American Indian/Alaska Native infants are 3.7 times aslikely as non-Hispanic white infants to have mothers whobegan prenatal care in the 3rd trimester or did notreceive prenatal care at all.
• American Indian/Alaska Native adults were 2.3 times aslikely as white adults to be diagnosed with diabetes.
• American Indian/Alaska Native adults were 1.6 times aslikely as White adults to be obese.

S-ECC?

Enamel Hypoplasia (EHP)
- pits -
EHP_Beijing, 1996

Linear enamel hypoplasia onprimary incisors
EHP + Caries
EHP_Beijing, 1996

Caries over EHP lesionspattern!
EHP_Beijing, 1996

Rapp R. & Winter GB, 1979
Prenatal EHPThe marked EHP affecting the 2/3 ofthe enamel on these maxillary primaryincisors is evidence of a severemetabolic disturbance occurredprobably during the 2nd and 3rd
trimesters of pregnancy.
Neonatal EHPThe wide band of EHP affecting theprimary teeth in this case wasassociated with preterm birth and awith weight of approximately 1.3 kg.LBW immature babies sufferconsiderable metabolic disturbanceduring the neonatal period and this isoften reflected in defectiveamelogenesis.

EHP first, then caries
Brazil_ 1999
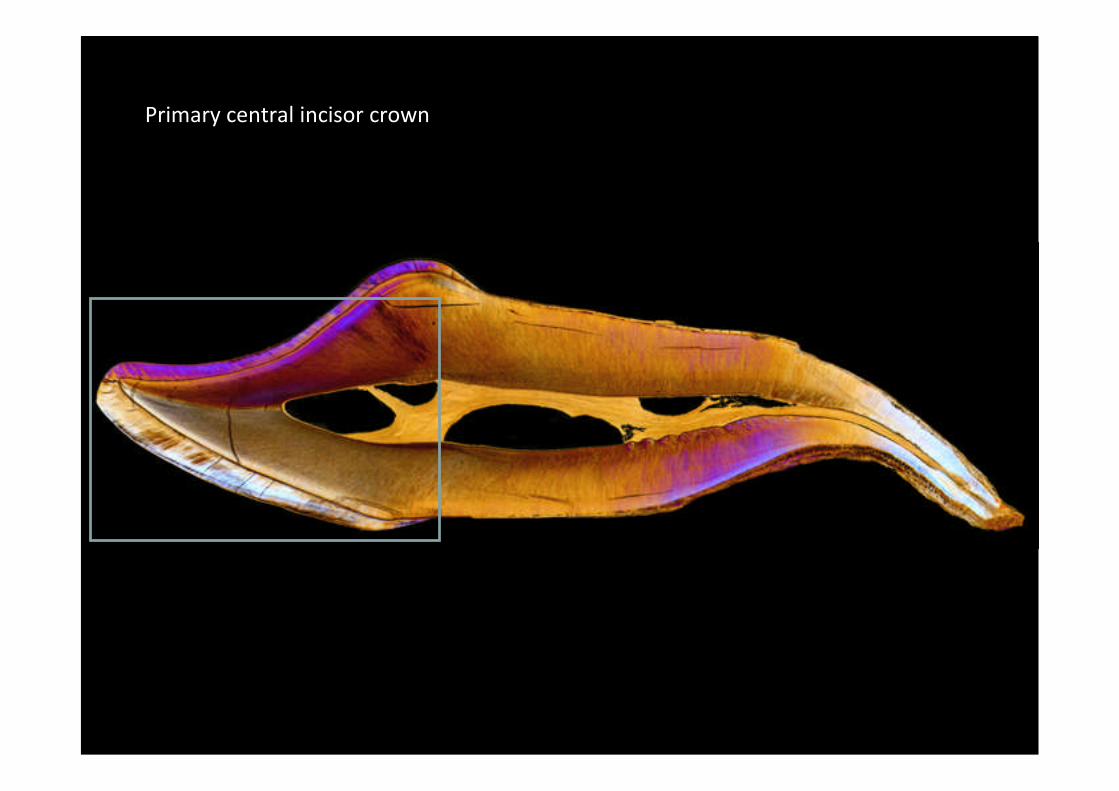
Primary central incisor crown

Neonatal lines in enamel and dentine
EDJ
Primary centralincisor crown fromchild with S- ECC
Carious enamel

Neonatal line in dentine only
Primary centralincisor crown fromnormal child

CROWN FORMATION

Appositional stage
Striae ofRetzius
Perikymata
Cross-striations
Imb
rica
tion
al
sta
ge
Enamel
Hunter-Schregerbands
Prisms
Dentine
EDJ
ENAMEL CROWN STRUCTURE
Rozzi, F.R., Walker, C., Bromage, T.G. 1999 Early hominid dental development and climate change. In (Bromage, T.G., Schrenk, F., Eds) African Biogeography, ClimateChange, and Early Hominid Evolution. Oxford University Press: New York. pp. 349-363.
Dentinehorns

Pulp
Dentine
Enamel
EDJ
*2
*1
*1
*2
Bromage, T.G. 1991 Enamel incremental periodicity in the Pigtailed Macaque: A polychrome fluorescent labeling study of dental hard tissues. American Journal of PhysicalAnthropology,86:205-214.
ENAMEL INCREMENTAL DEVELOPMENT

ENAMEL CELLS SHOW CIRCADIAN OSCILLATION

Enamelprismorientationand directionof growth
Striae ofRetzius andtheinstantaneousforming front
Daily cross striations
ENAMEL CROSS STRIATIONS

Striae of Retzius
ENAMEL STRIAE OF RETZIUS

ENAMEL STRIAE OF RETZIUS AND HOMININ BODYSIZE
Bromage, T.G., Lacruz, R.S., Hogg, R., Goldman, H.M., McFarlin, S.C., Warshaw, J., Dirks, W., Perez-Ochoa, A., Smolyar, I., Enlow, D.H., Boyde, A. 2009Lamellar bone is an incremental tissue reconciling enamel rhythms, body size, and organismal life history. Calcified Tissue International 84: 388-404.
Modern Human:
Range: 6-12 days♀ avg: 9 days♂ avg: 8 days

Basal Metabolic Rate (log)
Stri
aeo
fR
etz
ius
Re
pe
atIn
terv
al
r = 0.90, p < 0.001Callithrix pygmaea,Callithrix jacchus , Sagunius oedipus
Callimico goeldii, Leontopithecus rosalia,Aotus sp., Saimiri sciureus
Erythrocebus patas,Hylobates lar
Alouatta palliata Pan troglodytes
Papio anubis
Homo sapiens sapeins
Pongo pygmaeus
Relationship Between Striae of Retzius Repeat Interval and BMR(ml O2/h) Among Primates

ENAMEL INCREMENTAL GROWTH RATE VARIABILITY

Striae of Retzius Perikymata
RELATIONSHIP BETWEEN STRIAE OF RETZIUSAND PERIKYMATA

Dean, M.C., Wood, B.A. 1981 Developing pongid dentition and its use for ageing individual crania in comparative cross-sectional growth studies. Folia Primatologia 36:111-127.
HUMAN DENTALDEVELOPMENT ANDCALIBRATED ENAMELINCREMENTS
Bromage, T.G. & Dean, M.C. 1985 Re-evaluation of the age at death of immature fossil hominids. Nature, 317:525-527.

PERIKYMATA (SEM)

PERIKYMATA(CSOM)

ENAMEL SURFACE TOPOGRAPHIESARE HAVENS FOR MICROBES