ena connection june/july 2014
DESCRIPTION
ÂTRANSCRIPT
connectionJune/July 2014 Volume 38, Issue 6
the Official Magazine of the Emergency Nurses Association
CLASSINCOMING
Tomorrow’s Looking Even Brighter as ENA Attracts
Surge of Students at NSNA Convention
14 - 15
PLUS ...♦ Record Number of Emergency Nurses at Day on the Hill 8
♦ How GENE Course Will Help a Hundred Times Over 24

The Emergency Nurses Association is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation.
Available Now Visit www.ena.org/TNCC to find a course near you.
2 Day Intensive Course § 24 Chapter Comprehensive Manual § Hands-on Skill Stations 5 Online Modules § Special Population Chapters § 17.65 Contact Hours
TNCC offers interactive learning with scenario-based assessments. § A Systematic Approach to the Initial Assessment § Hands-on Training to Provide Expert Care § Evidence-based Content Developed by Trauma Experts § Patient Advocacy Regarding Pain Management and Family Presence
SEVENTH EDITIONThe Premier Course for Trauma Care
TNCC Ad_Connection_Full_05 2014.indd 1 4/7/14 10:32 AM

3
Advocating For Children Who Need Emergency Care
FROM THE PRESIDENT | Deena Brecher, MSN, RN, APN, ACNS-BC, CEN, CPEN
ENA has made support for the EMSC
program one of its top priorities. In fiscal
year 2014, ENA worked closely with other
national health care groups, especially the
American Academy of Pediatrics, to prevent
further devastating cuts for EMSC. For fiscal
year 2015, which starts Oct. 1, we joined our
coalition partners in sending a letter to the
House and Senate Appropriations Committee
requesting $21.1 million for EMSC.
In addition to protecting federal funding
for the EMSC program, ENA is actively
supporting House and Senate bills (H.R.
4290 and S. 2154) that would continue the
EMSC program until 2019. Without the
passage of the reauthorization legislation,
the EMSC program will expire at the end of
the fiscal year on Sept. 30.
In 2013, ENA supported two
major EMSC initiatives, the
National Pediatric Readiness
Project (left) and the Pediatric
Interfacility Transport Toolkit (below,
left). The toolkit was a joint venture
between EMSC, ENA and the Society of
Trauma Nurses and provides
resources to facilitate the safe
transfer and transport of a
pediatric patient.
The National Pediatric Readiness Project
was an effort vigorously supported by ENA
on the national, state and local levels. The
goal of this project was to measure an ED’s
readiness to care for a child in an emergency
situation. ENA joined the AAP and the
American College of Emergency Physicians
as strong supporters of this effort. In 2013,
we asked members to identify departmental
leaders and encourage their EDs to
participate in the survey. We encouraged
our members to partner with
their state EMSC program
manager (left) to identify ways
to work together to increase
participation in the survey.
All of the partnering and support paid
off. The results are in, and more than 4,000
EDs participated in the survey. As a nation,
the average readiness score was 69. The
Dates to Remember
PAGE 4Free CE of the Month Members in Motion
PAGE 25Future of Your Nursing
PAGE 28ENA Foundation
PAGE 36Academy of Emergency Nursing
Regular Features
Through June 11, 2014, noon CDT Voting for ENA National Elections (www.ena.org/about/elections)
June 13, 2014 Application deadline for Emergency Nursing 2015 Conference Planning Committee
PAGE 6Update From ENA Headquarters
PAGE 8Day on the Hill 2014
PAGE 10Washington Watch: New Bipartisan Law Expands Access For Mentally Ill
PAGES 12ENA Merging Conferences in 2015 to Create Single Amazing Experience
PAGE 14Student Nurses Swarm Up to ENA
PAGE 21Survey Says! Your Voice Carries
PAGE 222014 Proposed Resolutions and Bylaws Amendments
PAGE 24Texas Health System Buys GENE Course in Bulk for ED Nurses
PAGE 26ENA Partners With Genentech to Launch Stroke Management Course
PAGE 27Know Your ENA Practice Resources
PAGE 34Military, ED Nurses Not So Different
ENA Exclusives
I recently had the opportunity to represent ENA at the Emergency Medical Services for
Children National Resource Center Advisory Council meeting. The mission of EMSC is to
reduce child and youth mortality and morbidity caused by severe illness or trauma.
Administered through the Health Resources and Service Administration, EMSC funds and
supports state grants to improve pediatric emergency care throughout the prehospital and
emergency department environments. The EMSC program has provided funding to
all 50 states, the District of Columbia and U.S. territories to support pediatric
emergency care improvement projects and initiatives. If you are unfamiliar with
EMSC, the QR code at left will take you to resources and information.
Official Magazine of the Emergency Nurses Association
Continued on page 11
Treatment methods
for hemorrhagic
shock have changed,
and the latest free
continuing
education session
from ENA will help you stay on top of the situation.
Available to you starting June 1 . . .‘‘Stop the Fluid! Permissive Hypotension and
Blood in the Shock Room,’’ presented by
Elda G. Ramirez,
PhD, RN,
FNP-BC, FAEN,
FAANP. (Credit:
1.0 contact hour.)
Ramirez leads a
review of the old
methods of
managing hemorragic shock and the current
research that changed the practice. From there,
you’ll revisit pathophysiology of shock and
coagulation factors and review the rationale for
how the new methods save trauma patients’ lives.
To take this and other eLearning courses free as
an ENA member:
• Go to www.ena.org/freeCE, where you’ll log
in as a member (or create an account).
• Add desired courses to your cart and
‘‘check out.’’
• Proceed to your Personal Learning Page to
start or complete any course for which you
have registered or to print a final certificate.
• To return to your Personal Learning Page later,
go to www.ena.org and find ‘‘Go to Personal
Learning Page’’ under the Education tab.
Please be sure you are using the e-mail address
associated with your membership when logging in.
If you have questions about any free eLearning
course or the checkout process, e-mail
ENA Connection is published 11 times per year from January to December by: The Emergency Nurses Association
915 Lee Street Des Plaines, IL 60016-6569
and is distributed to members of the association as a direct benefit of membership. Copyright ©2014 by the Emergency Nurses Association. Printed in the U.S.A.Periodicals postage paid at the Des Plaines, IL, Post Office and additional mailing offices.
POSTMASTER: Send address changes to ENA Connection915 Lee StreetDes Plaines, IL 60016-6569ISSN: 1534-2565Fax: 847-460-4002 Website: www.ena.orgE-mail: [email protected]
Non-member subscriptions are available for $50 (USA) and $60 (foreign). For editorial inquiries, e-mail [email protected]
Publisher:Kathy Szumanski, MSN, RN, NE-BCEditor-in-Chief:Amy Carpenter AquinoAssociate Editor:Josh GabySenior Writer:Kendra Y. MimsEditorial Assistant:Renée Herrmann
BOARD OF DIRECTORSOfficers:President:
Deena Brecher, MSN, RN, APN, ACNS-BC, CEN, CPEN
President-elect: Matthew F. Powers, MS, BSN, RN, MICP, CEN
Secretary/Treasurer: Kathleen E. Carlson, MSN, RN, CEN, FAEN
Immediate Past President: JoAnn Lazarus, MSN, RN, CEN
Directors:
Ellen (Ellie) H. Encapera, RN, CENMitch Jewett, AA, RN, CEN, CPEN Michael D. Moon, PhD, MSN, RN,
CNS-CC, CEN, FAENSally K. Snow, BSN, RN, CPEN, FAENJeff Solheim, MSN, RN-BC, CEN,
CFRN, FAENJoan Somes, PhD, MSN, RN-BC, CEN,
CPEN, FAEN, NREMT-PKaren K. Wiley, MSN, RN, CEN
Executive Director: Susan M. Hohenhaus, LPD, RN, CEN, FAEN
Member Services: 800-900-9659
Nightingale Honor for Direct CareDonna Gorman, BSN, RN, a staff
nurse at Bethesda Butler Hospital
Emergency Department in
Hamilton, Ohio, shares that
colleague David Sens, RN, has
received the Florence Nightingale
Award recognizing professional
nurses in the
greater Cincinnati
area for their
contributions to
direct patient care.
Sens is co-leader of
the ED’s shared
leadership and
patient satisfaction committees. He
also participates in two to three
nursing mission trips per year and
recently returned from Haiti.
◆ The emergency department of
Terra Haute Regional Hospital in
Terre Haute, Ind., was the
department with the greatest
number of certified nurses — 11,
up from two — and was treated to
breakfast by the hospital as part of
its Certified Nurses Day observance
March 19. ED staff nurse Merry
Addison, RN, MSN, CEN, FAEN,
also reports that the ED staff has
reached out to the critical care unit,
sponsoring one CCRN exam each
year for the last three years. The
number of CCRN nurses in the
intensive care unit has jumped
from one to four, with six other
nurses studying for the exam.
◆ Kristine Kenney Powell, RN,
MSN, CEN, NEA-BC, director of
emergency services for Baylor
Health Care System, has been
appointed to represent ENA on the
Joint Commission’s Professional and
Technical Advisory Committee
(PTAC), which reviews
recommendations for the
commission’s Hospital Accreditation
Program. More than 40 national
health care associations and the
public are represented on the
committee. Powell’s term runs
through 2019. Deena Brecher,
MSN, RN, APN, ACNS-BC, CEN,
CPEN, the 2014 ENA president, is
the alternate representative, and
ENA Chief Nursing Officer Kathy
Szumanski, MSN, RN, NE-BC,
serves as the ENA liaison. The
PTAC’s first call was April 2, with
the next scheduled for June 25.
Do you have a recent professional or educational success story you want to share about yourself or an ENA member colleague? E-mail it to [email protected] with the subject line “Members in Motion.”
David Sens

When vascular access presents a challenge
Go directly to the bone with the EZ-IO® Intraosseous Vascular Access SystemTrust the EZ-IO Intraosseous Vascular Access System for immediate vascular access for your difficult vascular access (DVA) patients
With the EZ-IO System, getting immediate vascular access for DVA patients is:
> Safe: <1% serious complication rate1*
> Fast: Vascular access with anesthesia and good flow in 90 seconds2*
> Efficient: 97% first-attempt access success rate3
> Versatile: Can be placed by any qualified healthcare provider
> Convenient: Requires no additional equipment or resources4*
Vidacare is now part of TeleflexVidacare.com for more information.
Potential complications may include local or systemic infection, hematoma, extravasations or other complications associated with percutaneous insertion of steri le devices.
References: 1. Rogers JJ, Fox M, Miller LJ, Philbeck TE. Safety of intraosseous vascular access in the 21st century [WoCoVA abstract O-079]. J Vasc Access. 2012;13(2): 1A-40A. 2. Paxton JH, Knuth TE, Klausner HA. Proximal humerus intraosseous infusion: a preferred emergency venous access. J Trauma. 2009;67(3):1-7. 3. Cooper BR, Mahoney PF, Hodgetts TJ, Mellor A. Intra-osseous access (Ez-IO®) for resuscitation: UK military combat experience. J R Army Med Corps. 2007; 153(4):314-316. 4. Dolister M, Miller S, Borron S, et al. Intraosseous vascular access is safe, effective and costs less than central venous catheters for patients in the hospital setting [published online ahead of print January 3, 2013]. J Vasc Access. doi:10.5301/jva.5000130.
*Research sponsored by the Vidacare Corporation.
Teleflex and EZ-IO are trademarks or registered trademarks of Teleflex Incorporated or its affiliates. © 2014 Teleflex Incorporated. 2014-2673
Intraosseous Vascular Access
2014-2673 - EZ-IO CCM-ENA ad-7.indd 1 1/24/14 3:46 PM

6 June/July 2014
After surviving
the coldest
and snowiest
winter in
Chicagoland’s
documented
history, ENA staff
are settled back
into the spring and
summer seasons, providing the warm
and excellent service that ENA members
have come to expect. Here are just a
few of the highlights of what’s
happening at ENA headquarters:
Strategic PartnershipsThe ENA Board of Directors appointed
liaisons to:
• The American Academy of
Pediatrics Pediatric Education for
Prehospital Professionals
course steering committee
(Jaclynn Haymon, RN,
Maryland)
• American College of Emergency
Physicians Hurricane Sandy Recovery
Research Project (Deb Cioffi, MSN, RN,
New Jersey)
• National Association of EMS
Physicians Prehospital Evidence-Based
Guidelines Project (Matthew F. Powers,
MS, BSN, RN, MICP, CEN, California)
• U.S. Department of Health and
Human Services Office of the Assistant
Secretary for Preparedness and
Response Pediatric Transport
Roundtable (Jerri Lynn Zinkan, MPH,
BSN, RN, CPEN, Alabama)
The ENA Board of Directors also
reviewed and commented on the AAP
draft policy Updated Guidelines for
Palivizumah Prophylaxis Among
Infants and Young Children at
Increased Risk of RSV Hospitalization.
The board also endorsed the ACEP
clinical policy Critical Issues in the
Evaluation and Management of
Adult Patients Presenting
to the Emergency
Department with Seizures.
Government RelationsENA’s Government Relations staff
focused on the following federal issues
in the first quarter of 2014: Poison
Control Network Act, Omnibus
Appropriation Bill, Excellence in Mental
Health Act and Trauma Care Legislation.
Government relations staff also
monitored and contacted regulators and
other stakeholders regarding the
shortage of IV saline solution.
At the state level, ENA government
affairs staff assisted the following state
councils:
• Idaho ENA, as the state became the
30th to make the crime of assault/
battery on an emergency nurse a felony
• Kansas ENA and Louisiana ENA,
to assist those states in introducing
similar bills
• Illinois ENA on issues related to
protecting Poison Center funding and
legislation related to credentialing vs.
licensing for emergency RNs,
pre-hospital RNs and trauma nurse
specialists.
Social MediaENA’s Facebook page climbed to
almost 27,000 ‘‘likes,’’ an increase of
7 percent over Q4 2013; Twitter
followers increased to 3,448 (up
8 percent); ENA’s LinkedIn account
grew to 3,118 followers. ENA’s e-mail
open rate also increased significantly
in Q1 2014 at 46.6 percent (Q4 2013
was 33 percent), and there were
171,288 unique visits to ENA’s website,
with 19 percent as mobile viewers.
Conferences and MeetingsENA’s Conferences and Meetings team
is working on the negotiations for
ENA’s 2016 Emergency Nursing
Conference in Los Angeles and the 2017
Emergency Nursing Conference in St.
Louis. The team is also finalizing details
for the 2014 ENA Annual Conference in
Indianapolis and the 2015 Emergency
Nursing Conference in Orlando, Fla., as
well as the 2015 ENA State and Chapter
Leaders Conference, the first time this
will be offered as a stand-alone
meeting. Details will be available soon
for state and chapter leaders.
Institute for Emergency Nursing Research (IENR)IENR staff completed a national
behavioral health study which has
been submitted to the Journal of
Emergency Nursing. A second study on
determining the criteria for discharge
for patients who receive narcotics in
the ED also has been completed. IENR
studies in progress include: Acuity
Assignment (exploring the minimum
data set required to make an accurate
acuity decision); Fatigue and Cognitive
Ability (exploring how fatigue impacts
cognitive ability in calculating weight-
based drug dosages); and Moral
Distress in Emergency Nursing
(exploring what circumstances cause
moral distress in emergency nurses).
Institute for Quality, Safety and Injury Prevention (IQSIP)IQSIP staff completed reviewer training
for Lantern Award cycle 4. IQSIP staff
UPDATE FROM ENA HEADQUARTERS | Susan M. Hohenhaus, LPD, RN, CEN, FAEN, Executive Director
There’s No Freezing ENA’s Progress

Official Magazine of the Emergency Nurses Association 7
State and Chapter Ad_Connection_half_0607 2014_print.pdf 1 5/7/14 9:51 AM
also facilitated committee work related
to ongoing development of a
community injury prevention toolkit, a
primer on implementation of electronic
health records in the ED and an ED
manager’s survival guide.
Institute for Emergency Nursing Education (IENE)Q1 registration for ENA’s free CE
member benefit was 1,357 for three
courses. Ninety-nine nurses purchased
ENA’s staffing guidelines online tool.
ENA’s newly revised
Geriatric Emergency
Nursing Education program,
which launched at the end
of 2013, had 86 registrants in Q1. TNCC
Seventh Edition launched in Q1 with a
total of 1,094 registered for the
eLearning modules and 2,423 registered
for the instructor update rollout.
Course OperationsWith the launch of the TNCC Seventh
Edition, Course Operations is working
with course directors and instructors to
ship new instructor supplements and
provider manuals and to schedule
Seventh Edition provider courses. From
January to March, the department’s
number of phone calls nearly doubled,
call time nearly tripled, and we expect
to see continued high activity through
the instructor update period that runs
through June.
ENPC Fourth Edition continues to
grow, with 12 percent more provider
courses already scheduled for this year.
Updated copies of the provider manual
were sent to all ENPC instructors at the
end of March, and updated copies of
the instructor supplement will go to
them this summer.
MembershipAt the end of Q1 2014, 40,870 members
were on the ENA membership roster.
So far this year we’ve added more than
1,100 members, an annualized growth
rate of more than 11 percent. More and
more emergency nurses are seeing the
value of joining their colleagues in this
member-centered association focused
on providing safe, quality care for
patients.
Financial PositionENA’s first quarter 2014 yielded
healthy, vibrant financial results. ENA’s
revenue growth was 7 percent over the
same time period in the first quarter of
2013, and operating income was more
than double last year’s first quarter,
thanks to growing membership and
courses and a successful Leadership
Conference. ENA staff have managed
expenses well in order to protect and
reinvest member dues and education
revenue in the profession and the
association.

8 June/July 2014
More than 100 ENA members descended upon Washington, D.C., for the association’s annual Day on the Hill event. On Tuesday, May 6, attendees were briefed by Capitol Hill staff and experts on ENA’s two Congressional requests for their meetings. The next day, they met with their senators and representatives in support of S. 153/H.R. 274, the Mental
Health First Aid Act, and H.R. 4080, the Trauma Care Systems and Regionalization of Emergency Care Reauthorization Act.
The morning of May 7 started with the ‘‘Coffee with Congress’’ event on Capitol Hill. Reps. Michael Burgess (R-Texas), the sponsor of H.R. 4080, Lois Capps (D-Calif.), a former nurse and co-chair of the House Nursing Caucus, and Diane Black (R-Tenn.), the only former emergency nurse serving in Congress, addressed ENA attendees.
In their meetings on Capitol Hill, ENA members met with more than 120 senators and representatives and their staffs. These meetings went a long way toward advancing ENA’s public policy agenda and, specifically, the prospects for enacting significant mental health and trauma care bills.
— Marie Grimaldi, ENA communication and PR manager
CAPITAL GAINSRecord Number of Emergency Nurses Attend Annual Day on the Hill
PHOTOS BY JULES CLIFFORD

Official Magazine of the Emergency Nurses Association 9
ENA President Deena Brecher, MSN, RN, APN, ACNS-BC, CEN, CPEN, discusses ENA goals with a staff member for Sen. Kelly Ayotte (R-N.H.).
Rep. Leonard Lance (R-N.J.) meets with a group that includes 2014 ENA President-Elect Matthew F. Powers, MS, BSN, RN, MICP, CEN (front, left).
Mitch Jewett, AA, RN, CEN, CPEN (left), of the ENA Board of Directors chats with Stanley Watkins, chief of staff for Rep. Bobby Rush (D-Ill.).
Look for expanded
coverage from Day on the Hill in the
August issue of ENA
Connection.

June/July 201410
WASHINGTON WATCH | Richard Mereu, JD, ENA Chief Government Relations Officer
As emergency nurses know all too
well, the demand for mental
health services is greater than ever as
untreated mental illness is a major
public health concern in the U.S.
According to the Substance Abuse
and Mental Health Services
Administration, more than 41 million
U.S. adults experienced mental illness
in 2011, and the majority of adults who
have mental health or substance use
disorders do not get the ongoing care
they need. Often, these patients seek
treatment in emergency departments.
This leads to boarding in EDs, as bed
space for psychiatric patients is often
difficult to locate, especially for patients
who lack insurance.
Community mental health clinics
attempt to address this crisis by
providing comprehensive treatment for
children and adults with serious
mental illnesses and addictions. These
facilities, which treat 8 million
Americans each year, are on the front
lines of improving health outcomes,
providing crisis response and
prevention and administering
outpatient mental health services.
Unfortunately, after decades of budget
cuts, these clinics are struggling to
meet the ever-increasing demand for
behavioral health services.
In response to the need for
community-based mental health
services, Sens. Debbie Stabenow
(D-Mich.) and Roy Blunt (R-Mo.) and
Reps. Doris Matsui (D-Calif.) and
Leonard Lance (R-N.J.) introduced the
Excellence in Mental Health Act. The
legislation was designed to improve
quality standards and expand access to
community mental health clinics. It
requires clinics to cover a broad range
of mental health services, including
24-hour psychiatric crisis care, full
assessments and better integration of
physical, mental and substance abuse
treatment.
The bill also addresses the issue of
inadequate funding by allowing
community mental health clinics to be
adequately reimbursed under Medicaid,
just as federally qualified community
health centers are reimbursed for
comprehensive primary care services.
This will give these clinics the financial
resources to provide care for a much
wider population.
Following its introduction, the
Excellence in Mental Health Act
received broad, bipartisan support. In
the House of Representatives, the bill
was co-sponsored by 45
representatives. A similar Senate
version of the bill had 24 co-sponsors.
The bill also was backed by more than
50 mental health, veteran and law
enforcement organizations.
ENA was a strong supporter of the
Excellence in Mental Health Act and
worked closely with both elected
representatives and other national
health care organizations as it made its
way through the House and Senate. In
New Bipartisan Law Expands Access For Mentally Ill

survey also provided a national
perspective about pediatric patient
volume in our EDs. Sixty-nine
percent of the EDs surveyed treat
fewer than 5,000 pediatric patients
per year, or fewer than 14 per day.
Why is this information important?
Expertise comes with experience. We
need to provide tools and resources
to help emergency nurses improve
pediatric emergency care. There are
some great ENA resources that every
emergency nurse who cares for
children should be aware of.
The first is the ‘‘Guidelines for
the Care of Children in the ED’’
(below, left). A joint policy statement
by ENA, ACEP and AAP, it provides a
primer for resources that every ED
that cares for children
should have. There is a
checklist that you can use
to identify strengths and
opportunities in your own ED.
A second resource that directly
impacts pediatric patient safety is the
ENA position statement
“Weighing Pediatric
Patients in Kilograms’’
(left).
There are two clinical
practice guidelines that
directly address pediatric
emergency care: Noninvasive
Temperature Measurement in the
ED (above, right) and Needle-
Related Procedural
Pain in Pediatric
Patients in the ED (left).
The EMSC National
Resource Center has educational
resources, toolkits, disaster
preparedness information and
many other resources (below,
right) available to the public. The
National Pediatric
Readiness Project website
is also a wealth of
information and resources.
How can you help support the
national effort to improve pediatric
emergency care? I ask you to do two
things:
1. Urge your state representatives
to co-sponsor H.R. 4290 and your
senators to co-sponsor S. 2154. Both
of these bills are bipartisan
legislation, co-sponsored by Rep.
Peter King and Sen. Orrin Hatch.
Not sure how to contact your
representatives? Visit the
EN411 Advocacy
Engagement Page (left)
and find your elected
officials. Let your representatives
know how important this program is
to the emergency care of children in
this country.
2. Find out if your ED participated
in the National Pediatric Readiness
Survey. Each hospital received its
score when it submitted the survey.
The EMSC program managers are
able to provide comparison data for
each state. Talk to your manager
about your ED’s strengths and
opportunities. Then commit to taking
an opportunity to work on a project
or initiative to improve pediatric
emergency care in your department.
Using the resources here, in the
Emergency Nursing Pediatric Course
or from your local or regional
pediatric hospital, I have no doubt
you will have the tools to safely care
for the pediatric patients in your ED.
Each of us has a voice and a role in
improving pediatric emergency care.
How will you use your voice?
March, the Excellence in Mental Health
Act was added to a larger piece of
legislation dealing with Medicare
payments for physicians. Attaching it to
a ‘‘must-pass’’ bill greatly improved the
chances that these important mental
health provisions would become law.
On March 27, the physician
Medicare payment legislation, which
included the Excellence in Mental
Health Act, passed the House of
Representatives on a voice vote. In the
Senate, the bill was approved on a
64-35 vote March 31. It was signed into
law by President Obama on April 1.
The enacted version of the
Excellence in Mental Health Act
establishes an eight-state
demonstration project to expand
mental health services in community-
based clinics. States will be able to
apply through the Department of
Health and Human Services.
The new law could help as many as
750,000 uninsured and low-income
Americans with the most serious and
persistent mental health conditions,
including 100,000 veterans returning
from Iraq and Afghanistan. After an
initial two-year period, the
demonstration program could be
extended to additional states.
The passage of the Excellence in
Mental Health Act is an important
milestone in enhancing the treatment
options for mentally ill patients. It also
represents a significant accomplishment
for ENA’s government relations efforts.
‘‘Many ENA members work in
emergency departments where
behavioral health patients often seek
treatment because of a lack of
community-based mental health
facilities,’’ said ENA President Deena
Brecher, MSN, RN, APN, ACNS-BC,
CEN, CPEN. ‘‘This new law will
improve the quality of care and
increase access for those who need
treatment.’’
From the President Continued from Page 3
Official Magazine of the Emergency Nurses Association 11

June/July 201412
CONFERENCES
From 2 to 1By Amy Carpenter Aquino, ENA Connection
T he land of innovation and celebration is the perfect
setting for ENA’s Emergency Nursing Conference.
Orlando, Fla., home to seven of the world’s top theme
parks, including Walt Disney World, is the host city for the
first ENA Emergency Nursing Conference. From Sept. 28 to
Oct. 3, 2015, ENA’s two conference experiences — Annual
and Leadership conferences — will become one integrated
event in Orlando.
‘‘We are all looking forward to providing our members
and guests an exciting and innovative Emergency Nursing
2015 Conference,’’ said Matthew F. Powers, MS, BSN, RN,
MICP, CEN, the 2014 ENA president-elect. ‘‘A few years
back, our members and vendors responded to a survey
about combining both our Leadership and Annual
conferences into one great conference. We are working
diligently to provide you the best experience in 2015, which
will address both leadership and clinical topics. There will
be opportunities for everyone to learn and grow with new
educational offerings and activities planned in Orlando.
Please join me and your ENA Board of Directors at our first
combined ENA Emergency Nursing Conference.’’
The combined conference will help ENA achieve its goal
of promoting safe practice and safe care through education,
networking and
advocacy. It
promises more
education, more
hands-on
learning labs,
more networking
opportunities and
more fun, all in
one conference.
Attendees can choose courses from both leadership and
clinical practice tracks in an expanded, six-day conference
schedule. The ENA General Assembly will still be held at the
beginning of the conference, but it will be divided into three
half-day formats, giving state leaders and delegates a more
flexible schedule. The new format will free up General
Assembly attendees to attend afternoon educational sessions
or connect and caucus with their states. Authors who need
to revise proposed bylaws amendments and resolutions will
have more focused time to spend on rewrites.
Special-interest groups and networking sessions will be
expanded as well, allowing members to visit two or three
sessions instead of only one.
ENA Combining Conferences in 2015 to Create Single Amazing Experience

Official Magazine of the Emergency Nurses Association 13
ANNUALCONFERENCE
2014
For the latest updates and event details, please visit www.ena.org/AC
Registration Opens June 5§Attend a wide range of educational sessions
§Learn about innovative products and services
§Network with colleagues from around the world
JOIN USINDIANAPOLIS
Indiana Convention Center
October 7-11, 2014
AC14_Connection_half_0607 2014.indd 1 5/8/14 3:36 PM
Expanded educational opportunities, formerly called
presessions, will be presented differently. Instead of being
scheduled before the educational portion of the conference,
these longer-format sessions will be held at different times
throughout the conference to be accessible to more attendees.
Attendees will have more social events for networking
with colleagues, including both an opening and closing
reception. Beginning in 2015, the ENA Awards Gala will
be held in the middle of the conference to give attendees
more opportunities to congratulate the award winners
throughout the week.
The new conference provides all attendees with more
time to take advantage of Orlando’s various attractions,
activities and nightlife.
For ENA staff, the switch to one conference allows
more time to explore new options and focus on
preparing the best
educational and
networking
opportunities for
emergency nurse
professionals.
For a sneak
peek of the ENA
Emergency Nursing
2015 Conference,
look up “Emergency
Nursing 2015 Trailer”
at www.youtube.
com.

June/July 201414
MEMBERSHIP
H ow excited is 23-year-old Carly
Campbell to be a new ENA
member?
She could cry.
Campbell, on the verge of
graduating May 10 from the Palm
Beach Atlantic University nursing
program in West Palm Beach, Fla.,
traveled with three friends to the
National Student Nurses’ Association
annual convention April 9-13 in
Nashville, Tenn. — her first time
attending. She already had visited
ENA’s booth and applied for a student
membership when she heard a
capacity-crowd presentation by ENA
President Deena Brecher, MSN, RN,
APN, ACNS-BS, CEN, CPEN, on what it
means to be an emergency nurse.
The ED is the only place in the
hospital we don’t say no to people. We
take care of every person who comes in
the door.
That, said Campbell, who did her
preceptorship in the emergency
department, was ‘‘the highlight of the
whole conference for me.’’
‘‘It totally clicked a lot of things for
me in my nursing career,’’ she said,
‘‘and I teared up a little bit, I loved it
so much. . . . There’s definitely a
specific personality of people that
gravitate toward the emergency room.
And so to be connected to people who
are actually passionate about
emergency nursing as a whole, and
not just addicted to adrenaline, is
really an amazing resource.’’
Lines of inspired students agreed.
Over three days, ENA signed up 163
new members from 40 states, about
double the signups from last year’s
convention, and added three more
through membership drawings. Traffic
spiked after Brecher’s presentations.
‘‘It was just like a mob,’’ said
Tennessee ENA State Council President
Randy Mitchell, MBA, RN, CEN, who
arranged for pairs of council
volunteers, himself included, to join
Brecher and ENA Member & Course
Services supervisor Lindsay Paxton in
fielding questions and handing out
materials. Answering the call were
Barbara Gibson, RN; Mona Kelley,
MSN, RN; Holly Kunz, MSN, RN, CEN,
CCRN; and Donna Mason, MS, RN,
CEN, FAEN.
By Josh Gaby, ENA Connection
SWARMING UP TO ENAStudent nurses fill the room to hear ENA President Deena Brecher, MSN, RN, APN, ACNS-BC, CEN, CPEN, who snapped this photo from the stage on April 11 and later shared it on her president’s blog (enapresident.wordpress.com).
Message Resonates at NSNA Convention, Leading to More Than 160 New Student Memberships Carly Campbell

‘‘There were so many people
[Saturday], they just filled the booths
next to us and in front of our booth,
and that’s how much of a crowd we
had,’’ Mitchell said. ‘‘It’s really nice to
see the excitement and the enthusiasm
of these young, to-be nurses. A lot of
them are in their last semesters, so
they’re seeing that light at the end of
the tunnel that they’re going to be able
to get out and start doing something.’’
One of those students was Jamie
Scoff, then a month from graduating
from the four-year nursing program at
Salisbury University in Salisbury, Md.
Though her internship the last seven
weeks of school was in an ED, the
NSNA convention was her first
exposure to ENA. Hearing Brecher
sold her on joining. She already is
applying what she’s learning.
‘‘[Brecher] had discussed jumping
right in and trying to impress and wow
everybody that you’re working with,
and so I’ve started arriving 15 minutes
earlier than they want me to come in
and really not holding back at all,’’
Scoff said.
Emily Anderson, who will get her
BSN in August from the nursing
program at Herzing University in
suburban Minneapolis, attended her
first NSNA convention with three
classmates, all of whom joined her in
becoming ENA members after hearing
about ENA’s courses, continuing
education and networking.
‘‘I was kind of in between
emergency nursing and ICU nursing,
and [Brecher] really cleared up a lot of
things about emergency room nursing
that I was a little unclear about,’’
Anderson said.
What no one should be unclear
about is why spreading the word at
NSNA matters.
‘‘When we look at membership and
our membership demographics, we are
starting to see a growth in the
under-30 nurse, which is incredibly
important,’’ Brecher said. ‘‘So I think
we’re starting to really recognize the
value of engaging nurses while they’re
still students.’’
Many of the visitors to the ENA
booth wanted to know how they
might be included as they start out in
emergency nursing. The answer: by
making the ED a mutual teaching
environment.
‘‘I looked at all of them and said,
‘You guys are all experts at evidence-
based practice and doing a lit search,
and that’s a skill that a lot of
experienced nurses that have been
practicing a while don’t have,’ ’’
Brecher said. ‘‘While I, as a new nurse,
might not have the experience to pick
out the sick patient just by looking at
them, I certainly have skills that will
help improve the practice in the
department.’’
Brecher stressed the importance of
ENA state councils and chapters
‘‘harnessing the pixie dust’’ by
including younger members in their
activities. Carly Campbell was already
ahead of her. She attended her first
meeting with the Palm Beach County
Chapter on April 22, less than two
weeks after joining ENA, and was
welcomed by chapter president Janine
Mangold, RN, and about 50 members.
Among them were Campbell’s charge
nurse and a trauma nurse from the
same ED who happens to be on the
chapter board. The topic of the night
was waveform capnography
monitoring — information that came
up the next week when Campbell was
getting ACLS-certified.
ENA is opening doors already.
‘‘As a student getting my footing in
emergency nursing in that career
choice, I was like, ‘Hey, what can you
teach me?’ ’’ Campbell said.
‘‘It was wonderful. I skipped home.
I was like, ‘This is the best.’ ’’
Official Magazine of the Emergency Nurses Association 15
Top: Brecher connects with students at the ENA booth in Nashville, which was staffed by a team of ENA enthusiasts that included (left, from left) Mona Kelley, MSN, RN; Brecher; Tennessee ENA President Randy Mitchell, MBA, RN, CEN; and ENA Member & Course Services supervisor Lindsay Paxton.

THE FIRST AND ONLY…
©2014 Teva Pharmaceuticals USA, Inc. All rights reserved. April 2014 Printed in USA. ADA-40010
When agitation escalates…
HOW LONG CAN YOU WAIT?
INDICATIONS AND USAGEADASUVE® (loxapine) inhalation powder, for oral inhalation use, is a typical antipsychotic indicated for the acute treatment of agitation associated with schizophrenia or bipolar I disorder in adults. Ef� cacy was demonstrated in 2 trials in acute agitation: one in schizophrenia and one in bipolar I disorder.Limitations of Use: As part of the ADASUVE Risk Evaluation and Mitigation Strategy (REMS) Program to mitigate the risk of bronchospasm, ADASUVE must be administered only in an enrolled healthcare facility.
IMPORTANT SAFETY INFORMATION (continued)• After ADASUVE administration, patients must be monitored for signs and symptoms of bronchospasm at
least every 15 minutes for at least 1 hour• ADASUVE can cause sedation, which can mask the symptoms of bronchospasm• Antipsychotic drugs can cause a potentially fatal symptom complex called Neuroleptic Malignant
Syndrome (NMS), manifested by hyperpyrexia, muscle rigidity, altered mental state, irregular pulse or blood pressure, tachycardia, diaphoresis, and cardiac dysrhythmia. Associated features can include escalated serum creatine phosphokinase (CPK) concentration, rhabdomyolysis, elevated serum and urine myoglobin concentration, and renal failure. If NMS occurs, immediately discontinue antipsychotic drugs and other drugs that may contribute to the underlying disorder, monitor and treat symptoms, and treat any concomitant serious medical problems
• ADASUVE can cause hypotension, orthostatic hypotension, and syncope. Use with caution in patients with known cardiovascular disease, cerebrovascular disease, or conditions that would predispose patients to hypotension. In the presence of severe hypotension requiring vasopressor therapy, epinephrine should not be used
• Use ADASUVE with caution in patients with a history of seizures or with conditions that lower the seizure threshold. ADASUVE lowers the seizure threshold. Seizures have occurred in patients treated with oral loxapine and can also occur in epileptic patients
• Use caution when driving or operating machinery. ADASUVE can impair judgment, thinking, and motor skills• The potential for cognitive and motor impairment is increased when ADASUVE is administered
concurrently with other CNS depressants• Treatment with antipsychotic drugs caused an increased incidence of stroke and transient ischemic
attack in elderly patients with dementia-related psychosis; ADASUVE is not approved for the treatment of patients with dementia-related psychosis
• Use of ADASUVE may exacerbate glaucoma or cause urinary retention• The most common adverse reactions (incidence ≥2% and greater than placebo) in clinical studies in
patients with agitation treated with ADASUVE were dysgeusia, sedation, and throat irritation• Pregnancy Category C. Neonates exposed to antipsychotic drugs during the third trimester of pregnancy
are at risk of extrapyramidal and/or withdrawal symptoms after delivery. ADASUVE should be used during pregnancy only if the potential bene� t justi� es the potential risk to the fetus
• Nursing mothers: Discontinue drug or nursing, taking into account the importance of the drug to the mother• The safety and effectiveness of ADASUVE in pediatric patients have not been established
• ADASUVE is contraindicated in patients with the following:— Current diagnosis or history of asthma, chronic obstructive pulmonary disease (COPD), or other lung
disease associated with bronchospasm— Acute respiratory signs/symptoms (eg, wheezing)— Current use of medications to treat airways disease, such as asthma or COPD— History of bronchospasm following ADASUVE treatment— Known hypersensitivity to loxapine or amoxapine. Serious skin reactions have occurred with oral
loxapine and amoxapine• ADASUVE must be administered only by a healthcare professional• Prior to administration, all patients must be screened for a history of pulmonary disease and examined
(including chest auscultation) for respiratory abnormalities (eg, wheezing)• Administer only a single 10 mg dose of ADASUVE within a 24-hour period by oral inhalation using the
single-use inhaler
IMPORTANT SAFETY INFORMATION
WARNING: BRONCHOSPASM andINCREASED MORTALITY IN ELDERLY PATIENTS WITH DEMENTIA-RELATED PSYCHOSIS
BronchospasmADASUVE can cause bronchospasm that has the potential to lead to respiratory distress and respiratory arrest. Administer ADASUVE only in an enrolled healthcare facility that has immediate access on-site to equipment and personnel trained to manage acute bronchospasm, including advanced airway management (intubation and mechanical ventilation). Prior to administering ADASUVE, screen patients regarding a current diagnosis, history, or symptoms of asthma, COPD and other lung diseases, and examine (including chest auscultation) patients for respiratory signs. Monitor for signs and symptoms of bronchospasm following treatment with ADASUVE.Because of the risk of bronchospasm, ADASUVE is available only through a restricted program under a Risk Evaluation and Mitigation Strategy (REMS) called the ADASUVE REMS.Increased Mortality in Elderly Patients With Dementia-Related PsychosisElderly patients with dementia-related psychosis treated with antipsychotic drugs are at an increased risk of death. ADASUVE is not approved for the treatment of patients with dementia-related psychosis.
ADASUVE® (loxapine) inhalation powder 10 mg
Please see Brief Summary of Prescribing Information, including Boxed Warnings, on following pages.
For REMS Program information, visit
ADASUVEREMS.COM or call 855-755-0492
For more information about ADASUVE,
visit ADASUVE.COM
ADASUVE® (loxapine) inhalation powder
HELP DEFUSE THE SITUATION BEFORE AGITATION ESCALATES FURTHER
Breath-actuated, single-use, ready-to-use inhaler1
ORAL INHALATION
FAST ONSET
Statistically signifi cant reduction in agitation at 2 hours, with improvement rapidly achieved at 10 minutes post-dose1
References: 1. ADASUVE [package insert]. Horsham, PA: Teva Select Brands, a division of Teva Pharmaceuticals USA, Inc; December 2013. 2. Data on fi le. Clinical Study Report 004-301. Teva Pharmaceuticals. 3. Data on fi le. Clinical Study Report 004-302. Teva Pharmaceuticals.
Orally inhaled medicine indicated for the acute treatment of agitation associated with schizophrenia or bipolar I disorder in adults
The mean baseline PEC scores in all treatment groups were 17.3 to 17.7.
BIPOLAR I DISORDERSCHIZOPHRENIAENDPOINT
AT 2 HOURS(PRIMARY)
AT 10 MINUTES (SECONDARY)
Reduction from baseline in agitation symptoms2,3
PEC=Positive and Negative Syndrome Scale-Excited Component. Intent-to-treat population with last observation carried forward. Agitation symptoms measured: tension, excitement, poor impulse control, uncooperativeness, hostility. Each item is scored on a scale from 1 to 7 (1=absent, 4=moderate, 7=extreme). Patient total PEC scores ranged from 14 to 31 out of a possible 35.The efficacy of ADASUVE 10 mg in the acute treatment of agitation associated with schizophrenia or bipolar I disorder was established in a short-term (24-hour), randomized, double-blind, placebo-controlled, fixed-dose trial including 344 patients who met DSM-IV criteria for schizophrenia and in another study, 314 patients who met DSM-IV criteria for bipolar I disorder, manic or mixed episodes with or without psychotic features.
ADASUVE ADASUVEPLACEBO PLACEBO
33%49%
10%19%
27%53%
10%23%
10min
S:9.5”
T:14”
T:10”
B:17”
B:12”
S:13.5”
THE FIRST AND ONLY…
©2014 Teva Pharmaceuticals USA, Inc. All rights reserved. April 2014 Printed in USA. ADA-40010
When agitation escalates…
HOW LONG CAN YOU WAIT?
INDICATIONS AND USAGEADASUVE® (loxapine) inhalation powder, for oral inhalation use, is a typical antipsychotic indicated for the acute treatment of agitation associated with schizophrenia or bipolar I disorder in adults. Ef� cacy was demonstrated in 2 trials in acute agitation: one in schizophrenia and one in bipolar I disorder.Limitations of Use: As part of the ADASUVE Risk Evaluation and Mitigation Strategy (REMS) Program to mitigate the risk of bronchospasm, ADASUVE must be administered only in an enrolled healthcare facility.
IMPORTANT SAFETY INFORMATION (continued)• After ADASUVE administration, patients must be monitored for signs and symptoms of bronchospasm at
least every 15 minutes for at least 1 hour• ADASUVE can cause sedation, which can mask the symptoms of bronchospasm• Antipsychotic drugs can cause a potentially fatal symptom complex called Neuroleptic Malignant
Syndrome (NMS), manifested by hyperpyrexia, muscle rigidity, altered mental state, irregular pulse or blood pressure, tachycardia, diaphoresis, and cardiac dysrhythmia. Associated features can include escalated serum creatine phosphokinase (CPK) concentration, rhabdomyolysis, elevated serum and urine myoglobin concentration, and renal failure. If NMS occurs, immediately discontinue antipsychotic drugs and other drugs that may contribute to the underlying disorder, monitor and treat symptoms, and treat any concomitant serious medical problems
• ADASUVE can cause hypotension, orthostatic hypotension, and syncope. Use with caution in patients with known cardiovascular disease, cerebrovascular disease, or conditions that would predispose patients to hypotension. In the presence of severe hypotension requiring vasopressor therapy, epinephrine should not be used
• Use ADASUVE with caution in patients with a history of seizures or with conditions that lower the seizure threshold. ADASUVE lowers the seizure threshold. Seizures have occurred in patients treated with oral loxapine and can also occur in epileptic patients
• Use caution when driving or operating machinery. ADASUVE can impair judgment, thinking, and motor skills• The potential for cognitive and motor impairment is increased when ADASUVE is administered
concurrently with other CNS depressants• Treatment with antipsychotic drugs caused an increased incidence of stroke and transient ischemic
attack in elderly patients with dementia-related psychosis; ADASUVE is not approved for the treatment of patients with dementia-related psychosis
• Use of ADASUVE may exacerbate glaucoma or cause urinary retention• The most common adverse reactions (incidence ≥2% and greater than placebo) in clinical studies in
patients with agitation treated with ADASUVE were dysgeusia, sedation, and throat irritation• Pregnancy Category C. Neonates exposed to antipsychotic drugs during the third trimester of pregnancy
are at risk of extrapyramidal and/or withdrawal symptoms after delivery. ADASUVE should be used during pregnancy only if the potential bene� t justi� es the potential risk to the fetus
• Nursing mothers: Discontinue drug or nursing, taking into account the importance of the drug to the mother• The safety and effectiveness of ADASUVE in pediatric patients have not been established
• ADASUVE is contraindicated in patients with the following:— Current diagnosis or history of asthma, chronic obstructive pulmonary disease (COPD), or other lung
disease associated with bronchospasm— Acute respiratory signs/symptoms (eg, wheezing)— Current use of medications to treat airways disease, such as asthma or COPD— History of bronchospasm following ADASUVE treatment— Known hypersensitivity to loxapine or amoxapine. Serious skin reactions have occurred with oral
loxapine and amoxapine• ADASUVE must be administered only by a healthcare professional• Prior to administration, all patients must be screened for a history of pulmonary disease and examined
(including chest auscultation) for respiratory abnormalities (eg, wheezing)• Administer only a single 10 mg dose of ADASUVE within a 24-hour period by oral inhalation using the
single-use inhaler
IMPORTANT SAFETY INFORMATION
WARNING: BRONCHOSPASM andINCREASED MORTALITY IN ELDERLY PATIENTS WITH DEMENTIA-RELATED PSYCHOSIS
BronchospasmADASUVE can cause bronchospasm that has the potential to lead to respiratory distress and respiratory arrest. Administer ADASUVE only in an enrolled healthcare facility that has immediate access on-site to equipment and personnel trained to manage acute bronchospasm, including advanced airway management (intubation and mechanical ventilation). Prior to administering ADASUVE, screen patients regarding a current diagnosis, history, or symptoms of asthma, COPD and other lung diseases, and examine (including chest auscultation) patients for respiratory signs. Monitor for signs and symptoms of bronchospasm following treatment with ADASUVE.Because of the risk of bronchospasm, ADASUVE is available only through a restricted program under a Risk Evaluation and Mitigation Strategy (REMS) called the ADASUVE REMS.Increased Mortality in Elderly Patients With Dementia-Related PsychosisElderly patients with dementia-related psychosis treated with antipsychotic drugs are at an increased risk of death. ADASUVE is not approved for the treatment of patients with dementia-related psychosis.
ADASUVE® (loxapine) inhalation powder 10 mg
Please see Brief Summary of Prescribing Information, including Boxed Warnings, on following pages.
For REMS Program information, visit
ADASUVEREMS.COM or call 855-755-0492
For more information about ADASUVE,
visit ADASUVE.COM
ADASUVE® (loxapine) inhalation powder
HELP DEFUSE THE SITUATION BEFORE AGITATION ESCALATES FURTHER
Breath-actuated, single-use, ready-to-use inhaler1
ORAL INHALATION
FAST ONSET
Statistically signifi cant reduction in agitation at 2 hours, with improvement rapidly achieved at 10 minutes post-dose1
References: 1. ADASUVE [package insert]. Horsham, PA: Teva Select Brands, a division of Teva Pharmaceuticals USA, Inc; December 2013. 2. Data on fi le. Clinical Study Report 004-301. Teva Pharmaceuticals. 3. Data on fi le. Clinical Study Report 004-302. Teva Pharmaceuticals.
Orally inhaled medicine indicated for the acute treatment of agitation associated with schizophrenia or bipolar I disorder in adults
The mean baseline PEC scores in all treatment groups were 17.3 to 17.7.
BIPOLAR I DISORDERSCHIZOPHRENIAENDPOINT
AT 2 HOURS(PRIMARY)
AT 10 MINUTES (SECONDARY)
Reduction from baseline in agitation symptoms2,3
PEC=Positive and Negative Syndrome Scale-Excited Component. Intent-to-treat population with last observation carried forward. Agitation symptoms measured: tension, excitement, poor impulse control, uncooperativeness, hostility. Each item is scored on a scale from 1 to 7 (1=absent, 4=moderate, 7=extreme). Patient total PEC scores ranged from 14 to 31 out of a possible 35.The efficacy of ADASUVE 10 mg in the acute treatment of agitation associated with schizophrenia or bipolar I disorder was established in a short-term (24-hour), randomized, double-blind, placebo-controlled, fixed-dose trial including 344 patients who met DSM-IV criteria for schizophrenia and in another study, 314 patients who met DSM-IV criteria for bipolar I disorder, manic or mixed episodes with or without psychotic features.
ADASUVE ADASUVEPLACEBO PLACEBO
33%49%
10%19%
27%53%
10%23%
10min
S:9.5”
T:14”
T:10”
B:17”
B:12”
S:13.5”
THE FIRST AND ONLY…
©2014 Teva Pharmaceuticals USA, Inc. All rights reserved. April 2014 Printed in USA. ADA-40010
When agitation escalates…
HOW LONG CAN YOU WAIT?
INDICATIONS AND USAGEADASUVE® (loxapine) inhalation powder, for oral inhalation use, is a typical antipsychotic indicated for the acute treatment of agitation associated with schizophrenia or bipolar I disorder in adults. Ef� cacy was demonstrated in 2 trials in acute agitation: one in schizophrenia and one in bipolar I disorder.Limitations of Use: As part of the ADASUVE Risk Evaluation and Mitigation Strategy (REMS) Program to mitigate the risk of bronchospasm, ADASUVE must be administered only in an enrolled healthcare facility.
IMPORTANT SAFETY INFORMATION (continued)• After ADASUVE administration, patients must be monitored for signs and symptoms of bronchospasm at
least every 15 minutes for at least 1 hour• ADASUVE can cause sedation, which can mask the symptoms of bronchospasm• Antipsychotic drugs can cause a potentially fatal symptom complex called Neuroleptic Malignant
Syndrome (NMS), manifested by hyperpyrexia, muscle rigidity, altered mental state, irregular pulse or blood pressure, tachycardia, diaphoresis, and cardiac dysrhythmia. Associated features can include escalated serum creatine phosphokinase (CPK) concentration, rhabdomyolysis, elevated serum and urine myoglobin concentration, and renal failure. If NMS occurs, immediately discontinue antipsychotic drugs and other drugs that may contribute to the underlying disorder, monitor and treat symptoms, and treat any concomitant serious medical problems
• ADASUVE can cause hypotension, orthostatic hypotension, and syncope. Use with caution in patients with known cardiovascular disease, cerebrovascular disease, or conditions that would predispose patients to hypotension. In the presence of severe hypotension requiring vasopressor therapy, epinephrine should not be used
• Use ADASUVE with caution in patients with a history of seizures or with conditions that lower the seizure threshold. ADASUVE lowers the seizure threshold. Seizures have occurred in patients treated with oral loxapine and can also occur in epileptic patients
• Use caution when driving or operating machinery. ADASUVE can impair judgment, thinking, and motor skills• The potential for cognitive and motor impairment is increased when ADASUVE is administered
concurrently with other CNS depressants• Treatment with antipsychotic drugs caused an increased incidence of stroke and transient ischemic
attack in elderly patients with dementia-related psychosis; ADASUVE is not approved for the treatment of patients with dementia-related psychosis
• Use of ADASUVE may exacerbate glaucoma or cause urinary retention• The most common adverse reactions (incidence ≥2% and greater than placebo) in clinical studies in
patients with agitation treated with ADASUVE were dysgeusia, sedation, and throat irritation• Pregnancy Category C. Neonates exposed to antipsychotic drugs during the third trimester of pregnancy
are at risk of extrapyramidal and/or withdrawal symptoms after delivery. ADASUVE should be used during pregnancy only if the potential bene� t justi� es the potential risk to the fetus
• Nursing mothers: Discontinue drug or nursing, taking into account the importance of the drug to the mother• The safety and effectiveness of ADASUVE in pediatric patients have not been established
• ADASUVE is contraindicated in patients with the following:— Current diagnosis or history of asthma, chronic obstructive pulmonary disease (COPD), or other lung
disease associated with bronchospasm— Acute respiratory signs/symptoms (eg, wheezing)— Current use of medications to treat airways disease, such as asthma or COPD— History of bronchospasm following ADASUVE treatment— Known hypersensitivity to loxapine or amoxapine. Serious skin reactions have occurred with oral
loxapine and amoxapine• ADASUVE must be administered only by a healthcare professional• Prior to administration, all patients must be screened for a history of pulmonary disease and examined
(including chest auscultation) for respiratory abnormalities (eg, wheezing)• Administer only a single 10 mg dose of ADASUVE within a 24-hour period by oral inhalation using the
single-use inhaler
IMPORTANT SAFETY INFORMATION
WARNING: BRONCHOSPASM andINCREASED MORTALITY IN ELDERLY PATIENTS WITH DEMENTIA-RELATED PSYCHOSIS
BronchospasmADASUVE can cause bronchospasm that has the potential to lead to respiratory distress and respiratory arrest. Administer ADASUVE only in an enrolled healthcare facility that has immediate access on-site to equipment and personnel trained to manage acute bronchospasm, including advanced airway management (intubation and mechanical ventilation). Prior to administering ADASUVE, screen patients regarding a current diagnosis, history, or symptoms of asthma, COPD and other lung diseases, and examine (including chest auscultation) patients for respiratory signs. Monitor for signs and symptoms of bronchospasm following treatment with ADASUVE.Because of the risk of bronchospasm, ADASUVE is available only through a restricted program under a Risk Evaluation and Mitigation Strategy (REMS) called the ADASUVE REMS.Increased Mortality in Elderly Patients With Dementia-Related PsychosisElderly patients with dementia-related psychosis treated with antipsychotic drugs are at an increased risk of death. ADASUVE is not approved for the treatment of patients with dementia-related psychosis.
ADASUVE® (loxapine) inhalation powder 10 mg
Please see Brief Summary of Prescribing Information, including Boxed Warnings, on following pages.
For REMS Program information, visit
ADASUVEREMS.COM or call 855-755-0492
For more information about ADASUVE,
visit ADASUVE.COM
ADASUVE® (loxapine) inhalation powder
HELP DEFUSE THE SITUATION BEFORE AGITATION ESCALATES FURTHER
Breath-actuated, single-use, ready-to-use inhaler1
ORAL INHALATION
FAST ONSET
Statistically signifi cant reduction in agitation at 2 hours, with improvement rapidly achieved at 10 minutes post-dose1
References: 1. ADASUVE [package insert]. Horsham, PA: Teva Select Brands, a division of Teva Pharmaceuticals USA, Inc; December 2013. 2. Data on fi le. Clinical Study Report 004-301. Teva Pharmaceuticals. 3. Data on fi le. Clinical Study Report 004-302. Teva Pharmaceuticals.
Orally inhaled medicine indicated for the acute treatment of agitation associated with schizophrenia or bipolar I disorder in adults
The mean baseline PEC scores in all treatment groups were 17.3 to 17.7.
BIPOLAR I DISORDERSCHIZOPHRENIAENDPOINT
AT 2 HOURS(PRIMARY)
AT 10 MINUTES (SECONDARY)
Reduction from baseline in agitation symptoms2,3
PEC=Positive and Negative Syndrome Scale-Excited Component. Intent-to-treat population with last observation carried forward. Agitation symptoms measured: tension, excitement, poor impulse control, uncooperativeness, hostility. Each item is scored on a scale from 1 to 7 (1=absent, 4=moderate, 7=extreme). Patient total PEC scores ranged from 14 to 31 out of a possible 35.The efficacy of ADASUVE 10 mg in the acute treatment of agitation associated with schizophrenia or bipolar I disorder was established in a short-term (24-hour), randomized, double-blind, placebo-controlled, fixed-dose trial including 344 patients who met DSM-IV criteria for schizophrenia and in another study, 314 patients who met DSM-IV criteria for bipolar I disorder, manic or mixed episodes with or without psychotic features.
ADASUVE ADASUVEPLACEBO PLACEBO
33%49%
10%19%
27%53%
10%23%
10min
S:9.5”
T:14”
T:10”
B:17”
B:12”
S:13.5”

THE FIRST AND ONLY…
©2014 Teva Pharmaceuticals USA, Inc. All rights reserved. April 2014 Printed in USA. ADA-40010
When agitation escalates…
HOW LONG CAN YOU WAIT?
INDICATIONS AND USAGEADASUVE® (loxapine) inhalation powder, for oral inhalation use, is a typical antipsychotic indicated for the acute treatment of agitation associated with schizophrenia or bipolar I disorder in adults. Ef� cacy was demonstrated in 2 trials in acute agitation: one in schizophrenia and one in bipolar I disorder.Limitations of Use: As part of the ADASUVE Risk Evaluation and Mitigation Strategy (REMS) Program to mitigate the risk of bronchospasm, ADASUVE must be administered only in an enrolled healthcare facility.
IMPORTANT SAFETY INFORMATION (continued)• After ADASUVE administration, patients must be monitored for signs and symptoms of bronchospasm at
least every 15 minutes for at least 1 hour• ADASUVE can cause sedation, which can mask the symptoms of bronchospasm• Antipsychotic drugs can cause a potentially fatal symptom complex called Neuroleptic Malignant
Syndrome (NMS), manifested by hyperpyrexia, muscle rigidity, altered mental state, irregular pulse or blood pressure, tachycardia, diaphoresis, and cardiac dysrhythmia. Associated features can include escalated serum creatine phosphokinase (CPK) concentration, rhabdomyolysis, elevated serum and urine myoglobin concentration, and renal failure. If NMS occurs, immediately discontinue antipsychotic drugs and other drugs that may contribute to the underlying disorder, monitor and treat symptoms, and treat any concomitant serious medical problems
• ADASUVE can cause hypotension, orthostatic hypotension, and syncope. Use with caution in patients with known cardiovascular disease, cerebrovascular disease, or conditions that would predispose patients to hypotension. In the presence of severe hypotension requiring vasopressor therapy, epinephrine should not be used
• Use ADASUVE with caution in patients with a history of seizures or with conditions that lower the seizure threshold. ADASUVE lowers the seizure threshold. Seizures have occurred in patients treated with oral loxapine and can also occur in epileptic patients
• Use caution when driving or operating machinery. ADASUVE can impair judgment, thinking, and motor skills• The potential for cognitive and motor impairment is increased when ADASUVE is administered
concurrently with other CNS depressants• Treatment with antipsychotic drugs caused an increased incidence of stroke and transient ischemic
attack in elderly patients with dementia-related psychosis; ADASUVE is not approved for the treatment of patients with dementia-related psychosis
• Use of ADASUVE may exacerbate glaucoma or cause urinary retention• The most common adverse reactions (incidence ≥2% and greater than placebo) in clinical studies in
patients with agitation treated with ADASUVE were dysgeusia, sedation, and throat irritation• Pregnancy Category C. Neonates exposed to antipsychotic drugs during the third trimester of pregnancy
are at risk of extrapyramidal and/or withdrawal symptoms after delivery. ADASUVE should be used during pregnancy only if the potential bene� t justi� es the potential risk to the fetus
• Nursing mothers: Discontinue drug or nursing, taking into account the importance of the drug to the mother• The safety and effectiveness of ADASUVE in pediatric patients have not been established
• ADASUVE is contraindicated in patients with the following:— Current diagnosis or history of asthma, chronic obstructive pulmonary disease (COPD), or other lung
disease associated with bronchospasm— Acute respiratory signs/symptoms (eg, wheezing)— Current use of medications to treat airways disease, such as asthma or COPD— History of bronchospasm following ADASUVE treatment— Known hypersensitivity to loxapine or amoxapine. Serious skin reactions have occurred with oral
loxapine and amoxapine• ADASUVE must be administered only by a healthcare professional• Prior to administration, all patients must be screened for a history of pulmonary disease and examined
(including chest auscultation) for respiratory abnormalities (eg, wheezing)• Administer only a single 10 mg dose of ADASUVE within a 24-hour period by oral inhalation using the
single-use inhaler
IMPORTANT SAFETY INFORMATION
WARNING: BRONCHOSPASM andINCREASED MORTALITY IN ELDERLY PATIENTS WITH DEMENTIA-RELATED PSYCHOSIS
BronchospasmADASUVE can cause bronchospasm that has the potential to lead to respiratory distress and respiratory arrest. Administer ADASUVE only in an enrolled healthcare facility that has immediate access on-site to equipment and personnel trained to manage acute bronchospasm, including advanced airway management (intubation and mechanical ventilation). Prior to administering ADASUVE, screen patients regarding a current diagnosis, history, or symptoms of asthma, COPD and other lung diseases, and examine (including chest auscultation) patients for respiratory signs. Monitor for signs and symptoms of bronchospasm following treatment with ADASUVE.Because of the risk of bronchospasm, ADASUVE is available only through a restricted program under a Risk Evaluation and Mitigation Strategy (REMS) called the ADASUVE REMS.Increased Mortality in Elderly Patients With Dementia-Related PsychosisElderly patients with dementia-related psychosis treated with antipsychotic drugs are at an increased risk of death. ADASUVE is not approved for the treatment of patients with dementia-related psychosis.
ADASUVE® (loxapine) inhalation powder 10 mg
Please see Brief Summary of Prescribing Information, including Boxed Warnings, on following pages.
For REMS Program information, visit
ADASUVEREMS.COM or call 855-755-0492
For more information about ADASUVE,
visit ADASUVE.COM
ADASUVE® (loxapine) inhalation powder
HELP DEFUSE THE SITUATION BEFORE AGITATION ESCALATES FURTHER
Breath-actuated, single-use, ready-to-use inhaler1
ORAL INHALATION
FAST ONSET
Statistically signifi cant reduction in agitation at 2 hours, with improvement rapidly achieved at 10 minutes post-dose1
References: 1. ADASUVE [package insert]. Horsham, PA: Teva Select Brands, a division of Teva Pharmaceuticals USA, Inc; December 2013. 2. Data on fi le. Clinical Study Report 004-301. Teva Pharmaceuticals. 3. Data on fi le. Clinical Study Report 004-302. Teva Pharmaceuticals.
Orally inhaled medicine indicated for the acute treatment of agitation associated with schizophrenia or bipolar I disorder in adults
The mean baseline PEC scores in all treatment groups were 17.3 to 17.7.
BIPOLAR I DISORDERSCHIZOPHRENIAENDPOINT
AT 2 HOURS(PRIMARY)
AT 10 MINUTES (SECONDARY)
Reduction from baseline in agitation symptoms2,3
PEC=Positive and Negative Syndrome Scale-Excited Component. Intent-to-treat population with last observation carried forward. Agitation symptoms measured: tension, excitement, poor impulse control, uncooperativeness, hostility. Each item is scored on a scale from 1 to 7 (1=absent, 4=moderate, 7=extreme). Patient total PEC scores ranged from 14 to 31 out of a possible 35.The efficacy of ADASUVE 10 mg in the acute treatment of agitation associated with schizophrenia or bipolar I disorder was established in a short-term (24-hour), randomized, double-blind, placebo-controlled, fixed-dose trial including 344 patients who met DSM-IV criteria for schizophrenia and in another study, 314 patients who met DSM-IV criteria for bipolar I disorder, manic or mixed episodes with or without psychotic features.
ADASUVE ADASUVEPLACEBO PLACEBO
33%49%
10%19%
27%53%
10%23%
10min
S:9.5”
T:14”
T:10”
B:17”
B:12”
S:13.5”
THE FIRST AND ONLY…
©2014 Teva Pharmaceuticals USA, Inc. All rights reserved. April 2014 Printed in USA. ADA-40010
When agitation escalates…
HOW LONG CAN YOU WAIT?
INDICATIONS AND USAGEADASUVE® (loxapine) inhalation powder, for oral inhalation use, is a typical antipsychotic indicated for the acute treatment of agitation associated with schizophrenia or bipolar I disorder in adults. Ef� cacy was demonstrated in 2 trials in acute agitation: one in schizophrenia and one in bipolar I disorder.Limitations of Use: As part of the ADASUVE Risk Evaluation and Mitigation Strategy (REMS) Program to mitigate the risk of bronchospasm, ADASUVE must be administered only in an enrolled healthcare facility.
IMPORTANT SAFETY INFORMATION (continued)• After ADASUVE administration, patients must be monitored for signs and symptoms of bronchospasm at
least every 15 minutes for at least 1 hour• ADASUVE can cause sedation, which can mask the symptoms of bronchospasm• Antipsychotic drugs can cause a potentially fatal symptom complex called Neuroleptic Malignant
Syndrome (NMS), manifested by hyperpyrexia, muscle rigidity, altered mental state, irregular pulse or blood pressure, tachycardia, diaphoresis, and cardiac dysrhythmia. Associated features can include escalated serum creatine phosphokinase (CPK) concentration, rhabdomyolysis, elevated serum and urine myoglobin concentration, and renal failure. If NMS occurs, immediately discontinue antipsychotic drugs and other drugs that may contribute to the underlying disorder, monitor and treat symptoms, and treat any concomitant serious medical problems
• ADASUVE can cause hypotension, orthostatic hypotension, and syncope. Use with caution in patients with known cardiovascular disease, cerebrovascular disease, or conditions that would predispose patients to hypotension. In the presence of severe hypotension requiring vasopressor therapy, epinephrine should not be used
• Use ADASUVE with caution in patients with a history of seizures or with conditions that lower the seizure threshold. ADASUVE lowers the seizure threshold. Seizures have occurred in patients treated with oral loxapine and can also occur in epileptic patients
• Use caution when driving or operating machinery. ADASUVE can impair judgment, thinking, and motor skills• The potential for cognitive and motor impairment is increased when ADASUVE is administered
concurrently with other CNS depressants• Treatment with antipsychotic drugs caused an increased incidence of stroke and transient ischemic
attack in elderly patients with dementia-related psychosis; ADASUVE is not approved for the treatment of patients with dementia-related psychosis
• Use of ADASUVE may exacerbate glaucoma or cause urinary retention• The most common adverse reactions (incidence ≥2% and greater than placebo) in clinical studies in
patients with agitation treated with ADASUVE were dysgeusia, sedation, and throat irritation• Pregnancy Category C. Neonates exposed to antipsychotic drugs during the third trimester of pregnancy
are at risk of extrapyramidal and/or withdrawal symptoms after delivery. ADASUVE should be used during pregnancy only if the potential bene� t justi� es the potential risk to the fetus
• Nursing mothers: Discontinue drug or nursing, taking into account the importance of the drug to the mother• The safety and effectiveness of ADASUVE in pediatric patients have not been established
• ADASUVE is contraindicated in patients with the following:— Current diagnosis or history of asthma, chronic obstructive pulmonary disease (COPD), or other lung
disease associated with bronchospasm— Acute respiratory signs/symptoms (eg, wheezing)— Current use of medications to treat airways disease, such as asthma or COPD— History of bronchospasm following ADASUVE treatment— Known hypersensitivity to loxapine or amoxapine. Serious skin reactions have occurred with oral
loxapine and amoxapine• ADASUVE must be administered only by a healthcare professional• Prior to administration, all patients must be screened for a history of pulmonary disease and examined
(including chest auscultation) for respiratory abnormalities (eg, wheezing)• Administer only a single 10 mg dose of ADASUVE within a 24-hour period by oral inhalation using the
single-use inhaler
IMPORTANT SAFETY INFORMATION
WARNING: BRONCHOSPASM andINCREASED MORTALITY IN ELDERLY PATIENTS WITH DEMENTIA-RELATED PSYCHOSIS
BronchospasmADASUVE can cause bronchospasm that has the potential to lead to respiratory distress and respiratory arrest. Administer ADASUVE only in an enrolled healthcare facility that has immediate access on-site to equipment and personnel trained to manage acute bronchospasm, including advanced airway management (intubation and mechanical ventilation). Prior to administering ADASUVE, screen patients regarding a current diagnosis, history, or symptoms of asthma, COPD and other lung diseases, and examine (including chest auscultation) patients for respiratory signs. Monitor for signs and symptoms of bronchospasm following treatment with ADASUVE.Because of the risk of bronchospasm, ADASUVE is available only through a restricted program under a Risk Evaluation and Mitigation Strategy (REMS) called the ADASUVE REMS.Increased Mortality in Elderly Patients With Dementia-Related PsychosisElderly patients with dementia-related psychosis treated with antipsychotic drugs are at an increased risk of death. ADASUVE is not approved for the treatment of patients with dementia-related psychosis.
ADASUVE® (loxapine) inhalation powder 10 mg
Please see Brief Summary of Prescribing Information, including Boxed Warnings, on following pages.
For REMS Program information, visit
ADASUVEREMS.COM or call 855-755-0492
For more information about ADASUVE,
visit ADASUVE.COM
ADASUVE® (loxapine) inhalation powder
HELP DEFUSE THE SITUATION BEFORE AGITATION ESCALATES FURTHER
Breath-actuated, single-use, ready-to-use inhaler1
ORAL INHALATION
FAST ONSET
Statistically signifi cant reduction in agitation at 2 hours, with improvement rapidly achieved at 10 minutes post-dose1
References: 1. ADASUVE [package insert]. Horsham, PA: Teva Select Brands, a division of Teva Pharmaceuticals USA, Inc; December 2013. 2. Data on fi le. Clinical Study Report 004-301. Teva Pharmaceuticals. 3. Data on fi le. Clinical Study Report 004-302. Teva Pharmaceuticals.
Orally inhaled medicine indicated for the acute treatment of agitation associated with schizophrenia or bipolar I disorder in adults
The mean baseline PEC scores in all treatment groups were 17.3 to 17.7.
BIPOLAR I DISORDERSCHIZOPHRENIAENDPOINT
AT 2 HOURS(PRIMARY)
AT 10 MINUTES (SECONDARY)
Reduction from baseline in agitation symptoms2,3
PEC=Positive and Negative Syndrome Scale-Excited Component. Intent-to-treat population with last observation carried forward. Agitation symptoms measured: tension, excitement, poor impulse control, uncooperativeness, hostility. Each item is scored on a scale from 1 to 7 (1=absent, 4=moderate, 7=extreme). Patient total PEC scores ranged from 14 to 31 out of a possible 35.The efficacy of ADASUVE 10 mg in the acute treatment of agitation associated with schizophrenia or bipolar I disorder was established in a short-term (24-hour), randomized, double-blind, placebo-controlled, fixed-dose trial including 344 patients who met DSM-IV criteria for schizophrenia and in another study, 314 patients who met DSM-IV criteria for bipolar I disorder, manic or mixed episodes with or without psychotic features.
ADASUVE ADASUVEPLACEBO PLACEBO
33%49%
10%19%
27%53%
10%23%
10min
S:9.5”
T:14”
T:10”
B:17”
B:12”
S:13.5”
THE FIRST AND ONLY…
©2014 Teva Pharmaceuticals USA, Inc. All rights reserved. April 2014 Printed in USA. ADA-40010
When agitation escalates…
HOW LONG CAN YOU WAIT?
INDICATIONS AND USAGEADASUVE® (loxapine) inhalation powder, for oral inhalation use, is a typical antipsychotic indicated for the acute treatment of agitation associated with schizophrenia or bipolar I disorder in adults. Ef� cacy was demonstrated in 2 trials in acute agitation: one in schizophrenia and one in bipolar I disorder.Limitations of Use: As part of the ADASUVE Risk Evaluation and Mitigation Strategy (REMS) Program to mitigate the risk of bronchospasm, ADASUVE must be administered only in an enrolled healthcare facility.
IMPORTANT SAFETY INFORMATION (continued)• After ADASUVE administration, patients must be monitored for signs and symptoms of bronchospasm at
least every 15 minutes for at least 1 hour• ADASUVE can cause sedation, which can mask the symptoms of bronchospasm• Antipsychotic drugs can cause a potentially fatal symptom complex called Neuroleptic Malignant
Syndrome (NMS), manifested by hyperpyrexia, muscle rigidity, altered mental state, irregular pulse or blood pressure, tachycardia, diaphoresis, and cardiac dysrhythmia. Associated features can include escalated serum creatine phosphokinase (CPK) concentration, rhabdomyolysis, elevated serum and urine myoglobin concentration, and renal failure. If NMS occurs, immediately discontinue antipsychotic drugs and other drugs that may contribute to the underlying disorder, monitor and treat symptoms, and treat any concomitant serious medical problems
• ADASUVE can cause hypotension, orthostatic hypotension, and syncope. Use with caution in patients with known cardiovascular disease, cerebrovascular disease, or conditions that would predispose patients to hypotension. In the presence of severe hypotension requiring vasopressor therapy, epinephrine should not be used
• Use ADASUVE with caution in patients with a history of seizures or with conditions that lower the seizure threshold. ADASUVE lowers the seizure threshold. Seizures have occurred in patients treated with oral loxapine and can also occur in epileptic patients
• Use caution when driving or operating machinery. ADASUVE can impair judgment, thinking, and motor skills• The potential for cognitive and motor impairment is increased when ADASUVE is administered
concurrently with other CNS depressants• Treatment with antipsychotic drugs caused an increased incidence of stroke and transient ischemic
attack in elderly patients with dementia-related psychosis; ADASUVE is not approved for the treatment of patients with dementia-related psychosis
• Use of ADASUVE may exacerbate glaucoma or cause urinary retention• The most common adverse reactions (incidence ≥2% and greater than placebo) in clinical studies in
patients with agitation treated with ADASUVE were dysgeusia, sedation, and throat irritation• Pregnancy Category C. Neonates exposed to antipsychotic drugs during the third trimester of pregnancy
are at risk of extrapyramidal and/or withdrawal symptoms after delivery. ADASUVE should be used during pregnancy only if the potential bene� t justi� es the potential risk to the fetus
• Nursing mothers: Discontinue drug or nursing, taking into account the importance of the drug to the mother• The safety and effectiveness of ADASUVE in pediatric patients have not been established
• ADASUVE is contraindicated in patients with the following:— Current diagnosis or history of asthma, chronic obstructive pulmonary disease (COPD), or other lung
disease associated with bronchospasm— Acute respiratory signs/symptoms (eg, wheezing)— Current use of medications to treat airways disease, such as asthma or COPD— History of bronchospasm following ADASUVE treatment— Known hypersensitivity to loxapine or amoxapine. Serious skin reactions have occurred with oral
loxapine and amoxapine• ADASUVE must be administered only by a healthcare professional• Prior to administration, all patients must be screened for a history of pulmonary disease and examined
(including chest auscultation) for respiratory abnormalities (eg, wheezing)• Administer only a single 10 mg dose of ADASUVE within a 24-hour period by oral inhalation using the
single-use inhaler
IMPORTANT SAFETY INFORMATION
WARNING: BRONCHOSPASM andINCREASED MORTALITY IN ELDERLY PATIENTS WITH DEMENTIA-RELATED PSYCHOSIS
BronchospasmADASUVE can cause bronchospasm that has the potential to lead to respiratory distress and respiratory arrest. Administer ADASUVE only in an enrolled healthcare facility that has immediate access on-site to equipment and personnel trained to manage acute bronchospasm, including advanced airway management (intubation and mechanical ventilation). Prior to administering ADASUVE, screen patients regarding a current diagnosis, history, or symptoms of asthma, COPD and other lung diseases, and examine (including chest auscultation) patients for respiratory signs. Monitor for signs and symptoms of bronchospasm following treatment with ADASUVE.Because of the risk of bronchospasm, ADASUVE is available only through a restricted program under a Risk Evaluation and Mitigation Strategy (REMS) called the ADASUVE REMS.Increased Mortality in Elderly Patients With Dementia-Related PsychosisElderly patients with dementia-related psychosis treated with antipsychotic drugs are at an increased risk of death. ADASUVE is not approved for the treatment of patients with dementia-related psychosis.
ADASUVE® (loxapine) inhalation powder 10 mg
Please see Brief Summary of Prescribing Information, including Boxed Warnings, on following pages.
For REMS Program information, visit
ADASUVEREMS.COM or call 855-755-0492
For more information about ADASUVE,
visit ADASUVE.COM
ADASUVE® (loxapine) inhalation powder
HELP DEFUSE THE SITUATION BEFORE AGITATION ESCALATES FURTHER
Breath-actuated, single-use, ready-to-use inhaler1
ORAL INHALATION
FAST ONSET
Statistically signifi cant reduction in agitation at 2 hours, with improvement rapidly achieved at 10 minutes post-dose1
References: 1. ADASUVE [package insert]. Horsham, PA: Teva Select Brands, a division of Teva Pharmaceuticals USA, Inc; December 2013. 2. Data on fi le. Clinical Study Report 004-301. Teva Pharmaceuticals. 3. Data on fi le. Clinical Study Report 004-302. Teva Pharmaceuticals.
Orally inhaled medicine indicated for the acute treatment of agitation associated with schizophrenia or bipolar I disorder in adults
The mean baseline PEC scores in all treatment groups were 17.3 to 17.7.
BIPOLAR I DISORDERSCHIZOPHRENIAENDPOINT
AT 2 HOURS(PRIMARY)
AT 10 MINUTES (SECONDARY)
Reduction from baseline in agitation symptoms2,3
PEC=Positive and Negative Syndrome Scale-Excited Component. Intent-to-treat population with last observation carried forward. Agitation symptoms measured: tension, excitement, poor impulse control, uncooperativeness, hostility. Each item is scored on a scale from 1 to 7 (1=absent, 4=moderate, 7=extreme). Patient total PEC scores ranged from 14 to 31 out of a possible 35.The efficacy of ADASUVE 10 mg in the acute treatment of agitation associated with schizophrenia or bipolar I disorder was established in a short-term (24-hour), randomized, double-blind, placebo-controlled, fixed-dose trial including 344 patients who met DSM-IV criteria for schizophrenia and in another study, 314 patients who met DSM-IV criteria for bipolar I disorder, manic or mixed episodes with or without psychotic features.
ADASUVE ADASUVEPLACEBO PLACEBO
33%49%
10%19%
27%53%
10%23%
10min
S:9.5”T:14”
T:10”B:17”
B:12”
S:13.5”

BRIEF SUMMARYADASUVE® (loxapine) inhalation powder, for oral inhalation use The following is a brief summary only; see full prescribing informa-tion, included Boxed Warnings for complete product information.
WARNING: BRONCHOSPASM and INCREASED MORTALITYIN ELDERLY PATIENTS WITH DEMENTIA-RELATED PSYCHOSIS
Bronchospasm ADASUVE can cause bronchospasm that has the potential to lead to respiratory distress and respiratory arrest. Administer ADASUVE only in an enrolled healthcare facility that has immediate access on-site to equipment and personnel trained to manage acute bron-chospasm, including advanced airway management (intubation and mechanical ventilation) [see Warnings and Precautions (5.1, 5.2)]. Prior to administering ADASUVE, screen patients regarding a current diagnosis, history, or symptoms of asthma, COPD and other lung diseases, and examine (including chest auscultation) patients for respiratory signs. Monitor for signs and symptoms of bronchospasm following treatment with ADASUVE [see Dosage and Administration (2.2, 2.4) and Contraindications (4)].Because of the risk of bronchospasm, ADASUVE is available only through a restricted program under a Risk Evaluation and Mitigation Strategy (REMS) called the ADASUVE REMS [see Warnings and Pre-cautions (5.2)]. Increased Mortality in Elderly Patients with Dementia-Related Psychosis Elderly patients with dementia-related psychosis treated with anti-psychotic drugs are at an increased risk of death. ADASUVE is not approved for the treatment of patients with dementia-related psycho-sis [see Warnings and Precautions (5.3)].
1 INDICATIONS AND USAGEADASUVE is a typical antipsychotic indicated for the acute treatment of agitation associated with schizophrenia or bipolar I disorder in adults.“Psychomotor agitation” is defined in DSM-IV as “excessive motor activity associated with a feeling of inner tension.” Patients experiencing agitation often manifest behaviors that interfere with their care (e.g., threatening behaviors, escalating or urgently distressing behavior, self-exhausting behav-ior), leading clinicians to the use of rapidly absorbed antipsychotic medica-tions to achieve immediate control of the agitation [see Clinical Studies (14)].The efficacy of ADASUVE was established in one study of acute agitation in patients with schizophrenia and one study of acute agitation in patients with bipolar I disorder [see Clinical Studies (14)]. Limitations of Use:As part of the ADASUVE REMS Program to mitigate the risk of broncho-spasm, ADASUVE must be administered only in an enrolled healthcare facility [see Warnings and Precautions (5.2)].4 CONTRAINDICATIONSADASUVE is contraindicated in patients with the following:• Current diagnosis or history of asthma, COPD, or other lung disease
associated with bronchospasm [see Warnings and Precautions (5.1)]• Acute respiratory symptomsor signs (e.g., wheezing) [see Warnings
and Precautions (5.1)]• Currentuseofmedicationstotreatairwaysdisease,suchasasthmaorCOPD[see Warnings and Precautions (5.1)]
• HistoryofbronchospasmfollowingADASUVEtreatment[see Warnings and Precautions (5.1)]
• Knownhypersensitivityto loxapineoramoxapine.Seriousskinreac-tions have occurred with oral loxapine and amoxapine.
5 WARNINGS AND PRECAUTIONS5.1 BronchospasmADASUVE can cause bronchospasm that has the potential to lead to respi-ratory distress and respiratory arrest [see Adverse Reactions (6.1)]. Administer ADASUVE only in an enrolled healthcare facility that has immediate access on-site to equipment and personnel trained to manage acute bronchospasm, including advanced airway management (intuba-tion and mechanical ventilation) [see Boxed Warning and Warnings and Precautions (5.2)].Prior to administering ADASUVE, screen patients regarding a current diagnosisorhistoryofasthma,COPD,andotherlungdiseaseassociatedwith bronchospasm, acute respiratory symptoms or signs, current use of medicationstotreatairwaysdisease,suchasasthmaorCOPD;andexam-ine patients (including chest auscultation) for respiratory abnormalities (e.g., wheezing) [See Dosage and Administration (2.2) and Contraindi-cations (4)]. Monitor patients for symptoms and signs of bronchospasm (i.e., vital signs and chest auscultation) at least every 15 minutes for a minimum of one hour following treatment with ADASUVE [see Dosage and Administration (2.4)]. ADASUVE can cause sedation, which can mask the symptoms of bronchospasm.
BecauseclinicaltrialsinpatientswithasthmaorCOPDdemonstratedthatthe degree of bronchospasm, as indicated by changes in forced expira-tory volume in 1 second (FEV1), was greater following a second dose of ADASUVE, limit ADASUVE use to a single dose within a 24 hour period. Advise all patients of the risk of bronchospasm. Advise them to inform the healthcare professional if they develop any breathing problems such as wheezing, shortness of breath, chest tightness, or cough following treatment with ADASUVE.5.2 ADASUVE REMS to Mitigate Bronchospasm Because of the risk of bronchospasm, ADASUVE is available only through a restricted program under a REMS called the ADASUVE REMS. [see Boxed Warning and Warnings and Precautions (5.1)] Required compo-nents of the ADASUVE REMS are:• Healthcarefacilities thatdispenseandadministerADASUVEmustbeenrolled and comply with the REMS requirements. Certified health-care facilities must have on-site access to equipment and personnel trained to provide advance airway management, including intubation and mechanical ventilation.
• WholesalersanddistributorsthatdistributeADASUVEmustenroll inthe program and distribute only to enrolled healthcare facilities.
Further information is available at www.adasuverems.com or 1-855-755-0492.5.3 Increased Mortality in Elderly Patients with Dementia-Related Psychosis Elderly patients with dementia-related psychosis treated with antipsy-chotic drugs are at increased risk of death. Analyses of 17 placebo- controlled trials (modal duration of 10 weeks), largely in patients tak-ing atypical antipsychotic drugs, revealed a risk of death in drug-treated patients of 1.6 to 1.7 times the risk of death in placebo-treated patients. Overthecourseofatypical10-weekcontrolledtrial,therateofdeathindrug-treated patients was about 4.5%, compared to a rate of about 2.6% in the placebo group. Although the cases of death were varied, most of the deaths appeared to be either cardiovascular (e.g., heart failure, sud-dendeath)orinfectious(e.g.,pneumonia)innature.Observationalstud-ies suggest that, similar to atypical antipsychotic drugs, treatment with conventional antipsychotic drugs may increase mortality. The extent to which the findings of increased mortality in observational studies can be attributed to the antipsychotic drug as opposed to some characteristic(s) of the patients is not clear. ADASUVE is not approved for the treatment of elderly patients with dementia-related psychosis [see Boxed Warning].5.4 Neuroleptic Malignant Syndrome Antipsychotic drugs can cause a potentially fatal symptom complex termedNeurolepticMalignantSyndrome(NMS).Clinicalmanifestationsof NMS include hyperpyrexia, muscle rigidity, altered mental status, and autonomic instability (irregular pulse or blood pressure, tachycardia, dia-phoresis, and cardiac dysrhythmia). Associated features can include ele-vatedserumcreatinephosphokinase(CPK)concentration,rhabdomyoly-sis, elevated serum and urine myoglobin concentration, and renal failure. NMS did not occur in the ADASUVE clinical program.The diagnostic evaluation of patients with this syndrome is complicated. It is important to consider the presence of other serious medical con-ditions (e.g.,pneumonia,systemic infection,heatstroke,primaryCNSpathology, central anticholinergic toxicity, extrapyramidal symptoms, or drug fever). The management of NMS should include: 1) immediate discontinua-tion of antipsychotic drugs and other drugs that may contribute to the underlying disorder, 2) intensive symptomatic treatment and medical mon-itoring, and 3) treatment of any concomitant serious medical problems. There is no general agreement about specific pharmacological treatment regimens for NMS.If a patient requires antipsychotic drug treatment after recovery from NMS, the potential reintroduction of drug therapy should be carefully considered. The patient should be carefully monitored, since recurrences of NMS have been reported. 5.5 Hypotension and SyncopeADASUVE can cause hypotension, orthostatic hypotension, and syncope. Use ADASUVE with caution in patients with known cardiovascular dis-ease (history of myocardial infarction or ischemic heart disease, heart failure or conduction abnormalities), cerebrovascular disease, or condi-tions that would predispose patients to hypotension (dehydration, hypo-volemia, or treatment with antihypertensive medications or other drugs that affect blood pressure or reduce heart rate).In the presence of severe hypotension requiring vasopressor therapy, the preferred drugs may be norepinephrine or phenylephrine. Epinephrine should not be used, because beta stimulation may worsen hypotension in the setting of ADASUVE-induced partial alpha blockade.In short-term (24-hour) placebo-controlled trials of patients with agitation associated with schizophrenia or bipolar I disorder, hypotension occurred in 0.4% and 0.8% in the ADASUVE 10 mg and placebo groups, respec-tively. There were no cases of orthostatic hypotension, postural symptoms,
Table 1. Adverse Reactions in 3 Pooled Short-Term, Placebo-Controlled Trials (Studies 1, 2, and 3) in Patients with Schizophrenia or Bipolar Disorder
Adverse ReactionPlacebo(n = 263)
ADASUVE(n = 259)
Dysgeusia 5% 14%Sedation 10% 12%Throat Irritation 0% 3%
Airway Adverse Reactions in the 3 Trials in Acute Agitation Agitated patients with Schizophrenia or Bipolar Disorder: In the 3 short-term (24-hour), placebo-controlled trials in patients with agitation asso-ciated with schizophrenia or bipolar disorder (Studies 1, 2, and 3), bron-chospasm (which includes reports of wheezing, shortness of breath and cough) occurred more frequently in the ADASUVE group, compared to the placebo group: 0% (0/263) in the placebo group and 0.8% (2/259) intheADASUVE10mggroup.Onepatientwithschizophrenia,withouta history of pulmonary disease, had significant bronchospasm requiring rescue treatment with a bronchodilator and oxygen. Bronchospasm and Airway Adverse Reactions in Pulmonary Safety TrialsClinicalpulmonarysafetytrialsdemonstratedthatADASUVEcancausebronchospasm as measured by FEV1, and as indicated by respiratory signs and symptoms in the trials. In addition, the trials demonstrated thatpatientswithasthmaorotherpulmonarydiseases,suchasCOPDare at increased risk of bronchospasm. The effect of ADASUVE on pulmonary function was evaluated in 3 randomized, double-blind, placebo-controlled clinical pulmonary safety trials in healthy volunteers, patientswithasthma,andpatientswithCOPD.Pulmonaryfunctionwasassessed by serial FEV1 tests, and respiratory signs and symptoms were assessed.IntheasthmaandCOPDtrials,patientswithrespiratorysymp-toms or FEV1 decrease of ≥ 20% were administered rescue treatment with albuterol (metered dose inhaler or nebulizer) as required. These patientswerenoteligibleforaseconddose;however,theyhadcontinuedFEV1 monitoring in the trial. HealthyVolunteers: In the healthy volunteer crossover trial, 30 subjects received 2 doses of either ADASUVE or placebo 8 hours apart, and 2 doses of the alternate treatment at least 4 days later. The results for maximum decrease in FEV1 are presented in Table 2. No subjects in this trial devel-oped airway related adverse reactions (cough, wheezing, chest tightness, or dyspnea).Asthma Patients: In the asthma trial, 52 patients with mild-moderate persistent asthma (with FEV1 ≥ 60% of predicted) were randomized to treatment with 2 doses of ADASUVE 10 mg or placebo. The second dose was to be administered 10 hours after the first dose. Approximately 67% of these patients had a baseline FEV1 ≥ 80% of predicted. The remaining patients had an FEV1 60-80% of predicted. Nine patients (17%) were former smokers. As shown in Table 2 and Figure 7, there was a marked decrease in FEV1 immediately following the first dose (maximum mean decreases in FEV1 and % predicted FEV1 were 303 mL and 9.1%, respec-tively). Furthermore, the effect on FEV1 was greater following the second dose (maximum mean decreases in FEV1 and % predicted FEV1 were 537 mL and 14.7 %, respectively). Respiratory-related adverse reactions (bronchospasm, chest discomfort, cough, dyspnea, throat tightness, and wheezing) occurred in 54% of ADASUVE-treated patients and 12% of placebo-treated patients. There were no serious adverse events. Nine of 26 (35%) patients in the ADASUVE group, compared to one of 26 (4%) in the placebo group, did not receive a second dose of study medication, because they had a ≥ 20% decrease in FEV1 or they developed respiratory symptoms after the first dose. Rescue medication (albuterol via metered dose inhaler or nebulizer) was administered to 54% of patients in the ADASUVE group [7 patients (27%) after the first dose and 7 of the remain-ing 17 patients (41%) after the second dose] and 12% in the placebo group (1 patient after the first dose and 2 patients after the second dose).COPDPatients:IntheCOPDtrial,53patientswithmildtosevereCOPD(withFEV1 ≥ 40% of predicted) were randomized to treatment with 2 doses of ADASUVE 10 mg or placebo. The second dose was to be administered 10 hours after the first dose. Approximately 57% of these patients had moderateCOPD[Global Initiative forChronicObstructiveLungDisease(GOLD)StageII];32%hadseveredisease(GOLDStageIII);and11%hadmilddisease(GOLDStageI).AsillustratedinTable2therewasadecreasein FEV1 soon after the first dose (maximum mean decreases in FEV1 and % predicted FEV1 were 96 mL and 3.5%, respectively), and the effect on FEV1 was greater following the second dose (maximum mean decreases in FEV1 and % predicted FEV1 were 125 mL and 4.5%, respectively). Respi-ratory adverse reactions occurred more frequently in the ADASUVE group (19%) than in the placebo group (11%). There were no serious adverse events. Seven of 25 (28%) patients in the ADASUVE group and 1of 27 (4%) in the placebo group did not receive a second dose of study medication because of a ≥ 20% decrease in FEV1 or the development of respiratory symptoms after the first dose. Rescue medication (albuterol via MDI or
presyncope or syncope. A systolic blood pressure ≤90mmHgwithadecrease of ≥20mmHgoccurredin1.5%and0.8%oftheADASUVE10 mg and placebo groups, respectively. A diastolic blood pressure ≤50mmHgwithadecreaseof≥15mmHgoccurredin0.8%and0.4%of the ADASUVE 10 mg and placebo groups, respectively.In 5 Phase 1 studies in normal volunteers, the incidence of hypotension was 3% and 0% in ADASUVE 10 mg and the placebo groups, respec-tively. The incidence of syncope or presyncope in normal volunteers was 2.3% and 0% in the ADASUVE and placebo groups, respectively. In nor-mal volunteers, a systolic blood pressure ≤90mmHgwithadecreaseof ≥20mmHgoccurredin5.3%and1.1%intheADASUVEandplacebogroups, respectively. A diastolic blood pressure ≤ 50 mm Hg with adecrease of ≥15mmHgoccurredin7.5%and3.3%intheADASUVEandplacebo groups, respectively.5.6 SeizuresADASUVE lowers the seizure threshold. Seizures have occurred in patients treated with oral loxapine. Seizures can occur in epileptic patients even during antiepileptic drug maintenance therapy. In short term (24 hour), placebo-controlled trials of ADASUVE, there were no reports of seizures. 5.7 Potential for Cognitive and Motor ImpairmentADASUVE can impair judgment, thinking, and motor skills. In short-term, placebo-controlled trials, sedation and/or somnolence were reported in 12% and 10% in the ADASUVE and placebo groups, respectively. No patients discontinued treatment because of sedation or somnolence.The potential for cognitive and motor impairment is increased when ADASUVEisadministeredconcurrentlywithotherCNSdepressants[see Drug Interactions (7.1)]. Caution patients about operating hazardousmachinery, including automobiles, until they are reasonably certain that therapy with ADASUVE does not affect them adversely. 5.8 Cerebrovascular Reactions, Including Stroke, in Elderly Patients with Dementia-Related PsychosisIn placebo-controlled trials with atypical antipsychotics in elderly patients with dementia-related psychosis, there was a higher incidence of cere-brovascular adverse reactions (stroke and transient ischemic attacks), including fatalities, compared to placebo-treated patients. ADASUVE is not approved for the treatment of patients with dementia-related psycho-sis [see Boxed Warning and Warnings and Precautions (5.3)].5.9 Anticholinergic Reactions Including Exacerbation of Glaucoma and Urinary RetentionADASUVE has anticholinergic activity, and it has the potential to cause anticholinergic adverse reactions including exacerbation of glaucoma or urinary retention. The concomitant use of other anticholinergic drugs (e.g., antiparkinson drugs) with ADASUVE could have additive effects. 6 ADVERSE REACTIONSThe following adverse reactions are discussed in more detail in other sections of the labeling:• Hypersensitivity(seriousskinreactions)[see Contraindications (4)] • Bronchospasm[see Warnings and Precautions (5.1)]• IncreasedMortalityinElderlyPatientswithDementia-RelatedPsycho-
sis [see Warnings and Precautions (5.3)]• NeurolepticMalignantSyndrome[see Warnings and Precautions (5.4)]• Hypotensionandsyncope[see Warnings and Precautions (5.5)]• Seizure[see Warnings and Precautions (5.6)]• Potential forCognitiveandMotorImpairment[see Warnings and Pre-
cautions (5.7)]• CerebrovascularReactions, IncludingStroke, inElderlyPatientswith
Dementia-Related Psychosis [see Warnings and Precautions (5.8)]• AnticholinergicReactionsIncludingExacerbationofGlaucomaandUri-
nary Retention [see Warnings and Precautions (5.9)]6.1 Clinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.The following findings are based on pooled data from three short-term (24-hour), randomized, double-blind, placebo-controlled clinical trials (Studies 1, 2, and 3) of ADASUVE 10 mg in the treatment of patients with acute agitation associated with schizophrenia or bipolar I disorder. In the 3 trials, 259 patients received ADASUVE 10 mg, and 263 received placebo [see Clinical Studies (14)].Commonly Observed Adverse Reactions: In the 3 trials in acute agita-tion, the most common adverse reactions were dysgeusia, sedation, and throat irritation. These reactions occurred at a rate of at least 2% of the ADASUVE group and at a rate greater than in the placebo group. (Refer to Table 1).
S:13.5”
S:9.5”
T:14”
T:10”
B:17”
B:12”

BRIEF SUMMARYADASUVE® (loxapine) inhalation powder, for oral inhalation use The following is a brief summary only; see full prescribing informa-tion, included Boxed Warnings for complete product information.
WARNING: BRONCHOSPASM and INCREASED MORTALITYIN ELDERLY PATIENTS WITH DEMENTIA-RELATED PSYCHOSIS
Bronchospasm ADASUVE can cause bronchospasm that has the potential to lead to respiratory distress and respiratory arrest. Administer ADASUVE only in an enrolled healthcare facility that has immediate access on-site to equipment and personnel trained to manage acute bron-chospasm, including advanced airway management (intubation and mechanical ventilation) [see Warnings and Precautions (5.1, 5.2)]. Prior to administering ADASUVE, screen patients regarding a current diagnosis, history, or symptoms of asthma, COPD and other lung diseases, and examine (including chest auscultation) patients for respiratory signs. Monitor for signs and symptoms of bronchospasm following treatment with ADASUVE [see Dosage and Administration (2.2, 2.4) and Contraindications (4)].Because of the risk of bronchospasm, ADASUVE is available only through a restricted program under a Risk Evaluation and Mitigation Strategy (REMS) called the ADASUVE REMS [see Warnings and Pre-cautions (5.2)]. Increased Mortality in Elderly Patients with Dementia-Related Psychosis Elderly patients with dementia-related psychosis treated with anti-psychotic drugs are at an increased risk of death. ADASUVE is not approved for the treatment of patients with dementia-related psycho-sis [see Warnings and Precautions (5.3)].
1 INDICATIONS AND USAGEADASUVE is a typical antipsychotic indicated for the acute treatment of agitation associated with schizophrenia or bipolar I disorder in adults.“Psychomotor agitation” is defined in DSM-IV as “excessive motor activity associated with a feeling of inner tension.” Patients experiencing agitation often manifest behaviors that interfere with their care (e.g., threatening behaviors, escalating or urgently distressing behavior, self-exhausting behav-ior), leading clinicians to the use of rapidly absorbed antipsychotic medica-tions to achieve immediate control of the agitation [see Clinical Studies (14)].The efficacy of ADASUVE was established in one study of acute agitation in patients with schizophrenia and one study of acute agitation in patients with bipolar I disorder [see Clinical Studies (14)]. Limitations of Use:As part of the ADASUVE REMS Program to mitigate the risk of broncho-spasm, ADASUVE must be administered only in an enrolled healthcare facility [see Warnings and Precautions (5.2)].4 CONTRAINDICATIONSADASUVE is contraindicated in patients with the following:• Current diagnosis or history of asthma, COPD, or other lung disease
associated with bronchospasm [see Warnings and Precautions (5.1)]• Acute respiratory symptomsor signs (e.g., wheezing) [see Warnings
and Precautions (5.1)]• Currentuseofmedicationstotreatairwaysdisease,suchasasthmaorCOPD[see Warnings and Precautions (5.1)]
• HistoryofbronchospasmfollowingADASUVEtreatment[see Warnings and Precautions (5.1)]
• Knownhypersensitivityto loxapineoramoxapine.Seriousskinreac-tions have occurred with oral loxapine and amoxapine.
5 WARNINGS AND PRECAUTIONS5.1 BronchospasmADASUVE can cause bronchospasm that has the potential to lead to respi-ratory distress and respiratory arrest [see Adverse Reactions (6.1)]. Administer ADASUVE only in an enrolled healthcare facility that has immediate access on-site to equipment and personnel trained to manage acute bronchospasm, including advanced airway management (intuba-tion and mechanical ventilation) [see Boxed Warning and Warnings and Precautions (5.2)].Prior to administering ADASUVE, screen patients regarding a current diagnosisorhistoryofasthma,COPD,andotherlungdiseaseassociatedwith bronchospasm, acute respiratory symptoms or signs, current use of medicationstotreatairwaysdisease,suchasasthmaorCOPD;andexam-ine patients (including chest auscultation) for respiratory abnormalities (e.g., wheezing) [See Dosage and Administration (2.2) and Contraindi-cations (4)]. Monitor patients for symptoms and signs of bronchospasm (i.e., vital signs and chest auscultation) at least every 15 minutes for a minimum of one hour following treatment with ADASUVE [see Dosage and Administration (2.4)]. ADASUVE can cause sedation, which can mask the symptoms of bronchospasm.
BecauseclinicaltrialsinpatientswithasthmaorCOPDdemonstratedthatthe degree of bronchospasm, as indicated by changes in forced expira-tory volume in 1 second (FEV1), was greater following a second dose of ADASUVE, limit ADASUVE use to a single dose within a 24 hour period. Advise all patients of the risk of bronchospasm. Advise them to inform the healthcare professional if they develop any breathing problems such as wheezing, shortness of breath, chest tightness, or cough following treatment with ADASUVE.5.2 ADASUVE REMS to Mitigate Bronchospasm Because of the risk of bronchospasm, ADASUVE is available only through a restricted program under a REMS called the ADASUVE REMS. [see Boxed Warning and Warnings and Precautions (5.1)] Required compo-nents of the ADASUVE REMS are:• Healthcarefacilities thatdispenseandadministerADASUVEmustbeenrolled and comply with the REMS requirements. Certified health-care facilities must have on-site access to equipment and personnel trained to provide advance airway management, including intubation and mechanical ventilation.
• WholesalersanddistributorsthatdistributeADASUVEmustenroll inthe program and distribute only to enrolled healthcare facilities.
Further information is available at www.adasuverems.com or 1-855-755-0492.5.3 Increased Mortality in Elderly Patients with Dementia-Related Psychosis Elderly patients with dementia-related psychosis treated with antipsy-chotic drugs are at increased risk of death. Analyses of 17 placebo- controlled trials (modal duration of 10 weeks), largely in patients tak-ing atypical antipsychotic drugs, revealed a risk of death in drug-treated patients of 1.6 to 1.7 times the risk of death in placebo-treated patients. Overthecourseofatypical10-weekcontrolledtrial,therateofdeathindrug-treated patients was about 4.5%, compared to a rate of about 2.6% in the placebo group. Although the cases of death were varied, most of the deaths appeared to be either cardiovascular (e.g., heart failure, sud-dendeath)orinfectious(e.g.,pneumonia)innature.Observationalstud-ies suggest that, similar to atypical antipsychotic drugs, treatment with conventional antipsychotic drugs may increase mortality. The extent to which the findings of increased mortality in observational studies can be attributed to the antipsychotic drug as opposed to some characteristic(s) of the patients is not clear. ADASUVE is not approved for the treatment of elderly patients with dementia-related psychosis [see Boxed Warning].5.4 Neuroleptic Malignant Syndrome Antipsychotic drugs can cause a potentially fatal symptom complex termedNeurolepticMalignantSyndrome(NMS).Clinicalmanifestationsof NMS include hyperpyrexia, muscle rigidity, altered mental status, and autonomic instability (irregular pulse or blood pressure, tachycardia, dia-phoresis, and cardiac dysrhythmia). Associated features can include ele-vatedserumcreatinephosphokinase(CPK)concentration,rhabdomyoly-sis, elevated serum and urine myoglobin concentration, and renal failure. NMS did not occur in the ADASUVE clinical program.The diagnostic evaluation of patients with this syndrome is complicated. It is important to consider the presence of other serious medical con-ditions (e.g.,pneumonia,systemic infection,heatstroke,primaryCNSpathology, central anticholinergic toxicity, extrapyramidal symptoms, or drug fever). The management of NMS should include: 1) immediate discontinua-tion of antipsychotic drugs and other drugs that may contribute to the underlying disorder, 2) intensive symptomatic treatment and medical mon-itoring, and 3) treatment of any concomitant serious medical problems. There is no general agreement about specific pharmacological treatment regimens for NMS.If a patient requires antipsychotic drug treatment after recovery from NMS, the potential reintroduction of drug therapy should be carefully considered. The patient should be carefully monitored, since recurrences of NMS have been reported. 5.5 Hypotension and SyncopeADASUVE can cause hypotension, orthostatic hypotension, and syncope. Use ADASUVE with caution in patients with known cardiovascular dis-ease (history of myocardial infarction or ischemic heart disease, heart failure or conduction abnormalities), cerebrovascular disease, or condi-tions that would predispose patients to hypotension (dehydration, hypo-volemia, or treatment with antihypertensive medications or other drugs that affect blood pressure or reduce heart rate).In the presence of severe hypotension requiring vasopressor therapy, the preferred drugs may be norepinephrine or phenylephrine. Epinephrine should not be used, because beta stimulation may worsen hypotension in the setting of ADASUVE-induced partial alpha blockade.In short-term (24-hour) placebo-controlled trials of patients with agitation associated with schizophrenia or bipolar I disorder, hypotension occurred in 0.4% and 0.8% in the ADASUVE 10 mg and placebo groups, respec-tively. There were no cases of orthostatic hypotension, postural symptoms,
Table 1. Adverse Reactions in 3 Pooled Short-Term, Placebo-Controlled Trials (Studies 1, 2, and 3) in Patients with Schizophrenia or Bipolar Disorder
Adverse ReactionPlacebo(n = 263)
ADASUVE(n = 259)
Dysgeusia 5% 14%Sedation 10% 12%Throat Irritation 0% 3%
Airway Adverse Reactions in the 3 Trials in Acute Agitation Agitated patients with Schizophrenia or Bipolar Disorder: In the 3 short-term (24-hour), placebo-controlled trials in patients with agitation asso-ciated with schizophrenia or bipolar disorder (Studies 1, 2, and 3), bron-chospasm (which includes reports of wheezing, shortness of breath and cough) occurred more frequently in the ADASUVE group, compared to the placebo group: 0% (0/263) in the placebo group and 0.8% (2/259) intheADASUVE10mggroup.Onepatientwithschizophrenia,withouta history of pulmonary disease, had significant bronchospasm requiring rescue treatment with a bronchodilator and oxygen. Bronchospasm and Airway Adverse Reactions in Pulmonary Safety TrialsClinicalpulmonarysafetytrialsdemonstratedthatADASUVEcancausebronchospasm as measured by FEV1, and as indicated by respiratory signs and symptoms in the trials. In addition, the trials demonstrated thatpatientswithasthmaorotherpulmonarydiseases,suchasCOPDare at increased risk of bronchospasm. The effect of ADASUVE on pulmonary function was evaluated in 3 randomized, double-blind, placebo-controlled clinical pulmonary safety trials in healthy volunteers, patientswithasthma,andpatientswithCOPD.Pulmonaryfunctionwasassessed by serial FEV1 tests, and respiratory signs and symptoms were assessed.IntheasthmaandCOPDtrials,patientswithrespiratorysymp-toms or FEV1 decrease of ≥ 20% were administered rescue treatment with albuterol (metered dose inhaler or nebulizer) as required. These patientswerenoteligibleforaseconddose;however,theyhadcontinuedFEV1 monitoring in the trial. HealthyVolunteers: In the healthy volunteer crossover trial, 30 subjects received 2 doses of either ADASUVE or placebo 8 hours apart, and 2 doses of the alternate treatment at least 4 days later. The results for maximum decrease in FEV1 are presented in Table 2. No subjects in this trial devel-oped airway related adverse reactions (cough, wheezing, chest tightness, or dyspnea).Asthma Patients: In the asthma trial, 52 patients with mild-moderate persistent asthma (with FEV1 ≥ 60% of predicted) were randomized to treatment with 2 doses of ADASUVE 10 mg or placebo. The second dose was to be administered 10 hours after the first dose. Approximately 67% of these patients had a baseline FEV1 ≥ 80% of predicted. The remaining patients had an FEV1 60-80% of predicted. Nine patients (17%) were former smokers. As shown in Table 2 and Figure 7, there was a marked decrease in FEV1 immediately following the first dose (maximum mean decreases in FEV1 and % predicted FEV1 were 303 mL and 9.1%, respec-tively). Furthermore, the effect on FEV1 was greater following the second dose (maximum mean decreases in FEV1 and % predicted FEV1 were 537 mL and 14.7 %, respectively). Respiratory-related adverse reactions (bronchospasm, chest discomfort, cough, dyspnea, throat tightness, and wheezing) occurred in 54% of ADASUVE-treated patients and 12% of placebo-treated patients. There were no serious adverse events. Nine of 26 (35%) patients in the ADASUVE group, compared to one of 26 (4%) in the placebo group, did not receive a second dose of study medication, because they had a ≥ 20% decrease in FEV1 or they developed respiratory symptoms after the first dose. Rescue medication (albuterol via metered dose inhaler or nebulizer) was administered to 54% of patients in the ADASUVE group [7 patients (27%) after the first dose and 7 of the remain-ing 17 patients (41%) after the second dose] and 12% in the placebo group (1 patient after the first dose and 2 patients after the second dose).COPDPatients:IntheCOPDtrial,53patientswithmildtosevereCOPD(withFEV1 ≥ 40% of predicted) were randomized to treatment with 2 doses of ADASUVE 10 mg or placebo. The second dose was to be administered 10 hours after the first dose. Approximately 57% of these patients had moderateCOPD[Global Initiative forChronicObstructiveLungDisease(GOLD)StageII];32%hadseveredisease(GOLDStageIII);and11%hadmilddisease(GOLDStageI).AsillustratedinTable2therewasadecreasein FEV1 soon after the first dose (maximum mean decreases in FEV1 and % predicted FEV1 were 96 mL and 3.5%, respectively), and the effect on FEV1 was greater following the second dose (maximum mean decreases in FEV1 and % predicted FEV1 were 125 mL and 4.5%, respectively). Respi-ratory adverse reactions occurred more frequently in the ADASUVE group (19%) than in the placebo group (11%). There were no serious adverse events. Seven of 25 (28%) patients in the ADASUVE group and 1of 27 (4%) in the placebo group did not receive a second dose of study medication because of a ≥ 20% decrease in FEV1 or the development of respiratory symptoms after the first dose. Rescue medication (albuterol via MDI or
presyncope or syncope. A systolic blood pressure ≤90mmHgwithadecrease of ≥20mmHgoccurredin1.5%and0.8%oftheADASUVE10 mg and placebo groups, respectively. A diastolic blood pressure ≤50mmHgwithadecreaseof≥15mmHgoccurredin0.8%and0.4%of the ADASUVE 10 mg and placebo groups, respectively.In 5 Phase 1 studies in normal volunteers, the incidence of hypotension was 3% and 0% in ADASUVE 10 mg and the placebo groups, respec-tively. The incidence of syncope or presyncope in normal volunteers was 2.3% and 0% in the ADASUVE and placebo groups, respectively. In nor-mal volunteers, a systolic blood pressure ≤90mmHgwithadecreaseof ≥20mmHgoccurredin5.3%and1.1%intheADASUVEandplacebogroups, respectively. A diastolic blood pressure ≤ 50 mm Hg with adecrease of ≥15mmHgoccurredin7.5%and3.3%intheADASUVEandplacebo groups, respectively.5.6 SeizuresADASUVE lowers the seizure threshold. Seizures have occurred in patients treated with oral loxapine. Seizures can occur in epileptic patients even during antiepileptic drug maintenance therapy. In short term (24 hour), placebo-controlled trials of ADASUVE, there were no reports of seizures. 5.7 Potential for Cognitive and Motor ImpairmentADASUVE can impair judgment, thinking, and motor skills. In short-term, placebo-controlled trials, sedation and/or somnolence were reported in 12% and 10% in the ADASUVE and placebo groups, respectively. No patients discontinued treatment because of sedation or somnolence.The potential for cognitive and motor impairment is increased when ADASUVEisadministeredconcurrentlywithotherCNSdepressants[see Drug Interactions (7.1)]. Caution patients about operating hazardousmachinery, including automobiles, until they are reasonably certain that therapy with ADASUVE does not affect them adversely. 5.8 Cerebrovascular Reactions, Including Stroke, in Elderly Patients with Dementia-Related PsychosisIn placebo-controlled trials with atypical antipsychotics in elderly patients with dementia-related psychosis, there was a higher incidence of cere-brovascular adverse reactions (stroke and transient ischemic attacks), including fatalities, compared to placebo-treated patients. ADASUVE is not approved for the treatment of patients with dementia-related psycho-sis [see Boxed Warning and Warnings and Precautions (5.3)].5.9 Anticholinergic Reactions Including Exacerbation of Glaucoma and Urinary RetentionADASUVE has anticholinergic activity, and it has the potential to cause anticholinergic adverse reactions including exacerbation of glaucoma or urinary retention. The concomitant use of other anticholinergic drugs (e.g., antiparkinson drugs) with ADASUVE could have additive effects. 6 ADVERSE REACTIONSThe following adverse reactions are discussed in more detail in other sections of the labeling:• Hypersensitivity(seriousskinreactions)[see Contraindications (4)] • Bronchospasm[see Warnings and Precautions (5.1)]• IncreasedMortalityinElderlyPatientswithDementia-RelatedPsycho-
sis [see Warnings and Precautions (5.3)]• NeurolepticMalignantSyndrome[see Warnings and Precautions (5.4)]• Hypotensionandsyncope[see Warnings and Precautions (5.5)]• Seizure[see Warnings and Precautions (5.6)]• Potential forCognitiveandMotorImpairment[see Warnings and Pre-
cautions (5.7)]• CerebrovascularReactions, IncludingStroke, inElderlyPatientswith
Dementia-Related Psychosis [see Warnings and Precautions (5.8)]• AnticholinergicReactionsIncludingExacerbationofGlaucomaandUri-
nary Retention [see Warnings and Precautions (5.9)]6.1 Clinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.The following findings are based on pooled data from three short-term (24-hour), randomized, double-blind, placebo-controlled clinical trials (Studies 1, 2, and 3) of ADASUVE 10 mg in the treatment of patients with acute agitation associated with schizophrenia or bipolar I disorder. In the 3 trials, 259 patients received ADASUVE 10 mg, and 263 received placebo [see Clinical Studies (14)].Commonly Observed Adverse Reactions: In the 3 trials in acute agita-tion, the most common adverse reactions were dysgeusia, sedation, and throat irritation. These reactions occurred at a rate of at least 2% of the ADASUVE group and at a rate greater than in the placebo group. (Refer to Table 1).
S:13.5”
S:9.5”
T:14”
T:10”
B:17”
B:12”
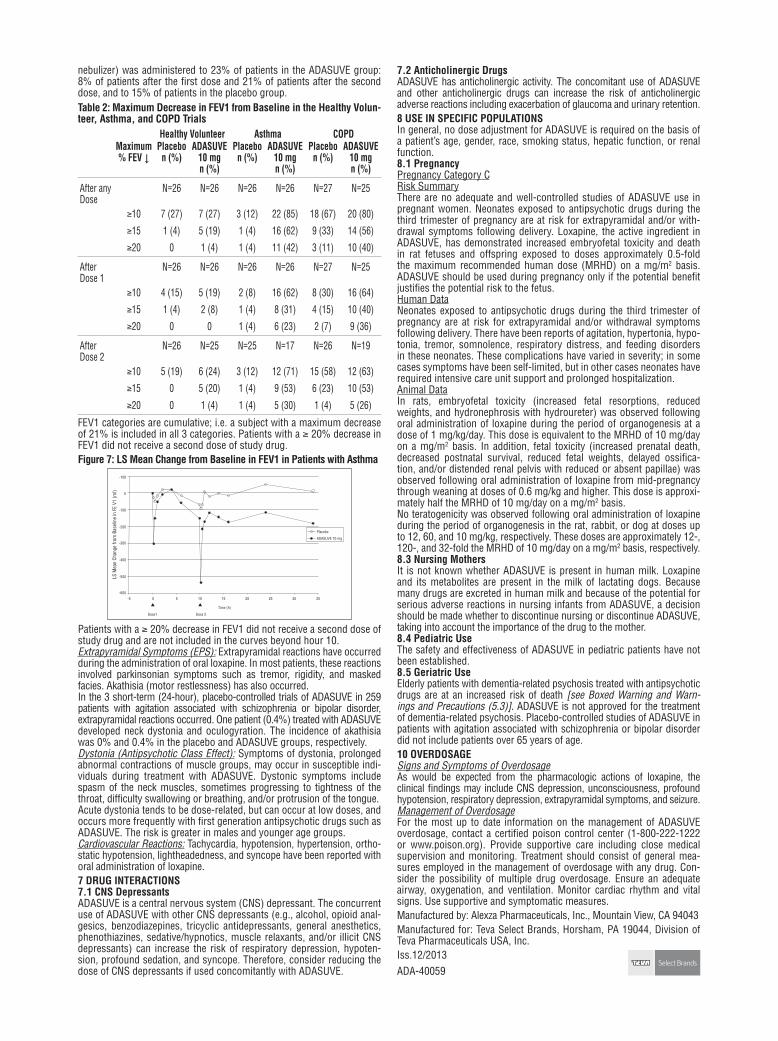
nebulizer) was administered to 23% of patients in the ADASUVE group: 8% of patients after the first dose and 21% of patients after the second dose, and to 15% of patients in the placebo group.Table 2: Maximum Decrease in FEV1 from Baseline in the Healthy Volun-teer, Asthma, and COPD Trials
Healthy Volunteer Asthma COPDMaximum% FEV ↓
Placebon (%)
ADASUVE10 mgn (%)
Placebon (%)
ADASUVE10 mgn (%)
Placebon (%)
ADASUVE10 mgn (%)
After any Dose
N=26 N=26 N=26 N=26 N=27 N=25
≥10 7 (27) 7 (27) 3 (12) 22 (85) 18 (67) 20 (80)
≥15 1 (4) 5 (19) 1 (4) 16 (62) 9 (33) 14 (56)
≥20 0 1 (4) 1 (4) 11 (42) 3 (11) 10 (40)
After Dose 1
N=26 N=26 N=26 N=26 N=27 N=25
≥10 4 (15) 5 (19) 2 (8) 16 (62) 8 (30) 16 (64)
≥15 1 (4) 2 (8) 1 (4) 8 (31) 4 (15) 10 (40)
≥20 0 0 1 (4) 6 (23) 2 (7) 9 (36)
After Dose 2
N=26 N=25 N=25 N=17 N=26 N=19
≥10 5 (19) 6 (24) 3 (12) 12 (71) 15 (58) 12 (63)
≥15 0 5 (20) 1 (4) 9 (53) 6 (23) 10 (53)
≥20 0 1 (4) 1 (4) 5 (30) 1 (4) 5 (26)
FEV1categoriesarecumulative;i.e.asubjectwithamaximumdecreaseof 21% is included in all 3 categories. Patients with a ≥ 20% decrease in FEV1 did not receive a second dose of study drug.Figure 7: LS Mean Change from Baseline in FEV1 in Patients with Asthma
Patients with a ≥ 20% decrease in FEV1 did not receive a second dose of study drug and are not included in the curves beyond hour 10.Extrapyramidal Symptoms (EPS): Extrapyramidal reactions have occurred during the administration of oral loxapine. In most patients, these reactions involved parkinsonian symptoms such as tremor, rigidity, and masked facies. Akathisia (motor restlessness) has also occurred.In the 3 short-term (24-hour), placebo-controlled trials of ADASUVE in 259 patients with agitation associated with schizophrenia or bipolar disorder, extrapyramidalreactionsoccurred.Onepatient(0.4%)treatedwithADASUVEdeveloped neck dystonia and oculogyration. The incidence of akathisia was 0% and 0.4% in the placebo and ADASUVE groups, respectively. Dystonia (Antipsychotic Class Effect): Symptoms of dystonia, prolonged abnormal contractions of muscle groups, may occur in susceptible indi-viduals during treatment with ADASUVE. Dystonic symptoms include spasm of the neck muscles, sometimes progressing to tightness of the throat, difficulty swallowing or breathing, and/or protrusion of the tongue. Acute dystonia tends to be dose-related, but can occur at low doses, and occurs more frequently with first generation antipsychotic drugs such as ADASUVE. The risk is greater in males and younger age groups.Cardiovascular Reactions: Tachycardia, hypotension, hypertension, ortho-static hypotension, lightheadedness, and syncope have been reported with oral administration of loxapine.7 DRUG INTERACTIONS7.1 CNS DepressantsADASUVEisacentralnervoussystem(CNS)depressant.TheconcurrentuseofADASUVEwithotherCNSdepressants(e.g.,alcohol,opioidanal-gesics, benzodiazepines, tricyclic antidepressants, general anesthetics, phenothiazines,sedative/hypnotics,musclerelaxants,and/or illicitCNSdepressants) can increase the risk of respiratory depression, hypoten-sion, profound sedation, and syncope. Therefore, consider reducing the doseofCNSdepressantsifusedconcomitantlywithADASUVE.
7.2 Anticholinergic DrugsADASUVE has anticholinergic activity. The concomitant use of ADASUVE and other anticholinergic drugs can increase the risk of anticholinergic adverse reactions including exacerbation of glaucoma and urinary retention.8 USE IN SPECIFIC POPULATIONSIn general, no dose adjustment for ADASUVE is required on the basis of a patient’s age, gender, race, smoking status, hepatic function, or renal function.8.1 PregnancyPregnancyCategoryCRisk SummaryThere are no adequate and well-controlled studies of ADASUVE use in pregnant women. Neonates exposed to antipsychotic drugs during the third trimester of pregnancy are at risk for extrapyramidal and/or with-drawal symptoms following delivery. Loxapine, the active ingredient in ADASUVE, has demonstrated increased embryofetal toxicity and death in rat fetuses and offspring exposed to doses approximately 0.5-fold themaximum recommendedhumandose (MRHD) on amg/m2 basis. ADASUVE should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.HumanDataNeonates exposed to antipsychotic drugs during the third trimester of pregnancy are at risk for extrapyramidal and/or withdrawal symptoms following delivery. There have been reports of agitation, hypertonia, hypo-tonia, tremor, somnolence, respiratory distress, and feeding disorders intheseneonates.Thesecomplicationshavevariedinseverity;insomecases symptoms have been self-limited, but in other cases neonates have required intensive care unit support and prolonged hospitalization.Animal DataIn rats, embryofetal toxicity (increased fetal resorptions, reduced weights, and hydronephrosis with hydroureter) was observed following oral administration of loxapine during the period of organogenesis at a doseof1mg/kg/day.ThisdoseisequivalenttotheMRHDof10mg/dayon a mg/m2 basis. In addition, fetal toxicity (increased prenatal death, decreased postnatal survival, reduced fetal weights, delayed ossifica-tion, and/or distended renal pelvis with reduced or absent papillae) was observed following oral administration of loxapine from mid-pregnancy through weaning at doses of 0.6 mg/kg and higher. This dose is approxi-matelyhalftheMRHDof10mg/dayonamg/m2 basis. No teratogenicity was observed following oral administration of loxapine during the period of organogenesis in the rat, rabbit, or dog at doses up to 12, 60, and 10 mg/kg, respectively. These doses are approximately 12-, 120-,and32-foldtheMRHDof10mg/dayonamg/m2 basis, respectively.8.3 Nursing Mothers It is not known whether ADASUVE is present in human milk. Loxapine and its metabolites are present in the milk of lactating dogs. Because many drugs are excreted in human milk and because of the potential for serious adverse reactions in nursing infants from ADASUVE, a decision should be made whether to discontinue nursing or discontinue ADASUVE, taking into account the importance of the drug to the mother.8.4 Pediatric UseThe safety and effectiveness of ADASUVE in pediatric patients have not been established.8.5 Geriatric UseElderly patients with dementia-related psychosis treated with antipsychotic drugs are at an increased risk of death [see Boxed Warning and Warn-ings and Precautions (5.3)]. ADASUVE is not approved for the treatment of dementia-related psychosis. Placebo-controlled studies of ADASUVE in patients with agitation associated with schizophrenia or bipolar disorder did not include patients over 65 years of age.10 OVERDOSAGESigns and Symptoms of OverdosageAs would be expected from the pharmacologic actions of loxapine, the clinicalfindingsmayincludeCNSdepression,unconsciousness,profoundhypotension, respiratory depression, extrapyramidal symptoms, and seizure.Management of OverdosageFor the most up to date information on the management of ADASUVE overdosage, contact a certified poison control center (1-800-222-1222 or www.poison.org). Provide supportive care including close medical supervision and monitoring. Treatment should consist of general mea-suresemployedinthemanagementofoverdosagewithanydrug.Con-sider the possibility of multiple drug overdosage. Ensure an adequate airway, oxygenation, and ventilation. Monitor cardiac rhythm and vital signs. Use supportive and symptomatic measures.Manufacturedby:AlexzaPharmaceuticals,Inc.,MountainView,CA94043Manufacturedfor:TevaSelectBrands,Horsham,PA19044,DivisionofTeva Pharmaceuticals USA, Inc.Iss.12/2013ADA-40059
S:6.5”
S:9.5”
T:7”
T:10”
B:10”
B:12”

Official Magazine of the Emergency Nurses Association 21
Call for 2015 ENA National Committees
Bring your passion for nursing to the national level! ENA
2014 President-elect Matthew F. Powers, MS, BSN, RN,
MICP, CEN, would like to invite you as an ENA member
to share your knowledge and experience on a national
ENA committee in 2015. We will be accepting applications
for each of our national committees July 1 - 31, 2014.
For a full description of each committee and to
apply beginning July 1, go to www.ena.org, then click
on ‘‘Get Involved.’’
National Committee applications must be submitted
online by 5 p.m. Central time Thursday, July 31.
While not required, a photo is requested with your
application. Photos do not have to be professionally done;
a quick snap from your smartphone will work. Look for
instructions on how to upload your photo in the
committee application.
MEMBER FEEDBACK
ENA values its members’ opinions
and provides several
opportunities for members to provide
feedback to the organization,
including via social media and directly
to their ENA Board of Directors state
liaisons at local and national meetings.
Another increasingly effective method
of gathering member feedback is
through market research surveys.
‘‘It is very important to us to
engage our members,’’ said Laura
Jiggens, who joined ENA in February
as market research manager.
Originally from England, Jiggens
came to ENA with more than 16 years
of market research experience, most
recently in the pharmaceutical
industry. While her involvement with
research findings typically concludes
with the delivery of a final report,
Jiggens was keen to ‘‘take market
research that next step further and
actually implement results and see the results come to life.’’
A number of ENA market research initiatives planned for
this year will help Jiggens realize that goal as she creates and
sends surveys on various topics to ENA members throughout
this year and beyond. Membership satisfaction and national
conference preferences are two of the topics that ENA
surveys will address in 2014.
Feedback from member surveys helps ENA headquarters
better connect with members and
make informed decisions. Member
opinions influence and guide
decisions on educational offerings,
organizational issues, strategic
planning, national conferences
and member services.
The majority of surveys will
not be sent to all 40,000 ENA
members, Jiggens said. ENA
realizes its members lead busy
lives and aims to minimize the
impact of being selected too
frequently for surveys.
‘‘For each study, we will select
a specific or random sample of
members,’’ she said. That makes it
even more critical that as many
ENA members as possible respond
when asked to participate. One
ENA member could represent
thousands of colleagues.
ENA plans to share some key
insights from survey results with
members in the pages of
ENA Connection, as well as
keep members updated on what the organization is doing
with the findings.
‘‘ENA wants members to know that we are really
listening,’’ Jiggens said.
Note: ENA respects members’ privacy and will never divulge
a respondent’s identity, personal information or individual
answers unless specifically given permission to do so.
By Amy Carpenter Aquino, ENA Connection
Survey Says! Your Voice Carries
“ENA wants members to know that we are really listening.’’
LAURA JIGGENS, ENA Market Research Manager

22
GOVERNANCE
T he 2014 ENA General Assembly
will be held Oct. 7-8 in
Indianapolis. ENA President Deena
Brecher, MSN, RN, APN, ACNS-BC,
CEN, CPEN, will preside.
Approximately 700 delegates
representing ENA’s state councils and
international members will debate and
vote on issues that affect the
emergency nursing profession.
Attending the 2014 General
Assembly is a wonderful opportunity
for members to understand how
decisions are made concerning the
direction and stewardship of the
association. The General Assembly
agenda includes the installation of the
2015 ENA Board of Directors and
Nominations Committee, with reports
by the president, president-elect,
treasurer and executive director.
Delegates will also consider and act on
proposed resolutions and bylaws
amendments.
At its May meeting, the ENA Board
of Directors reviewed this year’s
proposals. Final proposals, including
any additional bylaws amendments
submitted by the July 10, 2014,
deadline, will be posted in August in
the online General Assembly
Handbook at www.ena.org for
viewing by all state councils, chapters
and assigned delegates.
Summaries of the proposed
resolutions and bylaws
amendments follow:
ENA ResolutionsUpdate the “Consensus
Statement on
Definitions for
Consistent Emergency
Department Metrics”:
This resolution recommends
that ENA work with stakeholder
organizations to revise and update the
‘‘Consensus Statement on Definitions
for Consistent Emergency Department
Metrics’’ to minimally include
definitions for the terms ‘‘disposition
decision time,’’ ‘‘admit decision time’’
and ‘‘boarded admitted patient.’’
ENA’s Role in Firearms Safety:
This resolution recommends that ENA
advocate for the creation of a national
background check before all firearm
purchases, a five-day waiting period
before purchase and support for
evidence-based education on firearm
safety. The General Assembly has
previously adopted resolutions
regarding firearms: GA01-02 and
GA10-13.
Emergency Nurses Advocate for
Reduction in Prescription Drug
Abuse: This resolution recommends
that ENA develop resources in the
areas of pain management, medication
storage and medication disposal;
encourage ongoing research on
evidence-based pain management
strategies; and collaborate with
organizations to reduce the incidence
of prescription drug recreational use
and overdose events.
Patient Education for Mild
Traumatic Brain Injury/
Concussion: This resolution
recommends that ENA
update the position
statement on Unintentional
Sport and Recreational
Injuries to recommend that emergency
departments provide 1) patient
education on post-concussive syndrome
and 2) cognitive rest and return-to-play
guidelines, and that ENA explore or
develop an educational resource on
mild traumatic brain injuries.
Use of Orientation Guidelines:
This resolution recommends that ENA
identify best practices for orientation
timelines, delivering content and
tracking the progress of new graduate
or new-to-the-specialty nurses.
Support of Creating a National
Trauma System: This resolution
recommends that ENA support
development of a national trauma
system across the continuum of
integrated care, including injury
prevention, and express support of this
endeavor through a position statement.
Meaningful Use and Nurse
Protocols: This resolution
recommends that ENA’s protocol
position statement be revised to
include identifying emergency
registered nurses as licensed health
care providers and verbiage regarding
the entry of protocols into the
electronic health record.
ENA Board of Directors Support:
This resolution recommends that the
2014 ENA General Assembly
acknowledge the ENA Board of
Directors’ diligence in performing its
leadership role, appreciate its efforts to
continue ENA’s growth and
We Have Much to Discuss in Indianapolis2014 Proposed Resolutions and Bylaws Amendments

Official Magazine of the Emergency Nurses Association 23
AGGRESSIVE BEHAVIOR......towards staff at work is dramatically on the increase, especially in our Hospitals. Verbal abuse, threats with weapons, cuts, punches, even serious injuries are becoming everyday occurrences. The impact on the confidence and morale of staff is damaging and costly and has a serious impact on the caring and commitment that lies at the heart of the staff/patient relationship. Installing an INSTANTalarm 5000
Staff Personal Alarm System will make a dramatic differenceINSTANTalarm does NOT• track you around the hospital• use radio-frequency• rely on unreliable wi-fi• have a computer controlling itINSTANTalarm, however, DOES• let you decide when you need help• pinpoint your location, to a room• work instantaneously• make you and your patients feel safer• reduce the frequency and impact of violent incidents
Which is why, over 20 years, INSTANTalarm 5000 has been probably the most widely-installed, staff duress alarm system in the world.
® 205.414.7541www.pinpointinc.com PROTECTING
PEOPLE AT WORK
®
development as a leader among
specialty associations and value its
efforts in ensuring a clear vision of
ENA’s future.
Standardization of Emergency
Codes Nationwide: This resolution
recommends that ENA advocate for
and take a leadership role in the
development and nationwide
implementation of standardized plain
language hospital emergency code
terminology.
Bylaws AmendmentsArticle VIII – Resolutions
Committee Name: The authors offer
this amendment to change the
committee name to properly reflect its
responsibilities.
Article VIII – Resolutions
Committee Composition: The authors
recommend this amendment to add an
additional member to the committee for
effective leadership succession planning
and increased productivity.
Article V – State Captains: The
authors propose this language for
consistent language throughout ENA
documents, with ‘‘state captains’’ in
place of ‘‘lead delegate.’’
Articles VIII and XII – Bylaws and
Election Rules Submission
Deadline: The intent of this
amendment is to standardize and
streamline the deadlines for submitting
materials for the General Assembly
meeting. The bylaws, resolutions,
election rules and General Assembly
Standing Rules of Procedure currently
have different timeframes. Standardized
submission dates will be clearer for the
members.
Article III – Dues Waiver
Eligibility for Senior Members: The
authors offer this proposal to retain
member benefits for senior members
without cost to the member.
Articles IV, VI and VIII —
Eligibility Requirements:
Background Checks: The authors
want to streamline the election process
by eliminating the employment
verification and highest academic
achievement verification from the
background check process.
Article VIII – Nominations
Committee Chairperson Election:
Adopting this proposal will allow the
committee to select its chairperson
without being attached to a specific
event.
Articles VIII – Nominations
Committee Name: The authors offer
this amendment to change the
committee name to properly reflect its
responsibilities.
Article III – Suspension and
Termination of Membership: The
authors offer this amendment to more
clearly define the grounds and
procedures for disciplinary action
against a member.

24
COURSES
In an effort to provide its emergency
nurses with proper training and
knowledge on caring for the elderly
population, Baylor Scott & White
Health-North Texas ordered 100
licenses of ENA’s Geriatric Emergency
Nursing Education online course in
March, making it ENA’s largest
GENE order to date.
ENA member Kristine
Powell, MSN, RN, CEN,
NEA-BC, director of emergency
services at Baylor Scott &
White-North Texas, said
improving care for the elderly
has been a strong focus at
Baylor for several years.
‘‘From the ED perspective, we are
looking at issues such as how to
prevent readmissions because a large
number of our elderly patients are at
high risk of avoidable readmissions,’’
she said. ‘‘We want to improve care
and reach out to them out in the
community to prevent exacerbations of
their chronic disease so that they don’t
end up back in the hospital. We are
really looking at patient-centered care
and want the quality of life for our
patients as optimal as possible. Part of
that has to do with education in the
emergency department. It’s one piece
of the larger puzzle.’’
According to the Deerbrook
Charitable Trust, more than 40 percent
of hospital patients are over 65, but
fewer than 2 percent of nurses have
certifications in geriatrics. Recognizing
the need to improve education for this
population, in 2011 the Deerbrook
Charitable Trust awarded Baylor
Health Care System a three-year grant
totaling $12.4 million. Powell said the
grant allowed the purchase of the 100
GENE licenses for emergency nurses,
reflecting about 20 percent of Baylor’s
emergency nurse population.
‘‘Baylor has been very innovative
and proactive in helping to manage
health care for this population,’’ she
said. ‘‘We received the grant
specifically to do work around
elderly care at Baylor, not just
in the hospital but also out in
the community. We’re trying to
build subject-matter experts in
our emergency department and
get them engaged with being a
clinical resource for frontline
staff. We have a definite need
within the ED for this knowledge, and
a focus on ED nursing education is
essential.’’
One of Powell’s priorities is to have
her nurse educators incorporate four of
the GENE licenses into their ED
internship program so new nurses can
receive the course content immediately.
‘‘As we continue to do this work,
we want to embed this clinical
information about the care of elderly
patients in the ED as standard practice
and standard knowledge,’’ she said.
‘‘We’re really taking it down two paths
— one is for nurses who are new to
the ED, and the other is a refresher for
our current nurses.’’
The average age of an
emergency nurse at Baylor
University Medical Center is 32,
Powell noted, adding that the ED
has a high number of Generation Y
nurses who haven’t received
education in geriatric care.
Powell is looking forward to
raising awareness of elderly
patients’ special needs and having
emergency nurses on the front lines as
subject-matter experts and clinical
resources for other nurses. But she is
also looking to do more.
‘‘I’m also looking to step it up a
notch to give a hundred of our nurses
that foundational education,’’ she said.
‘‘I want to be able to pull them
together to look at how we care for
elderly patients in our ED and really
start building better workflows.’’
Powell attended the previous GENE
pilot program, delivered in a classroom
setting at the 2004 ENA Annual
Conference in San Diego. She is
confident the new online course will
be beneficial to emergency nurses.
‘‘I’m an ER nurse, and I am a lifetime
member of ENA,’’ she said. ‘‘I have
been active in ENA for 25 years. This is
an evidenced-based program developed
by my professional organization. I am
also a TNCC and ENPC instructor and
course director, so I know the caliber of
the programs that ENA puts out, and I
trust ENA’s products.’’
For more information on the new
GENE online course or to find out how
you can purchase it for your
emergency department, e-mail
[email protected], call 847-460-4055 or
visit www.ena.org/education/
education/GENE.
BETTER CARE x100By Kendra Y. Mims, ENA Connection
Texas Health System Buys GENE Course in Bulk for ED Nurses
Kristine Powell

Official Magazine of the Emergency Nurses Association 25
17 Interactive Modules15.21 Contact Hours
Geriatric Evidence-based Research
Comprehensive Geriatric Online Course
GENE provides: § Best geriatric practices from triage
to discharge § Patient and family education § Learning material for all healthcare
professionals who work with older adults
Purchase Today! Group Pricing Available
www.ena.org/geneThe Emergency Nurses Association is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation.
GENE Ad_Connection_half vertical_0607 2014.indd 1 5/6/14 1:42 PM
W hen the time for your annual
performance evaluation rolls
around, do you dread it and consider
calling in sick to avoid it, or do you
welcome it? Many individuals take a
let’s-just-get-it-over-with approach. But I
challenge you to welcome your annual performance
evaluation, to take it as an opportunity to own your career
and take charge of your professional development.
Here are a few tips as you enter into your own annual
evaluation period:
• Spend time on self-assessment; honestly reflect on
your accomplishments and your challenges during the year.
• Be prepared to have a detailed discussion with your
supervisor about your goals, your questions and your
opportunities.
• Remember that feedback is a gift; be accepting of the
gift being given to you and figure out how to make the
most of it for your personal and professional development.
• Make a plan for the upcoming year and obtain support
and guidance from your supervisor and other mentors.
• Stay focused on your plan; schedule checkpoints,
look for opportunities to accomplish stretch goals and add
to your professional experiences.
As your professional organization, ENA is committed to
helping you accomplish your professional goals. For more
resources and information, visit the career wellness page at
www.ena.org/membership/Career Center or e-mail
FUTURE OF YOUR NURSING Bridget Walsh, PHR, Chief Talent Officer
Performance Evaluation: Love It or Hate It
Call for Memorial Requests at 2014 ENA General Assembly
Deadline: Wednesday, Aug. 20, 5 p.m. Central time
ENA will honor our members who have died in the last
year during a special memoriam presentation during the
2014 General Assembly in Indianapolis. If you would like
to recognize a member who has died, please complete
the request form found in the General Assembly area
(members only) at www.ena.org. All requests must be
submitted electronically to [email protected].

June/July 201426
ONLINE LEARNING
Stroke is a leading cause of death
and disability in the United States.
ENA and Genentech have joined forces
to provide online training, with critical
educational resources to help
emergency nurses better identify,
diagnose and treat stroke.
ENA launched the free online
training modules on its learning
management system at www.ena.org
in April. The stroke management
learning system will be available for
one year until April 2015.
The program is divided into three
modules designed to introduce
emergency nurses to some key
concepts surrounding stroke with an
emphasis on acute ischemic stroke.
Module 1 covers basic stroke
education. Topics include stroke
epidemiology, ischemic
pathophysiology and brain anatomy.
Participants will learn how to identify
risk factors for stroke as well as
potentially modifiable risk factors such
as hypertension, diabetes, obesity,
high cholesterol and smoking, and
non-modifiable risk factors such as
previous stroke, family history, age
and hypercoaguable states. The
modules also cover the two different
types of stroke.
Module 2 focuses on in-hospital
diagnosis of acute ischemic stroke.
Learners will discover effective ways to
rapidly recognize stroke symptoms,
apply time-saving recommendations
and determine treatment options.
Vibrant graphics illustrate the
differences between what happens to
the body during a large vessel
ischemic stroke and during a transient
ischemic attack. Participants also will
learn how delays in medical
management of acute ischemic stroke
patients can affect their outcome.
Module 3 teaches stroke treatment
and management of acute ischemic
stroke, with an emphasis on the
management of confirmed acute
ischemic stroke. It includes review of
patient eligibility for treatment,
potential risks and benefits of therapy,
dosing and administration, and
post-treatment monitoring and care.
The modules provide a variety of
teaching techniques, including videos
and an option to click on new or
unfamiliar terms for pop-up
definitions.
“This program will provide an
overview of stroke basics; review the
assessment of a patient with suspected
stroke; and comprehensive treatment
guidelines with fibrinolytic therapy for
a patient with an ischemic stroke,’’ said
Alyssa Kelly, MSN, RN, CNS, CEN,
senior associate, ENA Institute for
Emergency Nursing Education. ‘‘It will
assist the learner in meeting the NINDS
in-hospital time goals for patients with
suspected stroke, thus improving
patient outcomes.’’
ENA Partners With Genentech to Launch Stroke Management Learning System
How to Take the CourseMembers can access the online education modules at www.ena.org/education/onlinelearning/Pages/Stroke.aspx or learn.healthstream.com/accesspoint/genentech.
Note: No continuing education credits are offered for this course. Participants will receive a certificate of completion.
By Amy Carpenter Aquino, ENA Connection
Official Magazine of the Emergency Nurses Association 27
T he influence of
evidence-based practice
resonates throughout
nursing, impacting education, practice and research.
The demand for evidence-based quality
improvement and performance requires nurses to
have the best tools and resources for success.
Applying research evidence and integrating the
knowledge into clinical practice is now the expected
standard of performance for a majority of health care
organizations. Understanding the various levels of
evidence assists nurses in evaluating and
determining its relevance and how it can be
incorporated into best practices. EBP is a systematic
and scientific approach that is constantly changing
but is compulsory for safe practice, safe care and
clinical decision-making.
As stated by Baker, et al.,1 emergency nurses are
in an exclusive position to not only improve care
but also improve nursing practice by implementing
and using several forms of scientific inquiry.
However, finding the right tools and resources can
be daunting; the overwhelming amount of
information available can make it difficult to know
what is authoritative, current and scholarly.
Fortunately, ENA has developed user-friendly clinical
resources and publications that provide electronic
and print materials to support nursing education,
practice and research. A variety of essential
information can be obtained from ENA’s practice
website: www.ena.org/practice-research/
Practice/Pages/PracticeResources.aspx.
Among these practice resources are clinical
practice guidelines, position statements, emergency
nursing scope and standards of practice, ENA’s
translation into practice, toolkits, topic briefs and
white papers. These tools and resources provide
current, scholarly and evidence-based information
which supports emergency nursing practice.
Practice resources have substantial supportive
information that can be used to not only guide
practice but also to improve health care delivery.2
The information obtained from the practice
Clinical Practice Guidelines• Evidence-based; assist in translating research into practice• Recommendations based on systematic review and critical analysis of current and scholarly literature• Formerly known as Emergency Nursing Resources
Position Statements• Statements of beliefs that reflect ENA’s stance on issues relating to safe practice, safe care and patient outcomes• ENA position statements, including joint statements and supported statements• Archived position statements
Emergency Nursing Scope and Standards of Practice• Benchmark guide for professional emergency nursing• Resource for practice, standards and competencies expected• Establish nursing professional performance standards
ENA’s Transitions into Practice • Quick reference with level of evidence recommendations• Assist in facilitating and applying current evidence into practice• Examine current topics in everyday emergency nursing practice and make recommendations for transition into practice
Toolkits• Collective resources that include education, forms, links and valuable material useful in implementing change and improving practice• Contain documents that will assist an individual to champion a project or implement a program
Topic Briefs• Supportive documents that provide detailed information on a given subject of importance, particularly to safe practice and safe care• Examine relevant issues: adult immunizations, the bariatric/obese patient, health literacy, health information technology and the health work environment
White Papers• Distinctive and authoritative reports focused on specific topics• Presentation of research with a specific purpose, audience and organization• Current white papers address care of the psychiatric patient in the ED and nurse fatigue
ENA PRACTICE RESOURCES
A Toolbox of Tips For SuccessBy Monica Escalante, MSN, RN, Senior Associate, Institute for Quality, Safety and Injury Prevention
Continued on page 31

June/July 201428
“Appreciation is a
wonderful thing. It makes
what is excellent in others
belong to us as well.”
Could Voltaire’s words be applied to the ENA
Foundation and its ongoing journey toward
building a strong foundation?
Since January, I have spoken with and written to many
ENA members to share my appreciation for their
contribution to our mission of enhancing emergency care
through education and research. We know and celebrate our
differences — various values, motivations and passion.
However, we are all linked inextricably by a common thread
of emergency nursing. The fact that you are drawn to
emergency nursing makes you committed to excellence, and
excellence is never an accident — it is a standard to which
we hold ourselves and others. We should all be involved in
building a strong foundation so that we can ensure the
integrity of not just the ideals of excellence for ourselves, but
also for our colleagues who work in the triage room, the
nurse who covers our break, the educator who teaches us,
the charge nurse who runs interference and the manager
who helps lead us inside and outside the ED. Virtually every
aspect of emergency care is entwined in the excellence of
those around us. If they perform well, we all perform well.
When we appreciate and help those around us, we all
succeed.
Let me share how scholarship recipients — and your
colleagues — praised your ENA Foundation at a recent
Maine ENA State Council meeting.
‘‘I am very proud to be a part of an organization that
supports and promotes its members through continuing
higher education,’’ said ED educator Lauren Vickerson, BSN,
RN, CEN.
‘‘I owe success to those who support the ENA Foundation
and who support emergency nurses throughout the country
. . . I am proud to be a part of such a professional and
well-respected group of peers,’’ said Jennifer Granata, MSN,
RN, CEN, an ED manager.
In Colorado, emergency physician Lee Shockley, MD,
described why he donates to the ENA Foundation: ‘‘Effective
emergency care requires teamwork and highly skilled
professionals. . . . As an emergency physician, I believe that
support for emergency nurses is one of my duties. The ENA
Foundation’s scholarships for emergency nursing education
are a way that I can help provide that support.’’
I would like to let you in on a badly kept secret: It’s not
only your peers who want to see you succeed. We receive
gifts from members of the public (yes, your patients) who
donate simply because they wish to pay it
forward and they see the benefit of having a
highly educated emergency team. On the ENA
Foundation Board of Trustees, highly engaged
corporate trustees participate to ensure that you
can continue to learn and that you get an opportunity to
grow.
Ken Craig, MBA, corporate trustee-at-large from Physio-
Control Inc., shared an experience with me: ‘‘I recently sat
next to someone at dinner that had benefited from an ENA
Foundation academic scholarship that helped her complete
her master’s degree and advance her hospital career. It was
heartwarming to hear how grateful she was to the ENA
Foundation and to those companies that provide funding for
those scholarships. The ENA Foundation really does make a
difference!’’
John Proctor, MD, MBA, FACEP, FAAP, American College
of Emergency Physicians Emergency Medicine Foundation
representative, said, ‘‘I know the foundation to be committed
to the welfare and success not only of the nursing providers
of emergency care, but to the patients we serve.’’
I hope you can see what is happening here: It’s Voltaire’s
excellence in motion. It is us appreciating our job, our
practice and each other by helping us become better at what
we do. This is a movement that you are either part of or not.
If you believe in it, donate today. You can become the
ultimate colleague by making a conscious decision to help
your team by making a donation. It’s you who is defining
our practice, it’s you who is creating the increase in
knowledge, it’s you who should also be donating to help
those who help you every day. I believe that you want
to continue to work with the best, so let’s give
the best a chance by supporting the ENA
Foundation so it can keep providing
scholarships and research grants.
This is building a strong foundation,
this is emergency nursing, this is excellence
in motion, this is your ENA Foundation and
this is why you should get involved and
make a donation. For the sake of excellence
and your colleagues, please make a donation
at www.enafoundation.org or call the ENA
Foundation at 847-460-4100.
Be the Ultimate ColleagueENA FOUNDATION | Seleem Choudhury, MBA, MSN, RN, CEN, 2014 ENA Foundation Chairperson

Bring instant relief to your patient’s faceIN 4 TO 10 SECONDS FLAT.
»
The INSTANT topical anesthetic.
{ {That’s how fast it works!
Pain doesn’t wait. Ease it in an instant. Prepare your patient for a needle procedure or minor surgery with Gebauer’s Pain Ease® topical anesthetic skin refrigerant.
» temporarily controls pain and anxiety in as few as 4 to 10 seconds
» use on intact skin, minor open wounds and intact oral mucous membranes
» may be used by any licensed healthcare practitioner without the order of a physician
Published clinical trial results support the use in children three years of age and older. Do not use on large areas of damaged skin, puncture wounds, animal bites or serious wounds. Do not spray in eyes. Over spraying may cause frostbite. Freezing may alter skin pigmentation. Use caution when using product on diabetics or persons with poor circulation. Apply only to intact oral mucous membranes. Do not use on genital mucous membranes. The thawing process may be painful and freezing may lower resistance to infection and delay healing. If skin irritation develops, discontinue use. CAUTION: Federal law restricts this device to sale by or on the order of a licensed healthcare practitioner.
IMPORTANT RISK AND SAFETY INFORMATION:
www.Gebauer.com/PainEase | T R Y PA I N E A S E T O D AY !
© 2014 Gebauer Company. All rights reserved. 841.1
ADVERTISEMENT
1.800.321.9348

June/July 201430
EMERGENCY NURSING RESEARCH
Every day, in every emergency
department throughout the United
States, emergency nurses are faced with
questions about how to provide the
safest, best-quality care to patients.
Nurses already adjust their practices
based on the latest evidence and
practice experience to deliver better
care to emergency patients. However,
what happens when nurses seek
answers to questions and find there is
no current evidence to answer these
questions?
Working with emergency nurses to
unearth evidence answering these
questions is the goal of the Institute for
Emergency Nursing Research. The IENR
seeks knowledge through research
studies that answer questions about
improving the safety and quality of
patient care.
The mission of the IENR is to
conduct and facilitate research and evidence-based practice
in emergency nursing, with a vision to be a source of
research and information for evidence-based emergency
nursing practice and care. Our mission and vision are active
in our many activities, such as authoring a series of research
articles in the Journal of Emergency Nursing and research
projects, such as seeking answers to help emergency nurses
deal with violence in the emergency department, identifying
educational needs in rural hospitals and recognizing issues
with behavioral health patients.
The IENR also organizes and staffs the Research Lounge
at the ENA national conference. The Research Lounge is
staffed with doctorally prepared emergency nurses who help
stretcherside nurses develop research projects. Research
Lounge attendees receive support creating research
questions, developing strategies to sample a target
population, developing a specific research methodology and
other assistance.
On April 22-23, the IENR advisory council met at ENA
headquarters in Des Plaines, Ill., to discuss burning questions
in emergency nursing. Studies carried out under the leadership
of director Lisa Wolf, PhD, RN, CEN, FAEN, include:
• Understanding current ED discharge processes for
patients receiving Schedule II and III pain medications (study
in data analysis phase).
• Investigating the relationship between emergency
nurses’ reported sleep and their perceived fatigue and
cognitive ability (study in preliminary development phase).
• Seeking out the nature of moral distress/despair
experienced by emergency nurses (study in preliminary
development phase).
IENR members were also updated on the March 2014
National Nursing Research Roundtable at the National
Institutes of Health, sponsored each year by the National
The 2014 IENR Advisory Council: Front row, from left: Gail Lenehan, EdD, MSN, RN, FAEN, FAAN; Board of Directors liaison Michael Moon, PhD, MSN, RN, CEN, CNS-CC, FAEN; IENR senior administrative assistant Leslie Gates; middle row: IENR senior associate Cydne Perhats, MPH, IENR; Kathleen E. Zavotsky, MS, RN, CEN, ACNS-BC, CCRN; Kathy M. Baker, PhD, RN, NE-BC; back row: Margaret J. Carman, DNP, MSN, RN, CEN, ACNP-BC; IENR senior associate Altair Delao, MPH; Paul R. Clark, PhD, MA, RN; IENR director Lisa Wolf, PhD, RN, CEN, FAEN; Kevin Langkiet, MSN, RN.
Better Care Through the IENRBy Paul R. Clark, PhD, MA, RN

Official Magazine of the Emergency Nurses Association 31
resources can be used as references for research,
educational purposes and to assist in implementing
change. For example, reviewing CPGs may influence
further investigation into an organization’s procedure
for using capnography during procedural sedation/
analgesia. Reviewing CPGs for prevention of blood
culture contamination might impact hospital policies
and protocols.
TIPs can act as a quick reference to simplify
applying current evidence in emergency nursing.
ENA’s available toolkits are valuable materials that can
assist individual champions to implement a program or
function as support for projects. Position statements,
the Emergency Nursing Scope and Standards of
Practice, topic briefs and white papers are also
essential practice resources with detailed evidence that
may serve as a reference or inspire change.
Diane Gurney, MS, RN, CEN, 2010 ENA president,
shared how ENA’s practice resources have helped her
provide safe care to her patients.
‘‘The ENA website is my ‘go-to’ place for emergency
nursing practice information,’’ Gurney said. ‘‘For years
I have relied on ENA for current, evidence-based
knowledge to support my emergency nursing practice.
The clinical practice guidelines have been invaluable
in assisting me with current scientific knowledge
regarding such practice issues as orthostatic vital signs,
non-invasive blood measurement and gastric tube
placement verification. As a manager, I used the ENA
position statements to help justify the need for trauma
nursing education, standards for triage nursing and the
importance of a hospital-wide multidisciplinary
approach to implementing strategies for holding and
crowding. It is all in one place, easy to use,
comprehensive and evidence-based.’’
References
1. Baker, K.M., Clark, P.R., Henderson, D., Wolf, L.A.,
Carman, M.J., Manton, A., & Zavotsky, K.E. (2014).
Identifying the differences between quality
improvement, evidence-based practice, and original
research. The Journal of Emergency Nursing, 40(2),
195-197. doi: 10.1016/j.jen.2013.12.016
2. Peterson, M.H., Barnason, S., Donnelly, B., Hill, K.,
Miley, H., Riggs, L., & Whitemand, K. (2014). Choosing
the best evidence to guide clinical practice: Application
of AACN levels of evidence. Critical Care Nurse, 34(2),
58-68. doi:10.4037/ccn2014411
ENA Practice Resources Continued from Page 27
Institute of Nursing Research. We also discussed ways to
improve ENA members’ access to research tools through the
research section of the ENA website and how to develop the
Research Lounge at the 2014 ENA Annual Conference in
Indianapolis.
The IENR encourages emergency nurses to seek answers to
questions that are not answered by current evidence. If you
have questions about initiating a research project in your
emergency department, contact Lisa Wolf at [email protected]
and visit the IENR website: www.ena.org/practice-
research/research.
2014 ED Operations CommitteeThe Emergency Department Operations Committee
convened at ENA headquarters for an onsite meeting
March 27-28. Members focused on committee charges by
reviewing and recommending topics for the Key Concepts
in ED Management program and developing content for
an ED manager survival guide.
The ED Operations Committee charges for 2014 are as
follows:
1. Provide subject-matter expertise related to
emergency department operations.
2. Identify and recommend resources for emergency
department operations/management.
Committee Members
Fred Neis, MS, RN, CEN, FACHE, FAEN, chairperson
Frances Damian, MS, RN, NEA-BC
Mark Mayes, MHA, BSN, RN, CEN
Kristine Powell, MS, RN, CEN, NEA-BC
Maryfran Hughes, MSN, RN (not pictured)
Board Liaison
Kathleen Carlson, MSN, RN, CEN, FAEN

June/July 201432
CERTIFICATION
ENA collaborated with the American Nurses Credentialing
Center in 2012 on a new methodology for assessment of
emergency nurse practitioners with the development of
certification by portfolio. A portfolio contains evidence of
professional practice. The ANCC portfolio program contains
requirements in four domains of practice: professional
development, professional and ethical nursing practice,
teamwork and collaboration, and quality and safety. No
examination is required. All portfolios submitted in this
certification program are subject to peer review. If the APRN
application is approved and passes the peer review program,
the certification of ENP-BC is awarded.
Nurses credentialed through the ANCC program are
established as experts in their specialty. Advanced practice
nurses practicing within an institution are required to comply
with the credentialing and privileging process in their facility,
which includes the common elements documented in this
ANCC portfolio certification. This certification is renewable
every five years.
As the momentum proceeds toward full implementation of
the Consensus Model for APRN Regulation, dialogue is
occurring in many states on aligning the necessary elements of
the model. Discussion on professional portfolios occurred this
year in Nevada, where a regulation passed in February
indicates all Nevada APRNs must maintain a professional
portfolio subject to audit by the board. Nevada further explains
that it may deny the renewal of a license to practice if it finds
an APRN has failed to maintain the portfolio required.
In a ‘‘President’s Blog’’ posted last fall, JoAnn Lazarus,
MSN, RN, CEN, the ENA 2013 president,
announced the launch of the ANCC
ENP-BC credential.
‘‘For advanced practice RNs,
credentialing by portfolio is an opportunity
to be recognized for meeting the criteria
established by emergency nurse
practitioner peers as having the
skill and knowledge
to practice,’’
Lazarus wrote.
Click. Shop. Done.•Leadershipbooks,studyguidesandreferencebooks
•ENAmerchandise–apparel,pinsandmore
•Memberdiscounts
Orderonline24/7atwww.ena.org/shop
ENA Marketplace Ad_Connection_half_05 2014.indd 1 3/26/14 10:10 AM
Emergency Nurse Practitioner Portfolio Credential Available

Official Magazine of the Emergency Nurses Association 33
Chamberlain College of Nursing | National Management Offi ces3005 Highland Parkway | Downers Grove, IL 60515 | 888.556.8CCN (8226) | chamberlain.edu
Comprehensive program-specifi c consumer information: chamberlain.edu/studentconsumerinfo. Program/program option availability varies by state/location. The Bachelor of Science in Nursing degree program and the Master of Science in Nursing degree program are accredited by the Commission on Collegiate Nursing Education (CCNE, One Dupont Circle, NW, Suite 530, Washington, DC 20036, 202.887.6791). Chamberlain College of Nursing, 2450 Crystal Drive, Arlington, VA 22202 is certifi ed to operate by the State Council of Higher Education for Virginia, 101 N. 14th Street, 10th Floor, James Monroe Building, Richmond, VA 23219, 804.225.2600. Chamberlain College of Nursing has provisional approval from the Virginia Board of Nursing, Perimeter Center, 9960 Mayland Drive, Suite 300, Henrico, VA 23233-1463, 804.367.4515. ©2013 Chamberlain College of Nursing, LLC. All rights reserved.
Take advantage of your ENA membership benefi ts at Chamberlain College of Nursing.
• 15% savings of current tuition rate• Online coursework• No mandatory login times
Find your extraordinary at chamberlain.edu/enaorg
RN to BSN | MSN | DNP
ExtraordinaryAn
Advantage
8-21-201312:00 PM
Element
LiveTrimBleed
PagesFolded SizeVDP
Notes
1/4 pg Print
3.25” x 4.75”
1 pgJob info
DateTime Round
100% JR1
Printed At Agency
3005 Highland Parkway | Downers Grove, IL 60515 | P: 630.512.8914 | F: 630.512.8888
12006 ENA Connection Ad (CCN #20421)
ApprovalsAPPROVED INITIALSDENIEDAPPROVED
W/ CHANGESDATE
Stephanie Gallo
Pub Info
Pub: Issue: Contact:
ENA ConnectionSeptember 2013Maureen [email protected]
Title:Location:Prod Co:Post Date:Quantity:
PR
INT
OO
H
FINAL CHECKLISTINITIALS INITIALS
Accreditation
Legal Line
SCHEV
INDI Code
NRW URL
Chamberlain URL
Inventory Code
3-Year BSN Copy
Chamberlain Address
Production Code
Heat Map Check
Other:
Chamberlain Phone888.556.8CCN (8226)
12006-Chamberlain_12006_EN
A_Connection_AdSize: 3.25" x 4.75"
T he appearance of
the Middle East
Respiratory Syndrome in
the United States has
prompted emergency
clinicians to take a critical
look at patients who have
a recent history of travel
to the countries in the
Saudi Arabian peninsula
and are presenting to
emergency departments
with respiratory illness.
MERS-CoV is caused
by a coronavirus. To
date, the Centers for
Disease Control and
Prevention have limited
information on the
pathogenic potential and
the transmission
dynamics of MERS-CoV
but note that the
incubation period is often
five days, with an outer
limit of 14 days.
CDC recommends
collecting multiple
specimens from different
sites after symptom onset.
The CDC guidelines for
collecting, handling and
testing clinical specimens
from suspected cases can
be found at www.ded.
gov. Many state health
departments are approved
for MERS-CoV testing.
Clinicians Advised to Watch for MERS
T he Consensus Model for APRN Regulation was crafted
five years ago to address issues related to practice for
advance practice registered nurses. The model provided a
framework for creating a uniform structure of APRN
regulation for use across the United States. It also aimed to
align the relationships among licensure, accreditation,
certification and education. This alignment would allow
APRNs to practice to the full extent of their education and to
move easily from state to state in order to increase access to
much-needed care for many patients. The model was
endorsed by ENA as well as 47 other nursing organizations.
The four APRN roles defined in the Consensus Model are:
• Certified Registered Nurse Anesthetist
• Certified Nurse Midwife
• Certified Clinical Nurse Specialist
• Certified Nurse Practitioner
Since the publication of the Consensus Model,
organizations representing licensure, accreditation,
certification and education have strived to make the changes
required to align with the Consensus Model, with an
intended full implementation target of January 2015. The
January publication of the Journal of Nursing Regulation
noted there are 229,955 individuals in the U.S. who currently
hold advanced practice nursing licenses, Maureen Cahill,
MSN, RN, APN-CNS, associate director of nursing regulation
at the National Council of State Boards of Nursing, said at a
LACE meeting in Chicago in April.
The APRN Campaign for Consensus initiative is focused on
assisting states in aligning their APRN regulation with the major
elements of the Consensus Model. Those major elements are:
• State recognition of each of the four described roles
• Licensure and title of APRN in the roles
• Graduate or post-graduate education from an
accredited program
• Certification at an advanced level from an accredited
program that is maintained
• Independent practice
• Independent prescribing
Cahill acknowledges the journey is 69 percent complete.
The status of individual states related to full implementation of
the consensus model can be found on the National Council of
State Boards of Nursing website at www.ncsb.org/aprn.
htm. The National Council 2012 document, A Health Care
Consumer’s Guide to Advanced Practice Registered Nurses, can
be downloaded for free from the website.
The Consensus Model for APRN Regulation: Status 2014

June/July 201434
MILITARY NURSING
Lt. Col. Kathleen Richardson still
remembers seeing her first
explosive injury during her first
deployment in Iraq. Although she had
seen amputations and partially injured
limbs before, this particular injury
pattern was unlike anything she had
ever witnessed during her 18-year
Army nursing career.
‘‘It was very graphic to me,’’ she
said. ‘‘I remember looking at that leg
and thinking that the bone reminded
me of slivers of wood.’’
Richardson, DNP, RN, ARNP, CNS,
NP-C, CEN, deployed to Iraq in 2007
for 15 months with a forward surgical
team. As the emergency medical
treatment officer in charge, she was
responsible for the entire management
and oversight of the 102nd Forward
Surgical Team emergency treatment
section. During the first part of the
deployment, her team was co-located
with the 86th Combat Support Hospital
during the troop surge, where they
worked alongside the hospital’s
physicians and nurses to treat various
traumas and illnesses, including a high
number of patients with appendicitis
and tuberculosis.
Richardson and her team found
themselves treating soldiers, coalition
forces and insurgents in the emergency
area at the same time.
‘‘We cared for everybody who came
into the hospital, and that was an
interesting thing to deal with,’’ she
said. ‘‘Some of the patients who came
in were afraid that we were going to
hurt them instead of treat them. You
could tell they were apprehensive and
hypervigilant until they realized that
we weren’t going to hurt them, and
then you could visibly see them relax.
It was an ongoing process to gain their
trust. They got the same standard of
care that we gave to everyone else.’’
Richardson discussed the danger of
having the interpreters there to help
them communicate. Sometimes the
interpreters had to hide from the
insurgents to protect their identities.
‘‘If one of the insurgents came in,
we made efforts to ensure that the
interpreters’ faces were not seen so
that they wouldn’t be identified,
because if the interpreters were
identified, their families could be at
risk,’’ Richardson said. ‘‘As we were
there longer, we started learning the
language so that we could
communicate without the interpreters.’’
Richardson described her
experience in Iraq as both rewarding
and challenging.
‘‘It was a growth experience, both
personally and professionally, and the
first time I had the opportunity to do
what I had joined the military to do
and what I was trained for,’’ she said.
‘‘I had the chance to meet a lot of
people from different walks of life,
whether they were from Iraq or the
coalition forces. We were able to learn
from some of the other health care
providers, and we taught trauma
training to some of the doctors and
nurses in Iraq who were going to be
stationed in hospitals out in the
population. That was very rewarding.’’
When Richardson returned from
Iraq she became the emergency and
critical care career manager/U.S. Army
Human Resources Command for
VETERAN OF TWO FRONTSBy Kendra Y. Mims, ENA Connection
Member Finds Military Nurses, Emergency Nurses Not So Different in Their Roles
Lt. Col. Kathleen Richardson, DNP, RN, ARNP, CNS, NP-C, CEN.

Official Magazine of the Emergency Nurses Association 35
Fourth Edition
The Emergency Nurses Association is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation.
The Authoritative Course for Pediatric Emergency Nursing• PediatricAssessmentTriangle
• EarlyIntervention
• FamilyPresence
Take the Course Today!www.ena.org/ENPC
�2DayIntensiveCourse �23ChapterComprehensiveManual
�Hands-onSkillStations �ContactHoursAvailable �4OnlineModules
ENPC Ad_Connection_half_05 2014.indd 1 4/9/14 11:52 AM
several years. She enjoyed her role as
the assignment officer and career
manager for emergency and critical
care nursing officers in the U.S. Army.
‘‘In the Army, you are managed by
an individual who looks at all of the
assignments across the world,’’ she
said. ‘‘We would make visits to
different hospitals to talk to individuals
face-to-face to learn more about their
personal and professional goals and
pair their goals with the training they
needed to be successful. We would
help them plan their careers, whether
it was moving up or getting out of the
Army and help them work through
making those decisions. We worked
closely to make sure that we had the
right people in the right places at the
right times, while ensuring that the
hospitals could still run efficiently
during their leave of absence.
Balancing that was the hard part.’’
Today, Richardson is the Uniformed
Services University, Doctor of Nursing
Practice phase II Residency director
and a practicing nurse practitioner at
Madigan Army Medical Center.
Looking back at her career, she
says becoming an Army nurse gave
her the opportunity to do things she
wouldn’t have accomplished if she had
worked in the civilian sector, such as
transporting patients via helicopter as a
flight nurse and developing flight
protocols.
‘‘I’ve had the opportunity to teach
and meet people from different
branches of the service,’’ she said.
‘‘Every time that I’ve met a new person
or went to a new facility, it’s helped
me grow and understand what my role
as a military nurse really means.
‘‘I think being an Army nurse is
really looking at what you want to do,
who you want to be and what you want
to contribute. Being an Army nurse has
helped me continue to strive to reach
my full potential and give back to the
nurses who are coming up behind me
to ensure they are getting the support
they need. They are going to take care
of me and my family someday, and if
they can use what I’ve learned to grow
even further, then we are bettering
nursing and health care as a whole.’’
Richardson believes the roles of
emergency and military nurses go
hand in hand.
‘‘The emergency nurse is that
frontline health care provider who is
there to ensure that individuals get the
support and care that they need,
whether it’s for a trauma or a cold,’’
she said. ‘‘I think the goal of the
military health system is to make sure
that soldiers are healthy and get the
care they need to do their jobs. When
it comes down to it, the army nurse
and emergency nurse are both there to
help the individual who is in need
right now get back to their life.
Whether it’s being a nurse in the ED in
the civilian sector or in the military
sector, it’s the same mission.’’

T he Academy of Emergency
Nursing launched the EMINENCE
(Establishing Mentors InterNationally
for Emergency Nurses Creating
Excellence) program in 2008 to pair
ENA emerging professionals with
experienced AEN fellows to work on
specific projects for one year. Previous
project topics have included writing for
publication, professional presentation,
research, program development,
advanced practice role development,
injury prevention and educational
conference planning.
ENA member Charlann Staab, MSN,
RN, CFRN, CHC, CHPC, clinical
services manager for Phi Air Medical,
LLC, always had wanted to write an
article for a publication but didn’t
know where to begin. In 2012, she
was one of 15 mentees selected to
participate in the EMINENCE program.
That gave her an opportunity to learn
from an emergency nurse who had
expertise in writing and editing for
publication.
She was paired with Carole Rush,
RN, M.Ed., CEN, FAEN, clinical nurse
educator at Okotoks Urgent Care, who
has more than 20 years of experience
in writing and editing for publications.
Rush was a co-section editor, with
Patricia Clutter, for the ‘‘International
Nursing’’ column in the Journal of
Emergency Nursing from 2007 to 2013
and is the case study section editor of
the International Emergency Nursing
Journal, based in the United Kingdom.
Several years ago, Staab developed
an interest in writing on the challenges
of pain management for patients taking
methadone. Once she became a
mentee in the EMINENCE program,
she discussed her aspirations with
Rush, who supported Staab’s goal and
provided her with writing guidance.
Staab is grateful for the support and
direction and said the EMINENCE
opportunity allowed them to build a
lasting relationship beyond the program.
‘‘I was attracted to the EMINENCE
program because you could be
matched with someone who is skilled
and is willing to give you that push,
direction and feedback,’’ she said.
‘‘That was the part I was interested in,
and Carole did that and so much more.
Carole is an editor and has been for
years, along with many other things,
and she was a natural to give me
insight into the writing process. She
gave me the pros and cons and helped
me learn the writing guidelines for
publications. She’s very honest, and
you need a mentor who can be honest
with you, who knows the ropes and
the process and who will help your
project be successful.’’
Rush also participated in the
2010-2011 program as a mentor for an
educational conference-planning
project topic.
‘‘It is challenging to start and
complete a project on one’s own,’’
Rush said. ‘‘The EMINENCE mentoring
program is a good opportunity to work
with emergency nurses who have
common interests and experiences and
who are willing to share their
knowledge and experience, time and
contacts. Everyone can benefit from
both being a mentor and a mentee, so
seek out those opportunities for a
specific project/goal.’’
As Staab’s mentor, Rush said she
learned a lot about the article’s focus,
methadone, and its impact on pain
management in emergency care.
‘‘By helping Charlann through the
writing process, I improved my editing
skills,’’ Rush said. ‘‘Working with
another nurse who is keen to learn and
complete a project is very motivating.
The most satisfying part is giving back
and helping another emergency nurse,
as I have been helped by many nurses
throughout my career.’’
Staab’s article has been accepted for
publication and will appear in the
‘‘Toxicology’’ column of JEN. She also
presented the article at the Arizona
ENA State Council’s ‘‘Hot Topics’’
conference in April.
Staab encourages members to share
their knowledge through the
mentoring program.
‘‘I highly recommend the
EMINENCE program to anyone who
has interest,’’ she said. ‘‘This program
provides you with networking
opportunities and resources, and it
matches you with a knowledgeable
mentor who is accessible and has the
expertise to help you reach your goal.
‘‘I think sharing knowledge is crucial
to our profession. There are a lot of ENA
members who have expertise in a
certain area, or they’ve had an
experience that other members can
learn from, but we’ve got to get it into a
medium where we can share it. Whether
it’s writing for publication, prepping you
to do a dynamite presentation or helping
you to achieve another goal, this
program has the best networking
resources of experts and members.’’
For more information on the
program, please visit www.ena.org/
about/academy/EMINENCE.
June/July 201436
By Kendra Y. Mims, ENA Connection
Find a Perfect Pairing Through EMINENCE
Charlann Staab
Carole Rush

For more than six years, ENA has
administered a State Council
Achievement Award program,
designed to assist ENA state
organizations in developing best
practices and to recognize the states
that have met or exceeded the
necessary requirements. This summer,
ENA will launch a new application
program to reward accountability and
recognize state councils for achieving
best practices and organizational
excellence beyond basic compliance.
The new program will improve
recognition of the states for their
efforts to 1) improve networking
and professional development
opportunities for members and
2) conduct state council affairs in a
sound business manner. State Council
Achievement Award recipients will be
honored based on their outstanding
performance and accomplishments.
The ENA Board of Directors
appointed the ENA State Council
Achievement Award Work Team to
review and recommend the new
application objective. Additionally, the
work team is charged with developing
the application and evaluation tool
and ultimately will be reviewing and
ratifying the applicants.
State councils must meet basic
compliance requirements to be
eligible to complete the award
application.
Standards Changing for State Council Achievement Awards
T he New England Regional Symposium celebrated its
40th anniversary April 16-18 in Mystic, Conn. Each year,
a different ENA state council plans the event, and this year
was the Connecticut ENA State Council’s turn.
Kara Cleveland, BSN, RN, CEN, and Mary Davis, BS, RN,
CEN, were co-chairs of the event. The theme was
‘‘Navigating Change,’’ inspired by the seaport setting of
Mystic along with trends in the current industry.
‘‘Change is all around, and everything is changing in
health care with the Affordable Care Act, high reliability and
hospitals becoming more transparent,’’ Cleveland said. ‘‘We
then focused on the nautical theme.’’
The planning committee worked diligently to create a
successful event. Cleveland noted that one unforeseen issue
was that the conference fell during Easter week.
‘‘We booked the venue in October 2012
and were hoping that since it was during
April break, people could bring their
families. When we realized it was Easter, it
put pressure on us to get the attendees,’’ she
said.
Because of the committee’s efforts
and a strong push during the weeks
leading up to
the event, about
160 nurses registered for the 2014 NERS.
For NERS’s ruby anniversary, the planning committee
focused on the color red. Bags and conference materials
were colored red, and attendees were entered into a raffle
for a ruby necklace. The committee also worked to bring in
presenters who have spoken on a national level, including
ENA President Deena Brecher, MSN, RN, APN, ACNS-BC,
CEN, CPEN, who delivered the keynote address, and ENA
Secretary/Treasurer Kathleen Carlson, MSN, RN, CEN, FAEN.
Feedback for the symposium has been positive, Cleveland
said. A highlight for her was Brecher’s keynote presentation.
‘‘It set the tone for the event,’’ she said. ‘‘The title was
‘My Patients Are Fine, I Am Going to Lunch,’ and it focused
on high reliability, transparency and patient safety.’’
Two events were held for attendees to take in the sights
of Mystic and network with colleagues. A welcome ‘‘Mystic
Pizza Party’’ was well received. ‘‘Drop Anchor at the
Aquarium’’ featured catered hors d’oeuvres and access to the
aquarium at night.
‘‘I think when you’re planning, it takes a whole team,’’
Cleveland said, ‘‘and we had a fantastic committee. They say
‘it takes a village,’ which may be a cliché, but it was our
whole team that pulled together [to make the event a
success].’’
Brecher agreed: ‘‘To have an emergency nursing
conference that spans 40 years is a tremendous
accomplishment. From the emergency nurses
who planned the events to the nurses who
attended, the focus on safe practice and safe
care was clear. It was exciting to be with ENA
members from New England as they
celebrated this great achievement.’’
The Maine ENA State
Council will host the 2015
event.
By Renée Herrmann, ENA Connection
40th Anniversary Celebration for NERS Truly Something to Sea
37

June/July 201438
connectionRecruitment & Professional
Opportunities
For ad rates and information, contact ENA Sales Representative Maureen Nolimal at 847-460-4076 or [email protected].
40 Blue Jay Consulting LLC www.bluejayconsulting.com
33 Chamberlain College of Nursing www.chamberlain.edu
29 Gebauer Company www.gebauer.com
38 JPS Health Network www.JPSNursing.org
39 New Hanover Regional Medical Center www.newhanovered.com
23 Pinpoint Inc. www.pinpointinc.com
5 Teleflex Incorporated www.teleflex.com
16- Teva20 www.tevausa.com
38 University of Virginia Health System www.uvajobsbeyondmeasure.com
ADVERTISER INDEXThese advertisers support ENA Connection. Let them know you saw their ad in this issue.
Love where you live, Love where you work!
Join our team today! Online: www.newhanovered.com
EOE
• Region’s only Level II Trauma Center and Tertiary Care Center
• 85,000 visits per year• Annual trauma admission volume
of 1,500• National recipient of 2013 Emergency
Nurses Association Research award, ENA Annual Leadership Conference
• AHA Mission LifeLine Gold Award Recipient in STEMI Care.
• Staff involvement in decision making. Lean incremental improvement, self scheduling, and shared governance.
New stand-alone ED opens in May of 2015! This new ED will include 10 treatment rooms, 2 observation rooms, 5 triage/low acuity spaces and a disposition lounge. Come be a part of our growth!
NHRMC’s Emergency Department:New Hanover Regional Medical Center’s Emergency Department is highly integrated to help ensure patients get the best care possible. It includes:
Emergency Department Nurses
Love where you work!Love where you work!
EOE/AA M/F/D/VThe University of Virginia is an equal opportunity and affirmative action employer. Women, minorities, veterans, and persons with disabilities are encouraged to apply.
linkedin/13NH9Yv /uvanurserecruitment @uvahealthjobs
When experience meets opportunity, great things happen. University of Virginia Medical Center seeks experienced, caring registered nurses for its emergency department, a Level I Trauma Center.
Join a dynamic team of nurses, patient care technicians, physicians and pharmacists that provide excellent quality care to patients from across the state and adjoining states by collaborating to develop innovative, team-activated protocols.
UVA Medical Center seeks registered nurses with 1–2 years of emergency department experience who are available to work 12–hour shifts during evening and night hours. BLS and ACLS required. TNCC and CEN certifications preferred.
Experienced registered nurses with a Bachelor of Science in Nursing and 2 or more years of experience will be offered a $5,000 sign on bonus and up to $5,000 relocation assistance for moves over 50 miles.
To learn more or apply, visit uvajobsbeyondmeasure.com or call 1-866-RNS-4UVA.
ER Nursing Opportunities atUVA Medical Center
“Every day brings an opportunity to see cutting edge trauma care. Nurses are the bedrock of our Emergency Department. It is our duty to provide the highest quality care.” - Meg Bryant, Director, Emergency Services
A major employer in the Fort Worth area, JPS is a teaching hospital and Level I Trauma Center. If you’re interested in joining our team, please visit www.JPSNursing.org
www.jpshealthnet.org

Love where you live, Love where you work!
Join our team today! Online: www.newhanovered.com
EOE
• Region’s only Level II Trauma Center and Tertiary Care Center
• 85,000 visits per year• Annual trauma admission volume
of 1,500• National recipient of 2013 Emergency
Nurses Association Research award, ENA Annual Leadership Conference
• AHA Mission LifeLine Gold Award Recipient in STEMI Care.
• Staff involvement in decision making. Lean incremental improvement, self scheduling, and shared governance.
New stand-alone ED opens in May of 2015! This new ED will include 10 treatment rooms, 2 observation rooms, 5 triage/low acuity spaces and a disposition lounge. Come be a part of our growth!
NHRMC’s Emergency Department:New Hanover Regional Medical Center’s Emergency Department is highly integrated to help ensure patients get the best care possible. It includes:
Emergency Department Nurses
Love where you work!Love where you work!

Improve emergency care, improve your career
You know us as recognized ED leaders who guide hospitals toward real and
effective change. Now we would like to get to know you. Blue Jay Consulting is
looking for professionals with the leadership insight and clinical experience to
bring process improvements to our clients, and the passion and commitment to
enhance the overall quality of emergency care. If you consider yourself among
the best in your fi eld, you’ll fi nd yourself in good company at Blue Jay Consulting.
Join the strongest team in the industry and improve your career.
Contact Jim Hoelz or Mark Feinberg at 407-210-6570 to discuss how we can capitalize
on one another’s strengths.
www.bluejayconsulting.com
“ As a Blue Jay consultant, I bring my 30 years of emergency department leadership experience to each client. Every assignment brings a unique set of challenges, but the tools to solve them are similar. We can often shorten the improvement process from years to months and create an environment that is better for patients, families and staff. I leave each assignment with a good feeling that I have left it better than when I arrived. I love being a Blue Jay consultant.”
— B I L L B R I G G S , M S N , R N , C E N , F A E N
Senior Consultant Blue Jay Consulting, LLC
41% 55%28% 68%
Average improvement in time from arrival to seeing a physician.
Typical improvement in patient satisfaction scores and likelihood to recommend
Average improvement in throughput for admitted and discharged patients
Average improvement in LWBS rates, resulting in an additional $1.6 million in collected revenue
13BJAC_ENA_RecruitmentAd 0807.indd 1 8/8/13 1:40 PM