ems training - epilepsy.com · ems training trainr’ gi 1 ems training epilepsy and seizure...
TRANSCRIPT
1EMS Training | Trainer’s Guide
EMS Training
Epilepsy and Seizure Management
TRAINER’S GUIDEFOR PERSONAL USE ONLY
The Epilepsy Foundation, a national non-profit with nearly 50 affiliated organizations throughout the United States, has led the fight against seizures since 1968.
The Foundation is an unwavering ally for individuals and families impacted by epilepsy and seizures. The mission of the Epilepsy Foundation is to stop seizures and SUDEP, find a cure, and overcome the challenges created by epilepsy through efforts including education, advocacy, and research to accelerate ideas into therapies.
The Foundation works to ensure that people with seizures have the opportunity to live their lives to their fullest potential.
For additional information, please visit www.epilepsy.com
© 2015 Epilepsy Foundation of America, Inc.
FOR PERSONAL USE ONLY
Introduction ........................................................................................................ 4 Training Goals ................................................................................................. 4 About This Trainer’s Guide.............................................................................. 5 The Layout ..................................................................................................... 5Training-at-a-Glance ........................................................................................... 6Resources/Materials .......................................................................................... 6Part 1: Training Opening & Overview ................................................................ 7 Opening/Introductions .................................................................................. 7 Highlights of the EMS Project ........................................................................ 7 Goals and Objectives ..................................................................................... 7Part 2: Understanding Seizures .......................................................................... 9 General seizure statistics ............................................................................... 9 Seizure description ........................................................................................ 9 Seizure vs intoxication ................................................................................. 10 Typical causes for seizures ........................................................................... 11Part 3: What is Epilepsy? .................................................................................. 12 Facts and myths about epilepsy ................................................................... 13 Define epilepsy ............................................................................................ 14 Epilepsy definition ....................................................................................... 14 Causes of epilepsy ....................................................................................... 14 Possible triggers for epilepsy-related seizures ............................................. 15 Two types of epilepsy-related seizures ........................................................ 15 Generalized seizures .................................................................................... 16 Partial seizures ............................................................................................. 17Part 4: Treating Seizures .................................................................................. 22 Treatment don’ts ......................................................................................... 23 Treatment do’s .............................................................................................. 24 Postictal phase ............................................................................................. 25 Situational treatments ................................................................................. 25 Treatment guidelines ................................................................................... 26 ALS circumstances ....................................................................................... 29 SAMPLE ........................................................................................................ 30Part 5: Wrap-Up ............................................................................................... 35 Medicines for Epilepsy Chart ....................................................................... 36
Table of Contents
FOR PERSONAL USE ONLY
4 Epilepsy Foundation
Introduction
About This Trainer’s Guide
The Epilepsy Foundation recognizes how important EMS response can be to the health and safety of people experiencing seizures. Proper training in responding to a seizure is particularly important considering the likelihood of EMS personnel encountering such a medical event – there are nearly three million Americans subject to seizures caused by epilepsy and millions more who may experience one or more seizure episodes as a result of trauma or other acute or chronic illness. This training is designed to prepare EMS responders for these events and provide them with the information necessary to provide appropriate treatment.
The Epilepsy Foundation realizes that not all facilitators of this training will be EMS or other medical personnel. To accommodate this likelihood, this trainer’s guide is designed to enable affiliate staff and/or trained volunteer facilitators to conduct the training as required.
NOTE: Whenever possible, it is highly recommended that affiliate staff partner/co-facilitate with someone from the local EMS team or another medical expert to ensure that technical questions are addressed and local protocols honored.
Training GoalsThis training is designed to:
• Strengthen EMS personnel knowledge about seizures.
• Enhance their ability to respond to those experiencing a seizure.
• Help EMS personnel make more informed decisions about additional care and hospital transport.
FOR PERSONAL USE ONLY

5EMS Training | Trainer’s Guide
The Layout
Each portion of this guide shows a time estimate at the top along with the section title. In some instances, the time estimate represents a range. This reflects the fact that there may be one or more optional activities that the trainer may choose depending on the amount of time available for the entire training.
Duration: X-XX minutes
Outline Content
TRAINING TIP:
PART X: Title
SAMPLE:
Trainer’s Notes:
The left-hand column lists points of discussion for that segment of the training. Once you become fully familiar with the content and structure of this document, you will find that the left-hand column serves as an at-a-glance outline.
The right-hand column contains the detailed content of the training, developed by a team of professionals. This area of the guide also serves as your sample script.
Shaded training tips.
Extra white space for handwritten notes.
FOR PERSONAL USE ONLY
6 Epilepsy Foundation
Training-at-a-Glance
Resources/Materials
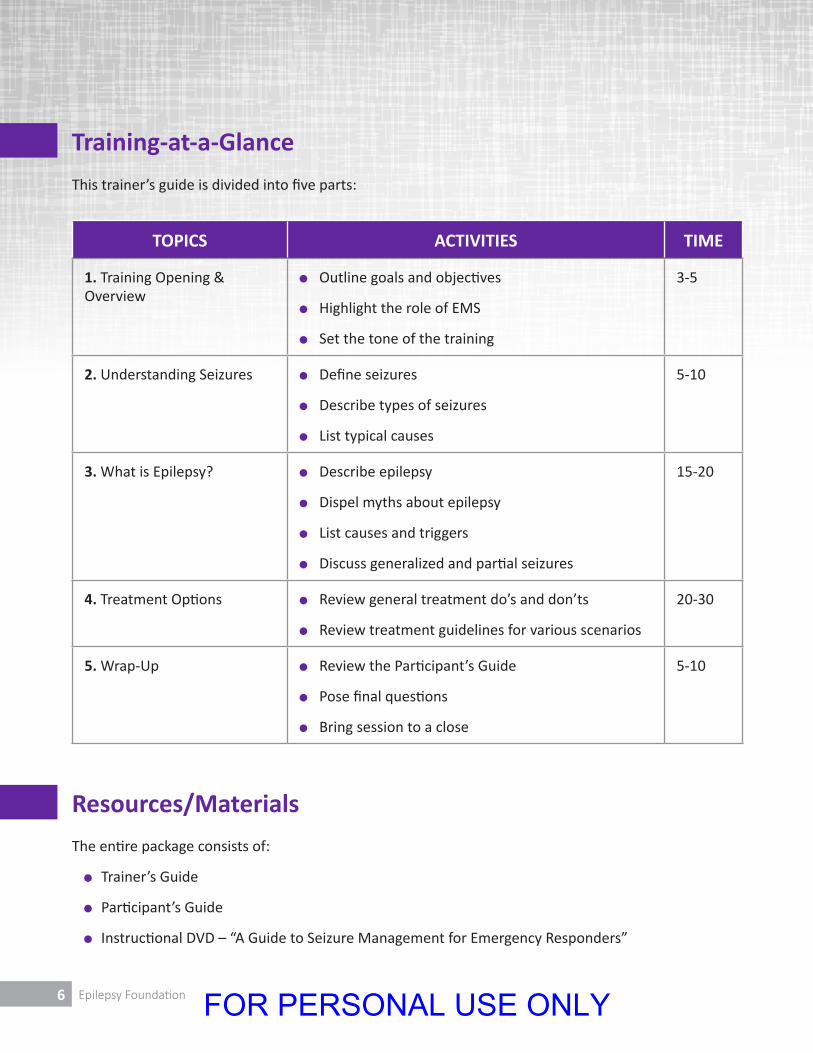
This trainer’s guide is divided into five parts:
The entire package consists of:
l Trainer’s Guide
l Participant’s Guide
l Instructional DVD – “A Guide to Seizure Management for Emergency Responders”
TOPICS ACTIVITIES TIME
1. Training Opening & Overview
l Outline goals and objectives
l Highlight the role of EMS
l Set the tone of the training
3-5
2. Understanding Seizures l Define seizures
l Describe types of seizures
l List typical causes
5-10
3. What is Epilepsy? l Describe epilepsy
l Dispel myths about epilepsy
l List causes and triggers
l Discuss generalized and partial seizures
15-20
4. Treatment Options l Review general treatment do’s and don’ts
l Review treatment guidelines for various scenarios
20-30
5. Wrap-Up l Review the Participant’s Guide
l Pose final questions
l Bring session to a close
5-10
FOR PERSONAL USE ONLY
7EMS Training | Trainer’s Guide
PART 1: Training Opening & Overview
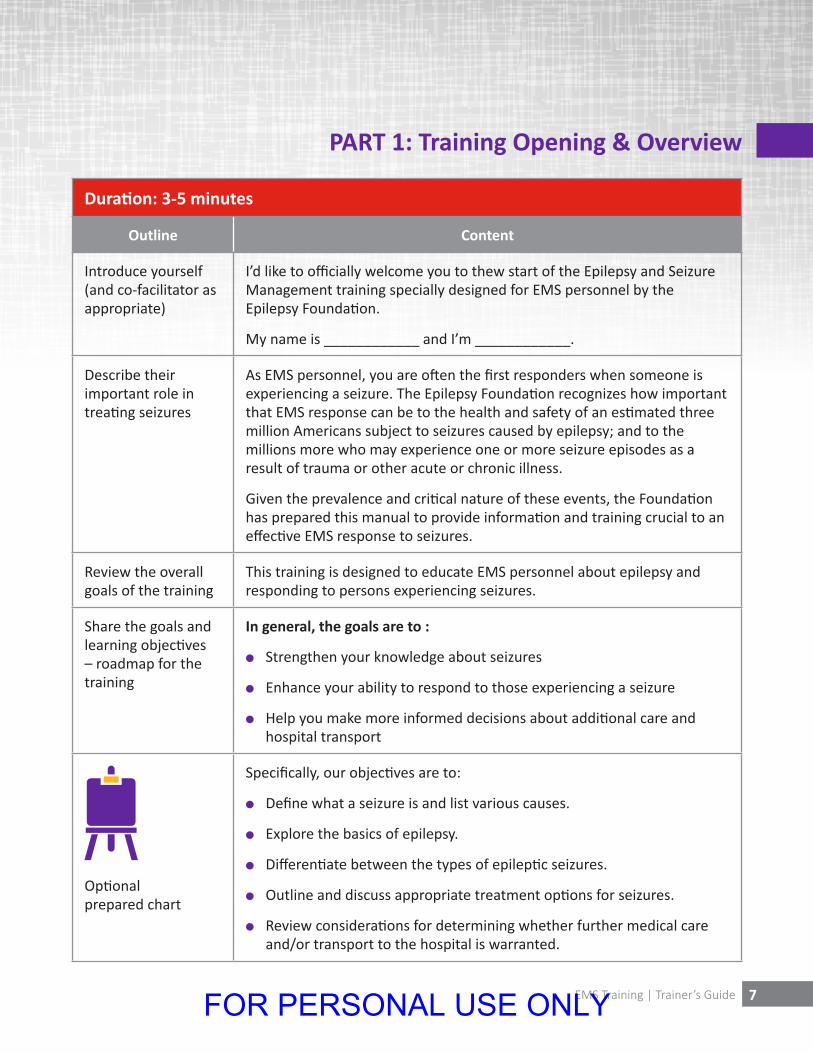
Duration: 3-5 minutes
Outline Content
Introduce yourself (and co-facilitator as appropriate)
I’d like to officially welcome you to thew start of the Epilepsy and Seizure Management training specially designed for EMS personnel by the Epilepsy Foundation.
My name is ____________ and I’m ____________.
Describe their important role in treating seizures
As EMS personnel, you are often the first responders when someone is experiencing a seizure. The Epilepsy Foundation recognizes how important that EMS response can be to the health and safety of an estimated three million Americans subject to seizures caused by epilepsy; and to the millions more who may experience one or more seizure episodes as a result of trauma or other acute or chronic illness.
Given the prevalence and critical nature of these events, the Foundation has prepared this manual to provide information and training crucial to an effective EMS response to seizures.
Review the overall goals of the training
This training is designed to educate EMS personnel about epilepsy and responding to persons experiencing seizures.
Share the goals and learning objectives – roadmap for the training
In general, the goals are to :
l Strengthen your knowledge about seizures
l Enhance your ability to respond to those experiencing a seizure
l Help you make more informed decisions about additional care and hospital transport
Optional prepared chart
Specifically, our objectives are to:
l Define what a seizure is and list various causes.
l Explore the basics of epilepsy.
l Differentiate between the types of epileptic seizures.
l Outline and discuss appropriate treatment options for seizures.
l Review considerations for determining whether further medical care and/or transport to the hospital is warranted.
FOR PERSONAL USE ONLY
8 Epilepsy Foundation
Outline Content
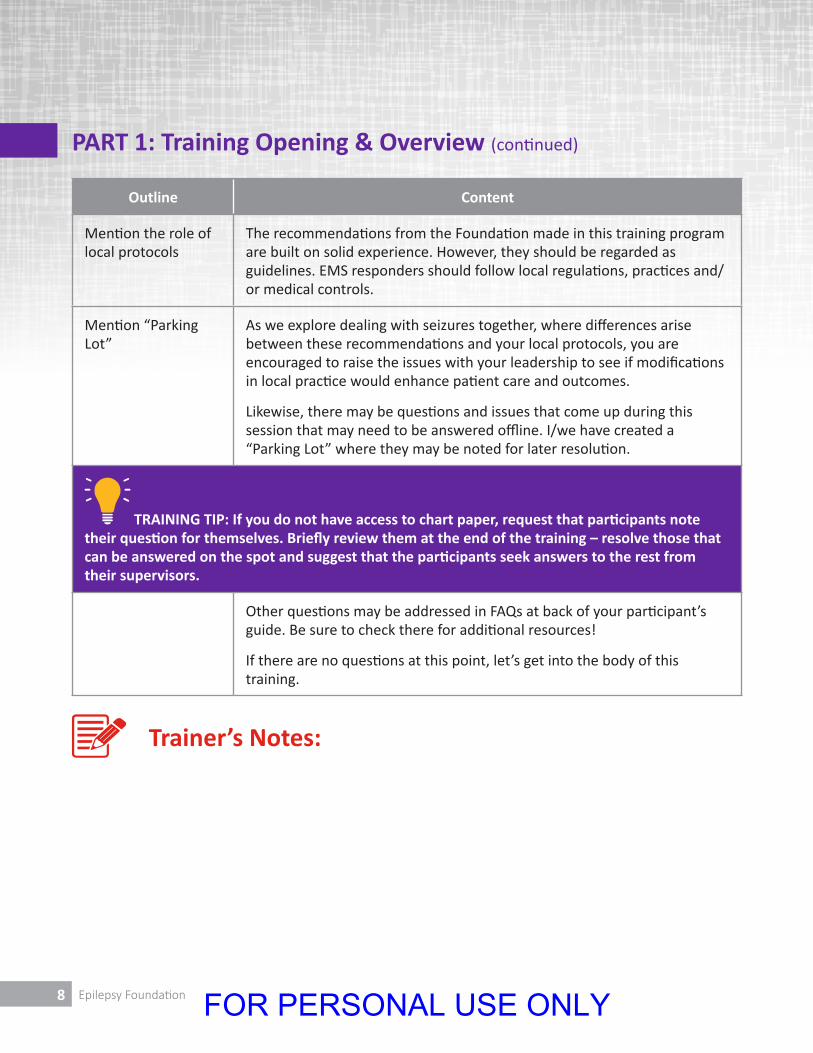
Mention the role of local protocols
The recommendations from the Foundation made in this training program are built on solid experience. However, they should be regarded as guidelines. EMS responders should follow local regulations, practices and/or medical controls.
Mention “Parking Lot”
As we explore dealing with seizures together, where differences arise between these recommendations and your local protocols, you are encouraged to raise the issues with your leadership to see if modifications in local practice would enhance patient care and outcomes.
Likewise, there may be questions and issues that come up during this session that may need to be answered offline. I/we have created a “Parking Lot” where they may be noted for later resolution.
TRAINING TIP: If you do not have access to chart paper, request that participants note their question for themselves. Briefly review them at the end of the training – resolve those that can be answered on the spot and suggest that the participants seek answers to the rest from their supervisors.
Other questions may be addressed in FAQs at back of your participant’s guide. Be sure to check there for additional resources!
If there are no questions at this point, let’s get into the body of this training.
PART 1: Training Opening & Overview (continued)
Trainer’s Notes:
FOR PERSONAL USE ONLY

9EMS Training | Trainer’s Guide
PART 2: Understanding Seizures
Duration: 5-10 minutes
Outline Content
Establish the importance of this training and topic
By a show of hands, how many of you here have ever responded to a seizure call? What do you remember about that experience?
TRAINING TIP: This question is designed to establish an idea of the experience level in the room and to engage the participants. Unless the group is small, taking comments from only a few participants will suffice to help you manage the limited time.
Discuss general statistics
It was mentioned earlier – what is the estimate for the number of people in the US who are subject to seizures caused by epilepsy?
There are an estimated three million Americans of all ages who are subject to seizures caused by epilepsy. And there are perhaps millions more who may experience one or more seizure episodes as a result of trauma or some other acute or chronic illness. That translates into roughly 1 in 100 Americans experiencing a seizure at some point in their lives. In fact, by age 80, nearly 10% of us will have experienced at least one seizure. At some point in time, you will encounter a seizure as an EMS responder.
Before we talk about protocols and treatment options, we need to first understand what a seizure is and some of the causes. This may be new information for some of us here and serve as a review for others.
Provide a high level description of a seizure
Normal nerve cells, or neurons, in the brain fire billions of electrical signals to each other by means of tiny bursts of energy. They start and then stop, over and over again. Think of these bursts as flashes of energy.
Introduce the idea of a generalized seizure
A seizure is a sudden, brief disruption of the normal functioning of neurons in the brain. The disruption in the neurological environment causes some nerve cells to fire without stopping and spread to involve other nerve cells. When this happens, a kind of electrical pulse sweeps through the brain and typically causes the affected person to stare, to fall, and to experience the massive muscular contractions generally known as convulsions. A seizure that involves the entire brain is called a generalized seizure. But not all seizures are dramatic.
FOR PERSONAL USE ONLY

10 Epilepsy Foundation
PART 2: Understanding Seizures (continued)
Outline Content
Introduce the idea of a partial seizure
More limited disruptions of brain function produce less dramatic changes in movement or behavior, depending on what part, or how much of the brain is affected. These episodes are all called seizures – better known as partial seizures because only part of the brain is affected. We’ll talk more about these two types of seizures shortly.
A seizure usually lasts a few seconds to a few minutes, and return to full awareness may be rapid or slow.
Describe seizures vs. intoxication
It may sometimes be tricky to differentiate between someone who is experiencing a seizure from someone who is intoxicated or reacting to legal or illegal substances.
A seizure begins suddenly, whereas intoxication is a slowly building process. Information from bystanders/friends about the way the episode began will help identify which condition is present. During a seizure, the muscles of the body alternately contract and relax while the patient is unconscious. This massive relaxation of muscles may include those involved with bladder and bowel control.
After a seizure, recovery may occur over a matter of minutes to an hour. An intoxicated person takes considerably longer to become alert, oriented and regain clear speech than someone suffering from a seizure. However, do not rely on the smell of alcohol as a telltale sign that it is intoxication rather than a seizure. The person may have simply had a glass of wine prior to the seizure episode.
A seizure begins suddenly, whereas intoxication is a slowly building process. Information from bystanders/friends about the way the episode began will help identify which condition is present. During a seizure, the muscles of the body alternately contract and relax while the patient is unconscious. This massive relaxation of muscles may include those involved with bladder and bowel control.
After a seizure, recovery may occur over a matter of minutes to an hour. An intoxicated person takes considerably longer to become alert, oriented and regain clear speech than someone suffering from a seizure. However, do not rely on the smell of alcohol as a telltale sign that it is intoxication rather than a seizure. The person may have simply had a glass of wine prior to the seizure episode.
FOR PERSONAL USE ONLY

11EMS Training | Trainer’s Guide
PART 2: Understanding Seizures (continued)
Outline Content
List typical causes of seizures
Optional prepared chart
A seizure may be idiopathic - that is, it is of unknown cause. Or a seizure may be secondary to an injury, infection or other disorder affecting the brain.
Typical causes (of the disruption in the neurological environment making way for a seizure) include:
l Head trauma
l Poisoning
l Chemical imbalances
l Certain drugs
l Severe infections of the brain
l High fever
l Flashing lights
Establish epilepsy as a common cause of seizures
One of the most common causes of seizures is epilepsy. It is a neurological disorder that has recurring seizures as its primary symptom.
Trainer’s Notes:
FOR PERSONAL USE ONLY
12 Epilepsy Foundation
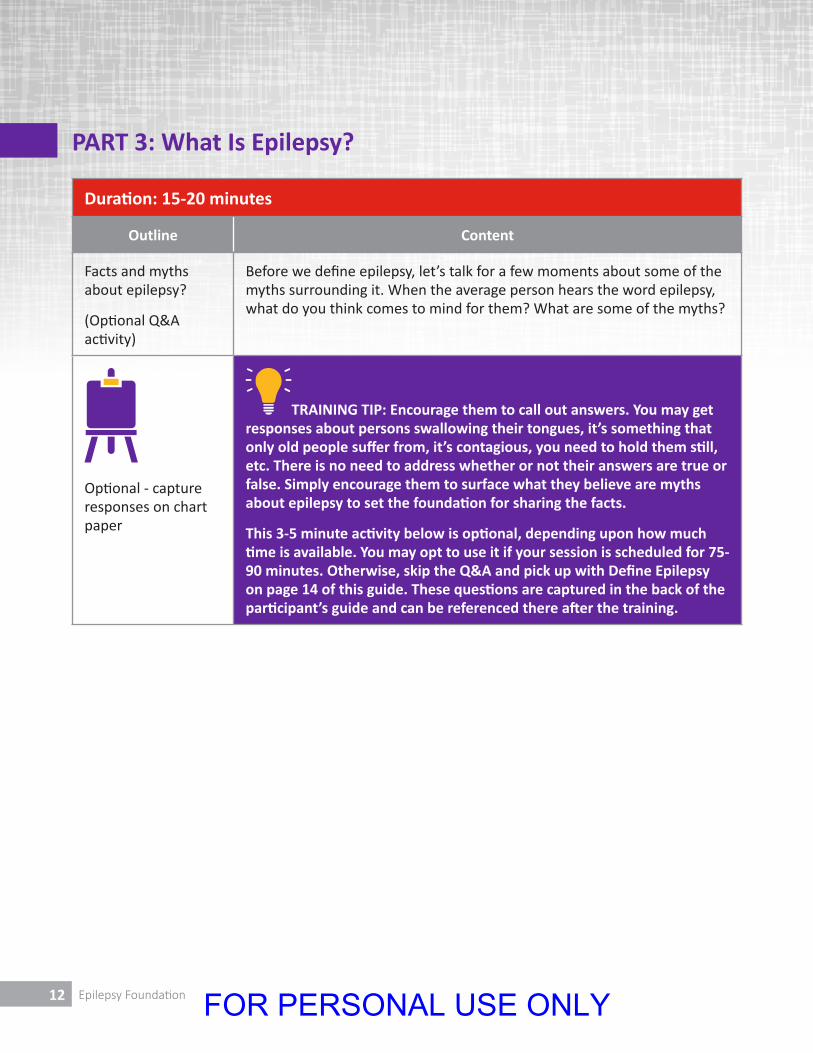
PART 3: What Is Epilepsy?
Duration: 15-20 minutes
Outline Content
Facts and myths about epilepsy?
(Optional Q&A activity)
Before we define epilepsy, let’s talk for a few moments about some of the myths surrounding it. When the average person hears the word epilepsy, what do you think comes to mind for them? What are some of the myths?
Optional - capture responses on chart paper
TRAINING TIP: Encourage them to call out answers. You may get responses about persons swallowing their tongues, it’s something that only old people suffer from, it’s contagious, you need to hold them still, etc. There is no need to address whether or not their answers are true or false. Simply encourage them to surface what they believe are myths about epilepsy to set the foundation for sharing the facts.
This 3-5 minute activity below is optional, depending upon how much time is available. You may opt to use it if your session is scheduled for 75-90 minutes. Otherwise, skip the Q&A and pick up with Define Epilepsy on page 14 of this guide. These questions are captured in the back of the participant’s guide and can be referenced there after the training.
FOR PERSONAL USE ONLY
13EMS Training | Trainer’s Guide
Outline Content
Address typical questions and myths about epilepsy
While we won’t be able to deal with all of the myths and questions about epilepsy today, let’s cover a few that often come up.
Q: Is it true that flashing lights can trigger a seizure?
Yes. Some people with epilepsy are photosensitive. This means that they may have a seizure if exposed to intense, strobe-type light or a group of lights flashing synchronously.
Q: Is epilepsy contagious?
No, epilepsy is not contagious in any way. People used to be afraid that contact with the saliva that may collect around the mouth when someone has a seizure could pass the condition on. However, we know now that this is totally untrue. You cannot catch epilepsy or seizure disorders.
Q: Then is epilepsy considered a disease?
Not in the sense that it can be caught from or passed on to another person. It is better described as a disorder or health condition.
Q: Do people with epilepsy have a mental illness?
Epilepsy is not considered to be a mental illness, although a seizure may briefly affect mental functioning. However, like any other person, people who have epilepsy may also have mental health problems including depression and anxiety.
Q: Is epilepsy the same as a seizure disorder?
Yes. Epilepsy may be referred to as a seizure disorder or vice versa. Because of the lingering stigma associated with the condition, some people may strongly deny that they have epilepsy. But they may acknowledge having a ‘seizure disorder’ instead. EMS responders should use both terms – epilepsy and seizure disorder – when taking a patient history.
PART 3: What Is Epilepsy? (continued)
FOR PERSONAL USE ONLY
14 Epilepsy Foundation
Outline Content
Define epilepsy What is epilepsy? It is one of the most common causes of seizures, and is also called a seizure disorder. Specifically, epilepsy is a neurological disorder characterized by recurring seizures not otherwise provoked by acute injury or other health emergency. It is one of the potential causes that should always be considered by EMS personnel when called to respond to a seizure event or a person displaying signs of altered mental functioning (mentation).
Share causes of epilepsy
In 70% of cases, no cause can be found and it’s estimated that genetic factors play a role. Known causes include head injuries, stroke, brain tumors, poisoning, problems in brain development before birth, or serious infections such as encephalitis or meningitis.
Among elderly people, epilepsy is most often caused by stroke, cardiovascular disease, brain tumors or Alzheimer’s disease. Epilepsy is also more prevalent in children with mental retardation, Down syndrome, autism, cerebral palsy, and other developmental disorders. Many returning veterans with head injuries develop epilepsy.
Except for stroke, epilepsy is the most common neurological disorder in the United States, affecting some three million Americans of all ages, or at least one in every 100 people
PART 3: What Is Epilepsy? (continued)
FOR PERSONAL USE ONLY

15EMS Training | Trainer’s Guide
Outline Content
List possible triggers for epilepsy-related seizures
In many cases, there is no obvious trigger for a seizure in someone who has been diagnosed with epilepsy. In addition, the possibility of seizures exists despite use of seizure-preventing medication. Nevertheless, there are some key triggers that may produce seizures in people with epilepsy. They include:
l Failure to take medication or running out of medication
l Effects of a planned change in medication or interaction with other medication, either purchased over the counter or prescribed
l Sleep deprivation
l Key points of the menstrual cycle in women
l Effects of hunger or excessive stress
l Heavy use of alcohol or other drugs, or withdrawal from such use
l High fever from infection
l Severe dehydration
l Exposure to flashing lights
Information from witnesses or family members may provide clues about whether or not one or more of these triggers were present, helping the EMS responder identify an epilepsy-related seizure.
Describe the two types of epilepsyrelated seizures – generalized and partial - in greater detail
We touched upon this earlier. There are two types of seizures associated with epilepsy based on how much of the brain is involved in the neurological disruption.
Does anyone remember the two types?
The first is called a generalized seizure which involves a disruption in the entire brain. The second type is called a partial seizure. Just as the name implies, this type of seizure affects only certain parts of the brain.
A generalized seizure affects the whole brain at once. This is the type of seizure that is most commonly encountered by EMS responders because of its dramatic symptoms. It is often marked by convulsions, and can also be caused by head trauma, brain tumors, poisoning, metabolic disorders (such as diabetes), or other acute conditions affecting the brain.
PART 3: What Is Epilepsy? (continued)
FOR PERSONAL USE ONLY

16 Epilepsy Foundation
Outline Content
Provide details regarding generalized seizures
(Pages 9-10 of the Participant’s Guide)
Under the category of generalized seizures, you may encounter:
Generalized Tonic Clonic
Generalized tonic clonic seizure:
l Formerly called grand mal seizures.
l Most common and best known type of generalized seizure.
l Begins with stiffening of the limbs (the tonic phase), followed by jerking of the limbs and face (the clonic phase).
Absence seizures Absence seizures:
l Formerly known as petit mal.
l Marked by lapses of awareness, sometimes with staring, that begin and end abruptly, lasting only a few seconds.
l There is no warning and no after-effect.
l Awareness and the ability to communicate usually quickly return after an absence seizure.
l More common in children than in adults, absence seizures are frequently so brief that they escape detection, even if the child is experiencing 50 to 100 attacks daily. They may occur for several months before a child is sent for a medical evaluation.
Myoclonic seizures Myoclonic seizures:
l Marked by rapid, brief contractions of the muscles, which usually occur at the same time on both sides of the body.
l Occasionally, they involve one arm or a foot.
l People usually think of them as sudden jerks or clumsiness. A variant of the experience, common to many people who do not have epilepsy, is the sudden jerk of a foot during sleep.
PART 3: What Is Epilepsy? (continued)
FOR PERSONAL USE ONLY

17EMS Training | Trainer’s Guide
Outline Content
Atonic seizures Atonic seizures:
l Create an abrupt loss of muscle tone.
l Sometimes called drop attacks, astatic or akinetic seizures.
l They result in head drops, loss of posture, or sudden collapse.
l Because they are so abrupt, without any warning, and because the people who experience them fall with force, atonic seizures can result in injuries to the head and face. Protective headgear is sometimes used by children and adults.
l Awareness and the ability to communicate usually quickly return after an atonic seizure.
l This type of generalized seizure tends to be resistant to drug therapy.
Infantile Spasms Infantile Spasms:
l Clusters of quick, sudden movements that start between 3 months and two years of age.
l If a child is sitting up, the head will fall forward, and the arms will flex forward.
l If lying down, the knees will be drawn up, with arms and head flexed forward as if the baby is reaching for support.
Remember, by definition, a generalized seizure means the electrical disruption involves the entire brain.
Provide details regarding partial seizures
(Pages 10-11 of the Participant’s Guide)
In partial seizures the electrical disturbance is limited to a specific area of one cerebral hemisphere (side of the brain). Partial seizures are the most common type of seizure experienced by people with epilepsy. Virtually any movement, sensory, or emotional symptom can occur as part of a partial seizure, including complex visual or auditory hallucinations. Partial seizures may spread to cause a generalized seizure, in which case the classification category is partial seizures secondarily generalized.
Two categories of partial seizures
Partial seizures are subdivided into simple partial seizures (in which consciousness is retained); and complex partial seizures (in which consciousness is impaired or lost).
PART 3: What Is Epilepsy? (continued)
FOR PERSONAL USE ONLY
18 Epilepsy Foundation
PART 3: What Is Epilepsy? (continued)
Outline Content
Simple Partial seizure
Simple partial seizure:
l May be no more than an odd feeling, a shaking limb, a change in how things look or smell.
l It could be experienced as a period of lost time that only the person having the seizure experiences.
l These episodes are unlikely to generate calls for emergency assistance unless they are continuous. However, they sometimes precede a generalized seizure.
l Family members or bystanders reporting that someone experiencing a convulsion or a period of changed awareness first had an odd feeling is helpful information for establishing a diagnosis.
Complex Partial seizure
Complex partial seizure:
l Easily mistaken for an episode of mental illness, intoxication, drug use or anti-social behavior.
l Depending on the function of the affected part of the brain and how extensive the disruption is, this type of seizure produces a kind of dreamstate, in which the person appears to be awake but is completely or almost completely out of touch with his or her surroundings.
l The person will be unable to respond to directions and may mumble or repeat a phrase over and over again.
l The person may wander into traffic or other danger quite oblivious to the risk of harm.
l In rare cases, people having this type of seizure may cry out, run, flail their arms, or experience extreme fear.
FOR PERSONAL USE ONLY
19EMS Training | Trainer’s Guide
PART 3: What Is Epilepsy? (continued)
Outline Content
Exercise caution in making assumptions about behaviors
Partial seizures are sometimes more difficult to recognize than generalized seizures because the outwards symptoms are more subtle and they will vary depending upon which part of the brain is impacted. While the overwhelming majority of EMS responders do an outstanding job recognizing and handling citizens experiencing seizures, in limited cases they may respond with inappropriate force to behaviors associated with seizures, especially complex partial seizures. These particular seizures cloud awareness, block normal communication, and produce a variety of undirected, involuntary and unorganized movements that may be mistakenly viewed as aggression. The results can be fatal, especially when dangerous restraint practices are used.
DO NOT FORCIBLY RESTRAIN A PERSON WHO IS HAVING A SEIZURE; THIS INCLUDES USE OF IMMOBILIZATION TECHNIQUES AND DEVICES.
Let’s recap a few major points before moving into seizure treatment.
TRAINING TIP: If time permits, you may present the recap as a series of questions actually posed to group to informally test their retention of the material and provide a degree of interactivity.
FOR PERSONAL USE ONLY
20 Epilepsy Foundation
PART 3: What Is Epilepsy? (continued)
Outline Content
Epilepsy can be defined as:
l A brain disorder marked by recurring seizures.
There are two kinds of seizures:
l Generalized
l Partial
Generalized seizures:
l Involve a disruption in the entire brain
l Are marked by convulsions and other dramatic/recognizable symptoms
l Often result in EMS calls because of their dramatic nature
Pages 9 and 10 of your Participant’s Guide summarizes the various types of generalized seizures.
Partial seizures:
l Involve only a portion of the brain
l Show different symptoms and behaviors depending upon which part of the brain is affected
l Are often mistaken for intoxication or drug use
TRAINING TIP: If your session is scheduled for 75-90 minutes and you have access to a DVD player and TV for viewing, you may recap the material covered up to this point by showing the first 5 minutes and 10 seconds (5:10) minutes of the video entitled “A Guide to Seizure Management for Emergency Medical Responders”.
FOR PERSONAL USE ONLY
21EMS Training | Trainer’s Guide
PART 3: What Is Epilepsy? (continued)
Trainer’s Notes:
Outline Content
Video Recap & Treatment Preview (Optional)
We have already laid the foundation in this training by describing what a seizure is and exploring the various types of seizures. Now let’s switch gears to discuss treatment options when you are called to the scene.
FOR PERSONAL USE ONLY
22 Epilepsy Foundation
PART 4: Treating Seizures
Duration: 20-30 minutes
Outline Content
Introduce the idea of BLS and ALS responses
The Epilepsy Foundation recognizes that training of EMS responders, authority for their practice, and the utilization of medications and treatments varies from location to location. This training should be viewed as guidelines, honoring local protocols. With this in mind, suggested response and treatments guidelines are divided into “All Responders/BLS Response (Basic Life Support)”, and “ALS Response (Advanced Life Support)”.
FOR PERSONAL USE ONLY
23EMS Training | Trainer’s Guide
PART 4: Treating Seizures (continued)
Outline Content
Review important treatment don’ts
There are a number of important cautions that you must be aware of:
Treatment Don’ts
l Don’t give anything by mouth - people with epilepsy should never be given epilepsy meds and/or fluids until the seizure is over and consciousness has returned.
l Don’t restrain - The EMS responder should never attempt to prevent further injury by restraining the jerking movements of someone having a seizure. Restraining involuntary muscle spasms that produce jerking may cause muscle tears or even fractures. It is better to let the movements take place freely, but to protect the head from continued impact on the ground by placing something flat and soft underneath. Make sure breathing is unimpeded.
l Don’t make assumptions - EMS responders should never assume that because an alcohol type odor isnoted on a person’s breath, the individual is intoxicated. The individual may have gone out to dinner and had a single drink prior to the seizure, but the two events are not necessarily connected. Withdrawal from alcohol or barbiturates is more likely to trigger a seizure.
l Don’t allow extended seizure - although not an actual type of seizure, status epilepticus is said to exist after 30 minutes of continuous seizure activity. It is a true medical emergency requiring immediate treatment or rapid transport to the hospital. However, current recommendations call for treatment to stop a convulsive seizure if it has continued for more than 5 minutes, followed by hospital transport.
While prolonged generalized convulsions are regarded as being of highest risk, it is also possible to experience prolonged partial seizures. These present as episodes of continual confusion lasting much longer than the 2 to 3 minutes that a normal seizure of this type would last. Because they represent continuing disruption of brain activity, they too require emergency treatment and need to be stopped as soon as possible.
FOR PERSONAL USE ONLY
24 Epilepsy Foundation
PART 4: Treating Seizures (continued)
Outline Content
Review general actions responders DO want to take
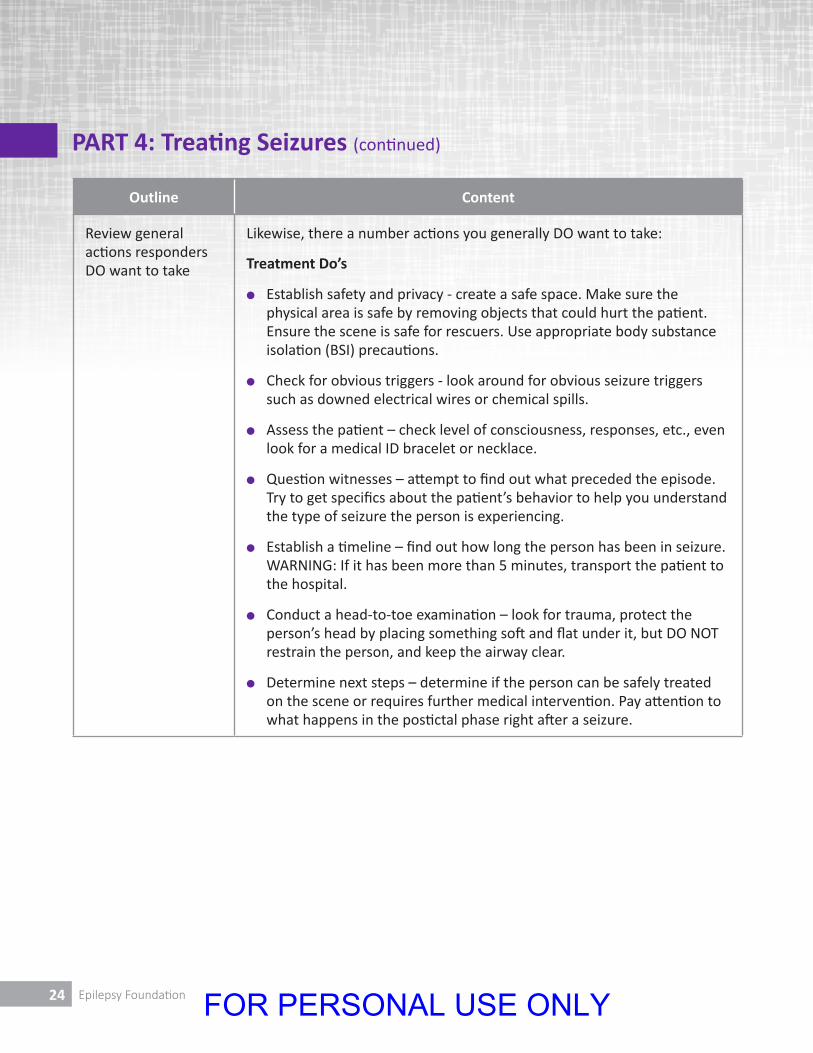
Likewise, there a number actions you generally DO want to take:
Treatment Do’s
l Establish safety and privacy - create a safe space. Make sure the physical area is safe by removing objects that could hurt the patient. Ensure the scene is safe for rescuers. Use appropriate body substance isolation (BSI) precautions.
l Check for obvious triggers - look around for obvious seizure triggers such as downed electrical wires or chemical spills.
l Assess the patient – check level of consciousness, responses, etc., even look for a medical ID bracelet or necklace.
l Question witnesses – attempt to find out what preceded the episode. Try to get specifics about the patient’s behavior to help you understand the type of seizure the person is experiencing.
l Establish a timeline – find out how long the person has been in seizure. WARNING: If it has been more than 5 minutes, transport the patient to the hospital.
l Conduct a head-to-toe examination – look for trauma, protect the person’s head by placing something soft and flat under it, but DO NOT restrain the person, and keep the airway clear.
l Determine next steps – determine if the person can be safely treated on the scene or requires further medical intervention. Pay attention to what happens in the postictal phase right after a seizure.
FOR PERSONAL USE ONLY
25EMS Training | Trainer’s Guide
PART 4: Treating Seizures (continued)
Outline Content
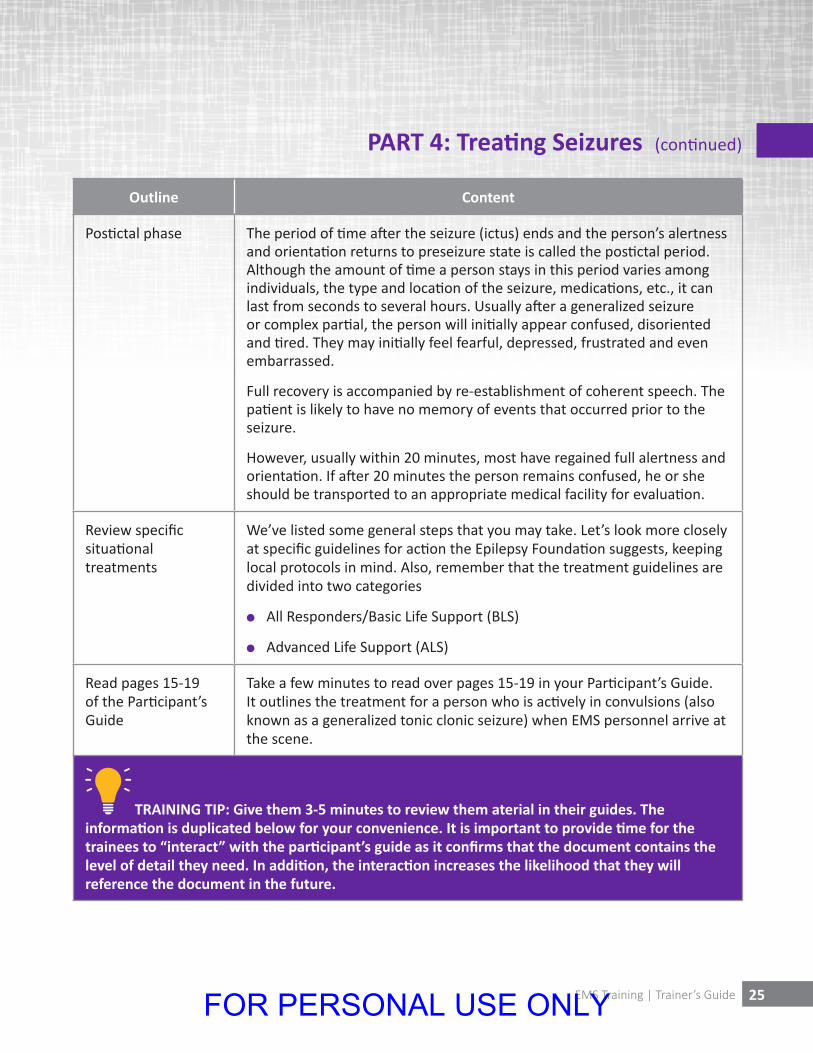
Postictal phase The period of time after the seizure (ictus) ends and the person’s alertness and orientation returns to preseizure state is called the postictal period. Although the amount of time a person stays in this period varies among individuals, the type and location of the seizure, medications, etc., it can last from seconds to several hours. Usually after a generalized seizure or complex partial, the person will initially appear confused, disoriented and tired. They may initially feel fearful, depressed, frustrated and even embarrassed.
Full recovery is accompanied by re-establishment of coherent speech. The patient is likely to have no memory of events that occurred prior to the seizure.
However, usually within 20 minutes, most have regained full alertness and orientation. If after 20 minutes the person remains confused, he or she should be transported to an appropriate medical facility for evaluation.
Review specific situational treatments
We’ve listed some general steps that you may take. Let’s look more closely at specific guidelines for action the Epilepsy Foundation suggests, keeping local protocols in mind. Also, remember that the treatment guidelines are divided into two categories
l All Responders/Basic Life Support (BLS)
l Advanced Life Support (ALS)
Read pages 15-19 of the Participant’s Guide
Take a few minutes to read over pages 15-19 in your Participant’s Guide. It outlines the treatment for a person who is actively in convulsions (also known as a generalized tonic clonic seizure) when EMS personnel arrive at the scene.
TRAINING TIP: Give them 3-5 minutes to review them aterial in their guides. The information is duplicated below for your convenience. It is important to provide time for the trainees to “interact” with the participant’s guide as it confirms that the document contains the level of detail they need. In addition, the interaction increases the likelihood that they will reference the document in the future.
FOR PERSONAL USE ONLY

26 Epilepsy Foundation
Outline Content
Review treatment guidelines for generalized tonic clonic - convulsive seizure in progress
PREHOSPITAL TREATMENT: CONVULSIVE SEIZURE IN PROGRESS (GENERALIZED TONIC CLONIC)
All Providers/BLS Response:
l Assure scene safety, utilize body substance isolation (BSI) precautions, and advocate for patient respect, rights and privacy.
l Do not restrain movements. DO NOT FORCIBLY RESTRAIN A PERSON WHO IS HAVING A SEIZURE; THIS INCLUDES USE OF IMMOBILIZATION TECHNIQUES AND DEVICES.
l Assess level of consciousness (LOC).
l Ask witnesses how long the seizure has been under way, precipitating factors, witnessed injury, and if they gave any medication or tried any treatments to stop the seizure prior to your arrival. Determine if they witnessed any blank stare, cry, fall, loss of consciousness, shaking or shaking on one side of the body that progressed to full blown seizure, staring, chewing movements of the mouth, followed by confusion and loss of awareness of environment.
PART 4: Treating Seizures (continued)
FOR PERSONAL USE ONLY
27EMS Training | Trainer’s Guide
PART 4: Treating Seizures (continued)
Outline Content
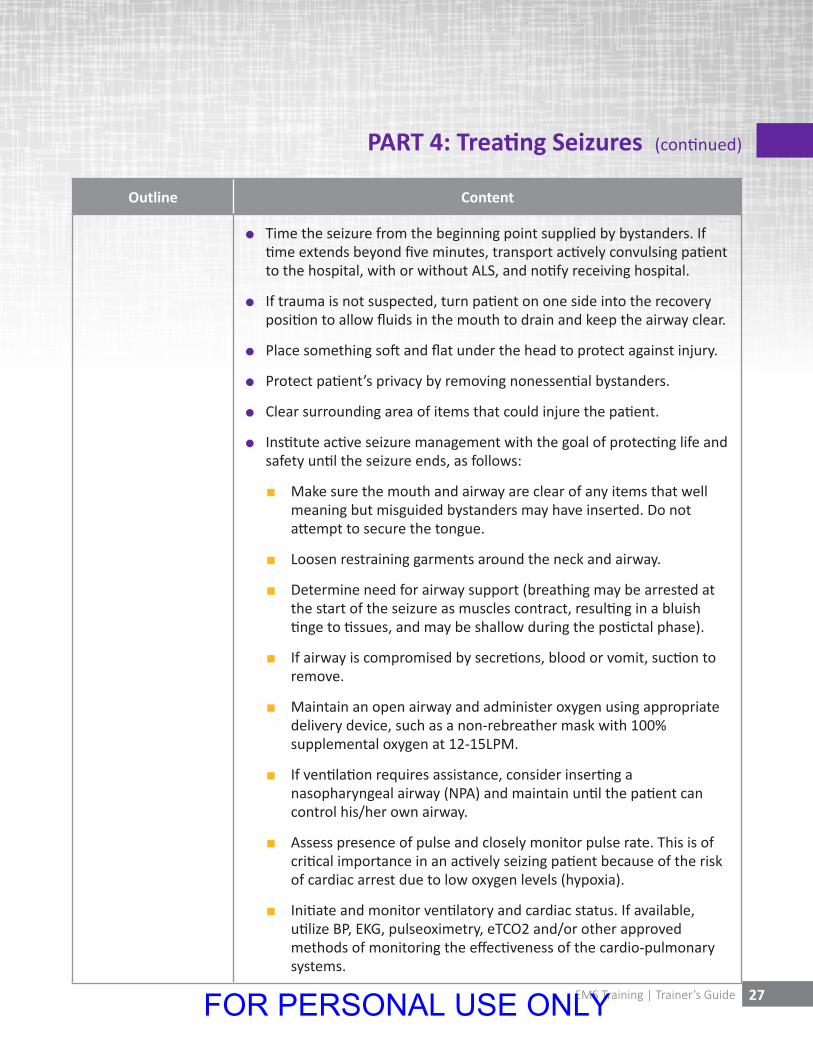
l Time the seizure from the beginning point supplied by bystanders. If time extends beyond five minutes, transport actively convulsing patient to the hospital, with or without ALS, and notify receiving hospital.
l If trauma is not suspected, turn patient on one side into the recovery position to allow fluids in the mouth to drain and keep the airway clear.
l Place something soft and flat under the head to protect against injury.
l Protect patient’s privacy by removing nonessential bystanders.
l Clear surrounding area of items that could injure the patient.
l Institute active seizure management with the goal of protecting life and safety until the seizure ends, as follows:
n Make sure the mouth and airway are clear of any items that well meaning but misguided bystanders may have inserted. Do not attempt to secure the tongue.
n Loosen restraining garments around the neck and airway.
n Determine need for airway support (breathing may be arrested at the start of the seizure as muscles contract, resulting in a bluish tinge to tissues, and may be shallow during the postictal phase).
n If airway is compromised by secretions, blood or vomit, suction to remove.
n Maintain an open airway and administer oxygen using appropriate delivery device, such as a non-rebreather mask with 100% supplemental oxygen at 12-15LPM.
n If ventilation requires assistance, consider inserting a nasopharyngeal airway (NPA) and maintain until the patient can control his/her own airway.
n Assess presence of pulse and closely monitor pulse rate. This is of critical importance in an actively seizing patient because of the risk of cardiac arrest due to low oxygen levels (hypoxia).
n Initiate and monitor ventilatory and cardiac status. If available, utilize BP, EKG, pulseoximetry, eTCO2 and/or other approved methods of monitoring the effectiveness of the cardio-pulmonary systems.
FOR PERSONAL USE ONLY
28 Epilepsy Foundation
Outline Content
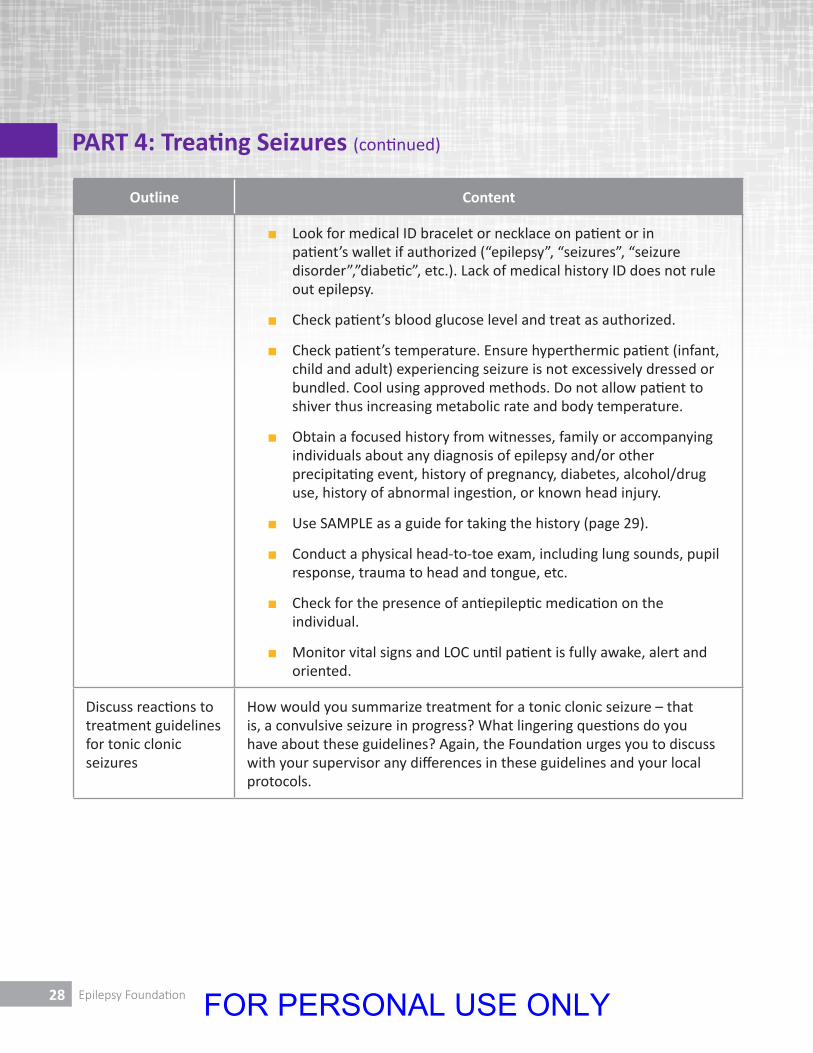
n Look for medical ID bracelet or necklace on patient or in patient’s wallet if authorized (“epilepsy”, “seizures”, “seizure disorder”,”diabetic”, etc.). Lack of medical history ID does not rule out epilepsy.
n Check patient’s blood glucose level and treat as authorized.
n Check patient’s temperature. Ensure hyperthermic patient (infant, child and adult) experiencing seizure is not excessively dressed or bundled. Cool using approved methods. Do not allow patient to shiver thus increasing metabolic rate and body temperature.
n Obtain a focused history from witnesses, family or accompanying individuals about any diagnosis of epilepsy and/or other precipitating event, history of pregnancy, diabetes, alcohol/drug use, history of abnormal ingestion, or known head injury.
n Use SAMPLE as a guide for taking the history (page 29).
n Conduct a physical head-to-toe exam, including lung sounds, pupil response, trauma to head and tongue, etc.
n Check for the presence of antiepileptic medication on the individual.
n Monitor vital signs and LOC until patient is fully awake, alert and oriented.
Discuss reactions to treatment guidelines for tonic clonic seizures
How would you summarize treatment for a tonic clonic seizure – that is, a convulsive seizure in progress? What lingering questions do you have about these guidelines? Again, the Foundation urges you to discuss with your supervisor any differences in these guidelines and your local protocols.
PART 4: Treating Seizures (continued)
FOR PERSONAL USE ONLY

29EMS Training | Trainer’s Guide
PART 4: Treating Seizures (continued)
Outline Content
Highlight ALS circumstances
Note that ALS (Advanced Life Support) techniques and/or rapid transport to the hospital are indicated if ANY of the circumstances noted on pages 17 and 18 is present. Initiate ALS if the person:
l Continues to seize after 5 minutes OR
l Experiences a second seizure shortly after the first OR
l Remains unconscious OR
l After 20 minutes, remains confused OR
l Is pregnant OR
l Has a co-morbid condition such as diabetes OR
l Experienced the seizure while in water OR
l Has been injured during or prior to the seizure or other event OR
l Is experiencing severe headache or other symptoms different from those usually associated with his or her seizures.
Page 23 of the Participant’s Guide lists some of the medications used to stop a seizure:
l Diazepam (Valium)
l Midazolam (Versed)
l Lorazepam (Ativan)
l Diazepam rectal gel (Diastat)
l Epilepsy medications administered intranasally are also available; use per local protocol.
FOR PERSONAL USE ONLY
30 Epilepsy Foundation
Outline Content
Reference the SAMPLE patient history tool
Gather as much information as possible from the postictal patient (who may still be fatigued and somewhat confused), witnesses or family members.
The commonly used mnemonic SAMPLE is an efficient way to gather data – it’s found on page 29 of your participant’s guide:
S signs and symptoms
A allergies
M medications
P pertinent medical history
L last oral intake
E events leading up to the seizure
Signs and Symptoms that may range from postictal confusion to a bleeding tongue bitten during the seizure, to bystander reports of how the seizure progressed, to types of injury if trauma is suspected as a cause. Remember that people often think that a seizure episode lasted longer than it actually did.
Allergies to any substance ingested prior to the seizure, including medications, foods, animals, dyes, or other sources. It is possible that an allergic reaction triggered the seizure.
Medications that the patient is taking. The presence of seizure-preventing medications (see list on page 23 of your guide) or a VNS implant under the chest wall is a strong indication that the seizure is the result of an ongoing epileptic condition. Withdrawal from seizure medications, or an abrupt drop in therapeutic blood level due to missed doses, are common causes of seizures in people with epilepsy. Changes in medications can also cause breakthrough seizures. Seizures may also be caused as a side effect of certain prescription drugs or use of illegal drugs such as cocaine or PCP.
Pertinent medical history which indicates that the patient has a history of epilepsy (seizure disorder), brain injury, hypoglycemia, diabetes, recent illness, other health conditions associated with seizures, or recent changes in his/her daily routine.
PART 4: Treating Seizures (continued)
FOR PERSONAL USE ONLY

31EMS Training | Trainer’s Guide
PART 4: Treating Seizures (continued)
Outline Content
Last oral intake to assess the likelihood of vomiting and aspiration as a complication of the seizure.
Events leading up to the incident which may prove to be important. Have the patient describe, as best s/he can, what s/he was doing before the seizure began, or if s/he cannot remember (not unusual), see if friends or witnesses can provide that information. Exposure to flashing lights, for example, may be a seizure trigger for some people. In young children a sudden rise in fever may trigger what is called a febrile (fever) seizure.
Recap major points
Video Recap (Optional)
Let’s briefly recap a few major points:
TRAINING TIP: If your session is scheduled for 75-90 minutes and you have access to a DVD player and TV for viewing, you may recap the material covered up to this point by showing the video entitled “A Guide to Seizure Management for Emergency Medical Responders” – minutes 5:10 - 9:42.
Otherwise, you may present the recap as a series of statements as noted below. For greater interactivity and to informally test retention, consider actually posing the information below as questions to the group rather than simply sharing statements.
FOR PERSONAL USE ONLY
32 Epilepsy Foundation
PART 4: Treating Seizures (continued)
Outline Content
When responding to someone experiencing a seizure, don’t:
l Give anything by mouth
l Restrain
l Make assumptions about behavior
l Allow the extended seizure
The things you do want to do include:
l Establishing a safe area and privacy
l Check for obvious triggers
l Assess the patient carefully
l Question witnesses
l Establish a timeline
l Conduct a head-to-toe examination
l Determine if hospital transport is necessary
One warning related to the length of the seizure is:
l Transport the patient to the hospital if the seizure lasted more than 5 minutes or another seizure started shortly after the first one.
FOR PERSONAL USE ONLY
33EMS Training | Trainer’s Guide
PART 4: Treating Seizures (continued)
Outline Content
In addition, transport to the hospital is always indicated when:
l The seizure continues for more than 5 minutes OR
l The person experiences another seizure shortly after the first one OR
l The person remains unconscious OR
l The person remains confused after 20 minutes OR
l There is some other medical condition such as diabetes OR
l The seizure happened in water OR
l There has been an injury either before or during the seizure OR
l The person is experiencing headaches or other symptoms not usually associated with his or her seizures.
The postictal phase is:
l The period right after a seizure. The person may still be somewhat confused, feel tired, etc. Full recovery often happens within about 20 minutes. If that doesn’t happen, consider transport to the hospital.
An easy way to remember what to ask regarding the person’s history is:
S - signs and symptoms
A – allergies
M –medications
P – pertinent history
L – last oral intake
E – events leading up to the seizure
FOR PERSONAL USE ONLY
34 Epilepsy Foundation
PART 4: Treating Seizures (continued)
Outline Content
Reference the Participant’s Guide
Before we move to the last portion of this training, take a few minutes to thumb through your Participant’s Guide. You will notice that there are treatment guidelines for various seizure scenarios, beginning with page 15, which we have already looked at in detail.
Page 20 and 21 notes treatment guidelines for a complex partial seizure.
Also pay particular attention to pages 21 and 22 which summarize factors that help determine when transport to the hospital may be indicated.
TRAINING TIP: If time permits, have the participants read and discuss the treatment guidelines for a complex partial seizure (pages 20 and 21 in the Particpant’s Guide). In addition, review the section titled Epilepsy and Seizures: Is Ambulance and Hospital Transport Needed? (pages 20 and 21 of the Participant’s Guide). Otherwise, simply provide a few minutes for the participants to thumb through the guide on their own as noted below.
Take a few minutes now to review the material in the Participant’s Guide. Then we will wrap up the session. In particular, read pages 20 and 21 which details treatment guidelines for a complex partial seizure.
TRAINING TIP: If your session is scheduled for 75-90 minutes and you have access to a DVD player and TV for viewing, you may recap the material covered up to this point by showing the video entitled “A Guide to Seizure Management for Emergency Medical Responders” – minutes 9:42 to 14:20 or the end.
Trainer’s Notes:
FOR PERSONAL USE ONLY
35EMS Training | Trainer’s Guide
PART 5: Wrap-Up
Duration: 5-10 minutes
Outline Content
Ask for Parking Lot questions and/or other urgent issues
We have covered a great deal of content in a short period of time.
Are there any questions that you would like to raise?
TRAINING TIP: Oftentimes, the answers are in the room. An experienced co-facilitator, colleague or even participant may be able to answer a question that you may not be able to fully address.
Please be sure to discuss issues with your supervisor as necessary, or call the Epilepsy Foundation for further information.
Ask for suggestions for improvement (Optional)
What suggestions would you offer to make this training more effective?
TRAINING TIP: You may also use a more formal evaluation form.
Thank the participants
Thank you for your time, attention, and participation. Most importantly, thank you for dedication to offering the best possible response for people who suffer from seizures.
Trainer’s Notes:
FOR PERSONAL USE ONLY
36 Epilepsy Foundation
Trainer’s Notes:
FOR PERSONAL USE ONLY
37EMS Training | Trainer’s Guide
Trainer’s Notes:
FOR PERSONAL USE ONLY
38 Epilepsy Foundation
Trainer’s Notes:
FOR PERSONAL USE ONLY
FOR PERSONAL USE ONLY
This Publication was made possible with funding from the Center for Disease Control (CDC) and Prevention under Cooperative agreement
number 1U58DP003832-04. Its contents are solely the responsibility of the authors and do not necessarily represent theofficial views of the CDC.
epilepsy.com800-332-1000
Reprinted 09/2015603EMS
FOR PERSONAL USE ONLY