empowerment for women and girls and the millennium ... · empowerment for women and girls and the...
TRANSCRIPT
Empowerment for women and girls and the Millennium Development Goals
Dr. Arletty Pinel – [email protected] Asian Women Parliamentarians’ and Ministers’ ConferenceBeijing, 27 November 2007

Some facts about the region
Over 60% of the world's population live in Asia and the Pacific region
6 out of the world's 10 most populous countries are in Asia: Bangladesh, China, India, Indonesia, Japan and Pakistan
Over the past 20 years, Asia has shown a rapid decline in population growth rates and fertility levels
However because of Asia's huge population base, half the world's annual population growth occurs in Asia
Population and Development
8.6 million people are living with HIV or AIDS in Asia, and about 1 million people become newly infected each year.
630,000 persons died from AIDS-related illnesses in 2006 in the region
The number of people receiving antiretroviral therapy (ARV) has increased more than three-fold since 2003; this represents about 16% of the total number of people in need of ARV in Asia.
HIV and AIDS in Asia
Gender-based violence is a critical issue in Asia
Early marriageHuman trafficking Physical and sexual violenceForced abortion, infanticide and domestic violence
associated with boy preference
Despite high prevalence of gender-based violence, physical, mental and social care system is still lacking.
Gender-Based Violence
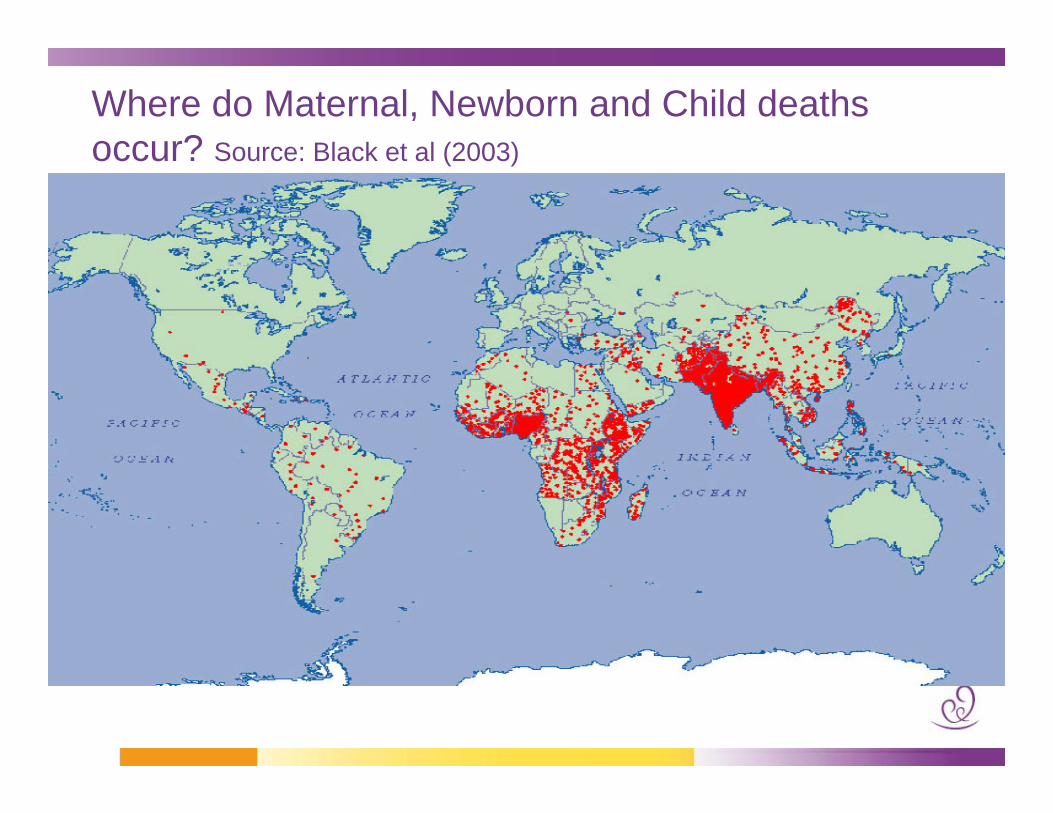
Where do Maternal, Newborn and Child deaths occur? Source: Black et al (2003)
Maternal mortality: an indicator of exclusion and disempowerment
The Cost of Giving Birth
Over 300 million women in developing countries suffer from complications of pregnancy and delivery
536,000 die each year – one woman every minute; 11 million deaths since the launch of the Safe Motherhood Initiative in 1987
8.5 million deaths per year among mothers, newborns and stillborn– HIV causes 2.9 million deaths per year
For every woman who dies, between 20 and 50 experience a long orshort-term morbidity
At least 2 million women living with obstetric fistula and up to 100,000 new cases each year
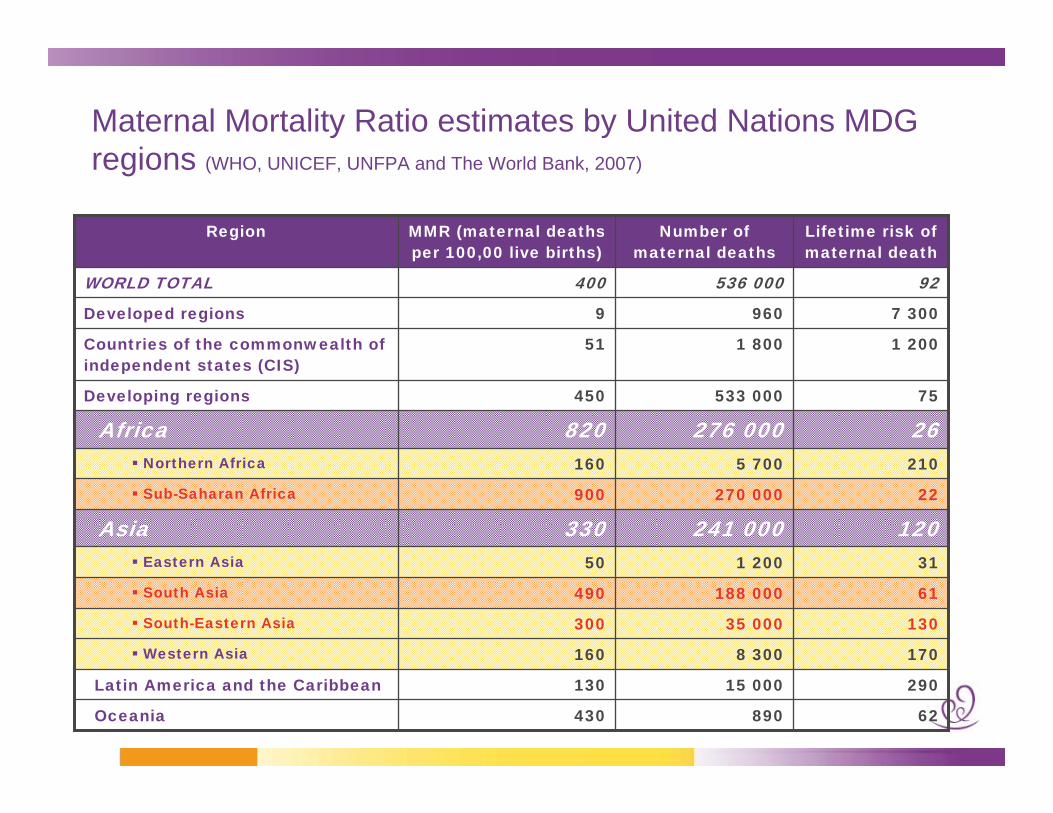
Maternal Mortality Ratio estimates by United Nations MDG regions (WHO, UNICEF, UNFPA and The World Bank, 2007)
92536 000400WORLD TOTAL
2105 700160Northern Africa
26276 000820Africa
13035 000300South-Eastern Asia
1708 300160Western Asia
61188 000490South Asia
62890430Oceania
29015 000130Latin America and the Caribbean
311 20050Eastern Asia
120241 000330Asia22270 000900Sub-Saharan Africa
75533 000450Developing regions
1 2001 80051Countries of the commonwealth of independent states (CIS)
7 3009609Developed regions
Lifetime risk of maternal death
Number of maternal deaths
MMR (maternal deaths per 100,00 live births)
Region
Vast inequities
Greatest disparity of any health indicator between industrialized and developing countries
Lifetime risk:1 in 16 in sub-Saharan Africa
1 in 46 in South-central Asia
1 in 2800 in more developed countries
Disparities within countries between the poorest and wealthiest women
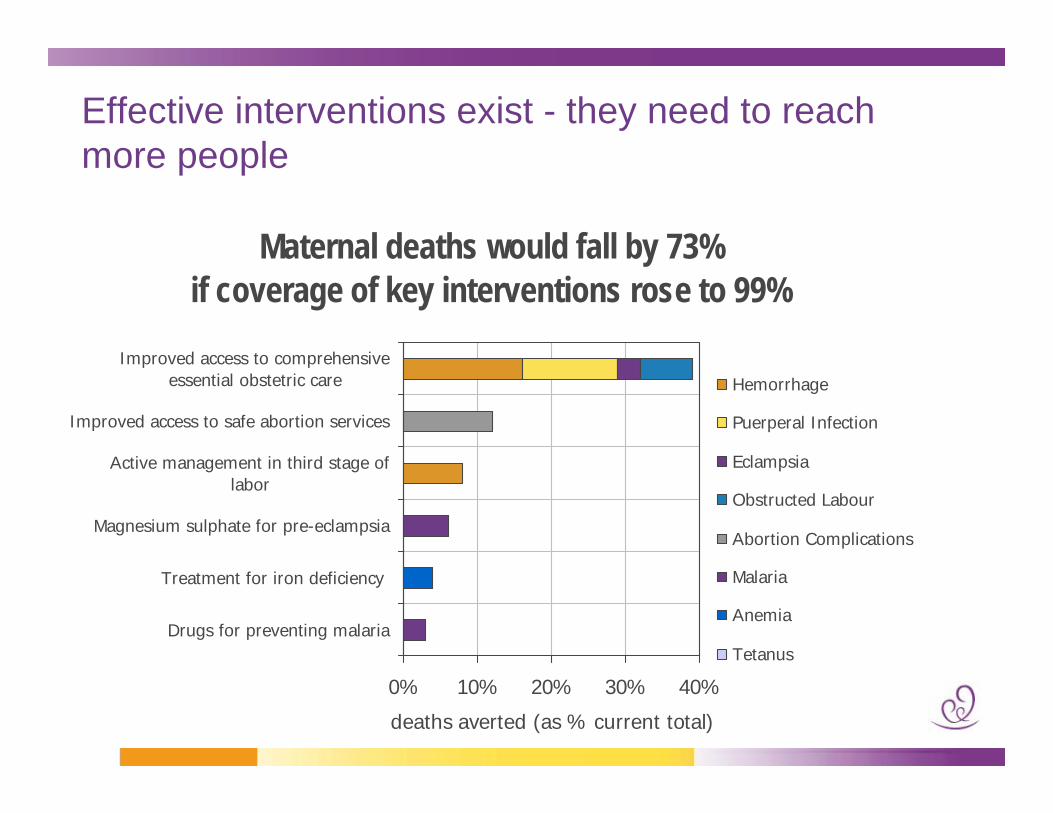
Maternal deaths would fall by 73% if coverage of key interventions rose to 99%
0% 10% 20% 30% 40%
Drugs for preventing malaria
Treatment for iron deficiency
Magnesium sulphate for pre-eclampsia
Active management in third stage oflabor
Improved access to safe abortion services
Improved access to comprehensiveessential obstetric care
deaths averted (as % current total)
Hemorrhage
Puerperal Infection
Eclampsia
Obstructed Labour
Abortion Complications
Malaria
Anemia
Tetanus
Effective interventions exist - they need to reach more people
So it’s an issue of inequity… women die because they are poor
Strategy for Reduction of Maternal Mortality and Morbidity
1. All women have access to contraception to avoid unwanted pregnancies and to plan their families
2. All pregnant women have access to skilled care at the time of birth
3. All those with complications have timely access to quality emergency obstetric care
Family planning
200 million women with unmet need for family planningFamily planning estimated to reduce maternal mortality by 25 to 30%Based on 2000 estimates, 90% of abortion-related and 20% of obstetric related deaths could have been averted if needs for family planning were met
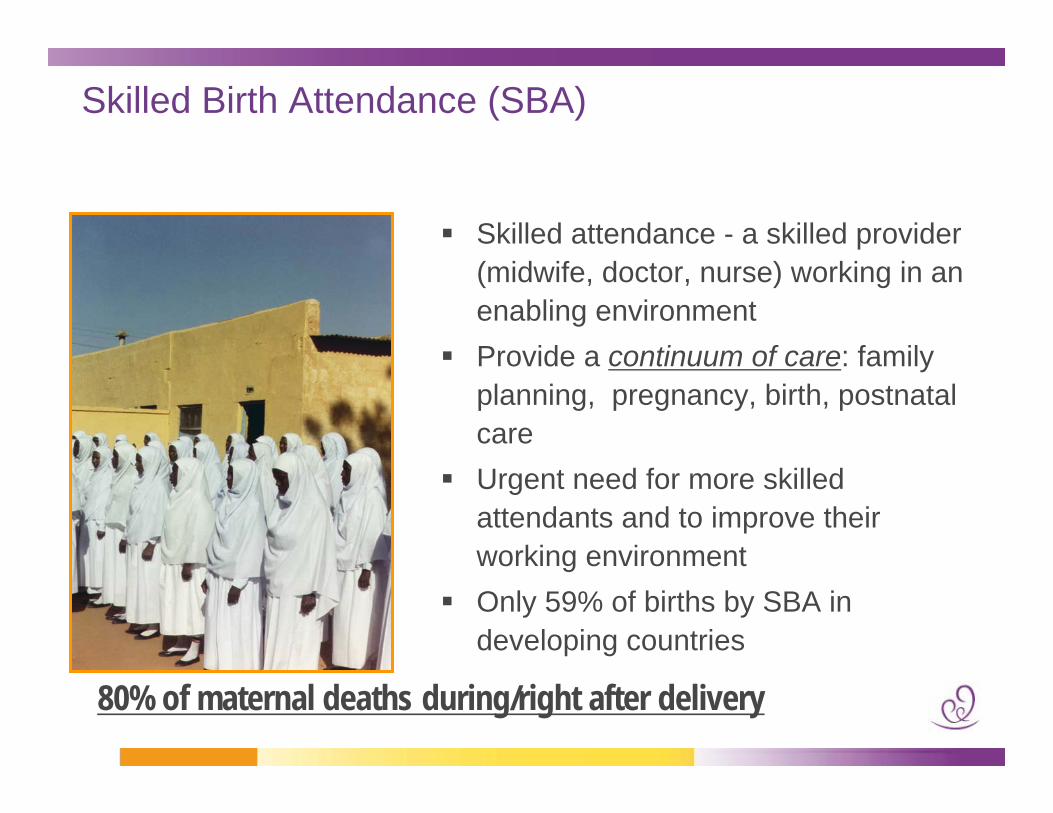
Skilled Birth Attendance (SBA)
Skilled attendance - a skilled provider (midwife, doctor, nurse) working in an enabling environmentProvide a continuum of care: family planning, pregnancy, birth, postnatal careUrgent need for more skilled attendants and to improve their working environmentOnly 59% of births by SBA in developing countries
80% of maternal deaths during/right after delivery
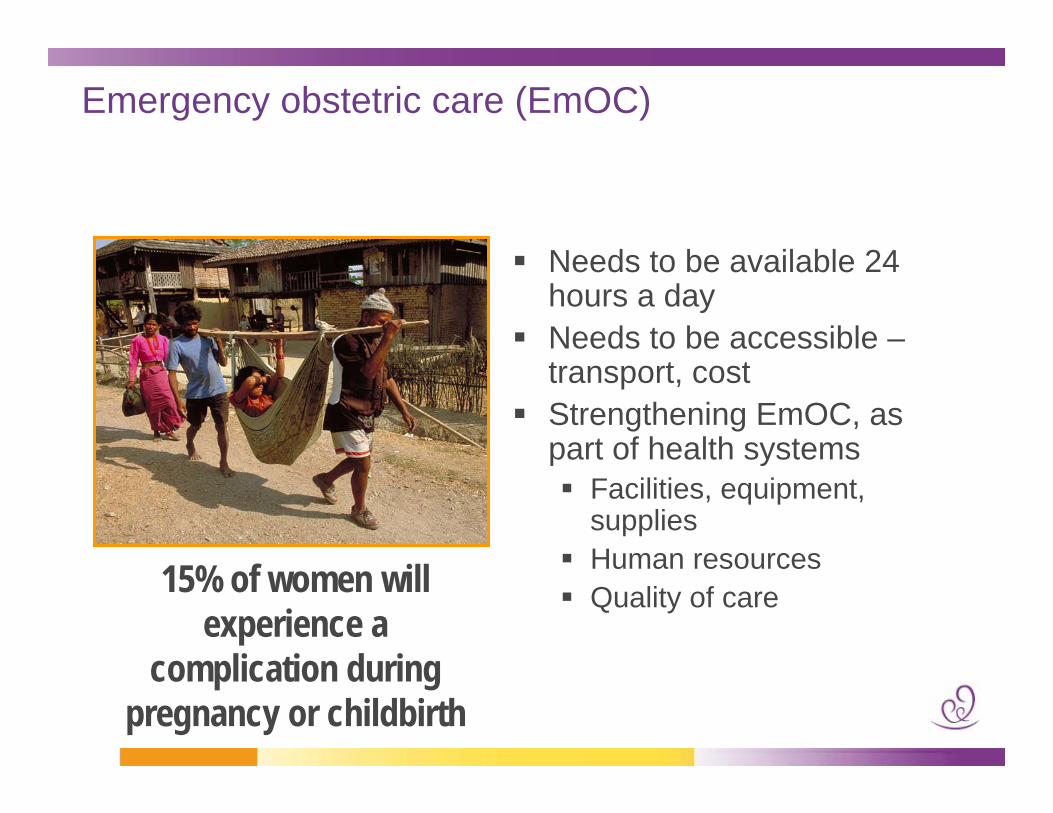
Emergency obstetric care (EmOC)
Needs to be available 24 hours a dayNeeds to be accessible –transport, costStrengthening EmOC, as part of health systems
Facilities, equipment, suppliesHuman resourcesQuality of care15% of women will
experience a complication during
pregnancy or childbirth
But it is also about education and women’s empowerment
Gender based violence is another important cause of maternal mortalityMidwives are a key health workforce to fight maternal, newborn and child mortality – but midwives are usually women and suffer the same gender biases and lack of protectionCountries with high maternal mortality usually have low girls enrollment in schools and fewer midwives (skilled birth attendants) – if girls cannot go to school and finish their secondary education, how can they become university trained midwives of nurses or doctors?

Improvements can happen…
Rapid gains are possible
"…maternal mortality can be halved in
developing countries every 7 to 10 years, …
regardless of income level and growth rate"
Source: World Bank (2003)
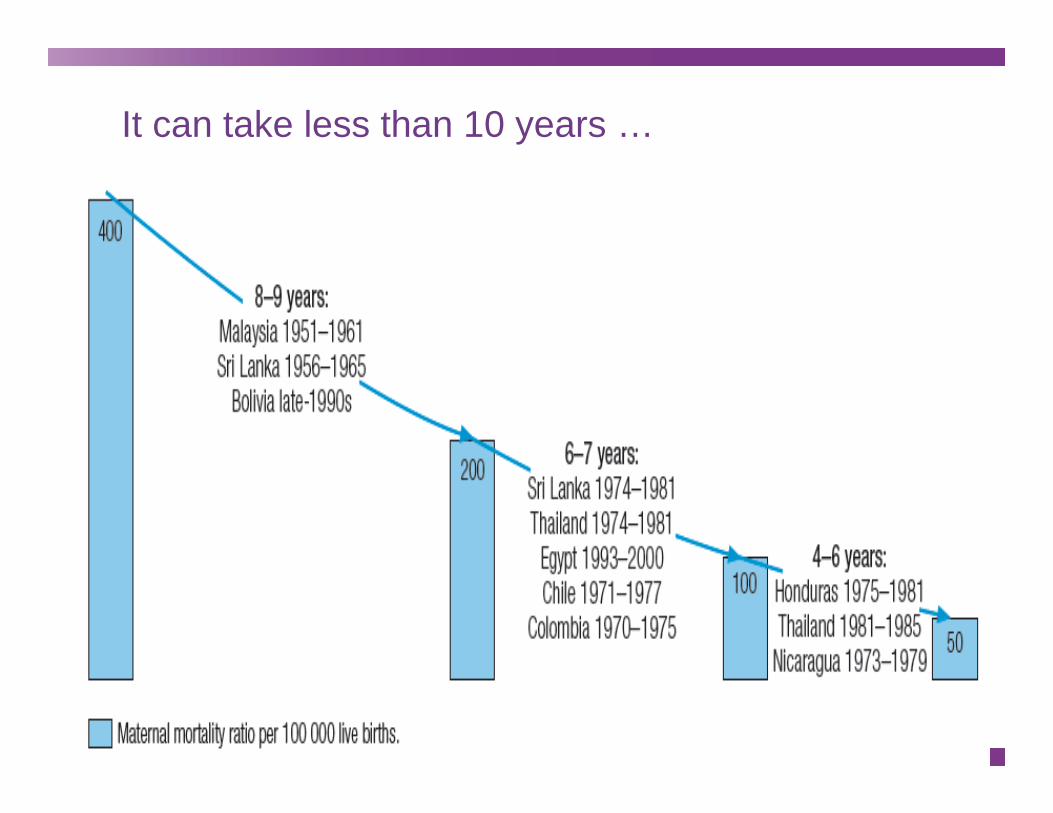
It can take less than 10 years …

Country example: Addressing obstetric fistula – a common complication of childbirth -- in Bangladesh
Over 900 women with obstetric fistula treated since 2003
2000 skilled birth attendants trained between 2002 and 2006
73 doctors & 60 nurses trained in fistula care since 2003
National fistula centre established, to be regional Centre of Excellence
Reintegration centre established
Outreach camps held at 7 regional medical college hospitals
Maternal mortality recognized as one of the 7 Millennium Development Goals (MDGs)
Goal 1: Eradicate extreme poverty and hunger
Goal 2: Achieve universal primary education
Goal 3: Promote gender equality and empower women
Goal 4: Reduce child mortality
Goal 5: Improve maternal healthGoal 6: Combat HIV/AIDS, malaria and other diseases
Goal 7: Ensure environmental sustainability
MDG 5: Improve Maternal Health
Target: Reduce maternal mortality ratios by 75% from 1990 levels
Indicators:Maternal mortality ratioProportion of births attended by skilled personnel
Target: Universal access to reproductive healthIndicators (still to be endorsed):
Age-specific fertility rate for women aged 15 to 19
Contraceptive prevalence rate (move from MDG 6)Unmet need for family planningProportion of women attending antenatal care (1 and 4+)

Global initiatives to address maternal, newborn and child mortality
The Partnership for Maternal, Newborn and Child Health
Launched in September 2005 as a global health partnership merging the world's three leading maternal, newborn and child health alliances:
Partnership for Safe Motherhood and Newborn Health, hosted by WHO and established in 2004, with linkages to the 1987 Safe Motherhood InitiativeHealthy Newborn Partnership (2000), based at Save
the ChildrenChild Survival Partnership (2004), hosted by UNICEF
Focus on mothers and children to support efforts toward achieving MDGs 4 and 5More than 180 partner organizations

Global Campaign for the Health MDGs
Launched jointly by the United Kingdom &
Norway, and joined by Canada, France and
Germany to build high level political thrust
around all health MDGs - and in particular
MDGs 4 & 5

The Global Campaign for the Health MDGs –the International Health Partnership (IHP)
Led by the United Kingdom: Accelerate action to
scale up coverage and use of health services
(through public, private or non-governmental
channels); deliver improved outcomes against
the health related MDGs and universal access
commitments. No new institutions or funding
streams.
The Global Campaign for the Health MDGs –what are the possible consequences for MNCH?
Led by Norway:More action:
Do more for women and children. Development of a set of new initiatives, most of which aim to accelerate progress on MDGs 4 & 5 (“Deliver Now for Women and Children”, “Catalytic Initiative”, “Global Network of Leaders ”, “Performance Based Financing”, “Providing for Health Initiative”)
Invest more:More resources for MNCH health, at national and global levels will be raisedInnovative sources of financing will be soughtInvest in a more effective way to produce results
The Global Campaign for the Health MDGs –The Initiative to Save a Million Lives
Led by Canada in partnership with UNICEF, The Bill & Melinda Gates Foundation, The World Bank and othersWill strengthen health systems by training frontline health workers and delivering affordable healthcare services directly to local communities.Will deliver basic, cost-effective and life-saving health services to mothers and children in countries where the needs are greatest
The Global Campaign for the Health MDGs –Deliver Now for Women + Children advocacy drive
Called by the Prime Minister of Norway with support from others to build a high level political thrust and mobilization of resources to facilitate the attainment of MDGs 4 & 5 Launched in New York Sept 26, 2007Coordinated by the Partnership for Maternal, Newborn and Child HealthPurpose:
Mobilizing public support and stimulating positive behaviors that reduce maternal, newborn and child deaths;Generating political support for key messages and actions to improve maternal, newborn and child health;Raising significant new money for maternal, newborn and child health as an integrated issue, in line with country-led efforts to improve health systems and achieve MDGs 4 and 5.
Deliver Now for Women + Children: Launch (I)
Norway pledges $1 billion for MDGs 4 & 5 at the Clinton Global Initiative annual meeting in New York on Sept. 26, 2007.
Deliver Now for Women + Children: Launch (II)
Public Rally for Deliver Now in Bryant Park, NY:Grammy winner Chaka Khan (right) performs.
Deliver Now for Women + Children: Launch (III)
Celebrity endorsements for Deliver Now:Nicole Kidman, Chaka Khan, Liya Kebede, Ricki Lake

Deliver Now for Women + Children: Launch (IV)
UN leaders, heads of state, and global activists at the Deliver Now launch on Sept. 26 in New York
Deliver Now for Women + Children: Web
Asking for civil society support: www.delivernow.org

The icon and its meaning: women are powerful

The icon can be “dressed” as it travels the world
Art for Health – Empowering Women
Contemporary art, by Italian artist ElisabettaFarina, funded by WHO Uses art to increase awareness about reproductive health issuesPromotes action towards the improvement of women’s sexual and reproductive health conditions around the world
Art for Health – Empowering WomenDifference in reproductive health status is the biggest social injustice of our timeThe paintings send positive messages for greater gender equityEncourage the viewer to see this women as willing and capable partners to advance women's health
Stara Thomas, Singer, Tanzania
Dr Margaret Chan, Director-General, World Health Organization
Art for Health – Empowering WomenExhibits around the world:
June 2007- Rome (Italy)October 2007- London (UK), Cape Town (South Africa)Jan-Mar 2008: tour around the USApril 2008: Auction by Christie's
Countdown to 2015
The Countdown to 2015 group was established to implement an overall mechanism for accountability, recognize accomplishments in child survival at the country-level, and convene a series of meetings every two years to evaluate progress
In 2008, the Countdown to 2015 will include MDGs4 and 5 for the first time
It will take place in April parallel to the 118th Assembly of the Inter-Parliamentary Union (IPU) in Cape Town, South Africa
What will the Asian women parliamentarians and ministers do to join the growing global awareness that ending maternal mortality is
also about demonstrating the benefits of healthy, educated women to the future of
humanity?
