embryo fragmentation as a determinant of blastocyst development in vitro and pregnancy outcomes...
TRANSCRIPT
American Journal of Obstetrics and Gynecology (2005) 192, 2014–20
www.ajog.org
Embryo fragmentation as a determinant of blastocystdevelopment in vitro and pregnancy outcomes followingembryo transfer
Bronte A. Stone, PhD, Jody Greene, Joyce M. Vargyas, MD, Guy E. Ringler, MD,Richard P. Marrs, MD*
California Fertility Partners and Institute for Fertility Research, Los Angeles, CA
Received for publication July 14, 2004; revised October 13, 2004; accepted February 1, 2005
KEY WORDSEmbryo
fragmentation
Blastocystdevelopment
Pregnancy rates
Embryo transfer
Objective(s): To determine how the type of embryo fragmentation on day 3 affects progression
of human embryos to blastocyst and pregnancy rates following embryo transfer.Study design: Retrospective analysis of all in vitro fertilization cycles in patients%40 years of ageor younger from January 2002 through December 2003, during which time surplus day 3 embryos
were transferred to blastocyst medium for extended culture. All embryos (4 cells or more) notsuitable for transfer or freezing 72 hours following in vitro fertilization were placed intomicrodroplets (60 mL) of blastocyst medium and cultured for an additional 48 hours to assessblastocyst formation. Normal blastocyst development required blastulation, a visible inner-cell
mass, trophectoderm cells covering 60% of the inner zona surface and thinning of the zona. Therate of blastocyst formation was then analyzed (c2 and analysis of variance) against the type offragmentation 72 hours after insemination. Pregnancy outcomes were analyzed with respect to the
pattern of fragmentation in cleaving embryos transferred after 3 days of culture.Results: A total of 1566 embryos were cultured beyond day 3 of development of which 229(14.6%) reached the blastocyst stage and were frozen. Embryos exhibiting no fragmentation or
type I fragmentation had significantly higher blastocyst development rates (27.9% and 19.9%)than embryos with type 2 or 3 fragmentation (13.9 and 8.8, respectively; P ! .001). No embryoswith type 4 or 5 fragmentation progressed to blastocyst. The average type of fragmentation intransferred embryos correlated with pregnancy outcome and embryo age.
Conclusion(s): More pervasive embryo fragmentation was associated with a decreasing rate ofblastocyst development with day 3 embryos. To the extent that blastocyst development rates ofday 3 embryos is an index of embryo viability, our findings establish that careful classification of
the type of embryo fragmentation is important in selection of day 3 embryos for transfer. Recentreports of associations among embryo fragmentation, aneuploidy, apoptosis, and patient agesupport these conclusions.
� 2005 Elsevier Inc. All rights reserved.
Presented at the 71st Annual Meeting of the Pacific Coast Obstetrical and Gynecological Society, October 19-24, 2004, Phoenix, Arizona.
* Reprint requests: Richard P. Marrs, MD, 11818 Wilshire Boulevard, Suite #300, Los Angeles, CA 90025.
E-mail: [email protected]
0002-9378/$ - see front matter � 2005 Elsevier Inc. All rights reserved.
doi:10.1016/j.ajog.2005.02.048

Stone et al 2015
Our laboratory adopts a standard grading system forday 3 embryos, the elements of which include blasto-mere number, blastomere size and symmetry, membranedefinition, cytoplasmic clarity, cell compaction, andfragmentation. This grading system is weighted towardblastomere number (usually representing 50% of thetotal possible embryo grade), in accord with thepublished evidence that this is an important determinantof embryo implantation.1,2 Using this system, thedifference in average grade of all embryos transferredpreceding a pregnancy (4.6) has historically remainedhigher than the respective average value for transferspreceding a failed conception (4.0; P ! .001), but thedifference in these average grades is relatively low, andwe remain constantly faced with discordant pregnancyoutcomes (ie, ‘‘perfect’’ embryos transferred with nopregnancies and poor-grade embryos yielding highimplantation rates).
Anucleate fragmentation in human embryos has beenassociated with a lower implantation potential.3,4 Accu-mulating data from preimplantation genetic diagnosishas also established a low likelihood of implantation ofaneuploid embryos and a very close association betweenthe amount of embryo fragmentation and chromosomeanomalies.5 The collective findings infer a close associ-ation between embryo fragmentation and implantationand have prompted us to review the fragmentationcomponent of our embryo grading with the view todetermining whether assessments of fragmentationshould represent more or less of the overall embryograde. Fragmentation is currently scored relative to theamount (0, 0% to 5%, 5% to 50%, more than 50%) andtype, based on criteria detailed previously,3 including:
� Type 1, minimal volume of the embryo affected (lessthan 5%), and fragments are typically associatedwith only 1 blastomere.
� Type 2, localized fragments predominantly occupy-ing the perivitelline space and representing 5% to50% of the embryonic volume.
� Type 3, small fragments distributed throughout theembryonic mass and usually representing 5% to 50%of the embryonic volume.
� Type 4, large fragments distributed throughout theembryonic mass and associated with pleiotropicblastomeres. Usually 50% or more of the embryonicvolume is affected.
� Type 5, fragments appear necrotic (grainy/darkcytoplasm), with granularity and cytoplasmic con-traction of neighboring blastomeres. More than 50%of the embryonic volume is affected.
Although the proportion of embryonic volume con-taining fragments currently represents up to 17% of thetotal embryo grade, the type of fragmentation has beendocumented but not factored into the grading system.This retrospective study therefore examines the associ-
ation between pregnancy outcomes and the type (asopposed to amount) of fragmentation in transferredembryos.
Material and methods
Study design
To project the relative lethality of the types of fragmen-tation on preimplantation embryonic development, weanalyzed relationships between the type of embryofragmentation on day 3 of embryo culture and theprogression to blastocyst of all embryos 4 cells or greaterthat were not transferred or frozen by day 3 of culture.Unless stipulated otherwise, the data presented in thisstudy were drawn only from women in whom embryoswere transferred were aged 40 years or younger and fromJanuary 2002 through December 2003, during whichtime the same blastocyst culture medium (Irvine Scien-tific, Irvine, Calif) had been in use. No other restrictionon patient or embryo parameters was applied. Noinstitutional review board approval was obtained be-cause of the observational nature of this retrospectivedata analysis.
Embryo transfer data from the same time period wereanalyzed to establish the likely relative significance of the(average) fragmentation type on pregnancy outcome. Inour comparisons against iterations of fragmentationtype, the statistical manipulations of the type score (eg,average) have been performed solely to rank groups ofobservations relative to (average) fragmentation type (ie,the score assigned to the type [0 to 5] is subjective and notcontinuously variable), so the score is not otherwiseamenable to parametric statistical analysis. Initially,therefore, data on scores of fragmentation type wereanalyzed to verify (determine) that the assigned type (0 to5) was aligned with embryo viability. That is, that anembryo with no fragmentation had a higher likelihood ofimplanting than an embryo with type 1 fragmentation,which in turn had a higher likelihood of implanting thanan embryo with type 2 fragmentation, and so on.Average values of the fragmentation type were thenreviewed in comparison with other established determi-nants of pregnancy following embryo transfer (embryoage, number of embryos transferred, blastomere number,embryo grade), and compared between groups of pa-tients who conceived and those who did not.
Results
Development of embryos to blastocyst
Table I summarizes outcomes of culture of all surplusday 3 embryos (4 cells or more) following 48 hours ofculture in blastocyst medium (Irvine Scientific) between
2016 Stone et al
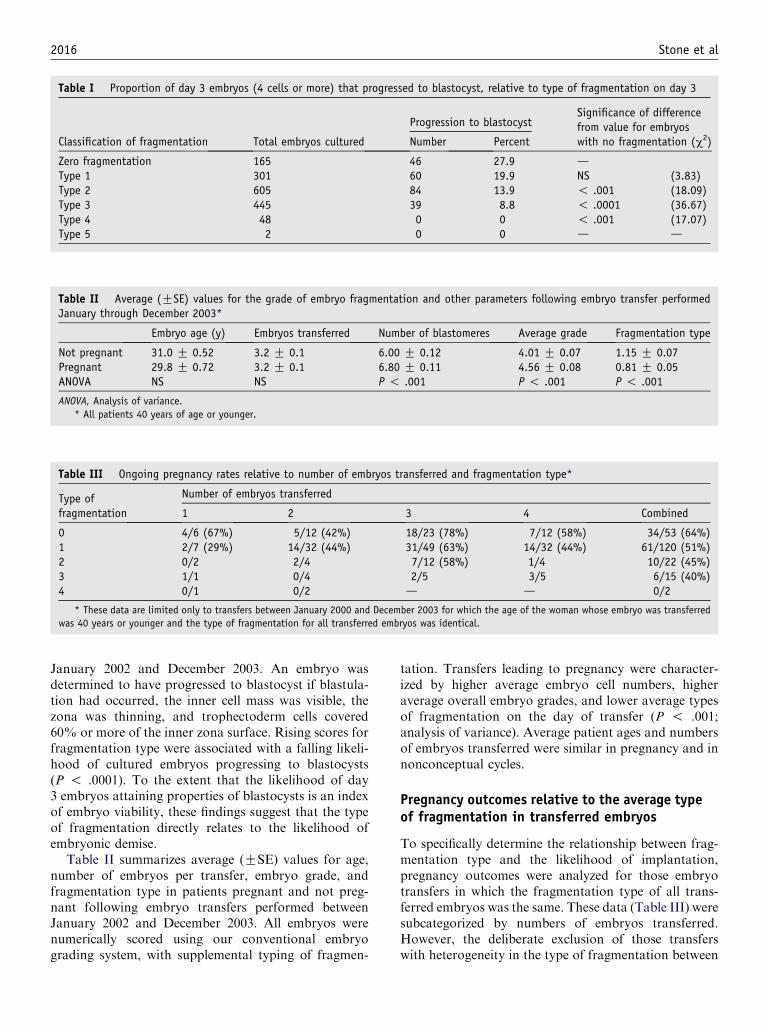
Table II Average (GSE) values for the grade of embryo fragmentation and other parameters following embryo transfer performedJanuary through December 2003*
Embryo age (y) Embryos transferred Number of blastomeres Average grade Fragmentation type
Not pregnant 31.0 G 0.52 3.2 G 0.1 6.00 G 0.12 4.01 G 0.07 1.15 G 0.07Pregnant 29.8 G 0.72 3.2 G 0.1 6.80 G 0.11 4.56 G 0.08 0.81 G 0.05ANOVA NS NS P ! .001 P ! .001 P ! .001
ANOVA, Analysis of variance.
* All patients 40 years of age or younger.
Table III Ongoing pregnancy rates relative to number of embryos transferred and fragmentation type*
Type offragmentation
Number of embryos transferred
1 2 3 4 Combined
0 4/6 (67%) 5/12 (42%) 18/23 (78%) 7/12 (58%) 34/53 (64%)1 2/7 (29%) 14/32 (44%) 31/49 (63%) 14/32 (44%) 61/120 (51%)2 0/2 2/4 7/12 (58%) 1/4 10/22 (45%)3 1/1 0/4 2/5 3/5 6/15 (40%)4 0/1 0/2 d d 0/2
* These data are limited only to transfers between January 2000 and December 2003 for which the age of the woman whose embryo was transferred
was 40 years or younger and the type of fragmentation for all transferred embryos was identical.
Table I Proportion of day 3 embryos (4 cells or more) that progressed to blastocyst, relative to type of fragmentation on day 3
Classification of fragmentation Total embryos cultured
Progression to blastocystSignificance of differencefrom value for embryoswith no fragmentation (c2)Number Percent
Zero fragmentation 165 46 27.9 dType 1 301 60 19.9 NS (3.83)Type 2 605 84 13.9 ! .001 (18.09)Type 3 445 39 8.8 ! .0001 (36.67)Type 4 48 0 0 ! .001 (17.07)Type 5 2 0 0 d d
January 2002 and December 2003. An embryo wasdetermined to have progressed to blastocyst if blastula-tion had occurred, the inner cell mass was visible, thezona was thinning, and trophectoderm cells covered60% or more of the inner zona surface. Rising scores forfragmentation type were associated with a falling likeli-hood of cultured embryos progressing to blastocysts(P ! .0001). To the extent that the likelihood of day3 embryos attaining properties of blastocysts is an indexof embryo viability, these findings suggest that the typeof fragmentation directly relates to the likelihood ofembryonic demise.
Table II summarizes average (GSE) values for age,number of embryos per transfer, embryo grade, andfragmentation type in patients pregnant and not preg-nant following embryo transfers performed betweenJanuary 2002 and December 2003. All embryos werenumerically scored using our conventional embryograding system, with supplemental typing of fragmen-
tation. Transfers leading to pregnancy were character-ized by higher average embryo cell numbers, higheraverage overall embryo grades, and lower average typesof fragmentation on the day of transfer (P ! .001;analysis of variance). Average patient ages and numbersof embryos transferred were similar in pregnancy and innonconceptual cycles.
Pregnancy outcomes relative to the average typeof fragmentation in transferred embryos
To specifically determine the relationship between frag-mentation type and the likelihood of implantation,pregnancy outcomes were analyzed for those embryotransfers in which the fragmentation type of all trans-ferred embryos was the same. These data (Table III) weresubcategorized by numbers of embryos transferred.However, the deliberate exclusion of those transferswith heterogeneity in the type of fragmentation between
Stone et al 2017
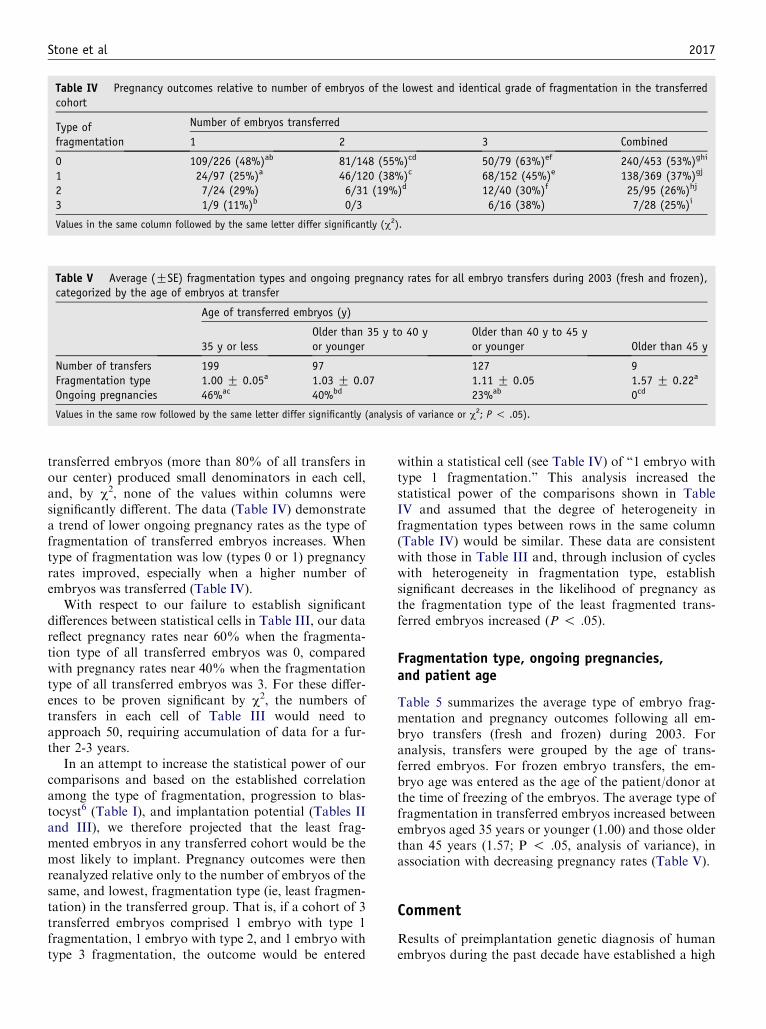
Table IV Pregnancy outcomes relative to number of embryos of the lowest and identical grade of fragmentation in the transferredcohort
Type offragmentation
Number of embryos transferred
1 2 3 Combined
0 109/226 (48%)ab 81/148 (55%)cd 50/79 (63%)ef 240/453 (53%)ghi
1 24/97 (25%)a 46/120 (38%)c 68/152 (45%)e 138/369 (37%)gj
2 7/24 (29%) 6/31 (19%)d 12/40 (30%)f 25/95 (26%)hj
3 1/9 (11%)b 0/3 6/16 (38%) 7/28 (25%)i
Values in the same column followed by the same letter differ significantly (c2).
Table V Average (GSE) fragmentation types and ongoing pregnancy rates for all embryo transfers during 2003 (fresh and frozen),categorized by the age of embryos at transfer
Age of transferred embryos (y)
35 y or lessOlder than 35 y to 40 yor younger
Older than 40 y to 45 yor younger Older than 45 y
Number of transfers 199 97 127 9Fragmentation type 1.00 G 0.05a 1.03 G 0.07 1.11 G 0.05 1.57 G 0.22a
Ongoing pregnancies 46%ac 40%bd 23%ab 0cd
Values in the same row followed by the same letter differ significantly (analysis of variance or c2; P ! .05).
transferred embryos (more than 80% of all transfers inour center) produced small denominators in each cell,and, by c2, none of the values within columns weresignificantly different. The data (Table IV) demonstratea trend of lower ongoing pregnancy rates as the type offragmentation of transferred embryos increases. Whentype of fragmentation was low (types 0 or 1) pregnancyrates improved, especially when a higher number ofembryos was transferred (Table IV).
With respect to our failure to establish significantdifferences between statistical cells in Table III, our datareflect pregnancy rates near 60% when the fragmenta-tion type of all transferred embryos was 0, comparedwith pregnancy rates near 40% when the fragmentationtype of all transferred embryos was 3. For these differ-ences to be proven significant by c2, the numbers oftransfers in each cell of Table III would need toapproach 50, requiring accumulation of data for a fur-ther 2-3 years.
In an attempt to increase the statistical power of ourcomparisons and based on the established correlationamong the type of fragmentation, progression to blas-tocyst6 (Table I), and implantation potential (Tables IIand III), we therefore projected that the least frag-mented embryos in any transferred cohort would be themost likely to implant. Pregnancy outcomes were thenreanalyzed relative only to the number of embryos of thesame, and lowest, fragmentation type (ie, least fragmen-tation) in the transferred group. That is, if a cohort of 3transferred embryos comprised 1 embryo with type 1fragmentation, 1 embryo with type 2, and 1 embryo withtype 3 fragmentation, the outcome would be entered
within a statistical cell (see Table IV) of ‘‘1 embryo withtype 1 fragmentation.’’ This analysis increased thestatistical power of the comparisons shown in TableIV and assumed that the degree of heterogeneity infragmentation types between rows in the same column(Table IV) would be similar. These data are consistentwith those in Table III and, through inclusion of cycleswith heterogeneity in fragmentation type, establishsignificant decreases in the likelihood of pregnancy asthe fragmentation type of the least fragmented trans-ferred embryos increased (P ! .05).
Fragmentation type, ongoing pregnancies,and patient age
Table 5 summarizes the average type of embryo frag-mentation and pregnancy outcomes following all em-bryo transfers (fresh and frozen) during 2003. Foranalysis, transfers were grouped by the age of trans-ferred embryos. For frozen embryo transfers, the em-bryo age was entered as the age of the patient/donor atthe time of freezing of the embryos. The average type offragmentation in transferred embryos increased betweenembryos aged 35 years or younger (1.00) and those olderthan 45 years (1.57; P ! .05, analysis of variance), inassociation with decreasing pregnancy rates (Table V).
Comment
Results of preimplantation genetic diagnosis of humanembryos during the past decade have established a high

2018 Stone et al
incidence of chromosomal abnormality, increasing fromprojected values near 40% at age 40 years to values near80% to 90% at age 45 years. The same literature hasestablished a high incidence of mosaicism for a range oftarget chromosomes.7,8 Furthermore, aneuploidy in up toapproximately 50% of the blastomeres in a day 3 embryocan be tolerated with resultant normal embryonic pro-gression.7 High risks of chromosomal misdiagnosis anddisposal of embryos with normal developmental poten-tial based on analysis of only 1 or 2 biopsied blastomeresare, therefore, self-evident.8
In this respect, elements of embryo morphology andcleavage kinetics have been independently related tochromosomal characteristics.9 Approximately 40% offragmented human embryos are aneuploid (30% to50%),5,8 the amount of fragmentation on the third dayof culture being directly associated with an increase inchromosomal abnormality.8 Ziebe et al8 also establishedthat the incidence of aneuploidy in human pre-embryoswas more closely associated with the degree of fragmen-tation than with blastomere size, cleavage rate (blasto-mere number), clarity of the blastomere cytoplasm, orearly cleavage (cleaved embryos 26 hours after insemi-nation). In the study by Ziebe et al,8 the proportion ofchromosomally normal embryos in the group selectedon the basis of minimal-absent fragmentation was 68%,compared with 55% in the unselected embryo group.
With respect to fragmentation and aneuploidy, ourfindings established more pervasive fragmentation inembryos from older patients (P ! .05; Table V), inassociation with lower pregnancy rates (Table V) andthe well-established increase in embryo aneuploidy withadvancing maternal age.9
Pleiomorphic fragmentation appears in themajority ofcultured human embryos. Certain common patterns offragmentation are not lethal or detrimental to the embryo(eg, localized or small and scattered fragments3 and othertypes of fragments are transient in nature), disappearingby resorption or lysis.10 In the present study, lesspervasive types of fragmentation (type I) on day 3 didnot diminish the likelihood of blastocyst formation(Table I) and were associated with minimal depressionsin the likelihood of pregnancy after embryo transfer,particularly when 2 or more embryos were transferred(Tables III and IV). More pervasive fragmentation (typeII or higher) was associated with significantly fewerblastocysts following extended culture as was previouslydescribed byAlikani et al,3 a very close inverse correlationwith embryo grade (P ! .0001; Table III), and a lowerlikelihood of pregnancy (P ! .0001; Table IV).
Fragmentation may also initiate apoptosis in humanembryos at the early cleavage stage,11 and the majorityof severely fragmented human embryos have been foundto stain positive with Annexin V, about 30% of whichare apoptotic (by terminal deoxynucleotidyl transferase-mediated deoxyuridine triphosphate nick end label-
ing).12 Other studies have determined that apoptosisoccurs only in fragmented embryos and that higheroxygen tensions in fragmenting embryos may predisposethem to apoptosis and cytoplasmic condensation.13
Our data establish close relationships between the typeof fragmentation of human embryos and their likelihoodof progressing to blastocysts in vitro and implantingfollowing embryo transfer. These relationships wereindependent of other elements of embryo grading andwere in accord with established lower pregnancy ratesfollowing transfer of frozen-thawed embryos and/orembryos from older patients. Our findings are consistentwith established correlations between early embryo frag-mentation and apoptosis, DNA fragmentation, andaneuploidy and emphasize the importance of assessmentof the type of fragmentation in selection of embryos forembryo transfer, particularly in older patients.
References
1. Hsu MI, Mayer J, Aronshon M, Lanzendorf S, Muasher S, Kolm
P, et al. Embryo implantation in in vitro fertilization and intra-
cytoplasmic sperm injection: impact of cleavage status, morphol-
ogy grade, and number of embryos transferred. Fertil Steril
1999;72:679-85.
2. Shapiro BS, Harris DC, Richter KS. Predictive value of 72-hour
blastomere cell number on blastocyst development and success of
subsequent transfer based on the degree of blastocyst development.
Fertil Steril 2000;73:582-6.
3. Alikani M, Cohen J, Tomkin G, Garrisi GJ, Mack C, Scott RT.
Human embryo fragmentation in vitro and its implications for
pregnancy and implantation. Fertil Steril 1999;71:836-42.
4. Moriwaki T, Suganuma N, Hayakawa M, Hibi H, Katsumata Y,
Oguchi H, et al. Embryo evaluation by analyzing blastomere
nuclei. Hum Reprod 2004;19:152-6.
5. Bongso A, Ng SC, Lim J, Fong CY, Ratnam S. Preimplantation
genetics: chromosomes of fragmented human embryos. Fertil Steril
1991;56:66-70.
6. Alikani M, Calderon G, Tomkin G, Garrisi J, Kokot M, Cohen J.
Cleavage anomalies in early human embryos and survival after
prolonged culture in vitro. Hum Reprod 2000;15:2634-43.
7. Bialanska M, Tan SL, Ao A. Chromosomal mosaicism throughout
human preimplantation development in vitro: incidence, type, and
relevance to embryo outcome. Hum Reprod 2002;17:413-9.
8. Ziebe S, Lundin K, Loft A, Bergh C, Nyboe Andersen A, Selleskog
U, et al. FISH analysis for chromosomes 13, 16, 18, 21, 22, X and
Y in all blastomeres of IVF pre-embryos from 144 randomly
selected donated human oocytes and impact on pre-embryo
morphology. Hum Reprod 2003;18:2575-81.
9. Munne S, Alikani M, Tomkin G, Grifo J, Cohen J. Embryo
morphology, developmental rates, and maternal age are correlated
with chromosome abnormalities. Fertil Steril 1995;64:382-91.
10. Van Blerkom J, Davis P, Alexander S. A microscopic and bio-
chemical study of fragmentation phenotypes in stage-appropriate
human embryos. Hum Reprod 2001;16:719-29.
11. Antczak M, Van Blerkom J. Temporal and spatial aspects of
fragmentation in early human embryos: possible effects on de-
velopmental competence and association with the differential
elimination of regulatory proteins from polarized domains. Hum
Reprod 1999;14:429-47.
12. Levy R, Benchaib M, Cordonier H, Guerin JF. Apoptosis in the
preimplantation embryo. Contracept Fertil Sex (France) 1998;26:
536-41.

determined by nanotechnology, possibly based on themetabolic function of the embryo in vitro. It is alsotempting to speculate that we will be able to look at thechromosomal complement in a noninvasive way tomake sure that only those embryos with a normal
Stone et al 2019
13. Yang HW, Hwang KJ, Kwon HC, Kim HS, Choi KW, Oh KS.
Detection of reactive oxygen species (ROS) and apoptosis in
human fragmented embryos. Hum Reprod 1998;13:998-1002.
Editor’s note: This manuscript was revised after thesediscussions were presented.
Discussion
DR RICHARD PAULSON, Los Angeles, Calif. The studythat Dr Marrs presented here addresses an importantaspect of the practice of in vitro fertilization, namelythat of embryo morphology and its ability to predictsubsequent pregnancy potential. Embryos undergoa predictable sequence of development in vitro or invivo, from fertilization to implantation. Because mostembryos are transferred back to the uterus at the 72-hour stage and because multiple embryos are typicallyavailable for transfer, it would be very useful to havea set of criteria that could be used to predict subsequentembryo development and eventually, implantation, andsuccessful pregnancy.
Dr Marrs and colleagues have chosen to focus on 1aspect of embryo morphology as a predictor of preg-nancy attainment, namely that of embryo fragmentation.
‘‘Fragmentation’’ is the term applied to anucleatepieces of cytoplasm surrounded by cell membrane, whichare formed during embryonic cellular division, in whichall of the cytoplasm does not divide into distinct,nucleated blastomeres. These so-called cellular fragmentsappear as small spherical particles inside the zonapellucida. During cell death or apoptosis, cells are notedto undergo this type of degeneration, and it has long beenthought that a large amount of embryo fragmentation isindicative of some degree of embryo degeneration andthus predictive of proof pregnancy potential.
Dr Marrs and colleagues performed a retrospectiveanalysis of all cycles in their program over a time span of2 years in which the female partner was under the age of40 years. They primarily investigated embryos, whichwere left in the laboratory after embryo transfer andobserved the progression of these embryos to theblastocyst stage 2 days later. Their findings were:
1. Fragmentation negatively correlated with blastocystdevelopment.
2. Cycles that resulted in pregnancy were associatedwith a lower fragmentation score than cycles inwhich pregnancy did not occur.
3. Embryo transfer analysis showed a trend towardbetter implantation with lower fragmentation score.
The present study contributes to our understandingof embryo morphology as a predictor of subsequentpregnancy success.
In the far future, we may predict that embryos will beselected on the basis of viability scores, which will be
karyotype are placed back in the uterus. However, atthe present time, morphological assessment remains thegold standard for embryo selection.
Therefore, I congratulate Dr Marrs and colleagues onthis large series that contributes to our understanding ofthis complex topic.
I have 4 questions for Dr Marrs:
1. How reliable is the ‘‘embryo score’’? Given thatmultiple individuals in the laboratory grade theembryos and that these observations are not blinded,what confidence can we have that this scoring systemmight be applied to other laboratories?
2. Have the authors attempted to calculate the per-embryo implantation rate? Because there appearedto be a lack of adequate power in the implantationanalysis, this might be a helpful strategy.
3. Did these cycles utilize donor or autologous oocytes,or was this a combination of both types, and werethe data stratified for age and type of in vitrofertilization (donor versus autologous)?
4. Have the authors noted any changes in the frag-mentation score over time, and can any suchchanges be attributed to changes in stimulationand/or culture conditions in the laboratory?
DR DAVID ADAMSON, Palo Alto, Calif. Trying toidentify a single score to predict outcome has clearlybeen a great challenge for us in the in vitro fertilizationworld. Have you considered looking at multiple re-gression on many of the variables that you haverecorded to see whether you might be able to come upwith a combined score that might be more predictivethan your fragmentation score? Have you changed yourcryopreservation criteria at all based on the results ofthis study? Could you comment on some recently highlypublicized data with regard to other biochemicalmarkers to predict the quality of embryos and ultimatepregnancy rates because, as you know, the search forsuch markers has been very complex and not successfulso far, at least in most people’s view.
DR FRANK GAMBERDELLA, Santa Barbara, Calif. Doyou see a role for embryo fragmentation scoring inselecting nonviable embryos for stem cell research?
DR SIMON HENDERSON, San Francisco, Calif. It is verydifficult to score these embryos and I was interested to seethat your top score was 8 cells or more when you arelooking at the number of cells on day 3. In our laboratory,we found there was a fall-off in how well these embryosdid if embryos were more than 8-cells; 10-cell and 12-cellembryos did not do nearly so well and would thereforehave a lower score in our scoring system. For example,