eliminating iodine deficiency disorders through … · the regional goodwill ambassador and former...
TRANSCRIPT

1
Eliminating iodine deficiency disorders through Universal Salt
Iodization
in Central Eastern Europe, Commonwealth Independent States
and the Baltic States (CEE/CIS/BS)
Draft Strategy Note
December 2004

2
1. Historic background
The UNICEF region of Central Eastern Europe and Commonwealth Independent States and the Baltic States (CEE/CIS/BS, also referred to in this article as ‘the region’) is comprised of 22
countries1. Salt iodization efforts date back to the time of the former Soviet Union2 when iodized salt was centrally produced and distributed to areas where goiter had been identified as an
endemic problem. The approach was generally limited to assessment and mass prophylaxis in endemic goiter areas only. Endemic goiter and cretinism were virtually eliminated through
targeted distribution of iodine tablets among vulnerable groups and careful monitoring. In the 1970’s and 80’s the monitoring system weakened and gradually IDD returned3,4. The entire system
collapsed with the break up of the Soviet Union in 1991 and iodized salt production was completely interrupted in countries across the region except in the Former Republic of Yugoslavia5 where salt
iodization continued.
In the early 1990’s the countries began to recognize an increase of goiter that indicated IDD was a recurring problem. The response in some cases included production and distribution of iodized salt,
but in most countries it was limited to the distribution of iodine supplements. Where salt iodization did take place it mainly included only table salt, leaving out other types of edible salt including salt
for food industry and animal consumption. Universal Salt Iodization (USI), the effort supported by UNICEF globally includes all consumable salt as the optimum way to protect every new born from
brain damage due to iodine deficiency. In most countries of the region, however, no sustainable effort took place toward USI until late 1990’s.
UNICEF initiated efforts to promote USI in the region in the early 1990’s. While establishing its
presence in the region efforts were stepped up in 1993 with advocacy for USI legislation through specially-organized meetings of national governments and salt industry partners6.
Many CIS countries have presented a unique set of challenges to the adoption of USI. These
include: the remnants of centrally-directed thinking; a salt industry that is often quasi-private
rather than private; a clinical perception of iodine deficiency; a lack of public awareness regarding
the nature and enormity of iodine deficiency; a lack of awareness that salt iodization is an effective
preventive measure; and the new and unique commercial structures producing alternative iodized
foods. On the other hand, the large and well-developed salt industries producing good quality salt
and a well educated population proved to be a good basis for salt iodization efforts.
As a result, initially, salt iodization did not increase significantly as shown by the household survey data of 2000 indicating that only 26% of households in the region were using adequately iodized
salt. This was the lowest rate among all the regions in the world (bar chart). The most recent results from several national surveys and iodized salt supply data indicate an increase of the
regional average of household using iodized salt to 48%.
The lack of progress toward USI urged UNICEF and other partners to increase efforts substantially. In 2001, UNICEF made elimination of iodine deficiency through USI a regional priority. The first
1 Albania, Armenia , Azerbaijan, Belarus, Bosnia and Herzegovina, Bulgaria, Croatia, Georgia, Kazakhstan, Kyrgyz Republic, Latvia,
Lithuania, UN administered province of Kosovo, TFYR Macedonia, Moldova, Romania, Russian Federation, Serbia and Montenegro,
Tajikistan, Turkey, Turkmenistan, Ukraine, Uzbekistan
2 This analysis and background information generally does only apply to the Republics of the Formers Soviet Union. Turkey
is also not reflected in the statements in the historic background 3 G.Gerasimov and F. Delange: Eastern Europe and Central Asia: Overview of IDD status. IDD Newsletter Volume 13 No
1, February 1997. 4 Gregory Gerasimov, IDD in Eastern Europe/Central Asia. IDD Newsletter Volume 18 No 3, August 2002. 5 Serbia & Montenegro, Macedonia, Bosnia & Herzegovina, Slovenia,Croatia, and UN Administered Province of Kosovo 6 UNICEF/ECO workshop in Turkmenistan 1994, PAMM training in Georgia 1998.

3
step was to strengthen internal technical and management capacity through recruitment of staff at the national and regional level. A thorough review of the programme identified weaknesses and
areas for improvement.
The main challenges that were identified included: 1. Weak political will to eliminate iodine deficiency through USI for which mandatory
legislation of iodization of all salt for human and animal consumption is required and its enforcement.
2. Lack of awareness among the medical and academic community, programme managers and decision makers of the nature and extent of the IDD problem beyond goiter. The effect on
brain development of the fetus during pregnancy and the consequences on society as a whole were widely ignored.
3. Poor understanding that iodine deficiency is a public health problem which requires a population wide intervention in the form of USI rather than a targeted approach screening
selected areas or individuals. 4. Little recognition by the government of the crucial role of the salt industry as a partner in
national USI efforts.
In response, support was increased to national partners to advocate for high level political commitment for USI legislation, build national partnership and coordination alliances, increase
iodized salt production through support of the salt industry, ensure consumer acceptance of iodized salt, and increase understanding among scientific partners.
Crucial in this approach has been the financial support from USAID, Kiwanis International, the Bill
and Melinda Gates Foundation, US Fund, and the Centers for Disease Control and Prevention (CDC). In (sub-)regional partnership with Asian Development Bank (ADB), ICCIDD, WHO, EU Salt,
USAID-MOST, and the Network for Sustainable Elimination of IDD, substantial progress has been made between 2001 and 2004.

4
2. Progress toward Sustainable Elimination of Iodine
Deficiency Progress towards the goal
With the World Fit for Children 2005 goal (sustainable elimination of iodine deficiency through USI) looming ahead there is still a long way to go for CEE/CIS/BS. Currently, 48% of the households
use iodized salt. Based on national population data and birth rates, 51% of the 5.4 million new born children in the region are protected. Unfortunately this also means that 2.7 million new born
children are not protected from IDD (table). Most of these children are born in Russia (1 million/year; 30% iodized salt use), Turkey (400,000/year; 70% iodized salt use) and Ukraine
(260,000/year; 31% iodized salt use). The regional average is greatly affected by these populous countries (see annex).
Recently, the UNICEF Regional Office made a projection of the national situations vis a vis the
progress towards the 2005 goal in each country. • Currently, USI (> 90% of households using iodized salt) has been achieved in 7
countries (Macedonia, Bulgaria, Serbia & Montenegro, Croatia, Turkmenistan, Bosnia & Herzegovina, Armenia). In Macedonia and Turkmenistan, also all other criteria for
sustainable elimination of iodine deficiency7 have been met, as confirmed by an external assessment team.
• In another 5 countries, elimination of iodine deficiency by 2005 is feasible (Lithuania, Kazakhstan, Georgia, Romania, and Azerbaijan) as well as in the UN Administered
Province of Kosovo. • The time-frame in the remaining countries to achieve the goal (Kyrgyzstan, Uzbekistan,
Tajikistan, Albania, Belarus, Moldova, Latvia and Turkey) is projected to last into 2006-2007, while in Russia and Ukraine perhaps longer time is required, depending on
political will to legislate USI.
Political commitment and USI legislation. Successful achievement of USI depends greatly on political commitment of key decision makers.
The main focus has been on evidence based advocacy for mandatory legislation. UNICEF focuses on mandatory legislation as a condition for achieving USI (the “push” factor) which is
complemented by communication activities to stimulate use of iodized salt (the “pull” factor). In absence of mandatory legislation the effect of communication activities is therefore limited.
Various regional and global events have been organized to advocate among high level decision makers for USI legislation.
Commitments by government and civil society to the World Summit for Children goals (1990)
including elimination of IDD were renewed through regional and national meetings related to the Global Movement for Children in Europe, namely, the Heads of CIS States Conference in Minsk
(April 2001) where a joint declaration to collaborate on national efforts to reach USI was signed. The United Nations Special Session on Children in 2002 resulted in an outcome document - a
World Fit for Children - which includes the goal to eliminate IDD through USI by 2005. This outcome document was signed by all governments in the region. Also, in October 2003 an
international advocacy meeting was organized in China where nine countries from the CEE/CIS/BS were represented at a high political level. Georgia and Turkey are examples of countries where a
big change in political will resulted in a rapid increase in usage rates of iodized salt from + 20% to + 70% in both countries.
The regional Goodwill Ambassador and former chess world champion, Anatoly Karpov has started
advocating for USI legislation since 2002 in several countries through his high-level public profile and personal contacts with politicians. In the Russian Federation, Karpov discussed draft USI
legislation with various government and Parliament members and succeeded to bring draft USI
7 ICCIDD, UNICEF, WHO: Assessment of Iodine Deficiency Disorders and Monitoring their Elimination. WHO, 2001.

5
legislation to the State Duma (parliament) in 2004, a significant step forward. In Ukraine, President Kuchma expressed his personal commitment for USI during a meeting with Karpov in
2002. Karpov also emphasized the need for more comprehensive USI efforts in various other countries including Lithuania, Kazakhstan, Serbia and Montenegro and Moldova.
Most advocacy activities by UNICEF and partners took place nationally. By using cost-benefit
figures, the consequences of USI and IDD have been presented as issues of national economic and social development, not simply health issues. Creative approaches have been used for example in
Russia where awareness and support was built in the Oblasts (regions) among local authorities, who then advocated for USI at the national level. A similar approach is now being followed in
Ukraine. Also civil society has shown to be powerful in advocating for USI (Azerbaijan, Russia, Ukraine).
All the efforts mentioned above have resulted in a legal framework for USI in 17 countries while in
the remaining 5 countries work continues on convincing the leadership to act. The Russian Federation and Ukraine have no USI legislation yet because of denial of the iodine
deficiency problem, leading to objections towards the mandatory iodization of all edible salt. Producers of other iodized products in Russia and Ukraine lobby strongly for alternative food
sources, leading to a bias against the acceptance of USI. The main focus will remain on advocacy for USI legislation at national and sub-national level. In countries where USI legislation is absent
and not expected soon, alternatives are being explored to increase the use of iodized salt in a sustainable way. For example, in the Russian Federation, merchandising techniques were tested in
2004 to help shop keepers shift salt sales to predominantly iodized salt.
Five countries have legislation on mandatory iodization of only table salt. Food producers in these countries believe (whether legitimate or not) that iodized salt affects the quality of their product.
As table salt comprises a small proportion of all salt consumed (30-40% in industrialized countries), achieving optimum iodine status throughout the population is unlikely to be successful
with iodization of table salt or food grade salt alone. Due to the high consumption of bread UNICEF advocates strongly to use iodized salt for baking of all bread and continues to work with other food
producers. Experiences from other countries (Bulgaria, Belarus, Macedonia, Western Europe) are used to address this concern.
Programme management and coordination National coordination alliances with more balanced involvement of public (government, medical
institutes), private (salt industry) and civic partners (consumer groups) to plan, manage and monitor are key for improving the ongoing national iodine deficiency elimination efforts. Support is
provided to build alliances and strengthen their required capacities.
Micronutrient programme management workshops organized regionally and nationally for members of national coordination teams helped to further develop understanding, communication,
and coordination of programme activities.
In addition, several programme review missions took place in all countries by consultants or UNICEF staff which helped to identify weaknesses in the current approach and work plans and how
to improve these.
National USI efforts were strengthened in many countries involving public, private and increasingly
the civic sector. Bulgaria is an example where multi-sectoral partnership has been successful. In Russia the Public Coordinating Committee (PCC), without government members, is strongly
lobbying for USI legislation resulting in discussion of the law in the State Duma.
National strategies sometimes include corrective actions of limited impact such as communication activities to improve household storage and utilization of iodized salt. Capacity building activities
are organized to strengthen strategies through workshops, on-the-job capacity building, inter-country exchange of experiences and round table discussions.

6
Production and supply of iodized salt
Production of only iodized edible salt is obviously the main pillar of the USI efforts. Several salt producers meetings were organized (Moscow 1997, regional producers meeting in Kiev 1999, Salt
2000, The Hague, Tashkent, 2002 and Bishkek, 2004) to raise awareness about USI, build partnerships and obtain a commitment to supply ever increasing amounts of iodized salt.
Initially, to increase production of iodized salt rapidly, support was provided for salt iodization
equipment, potassium iodate, laboratory equipment and supplies for quality control within the factory. Technical support was provided for salt iodization and quality assurance which resulted in
better quality iodized salt. Emphasis was also placed on involving the salt producers/importers as equally important partners in the national coordination bodies. Salt producers have been
supported to form associations that have facilitated work and communications amongst partners.
To sustain production of iodized salt, efforts were focused on increasing awareness among the producers, importers, wholesalers, and retailers. With new legislations in place, enforcement is still
weak in many countries. Therefore, mobilizing the suppliers to produce, promote and sell only iodized salt is crucial. Maintenance of salt iodization without external support is a sustainability
concern. UNICEF helps to identify potassium iodate producers and importing companies as well as negotiating more favorable import conditions.
Iodized salt production data is a useful and reliable monitoring tool, which provides roughly the
same proportion as household survey data. It serves as an easy tool to monitor progress frequently. There has been an increase in total production of iodized salt (as % of total salt
required) from 20% in 1999/2000 to 52% in 2003 (see graph).
Awareness raising and ensuring acceptance among partners and the end users As the approach and quality of communication activities vary greatly amongst countries in the
region, in 2003 UNICEF commissioned a review of IDD/USI communication activities in nine countries conducted by the Johns Hopkins University. The main conclusions pointed out an
inadequate capacity in the area of communication, an under-utilization of the private sector as a communication channel, the need for scaling up of communication activities, and the limited
impact of communication in absence of USI legislation as a ”push factor”.
Awareness raising and increasing acceptance among all stakeholders needs to be continuous and sustainable, as campaign-like activities are expensive. Incorporation of iodine deficiency
elimination and USI in the curriculum of primary/secondary education, and in technical, medical and public health training ensures long-term awareness raising. This approach is now pursued in
several countries. Messages on the iodized salt package and information for the consumer in sales outlets is another way of ongoing awareness raising. The involvement of communities and school
children as social mobilization activity was well demonstrated in Uzbekistan where more than 6 million school children were included in a campaign to test salt brought from their homes for the
presence of iodine. This example is being followed in many other countries of the region.
The communication strategy is often weak in addressing the critical information gaps such as mobilization of the salt supply channel, the lack of knowledge among food processing industries in
using iodized salt, and the lack of evidence-based material on the transient effects of introduction of iodized salt in an iodine deficient population. Development of communication plans are
supported as well as better exchange of experiences between countries.
Documenting lessons learned and utilization of regional expertise
A wealth of experience and expertise exists in countries. Efforts have been made to improve documentation of lessons learned and make them available to relevant countries. Inter-country

7
study tours, use of local expertise and technical assistance has become more common and has not only led to more successful transfer and sharing of knowledge but also empowered country teams.
A resource package is under development and includes scientific and technical material, guidelines on topics such as monitoring, communication, legislation, and also contains lessons learned from
several countries on a variety of topics.
Monitoring Monitoring the process of salt iodization and its impact on iodine status in the population is of
major importance to ensure efficiency and efficacy of USI. Monitoring and enforcement both serve a programme management purpose and need to be integrated. While more countries have USI
legislation and an increased production of iodized salt, monitoring receives more attention in the last few years. With insufficient funding for monitoring, the main challenge is to set up an
effective, affordable and manageable system. Monitoring of USI in CEE/CIS/BS is challenged by: i) poor quality data; ii) inadequate analysis and use of data for corrective actions; iii) weak capacity
(technical, staff, unclear responsibilities); and iv) an incoherent and fragmented system with numerous responsible parties.
UNICEF in collaboration with ADB, MOST-USAID8, CDC9 and KAN10 has provided support to
monitoring of USI through a variety of mechanisms including: consensus building workshops, technical support by consultants, and through exchange visits between countries (Romania with
Bulgaria, former Yugoslav Republic of Macedonia with Kosovo, Russian Federation & Bulgaria with Turkmenistan, Tajikistan with Iran, Armenia with Italy, Kyrgyz Republic with Bangladesh, etc.).
Experiences show that transfer of information and development of monitoring systems alone needs
to be complemented with consensus building among all responsible parties and adoption of the monitoring plan by higher level decision makers. In addition, the ownership and empowerment of
partners is markedly enhanced during study tours and inter-country exchange with colleague specialists. Also, monitoring cannot be seen in isolation from programmatic characteristics and
concerns. For example, illegally packaged salt (and sold as iodized), and “leakage” of industry salt (non-iodized) into the consumer market have to be taken into consideration when reviewing the
information to be collected. Finally, monitoring activities for iodine deficiency elimination need to be built into existing monitoring activities for other food fortification interventions.
Sustainability
While rapid progress is noted, sustainability of USI efforts remains a major concern because of: lack of national ownership, international agencies like UNICEF are often seen as the driving force;
a weak political will at the highest levels of government, regulatory agencies and salt industry; the salt industry is not or inadequately represented in the national coordinating alliance; producers of
iodized salt do not maintain salt iodization without external support; and continued dependency on external funding.
UNICEF will further focus on strengthening the national coordination and oversight function and recognizes that limited external funding is still required once USI has been achieved.
8 Micronutrient organization of USAID 9 Centers for Disease Control and Prevention, Atlanta USA 10 Kazakh Academy of Nutrition, Almaty Kazakhstan

8
3. Strategic support for Sustainable Elimination of IDD
Lessons learned The progress achieved in CEE/CIS/BS since the late 1990’s is the result of the national commitment and efforts of UNICEF and other partners in supportive roles. In order to define the
future support role that UNICEF should play in ensuring sustainable elimination in all countries of CEE/CIS/BS, it is important to consider the main lessons learned:
1. High level advocacy using evidence based arguments that reflect on consequences of IDD beyond health is not only crucial in initial phases but should be seen as a continuous
periodic activity to keep decision makers engaged and alert. 2. One main lesson learned from other regions in the world with long-standing IDD elimination
programmes is that success, once achieved, can easily slide back. Once IDD has been eliminated the effort needs to be sustained forever. Sustainability aspects need to be
addressed in all programme elements while high-level commitment needs periodic renewal. 3. Coordination of the programme activities requires a coalition at national level with
presence of government (public), salt industry (private), and consumer (civic) representatives. Recommendations for action need to carry weight and require follow up at
higher decision-making level. 4. USI legislation is key for sustained elimination of IDD and a priority of UNICEF support.
Enforcement remains a major weakness, however, which needs not only to be stressed through with enforcement agencies but also through mobilization and awareness raising
activities along the salt supply channel and consumers. 5. Permanent and adequate supplies of iodized salt is the sole responsibility of the salt
industry. Maintenance of equipment and procurement of fortificant needs to be self-sustaining.
6. Use of iodized salt in food processing (home based and industrially) is a concern in several countries (reflected in legislations) which can undermine the achievement of IDD
elimination. For these countries, specific support is required to increase the use of iodized salt in food, where proven and accepted.
7. Consumer perception and behavior can greatly affect the success of the elimination efforts. Communication activities need to be in place to inform the consumer and needs
continuous adaptation to the changing situation. 8. Monitoring and enforcement are to be seen as an integrated instrument to provide
information on the performance and impact of the efforts which should be used for corrective programmatic actions. Support should not only focus on defining the minimum
monitoring framework but should play a major role in building consensus among all responsible parties and in obtaining buy-in from decision makers.
9. A number of countries (in particular Russian Federation, Ukraine, and CARK) in CEE/CIS/BS present a unique situation where USI competes with a large range of other iodized food
products and supplements. This results in negative publicity for USI, resistant scientists with vested business interest in iodized products, and a compromised support for salt
iodization. Creative response is required to obtain political commitment, to incorporate USI in legal frameworks, to coordinate USI efforts, and to convince crucial partners.
10. Ample experience and programme knowledge exists throughout the region on a wide range of issues (use of iodized salt in food, monitoring data on TSH and iodine induced
hyperthyroidism, community mobilization, marketing and merchandising techniques, working with salt industry, sub-national advocacy, etc). Better documentation and creative
ways of sharing is required to maximize benefits for other countries.
UNICEF strategic support at regional and national level The proposed UNICEF supporting role in the various stages of IDD elimination is the result of a consultation process with Country Office staff. The regional overview including lessons learned and
the main thoughts on UNICEF support was shared and discussed at the Health and Nutrition
9
Cluster meeting in Turkey in July 2004. This stimulated discussion with partners at national level on their elimination strategy. Feed back was provided to the Regional Office indicating the type,
duration and level (funding needs) of support UNICEF would be providing. While recognizing the fact that any progress made in countries is the result of national efforts by all partners, support
from UNICEF plays a catalyzing and essential role. In all countries some level of support is required not only to achieve elimination of IDD but also during the 2-3 years to follow to address
national ownership and sustainability. Two main stages for support in IDD elimination are distinguished: a) the achievement of USI and
IDD elimination, and b) sustaining the success.
a) The achievement of USI and IDD elimination The role of UNICEF in a whole range of activities resulting in increased salt iodization lies in
advocacy for political commitment for USI and legislation, strengthening management and
operational capacity, development of national partnerships, development of monitoring and
enforcement systems, raising public awareness and ensuring permanent and adequate supplies
of iodized salt.
Focus in countries with low use of iodized salt require support in areas including commitment
building, production and supply, communication, and partnership building. Countries close to
reaching the goal need support in monitoring and enforcement, communication and
management. UNICEF’s continued guaranteed support is very important at this stage.
b) Sustaining the success
In countries where IDD has been eliminated UNICEF’s support will gradually be reduced and will focus on sustaining the success, periodic renewal of commitments of national leaderships,
strengthening of national oversight functions and consolidation of habitual norms in industry, and consumption patterns. Support is also required for improved monitoring and sustainable
communication activities. Countries in this phase will require continued support for another 3 years.
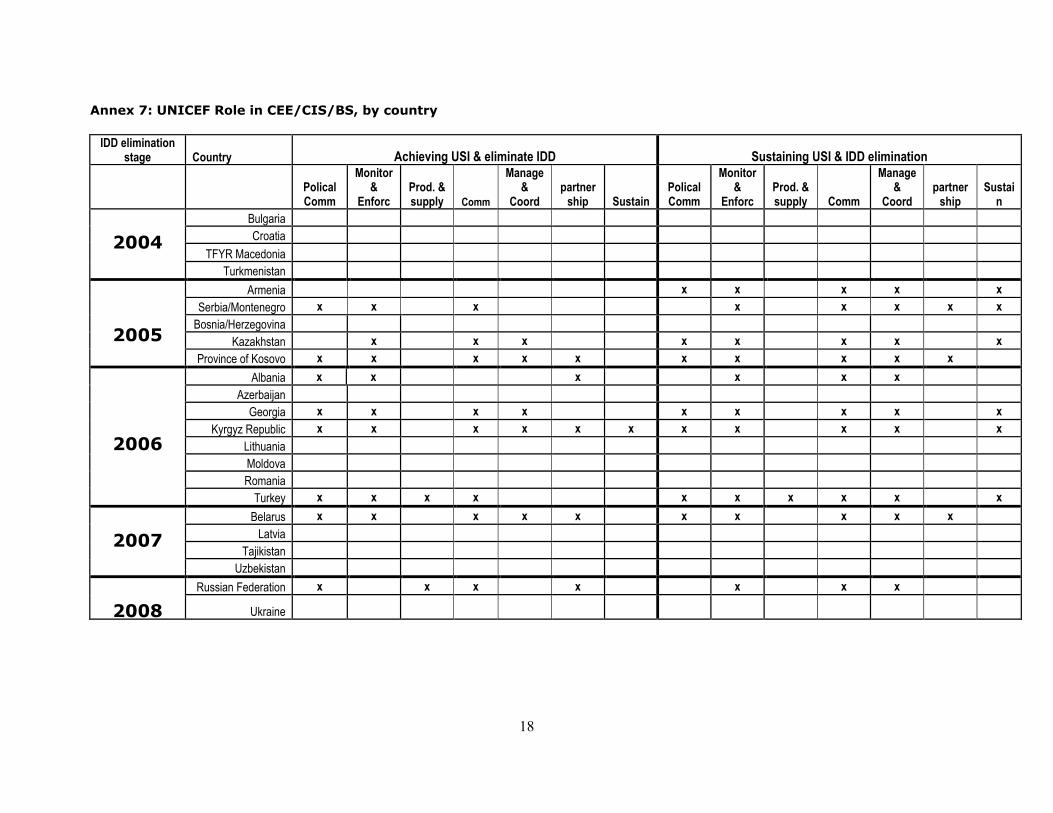
Annex 7 provides an overview of the support UNICEF would be providing to fully accomplish these
tasks. Estimated levels of funding requirements are available upon request.
UNICEF strategic support at national and regional level
UNICEF Country Offices will provide direct support to programme implementation and focus on challenges specific to the country. This will be described in more detail below.
UNICEF Regional Office will play an overall strategic role in support to countries while addressing the main challenges also from a regional perspective. The core functions include monitoring and
reporting of programme performance, optimize partnerships, knowledge building and innovative approaches, integrate approaches and strategies to address micronutrient deficiencies, build
capacity of country staff and to secure funding. Specific activities will be elaborated below.
Advocacy for high political commitment and USI legislation
a) National In countries without firm political commitment and/or USI legislation, focus will remain on
evidence based advocacy using arguments addressing consequences of iodine deficiency beyond health. In Russian Federation and Ukraine, regional advocacy among local governments will be
more strongly pursued in order to extend the pressure for USI beyond national partners. In several countries enforcement is major challenge which is mainly due to inadequate capacity
(staff, technical, equipment) and fragmentation of the enforcement agencies (unclear roles and responsibilities). In addition to strengthening multi-partner discussion on monitoring and
enforcement reform, mobilization activities will target the salt supply channel and consumers to sell and use iodized salt.

10
b) Regional Experiences have shown the need for continued renewal of commitment to ensure sustained
success of IDD elimination. The regional office plays a crucial role in bringing USI and IDD elimination on the agenda of region-wide political conferences (CIS meeting, MCH forum), in
individual meetings with political leaders (Regional Director during visits and World Health Assembly) and through the work of Regional Goodwill Ambassador Karpov. In large countries
Russian Federation, Ukraine, and Turkey the regional office directly advocates with high-level decision makers.
Success stories will be documented and highlighted in the media and will be used for advocacy in other countries. High-level advocacy material with tailored information addressing the specific
audience requires more focus. Material like the Damage Assessment Report needs to be developed for other countries and for tailored use at regional and country level.
Programme management and coordination a) National
National events (round table, workshops) aim to strengthen micronutrient elimination strategies and will include a consensus building and advocacy component to obtain buy-in from high level
decision makers. Capacity building in technical areas like monitoring and communication will strengthen the partnership and management. More support will be given to strengthen a
sustainable national alliance with management and oversight function, and with public reporting on programme performance. National ownership and self-funding of programme functions are key
characteristics which are long term efforts. b) Regional
The regional workshops on ‘Strengthening Strategies for the Elimination of Micronutrient Malnutrition’ in Almaty (2003, CDC supported) and Ankara (2004, USAID supported) were
successful in bringing together national partners and discuss main strategic choices for micronutrient programmes. The exchange of views and experiences between countries was
perceived as extremely valuable. Moreover, the workshops increased commitment and follow up upon return in their respective countries. The last of these workshops for the remaining countries
in South Eastern Europe is scheduled for March 2005. National alliances are the basis for eliminating IDD and for sustaining its success. International
agencies like UNICEF and ABD are often the driving force behind these alliances. Now that many countries have or are close to eliminating IDD national partnerships need to be strengthened.
Equal membership of government, salt industry and consumer organizations needs to be ensured. In addition, the alliance should function as a national watch whose advise leads to programme
adjustments. To strengthen national micronutrient strategies as well as national partnerships, workshops could
be organized with 3-4 participating countries at a time, to strengthen partnerships by jointly developing national plans of action, building consensus and obtaining national buy-in from decision
makers.
Regional and global partnerships
a) Regional In the CEE/CIS/BS, the regional office has had close partnership with traditional partners like WHO
and ICCIDD. More recent partnerships include ADB, CDC, MOST-USAID, and to a certain extent with the private sector and academic institutions. In order to address some of the challenges and
to further strategic thinking, collaboration with partners needs to be strengthened and expanded. Salt producing or trading companies for example EU salt, Akzo Nobel, Unilever can provide specific
technical support to countries on marketing, merchandising, trade issues, and assist in local distribution and sale of iodized salt. Specialized marketing support can help to study consumer
perception and develop strategies to better address perception barriers. In the areas of monitoring and strategy development, collaboration with CDC, MOST-USAID,
Emory University, and Kazakh Academy of Nutrition has played an important role to increase the capacity, improve country strategies and action plans, and resulted in better performance. Further

11
work is required with these and new partners specifically to a) strengthen monitoring through consensus building workshops, b) develop long term integrated micronutrient action plans, c)
apply newly emerging technologies of double fortified salt in population wide interventions, and d) obtain better information on iodine status of pregnant women.
Monitoring of programme performance and impact Regular feed back on programme activities will provide information on progress, identify problem
areas, new emerging challenges and opportunities for action. For example, it is important to identify areas/population groups with low use of iodized salt, trends in iodized salt production,
sustainability concerns, etc. a) National
Support for monitoring will become more important in advanced phases of salt iodization. Establishing effective, affordable and manageable systems has proven to be a challenge.
Consensus building and endorsement from decision makers will receive more focus. b) Regional
RO has developed monitoring tools in 2004, serving country and regional purpose, for iodized salt supply and for monitoring critical success factors of sustainable IDD elimination. Further work is
required to improve these and fully maximize their purpose by incorporating them in routine programme management. It will also help to streamline the approach and technical support
provided by consultants. Suggested activities: consultancy to improve monitoring tools based on country feed back, on-the-
job training, include as part of workshops, adjust Terms of Reference for consultants, incorporate in monitoring and reporting procedures, establishment of programme database.
Knowledge building and development of new approaches a) National
Useful experiences will be identified and documented and made available for colleagues in other countries. Exchange will also take place between national partners at meetings, inter-country visits
and study tours. Better coordination is required between countries to maximize these exchanges. Regional
The challenge in better utilization of available experience and expertise in the region is to make these widely available and explore alternative ways of sharing.
The regional office has started to stimulate documentation of lessons learned and utilization of regional expertise through study tours, exchange of country expertise through visiting consultants,
sharing of lessons learned with country staff, and the development of the IDD elimination resource package. The resource package includes a wealth of information for managers and partners to
learn from other countries’ experiences, to obtain ‘how to’ guidance on areas like monitoring and communication, and to find information on how to deal with common challenges. One next step
will be to develop a more continuous medium, for example a website, that will help exchange of information. The Regional Office will also need to play a more structured coordinating role to link
countries together for exchange of information, study tours, etc. The knowledge building is an important role of the regional office to keep pace not only with new
scientific developments but also to identify and discuss programmatic areas that require attention. Substantive effort is required through meetings on thematic issues with participation from regional
and global technical and programme persons. New ideas coming out of these meetings may require support for example implementation of scalable innovative solutions e.g. double fortified
salt with iodine and iron in partnership with salt industry partner. Another example is exploring more sustainable monitoring methods through sentinel sites or through clinics surveying pregnant
women.
Awareness raising and ensuring acceptance among partners and the end users
a) National
12
Together with the strengthening of the enforcement system more focus will go toward mobilization and motivation of salt supply channel (producers, importers, wholesalers, retailers) to ensure
compliance to only provide iodized salt. In certain areas where the capacity of the salt producers is limited to iodize salt (small producers) or where (poor quality) salt is produced by unlicensed
enterprises, the consumers/community will be mobilized to demand iodized salt. This approach is of particular importance when big industries iodize their salt but where smaller producers in
difficult to reach areas (often severely affected by IDD) do or can not adhere to government regulations. These countries often show stagnating usage rates at insufficient levels (60-80%).
A particular challenge is the use of iodized salt in food production (meat, cheese, pickles, bread, etc). Mobilization activities using evidence and experiences from other countries are required to
achieve the use of iodized salt in a minimum number of food items, in particular bread. Medical professionals showing concern that introduction of iodized salt will lead to increased health
risk certain individuals need to be included in targeted communication activities as well. Furthermore, the focus at national level will the sustainability of communication activities through
incorporating messages in curriculum at schools and in training programmes of medical professionals and through product promotion and consumer information by the private sector.
b) Regional Based on an extensive review of communication activities in 9 countries in the region by Johns
Hopkins University in 2003, it has become apparent that communication activities need to be scaled up and planned in a structured manner with a focus on sustainability. The quality in
communication plans vary widely between countries. The regional office has to address these gaps through development of a comprehensive communication strategy that will serve as guidance for
communication plans in all countries. The main aspects include: 1. Communication needs to be an integral part of other programme activities especially
monitoring, enforcement and supply of iodized salt. 2. The main purpose of communication is ensuring acceptance and increase immediate use of
iodized salt through campaigns (short-term, and curriculum and product promotion (long-term)
3. The purpose and expected outcome has to be in conjunction and mutually supportive with mandatory legislation, for example enforcement needs to be complemented by mobilization
of salt wholesalers, retailers and consumers 4. The communication activities should anticipate rumours and adverse effects. Media training
and examples from other countries need to be included. 5. Clear guidance is required for development of messages
6. All aspects need to be laid out in a communication plan. Support is required to develop national communication plans through workshops and/or
consultancies.
Production and supply of iodized salt a) National and regional
Sustaining salt iodization without external support is a sustainability concern. Free donation of potassium iodate is no longer authorized and iodization equipment is only provided in exceptional
cases (where iodization efforts are scaling up). Support is required to link salt producers to potassium iodate producers in the region for direct procurement or through importing companies
or distributors who can include potassium iodate in their supply list. UNICEF can also assist in negotiating more favorable import conditions (tariffs, clearing procedures, etc). In exceptional
cases UNICEF can also assist in revolving funds or offering procurement services for potassium iodate. Procurement workshops and specific technical expertise are planned.
Salt industries are often seen as passive actors in the salt iodization effort. Self-sustained salt iodization requires better understanding by the other partners of the industry’s perspective and to
increase national ownership. Country Offices will focus more on mobilizing salt producers to self-sustain production of iodized salt. Technical support may be provided for marketing.
Iodized salt production data is a useful and reliable monitoring tool, which provides roughly the same information on proportion of iodized salt use as household survey data. It serves as an easy
tool to monitor progress frequently. Regional office has introduced the periodic monitoring of

13
iodized salt supply data with all Country Offices. Further work is required to facilitate use of the monitoring tool with Country Offices and dissemination of compiled overviews with salt suppliers.
Integrated approach for micronutrient interventions a) National and regional
Multiple activities have been carried out in the region where other micronutrients beyond iodine were addressed. With limited resources available both from national budget and from external
funding it makes sense to focus on cross cutting issues for other micronutrients than iodine at the same time. Globally, resources to address iron, folic acid, and zinc deficiency are still relatively
scarce. Iron deficiency is a universal problem in CEE/CIS/BS with significant impact on maternal and child survival, and, although many opportunities exist through the high consumption of flour
which is produced in large mills, flour fortification can not be taken on at large scale by UNICEF due to limited resources.
Also from scientific point of view an integrated approach makes sense. Evidence increasingly suggests the synergistic interaction between micronutrients which in programmatic terms makes
an investment more effective if more micronutrient deficiencies are addressed through the same intervention. Double fortification of salt, multi-micronutrient supplementation, and fortification of
flour with a mix of micronutrients are some of the many examples. The regional office wants to better integrate micronutrient interventions and plans to advance
known and explore new opportunities (complementary food fortification with multiple micronutrients, home-based fortification using sprinkles or food-lets, flour and oil fortification,
double fortification of salt, etc).
Conclusion
CEE/CIS/BS has made a remarkable leap forward in a very short period of time. While further attainment of the success is imperative, UNICEF recognizes the challenges that lie ahead which
need to be reflected in its strategic support. Because of the unique character of CEE/CIS/BS, UNICEF’s role needs constant adjustment. Focus of support remains on advocacy for USI
legislation, a balanced and effective national coordination alliance with involvement of the salt industry as an equal partner, sustainable monitoring and enforcement, and ensuring acceptance of
iodized salt. There is need for constant renewal of high-level political commitments and national oversight.
UNICEF initial role to establish rapid increase of salt iodization has slowly been shifting towards addressing sustainability concerns and national ownership, taking into account the lessons learned
worldwide. The momentum built in CEE/CIS/BS creates an excellent opportunity to achieve elimination of iodine deficiency in more countries of the region, and thus ensure learning ability of
the future generation within the next few years to come. Continued support is required to achieve these objectives.

14
Annex 1: Percentage of households in CEE/CIS/BS using adequately iodized salt
% of households using adequately
iodized salt in CEE/CIS (survey based)
0
20
40
60
80
100
Lithuania
Russian Fed.
Tajikistan
Kazakhstan
Ukraine
Uzbekistan
Bosnia/Herzegovina
Moldova
Romania
Albania
Belarus
Turkey
Georgia
Azerbaijan
Serbia & Montenegro
Kyrgyz Republic
Armenia
Kosovo
Croatia
TFYR Macedonia
Bulgaria
Turkmenistan
Latvia
CEE/CIS region
1999-2000 2003
>90% : 4
50-90% : 13
<50% : 5

15
Annex 2: Relationship between schoolchild urinary iodine and household iodized salt use in 11 CEE/CIS/BS countries
Relationship between schoolchild urinary iodine and
household iodized salt use in 11 CEE/CIS countries
0
50
100
150
200
250
0 20 40 60 80 100 120
% Households using iodized salt
Urinary iodine (mcg/L)
Annex 3: Change in household iodized salt use between 2000 and 2003 for all UNICEF
regions
R =0.692
Changes in household iodized salt use, 2000 & 2003
0%10%20%30%40%50%
60%70%80%90%100%
East/Southern Africa
West/Central Africa
N Africa/M East
South Asia
E Asia/Pacific
L America/Caribbean
E-Europe & C-Asia
All regions
2000 2003

16
Annex 4: Map of CEE/CIS/BS region by % households using iodized salt
Annex 5: Trend in supply of iodized salt in CEE/CIS/BS from 1999 to 2003
Trend in supply of iodized salt in CEE/CIS/BS
ArmeniaAzerbaijan
Georgia
Kazakhstan
Kyrgyzstan
TajikistanTurkmenistanTurkey
UzbekistanAlbania
Bulgaria
Belarus
Croatia
Lithuania
Macedonia
Romania
Serbia & Montenegro
Ukraine
Source: UNICEF regional Office for CEE/CIS/BS 2004
Percent of households using adequately iodized salt
10 - 49 50 - 90 91 - 98
Missing data
Percent
Russian Federation
iodized salt as % of total salt required
( + 3.5 kg per person per year)
20
38
52
0
50
100
150
supply of iodized salt
1999-2000 2001-2 2003

Annex 6: Household use of iodized salt (%) and protected new born children in CEE/CIS/BS, by country
2003 Population
(millions)
Household salt iodized 2003 Annual births (thousands)
UNICEF region Country Total
Protected against ID % Year
per 1,000 population Total
number protected
number unprotected
% of region's unprotected in IDD affected countries
East Europe, CIS, and Baltics
CEE/CIS Russian Federation 145.5 43.7 30 10 1,455 437 1,019 38%
CEE/CIS Turkey 71.2 49.8 70 2003 22 1,566 1,096 470 17%
CEE/CIS Ukraine 47.8 14.8 31 2002 8 382 119 264 10%
CEE/CIS Uzbekistan 25.7 14.4 56 2003 20 514 288 226 8%
CEE/CIS Romania 21.6 11.4 53 2002 10 216 114 102 4%
CEE/CIS Kazakhstan 14.8 4.3 29 1999 15 222 64 158 6%
CEE/CIS Tajikistan 6.6 1.8 28 2003 19 125 35 90
CEE/CIS Azerbaijan 8.2 3.4 41 2000 14 115 47 67
CEE/CIS Belarus 9.9 5.4 55 2003 9 89 49 40
CEE/CIS Serbia/Montenegro 10.7 7.8 73 2000 12 128 94 34
CEE/CIS province of Kosovo 2.0 1.7 84 2002
CEE/CIS Kyrgyz Republic 5.0 3.4 67 2003 20 100 67 33
CEE/CIS Lithuania 3.5 10 2003 9 32 3 28
CEE/CIS Moldova 4.3 2.2 52 2003 9 39 20 19
CEE/CIS Albania 3.1 1.7 56 2000 16 50 28 22
CEE/CIS Latvia 2.3 9 21 21
CEE/CIS Georgia 4.7 3.2 68 2003 9 42 29 14
CEE/CIS Turkmenistan 5.7 5.7 100 2004 19 108 108 0
CEE/CIS Bosnia/Herzegovina 3.9 3.0 77 2003 10 39 30 9
CEE/CIS Armenia 3.2 2.7 84 2000 14 45 38 7
CEE/CIS Croatia 4.3 3.9 90 2000 9 39 35 4
CEE/CIS Bulgaria 7.5 7.3 98 2003 8 60 59 1
CEE/CIS TFYR Macedonia 2.1 2.1 100 2003 13 27 27 0 % new borns protected
Total 413.6 192.5 48% 13.2 5,414
2,787 2,627 51%
18
Annex 7: UNICEF Role in CEE/CIS/BS, by country
IDD elimination
stage Country Achieving USI & eliminate IDD Sustaining USI & IDD elimination
Polical Comm
Monitor &
Enforc Prod. & supply Comm
Manage&
Coord partnership Sustain
Polical Comm
Monitor &
Enforc Prod. & supply Comm
Manage&
Coord partnership
Sustain
Bulgaria
Croatia
TFYR Macedonia
2004
Turkmenistan
Armenia x x x x x
Serbia/Montenegro x x x x x x x x
Bosnia/Herzegovina
Kazakhstan x x x x x x x x
2005
Province of Kosovo x x x x x x x x x x
Albania x x x x x x
Azerbaijan
Georgia x x x x x x x x x
Kyrgyz Republic x x x x x x x x x x x
Lithuania
Moldova
Romania
2006
Turkey x x x x x x x x x x
Belarus x x x x x x x x x x
Latvia
Tajikistan
2007
Uzbekistan
Russian Federation x x x x x x x
2008 Ukraine