electronic health records - university of...
TRANSCRIPT
Chapter 5
Electronic HealthRecords
Chapter Outline
Key Termscharacterclinical data repositorycomputer-based patient
record (CPR)computerized medical recordsdatadocument imagingelectronic health record (EHR)electronic medical record (EMR)field
filehealth datahealth informationhealth information exchange (HIE)Health Level Seven (HL7)hybrid recordsindexedinformationlongitudinal patient recordoptical disk imaging
patient monitoring systempersonal health record (PHR)recordrecord transitional templateregional health information
organization (RHIO)registration-admission-
discharge-transfer system (RADT)
scanner
• Key Terms
• Objectives
• Introduction
• Evolution of Electronic Health Records
• Electronic Health Record Systems
• Regional Health Information Organization
• Components of Electronic Health RecordSystems Used in Health Care
• Internet Links
• Summary
• Study Checklist
• Case Study
• Chapter Review
107
9781133889731, Essentials of Health Information Management: Principles and Practices, Second Edition, Green/Bowie - © Cengage Learning.
All rights reserved. No distribution allowed without express authorization.

INTRODUCTION
The health information profession is being transformedfrom a paper environment to a virtual electronic world.Health information professionals have unique patientinformation management skills that will assist facilitiesin making the transition to electronic health record.
EVOLUTION OF ELECTRONIC HEALTH RECORDS
From the 1960s to the present, many terms have beenused to describe automated medical record systems.The terms used to describe these systems have changeddue to the advancement of technology and becauseautomated systems have evolved from single computerapplications to a combination of numerous systemsthat are networked together.
In the period 1970–1980, the term computerizedmedical records was used to describe the early medicalrecord automation attempts. The early automation efforts focused on the development of alerts, medicationadministration records, provider orders communication,and notes. Automation was primarily used in the fol-lowing types of systems: patient registration, finance,laboratory, radiology, pharmacy, nursing, and respira-tory therapy. During the 1970s, most computerizedmedical records were developed in university settingsfor use that was tailored to the needs of the developingentity; therefore, these early systems could not be easily implemented at other facilities.
Throughout the 1980s, the development of auto-mated systems was slow, but the vision of electronicrecord systems was a goal of the health care industry.The Institute of Medicine (IOM), in 1991, released a report entitled The Computer-based Patient Record: AnEssential Technology for Health Care. The vision from thisreport was to develop automated systems that wouldprovide a longitudinal patient record. A longitudinalpatient record contains records from different episodesof care, providers, and facilities that are linked to forma view, over time, of a patient’s health care encounters.The IOM concluded that this could be accomplishedthrough a computer-based patient record (CPR). The
108 • Chapter 5
term CPR was used to describe a broader view of thepatient record than was present in the 1990s.
The CPR is multidisciplinary and multienterprise,(Figure 5-1), and it has the ability to link patient informa-tion at different locations according to a unique patientidentifier. Although this is the primary advantage ofCPR systems, there are also many other advantages of automated records systems. Refer to Table 5-1 for a comparison of manual and automated record systems.A CPR also provides access to complete and accuratehealth problems, status, and treatment data; and itcontains alerts (e.g., drug interaction) and reminders(e.g., prescription renewal notice) for health careproviders. According to the Institute of Medicine’s1991 report, electronic records should support the following:
• Physician access to patient information• New and past test results in multiple-care settings• Computerized order entry• Computerized decision-support systems to prevent
drug interactions and improve compliance with bestpractices
• Secure electronic communication among providersand patients
• Patient access to records, disease management tools,and health information resources
• Computerized administration processes, such asscheduling systems
• Standards-based electronic data storage• Reporting for patient safety and disease surveillance
efforts
A second edition of the report was released in 1997,which further validated the need for the developmentof automated medical record systems.
As automated systems developed throughout the1990s, dictation, transcription, and document imagingfunctions were merged with CPR functions. Documentimaging and optical disk imaging provided an alterna-tive to traditional microfilm or remote storage systemsbecause patient records are converted to an electronicimage and saved on servers or optical disks. Optical diskimaging uses laser technology to create the image.
ObjectivesAt the end of this chapter, the student shouldbe able to:• Define key terms
• Distinguish between computerized patient records,electronic patient records, and electronic health records
• Discuss electronic record implementation issues
• Define and discuss the importance of regional health information organizations
• Identify the administrative and clinical applicationsfound in electronic health records
9781133889731, Essentials of Health Information Management: Principles and Practices, Second Edition, Green/Bowie - © Cengage Learning.
All rights reserved. No distribution allowed without express authorization.
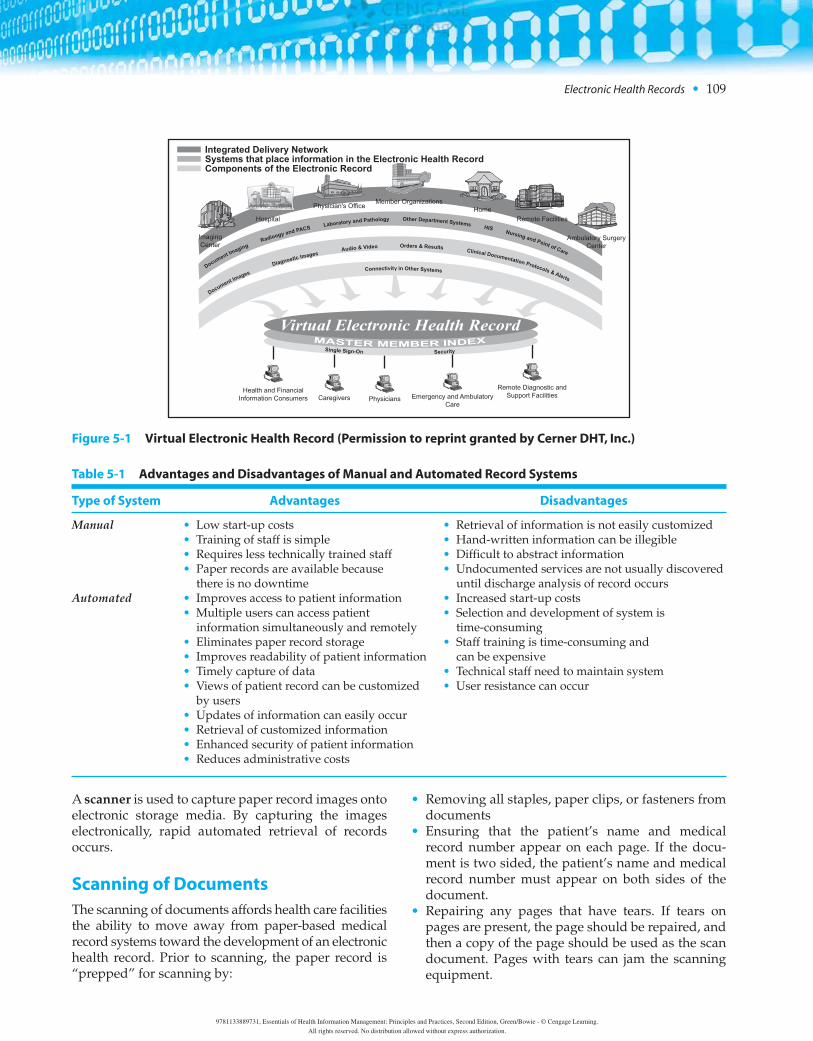
A scanner is used to capture paper record images ontoelectronic storage media. By capturing the imageselectronically, rapid automated retrieval of records occurs.
Scanning of DocumentsThe scanning of documents affords health care facilitiesthe ability to move away from paper-based medicalrecord systems toward the development of an electronichealth record. Prior to scanning, the paper record is“prepped” for scanning by:
• Removing all staples, paper clips, or fasteners fromdocuments
• Ensuring that the patient’s name and medicalrecord number appear on each page. If the docu-ment is two sided, the patient’s name and medicalrecord number must appear on both sides of thedocument.
• Repairing any pages that have tears. If tears onpages are present, the page should be repaired, andthen a copy of the page should be used as the scandocument. Pages with tears can jam the scanningequipment.
Electronic Health Records • 109
Health and FinancialInformation Consumers Caregivers Physicians Emergency and Ambulatory
Care
Remote Diagnostic andSupport Facilities
ImagingCenter
Hospital
Physician's OfficeMember Organizations
HomeRemote Facilities
Ambulatory SurgeryCenter
Virtual Electronic Health RecordMASTER MEMBER INDEX
Single Sign-On Security
Document Imaging
Radioogy and PACSLaboratory and Pathology Other Department Systems
HISNursing and Point of Care
Document Images
Diagnostic ImagesAudio & Video Orders & Results
Clinical Documentation Protocols & Alerts
Connectivity in Other Systems
Integrated Delivery NetworkSystems that place information in the Electronic Health RecordComponents of the Electronic Record
Figure 5-1 Virtual Electronic Health Record (Permission to reprint granted by Cerner DHT, Inc.)
Table 5-1 Advantages and Disadvantages of Manual and Automated Record Systems
Type of System Advantages Disadvantages
Manual • Low start-up costs • Retrieval of information is not easily customized• Training of staff is simple • Hand-written information can be illegible• Requires less technically trained staff • Difficult to abstract information• Paper records are available because • Undocumented services are not usually discovered
there is no downtime until discharge analysis of record occursAutomated • Improves access to patient information • Increased start-up costs
• Multiple users can access patient • Selection and development of system is information simultaneously and remotely time-consuming
• Eliminates paper record storage • Staff training is time-consuming and • Improves readability of patient information can be expensive• Timely capture of data • Technical staff need to maintain system• Views of patient record can be customized • User resistance can occur
by users• Updates of information can easily occur• Retrieval of customized information• Enhanced security of patient information• Reduces administrative costs
9781133889731, Essentials of Health Information Management: Principles and Practices, Second Edition, Green/Bowie - © Cengage Learning.
All rights reserved. No distribution allowed without express authorization.

After preparation of the documents, the paper is inserted into a scanner. As document imaging systemshave advanced, many document-imaging system,now index the scanned forms to aid in data retrieval.Each scanned page is indexed, which means it is iden-tified according to a unique identification number,which is commonly the patient’s medical record num-ber. Because of document indexing, all documents forthe same patient do not have to be scanned at the sametime. The complete patient record can be retrieved because each page has been indexed.
After the pages are scanned, the quality of thescanned document should be verified prior to the destruction of the original document. Many facilitieshave two quality reviews of the scanned documents.The first review is by the person scanning the docu-ment, and the second review is completed by a secondstaff member.
Continued Evolution of Electronic RecordsThe next step in the evolution of electronic records includes the merging of data from different data systems into one centralized database known as a clinical data repository, which provides easy access todata in electronic or printed form. The term electronicmedical record (EMR) was used in the late 1990s todescribe systems that were based on imaging and themerging of data from various stand-alone systems.The terms “computerized patient records” and “elec-tronic medical records” were used interchangeably.During this period of time, many vendors developedelectronic medical record systems for use in ambula-tory care and primarily physician offices. Many inpa-tient facilities were also using electronic medicalrecord systems, but there was limited networking between the inpatient and ambulatory worlds.
In July 2003, IOM submitted a letter entitled Key Capabilities of an Electronic Health Record System to theDepartment of Health and Human Services, whichused the term electronic health record (EHR). Duringthis period of time, President George W. Bush, in his2004 State of the Union Address, supported the use ofelectronic health records to improve care and reducemedical mistakes and costs. President Bush issued anexecutive order to establish the position of the NationalCoordinator for Health Information Technology withinthe Office of the Secretary of HHS. This position wascreated for the primary purpose of aiding the Secretaryof HHS in achieving the president’s goal. In February2009, Congress enacted the American Recovery and
Reinvestment Act, which includes an estimated net in-vestment of $19 billion for health information technol-ogy, including the development of technologies toenhance the advancement of electronic health records.
The term “electronic health record” is currently beingused by the IOM and Health Level Seven (HL7) in thedevelopment of standards that relate to the exchange ofclinical health information. Health Level Seven (HL7) isa standards development organization that developsEHR standards under the direction of the U.S. Depart-ment of Health and Human Services. The standards out-line the process for the exchange of health informationand help to develop a nationwide interoperability planfor providing common parameters that will be used forelectronic data and record exchange.
Although there is no universal definition of an electronic health record, the following definition byAHIMA should be noted. AHIMA defines EHR as acomputerized record of health information and asso-ciated processes. Another term that is currently used is“personal health record (PHR),” which is an electronicor paper medical record maintained and updated byan individual for his or her own personal use.
Exercise 5–1 Evolution of Electronic Health Records
Fill-In-The-Blank: Enter the appropriate terms(s) tocomplete each statement.
1. Merging the data from different data systems intoone centralized database is known as a _________.
2. A ___________ contains records from differentepisodes of care, providers, and facilities that arelinked to form a view, over time, of a patient’shealth care encounters.
3. An electronic or paper medical record maintainedand updated by an individual for his or her ownpersonal use is known as a __________.
4. The standards for the exchange of health informa-tion are being developed by __________.
5. AHIMA defines the __________ as a computerizedrecord of health information and associatedprocesses.
ELECTRONIC HEALTH RECORD SYSTEMS
No two facilities have the same electronic health recordsystem. Electronic health record systems that are usedin various facilities today are combinations of various
110 • Chapter 5
9781133889731, Essentials of Health Information Management: Principles and Practices, Second Edition, Green/Bowie - © Cengage Learning.
All rights reserved. No distribution allowed without express authorization.

Electronic Health Records • 111
systems that integrate medical documentation needsinto an electronic format. Author Bowie has workedwith numerous facilities to implement electronic healthrecord systems in a variety of types of health care organizations. Each implementation has been a uniquejourney based on the information needs, budget, existingautomated systems, and other factors.
Transition from Paper Records to Electronic Health RecordsFacilities are in various transitional states in regardto having electronic health records. Many facilitieshave hybrid records, a part paper and part elec-tronic record. This is considered as a transitionalstate until a true electronic health record can be realized. In a hybrid system, some documents remain on paper while other parts of the record areelectronic. One of the most important issues to iden-tify, when managing a hybrid record, is the facility’sdefinition of its legal record. It should be noted thatstate law is the primary basis for the definition ofthe legal patient record.
Issues Impacting the Electronic Legal Health RecordFacilities need to clearly define their legal record to beable to respond to various requests for an entire pa-tient’s record. The content of the legal record must bedefined in facility policy, and standards for maintain-ing the security and integrity of the record need to beclearly defined. In a hybrid patient record system, partof the record will be retrieved manually while the re-maining part will be housed in the automated system.It is essential that all aspects of the record regardless ofthe media used to store the record, paper or electronic,be addressed in facility policy.
As facilities are in transition from paper to electronicformats, it is most helpful to develop a document thatdelineates the various sources of the component partsof the patient’s record. Figure 5-2 illustrates this typeof document known as a record transitional template.As the facility moves down the path to a full electronicformat, the document should be modified to reflect thecurrent state of the record. For example, in Figure 5-2,it should be noted that at Sunny Valley Hospital the
Paper Document Name and Number Location Format
Inpatient Face Sheet- MR 001 Patient registration screen electronic
Authorization for Consent to Treatment MR 002 Section 1 of paper record paper
Nursing In-Take- MRN 001 Section 2 of paper record paper
Laboratory Reports- MRL 001- 124 Laboratory report screen 1–55 electronic
Radiology Reports- MRR- 001- 023 Radiology report screen 1–20 electronic
Medication Medication order screen– 1 electronic
Medication Administration Record- MRN-027 Medication administration screen – 1 electronic
Admission History and Physical- MRP-002 Section 2 of paper record paper
Operative Report- MRP-003 Section 3 of paper record paper
Discharge Summary- MRP- 004 Section 4 of paper record paper Nursing Progress Notes- MRN 002 Nursing Bedside screen 1–58 electronic
Preanesthesia Evaluation- MRA- 001 Section 4 of paper record paper
Recovery Room Record- MRA- 002 Surgery Recovery screen electronic
Postanesthesia Evaluation- MRA- 003 Section 4 of paper record paper
Pathology Report- MRN 125- 135 Laboratory report screen 56–75 electronic
Ancillary Reports- MRAR- 1-94 Section 4 of paper record paper
Physical Therapy Report- MRPT- 001-035 Physical Therapy screens 1–21 electronic
Occupational Therapy Report- MROT-001- 021 Occupational Therapy screens 1–16 electronicGraphic Reports- MRN- 039- 55 Graphic Report Generator screens electronic
All reports in paper record are filed in chronological date order within each section.
Figure 5-2 Sunny Valley Hospital Record Transitional Template (Courtesy Delmar/Cengage Learning.)
9781133889731, Essentials of Health Information Management: Principles and Practices, Second Edition, Green/Bowie - © Cengage Learning.
All rights reserved. No distribution allowed without express authorization.

Nursing Intake is currently in paper format. If the facility were to develop this form in an electronic format, the record transitional template would need tobe modified to document this change.
Another issue that should be addressed in facilitypolicy is document completion and the time period inwhich documents can be changed before they are finalsaved as part of the legal record. Facilities need to es-tablish policies that address the management of differ-ent versions of electronic documentation.
EXAMPLE
Sunny Valley Hospital has an electronic health recordthat includes electronic progress notes. After seeing thepatient, the clinical staff documents the progress of thepatient in an electronic note. The note is considered indraft format and needs to be final saved by the clinicianentering the note. If the clinician is called away from thecomputer prior to completion, the system will automati-cally lock down the note after 3 minutes. Since the docu-ment was not final saved by the clinician, the note can becompleted and edited. However, if the note is final saved,the note cannot be edited.
There is more than one manner in which documentsare final saved in electronic systems. It is important forHIM professionals to identify the manner in whichdocuments are final saved and to develop policies thatfacilitate a complete and accurate record. Organiza-tions need to establish policies that delineate the acceptable time period for a document to remain indraft format. After a document is final saved, the doc-ument must not be altered. If the document needs tobe changed after it has been final saved, the correctionneeds to occur following the procedure for record cor-rection, late entry, or amendment. Policies that governcorrections, late entries, and amendments to patientrecords need to be established based on the function-ality of the electronic health record. When subsequentcorrections are made, the original entry will remainwith the corrected version.
Typically, the HIM staff is responsible for ensuringthat all entries are authenticated and final saved. PerThe Joint Commission standards, inpatient hospitalrecords must be completed within 30 days after dis-charge regardless of the storage media of the record. Ina paper system, the documents are reviewed manually,whereas in an electronic system, reports can be gener-ated to identify documents that are not final saved.This demonstrates how the role of HIM professionalshas changed with the adoption of electronic records.In the electronic environment, HIM professionals donot have to manually complete a task; instead, they
have to monitor the task to ensure completion by clinicians.
Another issue that must be considered when transi-tioning to electronic health records is how the recordwill look when it is printed from its electronic format.One of the greatest challenges facing HIM professionalstoday is how to print the entire electronic record whenneeded. HIM and information technology professionalsneed to work cooperatively to develop a hard copy ofthe electronic record.
REGIONAL HEALTH INFORMATIONORGANIZATION
With an increasing number of health care facilities developing electronic health record systems, the net-working of electronic information between facilitieshas become a reality in many areas of the country bythe establishment of regional health information organizations (RHIOs). A regional health informationorganization is an electronic network of patient medicalinformation gathered from multiple health care organ-izations in a geographical region. The goal of the RHIOis to allow health care providers the opportunity to access patient information that was generated at otherfacilities, thus allowing for health information exchange (HIE). RHIOs allow access to multiple typesof patient information such as lab reports, test results, encounter information, and so on, regardless of wherethe patient might have been seen.
The first step in the establishment of an RHIO is fora group of stakeholders to come together to establishthe need for the RHIO and to articulate the vision. Although each stakeholder gains different benefits,successful RHIOs are developed through the collabo-rative efforts of the following stakeholders:
• Hospitals—Benefits for hospitals include reducedadministrative costs, improved patient care, reducedadmission times, improved testing result delivery,and a reduction in medical errors due to increasedavailability of clinical patient information.
• Physicians—Rapid access to patient information occurs when providers use an RHIO. The providercan easily access information that was generated atvarious levels of care, thus streamlining access totimely information.
• Patients—The benefits for patients include compre-hensive documentation of medical information, improved coordination of care, and improved patient safety.
112 • Chapter 5
9781133889731, Essentials of Health Information Management: Principles and Practices, Second Edition, Green/Bowie - © Cengage Learning.
All rights reserved. No distribution allowed without express authorization.

• Health Plans and Insurers—Administrative savingsoccur when health plans and insurers participate inan RHIO because they can more efficiently accessmedical records. A reduction in duplicate testingalso helps to reduce costs.
• Public/Governmental Health Agencies—Participationby this type of stakeholder has been limited at this time; however, there is an increased ability to monitor public health issues through the use of aggregate data.
As RHIOS are established, there are a number of patient information security issues that must be addressed. One of the most important issues is theneed to establish a HIPAA compliant notice of privacypractices (NPP), which will address the exchange ofinformation via the RHIO. The RHIO participants willhave to determine if a separate NPP will be used or ifall RHIO participants will use an NPP designed by theRHIO. Many states now have policies on the writtenconsent of the patient in an RHIO.
EXAMPLE
In New York State, a patient must sign an approved NYSDepartment of Health (DOH) consent form, which willallow the RHIO to exchange patient information for treat-ment purposes when patients are seen at different healthsystems and medical facilities that are participating in theRHIO.
The development of RHIOs has mostly occurred byprivate and nonprofit organizations coming together.With the passage of the American Recovery Reinvest-ment Act of 2009, Public Law 111-5, health informationexchange will be enhanced through funding mecha-nisms and national efforts to develop nationwidehealth information exchange.
Impact of the American RecoveryReinvestment Act, Public Law 111-5At the time of writing, the federal government has justreleased information on the American Recovery Rein-vestment Act. The impact of this act on health infor-mation technology will be a major force in moving theU.S. health care system into the electronic record envi-ronment. Areas that the act will impact include:
• Incentives for adoption of EHRs throughout thehealth care industry
• The advancement of health information exchange(HIE)
• New privacy regulations for both HIPAA and non-HIPAA entities
• HIM workforce opportunities that will expand theopportunities for professionals
The entire Act can be reviewed at:
http://frwebgate.access.gpo.gov/cgi-bin/getdoc.cgi? dbname=111_cong_bills&docid=f%3Ah1enr.txt.pdf
AHIMA has completed the following reports that review the impact of the act on health information technology. The documents can be found at the fol-lowing Web sites:AHIMA review of ARRA can be found at:
http://www.ahima.org/dc/documents/ARRAReview DDAFinal4102009.pdf
AHIMA review of ARRA required reports can be found at:
http://www.ahima.org/dc/documents/AHIMAReviewofARRARequiredReports.pdf
AHIMA analysis of ARRA privacy can be found at:
http://www.ahima.org/dc/documents/AnalysisofARRAPrivacy-fin-3-2009a.pdf
COMPONENTS OF ELECTRONICHEALTH RECORD SYSTEMS USED IN HEALTH CARE
As stated earlier in this chapter, there are numerouselectronic health record systems used in facilities. Re-gardless of the system used, the goal is the same: tocollect, analyze, process, display, and retrieve healthcare data and information.
In any system, the collection of data must occur.Data is defined as raw facts that are not interpreted orprocessed, such as numbers, letters, images, symbols,and sounds. Data is described and organized in a hi-erarchy that begins with the smallest piece of data,known as a character. A character is a lowercase or anuppercase letter, numeric digit, or special character. Agroup of characters forms a field, while a collection ofrelated fields forms a record. A collection of relatedrecords is a file. Examples of a character and field areillustrated in Figure 5-3. Figure 5-3 is a screen that isused at the time of patient registration. The followingareas on the screen represent a field:
Account No, MRN, Name, Address1, Address2.The following represent characters:
The individual numbers of the account number: 1, 0, 6, 0.
Electronic Health Records • 113
9781133889731, Essentials of Health Information Management: Principles and Practices, Second Edition, Green/Bowie - © Cengage Learning.
All rights reserved. No distribution allowed without express authorization.

After data has been collected, it is given meaningand is useful for decision making. Data then becomesinformation.
EXAMPLE
The numbers 120/80 are a form of data, but when we de-fine the numbers as a patient’s blood pressure readingthey become information.
The blood pressure reading also represents healthdata. Health data is health facts that are collected abouta patient or group of patients that describe a health issue.If a facility has collected the blood pressure readings onall patients on the coronary care unit, this would pres-ent health data that relates to this group of patients. Ifthe blood pressure readings were analyzed and givenmeaning, health information would be generated.Health information is defined as health data that hasbeen given meaning and has been processed or organ-ized in a manner that is useful for decision making. Forexample, if the blood pressures of the coronary careunit patients were all found to be higher, this informationwould be clinically relevant and would be used in themedical decision-making process.
Administrative and Clinical ElectronicHealth Record ApplicationsIn all electronic health record applications, there aretwo major components of the system: administrativeand clinical. Administrative applications include patientscheduling, admission/registration, business/financialfunctions, and other management applications. Clinicalapplications include the collection, storage, and displayof clinical information.
One of the basic functions that are found in all systems is the collection of patient demographic andinsurance information. The accuracy of the data col-lected during the patient registration process is essen-tial. This data is entered into screens that are part of a registration-admission-discharge-transfer system(RADT). The application creates a centralized data-base of patient demographic information and has replaced the paper master patient index in the virtualworld. Figures 5-3 and 5-4 illustrate patient intakescreens that collect patient demographic and insur-ance information.
The value of any electronic record system is depen-dent on the clinical applications that exist within the
114 • Chapter 5
Figure 5-3 Patient Registration Screen (Courtesy Delmar/Cengage Learning.)
9781133889731, Essentials of Health Information Management: Principles and Practices, Second Edition, Green/Bowie - © Cengage Learning.
All rights reserved. No distribution allowed without express authorization.

system. For the purpose of this textbook, various typesof clinical applications can be summarized as follows:
• Patient Monitoring Systems—A patient monitoringsystem includes systems that collect and monitorpatient physiological data and record the information.For example, patients’ vital signs are monitored inintensive care units via patient monitoring systems.These systems allow for the continuous monitoringand collection of vital signs. Alerts will occur if thepatient’s vital signs are abnormal.
• Pharmacy Applications—Pharmacy applicationsautomate various aspects of the processing of patientmedications. The following functions can be includedin pharmacy applications: order entry, identificationof drug interactions, pharmacist review, medical labelprinting, and pharmacy administrative reports suchas inventory control and drug usage.
• Laboratory Applications—Automation of labora-tory functions include the processing of laboratoryorders and the management of the laboratory func-tions. The basic functions include the ordering oftests, the reporting of test results, and report gener-ation. Many laboratory applications provide test re-sults to providers via electronic health information
exchange. This function allows the provider to viewtest results from remote locations.
• Radiology Applications—The functions of radiologyapplications include the ordering of tests, the creationof radiological images, reporting of test results, andvarious administrative functions. With the shortageof radiologists, systems have been developed thatallow radiological images to be taken at a facilityand the image reviewed by a radiologist who is at another location. The reports are then electroni-cally generated and can be accessed by the orderingfacility.
• Nursing Applications—There are numerous nurs-ing applications that are used to support both theclinical and administrative nursing functions. Auto-mated clinical functions include the developmentof nursing intake assessments, documentation ofnursing care, ongoing assessments of patients, med-ication administrative records, and various othercharting functions. Many administrative nursingactivities are also imbedded in electronic nursingapplications and vary depending on the functionalityof the system. Nursing management applicationscan include reports on late dosing of medications,infection rates, nursing response times, assessments
Electronic Health Records • 115
Figure 5-4 Patient Registration Insurance Screen (Courtesy Delmar/Cengage Learning.)
9781133889731, Essentials of Health Information Management: Principles and Practices, Second Edition, Green/Bowie - © Cengage Learning.
All rights reserved. No distribution allowed without express authorization.

on the quality of nursing services, and personnel resource management.
• Medical Documentation Applications—Medicaldocumentation applications include a multitude ofcharting functions including progress note documen-tation, medication and diagnostic profiles, treatmentplanning, and the tracking of patient vital signs toname a few. Figure 5-5 illustrates a screen that is usedto collect a past medical history on a patient, andFigure 5-6 illustrates a screen that is used to collectinformation recorded at the time of a patient exam.
Health information professionals must have a basicunderstanding of the various applications that exist tobe an active participant in the selection of electronicrecord systems. Transitioning to electronic record sys-tems is an evolving process that can take years to ac-complish within an organization. There are numerouschallenges that will have to be met, but the end resultwill positively impact patient care and the delivery ofhealth care.
INTERNET LINKS
To review AHIMA practice briefs on electronic recordtopics, visit www.ahima.org. On the home page, click on HIM RESOURCES AND THEN PRACTICE BRIEFS/TOOLS, thenclick on E-HIM AND ELECTRONIC RECORDS. Here, there are 50documents regarding electronic record topics.Visit www.cpsr.org the home page of Computer Professionalsfor Social Responsibility. On this site, search the term“medical records.” Numerous articles will then display.
The Office of the National Coordinator for Health Information Technology provides counsel to the Secretaryof HHS and departmental leadership for the developmentand nationwide implementation of an interoperable healthinformation technology infrastructure. To obtain informationon this office, visit: www.hhs.gov/healthit/onc/mission.
To learn more about RHIOs, log on to wwwg.rrhio.org.This is the home page for the Rochester Regional Health Information Organization, which was developed by and fordoctors, hospital systems, health insurers, and privacy offi-cers in the nine-county Greater Rochester New York area.
Visit http://www.ehealthinitiative.org/ for the latestupdates on national eHealth initiatives.
116 • Chapter 5
Figure 5-5 Past Medical History Screen (Courtesy Delmar/Cengage Learning.)
Figure 5-6 Patient Exam Screen (Courtesy Delmar/Cengage Learning.)
9781133889731, Essentials of Health Information Management: Principles and Practices, Second Edition, Green/Bowie - © Cengage Learning.
All rights reserved. No distribution allowed without express authorization.
SUMMARY
The terms “computerized patient records,” “electronicpatient records,” and “electronic health records” allhave unique meanings and define various stages ofautomated health record systems. Transitioning recordsfrom a paper format to electronic formats presents thehealth care industry with many development and implementation issues. The exchange of health care information will continue to be enhanced by the de-velopment of regional health information organizationsand other federal initiatives. Each facility has to establisha plan for the integration of electronic administrativeand clinical applications.
STUDY CHECKLIST
• Read the textbook chapter, and highlight key con-cepts. (Use colored highlighter sparingly throughoutthe chapter.)
• Create an index card for each key term. (Write the keyterm on one side of the index card and the concepton the other. Learn the definition of each key term,and match the term to the concept.)
• Access chapter Internet links to learn more aboutconcepts.
• Answer the chapter Exercises and Review Questions,verifying answers with your instructor.
• Complete the chapter StudyWare activities.• Complete WebTutor assignments and take online
quizzes.• Complete the lab manual assignments verifying
answers with your instructor.• Form a study group with classmates to discuss
chapter concepts in preparation for an exam.
CASE STUDY
Assume that you are the health information manage-ment director of Sunny Valley Hospital. Currently,the medical record system is a paper-based system.The CEO of the facility would like to explore theselection and implementation of an electronic healthrecord. The CEO has determined that a planningteam needs to be established to explore electronicrecord systems and has asked you to respond to thefollowing questions:
1. What disciplines should be represented on theplanning team?
2. Do you feel that you could act as the chairpersonfor the planning team? Explain your answer.
3. What questions/issues need to be a part of the initialinvestigation of the selection and implementationof an electronic health record?
CHAPTER REVIEW
True/False: Indicate whether each statement is True(T) or False (F).
1. According to the IOM’s 1991 study, the health careindustry’s development of automated systemswas fast paced.
2. A patient monitoring system includes systemsthat collect patient demographic information.
3. Electronic health records will improve care and reduce medical mistakes and costs.
4. Per The Joint Commission standards, inpatienthospital records must be completed within 30 days after discharge for paper records andwithin 20 days for electronic records.
5. The benefits of electronic health data exchange forpatients include comprehensive documentation ofmedical information, improved coordination ofcare, and improved patient safety.
Multiple Choice: Select the most appropriate response.
6. Which of the following is not an administrativeapplication of an electronic record system?a. admission/registrationb. business/financial functionsc. patient schedulingd. pathology reports
7. In the period 1970–1980, the term ________ wasused to describe the early medical record automa-tion attempts.a. computerized medical recordsb. electronic medical recordc. longitudinal health recordd. personal health record
8. Which term was used starting in the late 1990s to describe systems that were based on imaging andthe merging of data from various stand-alone systems?a. computerized medical recordsb. electronic medical record
Electronic Health Records • 117
9781133889731, Essentials of Health Information Management: Principles and Practices, Second Edition, Green/Bowie - © Cengage Learning.
All rights reserved. No distribution allowed without express authorization.

c. longitudinal health recordd. personal health record
9. An electronic or paper medical record maintainedand updated by individuals for their own personaluse is known as a(n)a. computerized medical record.b. electronic medical record.c. longitudinal health record.d. personal health record.
10. A system that collects and monitors patient phys-iological data and records the information isknown as a(n)a. nursing clinical application.b. patient monitoring system.c. physiological application.d. electronic monitoring system.
11. Which of the following is not a benefit of the establishment of an RHIO for patients?a. comprehensive documentation of medical
informationb. decreased waiting time to see providersc. improved coordination of cared. improved patient safety
12. Sunny Valley Hospital has purchased an applicationthat includes the following functions: order entry,identification of drug interactions, medical labelprinting, and administrative reports such as drugusage. This type of application is known as a(n)a. drug application.b. medical documentation application.c. pharmacy application.d. order-entry application.
13. Raw facts that are not interpreted or processed,such as numbers, letters, images, symbols, andsounds, are referred to asa. characters.b. data.c. information.d. fields.
14. A group of characters form a ________.a. field.b. file.c. record.d. screen.
15. Records that are part paper and part electronic areknown asa. computerized medical records.b. hybrid records.c. longitudinal records.d. personal health records.
Short Answer: Briefly respond to each question.
16. Compare and contrast the advantages and dis-advantages of paper and automated recordssystems.
17. Outline the steps that should be taken to preparedocuments for scanning.
18. Discuss how health information professionals cancontribute to the transition to electronic recordsystems.
19. Summarize the impact of electronic health infor-mation exchange on the quality of patient care.
20. List and discuss three electronic clinical applications.
118 • Chapter 5
9781133889731, Essentials of Health Information Management: Principles and Practices, Second Edition, Green/Bowie - © Cengage Learning.
All rights reserved. No distribution allowed without express authorization.