elective groin irradiation is not indicated for patients with adenocarcinoma of the rectum extending...
TRANSCRIPT

PII S0360-3016(01)01687-X
CLINICAL INVESTIGATION Anal Canal
ELECTIVE GROIN IRRADIATION IS NOT INDICATED FOR PATIENTSWITH ADENOCARCINOMA OF THE RECTUM EXTENDING TO THE
ANAL CANAL
NOAH TAYLOR, M.D.,* CHRISTOPHERCRANE, M.D.,* JOHN SKIBBER, M.D.,† BARRY FEIG, M.D.,†
LEE ELLIS, M.D.,† JEAN-NICHOLAS VAUTHEY, M.D.,† STANLEY HAMILTON , M.D.,‡
KAREN CLEARY, M.D.,‡ RONELLE DUBROW, M.D.,§ THOMAS BROWN, M.D.,� ROBERT WOLFF, M.D.,�
PAULO HOFF, M.D.,� NICHOLAS SANFILIPPO, M.D.,¶ AND NORA JANJAN, M.D.*
Departments of *Radiation Oncology,†Surgical Oncology,‡Pathology,§Diagnostic Imaging, and�Medical Oncology, University ofTexas M. D. Anderson Cancer Center, Houston, TX;¶Department of Radiation Oncology, University of Pennsylvania, Philadelphia, PA
Purpose: To evaluate the inguinal nodal failure rate in patients with locally advanced rectal cancer with analcanal involvement (ACI) treated with pelvic chemoradiation without elective inguinal irradiation.Methods and Materials: From 1990 and 1998, 536 patients received preoperative or postoperative chemoradia-tion for rectal cancer with curative intent; 186 patients had ACI (<4 cm from the anal verge on rigidproctoscopy). Two patients had positive inguinal nodes at presentation. Chemoradiation was delivered preop-eratively (45 Gy in 25 fraction) or postoperatively (53 Gy in 29 fractions) with concurrent continuous infusion of5-fluorouracil (300 mg/m2/d). The inguinal region was specifically irradiated in only 2 patients who haddocumented inguinal nodal disease.Results: The median follow-up was 50 months. Only 6 of 184 ACI patients who had clinically negative inguinalnodes at presentation developed inguinal nodal recurrence (5-year actuarial rate 4%); 4 of the 6 cases wereisolated. Two patients underwent successful salvage. Only 1 died of uncontrolled groin disease. Local control wasachieved in both patients with inguinal nodal disease at presentation, but both died of metastatic disease. Only3 patients with tumors >4 cm from the verge developed inguinal recurrence (5-year actuarial rate <1%).Conclusions: Inguinal nodal failure in rectal cancer patients with ACI treated with neoadjuvant or adjuvantchemoradiation is not high enough to justify routine elective groin irradiation. © 2001 Elsevier Science Inc.
Rectal cancer, Lymphatic metastases, Chemoradiation, Inguinal nodes, Anal canal.
INTRODUCTION
The primary lymphatic drainage of the rectum is to theperirectal and pelvic lymph nodes (1–3). Inguinal lymphnode metastases from rectal adenocarcinoma are rare andare usually associated with locally advanced disease (4).Drainage to the groin has been reported in patients withsignificant lymphatic involvement (5). However, direct lym-phatic drainage from the anal canal to the groin regions mayoccur (6). Therefore, low rectal cancer with anal canalinvolvement (ACI) has been postulated to metastasize to thegroin nodes, even in patients with small primary tumors (7).
Adjuvant or neoadjuvant chemoradiation plays an impor-tant role in the treatment of patients with Stage II or IIIrectal cancer (8). The perirectal and pelvic lymph noderegions are included in standard radiotherapy (RT) treat-ment fields. Considering the potential for lymphatic drain-
age of the anal canal to the inguinal lymph nodes, somehave advocated routine elective irradiation of these regions(9, 10). This is supported by the experience in the treatmentof squamous cell anal carcinoma, in which coverage of thegroin regions is recommended because of findings of sig-nificant recurrence rates in these nodal stations withoutelective treatment (11–14). Additionally, the salvage rate ofinguinal metastases from rectal adenocarcinoma has beenreported to be poor (7, 15).
Inguinal recurrence can be prevented using RT (9), butnot without severe acute morbidity in most patients. Thetreatment techniques must be altered to include the groinnodes. The anterior and posterior fields must be used to treatthese areas, which leads to an increase in normal tissueirradiation and subsequent acute reactions involving theskin, small bowel, and genitalia. Abdominal wound com-plications may also increase (16, 17).
Reprint requests to: Christopher Crane, M.D., Department ofRadiation Oncology, Box 97, University of Texas M. D. AndersonCancer Center, 1515 Holcombe Blvd., Houston, TX 77030. Tel:(713) 792-0782; Fax: (713) 794-5573; E-mail: [email protected]
Presented at the 86th Scientific Assembly and Annual Meetingof the Radiological Society of North America, Chicago, IL, No-vember 2000.
Received Mar 13, 2001, and in revised form May 11, 2001.Accepted for publication May 19, 2001.
Int. J. Radiation Oncology Biol. Phys., Vol. 51, No. 3, pp. 741–747, 2001Copyright © 2001 Elsevier Science Inc.Printed in the USA. All rights reserved
0360-3016/01/$–see front matter
741
No published reports in the literature define the groinfailure rate in this population. Our policy at the Universityof Texas M. D. Anderson Cancer Center has been to notinclude the inguinal lymph node regions routinely whentreating adenocarcinoma of the low rectum using chemora-diation. The prognosis for, and treatment of, patients withinguinal metastases are well described (4, 7, 15), but the trueincidence of inguinal lymph node involvement in patientswho had low rectal cancer treated using adjuvant chemora-diation without elective groin irradiation is unknown.Therefore, we performed a retrospective analysis of allpatients who received chemoradiation for rectal cancer ex-tending to the anal canal at M.D. Anderson Cancer Centersince 1990 to determine the groin failure rate and subse-quently whether elective groin irradiation is indicated.
METHODS AND MATERIALS
From 1990 and 1998, 536 patients who had Stage II, III,or IV rectal adenocarcinoma received adjuvant or neoadju-vant chemoradiation with curative intent at the M. D.Anderson Department of Radiation Oncology. Only patientswho had either localized disease or surgically curable met-astatic disease were included. The anal canal was involvedin 186 of the 536 patients. The anal canal was defined astumor extension �4 cm from the anal verge on rigid proc-toscopy or digital rectal examination. If the assessments ofthe lower extent of the tumor were discordant, the rigidproctoscopy distance was used. A retrospective analysis ofthe medical records and follow-up data of all 536 patientswas performed. Patients with ACI were compared withpatients without ACI.
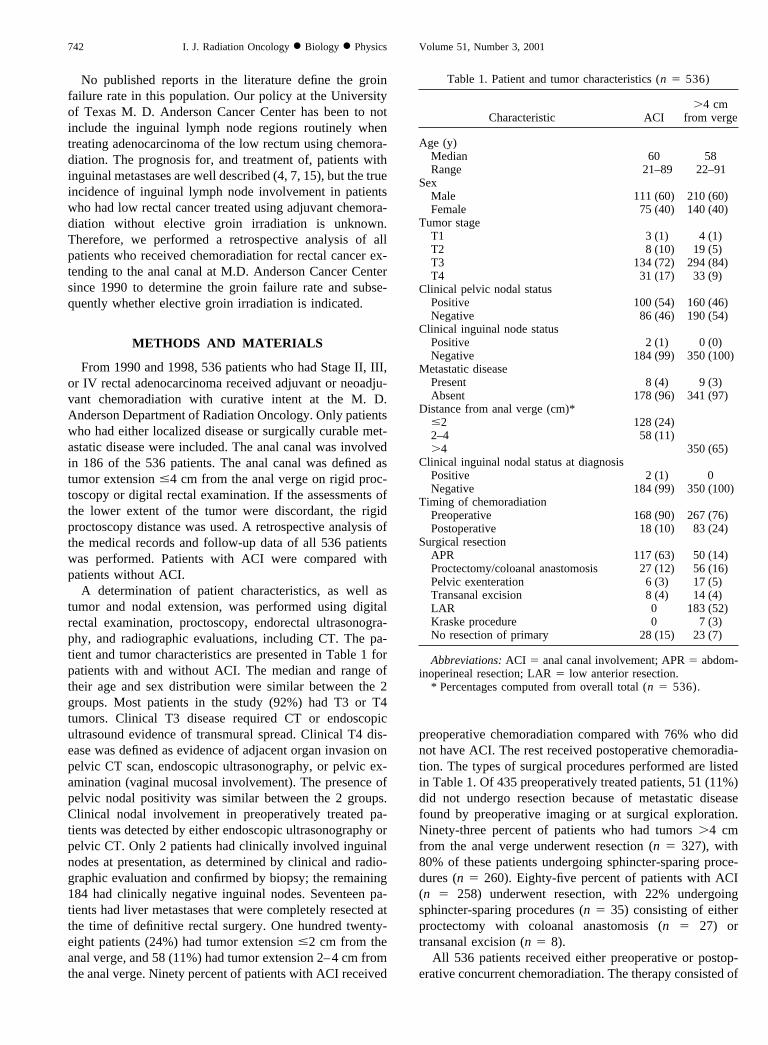
A determination of patient characteristics, as well astumor and nodal extension, was performed using digitalrectal examination, proctoscopy, endorectal ultrasonogra-phy, and radiographic evaluations, including CT. The pa-tient and tumor characteristics are presented in Table 1 forpatients with and without ACI. The median and range oftheir age and sex distribution were similar between the 2groups. Most patients in the study (92%) had T3 or T4tumors. Clinical T3 disease required CT or endoscopicultrasound evidence of transmural spread. Clinical T4 dis-ease was defined as evidence of adjacent organ invasion onpelvic CT scan, endoscopic ultrasonography, or pelvic ex-amination (vaginal mucosal involvement). The presence ofpelvic nodal positivity was similar between the 2 groups.Clinical nodal involvement in preoperatively treated pa-tients was detected by either endoscopic ultrasonography orpelvic CT. Only 2 patients had clinically involved inguinalnodes at presentation, as determined by clinical and radio-graphic evaluation and confirmed by biopsy; the remaining184 had clinically negative inguinal nodes. Seventeen pa-tients had liver metastases that were completely resected atthe time of definitive rectal surgery. One hundred twenty-eight patients (24%) had tumor extension �2 cm from theanal verge, and 58 (11%) had tumor extension 2–4 cm fromthe anal verge. Ninety percent of patients with ACI received
preoperative chemoradiation compared with 76% who didnot have ACI. The rest received postoperative chemoradia-tion. The types of surgical procedures performed are listedin Table 1. Of 435 preoperatively treated patients, 51 (11%)did not undergo resection because of metastatic diseasefound by preoperative imaging or at surgical exploration.Ninety-three percent of patients who had tumors �4 cmfrom the anal verge underwent resection (n � 327), with80% of these patients undergoing sphincter-sparing proce-dures (n � 260). Eighty-five percent of patients with ACI(n � 258) underwent resection, with 22% undergoingsphincter-sparing procedures (n � 35) consisting of eitherproctectomy with coloanal anastomosis (n � 27) ortransanal excision (n � 8).
All 536 patients received either preoperative or postop-erative concurrent chemoradiation. The therapy consisted of
Table 1. Patient and tumor characteristics (n � 536)
Characteristic ACI�4 cm
from verge
Age (y)Median 60 58Range 21–89 22–91
SexMale 111 (60) 210 (60)Female 75 (40) 140 (40)
Tumor stageT1 3 (1) 4 (1)T2 8 (10) 19 (5)T3 134 (72) 294 (84)T4 31 (17) 33 (9)
Clinical pelvic nodal statusPositive 100 (54) 160 (46)Negative 86 (46) 190 (54)
Clinical inguinal node statusPositive 2 (1) 0 (0)Negative 184 (99) 350 (100)
Metastatic diseasePresent 8 (4) 9 (3)Absent 178 (96) 341 (97)
Distance from anal verge (cm)*�2 128 (24)2–4 58 (11)�4 350 (65)
Clinical inguinal nodal status at diagnosisPositive 2 (1) 0Negative 184 (99) 350 (100)
Timing of chemoradiationPreoperative 168 (90) 267 (76)Postoperative 18 (10) 83 (24)
Surgical resectionAPR 117 (63) 50 (14)Proctectomy/coloanal anastomosis 27 (12) 56 (16)Pelvic exenteration 6 (3) 17 (5)Transanal excision 8 (4) 14 (4)LAR 0 183 (52)Kraske procedure 0 7 (3)No resection of primary 28 (15) 23 (7)
Abbreviations: ACI � anal canal involvement; APR � abdom-inoperineal resection; LAR � low anterior resection.
* Percentages computed from overall total (n � 536).
742 I. J. Radiation Oncology ● Biology ● Physics Volume 51, Number 3, 2001

45 Gy administered to the pelvis preoperatively (435 pa-tients) or 53 Gy administered postoperatively (101 patients)using 18 MV photons at 1.8 Gy/fraction with a 3-field bellyboard technique and concurrent continuous infusion of5-fluorouracil. 5-Fluorouracil was prescribed at 300 mg/m2/d administered 5 d/wk during RT and delivered usingelectromechanical pumps.
The weighting of the treatment fields was 2:1:1 for theposterior, right lateral, and left lateral fields; 45° wedgeswere used in the lateral fields. The RT dose was prescribedto the 95% isodose line. The superior border of the pelvicfield was placed at the L5–S1 interspace, and the inferiorborder was placed 4–5 cm distal to the tumor. The inferiorborder was always at or below the obturator foramen. Inaddition, the lateral borders of the posterior field wereplaced 1.5 cm outside the true bony pelvis. The lateral RTfields included the sacrum and coccyx posteriorly, and theanterior border was placed 1–2 cm posterior to the pubisinferiorly and 2–3 cm anterior to the sacral promontorysuperiorly.
Four patients were treated with anterior–posterior portalsbecause of anterior extension of their disease. Also, bothpatients with documented inguinal nodal disease at presen-tation were treated with anterior–posterior fields in thesupine position followed by a 3-field technique; electronswere used to boost the involved groin. Additionally, 11patients received a boost given concomitantly with a 6-hourinterfraction interval during the last week of chemoradia-tion, on a Phase II protocol. The boost consisted of 7.5 Gyin 5 fractions and was given to gross disease with a 2-cmmargin prescribed to the 95% isodose line.
The actuarial rate of inguinal nodal recurrence in thecohort who had low rectal cancer, stratified by tumor ex-tension �2 cm or 2–4 cm from the anal verge, was theprimary endpoint. The pelvic failure rate of all resectedpatients, stratified by the presence or absence of ACI, wasthe secondary endpoint. All endpoints were calculated usingthe Kaplan–Meier method, and statistical significance wasdetermined using the log–rank test.
RESULTS
Follow-upThe median follow-up in ACI patients who survived was
50 months (range 3–112) and was 42 months (range 2–112)for all 186 patients. Of those who had tumors �4 cm fromthe anal verge, the median length of follow-up was 49months (range 2–133) in surviving patients and 42 months(range 2–133) in all patients.
Inguinal nodal recurrenceOnly 6 patients (3%) who had tumors with ACI and
clinically negative inguinal nodes at presentation developedinguinal nodal recurrence (Table 2). The 5-year actuarialrate of inguinal recurrence was 4%. Four of these failureswere isolated, 2 were synchronous with the appearance oflocal recurrence and, in 1 of these 2, distant metastaticdisease. Five patients who had recurrence had T3 disease,and 1 had T4 disease. Also, 3 patients had positive pelvicnodes at presentation. The primary tumor was located belowthe dentate line (defined as �2 cm from the anal verge) in5 patients, and 2–4 cm from the anal verge in 1 patient
Table 2. Characteristics and outcomes of patients with inguinal recurrence (primary �4 cm from anal verge)
Pt. No.
Primarytumorstage
Nodalstatus
Primarytumor
location(cm)
Inguinal failurepattern Treatment
Follow-up after
INR(mo) Outcome
1 T3 N0 2–4 Isolated Chemo-RT 54 Died ofintercurrentdisease
2 T3 N1 �2 Isolated None 6 Died ofuncontrolledgroindisease
3 T3 N1 �2 Simultaneouslocal anddistant
Chemo-RT 8 Died ofmetastaticrectalcancer
4 T3 N1 �2 Simultaneouslocal only
Chemo-RT 29 Died ofmetastaticrectalcancer
5 T3 N0 �2 Isolated Chemo-RT 28 Alive withrectalcancer
6 T4 N0 �2 Isolated Chemo-RT 61 Alive, NED
Abbreviations: Pt. No. � Patient number; Chemo-RT � chemotherapy and radiotherapy; INR � inguinal recurrence; NED � no evidenceof disease.
743Elective groin irradiation in low rectal cancer ● N. TAYLOR et al.

(5-year actuarial inguinal failure rate 4% and 2%, respec-tively).
Salvage therapy consisted of RT delivered to the groinfollowed by systemic chemotherapy in 3 of the patients withisolated inguinal recurrence. All 3 achieved local control inthe groin. Salvage treatment was successful in 2 of these 3patients. One had no evidence of disease at 61 months aftersalvage therapy and the other died of intercurrent disease 54months after salvage therapy without evidence of rectalcancer. The third patient eventually developed distant met-astatic disease and was alive with disease 28 months aftersalvage therapy. This patient was also the only patient withisolated groin failure to subsequently develop local (pelvic)failure. The only other patient with isolated inguinal failurehad a delay in presentation of her recurrent disease afterelecting to be followed at another institution. The mass wasunresectable, no salvage was attempted, and the patient diedof rectal cancer with uncontrolled groin disease. The 2patients with inguinal failure and synchronous local and/ordistant failure died of disease with symptomatic control inthe pelvis and groin after salvage chemoradiation.
Both patients with inguinal nodal disease at presentationachieved local control in the pelvis and inguinal regionsafter preoperative chemoradiation and definitive surgery.However, they both developed metastatic disease and dieddespite receiving aggressive systemic chemotherapy.
Only 3 patients with tumors �4 cm from the anal vergedeveloped inguinal recurrence (5-year actuarial rate �1%).In all 3, the appearance of inguinal metastases was synchro-nous with local failure in the pelvis. In 2, it was synchro-nous with distant metastatic disease. Salvage treatment withchemoradiation was attempted in only 1 patient. All 3patients died of rectal cancer.
Local control and overall survivalOverall, 27 resected patients who had tumors with ACI
developed pelvic recurrences (Fig. 1A). The 5-year actuarialrate of local control in these patients was 81% comparedwith 92% in patients who had tumors �4 cm from the analverge (p � 0.007). This significant difference in local con-trol was explained at least in part by the poor control in ACIpatients who had T4 tumors. Among patients who hadT1–T3 tumors, the local control rate was 86% at 5 years inthose who had low rectal cancer (ACI) resected comparedwith 91% in those who had tumors �4 cm from the analverge resected (p � 0.10, Fig. 1B). However, among pa-tients who had T4 primary tumors, the local control wassignificantly worse in those resected patients who had ACIcompared with those who had tumors �4 cm from the analverge (p � 0.01, Fig. 1C). The sites of pelvic failure, otherthan the inguinal nodes, for resected patients with ACIincluded the rectum and presacral tissues in 8 patients,pelvic viscera in 4 patients (2 in the bladder, 1 in theprostate, and 1 in the vagina), pelvic nodes in 9 patients, andthe surgical anastomotic site in 2 patients. Forty-six patientswith ACI developed metastatic disease, and 57 have died.
The 5-year actuarial overall survival rate in all patients withACI was 65%.
DISCUSSION
Inguinal lymph node metastases from rectal adenocarci-noma are rare. The mechanism of metastasis to the inguinalnodes has been postulated to be retrograde lymphatic flowfrom bulky pelvic disease (7, 18). However, it has also beenpostulated that involvement of the anal canal by rectalcancer, even with minimal disease, may provide directaccess to the inguinal nodes and that this may be a signif-icant site of recurrence (7). Additionally, primary squamouscell carcinoma of the anal canal has been found to have asignificant rate of inguinal recurrence in the absence ofelective treatment (19). For this reason, some have advo-cated elective irradiation of the inguinal nodes in patientswith rectal cancer involving the anal canal (9). In a study bythe University of Florida (10), all patients who had pelvictumors and a perceived high incidence of groin failurereceived RT that included coverage of the bilateral inguinalregions. Thirty-four patients who had low rectal adenocar-cinoma treated using adjuvant RT were analyzed; none ofthe patients experienced groin failure after elective irradia-tion. The authors concluded that elective irradiation of thegroin is indicated and can be delivered with acceptablemorbidity. However, that study did not address the inci-dence of failure without elective treatment.
Before the current study, the incidence of groin failure inpatients with adenocarcinoma of the rectum extending to theanal canal who had not received elective treatment had notbeen established. Previous studies focused only on the prog-nosis and treatment of patients with inguinal recurrence. Forexample, Tocci et al. (15) reported on a series of 21 patientswho had inguinal metastases, Graham and Hohn (7) re-ported on a series of 40 patients, and Mesko et al. reportedon a series of 18 patients (4). These studies included patientswith tumors located a variety of distances from the analverge and did not address the inguinal failure rate for rectalcancer involving the anal canal. Although we also observedgroin recurrences from primary tumors located at a varietyof distances from the anal verge, higher tumors only rarelyrecurred in the groin. Four percent of patients with ACI,compared with �1% of patients with original primary dis-ease above the anal canal, developed inguinal recurrences.In the latter group, inguinal metastases only occurred withsynchronous local recurrence. Altered lymphatic drainagedue to obstruction by tumor or previous surgery couldexplain this unusual pattern of spread.
Additionally, recent studies have shown a relatively low(�10%) rate of inguinal failure in patients with squamouscell carcinoma of the anal canal and clinically negativegroin nodes at diagnosis, contradictory to previous reports(20). In the present study, we found the incidence of isolatedinguinal metastases from low rectal cancer to be surpris-ingly low (2%).
Inguinal nodal recurrences have been reported to carry a
744 I. J. Radiation Oncology ● Biology ● Physics Volume 51, Number 3, 2001

grave prognosis (21). Only isolated incidences of long-termsurvival in patients presenting with inguinal metastasesfrom rectal cancer have been reported. Specifically, Tocci etal. (15) found a median survival of 14.8 months in patientswho developed inguinal metastases after definitive treat-ment of rectal cancer, with no patient surviving �4 years. Inaddition, Avill (22) reported only 1 patient who had noevidence of disease 12 years after groin dissection andsystemic chemotherapy for inguinal metastasis. Of 18 totalpatients who had rectal cancer and groin failure, Mesko etal. (4) found 1 long-term survivor at 50 months of follow-up. However, as stated above, these reports included rectalcancer patients who had significant local disease and a pooroverall prognosis. In contrast, Graham and Hohn (7) iden-tified a group of patients with low rectal cancer (medianprimary distance from the anal verge 3.5 cm) who devel-oped inguinal recurrence, without synchronous or meta-chronous pelvic recurrence, in whom 2 of 8 had long-termdisease-free survival. Additionally, Tocci et al. (15) re-ported that the median survival was significantly longer inpatients presenting with inguinal metastases �1 year afterinitial diagnosis compared with those presenting with ingui-nal metastases within 1 year or those who had inguinalinvolvement at diagnosis. In the present study, 2 of the 4patients who developed isolated inguinal recurrences weresalvaged, and inguinal disease was controlled in 8 of 9inguinal recurrences. The only patient who died with un-controlled groin disease had a significant delay in presen-tation with recurrent disease, and salvage was not at-tempted. Thus, it is possible to salvage isolated inguinalrecurrences.
Although inguinal recurrence can be prevented with elec-tive irradiation, any potential benefit of elective irradiationmust be compared with the potential cost in terms of mor-bidity. Because the isolated inguinal failure rate is low andsalvage possible, the morbidity must be very low if electivetreatment is to be justified. Irradiation of the groin region,even with low doses, as is the standard in patients withsquamous cell carcinoma of the anus, is associated withsignificant morbidity (14, 23). For instance, of 164 patientswho had pelvic tumors who underwent irradiation of thegroins, Lee et al. (9) reported common acute inguinal com-
Fig. 1. (A) Pelvic control in patients with T1–T4 rectal cancer whounderwent resection, stratified by ACI (top curve, �4 cm fromanal verge; bottom curve, �4 cm from anal verge). Five-yearactuarial rate of local control was 81% for tumors with ACI versus92% for patients with tumors �4 cm from the anal verge (p �0.007). (B) Pelvic control in patients with T1–T3 rectal cancer whounderwent resection, stratified by ACI (top curve, �4 cm fromanal verge; bottom curve, �4 cm from anal verge). Five-yearactuarial rate of local control was 86% for tumors with ACI versus91% for patients with tumors �4 cm from the anal verge (p �0.10). (C) Pelvic control in patients with T4 rectal cancer whounderwent resection, stratified by ACI (p � 0.01). The poor pelviccontrol in resected T4 patients who had ACI represented a sub-stantial proportion of the difference in local control in all resectedpatients stratified by primary tumor distance from the anal verge.
745Elective groin irradiation in low rectal cancer ● N. TAYLOR et al.

plications, including moist desquamation of the skin andgenital edema, and late complications (inguinal fibrosis andfemoral neck fractures) that were attributed to groin irradi-ation in 13 patients. Leg edema is also a potential, albeitrare, complication (24). Additionally, potential increases ingenital, bowel, and abdominal wound complications mayoccur because of alterations in RT techniques to include thegroin.
Accurate identification of the few patients with pelvictumors and subclinical disease in the groin at diagnosiswould be valuable. These patients would benefit from elec-tive groin irradiation and the others would be spared themorbidity of RT. Recent experience in the use of sentinelnode biopsy of the groin at diagnosis for patients with analcancer has been reported (20). Twelve percent of the pa-tients who had clinically negative groin nodes were found tohave positive sentinel nodes. This technique is interestingbut remains investigational for the identification of subclin-ical inguinal disease in this setting. The added cost andmorbidity risk of this procedure for adenocarcinoma of therectum extending to the anal canal would certainly not bewarranted because of the probable low yield indicated bythis analysis.
We found a higher rate of overall pelvic failure in patientswho had tumors �4 cm from the anal verge despite the useof chemoradiation and an aggressive surgical approach.Most of these failures were in-field. The overall failure ratewas high partially because of a high pelvic failure rateamong patients with low T4 tumors. However, the rate oflocal control in the present study is comparable to otherreports in the literature (25, 26).
The pelvic failure rate in the subset of patients withlow rectal cancer was significantly higher than the failurerate in patients who had tumors �4 cm from the analverge. This difference was only partially explained by thehigher inguinal failure rate in patients who had low rectaltumors. Elective inguinal coverage in these cases wouldhave potentially prevented only the 4 isolated local fail-ures and subsequently less than one quarter of the differ-ence in absolute recurrences between the high and lowrectal tumors. Previous studies have shown a higher localfailure rate for low rectal cancer than for middle andproximal tumors (27). This difference was postulated tobe due to the increased difficulty in obtaining wide sur-gical margins, easier perirectal/nodal spread, and higher
stage tumors. Patients who had a T4 primary tumor andlow rectal cancer had particularly poor pelvic control.The disease characteristics of these patients were respon-sible for a large part of the difference in local control inrelation to the distance from the anal verge. This may bepartially explained as a function of tumor size and extent:bulky T4 rectal tumors that invade adjacent organs oftenextend into the anal canal as well.
Finally, isolated recurrence in the inguinal nodes in thepresent study represented 4 (15%) of 27 locoregionalfailures in patients with ACI. With the potential futurereduction of the in-field failure rate using RT dose esca-lation or improved radiosensitizing chemotherapy, theisolated marginal failure in the groin, such as was seen inthis study, may become proportionally greater. With thisreduction in the competing risk of in-field failure, routineelective irradiation of the inguinal regions may, thus,become more important. Should the morbidity of electivegroin irradiation be simultaneously reduced, its use maybecome more reasonable. The use of intensity-modulatedRT techniques to spare the volume of skin folds, externalgenitalia, and small bowel irradiated when the inguinalnodes are included in the treatment ports has been re-cently reported (28); this strategy shows promise in po-tentially reducing the acute and long-term toxicities.However, until such strategies are widely implemented,the morbidity of standard pelvic RT that includes theinguinal nodes in the treatment ports outweighs any po-tential benefit of this elective treatment.
Our treatment policy at M. D. Anderson during the past10 years has been to not electively irradiate the groinregions in patients with low rectal adenocarcinoma treatedwith either preoperative or postoperative chemoradiation. Inthe present study, we tested this hypothesis by reviewing thepattern of failure in 536 patients and found that the inci-dence of groin failure in this population was low (4%).Furthermore, the isolated groin failure rate was only 2%,one half of which were salvaged.
In conclusion, the overall rate of inguinal nodal failurein patients with rectal adenocarcinoma extending to theanal canal treated using neoadjuvant or adjuvant chemo-radiation without elective inguinal irradiation is low. Themorbidity of elective groin irradiation is significant.Therefore, routine elective groin irradiation is not justi-fied in these patients.
REFERENCES
1. Gilchrist R, David V. A consideration of pathological factorsinfluencing five year survival in radical resection of the largebowel and rectum for carcinoma. Ann Surg 1947;126:421–438.
2. Grinnell RS. The lymphatic and venous spread of carcinomaof the rectum. Ann Surg 1942;116:200–216.
3. Hojo K, Koyama Y, Moriya Y. Lymphatic spread and itsprognostic value in patients with rectal cancer. Am J Surg1982;144:350–354.
4. Mesko TW, Rodriguez-Bigas MA, Petrelli NJ, et al. Inguinal
lymph node metastases from adenocarcinoma of the rectum.Am J Surg 1994;168:285–287.
5. Huddy SP, Husband EM, Cook MG, et al. Lymph nodemetastases in early rectal cancer. Br J Surg 1993;80:1457–1458.
6. Bykov SA, Metelev VV. Intravital study of lymph outflow inrectal cancer. Vopr Onkol 1989;35:1059–1062.
7. Graham RA, Hohn DC. Management of inguinal lymph nodemetastases from adenocarcinoma of the rectum. Dis ColonRectum 1990;33:212–216.
746 I. J. Radiation Oncology ● Biology ● Physics Volume 51, Number 3, 2001

8. Freedman GM, Coia LR. Adjuvant and neoadjuvant treatmentof rectal cancer. Semin Oncol 1995;22:611–624.
9. Lee WR, McCollough WM, Mendenhall WM, et al. Electiveinguinal lymph node irradiation for pelvic carcinomas: TheUniversity of Florida experience. Cancer 1993;72:2058–2065.
10. Henderson RH, Parsons JT, Morgan L, et al. Elective ilioin-guinal lymph node irradiation. Int J Radiat Oncol Biol Phys1984;10:811–819.
11. Boman B, Moerel C. Carcinoma of the anal canal: A clinicaland pathological study of 188 cases. Cancer 1984;54:114–125.
12. Cohen AM, Wong WD. Anal squamous cell cancer nodalmetastases: Prognostic significance and therapeutic consider-ations. Surg Oncol Clin North Am 1996;5:203–210.
13. Golden G, Horsley J. Surgical management of epidermoidcarcinoma of the anus. Am J Surg 1976;131:275–280.
14. Stearns MW, Urmacher C, Sternberg SS, et al. Cancer of theanal canal. Curr Probl Cancer 1980;4:1–44.
15. Tocci A, Lepre L, Costa G. Rectal cancer and inguinal me-tastases: Prognostic role and therapeutic indications. Dis Co-lon Rectum 1999;42:1464–1466.
16. Doci R, Zucali R, Bombelli L, et al. Combined chemoradia-tion therapy for anal cancer: A report of 56 cases. Ann Surg1992;215:150–156.
17. Cummings BJ. Anal cancer. Int J Radiat Oncol Biol Phys1990;19:1309–1315.
18. Grinnell RS. Lymphatic block with atypical and retrogradelymphatic metastasis and spread in carcinoma of the colon andrectum. Ann Surg 1966;163:272.
19. Shindo K. Epidermoid carcinoma compared with adenocarci-noma of the anal canal. Aust N Z J Surg 1981;51:426–429.
20. Gerard JP, Bobin JY, Romestaing P, et al. Sentinel inguinalnode detection in carcinoma of the anal canal (CAC) [Ab-stract]. Radiat Oncol 2000;56(Suppl.):63–64.
21. Clark J, Petrelli N, Herrera L, et al. Epidermoid carcinoma ofthe anal canal. Cancer 1986;57:400–406.
22. Avill R. Carcinoma of the rectum and anal canal with inguinallymph node metastases: Long term survival. Br J Clin Pract1984;28:324–325.
23. Kuehn P, Beckett R. Epidermoid carcinoma of the perianalskin and anal canal: A review of 157 cases. N Engl J Med1964;270:614–617.
24. Schlag PM, Hunerbein M. Anal cancer: Multimodal therapy.World J Surg 1995;19:282–286.
25. Cedermark B, Johansson H, Rutqvist LE, et al. The StockholmI trial of preoperative short term radiotherapy in operablerectal carcinoma: A prospective randomized trial. Cancer1995;75:2269–2275.
26. Gastrointestinal Tumor Study Group. Prolongation of the dis-ease-free interval in surgically treated rectal carcinoma.N Engl J Med 1985;312:1465–1472.
27. Konn M, Morita T, Hada R, et al. Survival and recurrenceafter low anterior resection and abdominoperineal resectionfor rectal cancer: The results of a long-term study with areview of the literature. Surg Today 1993;23:21–30.
28. Black QC, Nuyttens JJ, Yan D, et al. The potential benefit ofintensity modulated radiation therapy (IMRT) for anus cancer[Abstract]. Radiology 2000;217(Suppl.):351–352.
747Elective groin irradiation in low rectal cancer ● N. TAYLOR et al.