effects of iproveratril and nitroglycerin in the heart and coronary circulation of dogs
TRANSCRIPT

Effects of iproveratril and nitroglycerin in
the heart and coronary circulation of dogs
Gordon Ross* Charles Jorgensen
Los Angeles, Cali’.
A lthough iproveratril (ar-isopropyl-a-[ (N- methyl-N-homoveratryl) - y -amino-
propyl] - 3,4 - dimethoxyphenylacetonitrile; IsoptinR) has been shown to increase coro- nary flow in animals1z2 and has been used successfully in the treatment of angina pec- toris,3-6 information concerning some of its cardiovascular actions is incomplete. For example, there have been no direct meas- urements of the effect of the agent on in- stantaneous coronary inflow, myocardial contractile force, or cardiac output in the intact animal. In the present study, non- cannulating electromagnetic flowmeters were used to measure blood flow in the ascending aorta and coronary arteries of anesthetized open-chest dogs. hlyo- cardial contractile force was determined by a Walton-Brodie strain-gauge arch. The effects of both intracoronary and intravenous iproveratril were observed and were compared with those of nitro- glycerin.
Methods
Ten dogs weighing 1.5 to 25 kilograms were anesthetized with 30 mg. per kilo- gram of intravenous pentobarbital sodium. Polyethylene catheters were placed in an external jugular vein and a common carotid
artery for intravenous injections and sys- temic arterial pressure measurements re- spectively. A lateral thoracotomy through the fourth left intercostal space was per- formed, ventilation being maintained by a Bird Mark 8 respirator. The pericardium was incised and the aorta was cleared of fat and connective tissue. A convenient branch-free segment of the anterior de- scending coronary artery about 1 cm. in length was dissected free from the epi- cardium. Noncannulating electromagnetic probes were placed on these vessels and a strain-gauge arch was sutured to the anterior left ventricular myocardium be- tween the interventricular groove and the apex. Flow was measured with 400 c.p.s. gated sine-wave flowmeters. The zero reference for coronary flow was obtained by means of a snare placed downstream from the coronary flow probe. The absence of interference between the aortic and coronary probes was confirmed by observ- ing the output of one, while turning off the magnet current of the other. Calibra- tion was performed by allowing saline to pass from a gravity feed reservoir through the lumen of the probe into a graduate. No arterial wall was used. The validity of this method of calibration has been pre-
From the Departments of Physiology and Medicine, UCLA School of Medicine, Los Angeles, Calif., 90024. Received for publication Aug. 14. 1967.
74
*Address: Department of Biophysics. UCLA School of Medicine. Los Angeles, Calif.. 90024.
American Heart Journal July, 1968 Vol. 76, Nci. 1, pp. 74-78

Volume 76 Number 1 Efects of iproveratrib and nitroglycerin 75
viously demonstrated by others.8 Systemic arterial pressure was measured with a Sanborn 267B transducer. Intracoronary injections were made downstream from the flow probe through an indwelling 25 gauge needle connected by polyethylene tubing to a microsyringe. Iproveratril was administered in the form of its hydro- chloride (Isoptin HCI) and doses are ex- pressed in terms of this salt.
Results
Intracoronary injections. Nitroglycerin, 4 to 40 pg, injected into the anterior de- scending coronary artery increased flow in this vessel. The response began within 2 to 4 seconds, reached a peak in 8 to 12 seconds, and returned to control values in less than 30 seconds (Fig. 1, A). Both systolic and diastolic flow increased and the end-diastolic pressure/flow ratio di-
A. 8.
30
ANT. DESC. $ 2o COR.FLOW 2 lo
t
./ -
0
minished. There was no change in arterial pressure, heart rate, or the relative dura- tions of systole or diastole. Intracoronary iproveratril 4 to 40 pg produced similar changes except that the duration of the coronary flow increase was considerably more prolonged and lasted 1 to 8 minutes (Fig. 1, I?).
Intravenous injections. Intravenous nitro- glycerin, 1 to 10 pg per kilogram, reduced systemic arterial pressure and produced a biphasic coronary flow response con- sisting of an initial brief increase followed by a more prolonged decrease which paralleled the fall in arterial pressure (Fig. 2, B). The instantaneous coronary flow changes during the period of increased flow were identical to those which followed intracoronary nitroglycerin (Fig. 3, B). During the period of decreased flow, both systolic and diastolic flow decreased and
AORTIC I” ‘00 - PRESS. f 5o C
t t +-lmln 1
Fig. 1. Effects of intracoronary nitroglycerin and iproveratril on coronary blood flow. Upper trace, mean flow in the left anterior descending coronary artery. Lower trace, mean aortic pressure. 8, Nitroglycerin, 40 pg; B, iproveratril, 40 pg.
Fig. 2. Effects of intravenous iproveratril and nitroglycerin on (from top to bottom) systemic arteri, cardiac output, anterior descending coronary flow, and myocardial contractile force. A, Iproveratril, kilogram; B, nitroglycerin, 5 pg per kilogram.
al press 0.1 mg
ure, per

76 Ross and Jorgensen Am. Heart .I. July, 1968
mm Hg
1 /min
ml/mitt
Fig. 3. Effects of intravenous nitroglycerin, 5 pg per kilogram, on systemic arterial pressure (upper trace), instantaneous aortic flow (middle trace), and instantaneous flow in the anterior descending coronary artery. A, Control; B, at maximum coronary flow; C, at maximum hypotension.
A. 0. 150
mmtlg 50 10
I/mill
Fig. 4. Effects of intravenous iproveratril, 0.1 mg. per kilogram, on systemic arterial pressttre (upper trace), instantaneous aortic flow (middle trace), and instantaneous flow in the anterior descending coronary artery. A, Control; B, at maximum coronary flow; C, at maximum hypotension.
systolic backflow was frequently observed (Fig. 3, C). Heart rate did not change significantly. Cardiac output and con- tractile force increased during the first minute of the response and then fell to preinjection levels. In some dogs a biphasic response was seen and, following the initial increase, both cardiac output and con- tractile force fell below preinjection levels before returning to normal values 3 to 6 minutes after injection (Figs. 2, B, and 3). The effects of iproveratril, 50 to 125 pg per kilogram, differed from those of nitro- glycerin in that coronary flow was in- creased throughout the period of hypo- tension (Fig. 2, A). In no case was a re- duction in coronary flow observed. Initially both systolic and diastolic coronary flow
increased (Fig. 4, B), but subsequently systolic flow returned to control values so that the increased coronary flow during the later stages of the response was solely due to increased diastolic flow (Fig. 4, C). The duration of the arterial pressure and coronary flow responses was 2 to 4 times longer than those induced by nitroglycerin. Contractile force changes were small and resembled those produced by nitroglycerin. Cardiac output increased slightly through- out the response (Figs. 2, A, and 4). No significant changes in the heart rate were observed with either nitroglycerin or ipro- veratril.
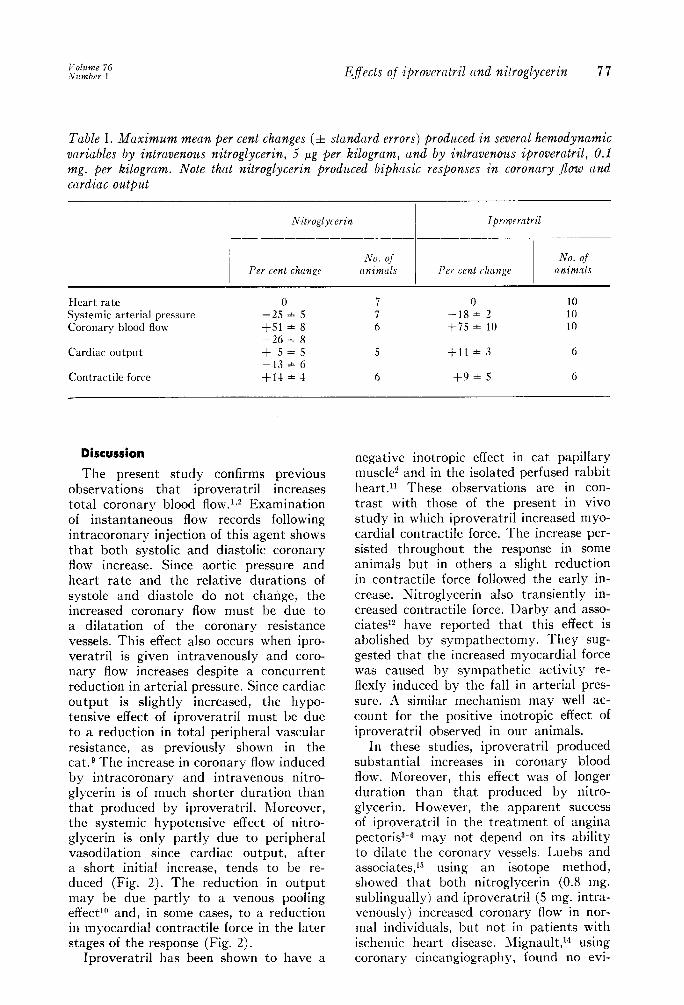
The quantitative changes produced by these agents in the variables studied are shown in Table 1.
Effects of iproveratril and nitroglycerin 77
Table I. Maximum mean per cent changes (h standard errors) produced in several hemodynamic variubles by intravenous nitroglycerin, 5 pg per kilogram, and by intravenous iproveratril, 0.1 mg. per kilogrum. Note that nitroglycerin prodzbced biphasic responses in coronary jlow and cardiac output
Nitroglycerin Iproveratril
Per cent change No. of
animals Per cent rkangr No. of
rlnimals
Heart rate Systemic arterial pressure Coronary blood flow
Cardiac output
Contractile force
0 7 0 10 -25 * 5 7 -18+ 2 10 f51 * 8 6 +i5 f 10 10 -2618 +s*s 5 +11* 3 6 -13 f 6 +14+ 4 6 +9 * 5 6
Discussion
The present study confirms previous observations that iproveratril increases total coronary blood flow.‘J Examination of instantaneous flow records following intracoronary injection of this agent shows that both systolic and diastolic coronary flow increase. Since aortic pressure and heart rate and the relative durations of systole and diastole do not change, the increased coronary flow must be due to a dilatation of the coronary resistance vessels. This effect also occurs when ipro- veratril is given intravenously and coro- nary tlow increases despite a concurrent reduction in arterial pressure. Since cardiac output is slightly increased, the hypo- tensive effect of iproveratril must be due to a reduction in total peripheral vascular resistance, as previously shown in the cat.g The increase in coronary flow induced by intracoronary and intravenous nitro- glycerin is of much shorter duration than that produced by iproveratril. Moreover, the systemic hypotensive effect of nitro- glycerin is only partly due to peripheral vasodilation since cardiac output, after a short initial increase, tends to be re- duced (Fig. 2). The reduction in output may be due partly to a venous pooling effectlo and, in some cases, to a reduction in myocardial contractile force in the later stages of the response (Fig. 2).
Iproveratril has been shown to have a
negative inotropic effect in cat papillary musclei and in the isolated perfused rabbit heart.” These observations are in con- trast with those of the present in vivo study in which iproveratril increased myo- cardial contractile force. The increase per- sisted throughout the response in some animals but in others a slight reduction in contractile force followed the early in- crease. Nitroglycerin also transiently in- creased contractile force. Darby and asso- ciate+? have reported that this effect is abolished by sympathectomy. They sug- gested that the increased myocardial force was caused by sympathetic activity re- flexly induced by the fall in arterial pres- sure. A similar mechanism may well ac- count for the positive inotropic effect of
iproveratril observed in our animals. In these studies, iproveratril produced
substantial increases in coronary blood flow. Moreover, this effect was of longer duration than that produced by nitro- glycerin. However, the apparent success of iproveratril in the treatment of angina pectoris+ may not depend on its ability to dilate the coronary vessels. Luebs and associates,*” using an isotope method, showed that both nitroglycerin (0.8 mg. sublingually) and iproveratril (5 mg. intra- venously) increased coronary flow in nor- mal individuals, but not in patients with ischemic heart disease. Jlignault,‘” using coronary cineangiography, found no evi-

78 Ross and Jorgensen Am. Heart J. Jdy, 1968
dence of coronary dilatation after ipro- veratril administration in patients with either normal or diseased coronary ar- teries, whereas coronary dilatation can be demonstrated by this technique after administration of nitrog1ycerin.n Melville and Benfey” reported that iproveratril had a /3-adrenergic blocking effect on isolated heart muscle preparations and Mignault14 suggested that this action may be responsible for its beneficial effect in angina. This seems unlikely since the conventional fl-adrenergic blocking agents produce striking reductions in myocardial contractile force16 and such changes were not observed in our animals. In earlier work on cats,g we were unable to demon- strate any effect of iproveratril in block- ing the actions of subsequently adminis- tered isoproterenol. The basis for the therapeutic action of this agent, like that of nitroglycerin, therefore remains obscure.
REFERENCES
1. Schlepper, M., and Witzleb, E.: Tierexperi- mentelle Untersuchungen iiber die Verander- ungen von Coronardurchhlutung und Sauer- stoffverbrauch des Herzens nach oc-Isopropyl-a- [(N-methyl-N-homoveratryl)--r-aminopropyl]-3, 4-dimethoxyphenylacetonitril, Arzneimittel- Forsch. 12:559, 1962.
2. Haas, H., and Hartfelder, G.: cr-Isopropyl-or- [(N-methyl-N-homoveratrylf-y-aminopropyl]-3, 4-dimethoxyphenylacetonitril, eine Substanz mit coronargefasserweiternden Eigenschaften, Arzneimittel-Forsch. 12:549, 1962.
3. Tschirdewahn, B., and Klepzig, H.: Klinische Untersuchmlg iiber die Wirkung von Isoptin und Isoptin S bei Patienten mit Koronar- insuffizienz, Deutsch. med. Wchnschr. 88:1702, 1963.
4. Knoch, G., Schlepper, M., and Witzleb, E.: Untersuchungen an Gesunden und Koronar-
kranken Patienten mit Isoptin, Med. Klin. 58:1485, 1963.
5. Neumann, M., and Luisada, A. A.: Double blind evaluation of orally administered ipro- veratril in patients with angina pectoris, Am. J. M. SC. 251:552, 1966.
6. Pezzo, G., Brina, A., and Barbera, G.: Tratta- mento delle coronaropatie: studio di un nuovo farmaco, l’iproveratril, Min. Med. 57:3341, 1966.
7. Kolin, A., and Kado, R. T.: Miniaturization of the electromagnetic blood flowmeter and its use for the recording of circulatory responses of conscious dogs to sensory stimuli, Proc. Nat. Acad. SC. 45:1312, 1959.
8. Gregg, D. E., Khouri, E. M., and Rayford, C. R.: Systemic and coronary energetics in the resting unanesthetized dog, Circulation Res. 1’6:102, 196.5.
9. Ross, G., and Jorgensen, C. R.: Cardiovascular actions of iproveratril, J. Pharmacol. & Exper. Therap. In press.
10. Case, R. B., and Roven, R. B.: Some considera- tions of coronary flow, Progr. Cardiovas. Dis. 6:45, 1963.
11. Melville, K. I., and Benfey, B. G.: Coronary vasodilator and cardiac adrenergic blocking effects of iproveratril, Canad. J. Physiol. Br Pharmacol. 43:339, 1965.
12. Darby, T. D., Sprouse, J. H., and Walton, R. P.: Evaluation of sympathetic reflex effects on the inotropic action of nitroglycerin, quini- dine, papaverine, aminophyllin, and isopro- terenol, J. Pharmacol. & Exper. Therap. 122:386, 1958.
13. Luebs, E. D., Cohen, A., Zaleski, E. J., and Bing, R. J.: Effect of nitroglycerin, intensain, isoptin, and papaverine on coronary blood flow in man, Am. J. Cardiol. 17:.535, 1966.
14. Mignault, J. de L.: Coronary cineangiographic study of intravenously administered isoptin, Canad. M. A. J. 95:1252, 1966.
15. Gensini, G. G.: Coronary angiography, Progr. Cardiovas. Dis. 6:155, 1963.
16. Nakano, J., and Kusakari, T.: Effect of beta adrenergic blockade on the cardiovascular dynamics, Am. J. Physiol. 210:833, 1966.