effects of inhaled versus systemic corticosteroids on exhaled nitric oxide in severe acute asthma
TRANSCRIPT

Respiratory Medicine (2009) 103, 614e620
ava i lab le a t www.sc iencedi rec t .com
journa l homepage : www.e lsev ie r . com/ loca te / rmed
Effects of inhaled versus systemic corticosteroids onexhaled nitric oxide in severe acute asthma
See Meng Khoo*,a, T.K. Lim a
Division of Respiratory and Critical Care Medicine, National University Hospital, Lower Kent Ridge Road,Singapore 119074, Singapore
Received 14 May 2008; accepted 10 October 2008Available online 20 November 2008
KEYWORDSAcute asthma;Airway inflammation;Exhaled nitric oxide;Inhaled corticosteroids;Systemic corticosteroids
Abbreviations: NO, nitric oxide; FEV1,1 s; AQLQ, asthma quality of lifecorticosteroids.
* Corresponding author. Tel.: þ65 67E-mail address: [email protected]
a Both authors were involved in thdata analysis and writing up of the st
0954-6111/$ - see front matter ª 200doi:10.1016/j.rmed.2008.10.009
Summary
Background: There is a paucity of information on the differential effects of systemic versusinhaled corticosteroids on airway inflammation in patients with acute asthma. This studyaimed to evaluate the effects of stopping systemic corticosteroids while maintaining theinhaled corticosteroids (ICS) on airway inflammation, lung function and asthma symptoms inpatients who had been discharged from hospital after treatment for severe acute asthma.Methods: Twenty-four adult patients with severe exacerbations of asthma were treated withboth oral and inhaled corticosteroids after discharge from hospital. Oral corticosteroids werestopped after 1 week. Spirometry, asthma quality of life questionnaire (AQLQ) score andexhaled nitric oxide (NO) were measured at discharge, 1 week, and 2 weeks after discharge.Results: Withdrawal of oral corticosteroids resulted in significant rebound in mean exhaled NOby 11.0 ppb (95% CI, 4.9e17.1 ppb, p < 0.001) or 47.7% (95% CI, 22.4e73.1%) despite uninter-rupted ICS treatment. The rebound in exhaled NO occurred despite significant improvement inthe mean AQLQ score (p Z 0.006) and frequency of reliever use (p Z 0.003) and was not asso-ciated with significant change in the mean FEV1 (p Z 0.64).Conclusions: In patients discharged from hospital after treatment for asthma exacerbations,withdrawal of oral corticosteroids resulted in increase in exhaled NO levels despite continuedICS treatment.ª 2008 Elsevier Ltd. All rights reserved.
forced expiratory volume inquestionnaire; ICS, inhale
72 4377; fax: þ65 6779 4112..sg (S.M. Khoo).e planning, data collection,udy.
8 Elsevier Ltd. All rights reserved
Introduction
Measurement of exhaled nitric oxide (NO) is a non-invasivetest for detection of endogenous inflammatory signals inpatient with asthma.1 Elevated levels of exhaled NO havebeen documented in patients with asthma.2,3 Exhaled NOlevels are further increased during asthma exacerbations,4,5
and fall following treatment with inhaled6 and systemiccorticosteroids.4 Oral prednisolone reduces exhaled NO in
.
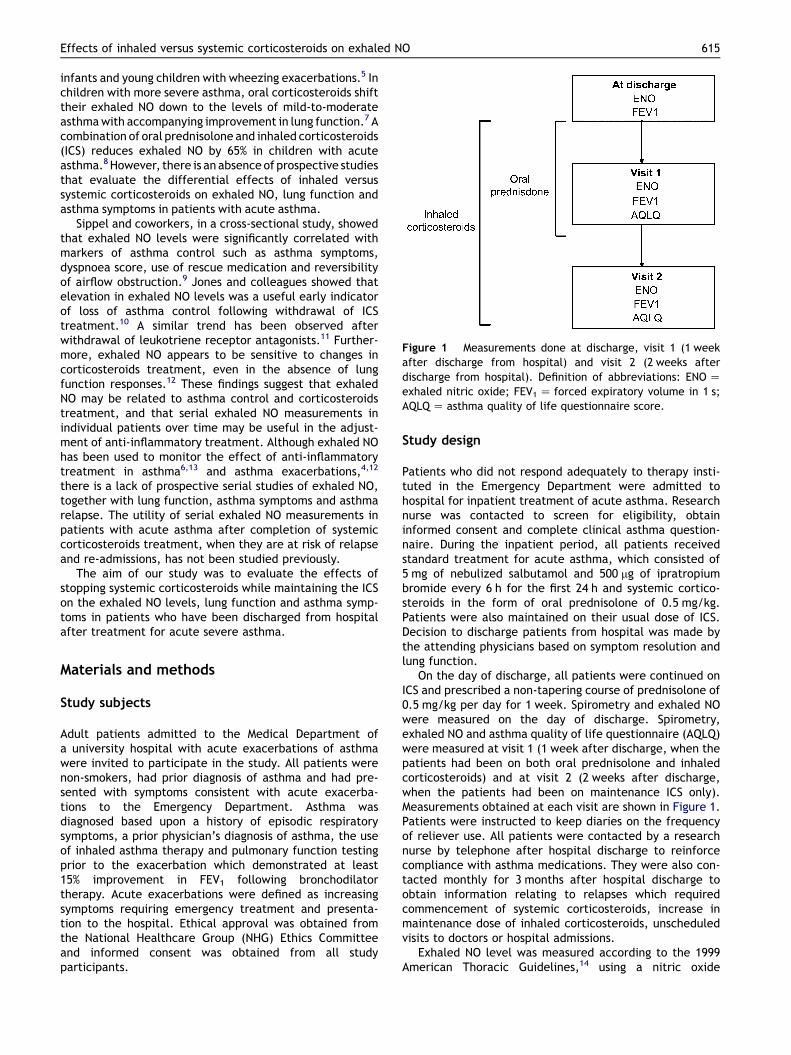
Figure 1 Measurements done at discharge, visit 1 (1 weekafter discharge from hospital) and visit 2 (2 weeks afterdischarge from hospital). Definition of abbreviations: ENO Zexhaled nitric oxide; FEV1 Z forced expiratory volume in 1 s;AQLQ Z asthma quality of life questionnaire score.
Effects of inhaled versus systemic corticosteroids on exhaled NO 615
infants and young children with wheezing exacerbations.5 Inchildren with more severe asthma, oral corticosteroids shifttheir exhaled NO down to the levels of mild-to-moderateasthma with accompanying improvement in lung function.7 Acombination of oral prednisolone and inhaled corticosteroids(ICS) reduces exhaled NO by 65% in children with acuteasthma.8 However, there is an absence of prospective studiesthat evaluate the differential effects of inhaled versussystemic corticosteroids on exhaled NO, lung function andasthma symptoms in patients with acute asthma.
Sippel and coworkers, in a cross-sectional study, showedthat exhaled NO levels were significantly correlated withmarkers of asthma control such as asthma symptoms,dyspnoea score, use of rescue medication and reversibilityof airflow obstruction.9 Jones and colleagues showed thatelevation in exhaled NO levels was a useful early indicatorof loss of asthma control following withdrawal of ICStreatment.10 A similar trend has been observed afterwithdrawal of leukotriene receptor antagonists.11 Further-more, exhaled NO appears to be sensitive to changes incorticosteroids treatment, even in the absence of lungfunction responses.12 These findings suggest that exhaledNO may be related to asthma control and corticosteroidstreatment, and that serial exhaled NO measurements inindividual patients over time may be useful in the adjust-ment of anti-inflammatory treatment. Although exhaled NOhas been used to monitor the effect of anti-inflammatorytreatment in asthma6,13 and asthma exacerbations,4,12
there is a lack of prospective serial studies of exhaled NO,together with lung function, asthma symptoms and asthmarelapse. The utility of serial exhaled NO measurements inpatients with acute asthma after completion of systemiccorticosteroids treatment, when they are at risk of relapseand re-admissions, has not been studied previously.
The aim of our study was to evaluate the effects ofstopping systemic corticosteroids while maintaining the ICSon the exhaled NO levels, lung function and asthma symp-toms in patients who have been discharged from hospitalafter treatment for acute severe asthma.
Materials and methods
Study subjects
Adult patients admitted to the Medical Department ofa university hospital with acute exacerbations of asthmawere invited to participate in the study. All patients werenon-smokers, had prior diagnosis of asthma and had pre-sented with symptoms consistent with acute exacerba-tions to the Emergency Department. Asthma wasdiagnosed based upon a history of episodic respiratorysymptoms, a prior physician’s diagnosis of asthma, the useof inhaled asthma therapy and pulmonary function testingprior to the exacerbation which demonstrated at least15% improvement in FEV1 following bronchodilatortherapy. Acute exacerbations were defined as increasingsymptoms requiring emergency treatment and presenta-tion to the hospital. Ethical approval was obtained fromthe National Healthcare Group (NHG) Ethics Committeeand informed consent was obtained from all studyparticipants.
Study design
Patients who did not respond adequately to therapy insti-tuted in the Emergency Department were admitted tohospital for inpatient treatment of acute asthma. Researchnurse was contacted to screen for eligibility, obtaininformed consent and complete clinical asthma question-naire. During the inpatient period, all patients receivedstandard treatment for acute asthma, which consisted of5 mg of nebulized salbutamol and 500 mg of ipratropiumbromide every 6 h for the first 24 h and systemic cortico-steroids in the form of oral prednisolone of 0.5 mg/kg.Patients were also maintained on their usual dose of ICS.Decision to discharge patients from hospital was made bythe attending physicians based on symptom resolution andlung function.
On the day of discharge, all patients were continued onICS and prescribed a non-tapering course of prednisolone of0.5 mg/kg per day for 1 week. Spirometry and exhaled NOwere measured on the day of discharge. Spirometry,exhaled NO and asthma quality of life questionnaire (AQLQ)were measured at visit 1 (1 week after discharge, when thepatients had been on both oral prednisolone and inhaledcorticosteroids) and at visit 2 (2 weeks after discharge,when the patients had been on maintenance ICS only).Measurements obtained at each visit are shown in Figure 1.Patients were instructed to keep diaries on the frequencyof reliever use. All patients were contacted by a researchnurse by telephone after hospital discharge to reinforcecompliance with asthma medications. They were also con-tacted monthly for 3 months after hospital discharge toobtain information relating to relapses which requiredcommencement of systemic corticosteroids, increase inmaintenance dose of inhaled corticosteroids, unscheduledvisits to doctors or hospital admissions.
Exhaled NO level was measured according to the 1999American Thoracic Guidelines,14 using a nitric oxide

Figure 2 Exhaled nitric oxide (ENO) measurements atdischarge, visit 1 and visit 2. ENO decreased significantly aftertreatment with oral and inhaled steroids (visit 1). ENOincreased significantly after withdrawal of oral steroids despitethe uninterrupted inhaled steroids treatment (visit 2). Defini-tion of abbreviations: ENO Z exhaled nitric oxide; ICS Z in-haled corticosteroids.
Figure 4 Asthma quality of life questionnaire (AQLQ) scoresat visit 1 and visit 2. With uninterrupted inhaled steroidstreatment, AQLQ scores improved significantly despite with-drawal of oral steroids.
616 S.M. Khoo, T.K. Lim
analyzer (NIOX, Aerocrine, Stockholm, Sweden) at anexpiratory flow rate of 50 mL/s.
Forced expiratory volume in 1 s (FEV1) and forced mid-expiratory flow rate (FEF25e75%) were measured accordingto American Thoracic Society standards15 and the bestvalue of three maneuvers was expressed as a percentage ofthe predicted value for the local population.16
A disease-specific quality of life measure, the AsthmaQuality of Life Questionnaire (AQLQ),17 was used in thisstudy. The instrument has been validated and demon-strated to be responsive to change.18 The minimal clinicallyimportant difference is a change in score of 0.5 (on a scaleof 7).19
Figure 3 FEV1 (% predicted) at discharge, visit 1 and visit 2.FEV1 improved significantly after treatment with oral andinhaled steroids (visit 1). No significant change in FEV1 afterwithdrawal of oral steroids (visit 2). Definition of abbrevia-tions: FEV1 Z forced expiratory volume in 1 s; ICS Z inhaledcorticosteroids.
Statistical analysis
Continuous variables are expressed as mean � standarddeviation unless otherwise specified. One-factor repeatedmeasures ANOVA with adjustment for multiple comparison(Bonferroni) was used to compare the exhaled NO levels,FEV1 and FEF25e75% at discharge, visit 1 and visit 2. Stu-dent’s paired t-test was used to compare AQLQ scoresbetween visit 1 and visit 2. Wilcoxon Signed Ranks test wasused to compare the paired data on frequency of relieveruse between visit 1 and visit 2. P values of <0.05 wereconsidered statistically significant.
Results
Twenty-four patients entered the study (a total of 30patients were approached for the study, of whom sixdeclined to participate). Demographic data are given inTable 1. None of the patients were on nasal corticosteroids.
Figure 5 Average daily frequency of reliever use in theweeks prior to visit 1 and visit 2. With uninterrupted inhaledsteroids treatment, frequency of reliever use decreasedsignificantly despite withdrawal of oral steroids.

Table 1 Subjects’ characteristics
Age, mean (range) 39 (18e65) yearMale/female 9/15Duration of asthma, mean (range) 15.9 (4e33) yearAsthma therapy n (%)
Budesonide 800 mg per day andshort-acting b2-agonist
11 (46)
Beclometasone 400 mg per dayand short-acting b2-agonist
7 (29)
Fluticasone 500 mg per dayand short-acting b2-agonist
5 (21)
Fluticasone 500 mg per dayand long-acting b2-agonist
1 (4)
Length of stay, mean (SD) 2.0 (1.2) daysFEV1 at discharge, mean (SD) 73.9 (20.0) % predictedENO at discharge, mean (SD) 60.3 (46.3) ppb
Effects of inhaled versus systemic corticosteroids on exhaled NO 617
The mean (�SD) exhaled NO level and FEV1 on the day ofdischarge from hospital were 60.3 � 46.3 ppb and73.9 � 20.0% predicted respectively. Average length of staywas 2.0 days (range, 1e5 days). All patients had beentreated with ICS for persistent asthma prior to the exac-erbations. None of the patients reported relapse of asthmaexacerbations which resulted in commencement ofsystemic corticosteroids, increase in maintenance dose ofinhaled corticosteroids, unscheduled visits to doctors orhospital admissions in the 3 months after discharge fromhospital.
Exhaled nitric oxide
The mean exhaled NO level on the day of discharge fromhospital was 60.3 � 46.3 ppb. Combined treatment withsystemic and inhaled corticosteroids over 7 days was asso-ciated with a significant decrease in the mean exhaled NOlevels by 24.2 ppb (95% CI, 6.5e41.8 ppb, p Z 0.005) or31.3% (95% CI, 16.3e46.2%) from baseline. Withdrawal ofsystemic corticosteroids resulted in a rebound of the meanexhaled NO level by 11.0 ppb (95% CI, 4.9e17.1 ppb,p < 0.001) or 47.7% (95% CI, 22.4e73.1%) despite thecontinued ICS treatment (Fig. 2).
Pulmonary function, quality of life and frequencyof reliever use
At discharge from hospital, the mean FEV1 was 73.9 � 20.0%predicted. At visit 1, the mean FEV1 improved significantlyby 13.6% predicted (95% CI, 5.8e21.4%, p < 0.001) aftertreatment with both systemic and inhaled corticosteroidsfor 7 days (Fig. 3). At visit 2, 1 week after the withdrawal ofthe systemic corticosteroids, the mean FEV1 showeda continued but non-significant improvement of 2.3%predicted (95% CI, �2.3 to 6.9, p Z 0.64). FEF25e75%
measurements showed a trend that was similar to that ofFEV1. The mean FEF25e75% improved by 17.8% predicted (95%CI, 5.8e29.9%, p Z 0.003) between discharge and visit 1,but did not show any significant change between visit 1 andvisit 2 (�0.12% predicted; 95% CI, �8.0 to 7.7%, p Z 1.00).
AQLQ scores improved significantly by 0.53 (95% CI,0.17e0.88, p Z 0.006) between visit 1 and visit 2 (Fig. 4).Frequency of reliever use (Fig. 5) also decreased signifi-cantly despite the withdrawal of systemic corticosteroidsand rebound in exhaled NO levels (p Z 0.003).
Discussion
The novel finding of this study was that in patients dis-charged from hospital after treatment for severe acuteasthma, withdrawal of oral corticosteroids resulted inrebound of exhaled NO levels despite continued ICS treat-ment. These changes in exhaled NO were not accompaniedby worsening of lung function or asthma symptoms.
There are a few possible explanations for our observa-tions. First, the increase in exhaled NO levels may bea reflection of a peripheral component of airway inflam-mation that is less influential or has a delayed effect onlung function and asthma symptoms. The rebound inexhaled NO levels despite uninterrupted ICS treatment maybe a result of the inability of ICS to penetrate beyondsmaller distal airways. It is possible that ICS are able tosuppress inducible NO synthase in the larger airways butunable to reach the distal airways to have effects on theperipheral parenchymal inflammation. Lehtimaki et al. hadused the two-compartment model described by Tsoukiasand George,20,21 and found that alveolar NO concentrationwas increased in asthmatic patients with nocturnal symp-toms.22 The same group also observed that inhaled fluti-casone decreased bronchial NO flux but had no effect onalveolar NO concentration.23 Gelb et al. reported increasedalveolar NO concentration in patients with clinically stableasthma despite treatment with ICS.24 Five days of 30 mgprednisone resulted in isolated significant decrease inalveolar NO concentration. Results from these studiessuggest the presence of inflammation in very distal gasexchanging respiratory bronchioles and alveoli in asthmaticpatients.24
There is an increasing body of evidence that there maybe a concomitant lung parenchymal component in asthma.Kraft et al. reported the presence of inflammatory cells inthe lung parenchyma obtained by fiberoptic bronchoscopybiopsy in patients with nocturnal asthma.25 Gelb et al.reported unexplained loss of lung parenchymal elasticrecoil properties not due to emphysema in stable, non-smoking, patients with chronic persistent asthma withabnormal expiratory airflow limitation.26,27 Berry et al.found that alveolar NO were elevated in patients withrefractory asthma and reduced by oral prednisolone treat-ment.28 Belda et al. reported that in patients with acuteasthma, oral prednisone reduced blood eosinophil counts,while inhaled fluticasone reduced airway eosinophil counts,suggesting that the anti-inflammatory performance ofinhaled fluticasone is exerted locally.29 The findings of thepresent study may be related to the presence of a separatecomponent of peripheral inflammation in patients withacute exacerbation of asthma that is not suppressed by ICS.
Second, changes in exhaled NO level may precede otherparameters such as lung function and may therefore serveas an early warning of loss of control. Previous studieshave yielded inconsistent data regarding the correlation

618 S.M. Khoo, T.K. Lim
between exhaled NO and the conventional measures ofasthma control.4,8,30 Kharitonov and colleagues havedescribed exhaled NO as a ‘‘rapid response’’ marker, whichis extremely sensitive to corticosteroid treatment as it maybe significantly reduced even after 6 h following a singletreatment with nebulized corticosteroids, or within 2e3 days after inhaled corticosteroids, reaching maximaleffect after 2e4 weeks of treatment.31 A possible expla-nation for our finding is, therefore, that our patients hadindeed had early sub-clinical airway inflammation, whichwas detected only by exhaled NO measurements followingoral corticosteroids withdrawal. However, the absence ofexacerbations in the 3 months after hospital discharge in alltwenty-four patients suggests that these early signals ofoccult airway inflammation may be of doubtful clinicalsignificance.
Third, our observations may be due to the dose-responseeffects of corticosteroids on airway inflammation andexhaled NO. It is possible that the rebound in exhaled NOhad resulted from the reduction in the total dose of corti-costeroids received by the study subjects after withdrawalof the oral corticosteroids. Previous studies have suggesteda dose-response relationship between exhaled NO andICS.32 However, these studies also found that a plateaueffect on exhaled NO was seen at a dose of 400 mg ofinhaled budesonide.32,33 In the present study, all thesubjects were maintained on ICS doses that were eitherequivalent to or above 400 mg of budesonide, putting themon the upper end of the dose-response curve. The reboundin exhaled NO was more likely to be due to the differentialeffect of oral corticosteroids withdrawal than the dose-response effect of corticosteroids on exhaled NO since allthe subjects were maintained on the upper end of the dose-response curve throughout the study period. In addition,commencement of oral prednisone has been shown toresult in a decrease in exhaled NO in patients with asthmawho were already on ICS, suggesting a separate effect oforal corticosteroids that may not be related to the dose-response relationship.24,28 The differential effects ofinhaled versus systemic corticosteroids on the threecomponents of asthma: airway inflammation, lung functionand clinical symptoms in patients with acute asthma arestill unclear.
Finally, it is possible that our observations had resultedfrom the isolated effects of corticosteroids on exhaled NOand were unrelated to airway inflammation. Corticosteroidshave been shown to reduce exhaled NO by directly inhib-iting the induction of nitric oxide synthase 2 (NOS2).34 Theincrease in exhaled NO levels after withdrawal of oralcorticosteroids may have been the result of a loss of directinhibition of NOS2 by systemic corticosteroids and not theremoval of suppression of pro-inflammatory cytokines.
Results of the present study have two important clinicalimplications. First, exhaled NO may have limited clinicalutility as a marker to guide anti-inflammatory therapy inthe period immediately after asthma exacerbations whenpatients are at risk of relapse. The lack of concordantresponse between exhaled NO and other measures ofasthma control suggests that exhaled NO level is highlysensitive to variations in oral corticosteroid treatment andmay not be a useful indicator of response to treatmentduring recovery from acute exacerbations of asthma in
patients who are on ICS. Recommencement of oral corti-costeroids or escalation in the dose of ICS in our patients inresponse to the increase in exhaled NO levels may haveresulted in over-treatment with corticosteroids. Second,the presence of a component of inflammation that is not ICSresponsive, if confirmed by further studies, challenges therole of ICS in the management of acute asthma.23,24,28 Anemerging area of study is the role of ICS in the treatment ofacute asthma. Trials in which ICS were compared withplacebo demonstrated clear beneficial effects of ICS. Incontrast, the evidence was conflicting in trials where ICSwere compared with systemic corticosteroids.35 Thesefindings may be related to the presence of peripheralinflammation that is suppressed by systemic corticosteroidsbut not ICS. The characteristics, anatomic site and clinicalsignificance of this component of airway inflammation needclarification with further studies.
Although our findings suggest a lack of concordantresponse between exhaled NO and other measures ofasthma control in patients treated for acute asthma, theresults must be interpreted with caution. First,the discordant relationship observed may have been due tothe small sample size. However, the consistent trend ofimprovement observed in lung function and asthma symp-toms suggests the presence of a genuine discordant rela-tionship between the inflammatory signals and lungfunction. Second, a parallel study design with a controlarm may have provided a better design to investigate theeffect of oral corticosteroids withdrawal. However,a parallel design would have required some of the studysubjects to be continued on oral prednisolone beyond1 week despite improvement in all the conventionalmeasures of asthma control (lung function, clinical symp-toms and frequency of reliever use). The fact that thestudy subjects were maintained on relatively high doses ofICS (upper end of the dose-response curve) throughout thestudy period and the consistent trend of rebound inexhaled NO suggest the presence of a significant exhaledNO signal associated with oral corticosteroids withdrawal.Third, exhaled NO levels, lung function and asthma symp-toms were monitored in the setting of uninterruptedmaintenance ICS treatment in the present study. This mayhence limit generalization of the results to patients whoare not on maintenance ICS after acute exacerbations.Fourth, we did not perform sputum eosinophils count orbronchial biopsy to ascertain the presence of airwayinflammation. However, the observed improvement in lungfunction, asthma symptoms and the absence of relapse inthe follow up period suggest the absence of clinicallyimportant airway inflammation that requires escalation ofanti-inflammatory treatment.
In conclusion, we found that in patients discharged fromhospital after treatment for severe asthma exacerbations,withdrawal of oral corticosteroids resulted in an increase inexhaled NO levels despite continued ICS treatment. Theincrease in exhaled NO was not accompanied by reductionin lung function and occurred despite improvement in AQLQscores and rescue medication use. The differential effectsof inhaled versus systemic corticosteroids on differentsources of exhaled NO and their relationships with differentcomponents of airway inflammation need further investi-gations and clarifications.

Effects of inhaled versus systemic corticosteroids on exhaled NO 619
Funding
Funded by NHG research fund (NHG-RPR/02059).
Disclosure
Both authors do not have financial interest in the subjectmatter to declare.
Originality and clinical relevance
There is a paucity of data on the differential effects ofinhaled versus systemic corticosteroids on airway inflam-mation, lung function and asthma symptoms in patientswith severe acute asthma. Our study found that withdrawalof oral corticosteroids resulted in an increase in exhaled NOlevels despite continued inhaled corticosteroid treatment.There was also a discordant relationship between exhaledNO, lung function and clinical symptoms. Our results mayhave important clinical implications relating to: (1) theclinical utility of exhaled NO in patients with acute asthma;and (2) the effects of inhaled corticosteroids on airwayinflammation in acute asthma.
Acknowledgements
We are grateful to our research and asthma nurses Ms. K.E.Thein, L.K. Tan, N. Said for their assistance in datacollection and the care of our patients, Ms. W.J. Ngerng forher help in data entry, and Dr. Y.H. Chan for his advice onbiostatistics.
References
1. Kharitonov SA, Barnes PJ. Exhaled biomarkers. Chest 2006;130:1541e6.
2. Kharitonov SA, Yates D, Robbins RA, Logan-Sinclair R,Shinebourne EA, Barnes PJ. Increased nitric oxide in exhaledair of asthmatic patients. Lancet 1994;343:133e5.
3. Persson MG, Zetterstrom O, Agrenius V, Ihre E, Gustafsson LE.Single-breath nitric oxide measurements in asthmatic patientsand smokers. Lancet 1994;343:146e7.
4. Massaro AF, Gaston B, Kita D, Fanta C, Stamler JS, Drazen JM.Expired nitric oxide levels during treatment of acute asthma.Am J Respir Crit Care Med 1995;152:800e3.
5. Baraldi E, Dario C, Ongaro R, et al. Exhaled nitric oxideconcentrations during treatment of wheezing exacerbation ininfants and young children. Am J Respir Crit Care Med 1999;159:1284e8.
6. Kharitonov SA, Yates DH, Barnes PJ. Inhaled glucocorticoidsdecrease nitric oxide in exhaled air of asthmatic patients. Am JRespir Crit Care Med 1996;153:454e7.
7. Baraldi E, Azzolin NM, Zanconato S, Dario C, Zacchello F.Corticosteroids decrease exhaled nitric oxide in children withacute asthma. J Pediatr 1997;131:381e5.
8. Lanz MJ, Leung DY, White CW. Comparison of exhaled nitricoxide to spirometry during emergency treatment of asthmaexacerbations with glucocorticoids in children. Ann AllergyAsthma Immunol 1999;82:161e4.
9. Sippel JM, Holden WE, Tilles SA, et al. Exhaled nitric oxidelevels correlate with measures of disease control in asthma. JAllergy Clin Immunol 2000;106:645e50.
10. Jones SL, Kittelson J, Cowan JO, et al. The predictive value ofexhaled nitric oxide measurements in assessing changes inasthma control. Am J Respir Crit Care Med 2001;164:738e43.
11. Montuschi P, Mondino C, Koch P, Ciabattoni G, Barnes PJ,Baviera G. Effects of montelukast treatment and withdrawalon fractional exhaled nitric oxide and lung function in childrenwith asthma. Chest 2007;132:1876e81.
12. Kharitonov SA, Yates DH, Chung KF, Barnes PJ. Changes in thedose of inhaled steroid affect exhaled nitric oxide levels inasthmatic patients. Eur Respir J 1996;9:196e201.
13. Gustafsson LE. Exhaled nitric oxide as a marker in asthma. EurRespir J Suppl 1998;26:49Se52S.
14. Recommendations for standardized procedures for the on-lineand off-line measurement of exhaled lower respiratory nitricoxide and nasal nitric oxide in adults and children-1999. Thisofficial statement of the American Thoracic Society wasadopted by the ATS Board of Directors, July 1999. Am J RespirCrit Care Med 1999;160:2104e17.
15. Standardization of spirometryd1987 update. Statement of theAmerican Thoracic Society. Am Rev Respir Dis 1987;136:1285e98.
16. da Costa JL. Pulmonary function studies in healthy Chineseadults in Singapore. Am Rev Respir Dis 1971;104:128e31.
17. Juniper EF, Guyatt GH, Ferrie PJ, Griffith LE. Measuring qualityof life in asthma. Am Rev Respir Dis 1993;147:832e8.
18. Juniper EF, Guyatt GH, Epstein RS, Ferrie PJ, Jaeschke R,Hiller TK. Evaluation of impairment of health related quality oflife in asthma: development of a questionnaire for use inclinical trials. Thorax 1992;47:76e83.
19. Juniper EF, Guyatt GH, Willan A, Griffith LE. Determininga minimal important change in a disease-specific Quality of LifeQuestionnaire. J Clin Epidemiol 1994;47:81e7.
20. Tsoukias NM, George SC. A two-compartment model ofpulmonary nitric oxide exchange dynamics. J Appl Physiol1998;85:653e66.
21. Tsoukias NM, Shin HW, Wilson AF, George SC. A single-breathtechnique with variable flow rate to characterize nitric oxideexchange dynamics in the lungs. J Appl Physiol 2001;91:477e87.
22. Lehtimaki L, Kankaanranta H, Saarelainen S, Turjanmaa V,Moilanen E. Increased alveolar nitric oxide concentration inasthmatic patients with nocturnal symptoms. Eur Respir J2002;20:841e5.
23. Lehtimaki L, Kankaanranta H, Saarelainen S, Turjanmaa V,Moilanen E. Inhaled fluticasone decreases bronchial but notalveolar nitric oxide output in asthma. Eur Respir J 2001;18:635e9.
24. Gelb AF, Taylor CF, Nussbaum E, et al. Alveolar and airway sitesof nitric oxide inflammation in treated asthma. Am J RespirCrit Care Med 2004;170:737e41.
25. Kraft M, Djukanovic R, Wilson S, Holgate ST, Martin RJ. Alveolartissue inflammation in asthma. Am J Respir Crit Care Med1996;154:1505e10.
26. Gelb AF, Zamel N. Unsuspected pseudophysiologic emphysemain chronic persistent asthma. Am J Respir Crit Care Med 2000;162:1778e82.
27. Gelb AF, Licuanan J, Shinar CM, Zamel N. Unsuspected loss oflung elastic recoil in chronic persistent asthma. Chest 2002;121:715e21.
28. Berry M, Hargadon B, Morgan A, et al. Alveolar nitric oxide inadults with asthma: evidence of distal lung inflammation inrefractory asthma. Eur Respir J 2005;25:986e91.
29. Belda J, Margarit G, Martinez C, et al. Anti-inflammatoryeffects of high-dose inhaled fluticasone versus oral prednisonein asthma exacerbations. Eur Respir J 2007;30:1143e9.
30. Stirling RG, Kharitonov SA, Campbell D, et al. Increase inexhaled nitric oxide levels in patients with difficult asthma andcorrelation with symptoms and disease severity despite

620 S.M. Khoo, T.K. Lim
treatment with oral and inhaled corticosteroids. Asthma andAllergy Group. Thorax 1998;53:1030e4.
31. Kharitonov SA, Barnes PJ. Exhaled markers of pulmonarydisease. Am J Respir Crit Care Med 2001;163:1693e722.
32. Jatakanon A, Kharitonov S, Lim S, Barnes PJ. Effect of differingdoses of inhaled budesonide on markers of airway inflamma-tion in patients with mild asthma. Thorax 1999;54:108e14.
33. Aziz I, Wilson AM, Lipworth BJ. Effects of once-daily formoteroland budesonide given alone or in combination on surrogate
inflammatory markers in asthmatic adults. Chest 2000;118:1049e58.
34. Guo FH, Comhair SA, Zheng S, et al. Molecular mechanisms ofincreased nitric oxide (NO) in asthma: evidence for transcrip-tional and post-translational regulation of NO synthesis.J Immunol 2000;164:5970e80.
35. Edmonds ML, Camargo Jr CA, Pollack Jr CV, Rowe BH. Early use ofinhaled corticosteroids in the emergency department treatmentofacuteasthma.CochraneDatabaseSystRev2003;(3).CD002308.