effects of combat deployment on risky and self-destructive … · and self-destructive behavior...
TRANSCRIPT
Naval Health Research Center
Effects of Combat Deployment on Risky
and Self-destructive Behavior Among
Active Duty Military Personnel
Cynthia J. Thomsen
Valerie A. Stander
Stephanie K. McWhorter
Mandy M. Rabenhorst
Joel S. Milner
Report No. 09-03
The views expressed in this article are those of the authors and do not nec-
essarily reflect the official policy or position of the Department of the
Navy, Department of Defense, nor the U. S. Government.
Approved for public release; distribution is unlimited
Naval Health Research Center
140 Sylvester Road
San Diego, California 92106

lable at ScienceDirect
Journal of Psychiatric Research 45 (2011) 1321e1331
Contents lists avai
Journal of Psychiatric Research
journal homepage: www.elsevier .com/locate/psychires
Effects of combat deployment on risky and self-destructive behavior among activeduty military personnel
Cynthia J. Thomsen a,*, Valerie A. Stander a, Stephanie K. McWhorter a, Mandy M. Rabenhorst b,Joel S. Milner b
aBehavioral Science and Epidemiology, Naval Health Research Center, 140 Sylvester Road, San Diego, CA 92106-3521, USAbCenter for the Study of Family Violence and Sexual Assault, Northern Illinois University, 125 Presidents Blvd, DeKalb, IL 60640, USA
a r t i c l e i n f o
Article history:Received 29 September 2010Received in revised form25 February 2011Accepted 7 April 2011
Keywords:Combat deploymentSelf-harmSuicide attemptsIllegal drugsRisk-takingUnprotected sexDepressionAnxietyPTSD
* Corresponding author. Tel.: þ1 619 553 7174; fax:E-mail address: [email protected] (C
0022-3956/$ e see front matter Published by Elseviedoi:10.1016/j.jpsychires.2011.04.003
a b s t r a c t
Although research has documented negative effects of combat deployment on mental health, few studieshave examined whether deployment increases risky or self-destructive behavior. The present studyaddressed this issue. In addition, we examined whether deployment effects on risky behavior varieddepending on history of pre-deployment risky behavior, and assessed whether psychiatric conditionsmediated effects of deployment on risky behavior. In an anonymous survey, active duty members of theU.S. Marine Corps and U.S. Navy (N ¼ 2116) described their deployment experiences and their partici-pation in risky recreational activities, unprotected sex, illegal drug use, self-injurious behavior, andsuicide attempts during three time frames (civilian, military pre-deployment, and military post-deployment). Respondents also reported whether they had problems with depression, anxiety, orPTSD during the same three time frames. Results revealed that risky behavior was much more commonin civilian than in military life, with personnel who had not deployed, compared to those who haddeployed, reporting more risky behavior and more psychiatric problems as civilians. For the current timeperiod, in contrast, personnel who had deployed (versus never deployed) were significantly more likelyto report both risky behavior and psychiatric problems. Importantly, deployment was associated withincreases in risky behavior only for personnel with a pre-deployment history of engaging in riskybehavior. Although psychiatric conditions were associated with higher levels of risky behavior, psychi-atric problems did not mediate associations between deployment and risky behavior. Implications forunderstanding effects of combat deployment on active duty personnel and directions for future researchare discussed.
Published by Elsevier Ltd.
1. Introduction
High levels of continuing U.S. military deployments in supportof war efforts in Iraq and Afghanistan have heightened concernsabout effects of combat on military personnel. Research has docu-mented increases in psychological problems among personnelreturning from combat deployment. Although most studies havefocused on post-traumatic stress disorder (PTSD), increases inrelated problems such as depression and substance abuse also havebeen demonstrated (Boscarino, 1995; Hoge et al., 2004). Compar-atively less attention has been paid to potential effects of deploy-ment on other psychological and behavioral health issues. Thepresent study investigated the effects of combat deployment on
þ1 619 553 8459..J. Thomsen).
r Ltd.
a constellation of behaviors that are either overtly self-destructiveor that place the individual at substantial risk of harm.
“Risky or self-destructive” behavior is a broad category. At oneend of the spectrum are activities that could result in harm to theself but are not necessarily intended to do so, such as risky recre-ation (e.g., extreme sports), risky driving (e.g., driving withouta seatbelt or after drinking), risky sexual activities (e.g., sex withstrangers, unprotected sex), and substance use or abuse; at theother end of the continuum are behaviors explicitly intended toharm the self, including deliberate self-harm without suicidalintent (“self-harm”), suicide attempts, and suicide. Although thesebehaviors may be subsumed under the rubric of “self-injuriousthoughts and behaviors” (Silverman et al., 2007), they do notconstitute a homogenous set; the behaviors likely differ in severalrespects, including their prevalence, motivational underpinnings,the potential severity of adverse consequences, and the nature andmagnitude of barriers to performing them. Nonetheless, different

C.J. Thomsen et al. / Journal of Psychiatric Research 45 (2011) 1321e13311322
types of risky behaviors tend to co-occur. For example, individualswho engage in self-harm are more likely than those who do not toattempt suicide (e.g., Muehlenkamp and Gutierrez, 2007), use illicitdrugs (e.g., Matsumoto et al., 2005), and be involved in other riskybehaviors (e.g., Laye-Gindhu and Schonert-Reichl, 2005). Similarly,both heavy drinking and heavy smoking are associated with riskysexual behavior (e.g., Leigh et al., 1994) and risky driving (e.g., Fearet al., 2008). Moreover, different types of risky behavior often sharecommon predictors. For example, most types of risky behavior aremore common among young men than among women or oldermen (Nell, 2002; Zuckerman, 2007).
The present study examined effects of combat deployment onfive specific types of risky or self-destructive behavior: dangerousrecreational activities, unprotected sex with someone other thana regular partner, illegal drug use, self-harm, and suicide attempts.Our primary hypothesis was that rates of each risky behavior wouldbe higher following combat deployment than before deployment.Of the five types of risky or self-destructive behavior considered inthe present study, only substance use and suicide-related thoughtsand behaviors have received significant research attention aspossible consequences of military deployment. Combat deploy-ment has been associated with increased likelihood of drug andalcohol problems (Browne et al., 2008; Calhoun et al., 2008; Hogeet al., 2004; Koenen et al., 2003). However, empirical findingsregarding the association between deployment and suicide-relatedideations and behaviors have been weak and inconsistent (Centersfor Disease Control, 1987; Hall, 1996; Hansen-Schwartz et al., 2002;Kaplan et al., 2009; O’Toole and Cantor, 1995; Thoresen et al., 2003;Wojcik et al., 2009; Wong et al., 2001).
Although we are aware of no previous research examining theimpact of deployment on risky recreational activity, unprotectedsex, or self-harm, combat deployment has been linked withincreases in risky driving behaviors (e.g., speeding, failing to wearone’s seat belt; Fear et al., 2008). In addition, in a sample of Armysoldiers returning from Iraq, specific combat experiences wererelated to scores on a scale assessing general preferences forengaging in risky activities (e.g., seeking the “thrill of danger,” likingto drive fast; Killgore et al., 2008). However, because risk-takingpreferences prior to deployment were not assessed in this study,it is not possible to determine whether combat exposure changedrisk preferences, or whether those who preferred risky situationssought out combat exposure; indeed, some evidence suggests thatmilitary personnel with higher risk-taking proclivities may bemorelikely to deploy and to volunteer for hazardous duties (Bell et al.,2010; Bricknell et al., 1999; Jobe et al., 1983; Zuckerman, 2007).
There are several mechanisms by which combat deploymentmight increase risky behavior. Joiner’s (2005) interpersonal-psychological theory of suicidal behavior posits that repeatedexposure to pain or fear-inducing situations (e.g., through combatexposure) results in habituation, i.e., greater tolerance for pain andlower levels of fear. In turn, this habituation increases the indi-vidual’s capability to enact lethal self-injury. Using similar logic,Killgore et al. (2008) suggested that habituation to danger asa result of long-term combat exposure may increase risk-takingpropensities among veterans. In support of these formulations,recent evidence indicates that combat exposure is associated withself-reported habituation to pain and decreases in fear (Brenneret al., 2008; Bryan et al., 2010). A related possibility is thatreturning combat veterans may engage in risky behavior in anattempt to create an “adrenaline rush” similar to those that theyexperienced in combat (Vaughan, 2006).
Increases in risky behaviors following deployment also mayresult from deployment-related increases in psychiatric symptomssuch as depression and PTSD (e.g., Hoge et al., 2004). Althoughnegative emotional states have been linked with both suicidality
and self-harm (e.g., Whitlock and Knox, 2007), links with lessovertly self-destructive behaviors such as risky recreation, unpro-tected sex, and illegal drug use are less clear. Nonetheless, riskybehaviors that are not intrinsically self-destructive sometimes maybe undertaken, either consciously or subconsciously, with self-destructive intent. Consistent with this view, accidental deathsand suicides have been found to have common risk factors (Steaet al., 2002; Thoresen and Mehlum, 2004). Previous findings ofelevated rates of accidental death among combat veterans (CatlinBoehmer et al., 2004; Kang et al., 2002; Knapik et al., 2009) maythus reflect some instances in which individuals purposefullyengaged in risky behaviors for self-destructive purposes. In thepresent study, we examined whether psychiatric conditions(depression, anxiety, and PTSD) were associated with riskybehavior. In addition, we examined whether these conditionsmediate the impact of deployment on risky behaviors.
In addition to predicting that combat deployment wouldincrease rates of risky behavior in general, we expected deploy-ment effects to differ depending on the individual’s prior history ofrisky behavior. Specifically, effects of deployment in increasingrisky behavior were expected to be most pronounced among thosewho had engaged in the behavior previously. Prior engagement inrisky behavior may be a marker for psychological difficulties orvulnerabilities that place the individual at risk of developingadverse reactions to deployment. At a minimum, prior engagementin a behavior indicates that it is part of the individual’s behavioralrepertoire. If the individual has engaged in a behavior in the past,perhaps as a means of coping with distress (e.g., Klonsky, 2007), heor she may turn to the same strategy again to copewith the stressesassociated with deployment or with readjustment followingdeployment. We could locate no prior research investigatingwhether deployment effects are moderated by prior behaviors.
In the present study, we first used within-subjects analyses toexamine changes in risky behavior from civilian to military life (forboth combat deployed and non-deployed personnel) and from pre-deployment to post-deployment life (for combat deployedpersonnel only). Next, we directly compared rates of risky behavioramong active duty personnel who had previously combat deployedand those who had not. In addition, we examined whether effectsof combat deployment on risky behavior differed depending onwhether the individual had engaged in that behavior in the past.We predicted that effects of deployment on a given risky behaviorwould be stronger among individuals who had a history ofengaging in that type of behavior. Each analysis was conductedacross five different types of risky behavior (risky recreationalactivities, unprotected sex, illegal drug use, self-harm, and suicideattempts), allowing for a determination of whether combatdeployment had similar or distinct effects on different types ofbehavior. A final set of analyses examined patterns of psychiatricproblems (depression, anxiety, and PTSD) before and afterdeployment and among deployers and non-deployers, and testedwhether deployment-related increases in psychiatric problemsmight account for any effects of deployment on risky or self-destructive behaviors.
2. Methods
2.1. Participants
The Naval Health Research Center (NHRC) Combat Stress andSubstance Use survey was conducted between August 2006 andAugust 2007. Participants were active duty military personnelserving at U.S. Marine Corps (USMC) installations in SouthernCalifornia and Arizona within three major commands: MarineCorps Air Station Yuma Arizona (primarily 3rd Marine Air Wing);

C.J. Thomsen et al. / Journal of Psychiatric Research 45 (2011) 1321e1331 1323
1st Marine Logistics Group, Camp Pendleton, California; and 1stMarine Division, Camp Pendleton and 29 Palms, California. Thesecommands represent air, support, and infantry units. A total of 2612personnel attended survey recruiting sessions. Of these, 2539participants completed some part of the survey, yielding a 97%participation rate. The present sample included only participantswho provided data about their deployments and who completed atleast 7 of the 8 items assessing risky behavior (N ¼ 2116; responserate ¼ 81%). Most participants (93%) were in the USMC; the other7% were Navy (USN) personnel embedded within USMC units. Asexpected, the majority of participants were young (M ¼ 24.09 yrs,SD ¼ 5.30), male (92%), and junior-ranking enlisted personnel(E1 � E5 ¼ 85%); only 4% were commissioned officers. Forty-sevenpercent reported at least some college or other post-secondarytechnical training. Approximately equal numbers were single(47%) andmarried or cohabiting (46%), with the remaining 7% beingdivorced, separated, or widowed. Compared to members of theUSMC as a whole (Marine Corps Community Services, 2007), USMCparticipants in the present sample were significantly younger (76%sample vs. 67% USMC aged 25 or younger), lower in rank (44%sample vs. 39% USMC ranked lower than E4), less likely to be offi-cers (4% sample vs. 11% USMC), and more likely to be female (8%sample vs. 6% USMC), ps < 0.01. USMC personnel in the sample didnot differ from the general USMC in terms of marital status (44% ofsample and 45% of USMC married).
2.2. Survey procedures
This research was conducted in compliance with all federalregulations regarding the protection of human subjects in research,and was approved by an Institutional Review Board at NHRC(protocol #NRHC 2006.0008). Commanders referred personnelfrom participating units tomeet with civilian survey administratorsat prearranged times and locations, based on their availabilitywithin the training schedule. Groups ranged in size from 28 to 408.At the beginning of each session, the survey was introduced as ananonymous questionnaire concerning the relationship betweencombat stress and substance use. Informed consent informationwas read aloud. Consent information included the following:participation was voluntary, with no repercussion for nonpartici-pation; participants could leave blank any questions they did notwant to answer, and could quit at any time; surveys werecompletely anonymous and would be processed by civilianresearchers, not military personnel; and individual data wouldnever be presented. To better ensure that participation wasvoluntary, officers and enlisted personnel participated in separatelocations. To increase the sense of anonymity, participants sealedtheir own completed surveys in stamped envelopes addressed toNorthern Illinois University (NIU); envelopes were mailed imme-diately following the session. Personnel who chose not to partici-pate were asked to sit quietly and then seal their blank surveys intheir mailing envelopes as though they had participated.
The survey assessed demographic characteristics (sex, age, rank,education level, marital status, number of children) and combatdeployment history (e.g., dates, locations, duties). A combatdeployment was defined by the receipt of imminent danger pay orcombat zone tax exclusion benefits; non-combat deploymentswere not considered. Eight items assessed risky behavior. Respon-dents were asked to indicate whether they had engaged in fivedifferent types of behavior: risky recreational activities (“donethings for fun that were so dangerous you were likely to be injuredor killed”), unprotected sex with someone other than one’s regularpartner, illegal drug use, self-harm (“hurt yourself physically tocalm down or feel better when you were tense, anxious, or upset”),and attempted suicide. Self-harm and illegal drug use were each
assessed by a single item; the other types of behavior were eachassessed by two items: one asked about engaging in the behaviorwhile drinking, and the other asked about engaging in the behaviorwhile not drinking (e.g., “attempted suicide after drinking alcohol”;“attempted suicide when you were not drinking alcohol”). In eachcase, respondents reported whether they had engaged in thebehavior (a) as a civilian, (b) while in the military before their firstcombat deployment, and (c) after returning from their first combatdeployment. Finally, for each of the same three time frames,respondents were asked whether they had ever “been told bya doctor or mental health counselor” that they had (1) depression,(2) anxiety, or (3) PTSD.
2.3. Analytic strategy
Prior to testing our hypotheses regarding the effects of deploy-ment on risky behavior, we provide descriptive information aboutboth combat deployments and rates of each type of risky behaviorwithin our sample. This includes an examination of demographicfactors associatedwith both deployment and risky behavior, as wellas associations between different types of risky behavior. We nextinvestigated changes in overall rates of risky behavior from civilianto military/pre-deployment life, separately for deployers and non-deployers. The hypothesis that risky behavior would increasefollowing deployment was examined in two ways. First, weexamined changes in risky behavior from pre-deployment to post-deployment among personnel who had combat deployed. Second,we compared the risky behavior of deployers and non-deployersduring different time periods (as a civilian, while in the military/pre-deployment, and currently). For deployers, current behaviorwas defined as post-deployment behavior; for non-deployedpersonnel, current behavior was defined as pre-deploymentbehavior (as there was no deployment period). In this set of anal-yses, deployment effects on risky behavior are indicated by differ-ences between deployers and non-deployers in current behavior(that were not apparent prior to deployment). After examining theoverall impact of deployment on risky behavior, additional analyseswere conducted to determine whether the impact of deploymenton each specific type of risky behavior was moderated by priorengagement in that type of risky behavior. A final set of analysesexamined whether deployment effects on risky behavior weremediated by mental health issues.
3. Results
3.1. Combat deployment
More than half (58%; n ¼ 1225) of respondents in the presentsample had been combat deployed. Most deployers (57%) had onedeployment, 29% had two, and 14% had three or more. Amongcombat deployers, 97% had deployed in support of Operation IraqiFreedom or Operation Enduring Freedom (91% OIF, 19% OEF, 13%otheroperations [e.g., Desert Shield/Storm]). Themodal deploymentlength was 7 months, with 35% of deployments being shorter and19% being longer (M ¼ 6.86;Mdn ¼ 7; range: 1e19 months). Three-quarters of deployers had returned fromdeploymentwithin the pastyear (45% in the past 6 months). Men (58%) and women (53%) wereequally likely to have deployed,c2 (1,N¼2066)¼ 2.09, n.s.However,personnel who were married or cohabiting (69%) or divorced,separated, or widowed (80%) were more likely to have deployedthan those who were single (45%), c2 (2, N ¼1921) ¼ 130.38,p < 0.001. USN personnel (70%) were more likely to have beendeployed than USMC personnel (57%), c2 (1, N ¼2058) ¼ 9.93,p < 0.01. In addition, deployers, compared to non-deployers, weresignificantly older (Ms ¼ 25.67 vs. 21.90 years), higher in rank

Table 1Associations (crude odds ratios) between lifetime engagement in high-risk behav-iors and demographic characteristics.
Predictor Type of high-risk behavior
Riskyrecreation
Unprotectedsex
Illegaldrug use
Self-harm Suicideattempt
Unprotected sex 5.42***Illegal drug use 3.45*** 3.54***Self-harm 6.16*** 2.39*** 2.08***Suicide attempt 4.43*** 3.42*** 2.43*** 11.84***Male 2.91*** 1.42* 1.70** 1.02 0.59*Older age 0.93*** 0.99 0.94*** 0.91*** 0.95*Higher rank 0.81*** 0.99 0.78*** 0.77*** 0.75***Higher education 0.82*** 1.07 0.82** 0.75*** 0.82USN (vs. USMC) 0.40*** 0.59** 0.50*** 0.56* 0.71Singlea 1.57*** 1.26* 1.15 1.42** 1.19Div/sep/widoweda 1.13 1.91** 1.09 1.02 2.35**
USN¼Navy; USMC¼Marine Corps. Ns vary from 1901 to 2097. ORs greater than 1.0indicate risk factors and ORs less than 1.0 indicate protective factors for high-riskbehavior.*p < 0.05. **p < 0.01. ***p < 0.001.
a The reference group was married/cohabiting.
C.J. Thomsen et al. / Journal of Psychiatric Research 45 (2011) 1321e13311324
(Ms¼ 4.62 [E4-E5] vs. 3.24 [E3]), and higher in education (Ms¼ 2.57vs. 2.44, where 2 ¼ high school diploma and 3 ¼ some college), ts(1974.8e2031.1) � 4.3, ps < 0.001.
0.3
0.6
0.9
1.2
1.5
1.8
tnerruCtnemyolped-erPnailiviC
Mea
n N
umbe
r of
Ris
ky B
ehav
iors
Time Frame
Total
Not Deployed
Deployed
Fig. 1. Mean number of risky behaviors reported by time period. Note. For non-deployed personnel, pre-deployment and current time frames are equivalent and arerepresented by the same data point.
3.2. Risky behavior
Nearly three-quarters (73%) of participants reported engaging inone or more types of risky behavior in their lifetimes (i.e., asa civilian or while in the military). Half (52%) reported engaging inunprotected sex with someone other than a regular partner, andhalf (49%) had engaged in recreational activities dangerous enoughto cause serious injury or death. Two in five (41%) had used illegaldrugs, and one in five (19%) reported engaging in self-harm.Attempted suicide was reported by 7% of respondents. Compari-sons of lifetime rates of risky behavior while drinking versus notdrinking alcohol were conducted for the three types of behavior forwhich this was assessed. Respondents were more likely to reportengaging in unprotected sex when they had been drinking thanwhen they had not (48% vs. 45%), Cochran’s Q (1, N¼ 2094)¼ 13.95,p < 0.001. In contrast, respondents were more likely to reportengaging in risky recreation or attempting suicide while notdrinking than while drinking (for risky recreation, 44% vs. 35%,Cochran’s Q (1, N ¼ 2098) ¼ 89.25, p < 0.001; for suicide attempts,5% vs. 3%, Cochran’s Q (1, N ¼ 2104) ¼ 15.14, p < 0.001). Despitethese differences, comparisons of deployers and non-deployersyielded identical patterns of effects for the alcohol and no-alcoholitems; therefore, alcohol and no-alcohol items for a given type ofrisky behavior were combined into a single index for all subsequentanalyses.
Table 1 provides associations among lifetime reports of differenttypes of risky behavior. Respondents who had engaged in any onetype of risky behavior were at significantly increased risk forengaging in every other type of risky behavior. As can be seen inTable 1, these associations were substantial, with odds ratios (ORs)ranging from 2 to nearly 12. An exploratory principal componentsanalysis with varimax rotation performed on lifetime rates of thefive risky behaviors revealed two underlying factors with eigen-values greater than 1. The first factor, accounting for 39% of the totalvariance, consisted of unprotected sex, use of illegal drugs, andrisky recreation; the second factor, accounting for 21% of the totalvariance, consisted of self-harm and suicide attempts. All loadingson the primary factor were greater than 0.7, and no cross-loadingswere greater than 0.3. This suggests that the five risky behaviors
constitute two underlying clusters, one representing deliberateself-harm and one representing behaviors that may increase thelikelihood of self harm, but are not necessarily intended to do so.
Considering the demographic predictors of lifetime riskybehavior, menwere more likely thanwomen to engage in risky, butnot explicitly self-destructive, behaviors; womenwere significantlymore likely to report attempting suicide (see Table 1). Relative toUSMC personnel, USN personnel were significantly less likely toengage in all of the behaviors except for suicide attempts. Age,education, and military rank were unrelated to the likelihood ofengaging in unprotected sex, but were negatively related to theother types of behavior. With respect tomarital status, respondentswho were single or formerly married (i.e., divorced, separated, orwidowed) were generally more likely to engage in risky behaviorsthan were married or cohabiting respondents (see Table 1).
3.3. Timing of risky behavior
Fig. 1 depicts the mean number of different risky behaviorsreported by deployed and non-deployed personnel for each of thethree time frames (i.e., civilian, pre-deployment, and current). It isimportant to note that for non-deployed personnel, estimates ofpre-deployment and current rates of risky behavior are based on thesamedata, because both time frames are equivalent for this group. Inthe sample as a whole, the likelihood of each type of risky behaviordecreased significantly from the civilian period to the military/pre-deployment period, McNemar c2 (1, Ns ¼ 2054e2116) � 17.78,ps < 0.001. Although the decline was most pronounced for illegaldrug use (from 39% to 5%), it was substantial for the other behaviorsas well: self-harm (13% to 6%), suicide attempts (5% to 2%), riskyrecreation (38% to 22%), and unprotected sex (37% to 29%). Table 2provides the percentage of respondents reporting each specificrisky behavior during each time frame, separately for deployers andnon-deployers. Declines in risky behavior from civilian to military/pre-deployment life were generally greater for non-deployed thanfor deployed personnel. For non-deployed personnel, all forms ofrisky behavior decreased significantly from civilian to military/pre-deployment periods, McNemar c2 (1, Ns ¼ 874e891) � 15.56,ps < 0.001; among deployed personnel, the reduction in riskybehavior was significant for four of the five behaviors [c2
(1,Ns¼ 1180e1225)� 7.58, ps< 0.01], but did not reach significancefor suicide attempts [c2 (1, N ¼ 1225) ¼ 2.94, p < 0.10].

Table 2Percentage of respondents reporting each type of high-risk behavior by time periodand combat deployment status.
Type of behavior/Deployment status Time period
Civilian Pre-dep Post-dep Lifetime
High-risk recreation 38 22 25 49Deployed (n ¼ 1225) 30 22 25 44Non-deployed (n ¼ 891) 50 22 e 56
Unprotected sex 37 29 29 52Deployed (n ¼ 1225) 33 29 29 51Non-deployed (n ¼ 891) 42 28 e 54
Illegal drug use 39 5 7 41Deployed (n ¼ 1180) 33 6 7 36Non-deployed (n ¼ 874) 47 5 e 48
Self-harm 13 6 10 19Deployed (n ¼ 1220) 8 5 10 16Non-deployed (n ¼ 889) 19 8 e 23
Suicide attempt 5 2 2 7Deployed (n ¼ 1225) 3 2 2 6Non-deployed (n ¼ 891) 7 3 e 9
pre-dep ¼ pre-deployment; post-dep ¼ post-deployment.
Table 4Results of logistic regression analyses predicting current high-risk behaviors(adjusted odds ratios).
Predictor Type of high-risk behavior
C.J. Thomsen et al. / Journal of Psychiatric Research 45 (2011) 1321e1331 1325
The hypothesis that risky behavior would increase followingdeployment was examined in two ways. First, we examinedchanges in high-risk behavior from pre-deployment to post-deployment among personnel who had combat deployed. Rele-vant percentages are provided in Table 2. Both risky recreation andself-harm increased significantly from pre- to post-deployment,McNemar c2 (1, Ns ¼ 1220 � 1225) ¼ 8.28 and 31.51, respectively,ps < 0.01. In contrast, changes in rates of unprotected sex, illegaldrug use, and suicide attempts from pre- to post-deployment werenot significant, McNemar c2 (1, Ns ¼ 1180 to 1225) � 2.54, n.s.
As an additional way of examining deployment effects on riskybehavior, we conducted a series of logistic regression analysescomparing the risky behavior of deployers and non-deployersduring three different time frames: as a civilian; while in themilitary, pre-deployment; and currently. For deployers, currentbehavior was defined as post-deployment behavior; for non-deployed personnel, current behavior was defined as pre-deployment behavior (as there was no deployment period). Ineach analysis, demographic variables (sex, age, rank, education,service [USMC vs. USN], and marital status) were entered on thefirst step, followed by deployment status. Table 3 provides theadjusted odds ratios for deployment effects on each type of riskybehavior during each time period. These ORs represent the extentto which deployers and non-deployers differed in the likelihood of
Table 3Adjusted odds ratios (ORs) representing differences between deployed and non-deployed personnel in rates of high-risk behaviors.
Type of behavior Civilian Pre-deployment Currenta
OR (CI95%) OR (CI95%) OR (CI95%)
High-risk recreation 0.56 0.45, 0.70 1.14 0.89, 1.47 1.59 1.24, 2.04Unprotected sex 0.68 0.55, 0.85 1.03 0.82, 1.29 1.15 0.91, 1.46Illegal drug use 0.72 0.58, 0.90 1.42 0.88, 2.29 1.86 1.18, 2.95Self-harm 0.62 0.45, 0.85 0.69 0.46, 1.05 1.52 1.06, 2.20Suicide attempt 0.66 0.39, 1.12 1.03 0.53, 2.03 0.86 0.44, 1.68
ORs greater than 1.0 (less than 1.0) indicate greater (lower) likelihood of high-riskbehavior among personnel who had combat deployed, relative to those who hadnot. Statistically significant ORs (p < 0.05) are in boldface type.
a Current behavior was defined as post-deployment behavior among personnelwho had previously deployed, and as pre-deployment military behavior amongpersonnel who had not previously deployed.
risky behavior after controlling for demographic factors, with ORsgreater than 1.0 indicating that risky behavior was more commonamong deployers.
As can be seen in the first column of Table 3, during the civiliantime frame, non-deployers were more likely than deployers toreport engaging in risky behavior. The difference between the twogroups was significant for all types of risky behavior except suicideattempts. Risky behavior while in the military but prior todeployment revealed a very different pattern. There were nosignificant differences between deployers and non-deployers in thelikelihood of any type of risky behavior for this time period (see thesecond column of Table 3). Most relevant to our primary hypothesisare the comparisons between deployers and non-deployers incurrent rates of risky behavior. As shown in the third column ofTable 3, deployers were significantly more likely than non-deployers to report current engagement in risky recreation, illegaldrug use, and self-harm; the two groups did not differ in reportedrates of unprotected sex or suicide attempts.
3.4. Previous risky behavior, combat deployment, and current riskybehavior
The next set of analyses examined whether the impact ofdeployment on each specific type of risky behavior was moder-ated by prior engagement in that type of risky behavior. Toexamine this issue, we conducted logistic regression analyses inwhich current risky behavior was predicted from demographicfactors (entered on the first step), prior engagement in thebehavior in question (entered on the second step), deploymentstatus (entered on the third step), and the interaction betweenprior behavior and deployment status (entered on the fourthstep). For those who had not deployed, previous behavior wasdefined as civilian behavior; for those who had deployed, itincluded both civilian behavior and military behavior prior todeployment. Results of these analyses are provided in Table 4.Among the demographic variables, only being divorced, sepa-rated, or widowed emerged as a consistent predictor of all formsof risky behavior. Not surprisingly, the strongest predictor ofcurrent engagement in each specific type of risky behavior washaving engaged in that type of behavior previously. Nonetheless,controlling for previous behavior did not alter the pattern of
Riskyrecreation
Unprotectedsex
Druguse
Self-harm Suicideattempt
Male 3.12*** 1.07 2.27 1.05 0.58Older age 0.95** 0.96** 0.95 0.94* 0.97Higher rank 0.99 1.08 0.83 1.01 0.76Higher education 1.18 1.06 1.52* 0.96 1.23USN (vs. USMC) 0.48** 0.62* 1.28 0.84 0.79Singlea 1.16 1.58*** 1.14 1.02 0.78Div/sep/widoweda 2.52** 2.55*** 2.59** 1.86* 3.90**Prior behavior 4.65*** 3.29*** 5.49*** 7.94*** 8.58***Combat deployment 1.94*** 1.19 2.14** 1.92** 0.86Prior behavior �
deployment2.54*** 1.27 1.39 2.27* 1.68
ORs greater than 1.0 indicate risk factors and ORs less than 1.0 indicate protectivefactors for high-risk behavior. Demographic variables were entered on Step 1, priorhigh-risk behavior (of the same type as the behavior being predicted) on Step 2,combat deployment on Step 3, and the interaction on Step 4 of the analyses. ORs arereported for the step on which the predictor entered the model. USN ¼ Navy;USMC ¼ Marine Corps.*p < 0.05. **p < 0.01. ***p < 0.001.
a The reference group was married/cohabiting.
0
5
10
15
20
25
Civilian
Time Frame
tnerruCtnemyolpeD-erP
Per
cent
age
Rep
orti
ng P
sych
iatr
ic C
ondi
tion
s TotalNot DeployedDeployed
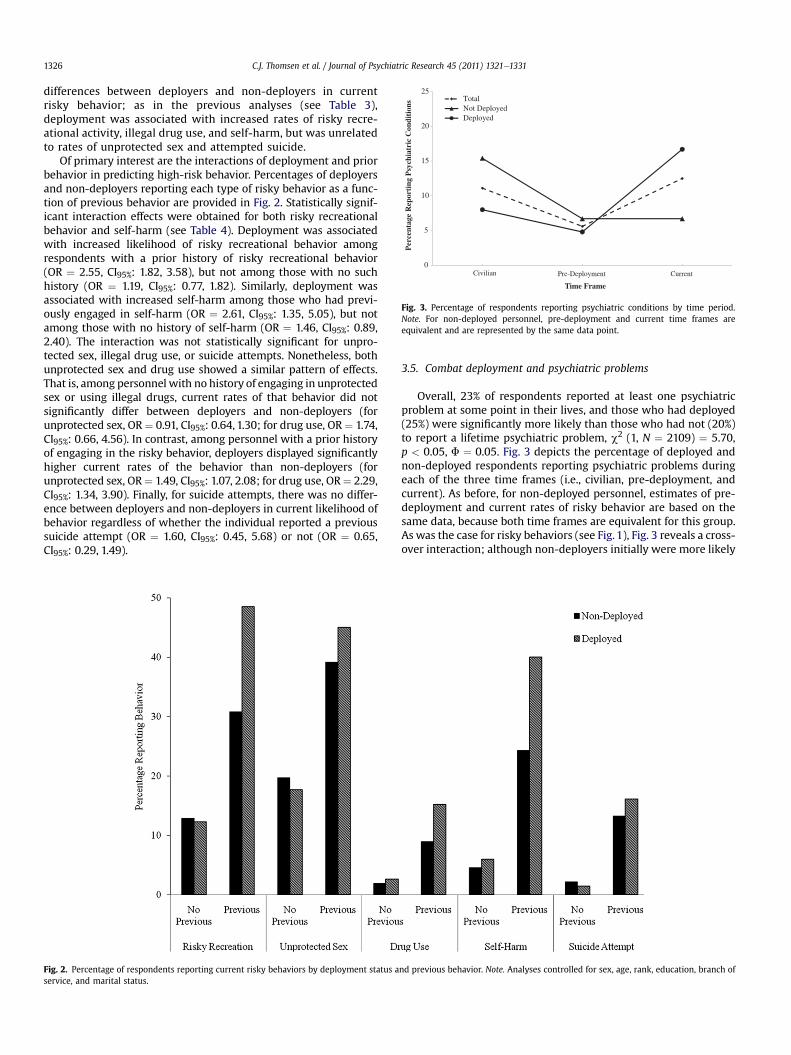
Fig. 3. Percentage of respondents reporting psychiatric conditions by time period.Note. For non-deployed personnel, pre-deployment and current time frames areequivalent and are represented by the same data point.
C.J. Thomsen et al. / Journal of Psychiatric Research 45 (2011) 1321e13311326
differences between deployers and non-deployers in currentrisky behavior; as in the previous analyses (see Table 3),deployment was associated with increased rates of risky recre-ational activity, illegal drug use, and self-harm, but was unrelatedto rates of unprotected sex and attempted suicide.
Of primary interest are the interactions of deployment and priorbehavior in predicting high-risk behavior. Percentages of deployersand non-deployers reporting each type of risky behavior as a func-tion of previous behavior are provided in Fig. 2. Statistically signif-icant interaction effects were obtained for both risky recreationalbehavior and self-harm (see Table 4). Deployment was associatedwith increased likelihood of risky recreational behavior amongrespondents with a prior history of risky recreational behavior(OR ¼ 2.55, CI95%: 1.82, 3.58), but not among those with no suchhistory (OR ¼ 1.19, CI95%: 0.77, 1.82). Similarly, deployment wasassociated with increased self-harm among those who had previ-ously engaged in self-harm (OR ¼ 2.61, CI95%: 1.35, 5.05), but notamong those with no history of self-harm (OR ¼ 1.46, CI95%: 0.89,2.40). The interaction was not statistically significant for unpro-tected sex, illegal drug use, or suicide attempts. Nonetheless, bothunprotected sex and drug use showed a similar pattern of effects.That is, among personnel with no history of engaging in unprotectedsex or using illegal drugs, current rates of that behavior did notsignificantly differ between deployers and non-deployers (forunprotected sex, OR¼ 0.91, CI95%: 0.64, 1.30; for drug use, OR¼ 1.74,CI95%: 0.66, 4.56). In contrast, among personnel with a prior historyof engaging in the risky behavior, deployers displayed significantlyhigher current rates of the behavior than non-deployers (forunprotected sex, OR¼ 1.49, CI95%: 1.07, 2.08; for drug use, OR¼ 2.29,CI95%: 1.34, 3.90). Finally, for suicide attempts, there was no differ-ence between deployers and non-deployers in current likelihood ofbehavior regardless of whether the individual reported a previoussuicide attempt (OR ¼ 1.60, CI95%: 0.45, 5.68) or not (OR ¼ 0.65,CI95%: 0.29, 1.49).
Fig. 2. Percentage of respondents reporting current risky behaviors by deployment status aservice, and marital status.
3.5. Combat deployment and psychiatric problems
Overall, 23% of respondents reported at least one psychiatricproblem at some point in their lives, and those who had deployed(25%) were significantly more likely than those who had not (20%)to report a lifetime psychiatric problem, c2 (1, N ¼ 2109) ¼ 5.70,p < 0.05, F ¼ 0.05. Fig. 3 depicts the percentage of deployed andnon-deployed respondents reporting psychiatric problems duringeach of the three time frames (i.e., civilian, pre-deployment, andcurrent). As before, for non-deployed personnel, estimates of pre-deployment and current rates of risky behavior are based on thesame data, because both time frames are equivalent for this group.As was the case for risky behaviors (see Fig. 1), Fig. 3 reveals a cross-over interaction; although non-deployers initially were more likely
nd previous behavior. Note. Analyses controlled for sex, age, rank, education, branch of

Table 5Percentage of respondents reporting each psychiatric condition by time period andcombat deployment status.
Psychiatric condition/Deployment status Time period
Civilian Pre-dep Post-dep Lifetime
Depression 9 5 10 18Deployed 6 4 10 17Non-deployed 14 6 e 18
Anxiety 6 4 9 14Deployed 4 3 9 14Non-deployed 8 5 e 13
PTSD 1 1 10 7Deployed < 1 1 10 11Non-deployed 1 1 e 2
pre-dep ¼ pre-deployment; post-dep ¼ post-deployment. PTSD ¼ post-traumaticstress disorder. For deployed, n ¼ 1225; for non-deployed, n ¼ 891.
Table 6Correlations (Phi coefficients) between psychiatric conditions and risky behaviors.
Risky behavior Condition
Depression Anxiety PTSD
Risky recreation 0.17*** 0.16*** 0.10***Unprotected sex 0.14*** 0.14*** 0.08***Drug use 0.15*** 0.09*** 0.02Self-harm 0.30*** 0.26*** 0.09***Suicide attempt 0.36*** 0.32*** 0.14***
Correlations are between lifetime reports of each diagnosis and of each type of riskybehavior. PTSD ¼ post-traumatic stress disorder.***p < 0.001.
C.J. Thomsen et al. / Journal of Psychiatric Research 45 (2011) 1321e1331 1327
than deployers to report psychiatric conditions, within the currenttime frame, deployers were more likely to report psychiatricconditions.
Table 5 provides the percentage of respondents reporting eachpsychiatric condition during each time frame, separately fordeployed and non-deployed personnel. Overall, depressionwas themost commonly reported problem (17%), followed by anxiety (14%),and PTSD (7%). Deployers and non-deployers did not differ in life-time rates of depression (17% and 18%, respectively), or anxiety (12%and 14%, respectively), ps � 0.20. However, deployers were signif-icantly more likely than non-deployers to report PTSD (11% vs. 2%),c2 (1, N ¼ 2089) ¼ 62.28, p < 0.001, F ¼ 0.17.
The next set of analyses examined differences in psychiatricproblems between deployers and non-deployers during each timeframe. As civilians, all three mental health conditions were morecommon among non-deployers than among deployers, 8.30� c2 (1,N ¼ 2116) � 34.13, p < 0.01, 0.06 � F � 0.12. Differences betweendeployers and non-deployers during military service but beforedeployment were similar to civilian differences, but smaller inmagnitude. Within this time frame, non-deployers were signifi-cantly more likely than deployers to report anxiety (p < 0.01), andthe difference in depression approached significance (p ¼ 0.05).However, rates of PTSD did not significantly differ (p > 0.4; seeTable 5). The pattern of differences between deployers and non-deployers during the current time frame was a complete reversalof the pattern observed during civilian life (and, to a lesser degree,military/pre-deployment life); that is, deployers reported signifi-cantly higher rates of all three conditions than non-deployersduring the current period, 14.70 � c2 (1, N ¼ 2116) � 78.23,p < 0.01, 0.08 � F � 0.19 (see Table 5).
McNemar change tests were used to examine whetherdeployers were more likely to report each condition followingdeployment than before deployment (i.e., civilian and military/
Table 7Results of logistic regression analyses predicting current high-risk behaviors (adjusted o
Predictora Type of high-risk behavior
Riskyrecreation
Unprotectesex
Prior behavior 4.70*** 3.17***Prior psychiatric condition 1.16 1.39*Current psychiatric condition 4.79*** 2.80***Combat deployment 1.64*** 1.06Prior behavior � deployment 2.50*** 1.18
*p < 0.05. **p < 0.01. ***p < 0.001.a Demographic variables were entered on the first step and are not reported here (see T
Step 2; combat deployment was entered on Step 3; the interaction was entered on Step 4factors for high-risk behavior. ORs are reported for the step on which the predictor ente
pre-deployment combined). Results revealed significantincreases in the likelihood of both depression (McNemar c2 [1,N ¼ 2116] ¼ 8.97, p < 0.01) and PTSD (McNemar c2 [1,N ¼ 2116] ¼ 68.97, p < 0.001). However, deployers were no morelikely to report anxiety problems post- than pre-deployment,McNemar c2 < 1, n.s.
3.6. Do psychiatric problems mediate associations betweendeployment and risky behavior?
The finding that psychiatric conditions show similar patterns ofeffects as risky behavior (as a joint function of deployment statusand time frame) is consistent with the possibility that mentalhealth problems mediate the association between deployment andrisky behavior. Also consistent with this possibility, psychiatricproblems were significantly correlated with risky behaviors (seeTable 6). Not surprisingly, correlations of psychiatric conditionswith overtly self-destructive behaviors (i.e., self-harm and suicideattempts) were generally stronger than correlations with riskybehaviors that are not overtly self-destructive.
To directly examine the hypothesis that psychiatric problemsmediate the association between deployment and risky behavior,we conducted additional logistic regression analyses parallelingthose described in Section 3.4, each predicting a different specifictype of current risky or self-destructive behavior. As before, tocontrol for possible demographic differences between groups,demographics were entered on the first step. On the second step,we entered prior engagement in that type of risky behavior, as wellas psychiatric condition (one variable representing prior psychi-atric problems and one representing current problems). On thethird and fourth steps, we entered deployment and the interactionof deployment � prior behavior, respectively. To the extent thatpsychiatric problems mediate the effects of deployment on riskybehavior, we would expect effects of deployment on risky behaviorto be weaker when history of psychiatric conditions is controlledthan when it is not.
dds ratios).
d Druguse
Self-harm Suicideattempt
5.32*** 7.19*** 6.29***1.16 1.11 0.732.48*** 4.29*** 14.00***1.90** 1.52* 0.501.33 2.09* 2.09
able 4); prior behavior and prior and current psychiatric condition were entered on. ORs greater than 1.0 indicate risk factors and ORs less than 1.0 indicate protectivered the model. USN ¼ Navy; USMC ¼ Marine Corps.

C.J. Thomsen et al. / Journal of Psychiatric Research 45 (2011) 1321e13311328
Results of these analyses are provided in Table 7. Because theyhave been provided previously (see Table 4) and are unaltered inthe present model, results for the demographic variables enteredon the first step are not tabled. A comparison of Tables 4 and 7 withrespect to the effects of prior behavior, combat deployment, andtheir interaction reveals that controlling for prior and currentpsychiatric conditions had little impact on the pattern of significanteffects: (1) prior behavior remained a strong and significantpredictor of every type of current behavior, even after controllingfor psychiatric problems; (2) combat deployment remaineda significant predictor of the same three outcomes as before (riskyrecreation, drug use, and self-harm); and (3) the interaction of priorbehavior and deployment remained significant for the same twooutcomes as before (risky recreation and self-harm). Thus, therewas little evidence that psychiatric problemsmediated deploymenteffects on risky behavior. Nonetheless, having a psychiatric condi-tion during the current time frame was strongly associated with allfive outcomes. In contrast, having a previous psychiatric conditionwas a significant predictor of only one current outcome (unpro-tected sex).
4. Discussion
The present study is the first, to our knowledge, to comparerates of a broad range of risky or self-destructive behaviors acrossdeploying and non-deploying military personnel and, amongdeployers, before versus after deployment. More specifically, weexamined the effects of deployment on rates of five types of risky orself-destructive behavior that seem quite disparate on the surface.Relationships between some of these behaviors have beendemonstrated in the past (e.g., Muehlenkamp and Gutierrez, 2007;Zuckerman, 2007). However, we could locate no published researchthat has examined associations among such a broad constellation ofrisky behaviors. Although all five behaviors were significantlyassociated, factor-analytic results suggested that they constitutetwo distinct clusters, one representing deliberate self-harm (self-harm and suicide attempts), and the other representing riskybehaviors that may or may not be motivated by self-destructiveimpulses (unprotected sex, risky recreational activities, and illegaldrug use). Nonetheless, because each type of behavior is concep-tually and practically distinct, we analyzed the effects of combatdeployment on individual behaviors rather than on these twounderlying factors.
In some cases, demographic correlates of different types of riskybehavior were similar. For example, married personnel and those inthe Navy (vs. Marine Corps) were generally at lower risk forengaging in all types of risky behavior. In other cases, associationswith demographic factors varied across different types of riskybehavior. For example, although higher ranking personnel, thosewhowere older, and thosewithmore education generally were lesslikely to report all types of risky behaviors, these characteristicswere unrelated to the likelihood of unprotected sex. Patterns of sexdifferences also varied across the risky behaviors examined.Consistent with previous research, men were more likely thanwomen to report risky activities associated with sensation seeking(risky recreational activities, unprotected sex, and illegal drug use;Zuckerman, 2007), but were less likely than women to reportattempted suicide (Zhang et al., 2005). There was no sex differencein the likelihood of self-harm. Although some studies have reportedthat women are more likely than men to engage in self-harm (e.g.,Whitlock et al., 2006), others (e.g., Briere and Gil, 1998), includinga previous study of military recruits (Klonsky et al., 2003), have not.
In the present sample, nearly three-quarters of respondentsreported that they had previously engaged in at least one type ofrisky behavior. The most commonly reported risky behaviors were
engaging in unprotected sexwith someone other than one’s regularpartner and participating in recreational activities that carrieda risk of severe injury or death; each of these was reported byapproximately half of participants. Illegal drug use also wascommon, reported by nearly two in five participants. Self-injuriousbehavior was reported by one in five, and attempted suicide wasreported by one in fourteen participants.
Compared to the USMC population as a whole, the presentsample was somewhat younger, lower in rank, and more likely tobe enlisted (vs. officers). This pattern of non-representativeness iscommon in research sampling military units during times of highoperational tempo (e.g., see Hoge et al., 2004), and likely reflectsthe fact that higher-ranking personnel are more likely than theirlower-ranking counterparts to be occupied with other activitiesduring scheduled research times. Given that risky behavior is mostcommon among young people, the present results may over-estimate rates of risky behavior in the USMC as a whole. However,this bias may be counterbalanced by the likelihood that personnelwho engage in the highest levels of risky behavior and those withthe most severe psychiatric problems may be unavailable forparticipation due to attrition, disciplinary action, or injury, whichwould reduce the apparent prevalence of risky behavior in thesample, relative to its true prevalence in the USMC.
We found that rates of all risky behaviors were considerablyhigher during civilian life and declined significantly upon enteringthemilitary. Given that most of the risky behaviors considered hereare more common at younger ages (Briere and Gil, 1998;Zuckerman, 2007), this decline may be partially attributable tomaturation effects. It also is likely that differences betweenmilitaryand civilian environments contribute to reductions in riskybehavior over time. For example, there is less tolerance of sometypes of risky behaviors in the military than in civilian environ-ments. With respect to illegal drug use in particular, aggressivemilitary policies have led to dramatic reductions over the past threedecades (see Bray et al., 2006; Bray et al., 2003). It is therefore notsurprising that illegal drug use showed the biggest declines fromcivilian to military life, from 39% to 5%. Similar arguments mightapply to reductions in other risky behaviors upon entering themilitary. Of course, the military and civilian worlds may differ innumerous other respects, as well, which also may influence thelikelihood of risky behavior. For example, self-harm and suicideattempts might decrease upon entering the military because themilitary provides an increased sense of purpose, greater structure,or more social support than the average civilian context.
As civilians, non-deployers were significantly more likely thandeployers to report four of five risky behaviors (the exception beingsuicide attempts) and all three psychiatric conditions. These find-ings are consistent with Haley’s (1998) notion of the “healthy-warrior effect”. That is, in an atmosphere in which deployment isthe norm, those who do not deploy are likely to have physical orpsychological problems that prevent them from doing so. (Foradditional evidence supporting this effect see Bell et al., 2010.)However, our results indicate that pre-deployment differencesbetween deployers and non-deployers in both risky behavior andpsychiatric problems were most pronounced during the civiliantime frame. Paradoxically, then, the present data suggest that, withrespect to risky behavior and psychiatric problems, the “healthy-warrior effect”may be substantially attenuated during military life,relative to civilian life.
Both within-subjects and between-group analyses revealedsignificant effects of deployment in increasing the likelihood ofself-harm and risky recreation. In addition, between-groups (butnot within-subjects) analyses indicated significant increases in theodds of illegal drug use among deployers relative to non-deployers,even after controlling for prior drug use. The magnitude of these

C.J. Thomsen et al. / Journal of Psychiatric Research 45 (2011) 1321e1331 1329
changes was small relative to the changes that were observedbetween civilian and military (pre-deployment) life (see Fig. 1). It isimportant to note, however, that any increase in risky behavior overtime occurs in opposition to the general decline in risky behaviorthat accompanies the aging process (Briere and Gil, 1998;Zuckerman, 2007). Because risky behavior is expected to decreaseover time, any increase e even of apparently small magnitude e isnoteworthy.
Of the two types of overtly self-destructive behavior examined,self-harm was significantly impacted by deployment whereassuicide attempts were not. Perhaps effects of deployment onsuicide-related thoughts and behaviors would have been morereadily apparent if we had assessed milder (and more prevalent)forms such as suicide-related ideation. Similarly, the inconsistenteffects of deployment on illegal drug use may reflect the fact thatthis is an uncommon behavior, at least during military life.However, reduced statistical power resulting from low base ratescannot account for the null finding regarding deployment effects onengaging in unprotected sexwith someone other than one’s regularpartner, as this was the most prevalent type of risky behavior in thepresent sample. It is not clear why risky sexual behavior, unlikerisky recreational behavior, was not influenced by deployment.However, one might speculate that motivations unrelated to risk-taking (e.g., sexual attraction, desire for intimacy) play a largerrole in sexual behavior than in the other types of risky behaviorexamined. Also, unprotected sex is only one type of risky sexualbehavior. In a review of characteristics predictive of sexual risk-taking, Hoyle et al. (2000) found that unprotected sex was moreweakly related to sensation seeking than other measures of sexualrisk-taking, such as number of partners and risky encounters (e.g.,sex with strangers). Perhaps other types of risky sexual behaviorare more strongly influenced by deployment.
One important finding of the present research is that not allindividuals were equally likely to demonstrate increases in riskybehavior following deployment. As predicted, deployment effectson risky behaviors were largely restricted to individuals who hadengaged in risky behaviors in the past. In fact, deployment did nothave a significant effect on any of the five risky behaviors examinedamong individuals with no prior history of engaging in that type ofrisky behavior. In contrast, deployment significantly increased fourof the five risky behaviors (the exception being suicide attempts)among individuals who had engaged in that behavior in the past.Thus, deployment does not appear to introduce new risk-takingbehaviors among those who had not engaged in them previously,but rather to increase engagement in risky behaviors among thosewho had already engaged in them. This finding is consistent withthe proposition that previous engagement in risky behavior mayserve as a marker for problems or vulnerabilities that are likely tobe exacerbated by deployment.
In addition to examining effects of deployment on risky and self-destructive behaviors, this study considered a potential mediator ofthese associations: psychiatric problems, including depression,anxiety, and PTSD. Nearly one in four (23%) of respondents reportedthat they had been told by a medical or mental health professionalthat they had one of these disorders. Depression was the mostcommonly reported problem (17%), followed by anxiety (14%), andPTSD (7%). Despite the fact that respondents may underreport nega-tive events due to social desirability concerns, we suspect that thisfiguremayoverestimate the percentage of personnelwithpsychiatricdisorders. This may be the case because people e including healthcare professionalseoftenuse the termsdepression, anxiety, andPTSDin a nontechnical way, in reference to symptoms that do not meetdiagnostic criteria.At thesame time, however, peoplewhoexperiencesignificant symptoms of these disorders do not necessarily commu-nicate those symptoms to a medical or mental health professional.
Therefore, although 23%may overestimate the number of personnelwho have been diagnosed with one of these three psychiatric prob-lems, it may underestimate the number of personnel who suffersymptoms associated with one of these disorders.
Preliminary analyses yielded evidence consistent with a medi-ating role of psychiatric conditions in the association betweendeployment and risky behavior. First, as for risky behavior, deploy-ment was associated with increases in psychiatric problems. Specif-ically, during the current time frame, deployersweremore likely thannon-deployers to report all three psychiatric conditions, and amongdeployers, the likelihood of depression and PTSD (but not anxiety)increased significantly from pre- to post-deployment (cf. Hoge et al.,2004). In addition, psychiatric problems were positively associatedwith riskybehavior.However, direct testsdidnot support amediatingrole for psychiatric problems. Psychiatric conditions e particularlythosewithin thecurrent time frameewereassociatedwith increasedlikelihood of risky behavior, above and beyond the effects of priorrisky behavior. Interestingly, this was true for both overtly self-destructive behaviors and behaviors that were less obviously inten-ded to harm the self. However, controlling for prior and currentpsychiatric conditions did not substantially reduce the impact oncurrent risky behavior of either the main effect of deployment or thedeployment by prior behavior interaction.
As noted previously, our measures of psychiatric conditions areimprecise. Similarly, ourmeasures of risky behaviors are each basedon only one or two items. Reliability and precision would beenhanced by including multiple items to assess each construct. Inaddition, there is causal ambiguity in interpreting associationsbetween current risky behaviors and current psychiatric condi-tions. Although this association could indicate that psychiatricissues are implicated in causing risky behavior, it is equally possiblethat engaging in risky behaviors is a marker of psychiatric prob-lems. That is, people who report engaging in risky, or especiallyself-destructive, behaviors may be most likely to be labeled bymedical or mental health professionals as having psychiatric issues.More generally, causal conclusions must be tempered by the factthat the present research is cross-sectional. Although our inclusionof both within-person and between-group comparisons and thereplication of effects across both types of comparisons enhancesthe validity of the present conclusions, only longitudinal researchcan yield firm causal conclusions.
In addition, it is important to consider thepossibility that responsebiases influenced the present results. The current study relied uponretrospective accounts of risky behaviors as well as psychiatricconditions. Themostobvious retrospectivebiaseunderreportingdueto forgetting e cannot account for the present results, given thatreports of risky behaviors were highest for the earliest period exam-ined (i.e., as a civilian). Another possibility is that psychiatric condi-tions may distort memory, such that individuals suffering fromdepression or PTSD more readily recall traumatic events. However,findings regarding this hypothesis have been inconsistent (Fergussonet al., 2000; Wilson et al., 2008); moreover, generalizing thishypothesis to encompass the recall of risky behaviors is notstraightforward. It also is possible that respondents underreportedtheir risky behaviors and psychiatric problems due to concerns thatsuch disclosures might negatively impact their careers. We do notthink this is likely, however. All personnel were assured that theirresponses were anonymous and surveys were mailed to universityresearchers for processing, rather than being collected by militarypersonnel. Previous research (Olson et al., 2004) has demonstratedthat self-reports of negative events (specifically, childhood abuse) areat much higher levels under these conditions than in official surveysthat would become part of the respondent’s military record.
The present results suggest that post-deployment increases inpsychiatric problems cannot account for increases in risky behavior

C.J. Thomsen et al. / Journal of Psychiatric Research 45 (2011) 1321e13311330
following deployment. Because this is thefirst test of this hypothesis,these results should be replicated. Ideally, this replication willincorporate additional types of risky behavior beyond those consid-ered here, as well as continuous measures of psychiatric symptoms,which are likely to be more valid, as well as more reliable andstatistically powerful, than the single-item categorical measuresused here. In addition to symptoms, further research should incor-porate measures of other potential mediators, including habituationto pain and fear (Joiner’s, 2005; Killgore et al., 2008) aswell as desireto recapture the excitement or “adrenaline rush” frequently experi-enced during deployment (Vaughan, 2006). In addition, givenevidence that symptoms are more strongly predicted by combatexposure than by deployment per se (e.g., Hotopf et al., 2006), itwould be instructive to examine the effects of specific combatexperiences on risky post-deployment behavior. Although thepresent study examined broad patterns of change in risky behaviorbefore and after the first combat deployment, future research mightexaminewhether effects of deployment or combat exposure on riskybehavior vary over the course of the deployment cycle. Someevidence suggests that mental health problems following returnfromcombat deployment peak four to sixmonths after return (Blieseet al., 2007; Grieger et al., 2006; Hoge et al., 2006); the samemay betrue for risky behavior. In addition, future research should examinewhether post-deployment increases in risk-taking are meaningfullyinfluenced by the number or duration of deployments experienced.
Because the present findings indicated that personnel witha history of risky behavior were most likely to exhibit increases inrisky behavior following deployment, it might be advantageous toscreen potential deployers for a prior history of risky behavior. Thiswould allow for identification of personnel at heightened risk ofexperiencing adverse consequences of deployment. However, asdiscussed previously, military personnel are often reluctant todisclose negative personal information when that information willbecome part of their official records (Olson et al., 2004).
Even if it were possible to obtain accurate information abouthistory of risky behavior, however, restricting the combat deploy-ments of personnel who have engaged in risky behavior in the pastmight be ill-advised. There is some evidence that high sensationseekers e who are prone to engage in a range of risky behaviors(Zuckerman, 2007) e may be particularly well-suited to enduringthe stresses and hardships associated with deployment. Militarypersonnel who are higher in risk-taking are more likely to receivemedals for heroism (Neria et al., 2000;Wansink et al., 2008) and areperceived by their peers as being more effective in combat(Himmelstein and Blaskovics,1960). In a sample of former prisonersof war, Solomon et al. (1995) found that high sensation seekers,relative to low sensation seekers, exhibited more adaptive copingstrategies during captivity, displayed fewer feelings of helplessnessand loss of control, and had better psychological outcomes twodecades later. Because the same overt risky behaviors might implyeither greater vulnerability to the stresses of deployment or greaterability to deal with those stresses, further research is necessary todetermine the utility of using previous engagement in riskybehaviors as a tool to aid in deployment decisions. Given thatreducing adverse reactions to deployment has enormous benefitsfor the individual, for the military, and for society at large, furtherexploration of these issues is clearly warranted.
Contributors
Cynthia J. Thomsen was primarily responsible for conceptual-izing the hypotheses and the analytic strategy for this study, con-ducting the statistical analyses and writing the research report. Inaddition, she participated in the design of the overarching projectand the selection and development of measures.
Valerie Stander was primarily responsible for conceptualizingthe overarching project, designing the survey, and obtainingfunding for this study. She supervised data collection efforts,contributed to the conceptualization of the hypotheses and analyticstrategy for the present study, and participated in revisions of themanuscript.
Stephanie McWhorter was involved in design of the overarchingproject, contributed to data collection and formatted the surveyinstrument. In addition, she participated in survey coding and inrevisions of the manuscript.
Mandy M. Rabenhorst assisted with conducting literaturesearches, supervised data entry and data cleaning, and contributedto revisions of the manuscript.
Joel S. Milner supervised the receipt of data and madesubstantial contributions to revisions of the manuscript.
All authors contributed to and have approved the finalmanuscript.
Role of the funding sourceFunding for this study was provided by the Office of Prevention
and Intervention (OPI), Headquarters Marine Corps, Manpower,under Work Unit No. 60202. The OPI had no further role in studydesign; in the collection, analysis, or interpretation of data; or in thewriting of the report. However, OPI personnel reviewed thismanuscript and approved its release for publication.
Conflict of interestNone of the authors declare any potential or actual conflict of
interest that could influence or be perceived to influence thedesign, analysis, or reporting of this study.
Acknowledgements
The views expressed in this article are those of the authors anddo not reflect the official policy or position of the Department of theNavy, Department of Defense, or the U.S. Government. Thisresearch has been conducted in compliance with all applicablefederal regulations governing the protection of human subjects inresearch. The authors acknowledge the generous support of theproject sponsors, Mr. Cruz Martinez and Mr. Gregory Goldstein,Headquarters Marine Corps Office of Prevention and Intervention.Sincere appreciation also is expressed to the command leadershipofMarine Corps Air Station Yuma,1st Marine Logistics Group, CampPendleton, and 1st Marine Division, Camp Pendleton. Finally, weare greatly indebted to the U.S. Marines who participated in thisstudy.
References
Bell NS, Amoroso PJ, Williams JO, Yore MM, Engel Jr CC, Senier L, et al. Demographicphysical and mental health factors associated with deployment of U.S. Armysoldiers to the Persian Gulf. Military Medicine 2010;175:227e37.
Bliese PD, Wright KM, Adler AB, Thomas JL, Hoge CW. Timing of postcombat mentalhealth assessments. Psychological Services 2007;4:141e8.
Boscarino JA. Post-traumatic stress and associated disorders among Vietnamveterans: the significance of combat exposure and social support. Journal ofTraumatic Stress 1995;8:317e36.
Bray RM, Hourani LL, Olmsted KLR, Witt M, Brown JM, Pemberton MR, et al. 2005Department of defense survey of health related behaviors among militarypersonnel. (RTI international Rep. No. RTI/7841/106-FR). Research Triangle Park,NC: Research Triangle Institute; 2006.
Bray RM, Hourani LL, Rae KL, Dever JA, Brown JM, Vincus AA, et al. 2002 Depart-ment of defense survey of health related behaviors among military personnel(RTI international Rep. No. RTI/7841/006-FR). Research Triangle Park, NC:Research Triangle Institute; 2003.
Brenner LA, Gutierrez PM, Cornette MM, Betthauser LM, Bahraini N. A qualitativestudy of potential suicide risk factors in returning combat veterans. Journal ofMental Health Counseling 2008;30:211e25.
Bricknell MC, Amoroso PJ, Yore MM. What is the risk associated with beinga qualified military parachutist? Occupational Medicine 1999;49:139e45.

C.J. Thomsen et al. / Journal of Psychiatric Research 45 (2011) 1321e1331 1331
Briere J, Gil E. Self-mutilation in clinical and general population samples: prevalence,correlates, and functions. American Journal of Orthopsychiatry 1998;68:609e20.
Browne T, Iversen AC, Hull L, Workman L, Barker C, Horn O, et al. How do experi-ences in Iraq affect alcohol use among male UK armed forces personnel?Occupational and Environmental Medicine 2008;65:628e33.
Bryan CJ, Cukrowicz KC, West CL, Morrow CE. Combat experience and the acquiredcapability for suicide. Journal of Clinical Psychology 2010;66:1044e56.
Calhoun PS, Elter JR, Jones ER, Kudler HS, Straits-Troster K. Hazardous alcohol useand receipt of risk reduction counseling among U.S. veterans of the wars in Iraqand Afghanistan. Journal of Clinical Psychiatry 2008;69:1686e93.
Catlin Boehmer TK, Flanders WD, McGeehin MA, Boyle C, Barrett DH. Postservicemortality in Vietnam veterans: 30-year follow-up. Archives of Internal Medi-cine 2004;164:1908e16.
Centers for Disease Control. Current trends: postservice mortality among Vietnamveterans. Morbidity and Mortality Weekly Report 1987;36:61e4.
Fear NT, Iversen AC, Chatterjee A, Jones M, Greenberg N, Hull L, et al. Risky drivingamong regular armed forces personnel from the United Kingdom. AmericanJournal of Preventive Medicine 2008;35:230e6.
Fergusson DM, Horwood LJ, Woodward LJ. The stability of child abuse reports:a longitudinal study of the reporting behaviour of young adults. PsychologicalMedicine 2000;30:529e44.
Grieger TA, Cozza SJ, Ursano RJ, Hoge C, Martinez PE, Engel CC, et al. Posttraumaticstress disorder and depression in battle-injured soldiers. American Journal ofPsychiatry 2006;163:1777e83.
Haley RW. Point: bias from the “healthy-warrior effect” and unequal follow-up inthree government studies of health effects of the Gulf War. American Journal ofEpidemiology 1998;148:315e23.
Hall DP. Stress, suicide, and military service during Operation Uphold Democracy.Military Medicine 1996;161:159e62.
Hansen-Schwartz J, Jessen G, Andersen K, Jørgensen HO. Suicide after deploymentin UN peacekeeping missionsdA Danish pilot study. Crisis 2002;23:55e8.
Himmelstein P, Blaskovics TL. Prediciton of an intermediate criterion of combateffectiveness with a biographical inventory. Journal of Applied Psychology1960;44:166e8.
Hoge CW, Auchterlonie JL, Milliken CS. Mental health problems, use of mentalhealth services, and attrition from military service after returning fromdeployment to Iraq or Afghanistan. Journal of the American Medical Association2006;295:1023e32.
Hoge CW, Castro CA, Messer SC, McGurk D, Cotting DI, Koffman RL. Combat duty inIraq and Afghanistan, mental health problems, and barriers to care. NewEngland Journal of Medicine 2004;351:13e22.
Hotopf M, Hull L, Fear NT, Browne T, Horn O, Iversen A, et al. The health of UKmilitary personnel who deployed to the 2003 Iraq War: a cohort study. Lancet2006;367:1731e41.
Hoyle R, Fejfar MC, Miller JD. Personality and sexual risk-taking: a quantitativereview. Journal of Personality 2000;68:1203e31.
Jobe JB, Holgate SH, Scrapansky TA. Risk taking as motivation for volunteering fora hazardous experiment. Journal of Personality 1983;51:95e107.
Joiner TE.Whypeople die by suicide. Cambridge,MA:HarvardUniversity Press; 2005.Kang HK, Bullman TA, Macfarlane GJ, Gray GC. Mortality among US and UK veterans
of the Persian Gulf War: a review. Occupational and Environmental Medicine2002;59:794e9.
Kaplan MS, McFarland BH, Huguet N. Firearm suicide among veterans in the generalpopulation: findings from the national violent death reporting System. Journalof Trauma-Injury Infection and Critical Care 2009;67:503e7.
Killgore WDS, Cotting DI, Thomas JL, Cox AL, McGurk D, Vo AH, et al. Post-combatinvincibility: violent combat experiences are associated with increased risk-taking propensity following deployment. Journal of Psychiatric Research 2008;42:1112e21.
Klonsky ED. The functions of deliberate self-injury: a review of the evidence.Clincial Psychology Review 2007;27:226e39.
Klonsky ED, Oltmanns TF, Turkheimer E. Deliberate self-harm in a nonclinicalpopulation: prevalence and psychological correlates. American Journal ofPsychiatry 2003;160:1501e8.
Knapik JJ, Marin RE, Grier TL, Jones BH. A systematic review of post-deploymentinjury-related mortality among military personnel deployed to conflict zones.BMC Public Health 2009;9.
Koenen KC, Lyons MJ, Goldberg J, Simpson J, Williams WM, Toomey R, et al. Co-twin control study of relationships among combat exposure, combat-relatedPTSD, and other mental disorders. Journal of Traumatic Stress 2003;16:433e8.
Laye-Gindhu A, Schonert-Reichl KA. Nonsuicidal self-harm among communityadolescents: understanding the “whats” and “whys” of self-harm. Journal ofYouth and Adolescence 2005;34:447e57.
Leigh BC, Temple MT, Trocki KF. The relationship of alcohol use to sexual activity ina U.S. national sample. Social Science Medicine 1994;39:1527e35.
Marine Corps Community Services. Marine Corps Community Services demo-graphics update. Retrieved March 18, 2008, from http://www.usmc-mccs.org/aboutmccs/downloads/pom/Demographics%20Update_Dec2007.pdf 2007,December.
Matsumoto T, Yamaguchi A, Asami T, Okada T, Yoshikawa K, Hirayasu Y. Charac-teristics of self-cutters among male inmates: association with bulimia anddissociation. Psychiatry and Clinical Neurosciences 2005;59:319e26.
Muehlenkamp JJ, Gutierrez PM. Risk for suicide attempts among adolescents whoengage in non-suicidal self-injury. Archives of Suicide Research 2007;11:69e82.
Nell V. Why young men drive dangerously: implications for injury prevention.Current Directions in Psychological Science 2002;11:75e9.
Neria Y, Solomon Z, Ginzburg K, Dekel R. Sensation seeking, wartime performance,and long-term adjustment among Israeli war veterans. Personality and Indi-vidual Differences 2000;29:921e32.
O’Toole BI, Cantor C. Suicide risk factors among Australian Vietnam era draftees.Suicide and Life-Threatening Behavior 1995;25:475e88.
Olson CB, Stander VA, Merrill LL. The influence of survey confidentiality andconstruct measurement in estimating rates of childhood victimization amongNavy recruits. Military Psychology 2004;16:53e69.
Silverman MM, Berman AL, Sanddal ND, O’Carroll PW, Joiner Jr TE. Rebuilding thetower of Babel: a revised nomenclature for the study of suicide and suicidalbehaviors Part 2: suicide-related ideations, communications, and behaviors.Suicide and Life-Threatening Behavior 2007;37:264e77.
Solomon Z, Ginzburg K, Neria Y, Ohry A. Coping with war captivity: the role ofsensation seeking. European Journal of Personality 1995;9:57e70.
Stea JB, Anderson MA, Bishop JM, Griffith LJ. Behavioral health force protection:optimizing injury prevention by identifying shared risk factors for suicide,unintentional injury, and violence. Military Medicine 2002;167:944e9.
Thoresen S, Mehlum L. Risk factors for fatal accidents and suicides in peacekeepers:is there an overlap? Military Medicine 2004;169:988e93.
Thoresen S, Mehlum L, Moller B. Suicide in peacekeepers: a cohort study ofmortality from suicide in 22,275 Norwegian veterans from internationalpeacekeeping operations. Social Psychiatry and Psychiatric Epidemiology 2003;38:605e10.
Vaughan D. Risky business. Today’s Officer; 2006:21e4.Wansink B, Payne CR, van Ittersum K. Profiling the heroic leader: empirical lessons
from combat-decorated veterans of World War II. The Leadership Quarterly2008;19:547e55.
Whitlock J, Eckenrode J, Silverman D. Self-injurious behaviors in a college pop-ulation. Pediatrics 2006;117:1939e48.
Whitlock J, Knox KL. The relationship between self-injurious behavior and suicidein a young adult population. Archives of Pediatric and Adolescent Medicine2007;161:634e40.
Wilson JP, Jones M, Hull L, Hotopf M, Wessely S, Rona RJ. Does prior psychologicalhealth influence recall of military experiences? A prospective study. Journal ofTraumatic Stress 2008;21:385e93.
Wojcik BE, Akhtar FZ, Hassell LH. Hospital admissions related to mental disordersin U.S. Army soldiers in Iraq and Afghanistan. Military Medicine 2009;174:1010e8.
Wong A, Escobar M, Lesage A, Loyer M, Vanier C, Sakinofsky I. Are UN peacekeepersat risk for suicide? Suicide and Life-Threatening Behavior 2001;31:103e12.
Zhang J, McKeown RE, Hussey JR, Thompson SJ, Woods JR. Gender differences in riskfactors for attempted suicide among young adults: findings from the thirdnational health and nutrition examination survey. Annals of Epidemiology2005;15:167e74.
Zuckerman M. Sensation seeking and risky behavior. Washington, DC: AmericanPsychological Association; 2007.
REPORT DOCUMENTATION PAGE
The public reporting burden for this collection of information is estimated to average 1 hour per response, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing the burden, to Washington Headquarters Services, Directorate for Information Operations and Reports, 1215 Jefferson Davis Highway, Suite 1204, Arlington, VA 22202-4302, Respondents should be aware that notwithstanding any other provision of law, no person shall be subject to any penalty for failing to comply with a collection of information if it does not display a currently valid OMB Control number. PLEASE DO NOT RETURN YOUR FORM TO THE ABOVE ADDRESS. 1. Report Date (DD MM YY) 29 10 08
T 2. Report Type Journal submission
3. DATES COVERED (from - to) August 2006 to August 2007
4. TITLE AND SUBTITLE Effects of Combat Deployment on Risky and Self-Destructive Behavior Among Active Duty Military Personnel
5a. Contract Number: see 5b. Grant Number: instructions 5c. Program Element: below 5d. Project Number: 5e. Task Number: 5f. Work Unit Number: 60202
6. AUTHORS Cynthia, J. Thomsen, PhD, Valerie A. Stander, PhD, Mandy M. Rabenhorst, PhD, Stephanie K. McWhorter, MA, Joel S. Milner, PhD
7. PERFORMING ORGANIZATION NAME(S) AND ADDRESS(ES) Commanding Officer Naval Health Research Center 140 Sylvester Rd San Diego, CA 92106-3521
8. PERFORMING ORGANIZATION REPORT NUMBER Report 09-03
8. SPONSORING/MONITORING AGENCY NAMES(S) AND ADDRESS(ES) Commanding Officer Commander Naval Medical Research Center Navy Medicine Support Command 503 Robert Grant Ave P.O. Box 140 Silver Spring, MD 20910-7500 Jacksonville, FL 32213-0140
10. Sponsor/Monitor's Acronyms(s) NMRC/NMSC 11. Sponsor/Monitor's Report Number(s)
12 DISTRIBUTION/AVAILABILITY STATEMENT Approved for public release; distribution is unlimited.
13. SUPPLEMENTARY NOTES
14. ABSTRACT (maximum 200 words)
Effects of deployment on high-risk and self-destructive behaviors were examined. Active duty military personnel (N = 2,116) described their deployment experiences and their participation in risky recreational activities, unprotected sex, illegal drug use, self-injurious behavior, and suicide attempts during three time frames (civilian, military pre-deployment, and military post-deployment). Personnel that had not deployed, relative to those that had deployed, were more likely to report high-risk behavior as civilians, but not after entering the military. Deployment was associated with increases in risky recreational behavior, illegal drug use, and self-injurious behavior. However, this effect was restricted to personnel with a prior history of engaging in high-risk behavior; among those with no prior history, effects of deployment on high-risk behavior were negligible.
14. SUBJECT TERMS deliberate self-harm, suicide attempts, illegal drugs, high-risk sex, high-risk recreation, combat deployment, Marine
Corps 16. SECURITY CLASSIFICATION OF: 17. LIMITATION
OF ABSTRACT UNCL
18. NUMBER OF PAGES
13
18a. NAME OF RESPONSIBLE PERSON Commanding Officer a. REPORT
UNCL b.ABSTRACT
UNCL b. THIS PAGE
UNCL 18b. TELEPHONE NUMBER (INCLUDING AREA CODE) COMM/DSN: (619) 553-8429
Standard Form 298 (Rev. 8-98) Prescribed by ANSI Std. Z39-18