effects and outcome of a policy of intermittent imatinib treatment in elderly patients with chronic...
TRANSCRIPT

Effects and outcome of a policy of intermittent Imatinib treatment in elderly patients with
chronic myeloid leukemia (CML)
D. Russo , M Baccarani et alBlood, 27 June 2013
MOHSIN
MAQBOOLPhd student aiims, new delhi

Introduction Chronic myeloid leukemia (CML)
Chronic myeloid leukemia (CML) – Chromosomal aberration t(9;22) [Philadelphia (Ph)]chromosome Oncogenic BCR-ABL gene fusion dysregulated expansion of myeloid tissue in the body
• Without effective treatment, the chronic phase progresses to an advanced phase
Blast crisisChronic phase Accelerated phase
BCR-ABLABL
Fusion protein
with tyrosine kinase activity
22
BCR
Ph (or 22q-)
99 q+
1
P210 BCR-ABLl
P190 BCR-ABL2-11
2-11
Chromosome 9
c-BCR
Chromosome 22
c-ABL
2-11
Exons
Introns
CML breakpoints
ALL breakpointst (9;22) translocation BCR-ABL gene structure

Evolution of therapy for CML
Pavlů J et al. Blood 2011;117:755-763

Contd….
TKIs targeting the BCR-ABL oncogene protein – standard therapy in CML
Imatinib and now 2G TKIs - nilotinib and dasatinib are approved for the treatment of CML
Imatinib therapy- changed the prognosis for CML patients

JCO, May 16, 2011
Imatinib
• Population-based Swedish Cancer Registry• Patients diagnosed with CML from 1973 to 2008 (35 yrs) (n = 3173; 1796 males and 1377 females; median age, 62 years)• Patients were categorized into five age groups and five calendar periods, the last being 2001 to 2008
• Shows a major improvement in outcome of patients with CML up to 79 years of age diagnosed from 2001 to 2008

Longer Time to Progression With Gleevec ( IRIS Trail)
Michael Deininger, T. P.Hughes , Blood

Imatinib – Excellent efficacy,…..Treatment related adverse effects remain problematic and reduce the quality of
life

Opportunity to maintain remission after discontinuation of imatinib - desirable
Imatinib discontinuation studies – demonstrated 40% of CML patients can maintain remission at 12 to 36 months after imatinib discontinuation – careful selection
Imatinib discontinuation in patients with persisting detectable BCR-ABL1 relapse (irrespective of molecular and cytogenetic response)
Goh HG et al, Leuk Lymphoma. 2009 , Kuwabara A et al, Blood 2010

Stop Imatinib Trail – STIMDiscontinuation of Imatinib in Patients with Chronic Myeloid
Leukemia Who Have Maintained Complete Molecular Response
• Eligibility (N = 100): • Molecular relapse: 61 patients
– 58 relapses during first 7 months
– 3 relapses at 19, 20 and 22 months
• Overall probability of maintenance of CMR at 24 and 36 months: 39% ( =40%)
All relapsed n= 58 patients sensitive to TKI rechallenge◦ Imatinib (n=48)◦ Nilotinib (n=5) ◦ Dasatinib (n=5)
38 patients - in DMR without any treatment Median follow up is 54 months (range : 24- 71).
Mahon FX, et al, Lancet Oncol 2010, ASH 2011, 2013

Branford S et al, Clin Can Rech ,2007
• Identifying the factors associated with stable, undetectable BCR-ABL1 for CML patients eligible for therapy discontinuation……
is Important
BCR ABL1 transcripts remain detectable
• BCR ABL1 transcripts remain detectable for many years in most of the patients with Imatinib

Contd….
Results have improved by the use of 2G TKIs, but toxicity remains an issue, if proven more successful , majority of patients have to take life long treatment
Concept of cure in attractive , but whether to continue life long therapy or to discontinue - is still debatable
Other possibilities or possible policies affordable in such settings
?? Identification of a schedule of IM (TKIs) , sufficient to maintain response and avoid progression without discontinuation and with less compliance

Aim INTERIM study, designed (5 years ago) to investigate -
alternative policy of treatment, intermittent administration of IM, would affect the surrogate markers of outcome, the cytogenetic and molecular response, as well as the outcome [PFS] and [OS]).

Objectives
To evaluate the proportion of patients who remained in CCgR after 1 year on INTERIM (study design 5year ago)
To determine the proportion of patients who would lose MMR, who would lose complete hematologic response
Who would develop BCR-ABL kinase(KD) domain point mutations
To evaluate the over all survival

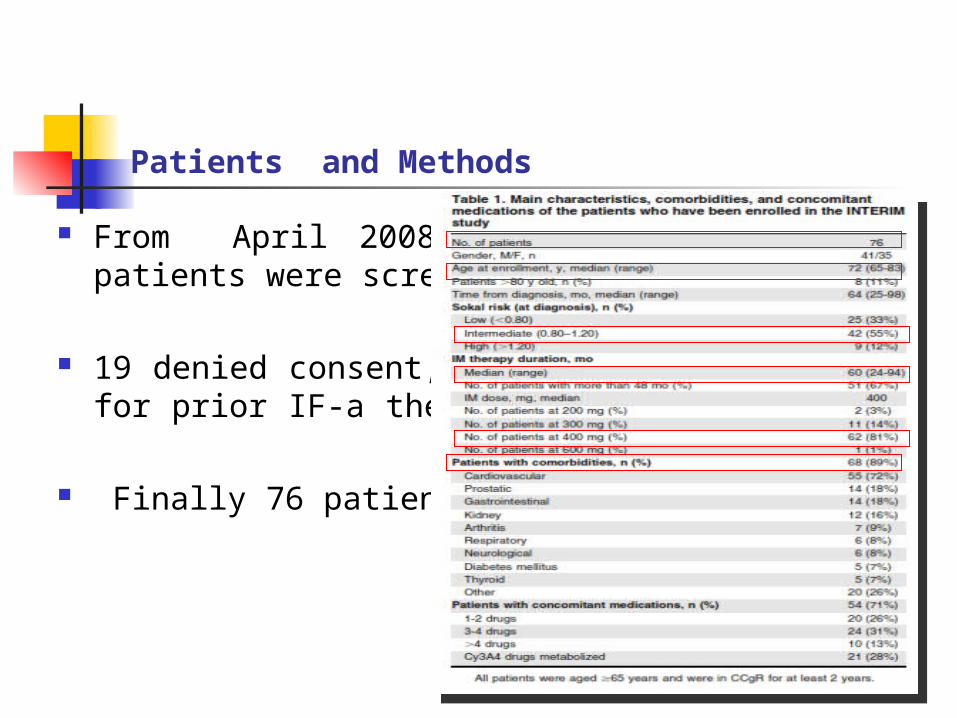
Patients and Methods
CML patients (Ph+ve, BCR-ABL +) , age >65 years treated with IM frontline (IM for 2 years or longer and in stable CCgR)
CCgR Stability documented by chromosome banding analysis(before and at the time of enrolment)
Written informed consent was taken and study conducted according to declaration of Helsinki
Patients and Methods
From April 2008 to Nov 2009, 114 CML patients were screened for the study
19 denied consent, another 19 were excluded for prior IF-a therapy or CCgR not achieved
Finally 76 patients enrolled
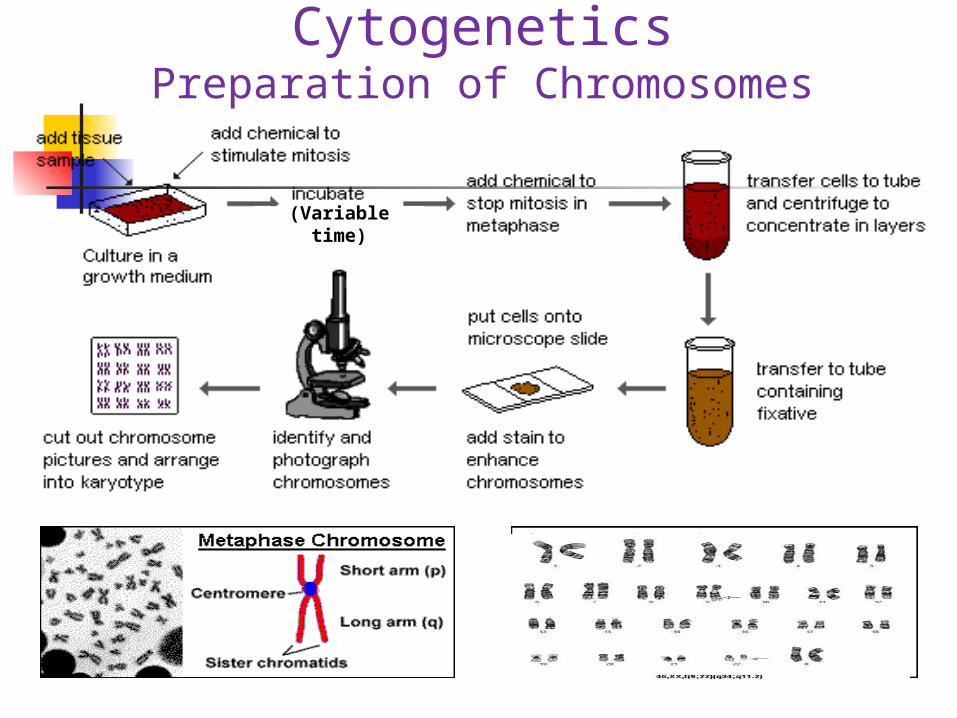
CytogeneticsPreparation of Chromosomes
(Variable time)

RT- PCR followed by RQ-PCR (RT-Q-PCR) (measurement of BCR-ABL1 transcripts)
PCR machine
RT_ PCRRNA
extraction
cDNA synthesis
RQ-PCR ( measurement of transcripts)

INTERIM Conditioning regime/plan
Multicentric , Phase II study, - to investigate how intermittent Tx with standard –dose IM would modify the surrogate markers of outcome, and treatment out come
Standard IM therapy - daily administration of IM at any dose (400mg) Intermittent IM therapy (INTERIM)- treatment same dose of IM
( 400mg%) given as Schedule: 1 week ON /1 week OFF for the 1st month (weeks 1-
4); 2 weeks ON /2 weeks OFF for the 2nd and 3rd months (weeks 5-12); 1 month ON/1 month OFF from the 4th month (week 13) to the 12th month and thereafter

Conditioning regime/plan….
Patients who lost the CCgR resumed the prestudy- daily IM treatment
Patients who lost the major molecular response (MMR) alone within the first year had to continue the intermittent schedule
After the first year, the patients who lost MMR alone were allowed to go back to the prestudy continuous treatment.

Response monitoring
Clinical evaluation, physical examination, blood counts, and differential biochemical tests- enrollment (baseline) and at every 3 months
Cytogenetics: karyotypes performed according to System HCN, evaluation of CCgR based on marrow cell metaphases and FISH performred for confirmation
BCR-ABL Transcript level: Real-time Quantitative reverse transcription polymerase chain reaction (RT-Q-PCR) , at base line and at every 3 months during the study
In case of loss of CCgR orMMR , BCR-ABL KD point mutation analysis performed

Statistics
Standard descriptive statistics such as mean, median, range and proportions used to summarize the patient sample
X2 test used to compare differences in percentages and Mann-Whitney U test to compare continuous variables
Kaplan-Meier method used to estimate survival (PFS,OS, CCgR, MMR loss)
Cox proportional hazard regression model for univarite and multivariate analysis

BASE LINE76 on INTERIMBASE LINE
76 on INTERIM
@ First year70 Pts on INTERIM
@ First year70 Pts on INTERIM
06 pts lostCCgR and MMR
@ 6 Months
6 patients Resumed IM
6 pts regained CCgR & MMR
07 pts lostCCgR and MMR
@ 13 - 24 Months
07 pts Resumed IM
06 patients regained CCgR & MMR
01 patient LFU
05 pts lost MMR
@ 13 - 24 Months
03 pts Resumed IM
03 patients regained CCgR & MMR
1 pt discontinuedINTERIM- artrail
fibrilation @ 15 Mo
1 pt died –MI in CCgR & MMR
@ 24 Mo
1 pt refused to continue on INTERIM
@ 24 Mo
@ 2nd year55 Pts on INTERIM
@ 2nd year55 Pts on INTERIM
INTERIM studyall the events occurring during the 48 mo of intermittent treatment
with IM are reported

01 pt lostCCgR and MMRFrom 24- 36 MO
01 patient Resumed IM
01 pts regained CCgR & MMR
02 pts lost MMR alone
@ 24 – 36 Months
1 pt died because of intracranial hemorrage in
CCgR & MMR @ 36 Mo
@ 4th year51 Pts on INTERIM
@ 4th year51 Pts on INTERIM
@ 2nd year55 Pts on INTERIM
@ 2nd year55 Pts on INTERIM
@ 3rd year51 Pts on INTERIM
@ 3rd year51 Pts on INTERIM

Results
76 patients (in CCgR & MMR) enrolled in INTERIM study
13 Patients (17%) lost CCgR and MMR @ 6- 27 mo…..resumed
continous IM and achieved CCgR & MMR , 01 Pt LFU
First CBA ( CCgR) @ 6 Mo,…..06 patients (8%) lost at 6Mo and & 07 pts at 13-27 mo
Estimated CCgRMaintainig was 92% (95% CI: 86-98) at 12 months and
81% (95% CI: 71-90) at 48 months
Estimated CCgRMaintainig was 92% (95% CI: 86-98) at 12 months and
81% (95% CI: 71-90) at 48 months

Results……
Loss of MMR occurred 3-9 Mo before loss of CCgR & all patients discontinued INTERIM study resumed daily IM, regained CCgR & MMR @ median of 7 & 6 mos respectively……in CP @ median FU of 48.5 Mos
5 more patients lost MMR alone @ 13-24 Mos, first MMR detected after 3 mo
6 patients lost MMR during first 12 Mos and 12 patients lost MMR at 13-24 Mos,…. And 03 patients at 36
MosEstimated MMR loss
was 80% (95% CI: 71-89) at 12 mo and 63% (95% CI: 52-74) at 48 mo.

Results…
All the patients who lost MMR alone continues IM daily and regained MMR after median 3 mo and are in CP after median Fu of 48 mos
Univariate and multivariate analysis - Age , sokal score , sex, base line BCR-ABL transcript level and duration of IM therapy before INTERIM not associated with loss of CCgR and MMR
No patient developed BCR-ABL KD mutations, none of the patients progressed to AP or BP ( 1 left study, 2 died of MI & I hemorrhage )PFS. Estimated PFS was 100% at 12 months and 96% (95% CI: 91-100)
at 48 months. The events were 2 deaths in remission (CCgR and MMR). Nopatients progressed to AP or BP.

Contd…
No patients complained of new or more severe side effects during the “on” months
Mild to grade 1 side effects were fluid retention, muscle cramps, skin erythema were in 20 pats and all side effects disappread in 8- 10 mos

Discussion
Prospective phase II, single arm study, - effect of policy of TKI Tx reduction
• who are optimal responders• Not fit for Tx discontinuation• Pat. Selection based on age
Schedule of 01 month “on” and 01 month “off” selected from several possibilities,….simplicity , pats show molecular relapse rapidly,
Intermittent dose taken into consideration, as the dose discontinuation or dose reduction have molecular relapses and emergence of resistant clones

Contd….
CCgR and molecular response was considered most surrogate markers for survival at the time of study design
Patients , carefully monitored & followed and protocol required resuming the standard IM dose if CCgR was lost and if MMR lost after the completion of the first year INTERIM
With the recommendations and stringent monitoring all patients regained CCgR & MMR with daily IM Tx
No BCR-ABL KD point mutation emerged & all patients remained free from progression to AP or BC - ultimate goal

Contd…
Study cannot prove policy of INTERIM Tx better or worse than the standard policy of continuing
Cannot lead to the recommendation to extend this policy either to the patients in eligible for Tx discontinuation or to the patients undergoing less monitoring cyto or molecular response

Conclusion
TKIs(Imatinib, 2G TKIs - nilotinib and dasatinib) targeting the BCR-ABL oncogene protein – standard therapy in CML
Tx realted problems ( toxicity, life long drug continuation and compliance remains problem) , so alternative Tx
Optimal responders to IM and eligible pts for INTERIM showed – 50% dose reduction result loss of CCgR in 17 %, MMR in 18 %, all can achieve response by standard IM dose
No patient died of progression or by leukemia,… affects cytogenetic and molecular response, but not the outcome
Results are not better or alternative for discontinuation study but help to open small door yet unexplored alternative policies of Tx

Thank you …!!

Thank you ..!

Background: Cancer Classification
No general approach has been made for identifying new cancer classes (class discovery) and assigning tumors to known classes(class prediction).
A generic approach to cancer classification based on gene expression monitoring by DNA microarrays is described and applied to acute human leukemia as a test case.
http://www.nejm.org/action/showMediaPlayer?doi=10.1056%2FNEJMoa1301689&aid=NEJMoa1301689_attach_1&area=
http://compbio.cs.brown.edu/aml_tcga/