effect of nursery environment on state regulation in very-low-birth-weight premature infants
TRANSCRIPT
INFANT BEHAVIOR AND DEVELOPMENT 13, 287-303 (19901
Effect of Nursery Environment on State Regulation in Very-low-Birth-
Weight Premature Infants
BARBARA FAJARDO, MARGARET BROWNING, DAVID FISHER, AND JOHN PATON
Michael Reese Hospital and Medical Center
Very-low-birth-weight fVLBW1 neonates were observed in two different nursery en- vironments from 32 to 36 weeks post conceptional age. Half of the subjects (n= 12) were observed in o control environment and the other half fn= 121 were placed in on olternative nursery environment more contingent on the infants’ states ond less stimulating than the control nursery. Subiects’ spontaneous states and state-relevant behaviors were recorded by tramed observers at the beginning and end of the 4-week period. These observations were used to measure state organizotion. We found a greater developmental change for infonts in the alternotive nursery. Infants in the alternative nursery group had longer state durations ot 36 weeks and fewer state changes per hour. This indicates that o nursery environment with diurnal cycles, less intense unpatterned stimuli, and a priority of state-contingent nursing can promote steodiness and longer durations of sleep states in vulnerable preterm neonates.
preterm neonote State regulation
nursery environment sleep development
Neonatal state is recognized as a window to early central nervous system (CNS) functioning (Parmelee, 1970; Sostek & Anders, 1981). The critical weeks during which organized states emerge are 32 to 36 weeks postcon- ceptional age (PCA) (Parmelee, Wenner, Akiyama, Schultz, & Stem, 1967), a period of hospitalization for the very-low-birth-weight (VLBW) pre- mature neonate. The hospital nursery environment is usually stressful (Lawson, Daum, & Turkewitz, 1977) and is disruptive to the spontaneous development of state organization in these neonates.
State organization is determined by both endogenous maturational factors and by exogenous environmental factors (Anders, Keener, & Krae- mer, 1985). This study was designed to assess the influence of the hospital nursery environment on the emerging state organization of very premature neonates. Knowledge about the impact of the environment and caretaking
We gratefully acknowledge Steven Shevell for his assistance in methodology and statistical analysis. This research was supported by grants from Barker Welfare and Hasbro Children’s Foundations.
Correspondence and requests for reprints should be sent to Barbara Fajardo, Develop- mental Institute K + K 5, Michael Reese Hospital and Medical Center, Lake Shore Drive at 31sl Street, Chicago, IL 60616.
287

288 FAJARDO, BROWNING, FISHER, AND PATON
practices can be applied to provide the best possible developmentally compensatory nursery.
We examine here whether a revised nursery environment can enable infants to develop superior state organization. The study contrasts the influence of two different nursery environments on state organization at 36 weeks PCA, after the infants were cared for in these nurseries for 4 weeks from 32 to 36 weeks PCA. This period corresponds with the emergence of organized states in development (Par-melee et al., 1967).
We measured the effects of contrasting environmental contexts (as in the work of Lawson, Turkewitz, Platt, & M&u-ton, 1985) rather than the effects of specific environmental or caretaking events and procedures (as in the work of Als et al., 1986). The two nursery environments differed in the clarity of diurnal cycles, in the intensity of nonpatterned light, sound and activity levels, and in the priority given to state-contingent nursing care.
We also examined the specific question of whether active sleep would be more affected by nursery environment than quiet sleep. Anders et al. (1985) concluded that, in infants studied after term, changes in quiet sleep are biologically rather than environmentally mediated, because they found the rate at which quiet sleep decreased to be the same for infants of equivalent postconceptional age, regardless of whether they were born prematurely or at term. On the other hand, changes in active sleep and wakefulness are more sensitive to exogenous and environmental factors. For example, active sleep decreases when infants are observed in a sleep lab compared to at home (Sostek & Anders, 1981). Thoman et al. (1985) found changes in active sleep and wakefulness, but not in quiet sleep, for infants given theophylline. These findings suggest that active sleep may have different functions in development than quiet sleep.
METHOD
Subjects Results are reported for 24 infants, 12 cared for in each nursery. Four additional infants had been enrolled at 32 weeks PCA but became sick while still in the nursery and therefore were dropped from the study. Two other infants were dropped because they were discharged or trans- ferred out of the unit before 36 weeks PCA. Another infant was excluded from the sample after data analysis because her scores on most variables were more than 2 SDS from the mean, raising concerns about organic CNS dysfunctions.
The 24 infants who completed the study were from the special care nursery of a large metropolitan hospital. All met the following criteria: (a) Age at birth was less than 31 weeks gestational age (as determined by maternal history, except in cases where this was apparently inaccurate,

NURSERY EFFECTS ON STATE REGULATION 289
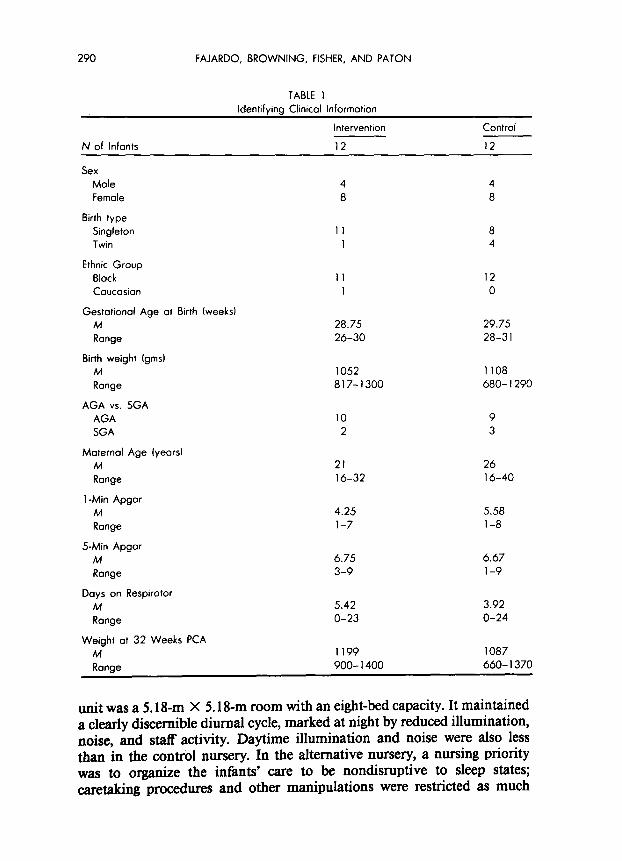
when age was determined instead by a revised version of Dubowitz’s infant maturity rating; Ballard, Kazmaier, & Driver, 1977); (b) birth- weight was under 1300 gms; (c) birth-weight was appropriate-for-gesta- tional-age (AGA; five infants selected to be AGA were later determined to be small-for-gestational-age (SGA) according to subsequently available maternal history but were not dropped from the study because their recovery course and medical management were no different than the other subjects); (d) health status permitted transfer from intensive to interme- diate care by 3 1.5 weeks PCA; (e) infants were “healthy,” that is, they had no medical or apparent developmental complications (this criterion eliminated infants with congenital abnormalities, major intraventricular hemorrhages, severe respiratory distress syndrome, or any medical problem severe enough to require readmission to intensive care after 32 weeks PCA. All but one child were from black urban families, with mothers considered by the nursery staff to be stable and responsible. Table 1 describes the two groups of infants.
There were no significant differences between groups at the outset on medical, social, or developmental characteristics. Age at birth and mother’s age were marginally different, p < . 10. The selection criteria made the sample an unusually homogeneous cohort of premature new- borns.
Procedures All subjects were initially in intensive care and were transferred to the main intermediate care unit by 31.5 weeks PCA. The first state observation was done at 32 weeks PCA in the main intermediate care unit after the infant had been there for at least 3 days. After this observation, subjects were assigned alternately to one of two nursery environments, remaining there for at least 4 weeks until discharge. At the conclusion of these weeks, when subjects were 36 weeks PCA, they were observed again for state organization. On the few occasions an infant required readmission to intensive care, he or she was dropped from the study, and the next infant enrolled was assigned to the appropriate nursery group to replace the other. On two occasions nursery priorities took precedence over research design, and subjects were assigned to a nursery group according to availability of beds on the units.
Experimental Groups Nursery Environment #I: Alternative Nursery. Subjects assigned to the
alternative nursery were transferred out of the main intermediate care unit after the first observation session. The alternative nursery was designed to be more sensitive to the development of premature newborns than the main intermediate care unit (Nursery #2: control nursery). The alternative
290 FAJARDO, BROWNING, FISHER, AND PATON
TABLE 1 Identifying Clinical Information
N of Infants
Sex Male Female
Birth type Singleton Twin
Ethnic Group Black
Caucasian
Gestotionol Age at Birth (weeks1 M Range
Birth weight fgmst M Range
AGA vs. SGA AGA
SGA
Maternal Age iyearsl M Range
1 -Min Apgar M Range
5-Min Apgar M Range
Days on Respirator M
Range
Weight at 32 Weeks PCA M Range
Intervention Control
12 12
4 4 8 8
I1 8 I 4
II 12 1 0
28.75 29.75 26-30 28-3 I
1052 1108 817-1300 680-I 290
10 9 2 3
21 26 16-32 16-40
4.25 5.58 l-7 l-8
6.75 6.67 3-9 l-9
5.42 3.92 O-23 O-24
1199 1087 900-l 400 660-I 370
unit was a 5.18-m X 5.18-m room with an eight-bed capacity. It maintained a clearly discernible diurnal cycle, marked at night by reduced illumination, noise, and staff activity. Daytime illumination and noise were also less than in the control nursery. In the alternative nursery, a nursing priority was to organize the infants’ care to be nondisruptive to sleep states; caretaking procedures and other manipulations were restricted as much

NURSERY EFFECTS ON STATE REGULATION 291
as possible to the time just before feeding. In general, the alternative nursery environment was designed to (a) promote a definite diurnal cycle, (b) reduce unpatterned intense stimulation, and (c) encourage state-con- tingent caretaking.
Illumination level was measured with a Gossen Lunasix light meter at the side of a bassinette every 15 min for a 24-hour period. The average light level from 7 a.m. to 7 p.m. was 60.0 footcandles; from 7 p.m. to 7 a.m., average light level was 0.5 footcandles. This nursery had a flexible lighting system allowing for many light conditions. There were overhead incandescent recessed lights with an individual on-off control for each patient area and the central area of the room (the central area lights also had dimmer control). Fluorescent lights on the wall above each infant station provided either direct or indirect lighting. Outside windows with adjustable blinds were along one wall. The illumination during daylight hours was even but not bright, either with natural or indoor lighting. At night, only dimmed central overhead lights were on, allowing relative darkness at infant stations against the walls. When nursing interventions required illumination, only the indirect lighting above the infant’s bed was used.
Noise in each nursery was rated during two 24hour periods. An observer sat by the side of an infant’s bassinette for a 15-min period every hour making note of each occurrence of various categories of “noise” that were potentially disturbing to the infant. The categories were equipment alarms, mechanical noises produced by activity such as housekeeping, conversa- tions subjectively judged to be loud in the context of background noise, overhead speaker, telephone, infant crying, and other noise. Mean oc- currence of equipment alarms per 15-min period (averaged over all 48 hours) for the alternative nursery was 2.76, in contrast to 6.29 for the normal (control) intermediate nursery (Nursery #2). Mean occurrences of overhead speaker and telephone were also lower in the alternative nursery (0.00 vs. 0.63 and 0.12 vs. 0.39, respectively). Mean occurrences of subjectively salient conversations, mechanical noises, crying, and other noises were found to be greater in the alternative unit than in Nursery #2 (4.33 Vs. 2.65, 4.05 VS. 2.17, 0.95 vs. 0.76, and 0.49 vs. 0.24, re- spectively), although this reflected primarily the lower level of background noise in the alternative nursery.
Nursery Environment #2: Control Nurse+ Subjects in this group re- mained in the main intermediate care section of the special care nursery until their discharge home. The design of this unit was typical of many present-day intermediate care nurseries. It was a large 15.85 m X 3.66 m) open-floor medical unit with a 20-bed capacity; a large open door connected to an adjacent IO-bed intensive care unit. It was not a nursing priority in this nursery to care for infants on a state-contingent basis.

292 FAJARDO, BROWNING, FISHER, AND PATON
The control nursery was frequently busy and noisy. Lighting was bright throughout the day and night. Measurement of illumination over two 24- hour periods showed an average level of 100 footcandles with no difference between day and night. Light was provided only by overhead fluorescent lights controlled in three sections around the room. One wall (15.85m) had continuous windows to the outside with adjustable blinds. The only modulation of light level for this nursery was during the daylight hours when indoor lights could be turned off and natural light from the outside could be modulated by blinds. However, these adjustments were used inconsistently, and typically all indoor lights were on during daylight hours. During the nighttime hours, all overhead lights were used.
Methods and Definition of State Infant sleep and waking states have been measured by an array of pro- cedures. These methods fall into two categories: (a) polygraphic recordings of physiological variables (e.g., Anders, 1974; Parmelee et al., 1967); and (b) a trained observer’s assessment of prevailing state (e.g., Brazelton, 1984; Thoman, 1975). These two types of methods have somewhat different purposes and distinct perspectives on the definition of sleep state. Phys- iological methods assign a state based on the integration and coordination of biophysiological systems within the child, as reflected in Prechtl’s concept of “concordance” of state-relevant parameters. The second type of method requires a trained observer to categorize an infant’s prevailing state based on specific behaviors and the contextual flow of events before and after the particular time unit being assessed. Thoman (1990) has noted that individual states represent regularly occurring behavior patterns and are readily recognized in any infant, although these behavior patterns are not stereotypical and are expressed differently in individual infants and across time within any particular infant. From the observational perspective, “state” is considered as an organization of behaviors con- veying important information to the observer and is meaningful within a &z& system, such as between mother and infant (Sander, 1987; Sander, Stechler, Bums, & Lee, 1979). This is different from the perspective on state that underlies the physiological methods, which focus on behavioral and physiological patterns within the infant as a monadic system.
In this study, the second type of method was used. The observer recorded behavioral events and prevailing state every 30 s. Even when state categorization was ambiguous, the observer assigned the prevailing state that best fit from among the four categories described below. We chose this approach on the view that state is a communicative, cue- sending pattern within a dyadic system which is interpreted meaningfully even when ambiguous. This approach to the assignment of state allowed for expected differences in clarity between younger and older infants; for

NURSERY EFFECTS ON STATE REGULATION 293
example, older infants display more normative behavior patterns than younger infants.
State Observations Subjects were first observed at 32 weeks PCA before assignment to one of the nurseries, and then again at 36 weeks PCA before discharge from the hospital. During the midday or last morning feeding-to-feeding interval, a trained observer sat by the infant’s bed recording observations. The observation began immediately after the nurse completed all feeding and other manipulations with the infant and placed the infant prone in bed, the observation was terminated when nursing interventions began again. The younger infants on a 3-hour feeding schedule were typically observed for 2.5 hours, whereas the older infants were observed for 3.5 hours if they had progressed to a Chour feeding schedule. The same two observers collected all the data, each observing for 1 hour before being relieved by the other. Observations were made for each 30-s period, which was signalled for the observer by a tone in earphones. Two types of observations were recorded for each 30-s period: the presence of state-related behaviors, and a judgment of prevailing state. A 1-min break was taken after each 10 min of observation.
Obsentation of Sfule-Re&ed Behaviors. Five state-related behaviors were observed. The observer held a clipboard with coding sheets and watched for the presence of each behavior within the 30-s period. When a behavior was seen, it was coded as present for that 30-s period. There was no further recording of its recurrence or duration during that 30-s period With some practice, the observer could record observations while continuing to watch the infant. Five behaviors were coded: (a) eyes open, defined as one or both eyes partially or fully open; (b) eye movement, which was apparent as movement of the eyes under closed or open eyelids; (c) body movement, including smooth, nonreflexive movements such as stretching of the whole body or simple nontremor movements of the face, arms or legs; (d) tremors and startles, including any sign of twitching, jerking, fluttering, and so on; and (e) sucking behavior, defined as two or more mouth movements of sucking. We did not encourage the subject to suck on anything (pacifier or intravenous board) during observations; instances of such sucking rarely occurred, and if they did, we excluded this time from analysis. We included as sucking behavior only distinctive rhythmical bursts of spontaneous sucking.
Respiration was recorded via a medi-trace machine attached to a Hewlett Packard monitor displaying ECG and respiration from one set of three electrodes placed on the chest of the infant. Many of these records were not easily interpretable because of continuous body movement (es- pecially in the 32-week infants) and frequent technical difficulties (e.g.,

294 FAJARDO, BROWNING, FISHER, AND PATON
electrode placement), so respiration was not included as a criterion of state.
Judgment of Prevailing State. As the observer watched for and recorded the presence of state-related behaviors, she also made an assessment of state. A judgment of the prevailing state during each 30-s period was made at the end of each period. Prevailing state was specified as one of four categories: quiet sleep (QS), active sleep (AS), drowse, and awake. These states were defined according to specific criteria. In QS, eyes are closed. Body movement and startling may be present but with maturation occur less and are sometimes rhythmic. In older infants, rhythmic sucking may occur. There are no rapid eye movements (REMs), unless isolated instances observed in the midst of an ongoing non-REM state. In AS, patterned or unpatterned REM often occurs, increasing with maturation. Some infants exhibit substantial body movement during AS, during both REM and non-REM periods, but startling in this state diminishes with maturation and increasing organization. Eyes are usually closed. The drowse state is distinguished by intermittent eye opening and variable body movement and may be accompanied by grunts and other noises. Drowse is sometimes difficult to distinguish from open-eyed REM AS in the youngest infants. The awake state, sometimes not clearly differentiated from drowse, is marked by continuous eye opening, with some visual scanning or fixation. The drowse and awake states occurred infrequently (see Table 2).
The two observers (B.F. and M.B.) were trained prior to data collection. Training consisted of many hours of observing infants simultaneously, discussing and refining the defining criteria for each state and each behavior to be coded. These criteria were informed by definitions in the literature, particularly the work of Thoman, Parmelee, and their colleagues (e.g., Parmelee et al., 1967; Thoman, 1975). Periodically the observers would independently and simultaneously score the same infant, until criteria and descriptions for each state and behavior resulted in an acceptable level of interrater reliability.
Interrater reliability for behaviors and state judgments was tested four times during data collection, twice with infants at 32 weeks PCA and twice with infants at 36 weeks PCA. Both observers simultaneously and independently rated the infants for 1 hour. For eyes open, eye movements, and sucking, percent agreement at both ages ranged from 89 to 100, with Cohen’s kappa (Cohen, 1960) ranging from .77 to 1.00. Reliability for body movement and startling was somewhat lower, with 84% agreement for body movement at 32 weeks (K = .42) and 86% agreement at 36 weeks (K = .68). Because there was only 66% agreement at 32 weeks for startling (with 77% at 36 weeks and K = .34 at both ages), this variable was dropped from our analyses. For state at 32 weeks, percent agreement
NURSERY EFFECTS ON STATE REGULATION 295
was 85 and K was .75; at 36 weeks, percent agreement was 89 and K was .83.
Measures Four different types of measures were created from our observational records:
1. Based on prevailing state judgments for each 30-s period, we assessed the relative amount of time spent in each of the four states by calculating percent time that each state occurred. Similarly, we calculated for each state-related behavior the percent of 30-s periods during which the behavior occurred.
2. The capacity to sustain a continuous state organization over time was assessed by calculating the mean duration of each state (QS, AS, drowse, awake). This was calculated based on the number of consecutive 30- s periods in which the same prevailing state was observed. The con- tinuous duration of a prevailing state ranged from 0.5 min (30-s) to 48.5 min. The interruptions created by the observer’s l-mm break every 10 min were ignored when the assignment of state was the same before and after the break (i.e., the state was assumed to be continuous and part of the same episode of a single prevailing state).
The continuity of occurrence for each of the state-related behaviors was similarly assessed by computing the mean number of consecutive 30-s periods over which the behavior occurred. The maximum number of consecutive 30-s periods during which a behavior might repeatedly occur was 20 (10 min), limited by the number of 30-s observation periods between observer rest breaks.
3. Based on the judgments of prevailing state, the number of state changes per hour of observation was computed as another measure of the capacity to maintain a continuous state.
4. Another estimate of capacity to maintain state over time was achieved by categorizing the length of a prevailing state. We defined an enduring episode as one lasting 10 min or more; a brief episode as one at least 6 but less than 10 min; and a fleeting episode as one less than 6 min. The rationale for choosing these post-hoc length categories was based on our data. Most 32-week and all 36-week infants maintained the same prevailing state for 10 min at least once during an observation. At the other extreme, prevailing states lasting less than 6 min tended to be embedded in an ongoing lack of discernible organization, with continuing shifts in state. Falling between these two extremes were episodes of prevailing state lasting between 6 and 10 min. Percent time spent in each of these categories (enduring, brief, and fleeting) and the mean length of enduring episodes were computed.

296 FAJARDO, BROWNING, FISHER, AND PATON
RESULTS AND DISCUSSION
‘The means (and standard errors) by Nursery Group and Age for all of our measures are given in Tables 2 through 6, along with tests of sig- nificance from a two-way repeated measures analysis of variance.
Developmental changes were expected for subjects from both groups (main effect of Age). The central question addressed by this study, that nursery environment affects state organization, implies an interaction effect between Age and Nursery Group. This would indicate that the amount of change in the dependent variables from 32 to 36 weeks PCA is different for the two nursery environments.
We found several expected age-related changes from 32 to 36 weeks for both nursery groups combined. The only change in percent time spent in the four states was an increase in drowse, F( 1,22) = 5.32, p -c .05; percent time in AS did not decrease significantly as expected, F( 1,22) = 3.78, p < .lO, nor did percent time spent in QS increase, F(1,22) = 0.59, n.s. (see Table 2). For both nursery groups combined, states became more enduring over the Cweek period (see Tables 3-5): Mean duration of QS and drowse increased over time, F( 1,22) = 5.04, p < .05, and F( 1,22) = 4.91, p < .05, respectively; number of state changes per hour decreased F( 1,22) = 6.07, p < .05; percent time spent in enduring states of 10 min or more increased, fl1,22) = 4.57, p < .05 and concomitantly percent time in fleeting states (less than 6 min) decreased, F(1,22) = 8.37, p -c .Ol.
Age changes in observed behaviors included an increase in occurrence of eye movements, F(1,22) = 7.26, p < .05, as well as an increase in the mean number of consecutive 30-s periods over which eye movements repeatedly occurred, F(1,22) = 9.68, p < .Ol (see Tables 2 and 3). These results confirm findings by other investigators (Parmelee & Stem, 1972).
Our main question was whether there would be greater developmental changes in state organization for infants in the alternative nursery com- pared to those in the control nursery. This hypothesis was supported by a number of significant interaction effects. The mean duration of AS increased over time for alternative nursery subjects but decreased for control nursery subjects F( 1,22) = 6.16, p < .05 (see Figure 1). (There was also a trend in the interaction effect for mean duration of QS, with alternative nursery subjects displaying a greater increase over time than control subjects (4 1,22) = 4.07, p < .lO).
Number of state changes per hour decreased for infants from the alternative nursery but slightly increased for control nursery subjects, F(1,22) = 6.47, p < .05 (see Figure 2). Percent time in enduring states (10 min or greater) increased more for alternative than control nursery subjects, F(1,22) = 4.47, p < .05 (see Figure 3), as did the mean duration of enduring states, F(1,22) = 5.53, p < .05. These results (see Tables

Stat
es
32
Wee
ks
PCA
TABL
E 2
Mea
n Pe
rcen
tage
of
Ob
serv
ation
Ti
me
fond
St
anda
rd
Erro
rs)
36
Wee
ks
PCA
Beho
viors
32
W
eeks
PC
A 36
W
eeks
PC
A
Quie
t Sl
eep
Eyes
Op
enb
Alte
rnat
ive
37.2
2 (2
.41
I 38
.80
12.5
81
Alte
rnat
ive
19.0
9 (3
.90)
18
.87
12.7
61
Cont
rol
35.6
6 13
.5 I
) 37
.91
I I .9
4)
Cont
rol
9.28
I I
531
9.
93
Il.74
1
Activ
e Sl
eep
Eye
Mov
emen
ts’
Alte
rnat
ive
55.2
4 (3
.45)
50
.23
(3.9
41
Alte
rnat
ive
35.6
3 I 1
.51
I 42
.53
ll.9O
l
Cont
rol
61.0
9 (3
.28)
55
.27
I I ,5
91
Cont
rol
37.4
4 (2
.82)
40
.1
I Il.
181
Drow
se”
Body
M
ovem
ent
Alte
rnat
ive
5.05
II.
511
9.22
12
.361
Al
tern
ative
45
.26
12.7
81
41.2
6 (3
.371
Co
ntro
l 2.
62
10.8
81
6.62
(2
.07)
Co
ntro
l 40
.32
13.5
61
39.9
3 12
.5
I )
Awak
e Su
ckin
g
Alte
rnat
ive
2.46
(1
.13)
1.
76
10.8
11
Alte
rnat
ive
4.15
Il.
221
6.26
I
,701
I
Cont
rol
0.63
(0
.331
0.
20
(0.1
21
Cont
rol
5.90
(1
.551
7.
56
I ,4
81
I
0 Fo
r Ag
e,
R1.2
2)
= 5.
32,
p <
.05.
b
For
Trea
tmen
t, F(
1.22
) =
7.92
, p
< .0
5.
c Fo
r Ag
e,
R1.2
21
= 7.
26,
p <
.05.

TABL
E 3
Mea
n Du
rotio
ns
in
Min
utes
(a
nd
Ston
dord
Er
rors
1
Stat
es
32
Wee
ks
PCA
36
Wee
ks
PCA
Beho
viors
32
W
eeks
PC
A 36
W
eeks
PC
A
Quie
t Sl
eep”
Ey
es
Open
Al
tern
otive
3.
93
10.8
71
8.18
(1
.711
Al
tern
otive
1.
07
IO.0
81
1.27
IO
.1
11
Cont
rol
4.59
(I.
231
4.82
(0
.541
Co
ntro
l 0.
93
10.0
91
I .02
IO
. 1
1 I
Activ
e Sl
eepb
Ey
e M
ovem
ents”
Al
tern
ative
4.
43
(0.8
1 I
6.
88
(0.8
1 I
Alte
rnat
ive
1.34
(0
.061
1.
70
(0.1
11
Cont
rol
6.37
10
.941
5.
25
10.5
51
Cont
rol
1.3
1 (0
.071
1.
39
(0.0
41
Drow
se’
Body
M
ovem
ent
Alte
rnat
ive
0.02
IO
.0
1)
0.05
IO
.01
I Al
tern
otive
1.
22
(0.0
71
1.23
lO
.08l
Cont
rol
0.01
10
.00)
0.
03
10.0
1 I
Cont
rol
I. 18
10
.13l
1.
09
10.0
61
Awak
ed
Suck
ing
Alte
rnot
ive
0.01
io
.011
0.
0 1
(0.0
01
Alte
rnat
ive
1.02
10
.21
I 1.
04
(0.2
01
Cont
rol
0.00
~0
.001
0.
00
io.0
01
Cont
rol
1.20
10
.181
1.
17
10.1
91
a Fo
r Ag
e,
fll,2
21
= 5.
04,
p <
.05.
b
For
Inte
ract
ion,
RI
,2
21
= 6.
16,
p <
.05.
(
For
Age,
HI
.221
=
4.91
, p
< .0
5.
d Fo
r Tr
eotm
ent,
H 1,
221
= 5.
43,
p <
.05.
‘F
or
Age,
RI
,221
=
9.68
, p
< .O
l; fo
r Tr
eatm
ent,
RI.2
21
= 5.
04,
p <
.05.

NURSERY EFFECTS ON STATE REGULATION 299
TABLE 4
Mean Number of Stote Chonges Per Hour land Stondord ErrorlO
32 Weeks PCA 36 Weeks PCA
Alternative 19.8 1 (2.42) 11.13 11.391
Control 14.99 (2.09) 15.13 11.681
D For Age, ffl,221 = 6.07, p < .05; for interaction, Fll.221 = 6.47, p < .05.
TABLE 5
Meon Percentage of Time in Enduring, Brief, and Fleeting States fond Stondord Errors)
32 Weeks PCA 36 Weeks PCA
Enduring0 Ahernotive 45.92 (6.421 69.00 13.47) Control 61.33 (5.841 61.50 (4.311
Brief Alternative 12.75 (2.361 9.50 (I.841 Control 6.83 i I .461 11.08 (2.14)
Fleetingb Afternotive 4 I .25 (5.761 2 I .50 (2.851 Control 3 1.92 (5.02) 27.42 13.3 1)
~For Age, F11.22) = 4.57, p < .05; for interaction, R1.22) = 4.47, p < .05. b For Age, H1.22) = 8.37, p < .Ol
TABLE 6 Meon Durotion of Endurino Stotes in Minutes iond Standord ErrorI’
Alternotive
Control
32 Weeks PCA 36 Weeks PCA
16.77 (I.281 24.30 (1.68)
20.93 12.51 I 19.93 (1.71)
a For interaction, Al ,221 = 5.53, p C .05.
4-6) are important because steady state maintenance facilitates accom- plishment of learning, and it has been demonstrated that learning is already taking place at this young preterm age (DeCasper & Fifer, 1980; DeCkper & Spence, 1986).
For state-related behaviors, there were no significant interaction effects found, although there was a trend in the mean number of consecutive 30-s periods over which eye movements occurred, with subjects in the alternative nursery showing a greater increase over time, F( 1,22) = 4.08, p < . 10 (see Table 3). Clustered eye movements have recognized im- portance in the development of AS and other CNS-related functions (Rotbvarg, Muzio, & Clement, 1966).
There were two unexpected significant main effects of Nursery Treat- ment Group which indicate differences between groups at both the onset

300 FAJARDO, BROWNING, FISHER, AND PATON
Minutea Mlnuter 10
8
6
4
2
10
8
II 0 4
2
32 36 =I 32 38
Altornatlve Control Figure 1. Mean duration of active sleep (for interaction, fl1.22) = 6.16, ,o < ,051.
Number
20
10
32 30 32
Number
20
1 10
Alternatlve
I 36
Control Figure 2. Meon number of stote changes per hour (for Age, RI,221 = 6.07, p < .05; for interaction, FI 1,221 = 6.47, p < ,051.
(32 weeks PCA) and conclusion of the Cweek intervention contrast period. Alternative nursery subjects at both ages exhibited a longer mean duration of awake state, F(1,22) = 5.43, p < .05, than control subjects (there was also a trend in the amount of time spent awake, with alternative nursery subjects displaying more, 41,22) = 4.03, p < .lO). Subjects from the alternative nursery also displayed more eyes open, F( 1,22) = 7.92, p < .05 (and there was a trend in the mean number of consecutive 30-s periods over which this behavior occurred, F(1,22) = 3.97, p < .lO). It is not clear how to interpret these differences. Most studies of emerging state organization in premature infants focus on the development of AS and QS. Little is known about drowse and awake states in infants this young, nor about the significance of eyes being open. In the preterm, eye opening

NURSERY EFFECTS ON STATE REGULATION 301
cl Endurlng
Percent Percent
32 36 32 36 AltarnatIve Control
Figure 3. Meon percentage of time in enduring, brief, ond fleeting states (enduring: for Age,
RI ,22)= 4.57, p < .05, and for interaction, R1,221= 4.47, p < .05; fleeting: for Age,
RI.221 = 8.37, p < ,011.
can occur not only during drowse and awake, but also during AS, par- ticularly in REM phases of AS and even during QS. The increased occurrence of eye opening among alternative nursery subjects and the corresponding states of drowse and awake for which it is an important criterion are not readily interpretable.
There were no initial clinical differences between nursery groups that could explain this finding, and sleep state for all subjects was initially observed in the same environment (control nursery). In order to check the possibility that this finding was due to initial differences in group sampling reflected in our state and behavior measures, nonorthogonal t tests were done on all 32-week sleep state and behavior measures. Sug- gestion of sampling bias was not found. Even using Fisher’s LSD procedure (Kirk, 1982, p. 115), which does not adequately control for multiple tests and therefore tends to overestimate the number of significant differences, only 2 out of 23 t tests resulted in p values below .lO. Two, of course, is the number expected by chance using random sampling (10% of 23). Furthermore, the two measures were percent time eyes were open (percent of 30-s observation periods when eyes were open at least once) and the percent time of brief states (states between 6 and 10 mm). Neither of these measures is relevant to the results presented above that concern the main hypothesis.

302 FAJARDO, BROWNING, FISHER, AND PATON
CONCLUSIONS
This study shows important effects of nursery environment on spontaneous state organization of prematurely born neonates during the 4 weeks from 32 to 36 weeks PCA. This is the period when organized states are emerging. A nursery environment that maintains diurnal cycles, minimizes intense unpatterned stimuli, and provides state-contingent nursing care promotes steadiness and duration of sleep states in these infants.
Other aspects of state organization were shown not to be affected by nursery environment (e.g., the percent time preterm neonates spend in different states or displaying different behaviors changes with age, regard- less of nursery environment). The suggestion that environment has more impact on AS than QS was not supported by our findings.
Analyzing state observations using measures of percent time is an approach that reflects a biologically-mediated developmental progression but does not index the capacity to sustain states over time. This latter capacity is a crucial aspect of state regulation that improves with age and, as shown here, can be enhanced by varying characteristics of the nursery environment. It is likely that the characteristics of the alternative nursery- patterned regularity and contingency of events-promote entrainment to environment and caretaker. Percent time measures, on the other hand, are sensitive to changes with age that occur regardless of specific envi- ronmental aspects of nurseries.
The infant’s capacity to be organized and display well-regulated states is an important component of optimal caretaker-child interaction, making the child more understandable and satisfyingly responsive to the parent (see Field, 1987). A nursery environment that is non-disruptive and state- contingent can be supportive of the early emergence of this state organi- zation and can be an important “intervention” in the development of the preterm neonate.
REFERENCES
Als. H., Lawhon, G., Brown, E., Gibes, R., DUG, F.H., McAnulty. G., & Blickman, J.G. (1986). Individualized behavioral and environmental care for the very low birth weight preterm infant at high risk for bronchopulmonary dysplasia: Neonatal intensive care unit and developmental outcome. Pedialrics. 78, I 123-I 132.
Anders, T.F. (1974). The infant sleep profile. Neuropediarrics. 5. 425-442. Anders, T.F., Keener, M.A., & Kraemer, H. (1985). Sleep-wake state organization, neonatal
assessment and development in premature infants during the first year of life. II. Sleep, 8, 193-206.
Ballard. J.L.. Kazmaier, K., & Driver, M. (1977). A simplified assessment of gestational age. Pediatric Research, 11, 374.
Brazelton, T.B. (1984). Neonaral behavioral assessmen scale. Clinics in developmenral tned- icine, 88 (2nd ed.). Philadelphia: J.B. Lippincott.
Cohen, J. (1960). A coefficient of agreement for nominal scales. Educational & Psychological Measuremenl, 20. 37-46.

NURSERY EFFECTS ON STATE REGULATION 303
DeCasper. A.J., & Fifer. W.P. (1980). Of human bonding: Newborns prefer their mothers’ voices. Scicncr. 208. I I74- I 176.
DeCasper. A.J.. & Spence, M.J. (1986). Prenatal maternal speech influences newborns’ perception of speech sounds. ItIfunt Behhatdor and De~lopmenl. 9. 133-150.
Field, T. (1987). Affective and interactive disturbances in infants. In J.D. Osofsky (Ed.), Handbook qfiqfanr developmen/ (2nd ed.). New York: Wiley.
Kirk. R.E. (I 982). Experirnenral design (2nd ed.). Monterey, CA: Brooks/Cole. Lawson. K.. Daum. C., & Turkewitz. G. (1977). Environmental characteristics of a neonatal
intensive-care unit. Child Development. 48. 1633-1639. Lawson, K.R., Turkewitz. G.. Platt. M., & McCarton, C. (1985). Infant state in relation to
its environmental context. I,!lhnr Behmior and Developmen/. 8. 269-28 I. Parmelee. A.H. (1970). Sleep studies for the neurologic assessment of the newborn. Neu-
ropaediarrie, 1. 35 l-353. Parmelee. A.H., & Stern, E. (1972). Development of states in infants. In C.D. Clemente.
D.P. Purpura. & F.E. Mayer (Eds.). S/eep and (he maturing nervous svstem. New York: Academic.
Parmelee, A.H.. Wenner. W.H.. Akiyama. Y.. Schultz, M., & Stern, E. (1967). Sleep states in premature infants. Developmental Medicine and Child Neurology. 9. 70-77.
Roffwarg, H.P.. Muzio. J.N.. & Dement. W.C. (1966). Ontogenetic development of the human sleep-dream cycle. Science, I-52. 604-6 19.
Sander. L. W. (I 987). Awareness of inner experience: A systems perspective of self-regulatory process in early development. Child Abuse & Neglect. II. 339-346.
Sander, L.W.. Stechler, G.. Burns, P., & Lee, A. (1979). Change in infant and caregiver variables over the first two months of life. In E.B. Thoman (Ed.), Origins q/ rhe iylhnt’s social responsiveness. Hillsdale, NJ: Erlbaum.
Sostek. A.M.. & Anders, T.F. (1981). The biosocial importance and environmental sensitivity of infant sleep-wake behaviors. In K. Bloom (Ed.), Prospective issues in ir?fancy resmrch. Hillsdale. NJ: Erlbaum.
Thoman, E.B., ( 1975). Sleep and wake behaviors in neonates: Consistencies and consequences. Merrill-Palmer Quarterlv. 21, 295-3 14.
Thoman, E.B. (1990). Sleeping and waking states in infants: A functional perspective. Neuroscience and Biobehavioral Reviews. 14. 93- 107.
Thoman, E.B., Davis, D.H., Raye, J.R.. Philipps, A.F.. Rowe, J.C., & Denenberg, V.H.
(I 985). Theophylline affects sleep-wake state development in premature infants. Neu- ropediarrics. 16. I3- 18.
24 March 1989; Revised 18 December 1989 n