effect of hydralazine on renal - semantic scholarhydralazine administration in patients with chf,and...
TRANSCRIPT

RENAL RESPONSE TO HYDRALAZINE IN CHF/Pierpont et al.
vasodilator drugs on transcapillary fluid exchange in the renalcortex. Am J Physiol 230: 1148, 1976
29. Krakoff LR, Guia DD, Vlachakis N, Stricker J, Goldstein M:Effect of sodium balance on arterial blood pressure and renalresponses to prostaglandin A, in man. Cire Res 33: 539, 1973
30. Merrill AJ: Mechanisms of salt and water retention in heartfailure. Am J Med 6: 357, 1949
31. Earley LE, Schrier RW: Intrarenal control of sodium excretionby hemodynamic and physical factors. In Handbook ofPhysiology. Section 8: Renal Physiology, edited by Orloff T,Berlinger RW. Washington, DC, American Physiological
Society, 1973, pp 721-76232. LeJemtel T, Hellman C, Elkayam U, Strom J, Blaufox MD,
Frishman W, Ribner H, Sonnenblick E: Hemodynamic andrenal response to oral hydralazine therapy in severe heartfailure. Circulation 56 (suppl III): 111-9, 1977
33. Birch AA, Boyce WH: Changing renal blood flow followingsodium nitroprusside in patients undergoing nephrolithotomy.Anesth Analg 56: 102, 1977
34. Pagani M, Vatner SF, Braunwald E: Hemodynamic effects ofintravenous sodium nitroprusside in the conscious dog. Circula-tion 57: 144, 1978
Effect of Hydralazine on Renal Failurein Patients with Congestive Heart Failure
GORDON L. PIERPONT, M.D., PH.D., DAVID C. BROWN, M.D., JOSEPH A. FRANCIOSA, M.D.,AND JAY N. COHN, M.D.
SUMMARY Hydralazine is known to improve cardiac function in patients with congestive heart failure(CHF), but its effects on renal function in CHF are less clear. Sodium retention is known to occur with long-term use of hydralazine to treat hypertension; if this occurs in patients with CHF it could be deleterious.Therefore, in a metabolic unit we studied renal effects of hydralazine in patients with stable class III or IVCHF. In a single-blind study, the patients were given placebo twice daily for 3 days (period P-1), 100 mg oforal hydralazine twice daily for 3 days (period P-H), and placebo for 3 more days (period P-2). The average24-hour creatinine clearance was 69.7 ± 7.7 ml/min (mean i SEM) in P-1, increased to 76.3 i 9.0 ml/minwith hydralazine (p < 0.01) and fell again when hydralazine was stopped (P-2) to 68.5 i 7.8 ml/min(p < 0.02). Though the slight improvement in sodium excretion was not statistically significant (60.2 ± 12.1mEq in P-1, 64.5 ± 12.4 mEq in P-H, 52.3 ± 7.7 mEq in P-2), serum osmolality decreased from 288 ± 1.8mosM in P-1 to 283 ± 1.9 mosM in P-H (p < 0.02) and rose to 286 ± 1.9 mosM in P-2 (NS). During thethree periods, serum sodium, chloride, potassium, carbon dioxide, blood urea nitrogen, creatinine and glucosewere unchanged, as were weight and urine volume. Systolic blood pressure was 109.6 ± 3.6 mm Hg in P-1,110.1 ± 3.9 mm Hg in P-H (NS), and 114.2 ± 5.0 mm Hg in P-2 (p < 0.05). Diastolic blood pressure, heartrate and respirations were unchanged. Thus, we found no evidence of sodium or water retention duringhydralazine administration in patients with CHF, and renal function was actually improved, as evidenced bythe increased creatinine clearance.
HYDRALAZINE improves left ventricular perfor-mance in patients with congestive heart failure (CHF)'and may be effective for long-term oral therapy ofpatients with chronic CHF.1 2 However, hydralazinecan lead to sodium and fluid retention when used totreat hypertension,3-5 and sodium retention has beenreported during administration of hydralazine in apatient with CHF.6 Such a response to hydralazine inpatients with CHF might limit the value of this drugfor long-term therapy or necessitate larger doses ofdiuretics. The present study assesses the effects ofhydralazine on renal function and sodium balance inpatients with CHF.
From the Department of Medicine, Cardiovascular and RenalSections, University of Minnesota Hospitals, and Veterans Ad-ministration Medical Center, Minneapolis, Minnesota.
Address for correspondence: Gordon L. Pierpont, M.D.,Veterans Administration Medical Center, Cardiovascular Section,Minneapolis, Minnesota 55417.
Received March 9, 1979; revision accepted August 20, 1979.Circulation 61, No. 2, 1980.
Methods
Nine male patients with New York Heart Associa-tion functional class III or IV heart failure (three classIV and six class III) who were on conventionaltherapy were studied. The patients were ages 47-64years (average 59 years). Three of the patients hadprimary myocardial disease and six had ischemicheart disease. Exclusion criteria included: insulin-dependent diabetes mellitus, severe pulmonary disease(Po2 < 50 mm Hg or Pco2 > 50 mm Hg), renal in-sufficiency (BUN > 40 mg/dl or creatinine > 2.0mg/dl), abnormal serum electrolytes, angina requir-ing nitrate therapy, myocardial infarction within thepast 3 months, significant primary heart valve disease,hypertension requiring nondiuretic antihypertensiveagents or heart failure due to restrictive heart disease.
After giving written informed consent, the patientswere admitted to a special diagnostic and treatmentunit (SDTU) of the Minneapolis Veterans Ad-ministration Medical Center for evaluation. Allpatients were clinically stable with a steady bodyweight when admitted to the SDTU. All patients were
323
by guest on Novem
ber 5, 2017http://circ.ahajournals.org/
Dow
nloaded from
VOL 61, No 2, FEBRUARY 1980
receiving a constant dose of diuretics, and eight of ninewere taking digitalis at the time of admission. Thesemedications, as well as any other medication thepatient was taking regularly, were continued at a con-stant dose throughout the study period. One patienthad been receiving isosorbide dinitrate, which wasstopped more than 24 hours before entry into thestudy.On admission to the SDTU a dietary history was
taken by a nutritionist and a diet constructed to matchthe usual sodium intake for each patient. Sodium andfluid intake were kept constant for the duration of thestudy and patients were allowed their normal level ofactivity. Supine blood pressure, heart rate, respira-tions and temperature were monitored four timesdaily, and the patients were weighed twice daily.The study protocol consisted of three periods of 3
days each. The first period consisted of 3 days ofplacebo administration (two tablets twice daily). Thiswas followed by 3 days of active hydralazine therapy,100 mg (two tablets twice daily) and another 3-dayplacebo period. The investigators, but not the patients,knew when hydralazine was being given. Each morn-
ing blood was drawn for determination of serum urea
nitrogen, creatinine, glucose, sodium, chloride, totalCO2, potassium and osmolality. In the last fivepatients studied, blood samples for plasma renin ac-
tivity (PRA) were drawn on the third day of eachperiod in the early morning with the patient supine.Urine was collected at 8-hour intervals throughout thestudy and analyzed for creatinine, potassium, sodiumand osmolality. Creatinine clearances were calculatedfor each of the three daily 8-hour urine collectionsusing the serum creatinine value obtained at the end ofthe day.
All data were analyzed using the paired t test anddifferences were considered statistically significant forp values less than 0.05. The mean of all values ob-tained during each 3-day period were compared, andanalysis of the data was repeated by averaging thevalues from the two placebo periods and comparingthem with the values from the hydralazine period.Combining the placebo periods would tend to correctfor trends during the course of hospitalization thatmight occur independent of hydralazine therapy. Inorder to examine the data for possible changes withineach drug period, an additional analysis of the morepertinent variables was performed using an analysis ofvariance.
Results
Table 1 shows the mean values during each periodfor mean arterial pressure (calculated as the diastolicpressure plus one-third of the pulse pressure), heartrate, body weight, serum creatinine, serum sodium,serum chloride, serum potassium and urine volume.None of these parameters changes significantly duringhydralazine therapy when compared with eachplacebo period or with the average of the two placeboperiods.
In addition to the data presented in table 1, there
TABLE 1. Clinical Data from the Three Study Periods
Study periodP1 H P2
BP(mm Hg) 85 2.1 84 -2.0 87 3.4HR (beats/min) 83 - 3.0 84 - 3.3 84 2.7Weight (lbs) 178 9.8 179- 9.8 177 10.1
Creat (mg/ml) 1.4 0.15 1.4- 0.18 1.4 0.16BUN (mg/dl) 25 - 3.9 24 - 4.7 25 4.0Na+ (mEq/l) 141 - 1.0 139 :1.5 140 1.6Cl- (mEq/l) 100 1.4 99 1.9 99 1.9
K+ (mEq/l) 4.3 0.1 4.3 0.1 4.2 +0.1Urine vol (1/24 hr) 2.1 0.26 2.2 0.27 2.1 i0.27
Values are average - SEM. None of the changes werestatistically significant when compared from one period toanother.
Abbreviations: BP = mean blood pressure; HR = heartrate; Creat = creatinine; BUN = blood urea nitrogen;Na+ = serum sodium; Cl- = serum chloride; K+ = serumpotassium; P1 = first placebo period; P2 = second placeboperiod; H = hydralazine.
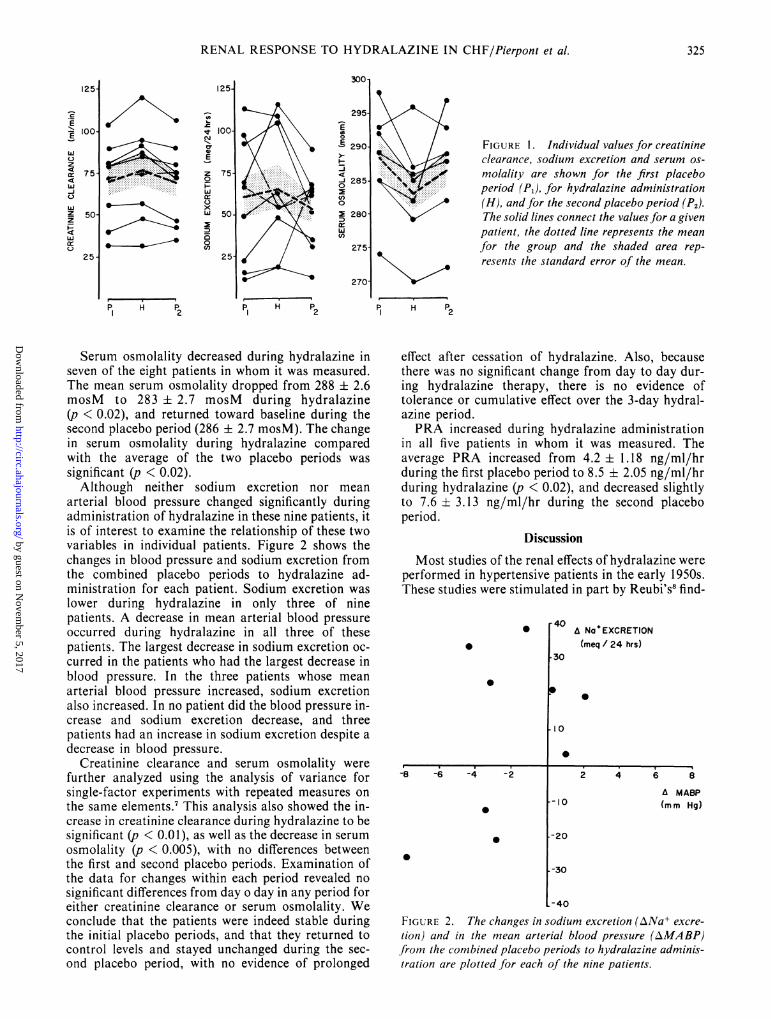
were no significant changes in respiratory rate, serumglucose, serum total CO2, creatinine excretion, sodiumbalance or combined sodium plus potassium excre-tion. Potassium excretion did not change from the firstplacebo period (102 ± 10.5 mEq/24 hours) to thedrug period (103 ± 11.8 mEq/24 hours), but thedecrease to 98 ± 11.1 mEq/24 hours in the secondplacebo period was statistically significant (p < 0.05)when compared with the active drug period. Becauseof this decrease during the second placebo period,potassium excretion was statistically higher (p < 0.05)during hydralazine therapy compared with theaverage of the two placebo periods.The effect of hydralazine on creatinine clearance,
sodium excretion and serum osmolality are shown infigure 1. The average of all values during each periodis shown for every patient, as well as the mean + SEMfor the whole group. Creatinine clearance increasedfrom an average of 69.7 i 7.7 ml/min during thefirst placebo period to 76.3 ± 9.0 ml/min duringhydralazine therapy (p < 0.01). In no patient didcreatinine clearance fall during administration ofhydralazine. The creatinine clearance fell again duringthe second placebo period to 68.5 ± 7.8 ml/min,which was significantly lower than during hydralazine(p < 0.02). This value was not significantly differentfrom the first placebo period. When compared withthe average of the two placebo periods, the increase increatinine clearance during hydralazine was signifi-cant (p < 0.01).Sodium excretion increased from 60.2 ± 12.1 mEq/
24 hours during placebo to 64.5 ± 12.4 mEq/24hours during hydralazine and decreased again to 52.3± 7.7 mEq/24 hours after hydralazine was stopped.These changes were not statistically significant whenthe hydralazine response was compared with eachplacebo period separately or with the pooled placeboperiods.
CIRCULATION324
by guest on Novem
ber 5, 2017http://circ.ahajournals.org/
Dow
nloaded from
RENAL RESPONSE TO HYDRALAZINE IN CHF/Pierpont et al.
1251
t 1001NI
CJ
E
z 750
W 50-
0
C,)125-
P1 H P2
295
E
E 290
1 285
c)
2 280
(n
275
270-
p1 H P2
FIGURE 1. Individual values for creatinineclearance, sodium excretion and serum os-molality are shown for the first placeboperiod (PJ, for hydralazine administration(H), and for the second placebo period (P2).The solid lines connect the values for a givenpatient, the dotted line represents the mean
for the group and the shaded area rep-
resents the standard error of the mean.
P H P1 ~~~2
Serum osmolality decreased during hydralazine inseven of the eight patients in whom it was measured.The mean serum osmolality dropped from 288 ± 2.6mosM to 283 2.7 mosM during hydralazine(p < 0.02), and returned toward baseline during thesecond placebo period (286 + 2.7 mosM). The changein serum osmolality during hydralazine comparedwith the average of the two placebo periods was
significant (p < 0.02).Although neither sodium excretion nor mean
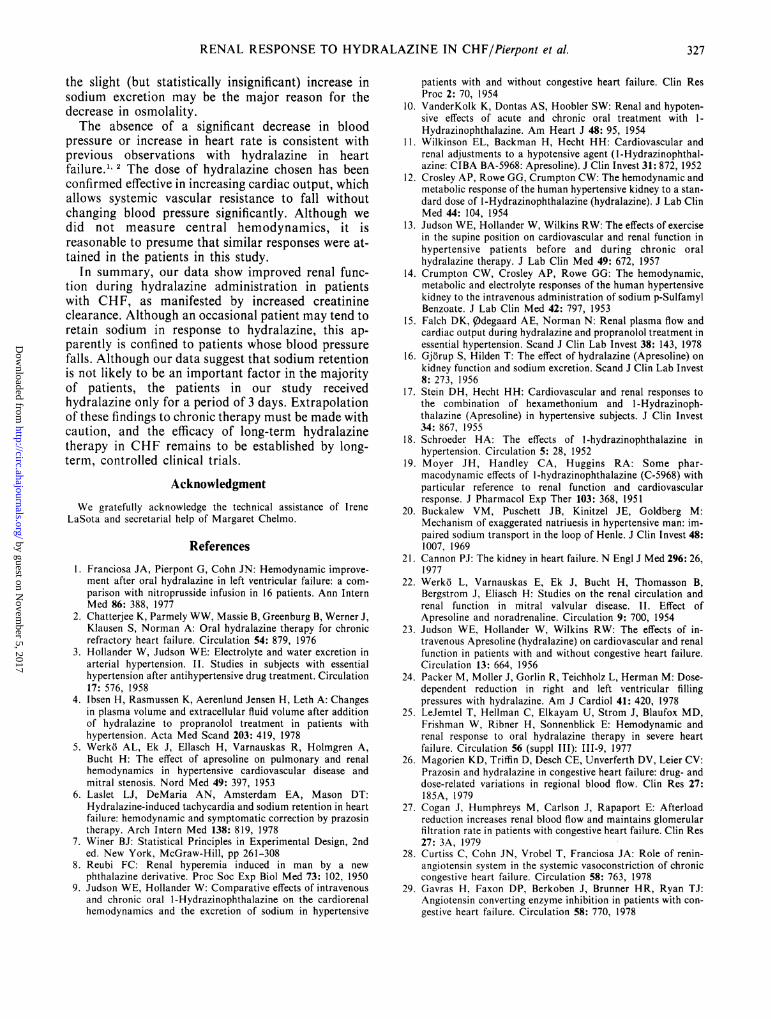
arterial blood pressure changed significantly duringadministration of hydralazine in these nine patients, itis of interest to examine the relationship of these twovariables in individual patients. Figure 2 shows thechanges in blood pressure and sodium excretion fromthe combined placebo periods to hydralazine ad-ministration for each patient. Sodium excretion waslower during hydralazine in only three of ninepatients. A decrease in mean arterial blood pressureoccurred during hydralazine in all three of thesepatients. The largest decrease in sodium excretion oc-curred in the patients who had the largest decrease inblood pressure. In the three patients whose meanarterial blood pressure increased, sodium excretionalso increased. In no patient did the blood pressure in-crease and sodium excretion decrease, and threepatients had an increase in sodium excretion despite adecrease in blood pressure.
Creatinine clearance and serum osmolality werefurther analyzed using the analysis of variance forsingle-factor experiments with repeated measures onthe same elements.7 This analysis also showed the in-crease in creatinine clearance during hydralazine to besignificant (p < 0.01), as well as the decrease in serumosmolality (p < 0.005), with no differences betweenthe first and second placebo periods. Examination ofthe data for changes within each period revealed no
significant differences from day o day in any period foreither creatinine clearance or serum osmolality. Weconclude that the patients were indeed stable duringthe initial placebo periods, and that they returned tocontrol levels and stayed unchanged during the sec-
ond placebo period, with no evidence of prolonged
effect after cessation of hydralazine. Also, becausethere was no significant change from day to day dur-ing hydralazine therapy, there is no evidence oftolerance or cumulative effect over the 3-day hydral-azine period.PRA increased during hydralazine administration
in all five patients in whom it was measured. Theaverage PRA increased from 4.2 1.18 ng/ml/hrduring the first placebo period to 8.5 2.05 ng/ml/hrduring hydralazine (p < 0.02), and decreased slightlyto 7.6 ± 3.13 ng/ml/hr during the second placeboperiod.
Discussion
Most studies of the renal effects of hydralazine wereperformed in hypertensive patients in the early 1950s.These studies were stimulated in part by Reubi's8 find-
0
-8 -6 -4 -2
0
0
* A NaoEXCRETION(meq / 24 hrs)
0
0
8
A MABP
(m m Hg)
-30
-40
FIGURE 2. The changes in sodium excretion (ANa+ excre-
tion) and in the mean arterial blood pressure (AMABP)from the combined placebo periods to hydralazine adminis-tration are plotted for each of the nine patients.
125
E' 100t
Wz4
z 75
-J
Z 50-z
4
25-
325
by guest on Novem
ber 5, 2017http://circ.ahajournals.org/
Dow
nloaded from

VOL 61, No 2, FEBRUARY 1980
ing of increased renal plasma flow with no change inglomerular filtration rate when six patients withhypertension and four normal subjects were given 10mg of hydralazine subcutaneously. Similar results inpatients with hypertension were subsequently reportedby other investigators.9"'4
In other studies in hypertensive patients, the renalhemodynamic responses to hydralazine were morevariable.'5-17 Falch et al.15 found no change in effectiverenal plasma flow in 11 patients with hypertension, butthe dose of hydralazine was only 25 mg given orally,twice a day. In six patients with essential hyperten-sion, Gjorup and Hilden'6 observed a variableresponse to intravenous hydralazine. They suggestedthat if the decrease in blood pressure was not marked,renal blood flow increased, whereas it decreased ifblood pressure dropped markedly. Our data suggestthat this might also be true in patients with CHF, assodium retention during hydralazine, if it occurred,appeared to be associated with a fall in blood pressure.Schroeder'8 found no change in urea clearance or ex-cretion of phenyl red in 50 hypertensives treated with50-120 mg of hydralazine for 10-30 days,
Despite the variability of some of these studies, theevidence suggests an increase in renal blood flow withlittle change in glomerular filtration rate as the usualresponse of hypertensive patients given hydralazine. Asimilar response is likely in normal subjects if the dataobtained by Moyer et al.19 in nonhypertensive dogs areapplicable to humans.
Because the pathophysiology of CHF differssignificantly from that of hypertension, we cannotreadily assume that the renal responses to hydralazinewould be the same in the two groups. In hypertension,the renal homeostatic mechanisms are altered towardincreased salt excretion.20 In contrast, in CHF, thekidneys tend to retain salt and water, at least partlybecause of renal vasoconstriction.21 Thus, it might beexpected that a vasodilator could improve salt excre-tion in CHF if renal perfusion is enhanced without adecrease in blood pressure.
Data on renal vascular effects of hydralazine inpatients with heart failure are scarce. Two studies-2' 23have reported on the renal responses of patients withmitral stenosis given hydralazine, but these patientsare not comparable to our study group. Judson et al.23included five patients with "cardiac insufficiency" intheir series, but four of the five were also hypertensive.Our study therefore represents one of the firstattempts to analyze the effects of hydralazinesystematically in nonhypertensive patients with CHFdue to left ventricular dysfunction. In an uncontrolledstudy, Packer et al.24 noted a brisk diuresis in some oftheir refractory heart failure patients placed onmaintenance hydralazine therapy, but no furtheranalysis of renal function is described. Preliminaryreports of improved renal blood flow with hydralazineadministration in heart failure patients have also beenpresented by LeJemtel et al.,25 Mantle et al.26 andCogan et al.27 In the patients of Cogan et al.,27glomerular filtration increased insignificantly.
and were reluctant to water-load class III or IV heartfailure patients, we did not measure para-amino-hippurate or inulin clearance in our patients. None-theless, creatinine clearance increased, consistent witha rise in glomerular filtration rate. Because hydral-azine is known to increase cardiac output in patientswith CHE," 2 it is likely that the improved creatinineclearance was accompanied by an increase in renalblood flow. We can thus infer that in contrast topatients with hypertension, glomerular filtration rateand renal blood flow are increased by hydralazine inpatients with CHF. This response could in part be at-tributed to the fact that renal blood flow andglomerular filtration rate are functionally reduced inCHF, probably because of renal vasoconstriction,which can then be relaxed as the cardiac output in-creases.Although we did not measure PRA in all patients,
PRA did increase during the period of hydralazine ad-ministration in all five patients in whom it wasmeasured. An increase in PRA also occurs whenhydralazine is given to hypertensives, and has beenthought to be related to the decrease in blood pressure.In this subgroup of five patients, renin increased eventhough blood pressure did not fall significantly and thecontrol PRA tended to be elevated. In these fivepatients, no relationship was apparent between thechange in mean blood pressure and change in PRA.Curtis et al.28 and Gavras et al.29 noted a wide range ofvalues for resting PRA in heart failure patients receiv-ing diuretics, with many patients having quite highlevels. They postulated a role of renin in maintainingthe abnormally high peripheral resistance observed inheart failure and noted hemodynamic improvementwith inhibition of the renin-angiotensin system. Theseobservations suggest that activation of the renin-angiotensin system may tend to counteract thevasodilator effect of hydralazine in CHF, and couldalso contribute to sustained renal vasoconstriction.The combination of a converting enzyme inhibitorwith hydralazine might therefore be appropriate forvasodilator therapy in heart failure. The rapidity ofonset of changes in PRA and the duration of effecthave not been studied, and our data are far too few tohelp define the time course of changes in PRA.
In this study, neither weight loss nor diuresis occurredduring the 3-day hydralazine period, despite the effecton creatinine clearance. Our patients were consideredstable and reasonably well compensated before entryinto the study. It is entirely possible that hydralazineadministration to patients with CHF and acutevolume overload would initiate or enhance diuresis.However, because of the instability of patients withvolume overload during hospitalization, the presentstudy was limited to patients who were relatively freeof edema.The decrease in serum osmolality that occurred
with hydralazine is probably related to changes inserum sodium concentration. Increased sodium excre-tion or water retention or both could alter the serumsodium concentration and the osmolality. As we notedno increase in body weight or decrease in urine output,
CIRCULATION326
Because we wanted to keep the study noninvasive
by guest on Novem
ber 5, 2017http://circ.ahajournals.org/
Dow
nloaded from
RENAL RESPONSE TO HYDRALAZINE IN CHF/Pierpont et al.
the slight (but statistically insignificant) increase insodium excretion may be the major reason for thedecrease in osmolality.The absence of a significant decrease in blood
pressure or increase in heart rate is consistent withprevious observations with hydralazine in heartfailure."' 2 The dose of hydralazine chosen has beenconfirmed effective in increasing cardiac output, whichallows systemic vascular resistance to fall withoutchanging blood pressure significantly. Although wedid not measure central hemodynamics, it isreasonable to presume that similar responses were at-tained in the patients in this study.
In summary, our data show improved renal func-tion during hydralazine administration in patientswith CHF, as manifested by increased creatinineclearance. Although an occasional patient may tend toretain sodium in response to hydralazine, this ap-parently is confined to patients whose blood pressurefalls. Although our data suggest that sodium retentionis not likely to be an important factor in the majorityof patients, the patients in our study receivedhydralazine only for a period of 3 days. Extrapolationof these findings to chronic therapy must be made withcaution, and the efficacy of long-term hydralazinetherapy in CHF remains to be established by long-term, controlled clinical trials.
AcknowledgmentWe gratefully acknowledge the technical assistance of Irene
LaSota and secretarial help of Margaret Chelmo.
References1. Franciosa JA, Pierpont G, Cohn JN: Hemodynamic improve-
ment after oral hydralazine in left ventricular failure: a com-parison with nitroprusside infusion in 16 patients. Ann InternMed 86: 388, 1977
2. Chatterjee K, Parmely WW, Massie B, Greenburg B, Werner J,Klausen S, Norman A: Oral hydralazine therapy for chronicrefractory heart failure. Circulation 54: 879, 1976
3. Hollander W, Judson WE: Electrolyte and water excretion inarterial hypertension. II. Studies in subjects with essentialhypertension after antihypertensive drug treatment. Circulation17: 576, 1958
4. Ibsen H, Rasmussen K, Aerenlund Jensen H, Leth A: Changesin plasma volume and extracellular fluid volume after additionof hydralazine to propranolol treatment in patients withhypertension. Acta Med Scand 203: 419, 1978
5. Werk6 AL, Ek J, Ellasch H, Varnauskas R, Holmgren A,Bucht H: The effect of apresoline on pulmonary and renalhemodynamics in hypertensive cardiovascular disease andmitral stenosis. Nord Med 49: 397, 1953
6. Laslet LJ, DeMaria AN, Amsterdam EA, Mason DT:Hydralazine-induced tachycardia and sodium retention in heartfailure: hemodynamic and symptomatic correction by prazosintherapy. Arch Intern Med 138: 819, 1978
7. Winer BJ: Statistical Principles in Experimental Design, 2nded. New York, McGraw-Hill, pp 261-308
8. Reubi FC: Renal hyperemia induced in man by a newphthalazine derivative. Proc Soc Exp Biol Med 73: 102, 1950
9. Judson WE, Hollander W: Comparative effects of intravenousand chronic oral 1-Hydrazinophthalazine on the cardiorenalhemodynamics and the excretion of sodium in hypertensive
patients with and without congestive heart failure. Clin ResProc 2: 70, 1954
10. VanderKolk K, Dontas AS, Hoobler SW: Renal and hypoten-sive effects of acute and chronic oral treatment with 1-Hydrazinophthalazine. Am Heart J 48: 95, 1954
11. Wilkinson EL, Backman H, Hecht HH: Cardiovascular andrenal adjustments to a hypotensive agent (1-Hydrazinophthal-azine: CIBA BA-5968: Apresoline). J Clin Invest 31: 872, 1952
12. Crosley AP, Rowe GG, Crumpton CW: The hemodynamic andmetabolic response of the human hypertensive kidney to a stan-dard dose of l-Hydrazinophthalazine (hydralazine). J Lab ClinMed 44: 104, 1954
13. Judson WE, Hollander W, Wilkins RW: The effects of exercisein the supine position on cardiovascular and renal function inhypertensive patients before and during chronic oralhydralazine therapy. J Lab Clin Med 49: 672, 1957
14. Crumpton CW, Crosley AP, Rowe GG: The hemodynamic,metabolic and electrolyte responses of the human hypertensivekidney to the intravenous administration of sodium p-SulfamylBenzoate. J Lab Clin Med 42: 797, 1953
15. Falch DK, Qdegaard AE, Norman N: Renal plasma flow andcardiac output during hydralazine and propranolol treatment inessential hypertension. Scand J Clin Lab Invest 38: 143, 1978
16. Gjorup S, Hilden T: The effect of hydralazine (Apresoline) onkidney function and sodium excretion. Scand J Clin Lab Invest8: 273, 1956
17. Stein DH, Hecht HH: Cardiovascular and renal responses tothe combination of hexamethonium and 1-Hydrazinoph-thalazine (Apresoline) in hypertensive subjects. J Clin Invest34: 867, 1955
18. Schroeder HA: The effects of l-hydrazinophthalazine inhypertension. Circulation 5: 28, 1952
19. Moyer JH, Handley CA, Huggins RA: Some phar-macodynamic effects of l-hydrazinophthalazine (C-5968) withparticular reference to renal function and cardiovascularresponse. J Pharmacol Exp Ther 103: 368, 1951
20. Buckalew VM, Puschett JB, Kinitzel JE, Goldberg M:Mechanism of exaggerated natriuesis in hypertensive man: im-paired sodium transport in the loop of Henle. J Clin Invest 48:1007, 1969
21. Cannon PJ: The kidney in heart failure. N Engl J Med 296: 26,1977
22. Werk6 L, Varnauskas E, Ek J, Bucht H, Thomasson B,Bergstrom J, Eliasch H: Studies on the renal circulation andrenal function in mitral valvular disease. II. Effect ofApresoline and noradrenaline. Circulation 9: 700, 1954
23. Judson WE, Hollander W, Wilkins RW: The effects of in-travenous Apresoline (hydralazine) on cardiovascular and renalfunction in patients with and without congestive heart failure.Circulation 13: 664, 1956
24. Packer M, Moller J, Gorlin R, Teichholz L, Herman M: Dose-dependent reduction in right and left ventricular fillingpressures with hydralazine. Am J Cardiol 41: 420, 1978
25. LeJemtel T, Hellman C, Elkayam U, Strom J, Blaufox MD,Frishman W, Ribner H, Sonnenblick E: Hemodynamic andrenal response to oral hydralazine therapy in severe heartfailure. Circulation 56 (suppl III): 111-9, 1977
26. Magorien KD, Triffin D, Desch CE, Unverferth DV, Leier CV:Prazosin and hydralazine in congestive heart failure: drug- anddose-related variations in regional blood flow. Clin Res 27:185A, 1979
27. Cogan J, Humphreys M, Carlson J, Rapaport E: Afterloadreduction increases renal blood flow and maintains glomerularfiltration rate in patients with congestive heart failure. Clin Res27: 3A, 1979
28. Curtiss C, Cohn JN, Vrobel T, Franciosa JA: Role of renin-angiotensin system in the systemic vasoconstriction of chroniccongestive heart failure. Circulation 58: 763, 1978
29. Gavras H, Faxon DP, Berkoben J, Brunner HR, Ryan TJ:Angiotensin converting enzyme inhibition in patients with con-gestive heart failure. Circulation 58: 770, 1978
327
by guest on Novem
ber 5, 2017http://circ.ahajournals.org/
Dow
nloaded from

G L Pierpont, D C Brown, J A Franciosa and J N CohnEffect of hydralazine on renal failure in patients with congestive heart failure.
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1980 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.61.2.323
1980;61:323-327Circulation.
http://circ.ahajournals.org/content/61/2/323.citationthe World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on Novem
ber 5, 2017http://circ.ahajournals.org/
Dow
nloaded from