effect of antibody to capsular polysaccharide on eosinophilic
TRANSCRIPT

1639
Effect of Antibody to Capsular Polysaccharide on Eosinophilic Pneumonia inMurine Infection with Cryptococcus neoformans
Marta Feldmesser, Yvonne Kress, and Arturo Casadevall Departments of Medicine (Division of Infectious Diseases), Pathology,and Microbiology and Immunology, Albert Einstein College of
Medicine, Bronx, New York
The effect of the murine IgG1 monoclonal antibody (MAb) 2H1, which binds to Cryptococcusneoformans glucuronoxylomannan (GXM), on pulmonary infection in immunocompetent C57Bl/6mice was examined. C57Bl/6 mice develop eosinophilic pneumonia in response to pulmonary crypto-coccal infection. Survival, organ fungus burden, serum anticapsular antibody levels, and histopathol-ogy by light and electron microscopy were studied. MAb administration prior to infection prolongedsurvival without reducing the number of yeast in the lung or extrapulmonary sites. Compared withuninfected mice, occasional control and MAb-treated mice produced more IgM antibody to GXMor low levels of GXM-binding IgG1, IgG2b, or IgG3 antibodies. MAb-treated mice had fewer granulesper eosinophil, indicating alteration in eosinophil physiology or degranulation (or both). Our resultsprovide additional evidence that antibody administration can produce quantitative and qualitativechanges in the inflammatory response to a pathogen.
Cryptococcus neoformans is a fungus that causes illness in nous antibody administration, as seen in intravenous models[14, 15].6%–8% of patients with AIDS [1]. The lung is the presumed
portal of entry for this fungus, and its most common clinical Additional immune derangements in A/J mice include de-fects in cellular immunity [16] and in cytokine receptor syn-manifestation is meningoencephalitis [2, 3]. Cell-mediated im-
mune mechanisms provide effective defense against C. neo- thesis in bone marrow progenitor cells [17, 18]. To examinethe possibility that these immune defects contributed toformans [4, 5]. In patients with AIDS, cryptococcal meningoen-
cephalitis is usually incurable and life-long therapy is required MAb-induced alteration of the inflammatory response to in-tratracheal C. neoformans infection, we studied antibody ef-to prevent relapse [6]. Consequently, therapeutic approaches
to enhance the host immune response are being investigated. ficacy in a murine intratracheal model using C57Bl/6 mice,a ‘‘normal’’ strain. An intratracheal model was used becauseTwo strategies are passive antibody administration [7] and vac-
cination with protein-polysaccharide conjugate [8]. human infection is believed to begin in the lung. C57Bl/6mice develop eosinophilic pneumonia in response to crypto-Administration of antibody specific for the capsular polysac-
charide modifies the course of C. neoformans infection in mice coccal infection [19].[9–12]. The mechanism of antibody-mediated protection ispoorly understood. In a prior study of intratracheal infectionin A/JCr mice [13], antibody administration greatly prolonged Materials and Methodssurvival without producing major reduction in tissue colony-
C. neoformans. ATCC strain 24067 (serotype D) cultures wereforming units (cfu). Remarkably, monoclonal antibodyprepared for mouse infection studies exactly as previously de-(MAb)–treated mice had more effective inflammatory re-scribed [13].sponses, suggesting synergy between humoral and cellular im-
MAbs and ELISAs. MAb 2H1 (IgG1) binds to C. neoformansmunity. Since the experiments had been done in C5-deficient
glucuronoxylomannan (GXM) [20]. MAb-containing ascites wasA/JCr mice, a possible explanation for this effect was compen- obtained by paracentesis of pristine-primed BALB/c mice injectedsation for the inflammatory cell recruitment defect by exoge- intraperitoneally with hybridoma cells. For some experiments,
MAb 2H1 was purified by protein G affinity chromatography(Pierce, Rockford, IL). MAb and serum antibody to GXM concen-trations were determined by ELISA relative to isotype-matched
Received 28 August 1997; revised 2 December 1997. standards [21]. Serum concentrations of immunoglobulin to GXMAnimal studies were performed in accordance with animal experimentation were determined in pooled sera from 5 uninfected mice as a con-
guidelines of the Albert Einstein College of Medicine.trol. Because pentavalent IgM antibodies can mask lower-affinityFinancial support: NIH (AI-01341 to M.F., and AI-22774, AI-13342, andIgG antibodies [22], 8 representative samples were incubated withHL-59842 to A.C.); Burroughs Wellcome Fund Developmental Therapeutics
Award (to A.C.). 0.15 M b-mercaptoethanol (in 25 mM Tris, 126 mM NaCl, andReprints or correspondence: Dr. Marta Feldmesser, Albert Einstein College 2.6 mM KCl, pH 7.2) for 1 h at 377C to disrupt IgM. The specific
of Medicine, Golding Bldg. Room 701, 1300 Morris Park Ave., Bronx, NYIgG concentrations were unaltered in these samples, and subclass10461 ([email protected]).determinations were done on untreated serum.
The Journal of Infectious Diseases 1998;177:1639–46Mice. Specific pathogen-free female C57Bl/6 mice (6–10q 1998 by The University of Chicago. All rights reserved.
0022–1899/98/7706–0027$02.00 weeks old) were obtained from the National Cancer Institute
/ 9d46$$ju22 04-08-98 11:07:30 jinfa UC: J Infect
Dow
nloaded from https://academ
ic.oup.com/jid/article-abstract/177/6/1639/2190900 by guest on 15 April 2019

1640 Feldmesser et al. JID 1998;177 (June)
(Bethesda, MD), Jackson Laboratory (Bar Harbor, ME), andCharles River Laboratories (Raleigh, NC). One day before infec-tion with 104 yeast cells, MAb 2H1–treated mice were injectedintraperitoneally with 1 mg of MAb 2H1 in ascites or with 500mg, 1 mg, or 1.5 mg of purified MAb 2H1. Control mice wereinjected with sterile PBS. Intratracheal infections were done asdescribed [13] except that the inocula for the electron microscopy(EM) experiments was 106 to facilitate finding yeast in tissue.
Survival and cfu experiments. Mice were infected, and deathswere recorded daily. On day 175, surviving mice (6 control and10 treated with MAb 2H1) were killed, their lungs were dissected,and the right upper lobe was studied by light microscopy (LM).cfu were determined for the remainder of the lung and for thebrain as described [13]. For cfu experiments, mice were bled fromthe retroorbital sinus and killed by cervical dislocation. In someexperiments, the right upper lobe was fixed in 10% neutral bufferedformalin (Sigma, St. Louis).
LM and lectin histochemistry. In addition to samples obtainedfrom cfu experiments, 8 control and 7 MAb 2H1–treated micewere infected as above, and the lungs were dissected on day 14solely for histopathologic study. Paraffin-embedded tissue sections(4-mm thick) were stained with hematoxylin and eosin or mucic-armine. Tissue lectin histochemistry with peroxidase-conjugatedGriffonia simplicifolia agglutinin B4 isolectin (Sigma) was doneas described [9]. Control sections were incubated in cation buffer.
EM. Four control and 2 MAb 2H1–treated mice were infectedfor EM study. Mice were killed on day 14, and their lungs wereplaced in Trump’s fixative (4% paraformaldehyde and 1% glutaral-dehyde in 0.1 M phosphate buffer) overnight. Tissue was preparedand EM was done as described [19]. Eosinophils were identified Figure 1. Survival of C57Bl/6 mice following intratracheal infec-
tion with 104 C. neoformans strain 24067. P value was obtained byby the presence of cytoplasmic-specific granules with crystallinelog-rank sum analysis.cores. For assessment of eosinophil degranulation,ú100 consecu-
tive eosinophils were imaged for 1 control mouse and 1 MAb2H1–treated mouse in each of two experiments. The number of
compared with surviving control mice, but the difference didprimary, secondary, and small granules per eosinophil was countedfrom photographs of these cells. For 2 control and 1 MAb 2H1– not reach statistical significance (table 1).treated mice, the right middle lobe of the lungs was removed prior cfu experiments. In an initial experiment, MAb administra-to fixation and processed as for LM. tion did not reduce lung or liver cfu. However, MAb 2H1–
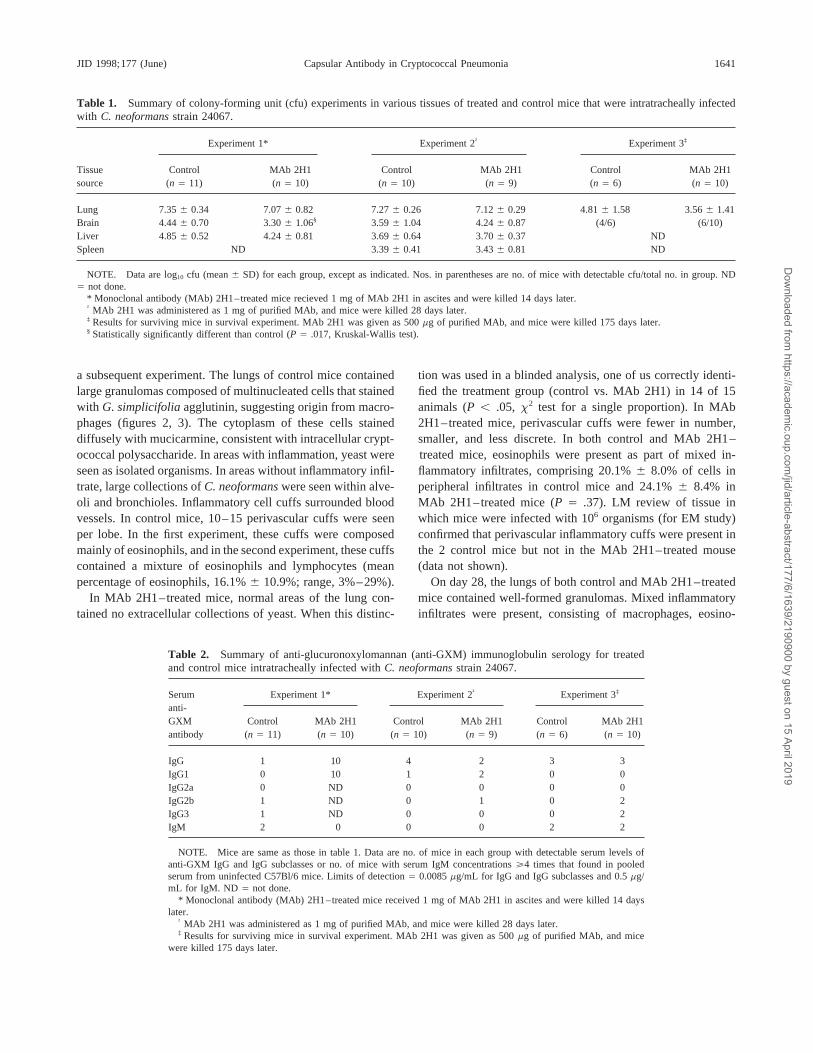
Statistical analysis. Statistical analysis was done using a soft- treated mice had significantly lower brain cfu (table 1, experi-ware program (Primer of Biostatistics: The Program, version 3.01; ment 1). On day 28, there was no difference in cfu in the lung,McGraw-Hill, New York). Nonparametric populations were com- brain, liver, or spleen (table 1, experiment 2). cfu were presentpared by use of the Kruskal-Wallis test. Significance of categorical
in all organs in all mice from both groups with the exceptionvariables was determined by use of Fisher’s exact test. P õ .05
of the spleen of 1 MAb 2H1–treated mouse.was considered statistically significant.Serology. On day 14 after infection, MAb 2H1–treated
mice had measurable serum levels of IgG1 to GXM (experi-ment 1: mean, 22.1 { 31.5 mg/mL) (table 2). From day 28,Resultsadministered IgG1 was no longer detectable. Most mice hadlow serum levels of IgM to GXM (range, õ0.5–22 mg/mL).Survival. Administration of MAb 2H1 to C57Bl/6 mice 1
day prior to infection significantly prolonged the average length Small numbers of mice in each experiment had IgM levels thatwere four times the level found in uninfected serum (2of survival (figure 1). The experiment was stopped on day 175,
at which time all 6 control mice and 6 of the 10 MAb 2H1– mg/mL). Small numbers of mice at each time point producedlow levels of IgG of the IgG1, IgG2b, or IgG3 subclasses;treated mice had detectable lung cfu (limit of detection Å 100
organisms; P Å .23, Fisher’s exact test). Four control and 2 levels were undetectable in uninfected mice. Production of IgGantibody did not correlate with the number of tissue yeast.MAb 2H1–treated mice had detectable brain cfu (P Å .12,
Fisher’s exact test). Three MAb 2H1–treated mice had no cfu LM pathology. On day 14, tissue for pathology was ob-tained for 1 control and 1 MAb 2H1–treated mouse in an initialin either organ. Hence, there was a trend toward reduced num-
bers of mice with detectable cfu in MAb 2H1–treated mice experiment and in 8 control and 7 MAb 2H1–treated mice in
/ 9d46$$ju22 04-08-98 11:07:30 jinfa UC: J Infect
Dow
nloaded from https://academ
ic.oup.com/jid/article-abstract/177/6/1639/2190900 by guest on 15 April 2019
1641JID 1998;177 (June) Capsular Antibody in Cryptococcal Pneumonia
Table 1. Summary of colony-forming unit (cfu) experiments in various tissues of treated and control mice that were intratracheally infectedwith C. neoformans strain 24067.
Experiment 1* Experiment 2† Experiment 3‡
Tissue Control MAb 2H1 Control MAb 2H1 Control MAb 2H1source (n Å 11) (n Å 10) (n Å 10) (n Å 9) (n Å 6) (n Å 10)
Lung 7.35 { 0.34 7.07 { 0.82 7.27 { 0.26 7.12 { 0.29 4.81 { 1.58 3.56 { 1.41Brain 4.44 { 0.70 3.30 { 1.06§ 3.59 { 1.04 4.24 { 0.87 (4/6) (6/10)Liver 4.85 { 0.52 4.24 { 0.81 3.69 { 0.64 3.70 { 0.37 NDSpleen ND 3.39 { 0.41 3.43 { 0.81 ND
NOTE. Data are log10 cfu (mean { SD) for each group, except as indicated. Nos. in parentheses are no. of mice with detectable cfu/total no. in group. NDÅ not done.
* Monoclonal antibody (MAb) 2H1–treated mice recieved 1 mg of MAb 2H1 in ascites and were killed 14 days later.† MAb 2H1 was administered as 1 mg of purified MAb, and mice were killed 28 days later.‡ Results for surviving mice in survival experiment. MAb 2H1 was given as 500 mg of purified MAb, and mice were killed 175 days later.§ Statistically significantly different than control (P Å .017, Kruskal-Wallis test).
a subsequent experiment. The lungs of control mice contained tion was used in a blinded analysis, one of us correctly identi-fied the treatment group (control vs. MAb 2H1) in 14 of 15large granulomas composed of multinucleated cells that stained
with G. simplicifolia agglutinin, suggesting origin from macro- animals (P õ .05, x2 test for a single proportion). In MAb2H1–treated mice, perivascular cuffs were fewer in number,phages (figures 2, 3). The cytoplasm of these cells stained
diffusely with mucicarmine, consistent with intracellular crypt- smaller, and less discrete. In both control and MAb 2H1–treated mice, eosinophils were present as part of mixed in-ococcal polysaccharide. In areas with inflammation, yeast were
seen as isolated organisms. In areas without inflammatory infil- flammatory infiltrates, comprising 20.1% { 8.0% of cells inperipheral infiltrates in control mice and 24.1% { 8.4% intrate, large collections of C. neoformans were seen within alve-
oli and bronchioles. Inflammatory cell cuffs surrounded blood MAb 2H1–treated mice (P Å .37). LM review of tissue inwhich mice were infected with 106 organisms (for EM study)vessels. In control mice, 10–15 perivascular cuffs were seen
per lobe. In the first experiment, these cuffs were composed confirmed that perivascular inflammatory cuffs were present inthe 2 control mice but not in the MAb 2H1–treated mousemainly of eosinophils, and in the second experiment, these cuffs
contained a mixture of eosinophils and lymphocytes (mean (data not shown).On day 28, the lungs of both control and MAb 2H1–treatedpercentage of eosinophils, 16.1% { 10.9%; range, 3%–29%).
In MAb 2H1–treated mice, normal areas of the lung con- mice contained well-formed granulomas. Mixed inflammatoryinfiltrates were present, consisting of macrophages, eosino-tained no extracellular collections of yeast. When this distinc-
Table 2. Summary of anti-glucuronoxylomannan (anti-GXM) immunoglobulin serology for treatedand control mice intratracheally infected with C. neoformans strain 24067.
Serum Experiment 1* Experiment 2† Experiment 3‡
anti-GXM Control MAb 2H1 Control MAb 2H1 Control MAb 2H1antibody (n Å 11) (n Å 10) (n Å 10) (n Å 9) (n Å 6) (n Å 10)
IgG 1 10 4 2 3 3IgG1 0 10 1 2 0 0IgG2a 0 ND 0 0 0 0IgG2b 1 ND 0 1 0 2IgG3 1 ND 0 0 0 2IgM 2 0 0 0 2 2
NOTE. Mice are same as those in table 1. Data are no. of mice in each group with detectable serum levels ofanti-GXM IgG and IgG subclasses or no. of mice with serum IgM concentrations §4 times that found in pooledserum from uninfected C57Bl/6 mice. Limits of detection Å 0.0085 mg/mL for IgG and IgG subclasses and 0.5 mg/mL for IgM. ND Å not done.
* Monoclonal antibody (MAb) 2H1–treated mice received 1 mg of MAb 2H1 in ascites and were killed 14 dayslater.
† MAb 2H1 was administered as 1 mg of purified MAb, and mice were killed 28 days later.‡ Results for surviving mice in survival experiment. MAb 2H1 was given as 500 mg of purified MAb, and mice
were killed 175 days later.
/ 9d46$$ju22 04-08-98 11:07:30 jinfa UC: J Infect
Dow
nloaded from https://academ
ic.oup.com/jid/article-abstract/177/6/1639/2190900 by guest on 15 April 2019

1642 Feldmesser et al. JID 1998;177 (June)
Figure 2. Histology of cryptococ-cal infection in lung by light micros-copy. A, Control mouse, day 14.Granulomatous inflammation is seenwith perivascular cuffs (arrow). Col-lections of extracellular organisms(*) widely infect airspace (1100). B,Control mouse, day 14. Inflamma-tory cell cuffs, composed mainly ofeosinophils and lymphocytes, sur-round blood vessels (arrows)(1200). C, MAb 2H1–treatedmouse, day 14. Granulomatous in-flammation with less diffuse appear-ance of cryptococci in airspaces(1100). D, MAb 2H1–treatedmouse, day 14. Arrow shows mostprominent perivascular inflamma-tory cell collection found (1200). E,Control mouse, day 28. Inflamma-tory response is more prominent thanon day 14, but large collections ofyeast are present in areas with littleinflammation. Arrowhead points to1 of many extracellular yeast(1200). F, MAb 2H1–treatedmouse, day 28. Cryptococci are con-tained within inflammatory foci. Ar-rowhead points to intracellularcryptococci (1200). G, Controlmouse, day 175. Less extensive lunginflammation is seen, although re-solving granulomas and collectionsof inflammatory cells are present(1100). H, Control mouse, day 175.Higher magnification of area en-closed in rectangle in G shows cellsin inflammatory collections to con-sist mostly of lymphocytes, in whichyeast were not seen (1400).
phils, neutrophils and lymphocytes. In 1 of 3 control mice On day 175, the portions of lung reserved for histologicstudy for 5 of the 6 control mice appeared normal, which mayand 1 of the 3 MAb 2H1–treated mice, large collections of
lymphocytes surrounded blood vessels. Collections of eosino- reflect sampling error. The lung of the sixth mouse had resolv-ing granulomas and many collections of lymphocytes, most ofphils were seen in control mice, but these no longer surrounded
blood vessels. In MAb 2H1–treated mice, large numbers of which surrounded blood vessels. The lungs of 7 of the 10MAb 2H1–treated mice contained similar dense collections ofeosinophils were present diffusely in areas of inflammation.
In control mice, organisms were found outside of areas of lymphocytes near areas of resolving granulomas, most of whichsurrounded blood vessels. Although lung cfu were present ininflammation and extending through large areas of intercon-
necting airspaces, while in MAb 2H1–treated mice, organisms all of these mice, no yeast were seen in the sections obtainedfor histology for any of the control or MAb 2H1–treated mice,were contained within inflammatory foci.
/ 9d46$$ju22 04-08-98 11:07:30 jinfa UC: J Infect
Dow
nloaded from https://academ
ic.oup.com/jid/article-abstract/177/6/1639/2190900 by guest on 15 April 2019

1643JID 1998;177 (June) Capsular Antibody in Cryptococcal Pneumonia
Figure 3. Control mouse, day 14.Immunohistochemistry shows largecell containing many cryptococcithat stain prominently with Griffoniasimplicifolia agglutinin, indicatingthat it is of macrophage origin(11000).
suggesting that these mice were resolving their pulmonary in- discrete than those in MAb 2H1–treated mice. Since the pres-ence of perivascular collections probably precedes the dispersalfections.of inflammatory cells in tissue, MAb administration mayEM pathology. At day 14 of infection, large numbers ofimprove the ability of inflammatory cells to reach infectiousintra- and extracellular yeast were present. Intracellular organ-foci. Ultrastructural analysis demonstrated that eosinophils inisms were within large multinucleated cells, which appearedMAb-treated mice contained fewer granules. The differenceto be of macrophage origin (figure 4). Numerous eosinophilsin granule number was not due to differences in endogenouswere present in inflammatory foci. Many macrophages andproduction of antibody to GXM. Hence, the mechanism ofeosinophils appeared to be dead in both groups, with pyknoticantibody-mediated protection is probably not limited to restora-nuclei and cell membrane disruption. Several eosinophils intion of the chemotactic activity missing from complement-each group contained specific granules with hyperlucent centraldeficient mice. Potential mechanisms of MAb action includecores, indicating selective loss of core protein. Some eosino-removal of GXM, which has both immunosuppressive andphils contained free granule cores in the cytoplasm. Eosinophilstoxic properties [23–28]; alterations in antigen presentationin MAb 2H1–treated mice contained significantly fewer gran-[29, 30]; alterations in cytokine expression causing differentules (table 3), consistent with more degranulation in these mice.recruitment of inflammatory cells [31]; and enhanced macro-phage antifungal activity [32]. The present study does not ad-Discussiondress these possibilities, which are areas for future study.
As seen with A/JCr mice, MAb administration to C57Bl/6 Specific antibody is required for eosinophil effector func-mice prior to infection prolonged survival without reducing cfu tions against several parasites [33–35]. Eosinophil Fcg recep-in the lung or extrapulmonary sites. Prolongation of survival tor expression is modified by cytokines and the state of eosino-without an early reduction in cfu suggests that antibody is phil activation [36–39]. In vitro, antibody binding to Fcgacting indirectly and may be enhancing cell-mediated immu- receptors can promote eosinophil degranulation, with releasenity. While MAb 2H1 administration did not produce a major of inflammatory mediators and cationic proteins [40–43]. Ef-reduction in cfu at early times after infection, control mice that forts to determine whether eosinophil degranulation occurs indied from their infection likely had higher levels of cfu than response to antibody in vivo have been inconclusive [44, 45].those that survived. Had these mice been included in the later Our study provides the first evidence that systemic administra-cfu data, a difference may have been demonstrable. As seen tion of IgG1 to mice may result in eosinophil degranulation inwith the A/JCr strain, MAb 2H1 administered to C57Bl/6 mice vivo. The presence of free intracytoplasmic specific granulequalitatively and quantitatively altered the inflammatory re- cores and specific granules that lacked cores suggests that thesponse. one-third reduction in the number of granules seen in MAb
LM study showed perivascular inflammatory cell cuffs in 2H1–treated mice resulted from increased degranulation. Al-ternatively, administration of systemic IgG1 may have blockedlungs of control mice that were fewer in number and less
/ 9d46$$ju22 04-08-98 11:07:30 jinfa UC: J Infect
Dow
nloaded from https://academ
ic.oup.com/jid/article-abstract/177/6/1639/2190900 by guest on 15 April 2019

1644 Feldmesser et al. JID 1998;177 (June)
Figure 4. Electron micrograph of control mouse lung on day 14 of infection. A, Large multinucleated cells containing multiple cryptococci(C) are in region of inflammation. N, cell nuclei. B, Large necrotic cell with disrupted cytoplasm and rounded nucleus (N) bordered by largeno. of eosinophils (X). Cryptococci (C) are inside phagosomes. 12000.
the increase in small granule numbers, as seen in a variety of eosinophils are not usually described as major components ofthe inflammatory response, although they have been found inconditions [46–48]. We cannot distinguish between these twothe cerebral spinal fluid of patients with cryptococcal meningi-possibilities.tis [52, 53], in pleural effusions [54], and in an epidural abscessThe role of eosinophils in cryptococcal infection is unknown.[55] due to C. neoformans infection. Peripheral blood eosino-While eosinophil granule products are potentially toxic tophilia with C. neoformans pulmonary infection has been re-cryptococci, the finding of similar cfu in control and MAbported [54, 56]. Direct histologic comparison is not appropriate,2H1–treated mice suggests that direct fungal toxicity is not ahowever, as rodent models represent primary acute infection,major result of eosinophil degranulation. Alternatively, en-a phase not typically seen in human pathologic specimens.hanced degranulation in the presence of IgG1 MAb may be aFurthermore, human tissue is often obtained from patients whomechanism for toxicity, since eosinophil products are toxicreceived antifungal therapy, which may alter cellular recruit-to respiratory epithelium [49–51]. In human cryptococcosis,ment, or from autopsy specimens, which demonstrate end-stagedisease.
Most mice had measurable IgM to GXM from 14 days afterTable 3. Eosinophil degranulation in monoclonal antibody (MAb)–infection (data not shown). The low titer of IgM to GXM intreated mice.noninfected mice likely represents antibody cross-reactive with
No. of granules per eosinophil cryptococcal polysaccharide [57], since specific pathogen–freemice were used. Small numbers of mice made specific IgG
Experiment 1 Experiment 2antibodies to GXM. Similar numbers of control and MAb 2H1–treated mice produced similar antibody responses to infection,Control 28.2 { 14.2 30.3 { 13.8suggesting that differences in eosinophil granule number do notMAb-treated 20.5 { 13.3 23.5 { 13.6
P õ.001 õ.001 result from different levels of endogenous antibody to GXM.In summary, systemic administration of anticapsular IgG1
NOTE. Data are mean no. of granules inú100 eosinophils { SD. Eosino-prolonged survival in immunocompetent C57Bl/6 mice, dem-phils were counted for 1 mouse in each group in 2 separate experiments. P
values were obtained by 2-tailed Students t test. onstrating that passive antibody efficacy in pulmonary infection
/ 9d46$$ju22 04-08-98 11:07:30 jinfa UC: J Infect
Dow
nloaded from https://academ
ic.oup.com/jid/article-abstract/177/6/1639/2190900 by guest on 15 April 2019

1645JID 1998;177 (June) Capsular Antibody in Cryptococcal Pneumonia
17. Leslie KB, Jalbert S, Orban P, Welham M, Duronio V, Schrader JW.is not limited to complement-deficient mice. In mice givenGenetic basis of hypo-responsiveness of A/J mice to interleukin-3.anticapsular IgG1, yeast were contained within inflammatoryBlood 1996;87:3186–94.
foci and eosinophils had fewer granules. Our findings reinforce 18. Ichihara M, Hara T, Takagi M, Cho LC, Gorman DM, Miyajima A.the concept that the presence of specific antibody can influence Impaired interleukin-3 (IL-3) response of the A/J mouse is caused by
a branch point deletion in the IL-3 receptor a subunit gene. EMBO Jthe inflammatory response and provide support for the potential1995;14:939–50.usefulness of humoral immunity in prevention and therapy of
19. Feldmesser M, Casadevall A, Kress Y, Spira G, Orlofsky A. Eosinophil–cryptococcosis.Cryptococcus neoformans interactions in vivo and in vitro. Infect Im-mun 1997;65:1899–907.
20. Casadevall A, Mukherjee J, Devi SJN, Schneerson R, Robbins JB, ScharffAcknowledgments
MD. Antibodies elicited by a Cryptococcus neoformans–tetanus toxoidconjugate vaccine have the same specificity as those elicited in infection.We thank Jorge Bermudez for outstanding preparation of histo-J Infect Dis 1992;165:1086–93.pathology specimens, Lin-Chi Chen for providing uninfected
21. Casadevall A, Scharff MD. The mouse antibody response to infection withC57Bl/6 serum, and Sunhee Lee for many valuable discussions. Cryptococcus neoformans: VH and VL usage in polysaccharide binding
antibodies. J Exp Med 1991;174:151–60.22. DeShaw M, Pirofski LA. Antibodies to the Cryptococcus neoformans
References capsular glucuronoxylomannan are ubiquitous in serum from HIV/ andHIV0 individuals. Clin Exp Immunol 1995;99:425–32.1. Currie BP, Casadevall A. Estimation of the prevalence of cryptococcal
23. Dong ZM, Murphy JW. Cryptococcal polysaccharides induce L-selectininfection among patients infected with the human immunodeficiencyshedding and tumor necrosis factor receptor loss from the surface ofvirus in New York City. Clin Infect Dis 1994;19:1029–33.human neutrophils. J Clin Invest 1996;97:689–98.2. Levitz SM. The ecology of Cryptococcus neoformans and the epidemiol-
24. Dong ZM, Murphy JW. Effects of the two varieties of Cryptococcusogy of cryptococcosis. Rev Infect Dis 1991;13:1163–9.neoformans cells and culture filtrate antigens on neutrophil locomotion.3. Mitchell TG, Perfect JR. Cryptococcosis in the era of AIDS—100 yearsInfect Immun 1995;63:2632–44.after the discovery of Cryptococcus neoformans. Clin Microbiol Rev
25. Hirano A, Zimmerman HM, Levine S. Fine structure of cerebral fluid1995;8:515–48.accumulation. Arch Neurol 1965;12:189–96.4. Murphy JW. Cryptococcal immunity and immunostimulation. Adv Exp
26. Drouhet E, Dupont B. Mycoses iatrogenes a localisation profonde duesMed Biol 1992;319:225–30.a des champignons levuriformes opportunistes. Dermatologica 1979;5. Graybill JR, Alford RH. Cell-mediated immunity in cryptococcosis. Cell159(suppl 1):94–112.Immunol 1974;14:12–21.
27. Murphy JW, Cozad GC. Immunological unresponsiveness induced by6. Zuger A, Louie E, Holzman RS, Simberkoff MS, Rahal JJ. Cryptococcalcryptococcal capsular polysaccharide assayed by the hemolytic plaquedisease in patients with the acquired immunodeficiency syndrome. Anntechnique. Infect Immun 1972;5:896–901.Intern Med 1986;104:234–40.
28. Blackstock R. Cryptococcal capsular polysaccharide utilizes an antigen-7. Zebedee SL, Koduri RK, Mukherjee J, et al. Mouse-human immunoglobu-presenting cell to induce a T-suppressor cell to secrete TsF. J Med Vetlin G1 chimeric antibodies with activities against Cryptococcus neo-Mycol 1996;34:19–30.
formans. Antimicrob Agents Chemother 1994;38:1507–14.29. Vecchiarelli A, Retini C, Casadevall A, Bistoni F. Monoclonal antibody
8. Devi SJN, Schneerson R, Egan W, et al. Cryptococcus neoformans sero-to Cryptococcus neoformans glucuronoxylomannan enhances antigen-
type A glucuronoxylomannan-protein conjugate vaccines: synthesis,presenting capacity of human monocytes [abstract 2.4]. In: Program
characterization, and immunogenicity. Infect Immun 1991;59:3700–7.and abstracts of the Third International Conference on Cryptococcus
9. Mukherjee S, Lee S, Mukherjee J, Scharff MD, Casadevall A. Monoclonaland Cryptococcosis (Paris). Paris: Institut Pasteur, 1996:162.
antibodies to Cryptococcus neoformans capsular polysaccharide modify30. Mody CH, Syme RM. Antigen processing and presentation of Cryptococ-
the course of intravenous infection in mice. Infect Immun 1994;62:cus neoformans [abstract IV.4]. In: Program and abstracts of the Third
1079–88.International Conference on Cryptococcus and Cryptococcosis (Paris).
10. Mukherjee J, Scharff MD, Casadevall A. Protective murine monoclonal Paris: Institut Pasteur, 1996:88–9.antibodies to Cryptococcus neoformans. Infect Immun 1992;60: 31. Feldmesser M, Casadevall A. Cytokine response to Cryptococcus neo-4534–41. formans in murine pulmonary infection [abstract 129]. In: Program and
11. Dromer F, Charreire J, Contrepois A, Carbon C, Yeni P. Protection of mice abstracts of the 35th Annual Meeting of the Infectious Diseases Societyagainst experimental cryptococcosis by anti–Cryptococcus neoformans of America (San Francisco). Alexandria, VA: IDSA, 1997:95.monoclonal antibody. Infect Immun 1987;55:749–52. 32. Mukherjee S, Lee SC, Casadevall A. Antibodies to Cryptococcus neo-
12. Mukherjee J, Pirofski L, Scharff MD, Casadevall A. Antibody-mediated formans glucuronoxylomannan enhance antifungal activity of murineprotection in mice with lethal intracerebral Cryptococcus neoformans macrophages. Infect Immun 1995;63:573–9.infection. Proc Natl Acad Sci USA 1993;90:3636–40. 33. De Azevedo NL, De Souza W. An ultrastructural and cytochemical study
13. Feldmesser M, Casadevall A. Effect of serum IgG1 to Cryptococcus neo- of Tritrichomonas foetus–eosinophil interaction. J Submicrosc Cytolformans glucuronoxylomannan on murine pulmonary infection. J Immu- Pathol 1996;28:243–9.nol 1997;158:790–9. 34. Sanderson CJ, De Souza W. A morphological study of the interaction
14. Dromer F, Perronne C, Barge J, Vilde JL, Yeni P. Role of IgG and between Trypanosoma cruzi and rat eosinophils, neutrophils and macro-complement component C5 in the initial course of experimental crypto- phages in vitro. J Cell Sci 1979;37:275–86.coccosis. Clin Exp Immunol 1989;78:412–7. 35. Butterworth AE, Remold HG, Houba V, et al. Antibody-dependent eosino-
15. Rhodes JC. Contribution of complement component C5 to the pathogenesis phil-mediated damage to 51CR-labeled schistosomula of Schistosomaof experimental murine cryptococcosis. Sabouraudia. 1985;23:225–34. mansoni: mediation by IgG and inhibition by antigen-antibody com-
16. Boraschi D, Meltzer MS. Defective tumoricidal capacity of macrophages plexes. J Immunol 1977;118:2230–6.from A/J mice I. Characterization of the macrophage cytotoxic defect 36. De Andres B, Cardaba B, Del Pozo V, et al. Modulation of the FcgII andafter in vivo and in vitro activation stimuli. J Immunol 1979;122: FcgIII induced by GM-CSF, IFN-g and IL-4 on murine eosinophils.
Immunol 1994;83:155–60.1587–91.
/ 9d46$$ju22 04-08-98 11:07:30 jinfa UC: J Infect
Dow
nloaded from https://academ
ic.oup.com/jid/article-abstract/177/6/1639/2190900 by guest on 15 April 2019

1646 Feldmesser et al. JID 1998;177 (June)
37. Valerius T, Repp R, Kalden JR, Platzer E. Effects of IFN on human 48. Dvorak AM, Monahan RA, Osage JE, Dickersin GR. Crohn’s disease:transmission electron microscopic studies II. Immunologic inflamma-eosinophils in comparison with other cytokines. A novel class of eosino-
phil activators with delayed onset of action. J Immunol 1990;145: tory response. Alterations of mast cells, basophils, eosinophils, and themicrovasculature. Hum Pathol 1980;11:606–19.2950–8.
38. Hartnell A, Kay AB, Wardlaw AJ. IFN-g induces expression of FcgRIII 49. Gleich GJ, Frigas E, Loegering DA, Wasson DL, Steinmuller D. Cytotoxicproperties of the eosinophil major basic protein. J Immunol 1979;123:(CD16) on human eosinophils. J Immunol 1992;148:1471–8.
39. Graziano RF, Looney RJ, Shen L, Fanger MW. FcgR-mediated killing by 2925–7.50. Davis WB, Fells GA, Sun X, Gadek Je, Venet A, Crystal RG. Eosinophil-eosinophils. J Immunol 1989;142:230–5.
40. Shaw RJ, Walsh GM, Cromwell O, Moqbel R, Spry CJF, Kay AB. Acti- mediated injury to lung parenchymal cells and interstitial matrix Apossible role for eosinophils in chronic inflammatory disorders of thevated human eosinophils generate SRS-A leukotrienes following IgG-
dependent stimulation. Nature 1985;316:150–2. lower respiratory tract. J Clin Invest 1984;74:269–78.51. De Monchy JGR, Kauffman HF, Venge P, et al. Bronchoalveolar eosino-41. Abu-Ghazaleh RI, Fujisawa T, Mestecky J, Kyle RA, Gleich GJ. IgA-
induced eosinophil degranulation. J Immunol 1989;142:2393–400. philia during allergen-induced late asthmatic reactions. Am Rev RespirDis 1985;131:373–6.42. Tomassini M, Tsicopoulos A, Tai PC, et al. Release of granule proteins
by eosinophils from allergic and nonallergic patients with eosinophilia 52. Muller W, Schorre W, Suchenwirth R, Zitz HM, Konorza G. A caseof fatal cryptococcal meningitis with intraventricular granuloma. Actaon immunoglobulin-dependent activation. J Allergy Clin Immunol
1991;88:365–75. Neurochir 1978;44:223–35.53. Anderson P, Macklis J, Brown M, Ory D. Eosinophilic cerebrospinal fluid43. Baskar P, Silberstein DS, Pincus SH. Inhibition of IgG-triggered human
eosinophil function by IL-4. J Immunol 1990;144:2321–6. pleocytosis and cryptococcal meningitis. Ann Intern Med 1985;103:306–7.44. Boomars KA, van Velzen-Blad H, Mulder PGH, Koenderman L, Lammers
JJ, van den Bosch JMM. Eosinophil cationic protein and immunoglobu- 54. Epstein R, Cole R, Hunt KK Jr. Pleural effusion secondary to pulmonarycryptococcosis. Chest 1972;61:296–8.lin levels in bronchoalveolar lavage fluid obtained from patients with
chronic eosinophilic pneumonia. Eur Respir J 1996;9:2488–93. 55. Brewer GE, Wood FC. Blastomycosis of the spine. Ann Surg 1908;48:889–96.45. Terada N, Konno A, Tada H, Shirotori K, Ishikawa K, Togawa K. The
effect of recombinant human interleukin-5 on eosinophil accumulation 56. Jensen WA, Rose RM, Hammer SM, Karchmer AW. Serologic diagnosisof focal pneumonia caused by Cryptococcus neoformans. Am Rev Re-and degranulation in human nasal mucosa. J Allergy Clin Immunol
1992;90:160–8. spir Dis 1985;132:189–91.57. Houpt DC, Pfrommer GST, Young BJ, Larson TA, Kozel TR. Occur-46. Komiyama A, Spicer SS. Microendocytosis in eosinophilic leukocytes. J
Cell Biol 1975;64:622–35. rences, immunoglobulin classes, and biological activities of antibodiesin normal human serum that are reactive with Cryptococcus neoformans47. Parmley RT, Spicer SS. Altered tissue eosinophils in Hodgkin’s disease.
Exp Mol Pathol 1975;23:70–82. glucuronoxylomannan. Infect Immun 1994;62:2857–64.
/ 9d46$$ju22 04-08-98 11:07:30 jinfa UC: J Infect
Dow
nloaded from https://academ
ic.oup.com/jid/article-abstract/177/6/1639/2190900 by guest on 15 April 2019