住院患者的血糖控制 - ylshb.gov.t · outline 1. frequency of hyperglycemia in non-critical...
TRANSCRIPT

住院患者的血糖控制
台大雲林分院 代謝內分泌科
賴瑩純醫師

Outline
1. Frequency of hyperglycemia in non-critical care setting
2. The association between hyperglycemia and outcome
3. Diagnosis and Recognition of Hyperglycemia and Diabetes
4. Glycemia Target
5. Management of Hyperglycemia
6. Hypoglycemia
Umpierrez et al. J Clin Endocrinol Metabol. 97(1): 16-38, 2012
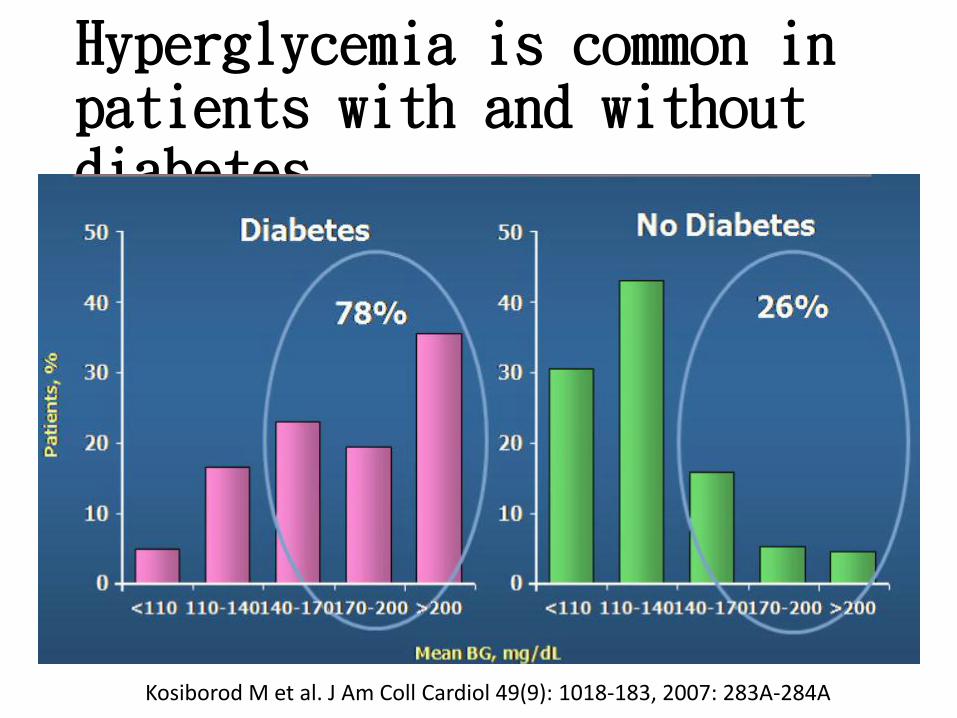
Hyperglycemia is common in patients with and without diabetes
Kosiborod M et al. J Am Coll Cardiol 49(9): 1018-183, 2007: 283A-284A

Hyperglycemia: A common Comorbidity in Medical-
Surgical P’t
[百分
比]
[百分
比]
[百分
比]
2
Normoglycemia
Known Diabetes
New Hyperglycemia
Umpierrez G et al, J Clin Endocrinol Metabol 87:978, 2002
New hyperglycemia: FPG≥ 126 mg/dl random blood glucose level ≥ 200 mg/dl X2N=2,020
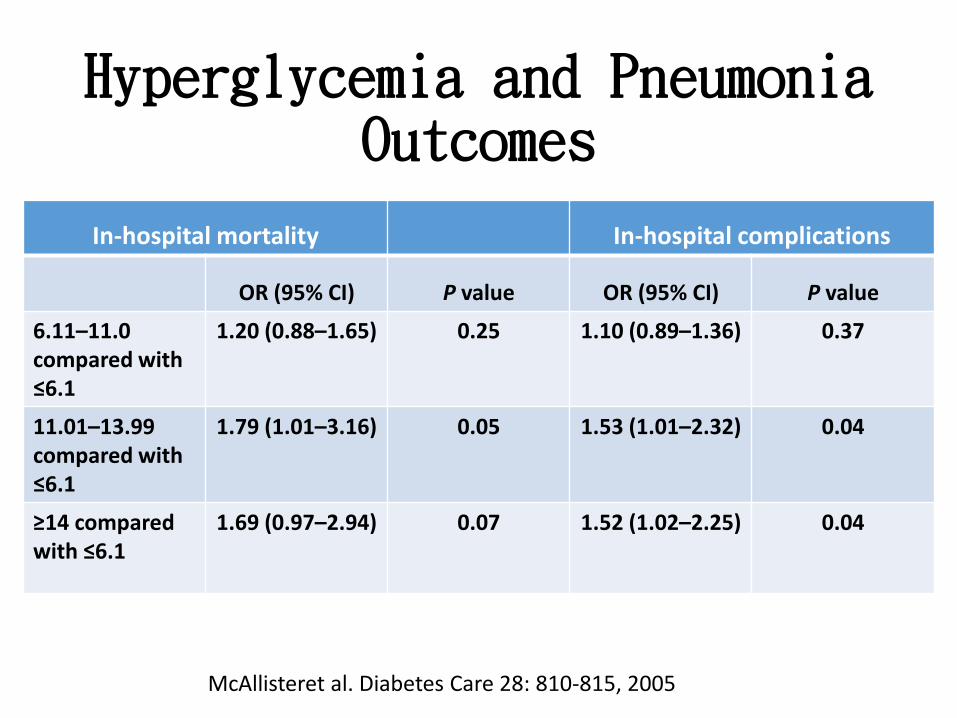
Hyperglycemia and Pneumonia Outcomes
McAllisteret al. Diabetes Care 28: 810-815, 2005
In-hospital mortality In-hospital complications
OR (95% CI) P value OR (95% CI) P value
6.11–11.0 compared with ≤6.1
1.20 (0.88–1.65) 0.25 1.10 (0.89–1.36) 0.37
11.01–13.99 compared with ≤6.1
1.79 (1.01–3.16) 0.05 1.53 (1.01–2.32) 0.04
≥14 compared with ≤6.1
1.69 (0.97–2.94) 0.07 1.52 (1.02–2.25) 0.04

Thirty-day mortality and in-hospital complication rates in patients with and without diabetes:
blood infection (combined bacteriemia and sepsis); urinary tract infection (UTI), acute
myocardial infarction (AMI), and ARF. *P < 0.001; †NS; ‡P < 0.017.
Frisch A et al. Dia Care 2010;33:1783-1788
Copyright © 2011 American Diabetes Association, Inc.

Hospital Mortality and Mean Glucose in Patient with AMI
Kosiborod M al. al CIrculation 117:1018, 2008
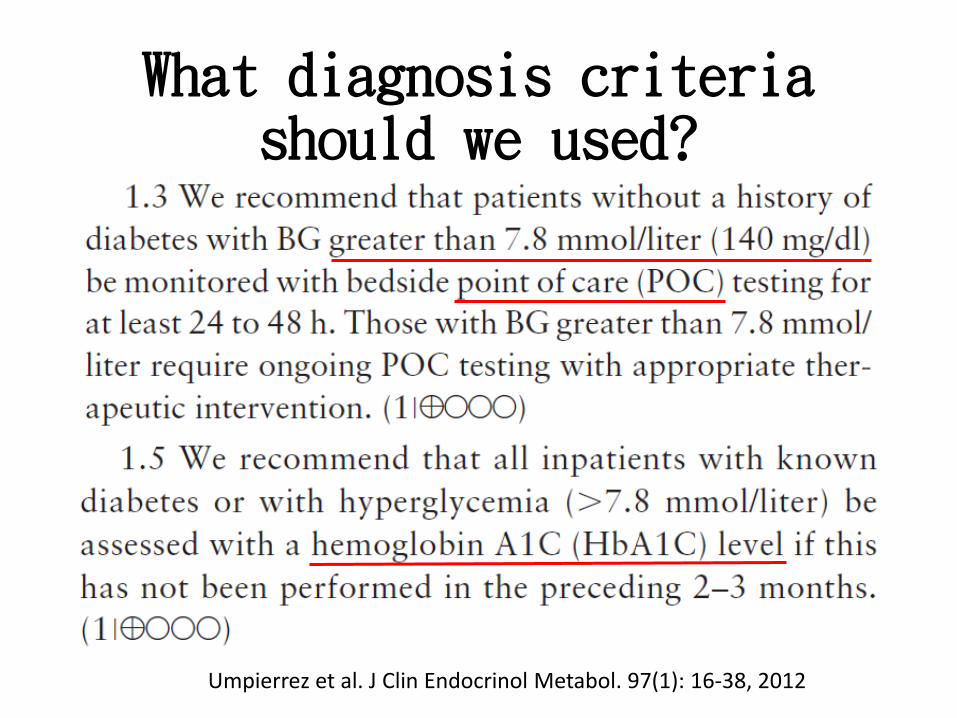
What diagnosis criteria should we used?
Umpierrez et al. J Clin Endocrinol Metabol. 97(1): 16-38, 2012
Factors influencing HbA1c
• Hemoglobinopathies
• High-dose salicylates
• Hemodialysis
• Blood transfusion
• Iron deficiency anemia
• Analysis : National GlycohemoglobinStandardization Program
J Clin Endocrinol Metabol. 97(7): 2447-2453, 2008

Glycemic Targets in Non-ICU P’t
AACE/ADA guideline• Premeal glucose < 140 mg/dL• Random blood glucose (BG) <180 mg/dL• To avoid of hypoglycemia, reassess insulin
regimen if BG levels fall below 100 mg/dL

Achieving Glycemic Goal in Non-ICU setting

Management of Hyperglycemia in Non-Critical setting
Insulin Therapy:•Sliding scale short-acting insulin•Basal/bolus therapy
•NPH and regular insulin•Long-acting and rapid acting insulin analogs

Randomized study of basal-bolus insulin therapy in the inpatient management of patients with type 2
diabetes (RABBIT 2 trial).• DC oral antidiabetic drugs on admission
• Starting total daily dose (TDD):
0.4 U/kg/d x BG between 140-200 mg/dL
0.5 U/kg/d X BG between 201-400 mg/dL
• Half of TDD as insulin glargine and half as rapid-acting insulin (glulisine)
Insulin glargine- once daily, at the same timeday
Glulisine- three equally divided dose (AC)
Umpierrez G E et al. Dia Care 2007;30:2181-2186

Clinical Diabetes Volume 29, Number1, 2011

Sliding Scale Insulin Regimen
BG (mg/dl) Insulin-sensitive
Usual Insulin resistance
>141-180 2 4 6
181-220 4 6 8
221-261 6 8 10
261-300 8 10 12
301-350 10 12 14
351-400 12 14 16
>400 14 16 18
Premeal: add to scheduled insulin doseBedtime: give half of SSI

glargine plus glulisine (•)
SSI (○). *P < 0.01; ¶P < 0.05.
Umpierrez G E et al. Dia Care 2007;30:2181-2186
Copyright © 2011 American Diabetes Association, Inc.

Umpierrez G E et al. Dia Care 2007;30:2181-2186
Copyright © 2011 American Diabetes Association, Inc.

Insulin Dose and Hypoglycemia
Basal bolus Group
SSI group
Glargine 22 ± 2 units/d -
Glulisine/RI 20 ± 1 units/d 12.5 ± 2 units/d
BG< 60 0.4 % 0.2%
BG<40 0 0

RABBIT Surgery
Umpierrez G E et al. Dia Care 2011, 34(2):1-6

Medical Nutrition Therapy (MNT)
Most patients receive 1500-2000 calories/day, with range of 12-15 carbohydrate servings
Special Situations
1. Transition from Intravenous Continuous Insulin Infusion (CII) to Subcutaneous Insulin Therapy
2. Patients Receiving Enteral or Parenteral Nutrition
3. Perioperative Blood Glucose Control4. Glucocorticoid-induced Diabetes
Hypoglycemia
• Definition: BG< 70 mg/dL
• Frequency: 3-30 % (serious events: 4%)
• Risk factors: older age, illness, BW loss, renal failure, Insulin or OAD treatment, missed meal, failure to adjust therapy..

Suggested Nurse-Initiated Strategies for Treating
Hypoglycemi• BG<70 mg/dL, P’t alert and able to eat
15-20 g rapid acting carbohydrate
• BG<70 mg/dL, P’t alsert but NPO
20ml 50% dextrose iv , then 5% dextrose 100ml/h
• BG<70 mg/dL, conscious change
25ml 50% dextrose iv , then 5% dextrose 100ml/h
• BG<70 mg/dL, conscious change, no IV cath
IM 1mg glucagon, two times
Repeat treat every 15 min until BG> 80 mg/dL

Discharge Insulin Algorithm
Discharge Treatment
A1C <7 % A1C 7-9 % A1C >9 %
Re-Start outpatient
treatment (OAD and/or insulin
Re-Start outpatient oral agent and on
glaargine once daily 50-80 % of
hospital dose
Basal bolus at same hospital dose
Alternative: Re-Start outpatient oral agent and on
glaargine once daily 50-80 % of
hospital dose

Patient Education
• Survival skills:
1. Basic meal planning
2. Medication administration
3. BG monitor
4. Hypoglycemia and hyperglycemia detection, treatment and prevention

Thank you for your attention